247
KERATOACANTOAME MULTIPLE ÎN ASOCIERE CULUPUS ERITEMATOS CRONIC – PREZENTARE DE CAZ
MULTIPLE KERATOACANTHOMAS ASSOCIATED WITHCHRONIC LUPUS ERYTHEMATOSUS – CASE PRESENTATION
VASILE BENEA*, MIRCEA TAMPA*,**, DIANA LEAHU*, ALICE RUSU*, CRISTINA RÃILEANU*,MIHAELA ANCA BENEA*, SIMONA ROXANA GEORGESCU*,**
* Clinica de Dermatologie, Spitalul clinic de Boli Infecþioase ºi Tropicale „Victor Babeº” Bucureºti.Dermatology Clinic, „Victor Babeº” Clinical Hospital of Infectious and Tropical Diseases, Bucharest.
** Universitatea de Medicinã ºi Farmacie „Carol Davila”, Bucureºti.„Carol Davila” University of Medicine and Pharmacy, Bucharest.
Rezumat
Keratoacantomul este o tumorã cutanatã caracterizatãprin creºtere rapidã ºi involuþie spontanã, ce apare maifrecvent pe zonele fotoexpuse ale persoanelor de vârstemijlocii ºi bãtrâni.
Keratoacantoamele multiple au fost descrise ca parte asindroamelor genetice (keratoacantoame eruptive gene-ralizate tip Grzybowsky, keratoacantoame multiplediseminate tip Ferguson-Smith, keratoacantoame tipWitten-Zak), ca urmare a diferitelor tipuri de traumatisme,expunerii îndelungate la carcinogeni chimici (gudroane,rãºini) sau secundar altor dermatoze (post herpes zoster,lupus eritematos discoid, psoriazis, pemfigus foliaceu,lichen plan, dermatitã atopicã, acnee conglobatã, vitiligoetc.).
Prezentãm cazul unei paciente în vârstã de 36 de anicare s-a prezentat în clinicã pentru multiple leziuni cusuprafaþa exofiticã, verucoasã, asociate cu plãci ºiplacarde eritematoase ºi hipopigmentate, localizate pezone fotoexpuse, debutate în urmã cu aproximativ 18 luni.
S-au efectuat biopsii din ambele tipuri de leziuni careau pus în evidenþã modificãri de tip keratoacantom,respectiv lupus discoid.
Sub tratament cu dermatocorticoizi de potenþã medie(pentru lupus), creme keratolitice ºi crioterapie (pentru
Summary
Keratoacanthoma is a cutaneous lesion, characterisedby rapid growth and spontaneous involution, occurringmost commonly on the sun-exposed skin areas of middle-aged and elderly people.
Multiple keratoacanthomas were described as part ofgenetic syndromes (generalised eruptive keratoacanthomasof Grzybowski, disseminated multiple keratoacanthomas ofthe Ferguson-Smith type, keratoacanthomas of Witten andZak) as a result of different types of traumas, prolongedexposure to chemical carcinogens (tars, resins) orsecondary to other dermatoses (post-herpes zoster, discoidlupus erythematosus, psoriasis, pemphigus foliaceus,lichen planus, atopic dermatitis, acne conglobata, vitiligoetc.).
We present the case of a 36-year-old female patient,who came to the clinic for multiple lesions with anexophytic verrucous surface, associated witherythematous and hypopigmented plaques located on thesun-exposed areas, which had started approximately 18months before.
Biopsies were performed for both types of lesions thatevidenced keratoacanthoma-type changes and respectivelydiscoid lupus.
Under treatment with medium potency dermo-corticoids (for lupus), and keratolytic creams and
CAZURI CLINICECLINICAL CASES

248
DermatoVenerol. (Buc.), 58: 247-262
Introducere
Keratoacantomul reprezintã o neoplazie acelulelor spinoase keratinizante, cu origineaprobabilã la nivelul foliculului pilosebaceu,caracterizatã prin creºtere rapidã ºi regresiespontanã.(1)A fost descris pentru prima datã deSir Jonathan Hutchinson in anul 1889, ca ulcercrateriform al feþei (2) ºi de atunci continuã sã fieo sursã de controverse în ceea ce priveºtepatogeneza ºi opþiunile terapeutice.(3)Termenulde keratoacantom a fost introdus de Freudenthalof Wroclaw la sfarºitul anilor 1940, datoritãacantozei considerabile observatã în tumorã.(2,4)
Deºi cauza acestor leziuni este necunoscutã,existã cazuri de keratoacantoame apãrute dupãdiverse tipuri de traumatisme sau secundar altordermatoze.(5)
Prezentare de caz
Prezentãm cazul unei paciente în vârstã de 36ani care s-a prezentat în clinicã pentru multipleleziuni keratozice extensive însoþite de plãci ºiplacarde eritematoase ºi/sau hipopigmentate,localizate la nivelul zonelor fotoexpuse (mâini,faþã, membre superioare), cu evoluþie deaproximativ 18 luni.
Istoricul familial a fost negativ pentru bolidermatologice. De asemenea, pacienta a negatcontactul cu substanþe chimice.
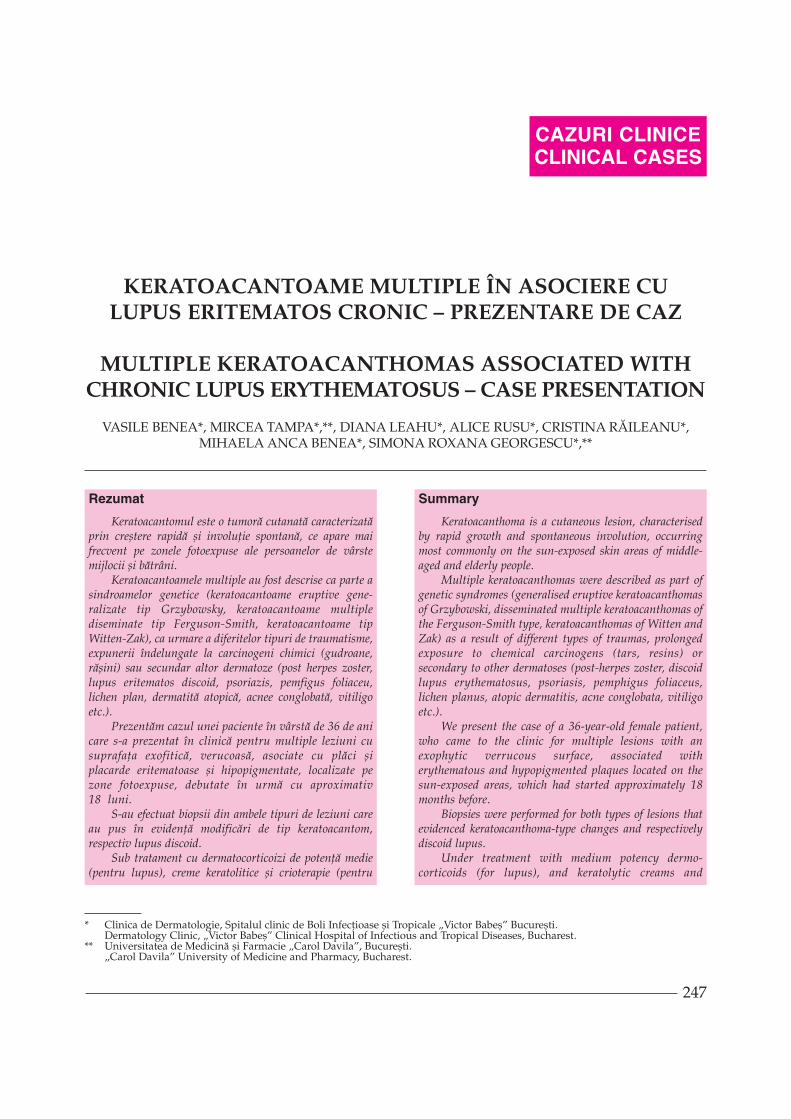
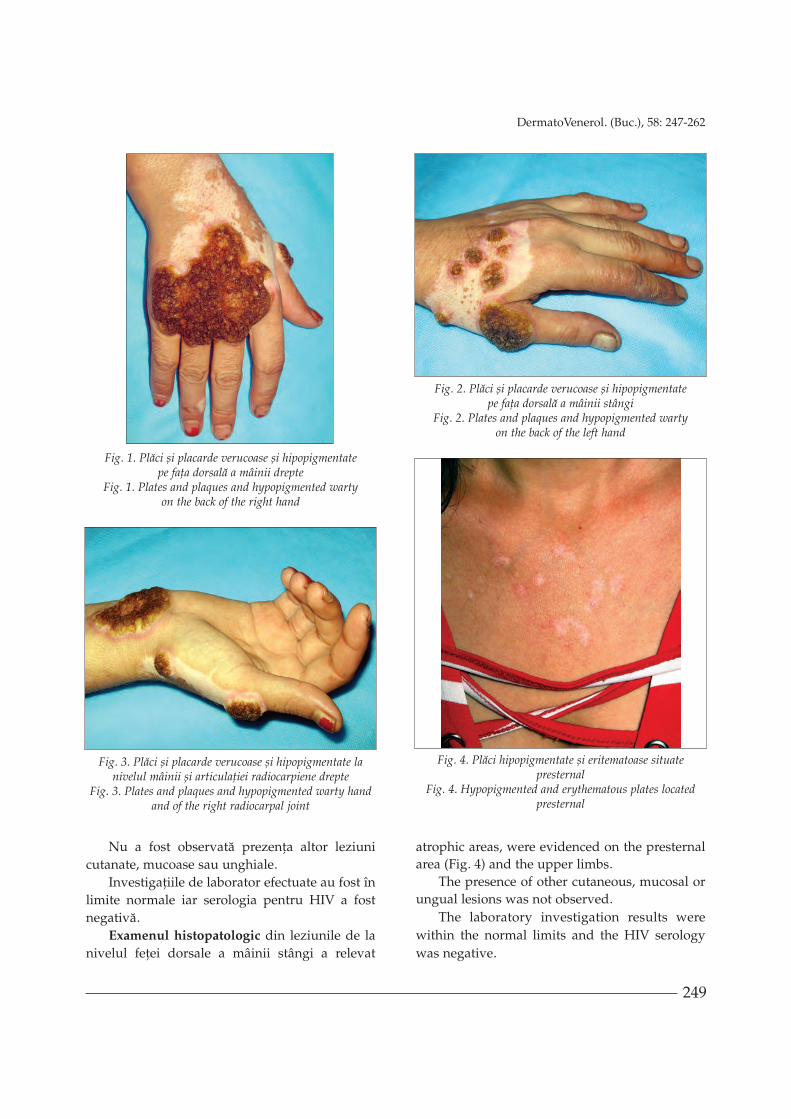
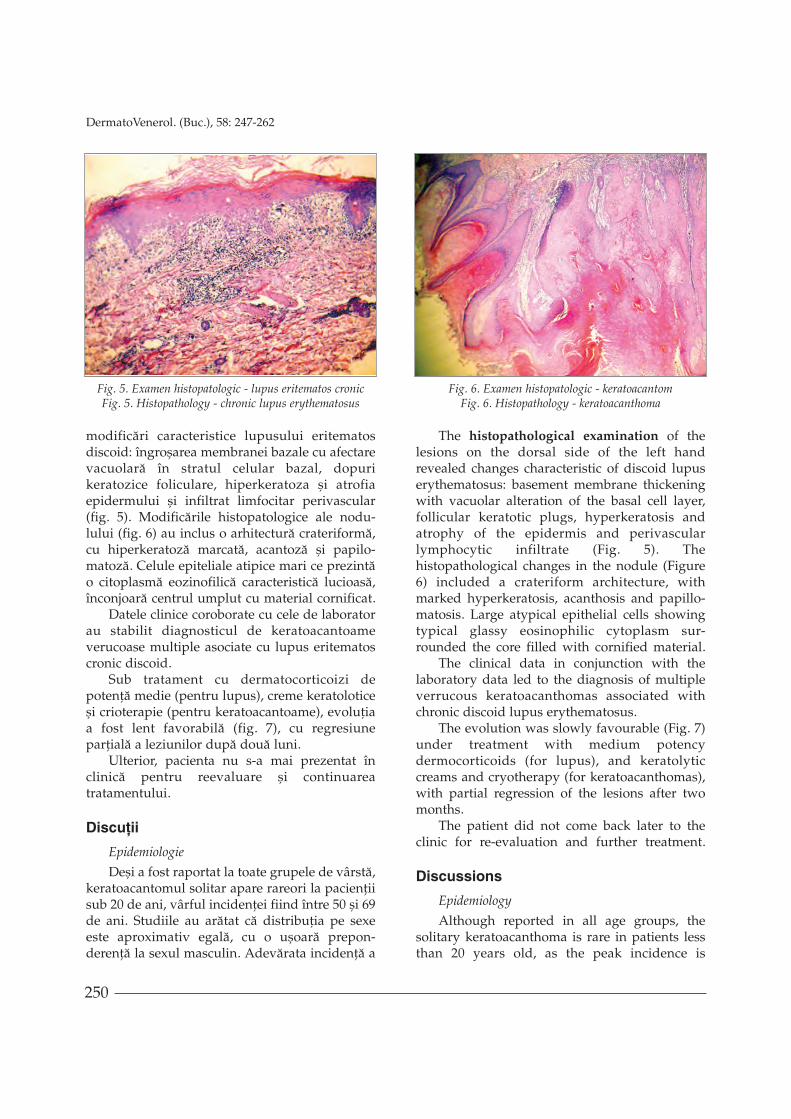
Examenul clinic a evidenþiat retromandibularun nodul hemisferic, bine delimitat, cu ulceraþiecentralã crateriformã, înconjurat de o zonãeritematoasã, la nivelul buzelor cheilitã, iar lanivelul feþei dorsale a mâinilor ºi feþei anterioarea antebraþului drept plãci ºi placarde binedelimitate, cu margini neregulate, de mãrimivariate (câþiva milimetri pânã la 6 cm) cusuprafaþa exofiticã, verucoasã (fig. 1-3). Presternal(fig. 4) ºi la nivelul membrelor superioare au fostpuse în evidenþã plãci ºi placarde eritematoaseºi/sau hipopigmentate, cu margini neregulate,neuniform colorate, cu zone atrofice.
Introduction
Keratoacanthoma is a neoplasia of thekeratin-producing squamous cells, likely tooriginate from the pilosebaceous follicle,characterised by rapid growth and spontaneousregression. (1) It was first described by SirJonathan Hutchinson in 1889 as a crateriformulcer of the face (2) and it has been a source ofcontroversy ever since with respect to thepathogenesis and therapeutic options. (3) Theterm keratoacanthoma was coined byFreudenthal of Wroclaw in the late 1940s due tothe considerable acanthosis observed in thetumour. (2, 4)
Although the cause of these lesions isunknown, there are cases of keratoacanthomasoccurring after various types of trauma orsecondary to other dermatoses. (5)
Case presentation
We present the case of a 36-year-old femalepatient who came to the clinic for multipleextensive keratotic lesions accompanied byerythematous and/or hypopigmented plaqueslocated on the sun-exposed areas (hands, face,upper limbs), with an evolution of approximately18 months.
The family history was negative for skindiseases. The patient also denied any contactwith chemicals.
The clinical examination revealed ahemispherical nodule in the retromandibularregion, which was well-defined with a centralcrateriform ulceration, surrounded by anerythematous area. The patient also presentedcheilitis and some well-defined plaques on thedorsal side of the hands and the anterior side ofthe right forearm, with irregular borders andvarious sizes (few millimetres to 6 cm) with anexophytic verrucous surface (Fig. 1-3).Erythematous and/or hypopigmented plaques,with irregular borders and uneven colour, with
keratoacantoame), evoluþia a fost favorabilã, cu remisiuneaparþialã a leziunilor.
Cuvinte cheie: keratoacantoame multiple, lupusdiscoid.
cryotherapy (for keratoacanthomas), the evolution wasfavourable, with partial remission of lesions.
Keywords: multiple keratoacanthomas, discoid lupus.
Intrat în redacþie: 16.10.2013
Acceptat: 11.11.2013
Received: 16.10.2013
Accepted: 11.11.2013
249
DermatoVenerol. (Buc.), 58: 247-262
Nu a fost observatã prezenþa altor leziunicutanate, mucoase sau unghiale.
Investigaþiile de laborator efectuate au fost înlimite normale iar serologia pentru HIV a fostnegativã.
Examenul histopatologic din leziunile de lanivelul feþei dorsale a mâinii stângi a relevat
atrophic areas, were evidenced on the presternalarea (Fig. 4) and the upper limbs.
The presence of other cutaneous, mucosal orungual lesions was not observed.
The laboratory investigation results werewithin the normal limits and the HIV serologywas negative.
Fig. 1. Plãci ºi placarde verucoase ºi hipopigmentate pe faþa dorsalã a mâinii drepte
Fig. 1. Plates and plaques and hypopigmented warty on the back of the right hand
Fig. 2. Plãci ºi placarde verucoase ºi hipopigmentate pe faþa dorsalã a mâinii stângi
Fig. 2. Plates and plaques and hypopigmented warty on the back of the left hand
Fig. 4. Plãci hipopigmentate ºi eritematoase situatepresternal
Fig. 4. Hypopigmented and erythematous plates locatedpresternal
Fig. 3. Plãci ºi placarde verucoase ºi hipopigmentate lanivelul mâinii ºi articulaþiei radiocarpiene drepte
Fig. 3. Plates and plaques and hypopigmented warty handand of the right radiocarpal joint
250
DermatoVenerol. (Buc.), 58: 247-262
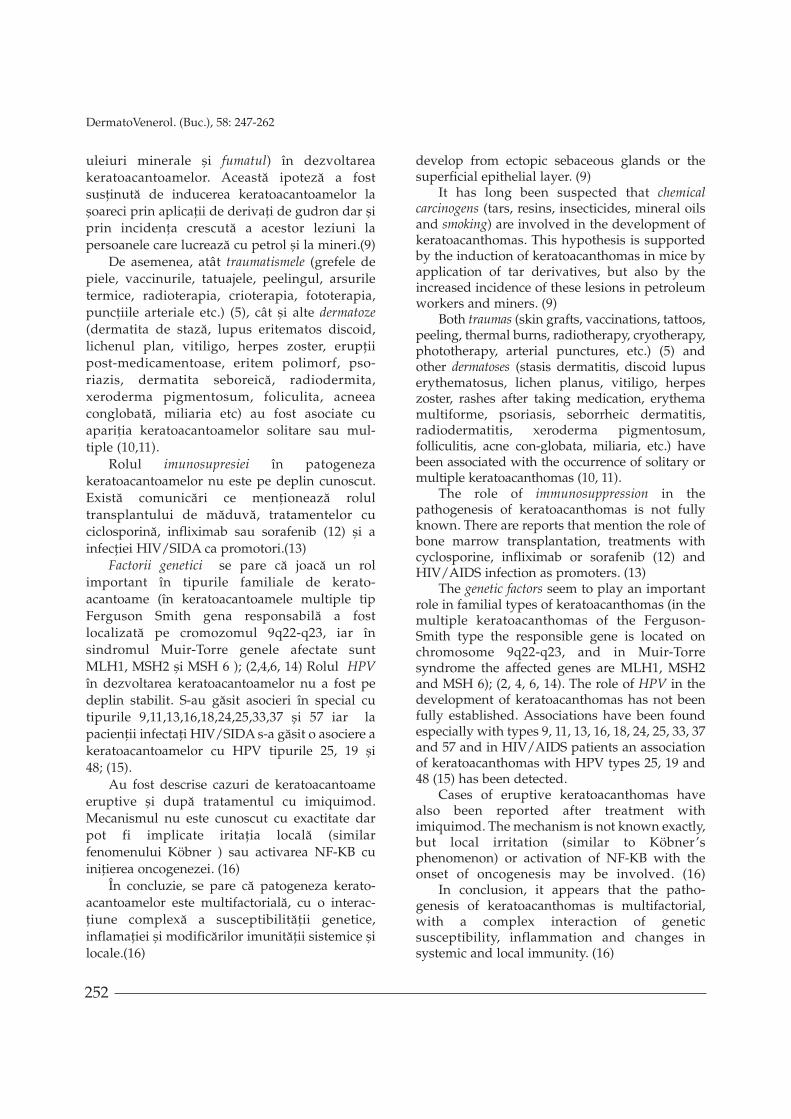
modificãri caracteristice lupusului eritematosdiscoid: îngroºarea membranei bazale cu afectarevacuolarã în stratul celular bazal, dopurikeratozice foliculare, hiperkeratoza ºi atrofiaepidermului ºi infiltrat limfocitar perivascular(fig. 5). Modificãrile histopatologice ale nodu-lului (fig. 6) au inclus o arhitecturã crateriformã,cu hiperkeratozã marcatã, acantozã ºi papilo-matozã. Celule epiteliale atipice mari ce prezintão citoplasmã eozinofilicã caracteristicã lucioasã,înconjoarã centrul umplut cu material cornificat.
Datele clinice coroborate cu cele de laboratorau stabilit diagnosticul de keratoacantoameverucoase multiple asociate cu lupus eritematoscronic discoid.
Sub tratament cu dermatocorticoizi depotenþã medie (pentru lupus), creme keratoloticeºi crioterapie (pentru keratoacantoame), evoluþiaa fost lent favorabilã (fig. 7), cu regresiuneparþialã a leziunilor dupã douã luni.
Ulterior, pacienta nu s-a mai prezentat înclinicã pentru reevaluare ºi continuareatratamentului.
Discuþii
Epidemiologie
Deºi a fost raportat la toate grupele de vârstã,keratoacantomul solitar apare rareori la pacienþiisub 20 de ani, vârful incidenþei fiind între 50 ºi 69de ani. Studiile au arãtat cã distribuþia pe sexeeste aproximativ egalã, cu o uºoarã prepon-derenþã la sexul masculin. Adevãrata incidenþã a
The histopathological examination of thelesions on the dorsal side of the left handrevealed changes characteristic of discoid lupuserythematosus: basement membrane thickeningwith vacuolar alteration of the basal cell layer,follicular keratotic plugs, hyperkeratosis andatrophy of the epidermis and perivascularlymphocytic infiltrate (Fig. 5). Thehistopathological changes in the nodule (Figure6) included a crateriform architecture, withmarked hyperkeratosis, acanthosis and papillo-matosis. Large atypical epithelial cells showingtypical glassy eosinophilic cytoplasm sur-rounded the core filled with cornified material.
The clinical data in conjunction with thelaboratory data led to the diagnosis of multipleverrucous keratoacanthomas associated withchronic discoid lupus erythematosus.
The evolution was slowly favourable (Fig. 7)under treatment with medium potencydermocorticoids (for lupus), and keratolyticcreams and cryotherapy (for keratoacanthomas),with partial regression of the lesions after twomonths.
The patient did not come back later to theclinic for re-evaluation and further treatment.
Discussions
Epidemiology
Although reported in all age groups, thesolitary keratoacanthoma is rare in patients lessthan 20 years old, as the peak incidence is
Fig. 5. Examen histopatologic - lupus eritematos cronicFig. 5. Histopathology - chronic lupus erythematosus
Fig. 6. Examen histopatologic - keratoacantomFig. 6. Histopathology - keratoacanthoma

251
DermatoVenerol. (Buc.), 58: 247-262
keratoacantoamelor nu este însã cunoscutã, înprincipal din cauzã cã unele leziuni regreseazãspontan, ºi, prin urmare, nu mai ajung sa fietratate de medici.
Incidenþa formelor multiple ºi particulare dekeratoacantoame rãmâne scãzutã. Tipul familialde keratoacantoame multiple, eruptive, FergusonSmith poate debuta în adolescenþã sau chiar mai devreme, cu o incidenþã pe sexe de B:F = 3:1, spre deosebire de keratoacantoameleeruptive tip Grzybowski care au o distribuþieegalã pe sexe (B:F = 1:1).(2,4,6).
Etiopatogenie
Etiologia keratoacantoamelor rãmâne necu-noscutã. Au fost descriºi multipli factori implicaþiîn patogeneza keratoacantomului. Apariþialeziunilor cu predilecþie pe zonele fotoexpuse, înxeroderma pigmentosum ºi la cei care au urmattratament PUVA sau fototerapie cu UVB (7,8)sugereazã cã expunerea cronicã la raze UV poatereprezenta un factor de risc important în apariþiakeratoacantoamelor. Se pare cã PUVA accelereazãdezvoltarea leziunilor, dar s-a demonstrat cãriscul de a dezvolta keratoacantoame dupãtratamentul PUVA este mai mic decât cel de adezvolta carcinoame spinocelulare.
Aparenta derivare a keratoacantoamelor dinfoliculii piloºi nu poate explica apariþia acestorleziuni la nivelul mucoaselor. S-a speculat cãleziunile de la nivelul mucoasei bucale sedezvoltã din glande sebacee ectopice sau dinstratul epitelial superficial.(9)
S-a bãnuit de mult timp implicarea carcino-
genilor chimici (gudroane, rãºini, insecticide,
between 50 and 69 years old. Studies have shownthat the gender distribution is approximatelyequal, with a slight predominance in males. Butthe true incidence of keratoacanthomas isunknown, mainly because some lesions regressspontaneously and therefore do not get to betreated by doctors.
The incidence of the multiple and particularforms of keratoacanthomas remains low. TheFerguson-Smith familial type of multipleeruptive keratoacanthomas may begin inadolescence or even earlier, with a genderincidence of M:F = 3:1, unlike eruptivekeratoacanthomas of Grzybowski that have equalgender distribution (M:F = 1:1). (2, 4, 6)
Etiopathogeny
The etiology of keratoacanthomas remainsunknown. Multiple factors involved in thepathogenesis of keratoacanthomas have beendescribed. The occurrence of lesions especially insun-exposed areas, in xeroderma pigmentosumand in people who received PUVA treatment orUVB phototherapy (7, 8) suggests that chronicexposure to UV rays may be an important riskfactor in the development of keratoacanthomas.It seems that PUVA accelerates the developmentof lesions, but it has been demonstrated that therisk of developing keratoacanthomas after PUVAtreatment is lower than that of developingsquamous cell carcinomas.
The apparent derivation of keratoacanthomasfrom hair follicles cannot explain the occurrence ofthese lesions in the mucous membranes. It hasbeen speculated that oral mucosal lesions
Fig. 7. Aspect clinicdupã o sãptãmânã detratamentFig. 7. Clinical aspectafter one week oftreatment
252
DermatoVenerol. (Buc.), 58: 247-262
uleiuri minerale ºi fumatul) în dezvoltareakeratoacantoamelor. Aceastã ipotezã a fostsusþinutã de inducerea keratoacantoamelor laºoareci prin aplicaþii de derivaþi de gudron dar ºiprin incidenþa crescutã a acestor leziuni lapersoanele care lucreazã cu petrol ºi la mineri.(9)
De asemenea, atât traumatismele (grefele depiele, vaccinurile, tatuajele, peelingul, arsuriletermice, radioterapia, crioterapia, fototerapia,puncþiile arteriale etc.) (5), cât ºi alte dermatoze
(dermatita de stazã, lupus eritematos discoid,lichenul plan, vitiligo, herpes zoster, erupþiipost-medicamentoase, eritem polimorf, pso-riazis, dermatita seboreicã, radiodermita,xeroderma pigmentosum, foliculita, acneeaconglobatã, miliaria etc) au fost asociate cuapariþia keratoacantoamelor solitare sau mul-tiple (10,11).
Rolul imunosupresiei în patogenezakeratoacantoamelor nu este pe deplin cunoscut.Existã comunicãri ce menþioneazã rolultransplantului de mãduvã, tratamentelor cuciclosporinã, infliximab sau sorafenib (12) ºi ainfecþiei HIV/SIDA ca promotori.(13)
Factorii genetici se pare cã joacã un rolimportant în tipurile familiale de kerato-acantoame (în keratoacantoamele multiple tipFerguson Smith gena responsabilã a fostlocalizatã pe cromozomul 9q22-q23, iar însindromul Muir-Torre genele afectate suntMLH1, MSH2 ºi MSH 6 ); (2,4,6, 14) Rolul HPV
în dezvoltarea keratoacantoamelor nu a fost pedeplin stabilit. S-au gãsit asocieri în special cutipurile 9,11,13,16,18,24,25,33,37 ºi 57 iar lapacienþii infectaþi HIV/SIDA s-a gãsit o asociere akeratoacantoamelor cu HPV tipurile 25, 19 ºi 48; (15).
Au fost descrise cazuri de keratoacantoameeruptive ºi dupã tratamentul cu imiquimod.Mecanismul nu este cunoscut cu exactitate darpot fi implicate iritaþia localã (similarfenomenului Köbner ) sau activarea NF-KB cuiniþierea oncogenezei. (16)
În concluzie, se pare cã patogeneza kerato-acantoamelor este multifactorialã, cu o interac-þiune complexã a susceptibilitãþii genetice,inflamaþiei ºi modificãrilor imunitãþii sistemice ºilocale.(16)
develop from ectopic sebaceous glands or thesuperficial epithelial layer. (9)
It has long been suspected that chemicalcarcinogens (tars, resins, insecticides, mineral oilsand smoking) are involved in the development ofkeratoacanthomas. This hypothesis is supportedby the induction of keratoacanthomas in mice byapplication of tar derivatives, but also by theincreased incidence of these lesions in petroleumworkers and miners. (9)
Both traumas (skin grafts, vaccinations, tattoos,peeling, thermal burns, radiotherapy, cryotherapy,phototherapy, arterial punctures, etc.) (5) andother dermatoses (stasis dermatitis, discoid lupuserythematosus, lichen planus, vitiligo, herpeszoster, rashes after taking medication, erythemamultiforme, psoriasis, seborrheic dermatitis,radiodermatitis, xeroderma pigmentosum,folliculitis, acne con-globata, miliaria, etc.) havebeen associated with the occurrence of solitary ormultiple keratoacanthomas (10, 11).
The role of immunosuppression in thepathogenesis of keratoacanthomas is not fullyknown. There are reports that mention the role ofbone marrow transplantation, treatments withcyclosporine, infliximab or sorafenib (12) andHIV/AIDS infection as promoters. (13)
The genetic factors seem to play an importantrole in familial types of keratoacanthomas (in themultiple keratoacanthomas of the Ferguson-Smith type the responsible gene is located onchromosome 9q22-q23, and in Muir-Torresyndrome the affected genes are MLH1, MSH2and MSH 6); (2, 4, 6, 14). The role of HPV in thedevelopment of keratoacanthomas has not beenfully established. Associations have been foundespecially with types 9, 11, 13, 16, 18, 24, 25, 33, 37and 57 and in HIV/AIDS patients an associationof keratoacanthomas with HPV types 25, 19 and48 (15) has been detected.
Cases of eruptive keratoacanthomas havealso been reported after treatment withimiquimod. The mechanism is not known exactly,but local irritation (similar to Köbner’sphenomenon) or activation of NF-KB with theonset of oncogenesis may be involved. (16)
In conclusion, it appears that the patho-genesis of keratoacanthomas is multifactorial,with a complex interaction of geneticsusceptibility, inflammation and changes insystemic and local immunity. (16)
253
DermatoVenerol. (Buc.), 58: 247-262
Aspecte clinice
Existã mai multe tipuri de keratoacantoamedescrise în literaturã. (Tabelul I)
Keratoacantomul solitar tipic rãmâne cea maiîntâlnitã formã ºi se dezvoltã de obicei pe zonelefotoexpuse (extremitatea cefalicã, gât ºi membre)evoluând în 3 faze: o fazã proliferativã (în careleziunea îsi mãreºte dimensiunile ajungând la 10-25 mm diametru în 6-8 sãptãmâni), faza dekeratoacantom matur (leziunea nu mai creºte,menþinându-ºi forma crateriformã) urmatã defaza de involuþie în care aproximativ 50% dinkeratoacantoame involueazã spontan (în 4-6sãptãmâni), lãsând o cicatrice atroficã ºihipopigmentatã. (4)
Keratoacantoamele mucoaselor sunt rare ºidificil de diagnosticat. Mai frecvent esteinteresatã mucoasa bucalã iar originea probabilãse aflã în stratul epitelial superficial (17)
Keratoacantoamele subunghiale nu au tendinþãde regresie spontanã ºi pot evolua cu erodareafalangei distale.
Keratoacantomul centrifug marginat reprezintão formã rarã de keratoacantom caracterizatã prin
Clinical aspects
The literature describes several types ofkeratoacanthomas. (Table I)
The typical solitary keratoacanthoma remainsthe most common form and usually develops onsun-exposed areas (cephalic extremity, neck andlimbs) and evolves in 3 phases: the proliferativephase (in which the lesion increases in size to 10-25 mm in diameter in 6-8 weeks), the maturekeratoacanthoma phase (the lesion no longergrows, maintaining its crateriform appearance),followed by the involution phase in whichapproximately 50% of the keratoacanthomasregress spontaneously (in 4-6 weeks), leaving anatrophic and hypopigmented scar. (4)
Mucosal keratoacanthomas are rare and difficultto diagnose. The buccal mucosa is affected moreoften and the probable origin is in the superficialepithelial layer (17).
Subungual keratoacanthomas do not tend toregress spontaneously and may evolve witherosion of the distal phalanx.
Keratoacanthoma centrifugum marginatum is arare form of keratoacanthoma characterised by
Tabelul I
Keratoacantoame solitare Keratoacantoame Keratoacantoame multiple sindromice
Keratoacantomul solitar tipic Keratoacantoame tip Sindromul Muir-TorreFerguson Smith
Keratoacantoame ale mucoaselor Keratoacantoame tip Sindromul KAVCSGrzybowski
Keratoacantoame subunghiale Keratoacantoame tip Witten-Zak
Keratoacantoame atipice: Keratoacantoame multipleKeratoacantomul centrifug marginat asociate cu alte afecþiuniKeratoacantomul gigant cutanate, cu imunodepresiaKeratoacantomul verucos sau induse
Table I
Solitary keratoacanthomas Multiple Syndromickeratoacanthomas keratoacanthomas
Typical solitary keratoacanthoma Ferguson-Smith type Muir-Torre syndrome of keratoacanthomas
Mucosal keratoacanthomas Keratoacanthomas of Grzybowski KAVCS syndromeSubungual keratoacanthomas Keratoacanthomas of Witten
and ZakAtypical keratoacanthomas: Multiple keratoacanthomas
Keratoacanthoma centrifugum marginatum associated with other cutaneousGiant keratoacanthoma disorders, with immuno depression Verrucous keratoacanthoma or induced
extindere perifericã progresivã ºi vindecarecentralã concomitentã. (18)
Keratoacantomul gigant a fost descris maifrecvent la indivizi imunodeprimaþi, apãrând cupredilecþie la nivelul nasului ºi pleoapelor.
Keratoacantoamele multiple tip Ferguson-Smith(keratoacantoame multiple autovindecabile)reprezintã o formã rarã, descrisã pentru primadatã în anul 1934. Este o boalã autozomaldominantã cu debutul în copilãrie sauadolescenþã, caracterizatã prin apariþia bruscã amultiple keratoacantoame, urmatã de involuþiespontanã ºi reapariþie periodicã. Distribuþialeziunilor predominant pe zonele fotoexpusearatã rolul major al radiaþiilor solare îndezvoltarea acestei boli la pacienþii cupredispoziþie geneticã. Deºi majoritatealeziunilor involueazã spontan, tratamentulgrãbeºte vindecarea ºi îmbunãtãþeºte rezultatulcosmetic. (19)
Keratoacantoamele multiple tip Grzybowski(keratoacantoame eruptive generalizate) repre-zintã o boalã foarte rarã, ce apare la adulþii devârstã medie (între a 5-a si a7-a decadã)caracterizatã prin apariþia a sute pânã la mii depapule keratotice foliculare pruriginoase ce sedezvoltã rapid, având tendinþã la confluare maiales la nivelul feþei, gâtului ºi regiunilorintertriginoase. Afectarea extinsã a feþei estefrecvent asociatã cu ectropion, ceea ce duce laxeroftalmie, conjunctivite repetate ºi keratopatiice pot necesita corecþie chirurgicalã. Evoluþiabolii este cronicã ºi, deºi au fost utilizate diferiteopþiuni terapeutice, nu existã o terapie standard,diagnosticul ºi tratamentul aceastei bolirãmânând în continuare o provocare. (9)
Keratoacantoamele tip Witten-Zak reprezintã o formã de keratoacantoame familiale multiplecare combinã caracteristicile tipurilor Grzybowskiºi Ferguson-Smith.(21)
Keratoacantoamele multiple se pot asocia cu alteafecþiuni cutanate (xeroderma pigmentosum, nevsebaceu Jadassohn, lichen plan hipertrofic,prurigo nudularis, papilomatoza cutanatã floridãetc.) (4,9), cu imunodepresia (dupã transplantulmedular, tratamentul cu ciclosporinã, infecþiaHIV/SIDA) (13) sau pot fi induse de medicamente(sorafenib), de traumatisme, sau de agenþichimici (gudron). (9)
progressive peripheral expansion andconcomitant central healing. (18)
Giant keratoacanthoma has been morefrequently reported in immunodepressedindividuals, occurring mainly at the level of thenose and eyelids.
Multiple keratoacanthomas of the Ferguson-Smithtype (multiple self-healing keratoacanthomas) arerare and they were first described in 1934. It is anautosomal dominant disorder with onset inchildhood or adolescence and characterised bythe sudden appearance of multiple kerato-acanthomas, followed by spontaneous involutionand periodical recurrence. The distribution of thelesions mainly on sun-exposed areas shows themajor role of solar radiation in the developmentof this condition in patients with geneticpredisposition. Although the majority of lesionsregresses spontaneously, the treatment speeds upthe healing process and improves the cosmeticoutcome. (19)
Multiple keratoacanthomas of Grzybowski(generalised eruptive keratoacanthoma) is a veryrare disease occurring in middle-aged adults(between the 5th and 7th decade), characterised bythe appearance of hundreds to thousands ofpruritic follicular keratotic papules that developrapidly, with a tendency to fuse in particular on theface, neck and intertriginous regions. An extensiveinvolvement of the face is frequently associatedwith ectropion, which leads to xerophthalmia,recurring conjunctivitis and keratopathy that mayrequire surgical correction. The evolution of thedisease is chronic and, although differenttherapeutic options have been used, there is nostandard therapy and the diagnosis and treatmentof this disease continue to be challenging. (9)
Keratoacanthomas of the Witten and Zak type area form of multiple familial keratoacanthomasthat combine the characteristics of Grzybowskiand Ferguson-Smith types. (21)
Multiple keratoacanthomas may associate withother cutaneous disorders (xeroderma pigmen-tosum, Jadassohn’s nevus sebaceous, hyper-trophic lichen planus, prurigo nodularis, floridcutaneous papillomatosis, etc.) (4, 9), withimmunodepression (after bone marrow transplant,treatment with cyclosporine, HIV/AIDSinfection) (13) or may be induced by medication(sorafenib), traumas or chemical agents (tar). (9)
254
DermatoVenerol. (Buc.), 58: 249-264

255
DermatoVenerol. (Buc.), 58: 247-262
Sindromul Muir-Torre asociazã tumori cutanate(tumori ale glandelor sebacee, keratoacantoame)cu neoplazii viscerale, în special cancer colo-rectal. (22)
Sindromul KAVCS (keratoacanthoma visceralcarcinoma syndrome) presupune keratoacan-toame multiple asociate cu neoplazii ale tractuluigenito-urinar. (22)
Diagnosticul pozitiv
Clinic, keratoacantoamele reprezintã forma-þiuni tumorale nedureroase rapid evolutive cutendinþã spre regresie spontanã în 4-6 luni, ce sedezvoltã cu predilecþie pe zonele fotoexpuse(faþã, gât ºi extremitãþi).
Keratoacantoamele tipice se prezintã subforma unor papule exofitice sau a unor noduli cucentrul deprimat, crateriform, ocupat de un dopkeratozic, cu mãrimi ce variazã de la câþivamilimetri pânã la câþiva centimetri. (23)
Examenul histopatologic rãmâne standardulde aur în diagnosticul keratoacantoamelor. Estede preferat ca leziunea sã fie excizatã înîntregime, cu margini de siguranþã, modificãrilehistopatologice ale bazei tumorii fiind de mareimportanþã în realizarea diagnosticului dife-renþial cu carcinomul spinocelular. (4)
Histopatologic, keratoacantomul se prezintãsub forma unei proliferãri scuamoaseexoendofitice, cu o depresiune crateriformãcentralã umplutã cu mase de keratinã. Epidermulsupraiacent se prelungeºte peste marginilecraterului formând “pinteni”. Keratinocitelesubiacente prezintã frecvent citoplasmãeozinofilicã sau sticloasã, ocazional putând fiprezente abcese intraepiteliale. Baza leziunii estebine delimitatã ºi, de regulã, nu depãºeºte nivelulglandelor sudoripare, fiind înconjuratã deinfiltrat inflamator marcat format din limfocite,histiocite, eozinofile ºi plasmocite. (24)
Totuºi, chiar ºi cu o biopsie corect realizatã,diagnosticul keratoacantomului rãmâne oprovocare, ca urmare a lipsei unor caracteristicihistopatologice suficient de sensibile sauspecifice pentru a-l distinge clar de carcinomulscuamocelular. Ulceraþiile, mitozele numeroase ºipleomorfismul/anaplazia marcate pledeazãpentru diagnosticul de carcinomul spinocelular.(4,23)
Muir-Torre syndrome associates cutaneoustumours (tumours of the sebaceous glands,keratoacanthomas) with visceral neoplasia,especially colorectal cancer. (22)
KAVCS syndrome (keratoacanthoma visceralcarcinoma syndrome) involves multiplekeratoacanthomas associated with genitourinarytract neoplasms. (22)
Positive diagnosis
In clinical terms, keratoacanthomas arerapidly progressing painless tumour formationswith a tendency to regress spontaneously in 4-6months, which develop mainly on sun-exposedareas (face, neck and extremities).
Typical keratoacanthomas are in the form ofexophytic papules or nodules with a depressedcrateriform centre, occupied by a keratotic plug,with sizes ranging from a few millimetres to afew centimetres. (23)
The histopathological examination remainsthe gold standard in the diagnosis ofkeratoacanthomas. It is preferred that the entirelesion is excised, with safety margins, as thehistopathological changes of the tumour base areof great importance in the differential diagnosiswith squamous-cell carcinoma. (4)
From a histopathological point of view, akeratoacanthoma appears as an exo-endophyticsquamous proliferation, with a centralcrateriform depression filled with keratin. Theoverlying epidermis extends over the borders ofthe crater forming “spurs”. Underlyingkeratinocytes often have eosinophilic or glassycytoplasm and intraepithelial abscesses may bepresent occasionally. The base of the lesion is welldefined and usually does not exceed the level ofthe sweat glands, being surrounded by markedinflammatory infiltrate composed oflymphocytes, histiocytes, eosinophils and plasmacells. (24)
However, even with a properly performedbiopsy, the diagnosis of keratoacanthomaremains a challenge due to the lack of histopatho-logical characteristics sensitive or specific enoughto clearly distinguish it from the squamous cellcarcinoma. Ulceration, numerous mitoses andmarked pleomorphism/anaplasia advocate forthe diagnosis of squamous-cell carcinoma. (4, 23)

256
DermatoVenerol. (Buc.), 58: 247-262
Au fost descrise cazuri de keratoacantoamecu evoluþie agresivã sau metastazante ridicândproblema dacã nu cumva keratoacantomul este ovariantã de carcinom spinocelular. (25). Uniiautori au sugerat cã aceastã evoluþie neaºteptatãa keratoacantomului este consecinþa diagnos-ticului greºit al unui carcinom spinocelulariniþial. (26)
Câteva studii au încercat sã gãseascã metodealternative pentru o diferenþiere mai precisã acelor douã entitãþi. O varietate de studii auinvestigat expresia diverºilor markeri celulari înkeratoacantom, incluzând: molecula de adeziunecelularã vascularã (VCAM)(CD106), molecula deadeziune intercelularã (ICAM)(CD54), receptorulde angiotensinã tip 1, p53, antigenul celularnuclear proliferativ (PCNA), telomeraza, ciclo-oxigenaza-2 (COX-2), bcl-2, Ki-67, E-caderina,p16, keratina, filagrina, IMP-3, etc. Din pãcate,nici una dintre aceste metode nu s-a dovedit a fispecificã ºi sigurã în diferenþierea kerato-acantomului de carcinomul spinocelular. (4,27,28,29,30,31)
Evaluarea expresiei TGF alfa în celuleletumorale din keratoacantom ºi carcinomulspinocelular a evidenþiat o coloraþie TGF alfa înprincipal difuzã ºi fãrã colorarea periferieicelulelor în 1-2 straturi în keratoacantom spredeosebire de carcinom spinocelular care aprezentat o coloraþie “în pete” ºi colorareaperiferiei celulelor în 1-2 straturi. (32)
Un studiu recent care a comparat celuleleimunosupresoare ºi imunomodulatoare implicateîn keratoacantom ºi carcinomul spinocelular aarãtat cã un numãr mai mare de celule CD3+
Fox3+ Tregs au fost observate în carcinoamelespinocelulare comparativ cu cele observate înkeratoacantoame. De asemenea, un numãr maimare de macrofageCD163+ ºi celule MMP-9+ aufost detectate în carcinoamele spinocelulare iarprezenþa celulelor producãtoare de IL-27 a fostcrescutã în keratoacantoame. În plus, expresiapSTAT1 în celulele tumorale a fost observatãnumai în keratoacantoame. Aceste constatãrisugereazã cã inducþia celulelor imunosupresoareºi imunomodulatorii diferã între keratoacantomºi carcinomul spinocelular. (33).
Cases of aggressively progressing ormetastatic keratoacanthomas have been reported,raising the issue of whether keratoacanthoma is avariant of squamous-cell carcinoma. (25). Someauthors have suggested that this unexpectedevolution of keratoacanthoma is the consequenceof an initial misdiagnosed squamous-cellcarcinoma. (26)
A few studies have attempted to findalternative methods for a more accuratedifferentiation of the two entities. A variety ofstudies have investigated the expression ofvarious cellular markers in keratoacanthomas,including: vascular cell adhesion molecule(VCAM) (CD106), intercellular adhesionmolecule (ICAM) (CD54), angiotensin receptortype 1, p53, proliferating cell nuclear antigen(PCNA), telomerase, cyclooxygenase-2 (COX-2),bcl-2, Ki-67, E-cadherin, p16, keratin, filaggrin,IMP-3, etc. Unfortunately, none of these methodshas proved to be specific and reliable indifferentiating keratoacanthoma from squamous-cell carcinoma. (4, 27, 28, 29, 30, 31)
The assessment of TGF-alpha expression intumour cells in keratoacanthomas andsquamous-cell carcinomas has showed TGF-alpha staining mainly diffusely and withoutperipheral staining of cells in 1-2 layers of thekeratoacanthoma unlike the squamous-cellcarcinoma that had a mostly “patchy” stainingand peripheral staining of cells in 1-2 layers. (32)
A recent study comparing the immuno-suppressive and immunomodulatory cellsinvolved in keratoacanthoma and squamous-cellcarcinoma has showed that a greater number ofCD3+ Foxp3+ Treg cells are observed insquamous-cell carcinomas compared to thatobserved in keratoacanthomas. Also, a greaternumber of CD163+ macrophages and MMP-9+cells are detected in squamous-cell carcinomasand the presence of IL-27-producing cells ishigher in keratoacanthomas. Moreover, thepSTAT1 expression in tumour cells is observedonly in keratoacanthomas. These findingssuggest that the induction of immuno-suppressive and immunomodulatory cells differsbetween keratoacanthoma and squamous-cellcarcinoma. (33).

257
DermatoVenerol. (Buc.), 58: 247-262
Diagnosticul diferenþial
Diagnosticul diferenþial al keratoacantomuluise face, în primul rînd, cu carcinomul spinocelular
datoritã caracteristicilor clinice ºi histopatologiceasemãnãtoare. De obicei, diferenþierea clinicã aacestor leziuni poate fi fãcutã relativ uºor datoritãcreºterii rapide ºi a aspectului caracteristic alkeratoacantomului. Keratoacantomul se prezintãsub forma unui nodul de formã molluscoidã cuun dop keratozic central, în timp ce carcinomulspinocelular se prezintã sub forma unui nodul saua unei ulceraþii care nu se vindecã spontan. (32)
Alte leziuni cutanate luate în discuþie pentrudiagnosticul diferenþial al keratoacantoamelorsunt reprezentate de: carcinomul bazocelular
nodular (tumorã nodularã cu margini perlate ºitelangiectazii pe suprafaþã ce prezintã frecventulceraþie centralã), verucile vulgare (papulehiperkeratozice, cu sângerãri punctiformevizibile pe suprafaþã), molluscum contagiosum
(multiple papule ombilicate central, de culoareapielii), prurigo nodular (noduli hiperkeratozici deculoare rosie-brunã, intens pruriginoºi), metastaze
cutanate (greu de diagnosticat, examenulhistopatologic, imunohistochimic ºi istoriculpersonal de neoplazii orienteazã diagnosticul),melanomul acromic ( nodul moale, uºor sângerândsau ulcerat, frecvent greu de diagnosticat),papuloza limfomatoidã (erupþie recurentã formatãdin papule ºi noduli brun-eritematoºi, uneoripapulonecrotici, care se vindecã spontan cuformare de cicatrice atrofice), keratoze actinice ºi
seboreice, cornul cutanat, chiste sebacee ºi epiteliale,carcinoame verucoase, ºancrul de sporotricozã, infecþii
atipice cu micobacterii etc. (34,35,36)
Tratamentul
Tratamentul profilactic presupune evitareafactorilor predispozanþi ºi/sau favorizanþi(evitarea expunerii la raze UV, carcinogenichimici, traumatisme, factori termici etc.)
Prevenþia ºi diagnosticul precoce al neo-plaziilor viscerale trebuie luate în considerare încazul pacienþilor cu sindrom Muir-Torre ºi arudelor lor. Frecvenþa crescutã a canceruluicolorectal la aceºti pacienþi justificã recoman-darea de a se efectua colonoscopie anual,începând cu vârsta de 25 de ani. (37)
Differential diagnosis
The differential diagnosis of keratoa-canthoma is performed primarily with thesquamous-cell carcinoma due to the similar clinicaland histopathological characteristics. The clinicaldifferentiation of these lesions is usuallyrelatively easily accomplished thanks to the rapidgrowth and the specific appearance ofkeratoacanthoma. A keratoacanthoma presents inthe shape of a molluscoid nodule with a centralkeratotic plug, while a squamous-cell carcinomapresents in the shape of a nodule or ulcer thatdoes not heal spontaneously. (32)
Other cutaneous lesions considered for thedifferential diagnosis of keratoacanthomas are:nodular basal cell carcinoma (nodular tumour withpearly-appearing borders and telangiectasias onthe surface showing frequent central ulceration),verruca vulgaris (hyperkeratotic papules withpinpoint bleeding visible on the surface),molluscum contagiosum (multiple skin-colouredpapules with central umbilication), prurigonodularis (intensely pruritic red-brownhyperkeratotic nodules), cutaneous metastases(difficult to diagnose, histopathological,immunohistochemical examination and personalhistory of neoplasia guide the diagnosis),achromic melanoma (soft nodule, slightly bleedingor ulcerated, often difficult to diagnose),lymphomatoid papulosis (recurrent rash consistingof papules and brown erythematous sometimespapulonecrotic nodules, which heal spon-taneously with atrophic scar formation), actinicand seborrheic keratoses, cutaneous horn, sebaceousand epithelial cysts, verrucous carcinomas, sporotri-chosis chancre, atypical mycobacterial infections, etc.(34, 35, 36)
Treatment
The prophylactic treatment involves theavoidance of predisposing and/or contributingfactors (avoidance of exposure to UV rays, chemicalcarcinogens, traumas, thermal factors, etc.).
The prevention and early diagnosis ofvisceral neoplasia should be considered inpatients with Muir-Torre syndrome and theirrelatives. The high frequency of colorectal cancerin these patients justifies the recommendation to conduct annual colonoscopies from the age of25. (37)
258
DermatoVenerol. (Buc.), 58: 247-262
Tratamentul curativ. Au fost descrise multiplemodalitãþi terapeutice pentru keratoacantoamelemultiple. (Tabel II)
Tratamentul chirurgical
Excizia chirurgicalã cu margini de siguranþãreprezintã tratamentul standard al kerato-acantoamelor solitare relativ mici. Chirurgiamicrograficã Mohs poate reprezenta tratamentulde elecþie pentru leziunile agresive, cu creºtererapidã, localizate la nivelul feþei. (4,22,23)Recidivele pot apãrea în 4-8% din cazuri la câtevasãptãmâni dupã intervenþie, ºi pot fi rezultatulunei excizii incomplete. (2,4)
Crioterapia, chiuretajul (+/- electrocauterizareabazei), terapia laser (argon, YAG sau CO2) au fostutilizate cu succes în tratamentul leziunilor mici,solitare. (4)
Radioterapia este utilã în tratamentulkeratoacantoamelor recidivante, pentru leziunileagresive sau în cazul pacienþilor în vârstã la carenu se poate realiza excizia chirurgicalã. (14,23)
Tratamentul intralezional ºi topic
Terapia intralezionalã la fiecare 2 sãptãmânicu metotrexat 12.5mg/ml, 5-fluorouracil 50mg/ml sau interferon alfa-2a s-au dovediteficiente în tratamentul leziunilor mari, izolate înaproximativ 4-6 sãptãmâni. (22,23). Interferonulalfa-2b intralezional, în doza de 3x1 milionUI/sãptãmânã pânã la 3x3 milioaneUI/sãptãmâmã s-a dovedit util în tratamentulkeratoacantoamelor mari, cu localizare care nupermite excizia sau în cazurile în care a fost
Curative treatment. Many therapeuticapproaches have been described for multiplekeratoacanthomas. (Table II)
Surgical treatment
The surgical excision with safety margins isthe standard treatment for relatively smallsolitary keratoacanthomas. Mohs micrographicsurgery may be the treatment of choice foraggressive fast-growing lesions, located on theface. (4, 22, 23) Relapses can occur in 4-8% ofcases in a few weeks after intervention and maybe the result of an incomplete excision. (2, 4)
Cryotherapy, curettage (+/-electrocauterisation ofthe base), laser therapy (argon, YAG or CO2) havebeen used successfully in the treatment of smallsolitary lesions. (4)
Radiotherapy is useful in the treatment ofrecurrent keratoacanthomas, of aggressivelesions or in elderly patients who cannot undergosurgical excision. (14, 23)
Intralesional and topical treatment
Intralesional therapy every 2 weeks withmethotrexate 12.5 mg/ml, 5-fluorouracil 50mg/ml or interferon alpha-2a has proved to beeffective in treating large isolated lesions inapproximately 4-6 weeks. (22, 23). Intralesionalinterferon alpha-2b in doses of 3x1 millionIU/week to 3x3 million IU/week has proved tobe useful in the treatment of largekeratoacanthomas whose location preventsexcision or in cases where surgical interventionwas refused, showing favourable results in 7-12
Tabelul II
Tratamentul ablativ Tratamentul intralezional Tratamentul topic Tratamentul sistemic
Excizia chirurgicalã Metotrexat Imiquimod RetinoiziChirurgia micrograficã Mohs 5-fluorouracil 5-fluorouracil MetotrexatCrioterapia Inteferon alfa-2a/2b Podofilinã CiclofosfamidãChiuretajul Bleomicinã 5-fluorouracilElectroterapia Corticosteroizi Interferon alfa-2aTerapia laser Erlotinib
Table II
Ablative treatment Intralesional treatment Topical treatment Systemic treatment
Surgical excision Methotrexate Imiquimod RetinoidsMohs micrographic surgery 5-fluorouracil 5-fluorouracil MethotrexateCryotherapy Interferon alpha 2a/2b Podophyllin CyclophosphamideCurettage Bleomycin 5-fluorouracilElectrotherapy Corticosteroids Interferon alpha-2aLaser therapy Erlotinib

259
DermatoVenerol. (Buc.), 58: 247-262
refuzatã intervenþia chirurgicalã cu rezultatefavorabile în 7-12 sãptãmâni. (38) Se pare cãterapia intralezionalã cu metotrexat necesitã maipuþine ºedinþe decât terapia intralezionalã cu 5-fluorouracil. Bleomicina intralezional, deºieficientã, a fost evitatã din cauza durerii asociatetratamentului. Triamcinolonul utilizat intra-lezional 5-10 mg/ml diluat în 2% lidocainã aprezentat o ratã de regresie de 70% dupa 2-3ºedinþe. Totuºi, ratele de regresie raportate dupãadministrarea de corticoizi intralezional nu suntla fel de mari ca ºi cele induse de alþi agenþi, ca 5-fluorouracilul. (39)
Tratamentele topice cu imiquimod cremã 5%sau cu 5-fluorouracil pot de asemenea sã fieeficiente. (2) Podofilina topic ºi-a dovediteficienþa, singurã sau asociatã chiuretãrii,electroterapiei sau radioterapiei. (40)
Terapia sistemicã
Terapia sistemicã a fost utilizatã pentrutratamentul formelor multiple. Retinoizii(etetrinat 1mg/kg/zi timp de 2 luni) pot fieficienþi în tratamentul keratoacantoamelormultiple eruptive tip Ferguson Smith, a formeieruptive generalizate tip Grzybowski ºi akeratoacantoamelor centrifuge marginate. (2,4)
Unele studii au descris utilizarea meto-trexatului sistemic, care este mai puþin costisitordecât alte medicamente, dar au fost raportatecazuri de pancitopenie, toxicitate hepaticã ºitoxicitate pulmonarã manifestatã prin tuse seacã,neproductivã. Ciclofosfamida ºi 5-fluorouracilulintravenos precum ºi terapia fotodinamicãreprezintã alte alternative. (4,14,41)
Combinaþiile de imiquimod cu chimioterapiasistemicã sau intralezionalã cu metotrexat, 5-fluorouracil, ciclofosfamidã, alfa-interferon-2a s-au dovedit utile dar cu asumarea riscurilortoxicitãþii. S-a mai raportat utilizarea imiquimo-dului 5% în asociere cu doze mici de retinoizi(acitretin 25mg po/zi) pentru tratamentulkeratoacantoamelor multiple, cu rezoluþiacompletã a leziunilor dupã 2 luni.(42)
Au mai fost prezentate cazuri de kerato-acantoame multiple sau keratoacantoame centri-fuge marginate nerezecabile, care au avutrãspuns bun la terapia cu erlotinib (inhibitor detirozin-kinazã) 150 mg/zi.(36,43)
weeks. (38) It appears that intralesional therapywith methotrexate requires fewer sessions thanintralesional therapy with 5-fluorouracil.Intralesional bleomycin, although effective, hasbeen avoided because of the pain associated withthe treatment. Intralesional triamcinolone 5-10mg/ml diluted in 2% lidocaine has showed aregression rate of 70% after 2-3 sessions.However, the regression rates reported after theadministration of intralesional corticoids are notas high as those induced by other agents, such as5-fluorouracil. (39)
Topical treatments with imiquimod cream 5%or 5-fluorouracil may also be effective. (2) Topicalpodophyllin has proved its effectiveness usedalone or in combination with curettage,electrotherapy or radiotherapy. (40)
Systemic therapy
Systemic therapy has been used to treatmultiple forms. Retinoids (etretinate 1mg/kg/day for 2 months) may be effective in thetreatment of the Ferguson-Smith type of multipleeruptive keratoacanthomas, of the generalisederuptive keratoacanthomas of Grzybowski and of keratoacanthoma cen-trifugum marginatum.(2, 4)
Some studies have described the use ofsystemic methotrexate, which is less expensivethan other medicines, but there have been casesof pancytopenia, hepatic toxicity and pulmonarytoxicity evidenced by dry unproductive cough.Intravenous cyclophosphamide and 5-fluoro-uracil, as well as photodynamic therapy arefurther alternatives. (4, 14, 41)
The combinations of imiquimod withsystemic chemotherapy or intralesionalmethotrexate, 5-fluorouracil, cyclophosphamide,interferon-alpha-2a have proved to be useful, butwith risks of toxicity. The use of imiquimod 5% incombination with small doses of retinoids(acitretin 25mg po/day) has also been reportedfor the treatment of multiple keratoacanthomas,with complete resolution of the lesions after 2months. (42)
There have also been cases of multiplekeratoacanthomas or unresectable kerato-acanthoma centrifugum marginatum that haveshown good response to therapy with erlotinib(tyrosine-kinase inhibitor) 150 mg/day. (36,43)

Evoluþie clinicã ºi prognostic
Prognosticul pentru keratoacantoamelesolitare este foarte bun dupã excizia chirurgicalã.Leziunile recidivante pot necesita tratament maiagresiv (6,23)
Pacienþii necesitã urmãrire atentã ºi de duratãîn vederea diagnosticãrii precoce a cancerelor depiele non-melanotice, cum ar fi carcinomulspinocelular. (23)
Deºi de obicei evoluþia keratoacantoameloreste benignã, cu vindecare spontanã, uneori potpersista mai mult timp sau pot progresa spre uncarcinom spinocelular motiv pentru care untratament aplicat precoce ºi corect poate scãdeariscul prejudiciilor funcþionale ºi estetice.
Concluzii
Keratoacantoamele multiple au fost descriseîn asociere cu alte afecþiuni dermatologice,inclusiv lupusul eritematos discoid, procesulinflamator putând reprezenta triggerul îndezvoltarea keratoacantoamelor. Un alt factorpredispozant ºi/sau favorizant este reprezentatde expunerea la raze ultraviolete, atât leziunile delupus eritematos discoid cât ºi kerato-acantoamele fiind prezente pe zonele fotoexpuse.
Tratamentul keratoacantoamelor multipleasociate cu alte leziuni inflamatorii rãmâne încontinuare o provocare, chirurgia fiind greupracticabilã pe de o parte din cauza leziunilorextinse, pe de altã parte din cauza substratuluiinflamator.
Clinical course and prognosis
The prognosis for solitary keratoacanthomasis very good after surgical excision. Recurrentlesions may require a more aggressive treatment(6, 23).
Patients need careful and long-lastingmonitoring in order to achieve early diagnosis ofnon-melanoma skin cancers, such as squamous-cell carcinoma. (23)
Although the evolution of keratoacanthomasis usually benign, with spontaneous healing,sometimes they may persist for a longer time ormay progress to squamous-cell carcinoma, whichis why an early and correct treatment can decreasethe risk of functional and aesthetic damage.
Conclusions
Multiple keratoacanthomas have beendescribed in association with otherdermatological disorders, including discoidlupus erythematosus, as the inflammatoryprocess may be the trigger in the development ofkeratoacanthomas. Another predisposing and/orcontributory factor is the exposure to UV rays,given that both discoid lupus erythematosuslesions and keratoacanthomas are present onsun-exposed areas.
The treatment of multiple keratoacanthomasassociated with other inflammatory lesionscontinues to be challenging, considering thatsurgery is difficult to perform on the one handdue to the extensive lesions, and on the otherhand due to the inflammatory substrate.
DermatoVenerol. (Buc.), 58: 249-264
260
Bibliografie / Bibliography
1. Kluger N, Minier-Thoumin C, Plantier F. Keratoacanthoma occurring within the red dye of a tattoo. J Cutan Pathol.2008; 35(5):504-7.
2. Schwartz RA. Keratoacanthoma: A ClinicoPathologic Enigma. Dermatol Surg 2004; 30:326-333.3. Leibovitch I, Huilgol SC, James CL, Hsuan JD, Davis G, Selva D. Periocular keratoacanthoma: can we always rely
on the clinical diagnosis?. Br J Ophthalmol. 2005; 89(9): 1201-4.4. Karaa A, Khachemoune A. Keratoacanthoma: a tumor in search of a classification. Int J Dermatol. 2007; 46(7):671-
8.5. Kaptanoglu AF, Kutluay L. Keratoacanthoma developing in previous cryotherapy site for solar keratosis. J Eur
Acad Dermatol Venereol. 2006; 20(2):197-8.6. Chuang Tsu-Yi, Brashear R. Keratoacanthoma. Medscape Reference. N.p., 18 May 2011.7. Weinstock MA, Coulter S, Bates J, et al. Human papillomavirus and widespread cutaneous carcinoma after PUVA
photochemotherapy. Arch Dermatol. 1995; 131:701–4.8. Craddock KJ, Lauzon GJ, Tron VA. Multiple keratoacanthomas arising post – UVB therapy. J Cut Med Surg. 2004;
8:239–43.
261
DermatoVenerol. (Buc.), 58: 247-262
9. Nofal A, Assaf M, Nofal E, Alradi M.Generalized eruptive keratoacanthoma:proposed diagnostic criteria andtherapeutic evaluation. J Eur Acad Dermatol Venereol. 2014; 28(4):397-404.
10. Kopf AW, Bart RS. Development of more keratoacanthomas following skin testing with nitrogen mustard in apatient with the multiple keratoacanthoma syndrome. J Dermatol Surg Oncol. 1979; 5(6):450-1.
11. Goldenberg G, Patel S, Patel MJ, Williford P, Sangueza O. Eruptive squamous cell carcinomas, keratoacanthomatype, arising in a multicolor tattoo. J Cutan Pathol. 2008; 35(1):62-4.
12. Smith KJ, Haley H, Hamza S, Skelton HG. Eruptive keratoacanthoma-type squamous cell carcinomas in patientstaking sorafenib for the treatment of solid tumors. Dermatol Surg. 2009; 35(11):1766-70.
13. Kar HK, Sabhnani ST, Gautam RK, Sharma PK, Solanki K, Bhardwaj M. Non-familial multiple keratoacanthomasin a 70 year-old long-term non-progressor HIV-seropositive man. Indian J Dermatol Venereol Leprol. 2008; 74 (2): 136-8.
14. Kurien A, Henderson C, Lee S. Recurrent keratoacanthoma with vascular invasion: a diagnostic and managementdilemma. Australas J Dermatol. 2009; 50(3):194-7.
15. Payne D, Newman C, Tyring S. Human papillomavirus DNA in nonanogenital keratoacanthoma and squamouscell carcinoma of patients with HIV infection. J Am Acad Dermatol. 1995; 33(6):1047-9.
16. Foxton G, Delaney T. Eruptive keratoacanthoma and squamous cell carcinoma complicating imiquimod therapy:response to oral acitretin. Australas J Dermatol. 2009; 50(3):194-7.
17. Eversole LR, Leider AS, Alexander G. Intraoral and labial keratoacanthoma. Oral Surg Oral Med Oral Pathol. 1982;54(6):663-7.
18. Mangas C, Bielsa I, Ribera M, Fernández-Figueras MT, Ferrándiz C. A case of multiple keratoacanthomacentrifugum marginatum. Dermatol Surg. 2004; 30(5):803-6.
19. Aydin F, Senturk N, Sabanciler E, Canturk MT, Turanli AY. A case of Ferguson-Smith type multiplekeratoacanthomas associated with keratoacanthoma centrifugum marginatum: response to oral acitretin. Clin ExpDermatol. 2007; 32(6):683-6.
20. Katoulis AC, Bozi E.Multiple Keratoacanthoma, Ferguson Smith Type.Orphanet Encyclopedia. August 2005http://www.orpha.net/data/patho/GB/uk-Keratoacanthoma.pdf.
21. Miller JJ. Multiple Keratoacanthomas, Ferguson-Smith Variant.Medscape www.medscape.com/viewarticle/714022_2.
22. Feldman RJ, Maize JC. Multiple keratoacanthomas in a young woman: report of a case emphasizing medicalmanagement and a review of the spectrum of multiple keratoacanthomas. Int J Dermatol. 2007; 46(1):77-9.
23. Khashayar S, Abdulhafe, Amor K. Sporadic and Syndromic Keratoacanthomas: Diagnosis and Management.Dermatology Nursing. 2007; 19(2):166.
24. Sleater JP, Beers BB, Stephens CA, Hendricks JB. Keratoacanthoma: a deficient squamous cell carcinoma? Study ofbcl-2 expression. J Cutan Pathol. 1994; 21(6):514-9.
25. Li J, Wang K, Gao F, Jensen TD, Li ST, DeAngelis PM, Kølvraa S, Proby C, Forslund O, Bolund L, Clausen F. ArrayComparative Genomic Hybridization of Keratoacanthomas and Squamous Cell Carcinomas: Different Patterns ofGenetic Aberrations Suggest Two Distinct Entities. Journal of Investigative Dermatology 2012; 132: 2060-6.
26. Annest NM, VanBeek MJ, Arpey CJ, Whitaker DC. Intralesional methotrexate treatment for keratoacanthomatumors: a retrospective study and review of the literature. J Am Acad Dermatol. 2007; 56(6):989-93.
27. Kaabipour E, Haupt HM, Stern JB, Kanetsky PA, Podolski VF, Martin AM. p16 expression in keratoacanthomasand squamous cell carcinomas of the skin: an immunohistochemical study. Arch Pathol Lab Med. 2006; 130(1):69-73.
28. Papadavid E, Pignatelli M, Zakynthinos S, Krausz T, Chu AC. The potential role of abnormal E-cadherin andalpha-, beta- and gamma-catenin immunoreactivity in the determination of the biological behaviour ofkeratoacanthoma. Br J Dermatol. 2001; 145(4):582-9.
29. Ito Y, Kurokawa I, Nishimura K, Hakamada A, Isoda K, Yamanaka K, Tsubura A, Mizutani H. Keratin andfilaggrin expression in keratoacanthoma. J Eur Acad Dermatol Venereol. 2008; 22(3):353-5.
30. Connolly M, Narayan S, Oxley J, de Berker DA. Immunohistochemical staining for the differentiation ofsubungual keratoacanthoma from subungual squamous cell carcinoma. Clin Exp Dermatol. 2008; 33(5):625-8.
31. Soddu S, Di Felice E, Cabras S, Castellanos ME, Atzori L, Faa G, Pilloni L. IMP-3 expression in keratoacanthomasand squamous cell carcinomas of the skin: an immunohistochemical study. Eur J Histochem. 2013; 57(1):e6.
32. Cabrijan L, Lipozenciæ J, Batinac T, Lenkoviæ M, Zgombiæ ZS. Differences between keratoacanthoma andsquamous cell carcinoma using TGF-alpha. Coll Antropol. 2013; 37(1):147-50.
33. Kambayashi Y, Fujimura T, Aiba S. Comparison of immunosuppressive and immunomodulatory cells inkeratoacanthoma and cutaneous squamous cell carcinoma. Acta Derm Venereol. 2013; 93(6):663-8.
262
DermatoVenerol. (Buc.), 58: 247-262
34. Muniz Tinoco AP, Gaia B, Kawa Kac B, Paes de Oliveira Neto M, Sporotrichosis chancre simulatingkeratoacanthoma followed by Sweet’s-like syndrome. J Am Acad Dermatol. 2007; 56(2):128.
35. V’lckova-Laskoska MT, Laskoski DS. Keratoacanthoma centrifugum marginatum: a rare atypical variant ofkeratoacanthoma. Clin Exp Dermatol. 2008; 33(3):259-61.
36. Bulj TK, Krunic AL, Cetner AS, Villano JL. Refractory aggressive keratoacanthoma centrifugum marginatum of thescalp controlled with the epidermal growth factor receptor inhibitor erlotinib. Br J Dermatol. 2010; 163(3):633-7.
37. Schwartz RA, Torre DP. The Muir-Torre syndrome: a 25-year retrospect. J Am Acad Dermatol. 1995; 33(1):90-104.38. Anadolu R, Akay BN, Bodamyali P, Akyol A. Giant keratoacanthoma-type low-grade squamous cell carcinoma of
the upper lip: Response to intralesional interferon alpha-2B. J Dermatolog Treat. 2011; 22(4):239-40.39. Sanders S, Busam KJ, Halpern AC, Nehal KS. Intralesional corticosteroid treatment of multiple eruptive
keratoacanthomas: case report and review of a controversial therapy. Dermatol Surg. 2002; 28(10):954-8.40. Cipollaro VA. The use of podophyllin in the treatment of keratoacanthoma. Int J Dermatol. 1983; 22(7):436-40.41. Leonard AL, Hanke CW. Treatment of giant keratoacanthoma with intralesional 5-fluorouracil. J Drugs Dermatol
2006; 5: 454–456.42. Barysch MJ, Kamarashev J, Lockwood LL, Dummer R. Successful treatment of multiple keratoacanthoma with
topical imiquimod and low-dose acitretin. J Dermatol. 2011; 38(4): 390-2.43. Reid DC, Guitart J, Agulnik M, Lacouture ME. Treatment of multiple keratoacanthomas with erlotinib. Int J Clin
Oncol. 2010; 15(4): 413-5.
Conflict de interese Conflict of interestNEDECLARATE NONE DECLARED
Adresa de corespondenþã: [email protected]
Correspondance address: [email protected]







