Download - legg calve Perthes disease

Legg calve perthes diseaseBy: Ala’a AlGhanem | 211508057 | B1
Learning Objectives: Normal anatomy of hip joint.
Introduction and epidemiology
Aetiology and classifications
Clinical presentation
Investigations
Treatment and prognosis
Complications
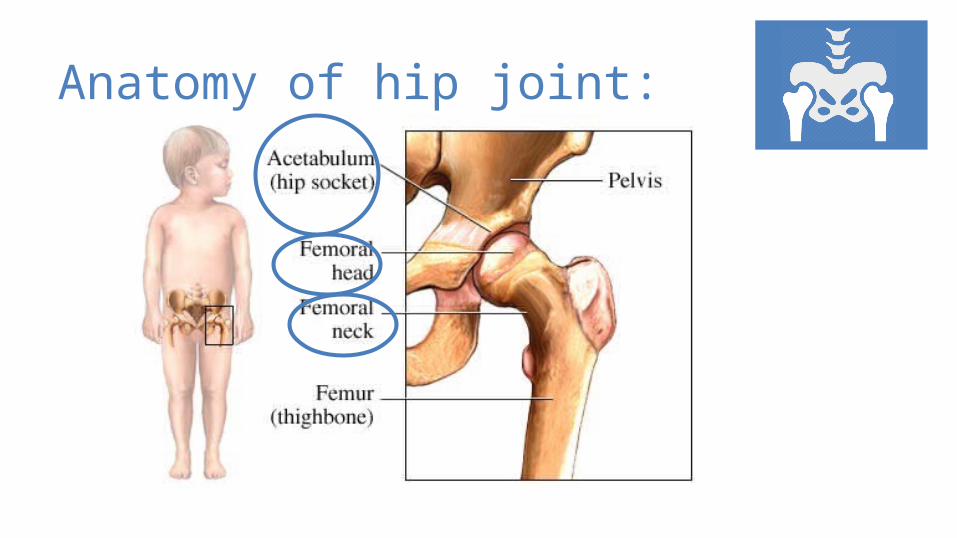
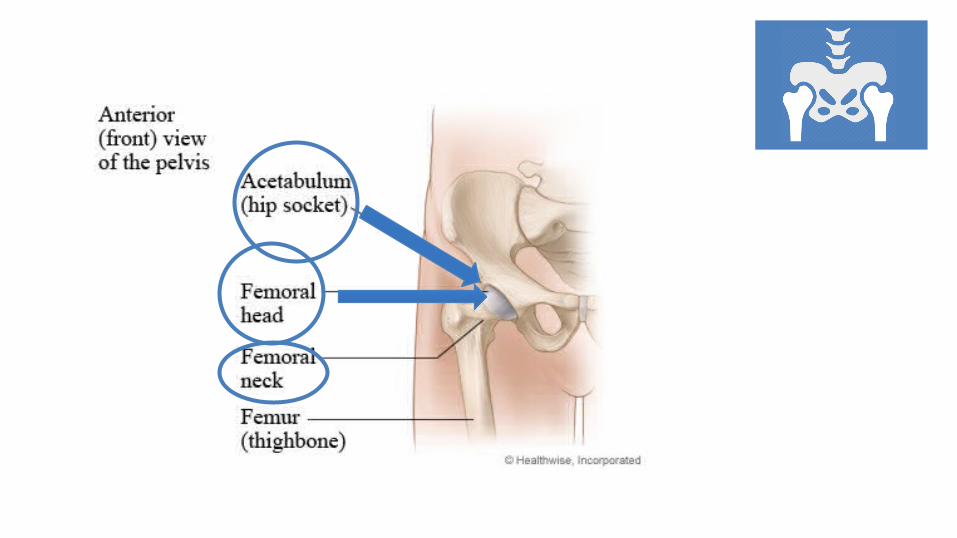
Anatomy of hip joint:

Legg calve perthes disease
Idiopathic avascular necrosis of the proximal femoral epiphysis in children
Legg Calve Perthes
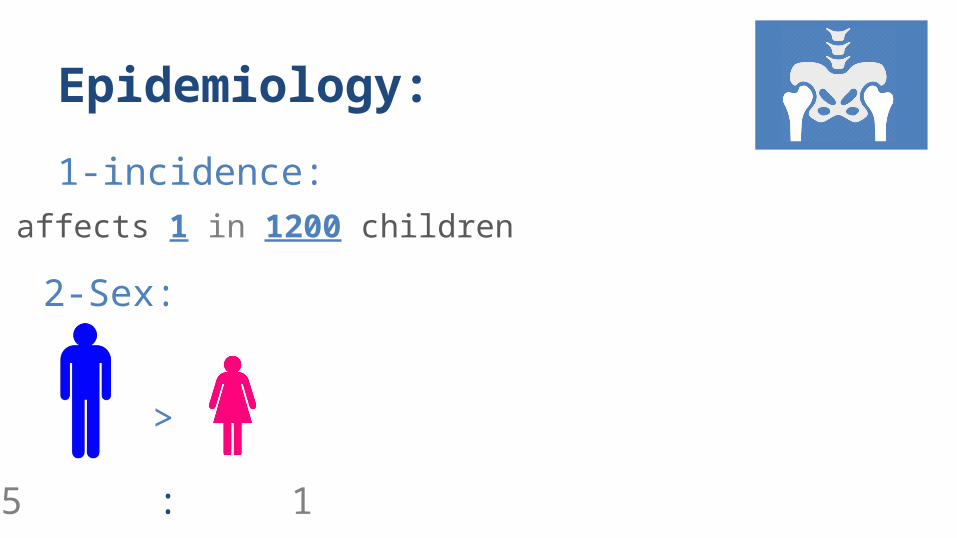
Epidemiology:
2-Sex:
1-incidence:affects 1 in 1200 children
>
5 : 1
3-Age
4-8 years is most common age of presentation
4-Population:
more commonly seen in urban populations versus rural
5-Location:bilateral in 12% (never at the same stage of disease)
the exact cause of disruption of blood supply remains unknown.
Etiology:
Associated conditions:
-ADHD (33%)
-delayed bone age (98%)
-Thrombophilia (50%)
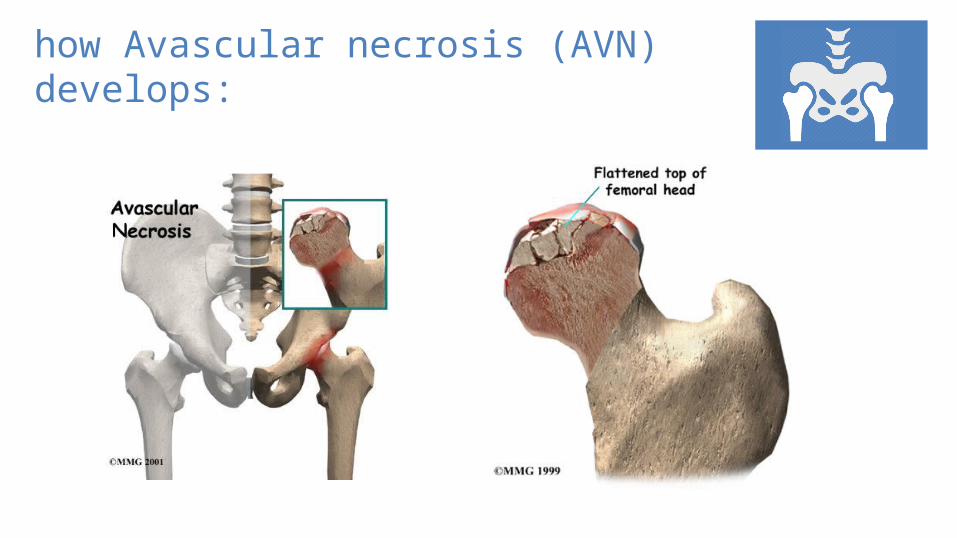
how Avascular necrosis (AVN) develops:
Risk Factors:
1-positive family history2-low birth weight3-abnormal birth presentation4-children exposed to second hand smoke
5-Asian, Inuit, and Central European decent

Classifications:Waldenström
Lateral Pillar (Herring ) Classification
Catterall Classification
Salter-Thompson classification
Stulberg classification
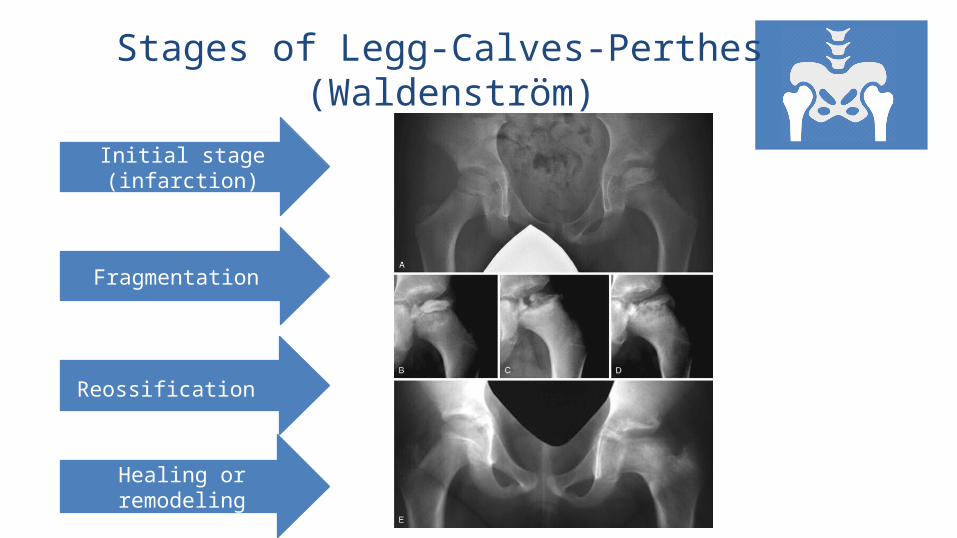
Stages of Legg-Calves-Perthes (Waldenström)
Initial stage (infarction)
Fragmentation
Reossification
Healing or remodeling
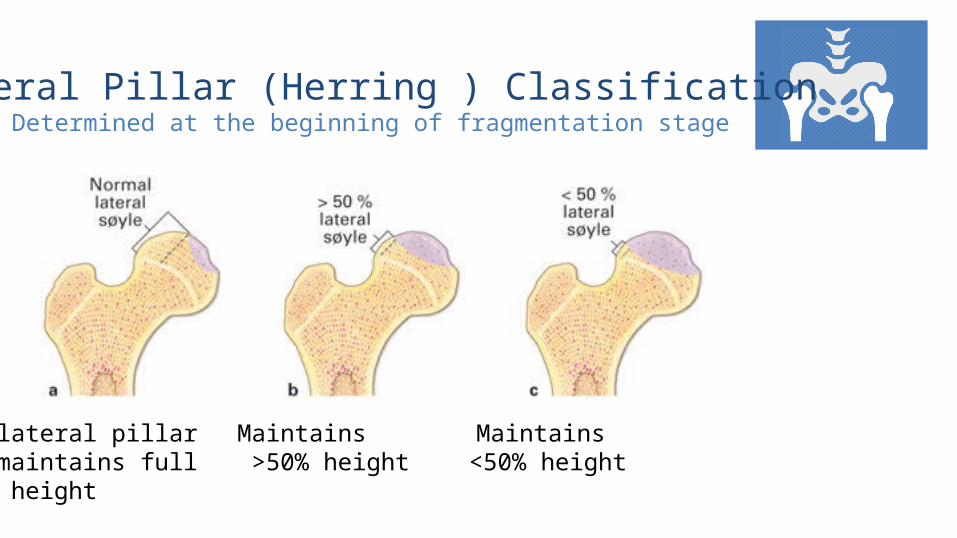
Lateral Pillar (Herring ) ClassificationDetermined at the beginning of fragmentation stage
lateral pillar maintains full height
Maintains >50% height
Maintains <50% height
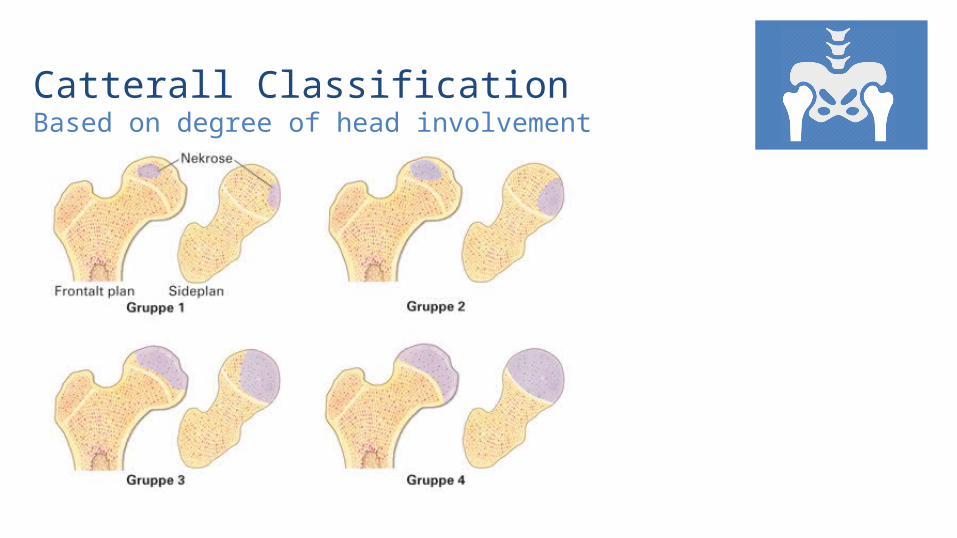
Catterall ClassificationBased on degree of head involvement
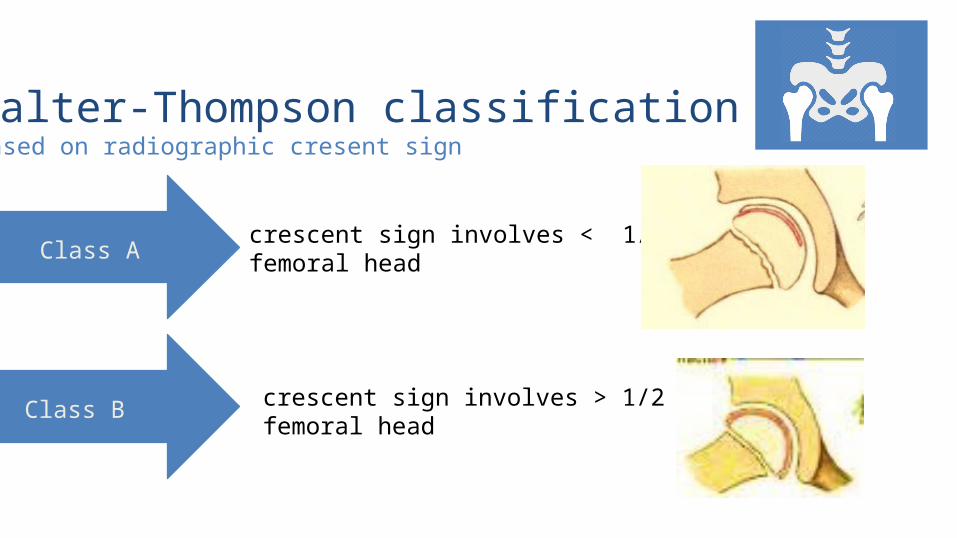
Salter-Thompson classificationBased on radiographic cresent sign
crescent sign involves < 1/2 of femoral head
crescent sign involves > 1/2 of femoral head
Class A
Class B
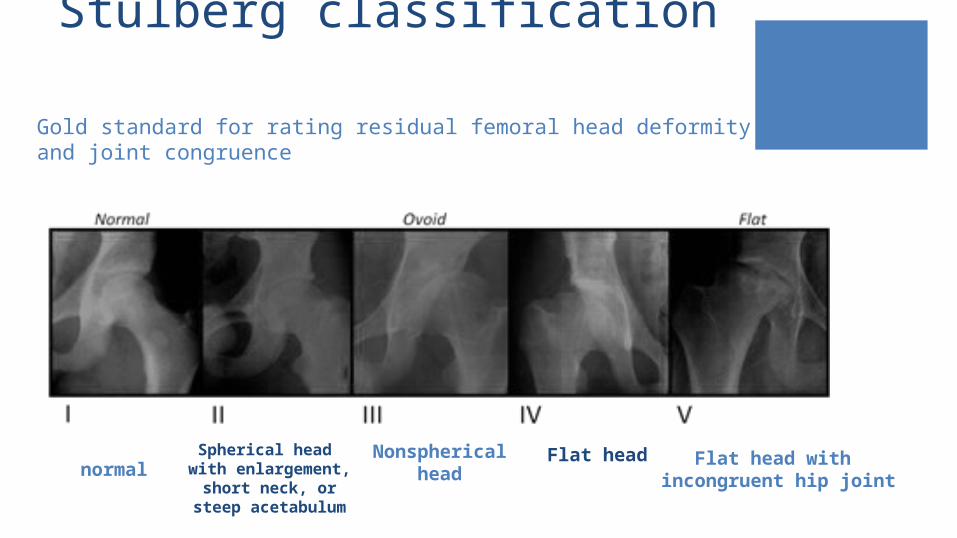
Stulberg classification
normalSpherical head
with enlargement, short neck, or
steep acetabulum
Nonspherical head
Flat head Flat head with incongruent hip joint
Gold standard for rating residual femoral head deformity and joint congruence
Clinical presentation:
-insidious onset-may cause
painless limp-intermittent
knee, hip, groin or thigh pain
Physical Exam:
Symptoms:
-Trendelenburg gait-antalgic limp
limb length discrepancy is a late finding
-hip stiffness with loss of internal rotation
and abduction-gait disturbance:
Investigations:Plain radiographs:
AP of pelvis and frog leg laterals
early findings include:
medial joint space widening (earliest)
irregularity of femoral head ossification
cresent sign (represents a subchondral fracture)
MRIcan provide early diagnosis revealing alterations in the
capital femoral epiphysis and physis.
Bone scan:
can confirm suspected case of LCP
decreased uptake (cold lesion) can predate changes on radiographs
Arthrograma dynamic arthrogram can demonstrate coverage and containment
of the femoral head
Differential Diagnosismultiple epiphyseal dysplasia
spondyloepiphyseal dysplasia
sickle cell disease
Gaucher disease
hypothyroidism
Meyers dysplasia
Treatment:The main Goals of treatment:
1-keep the femoral head contained and maintain good motion
2-containment limits deformity and minimizes loss of sphericity and lessen subsequent degenerative changes.
Non-operative:
observation alone, activity restriction, and physical therapy
Indications:
1-children < 8 years of age2-children with lateral pillar A3-consider activity restriction and protected weight-bearing during earlier stages until reossification is complete
techniques:
Cast Brace
Operative:
Femoral or pelvic osteotomy
Indications:1-children > 8 years of age, especially lateral pillar B and B/C
improved outcomes with surgery for lateral pillar B and B/C in children > 8 years poor outcome for lateral pillar C regardless of treatment.
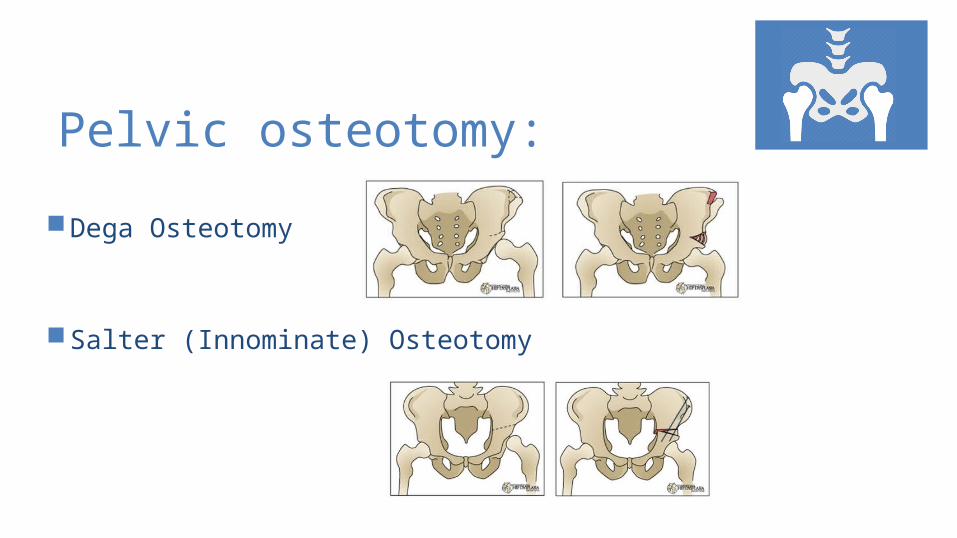
Pelvic osteotomy:
Dega Osteotomy
Salter (Innominate) Osteotomy
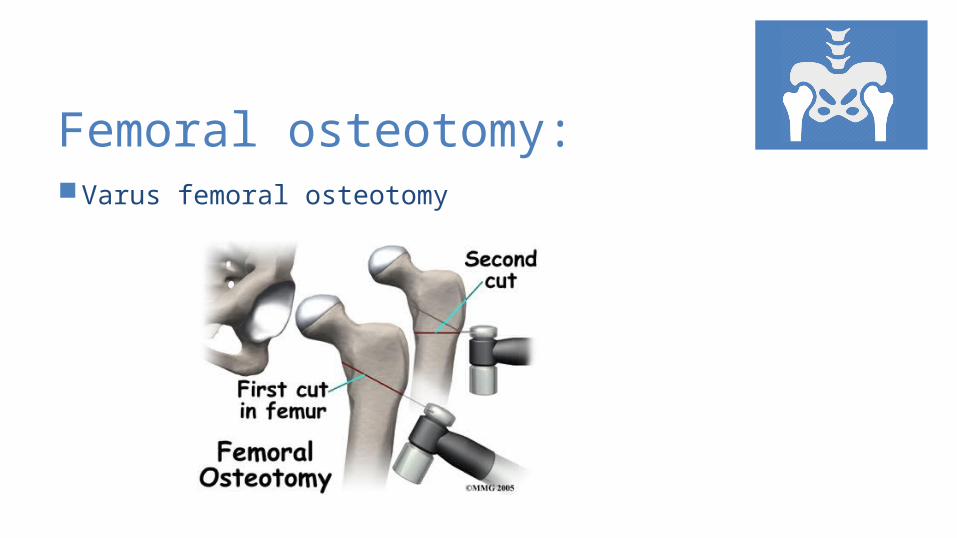
Femoral osteotomy: Varus femoral osteotomy
Prognosis:prognosis worse with:
1-age (bone age) > 6 years at presentation
2-female sex
3-decreased hip range of motion (abduction)
prognosis improved with:
1-age (bone age) < 6 years at presentation
Complications: The head of the femur may lose its normal, spherical
shape and/or collapse.
Also, degenerative joint disease can occur (i.e. as occurs in osteoarthritis).
The affected leg may lose some of its motion and may become shorter than the normal leg.

References:
Johns Hopkins Pediatric Orthopaedics Patient
Thank You







