PATHOLOGY FINDINGS ON PEPTIC ULCER
DYAH FAUZIAHDepartment of Anatomical Pathology
Faculty of Medicine, Universitas Airlangga / Dr. Soetomo Hospital
Surabaya
INTRODUCTION
• Gastric ulcer: loss of the entire mucosa, including muscularis mucosae. May extend deep into submucosa and muscularis propia.
• Erosion ≠ Ulcer
• Gastric Ulcers
– Peptic ulcers
– Acute stress ulcers
– Tumors (benign & malignant)
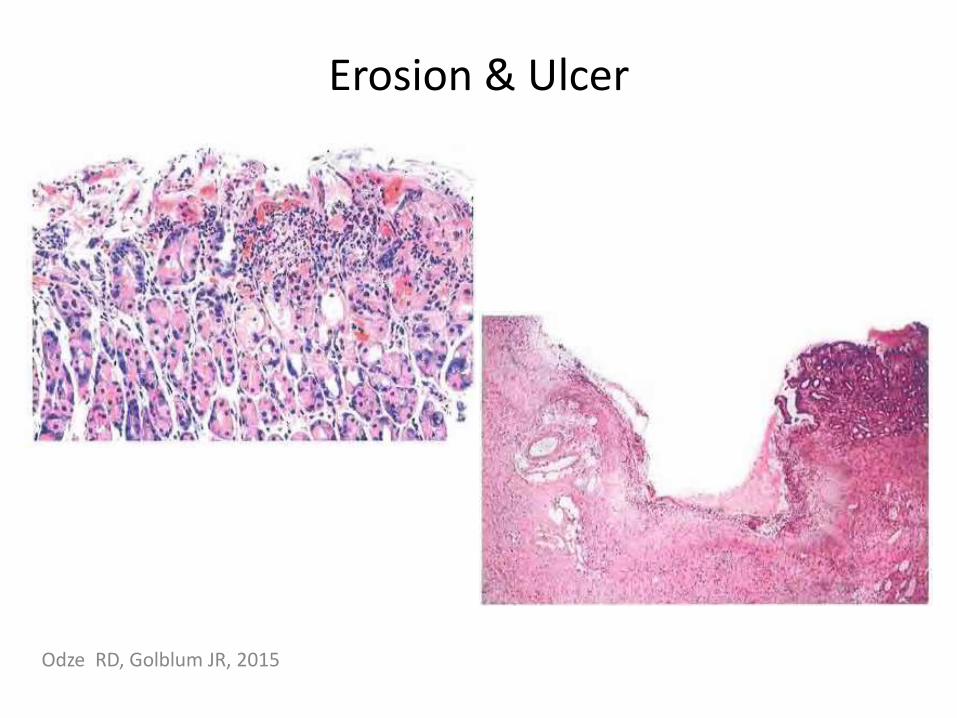
Erosion & Ulcer
Odze RD, Golblum JR, 2015
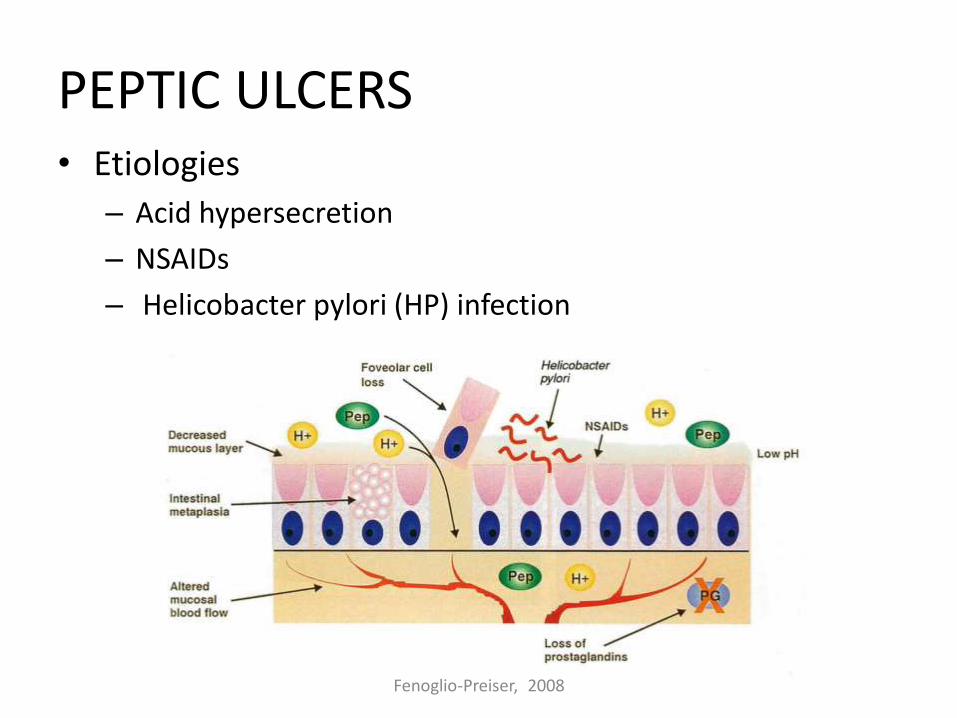
PEPTIC ULCERS• Etiologies
– Acid hypersecretion
– NSAIDs
– Helicobacter pylori (HP) infection
Fenoglio-Preiser, 2008
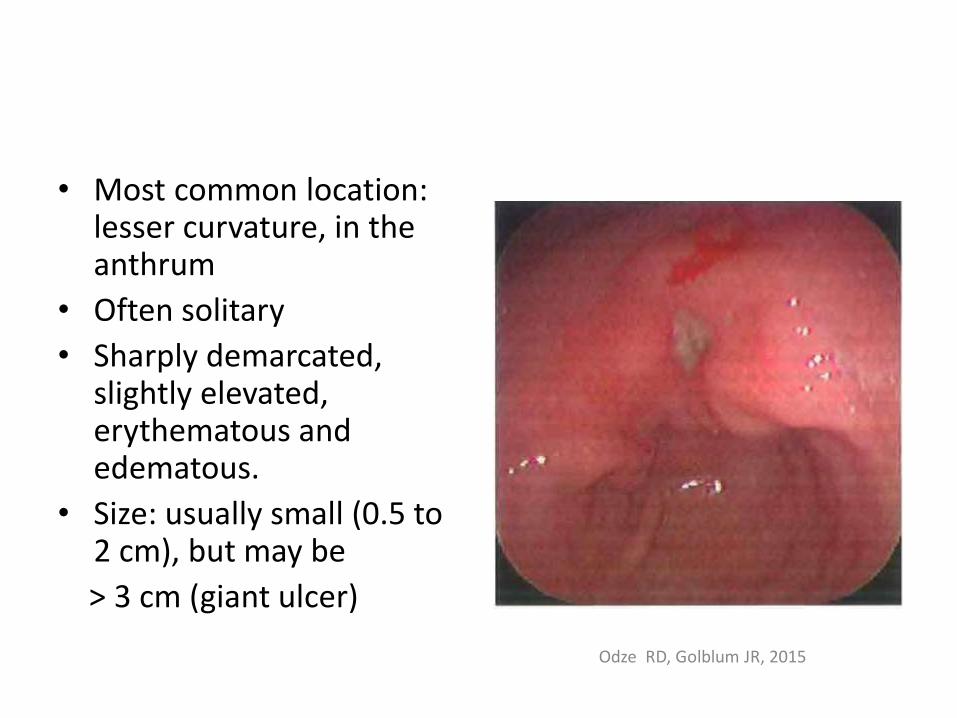
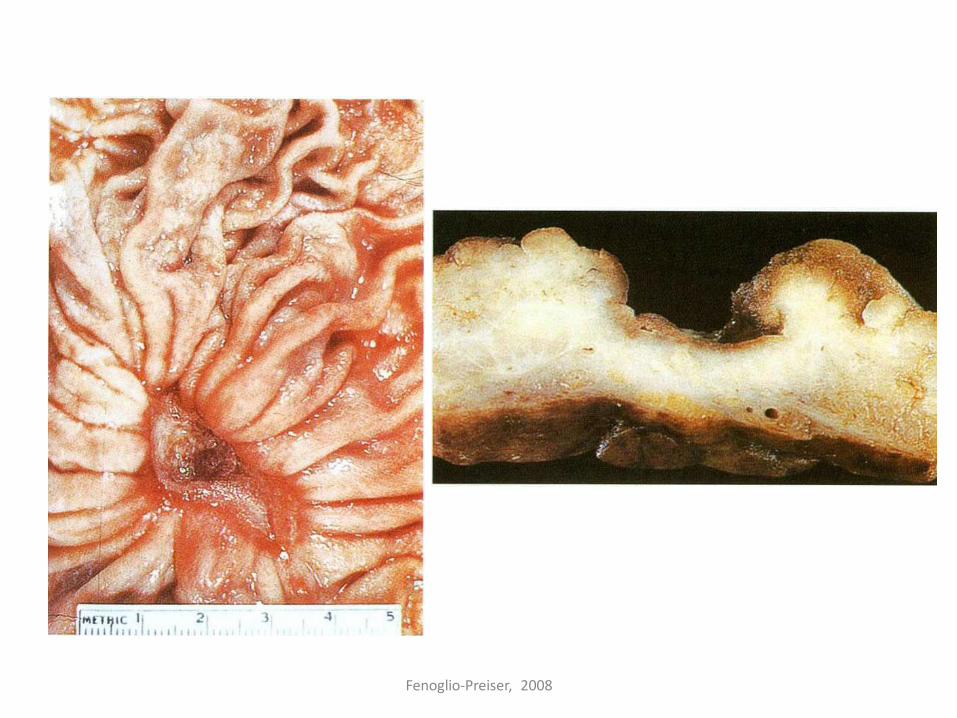
• Most common location: lesser curvature, in the anthrum
• Often solitary
• Sharply demarcated, slightly elevated, erythematous and edematous.
• Size: usually small (0.5 to 2 cm), but may be
> 3 cm (giant ulcer)
Odze RD, Golblum JR, 2015
Fenoglio-Preiser, 2008
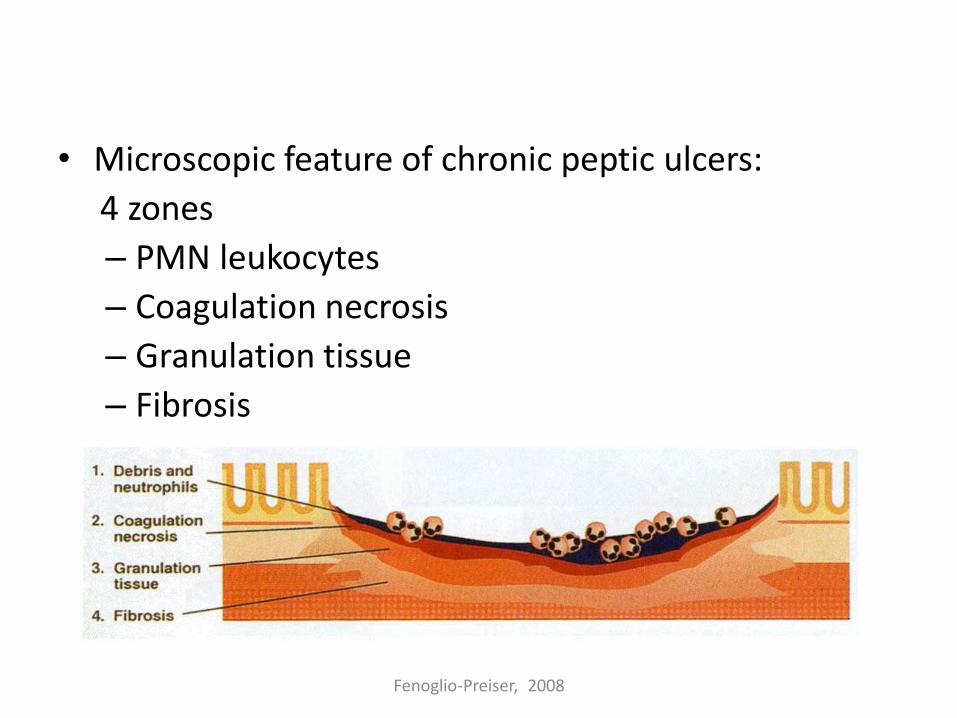
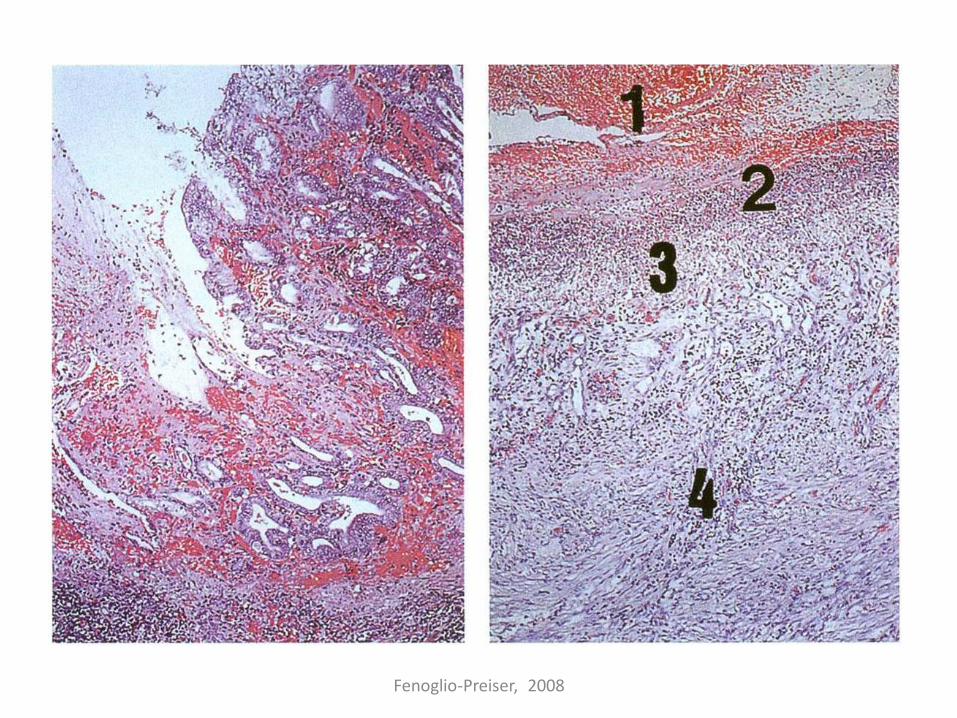
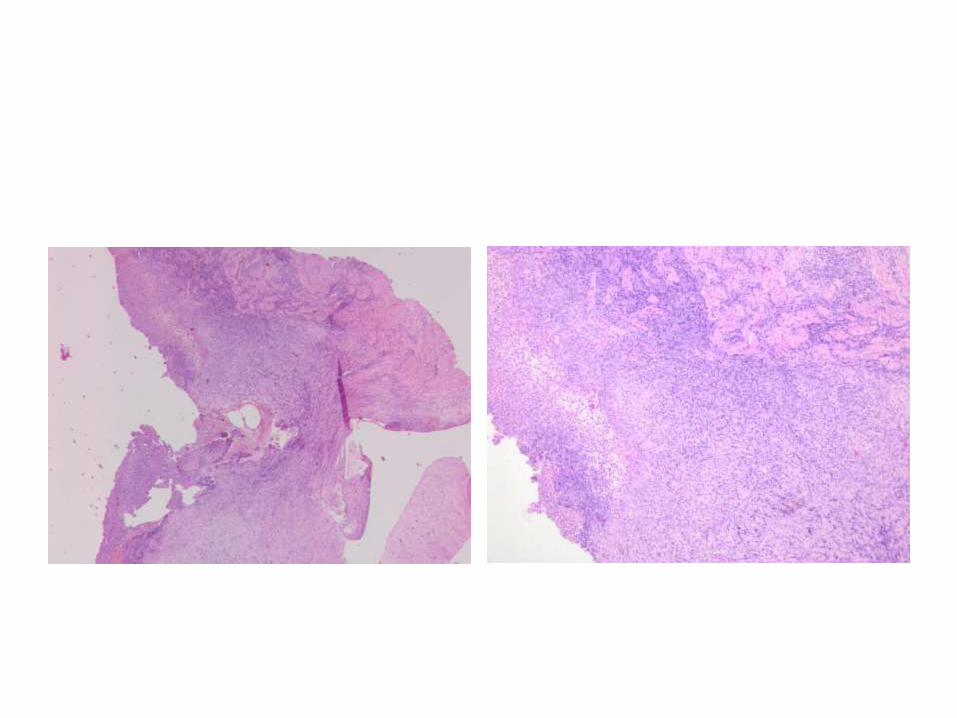
• Microscopic feature of chronic peptic ulcers:
4 zones
– PMN leukocytes
– Coagulation necrosis
– Granulation tissue
– Fibrosis
Fenoglio-Preiser, 2008
Fenoglio-Preiser, 2008
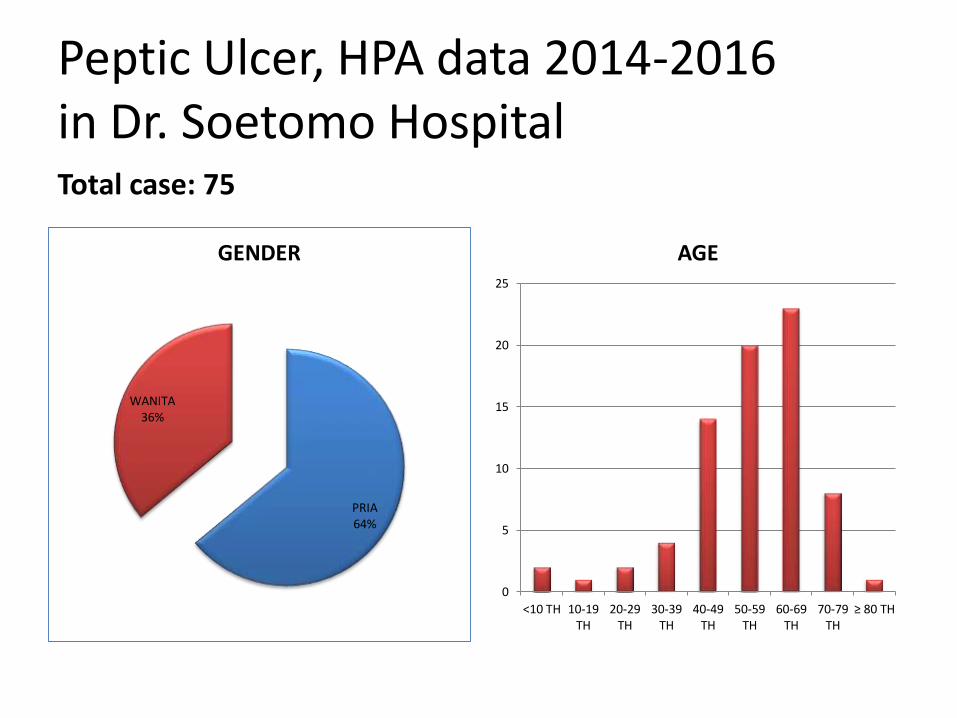
Peptic Ulcer, HPA data 2014-2016 in Dr. Soetomo HospitalTotal case: 75
PRIA64%
WANITA36%
GENDER
0
5
10
15
20
25
<10 TH 10-19TH
20-29TH
30-39TH
40-49TH
50-59TH
60-69TH
70-79TH
≥ 80 TH
AGE
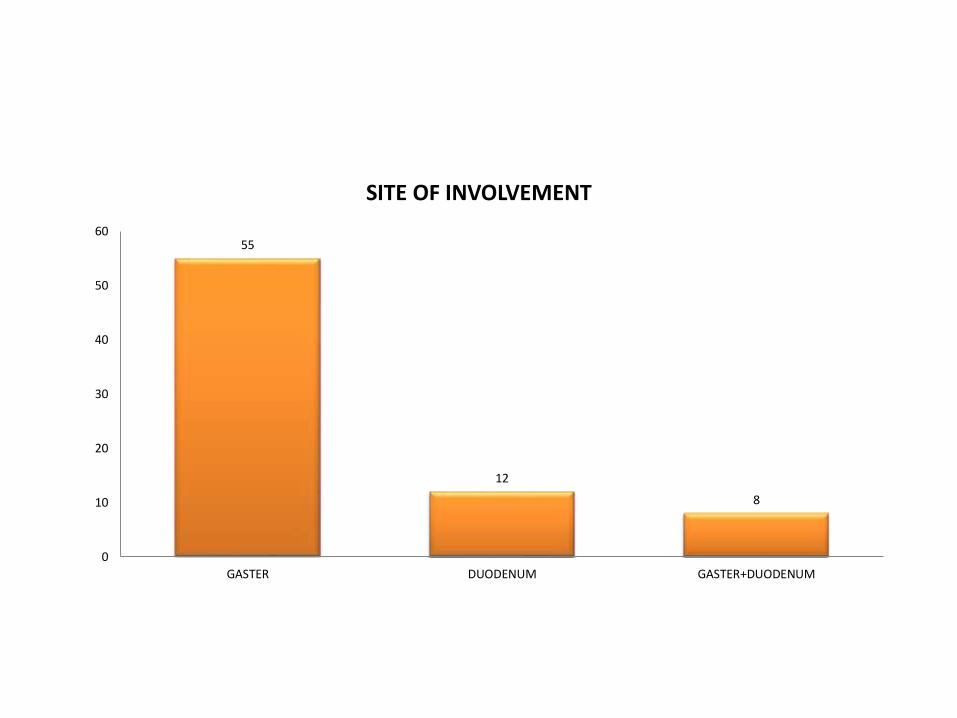
55
12
8
0
10
20
30
40
50
60
GASTER DUODENUM GASTER+DUODENUM
SITE OF INVOLVEMENT
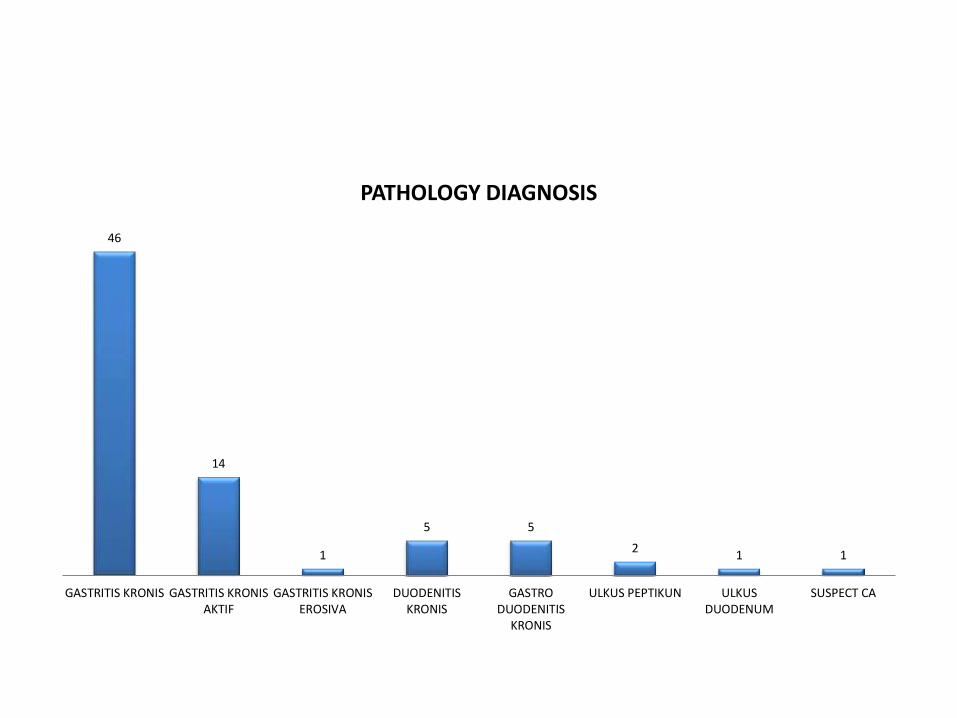
46
14
1
5 5
21 1
GASTRITIS KRONIS GASTRITIS KRONISAKTIF
GASTRITIS KRONISEROSIVA
DUODENITISKRONIS
GASTRODUODENITIS
KRONIS
ULKUS PEPTIKUN ULKUSDUODENUM
SUSPECT CA
PATHOLOGY DIAGNOSIS
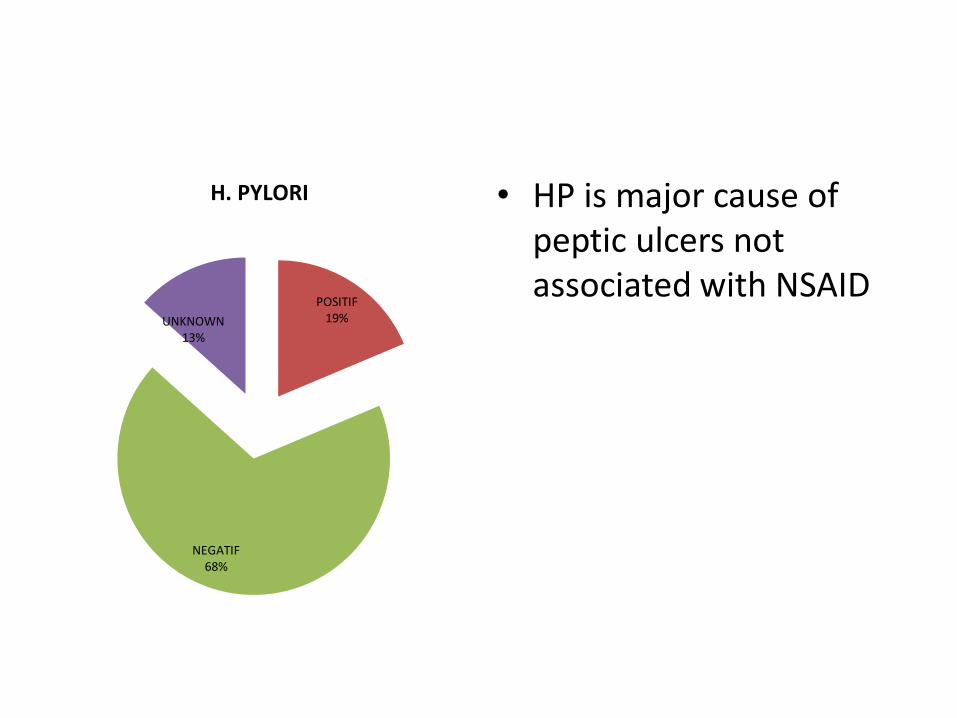
POSITIF19%
NEGATIF68%
UNKNOWN13%
H. PYLORI • HP is major cause of peptic ulcers not associated with NSAID
• Identification of HP
– Normally infects antral & corpus mucosa.
– HP can be identified in about 70% on biopsy specimen from HP(+) subjects by routine HE, 30% cases need more sensitive staining.
– Cheap and commonly used staining: Giemsa and Diff-Quik
– Immunohistochemistry for HP increase sensitivity, particularly after HP treatment.
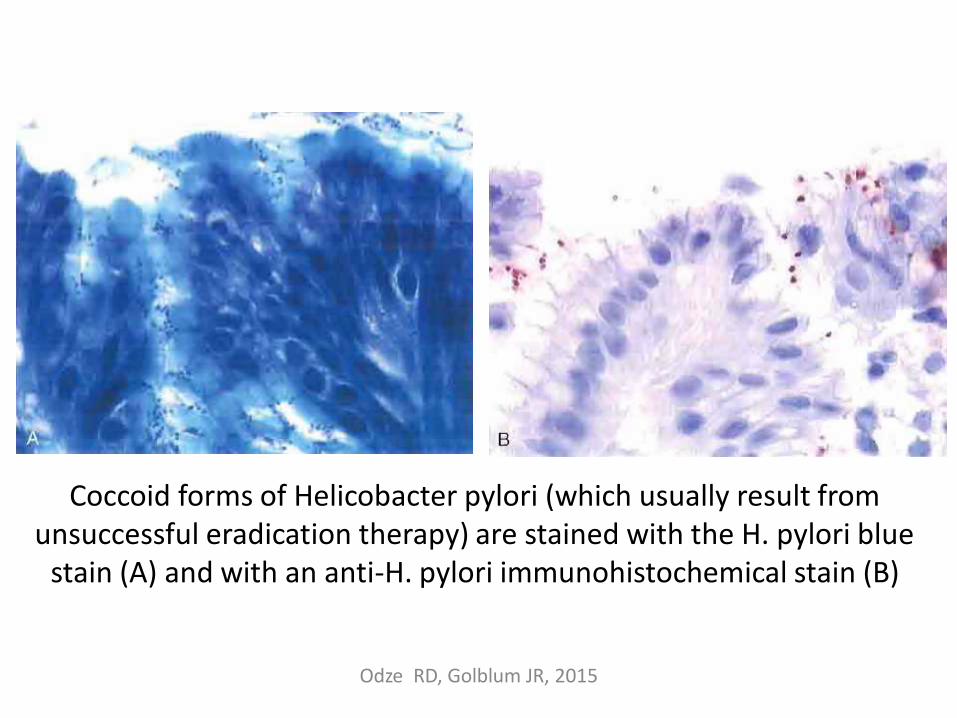
Coccoid forms of Helicobacter pylori (which usually result from unsuccessful eradication therapy) are stained with the H. pylori blue
stain (A) and with an anti-H. pylori immunohistochemical stain (B)
Odze RD, Golblum JR, 2015
• Histology: provide information related to mucosa (severity of inflammation, intestinal metaplasia, atrophy, dysplasia, neoplasia)
• Sensitivity and specificity of histology for HP detection: 53% up to 90%.
• Depending on:– Density of colonization
– Number of biopsies
– Pathologist’s experience
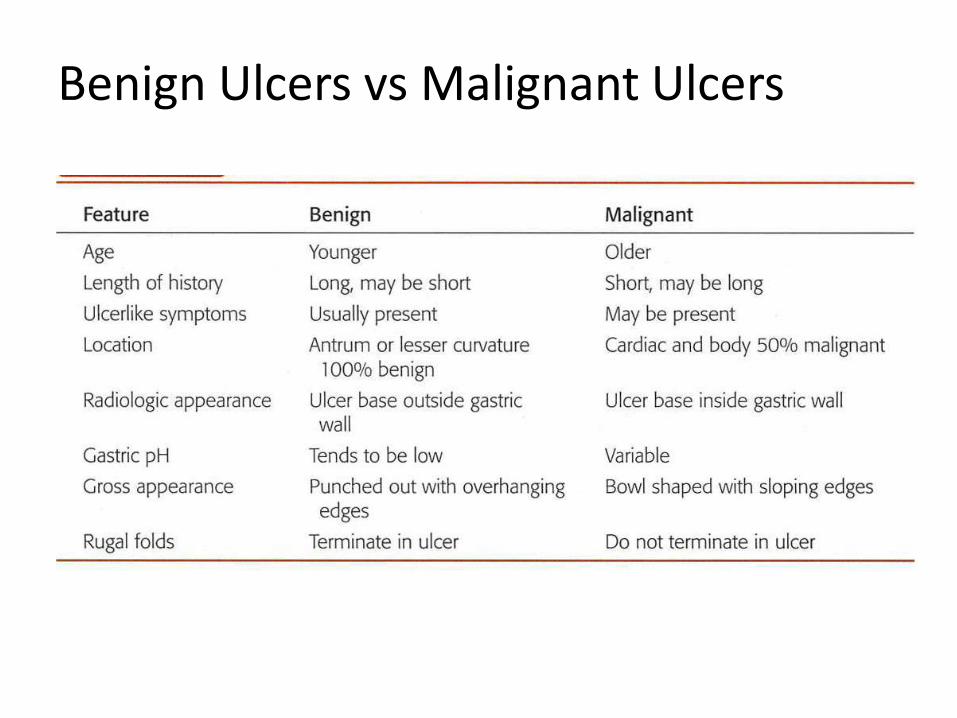
Benign Ulcers vs Malignant Ulcers
• Benign vs malignant ulcers, problem in biopsy specimen: – Malignant cells vs degenerative atypia
– Tumor cells invasion vs distorted regenerating glands
- rebiopsy after inflammation subsides
- Clinically suspicious benign ulcer: treat and reevaluation
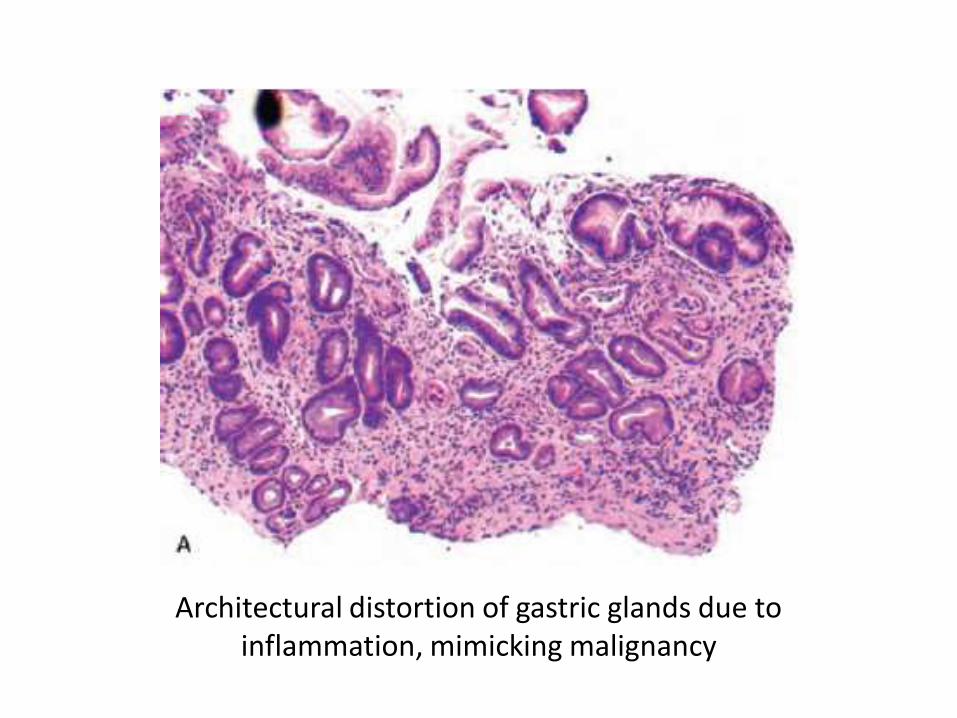
Architectural distortion of gastric glands due to inflammation, mimicking malignancy
• Complication of Peptic Ulcers
– Hemorrhage
– Perforation
– Obstruction
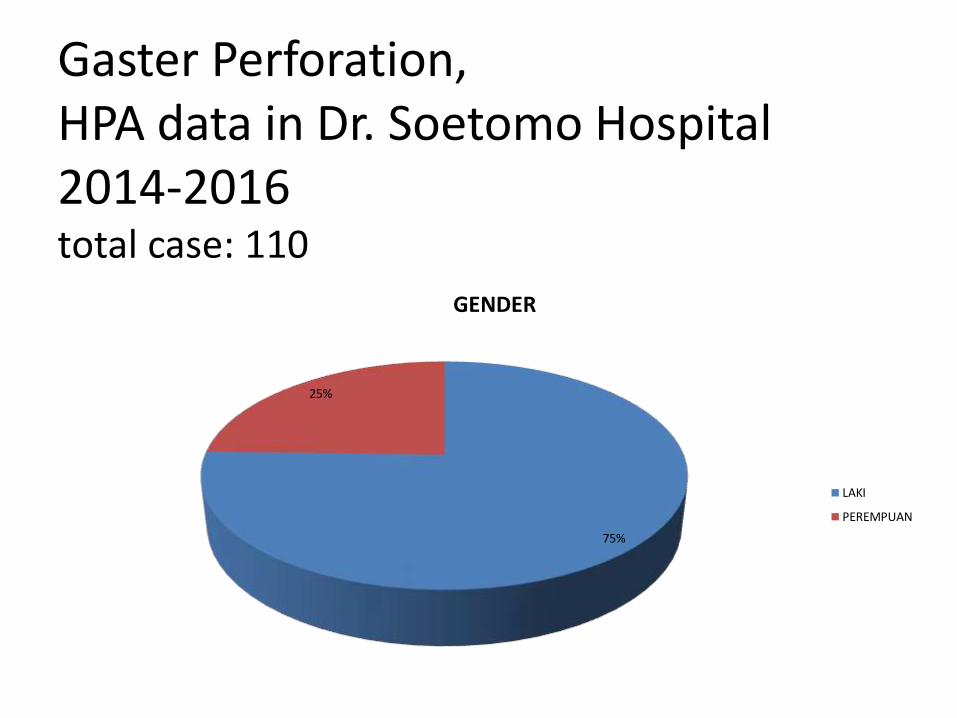
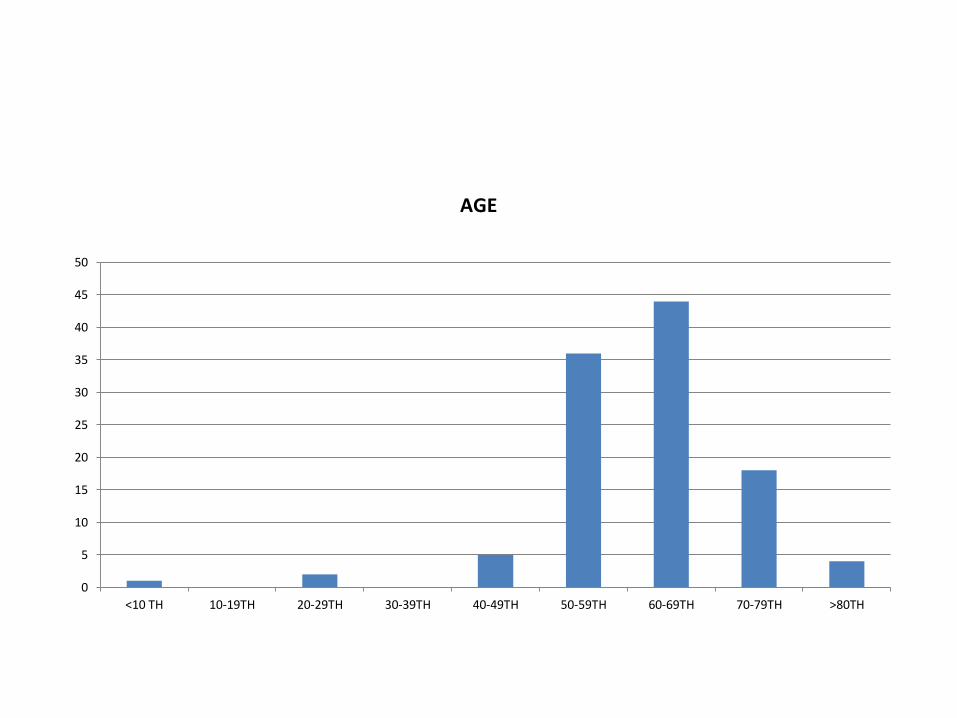
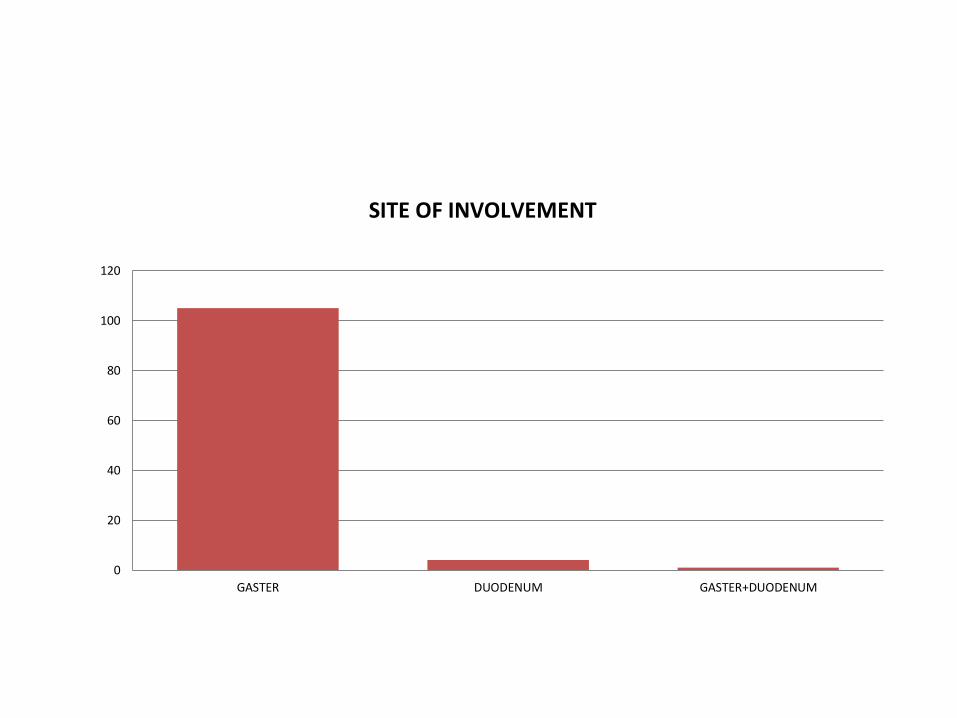
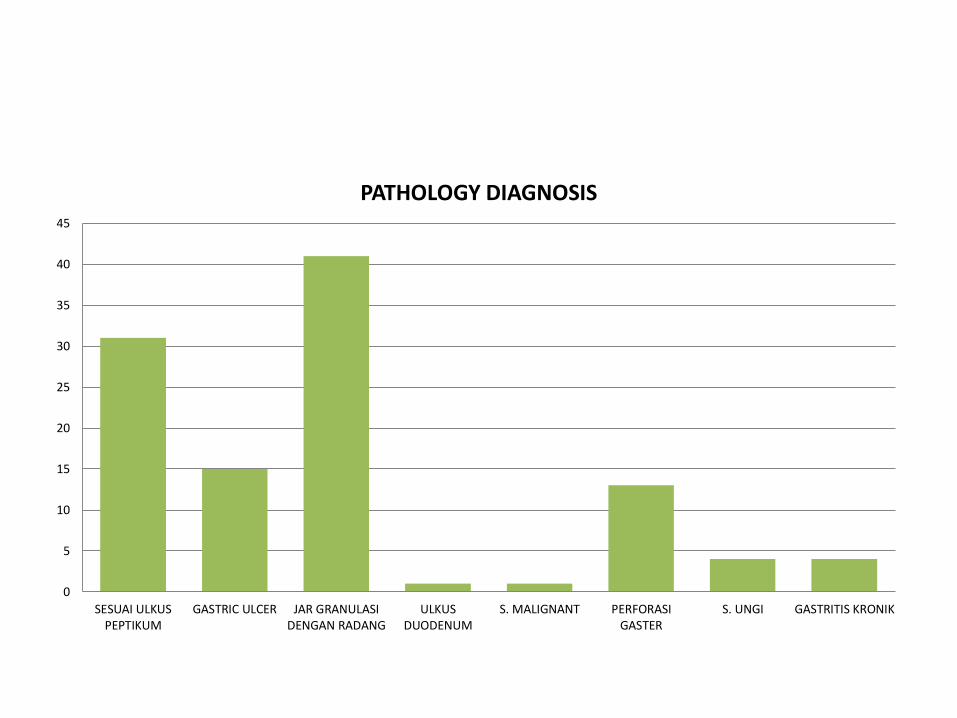
Gaster Perforation, HPA data in Dr. Soetomo Hospital2014-2016total case: 110
75%
25%
GENDER
LAKI
PEREMPUAN
0
5
10
15
20
25
30
35
40
45
50
<10 TH 10-19TH 20-29TH 30-39TH 40-49TH 50-59TH 60-69TH 70-79TH >80TH
AGE
0
20
40
60
80
100
120
GASTER DUODENUM GASTER+DUODENUM
SITE OF INVOLVEMENT
0
5
10
15
20
25
30
35
40
45
SESUAI ULKUSPEPTIKUM
GASTRIC ULCER JAR GRANULASIDENGAN RADANG
ULKUSDUODENUM
S. MALIGNANT PERFORASIGASTER
S. UNGI GASTRITIS KRONIK
PATHOLOGY DIAGNOSIS
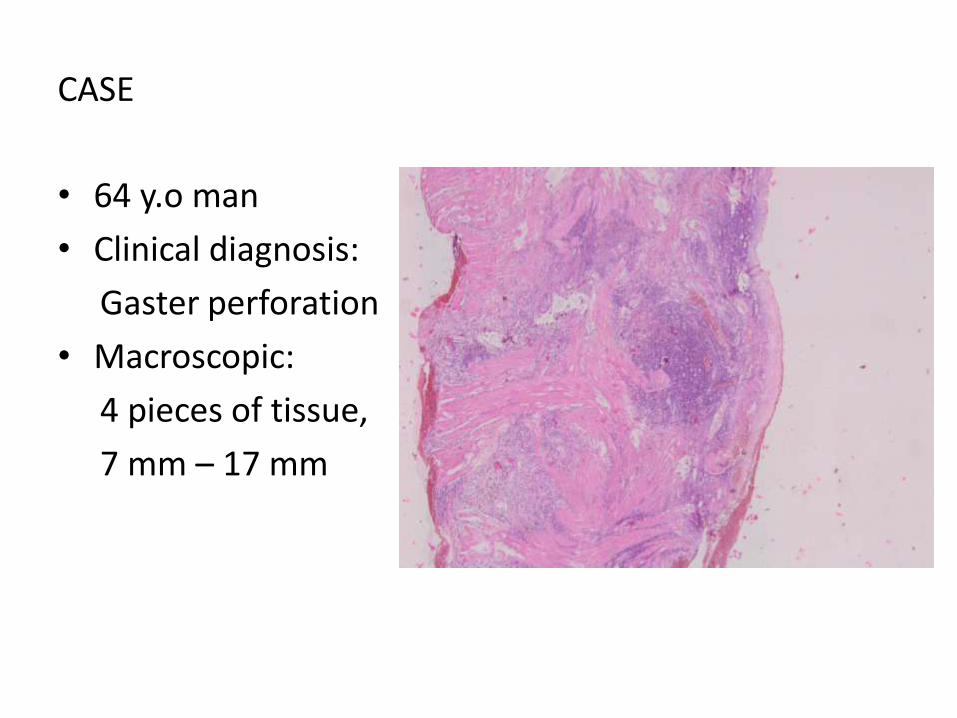
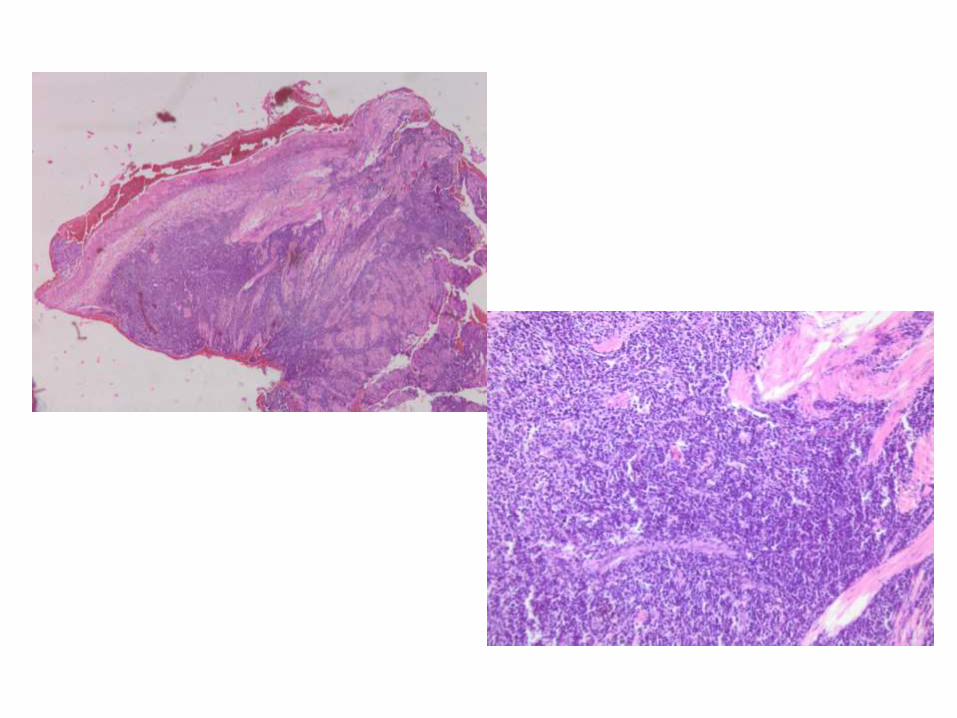
CASE
• 64 y.o man
• Clinical diagnosis:
Gaster perforation
• Macroscopic:
4 pieces of tissue,
7 mm – 17 mm
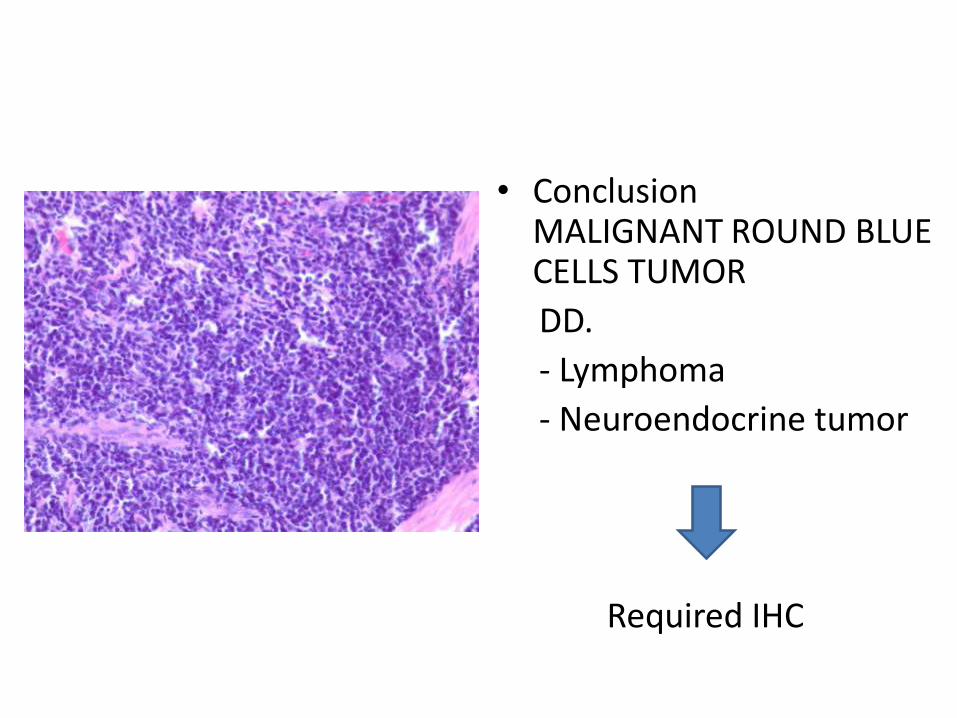
• ConclusionMALIGNANT ROUND BLUE CELLS TUMOR
DD.
- Lymphoma
- Neuroendocrine tumor
Required IHC
conclusion
• Gastric Ulcers: Peptic ulcers, Acute stress ulcers, Tumors (benign & malignant).
• Pathology examination has role in:
• determining benign and malifgnant ulcer
• etiology
THANK YOU







