
Mic
higa
n Ea
r In
stitu
te
Facial NerveProblems
www.michiganear.com
34015-56111-110 BOOK Facial Nerve Problems.indd 1 2/13/18 10:09 AM

1
Dennis I. Bojrab, MD
Seilesh C. Babu, MD
John J. Zappia, MD, FACS
Eric W. Sargent, MD, FACS
Eleanor Y. Chan, MD
Robert S. Hong, MD
Ilka C. Naumann, MD
Candice C. Colby, MD
Christopher A. Schutt, MD
Providence Medical Building30055 Northwestern HighwaySuite 101Farmington Hills, MI 48334
Beaumont Medical Building3555 W. Thirteen Mile RoadSuite N-210Royal Oak, MI 48073
Oakwood Medical Building18181 Oakwood Blvd.Suite 402Dearborn, MI 48126
Providence Medical Center26850 Providence ParkwaySuite 130Novi, MI 48374
248-865-4444 phone248-865-6161 fax
DO
CTO
RS
LOC
AT
ION
S
34015-56111-110 BOOK Facial Nerve Problems.indd 1 2/13/18 10:09 AM

3
WELCOME
Welcome to the Michigan Ear Institute, one of the nation’s leading surgical groups specializing in hearing, balance and facial nerve disorders. The Michigan Ear Institute is committed to providing you with the highest quality diagnostic and surgical treatment possible.
Our highly experienced team of physicians, audiologists and clinical physiologists have established international reputations for their innovative diagnostic and surgical capabilities, and our modern, attractive facility has been designed with patient care and convenience as the foremost criteria.
It is our privilege to be able to provide care for your medical problems and we will strive to make your visit to the Michigan Ear Institute a positive and rewarding experience.
34015-56111-110 BOOK Facial Nerve Problems.indd 3 2/13/18 10:09 AM

4
A DISCUSSION OF FACIAL NERVE PROBLEMS
Twitching, weakness or paralysis of the face is a symptom of some disorders involving the facial nerve. It is not a disease in itself. The disorder may be caused by many different diseases, including cir-culatory disturbances, injury, infection or a tumor.
Facial nerve disorders are accompanied at times by a hearing impairment. This impairment may or may not be related to the facial nerve problems.
FUNCTION OF THE FACIAL NERVE
The facial nerve resembles a telephone cable and contains hundreds of individual nerve fibers. Each fiber carries electrical impulses to a specific facial muscle. Acting as a unit this nerve allows us to laugh, cry, smile or frown, hence the name, “the nerve of facial expression”. Each of the two facial nerves not only carries nerve impulses to the mus-cles of one side of the face, but also carries nerve impulses to the tear glands, saliva glands, to the muscle of a small middle ear bone (the stapes) and transmits taste fibers from the front of the tongue and pain fibers from the ear canal. As such, a disorder of the facial nerve may result in twitching, weak-ness or paralysis of the face, dryness of the eye or the mouth, loss of taste, increased sensitivity to loud sound and pain in the ear.
An ear specialist is often called upon to manage fa-cial nerve problems because of the close association of this nerve with the ear structures. After leaving the brain the facial nerve enters the temporal bone (ear bone) through a small bony tube (the internal audi-tory canal) in very close association with the hearing and balance nerves. Along its inch and a half course through a small bony canal in the temporal bone
34015-56111-110 BOOK Facial Nerve Problems.indd 4 2/13/18 10:09 AM

5
the facial nerve winds around the three middle ear bones, in back of the eardrum, and then through the mastoid to exit below the ear. Here it divides into many branches to supply the facial muscles. During its course through the temporal bone the facial nerve gives off several branches: to the tear gland, to the stapes muscle, to the tongue and saliva glands and to the ear canal.
DIAGNOSIS OF A FACIAL NERVE DISORDER
Abnormality of facial nerve function may result from circulatory changes, infections, tumors, or injuries. An extensive evaluation is often necessary to deter-mine the cause of the disorder and localize the area of nerve involvement.
Hearing TestTests of hearing are done to determine if the nerve disorder has involved the delicate hearing mecha-nism. When the face is totally paralyzed a special hearing test (stapedius reflex) helps to localize the problem area.
Internal Auditory Canal Brain
TEARING
TASTE
FACIAL EXPRESSION
FACIAL N.
External Ear Canal
Mastoid Bone
Ear Drum
Stapes Muscle
Balance Canals
34015-56111-110 BOOK Facial Nerve Problems.indd 5 2/13/18 10:09 AM

6
“X-Rays”Scans are usually taken to determine if there is infec-tion, tumor or bone fracture. (CT or MRI scans).
Tear TestA test of eye’s ability to tear may be helpful to deter-mine the location of the facial nerve involvement.
Balance TestAn ENG (electronystagmography) test of the balance system is advised in some cases to clarify the cause or location of the facial nerve disorder.
Electrical TestsThere are three electrical tests of the facial nerve function that we may use: nerve excitability test, electroneurography and electromyography.
Nerve Excitability TestThe facial nerve excitability test helps us to deter-mine the extent of nerve fiber damage in cases of total paralysis. The test may be normal despite the paralysis, indicating a better outlook for return of function. In such cases the excitability test may be repeated every day or so to detect any change which would indicate progressive deterioration.
Electroneurography (ENoG)Electroneurography involves the use of a computer to measure the muscle response to electrical stimu-lation of the facial nerve. Recording electrodes are placed on the face and the facial nerve is stimulated with small electrical currents. Muscle contractions are recorded by the computer.
ElectromyographyElectromyography may be indicated in cases of long standing paralysis. This test helps us to know if the nerve and muscles are recovering. Tiny needles are used to measure the responses.
34015-56111-110 BOOK Facial Nerve Problems.indd 6 2/13/18 10:09 AM

7
EYE CAREThe most serious complication that may develop as the result of total facial nerve paralysis is an ulcer of the cornea of the eye. It is important that the eye on the involved side be protected from this complica-tion by keeping the eye moist. Closing the eye with the finger is an effective way of keeping the eye moist. One should use the back of the finger rather that the tip in doing this to insure that the eye is not injured.
Glasses should be worn whenever you are outside. This will help prevent particles of dust from becom-ing lodged in the eye.
If the eye is dry, you may be advised to use artificial tears. The drops should be used as often as necessary to keep the eye moist. Ointment may be prescribed for use at bedtime.
At times it is necessary to tape the eyelid closed with tape. It is best for a family member to do this to insure that the eye is firmly closed and will not be injured by the tape.
If pain, redness or visual loss occurs despite lubri-cation, you should see an ophthalmologist (eye specialist) immediately.
In many cases where long standing paralysis is anticipated it may be necessary to insert a tiny gold weight into the eyelid or perform some other long standing procedure to help the eyelid close.
34015-56111-110 BOOK Facial Nerve Problems.indd 7 2/13/18 10:09 AM

8
BELL’S PALSY AND HERPES ZOSTER
Bell’s PalsyThe most common condition resulting in facial nerve weakness or paralysis is Bell’s palsy, named after Sir Charles Bell who first described the condition. The underlying cause of Bell’s palsy is not known, but it probably is due to a virus infection of the nerve. We know that the nerve swells in its tight bony canal. This swelling results in pressure on the nerve fibers and their blood vessels. Treatment is directed at de-creasing the swelling and restoring the circulation so that the nerve fibers may again function normally.
Herpes Zoster OticusA condition similar to Bell’s palsy is herpes zoster oticus, “shingles” of the facial nerve. In this condi-tion there is not only facial weakness but often hear-ing loss, unsteadiness and painful ear blisters. These additional symptoms usually subside spontaneously but some hearing loss may be permanent.
TreatmentTreatment of the facial paralysis in these two condi-tions may be either medical or surgical.
Medical TreatmentMedical treatment, (with steroids or antiviral medica-tions), may be instituted to decrease the swelling and stimulate the circulation.
Surgical Treatment❒ Mastoid decompression of the facial nerve. Surgi-cal decompression of the facial nerve is indicated in cases of paralysis when the electrical tests show that the nerve function is deteriorating. This operation is performed under general anesthesia and requires hospitalization for two to four days. Through an inci-sion behind the ear the rigid mastoid bone around
34015-56111-110 BOOK Facial Nerve Problems.indd 8 2/13/18 10:09 AM

9
the swollen nerve is removed, relieving pressure so that the circulation may be restored.
The degree and rapidity of recovery of facial nerve function depends upon the amount of damage pres-ent in the nerve at the time of surgery. Recovery may take from 3 to 12 months and may not be complete. Fortunately, it is unusual to develop a hearing im-pairment following surgery but this depends on the extent of surgery needed in the individual case.
❒ Middle fossa facial nerve decompression. At times deeper portions of the facial nerve are affected. In that case surgery may also involve an incision above the ear, with removal of a small portion of the skull. The need for this procedure can usually be deter-mined by tests before surgery.
❒ Mastoid and middle cranial fossa facial nerve de-compression. This procedure is a combination of the previously described surgeries.
RISKS AND COMPLICATIONS OF FACIAL NERVE SURGERY
Hearing LossAll patients notice some hearing impairment in the operated ear immediately following surgery. This is due to swelling and fluid collection in the mastoid and middle ear. This swelling usually subsides within 2 to 4 weeks and the hearing returns to its preopera-tive level. In an occasional case scar tissue forms and results in a permanent hearing impairment. It is rare to develop a severe impairment.
DizzinessDizziness is common following surgery due to swell-ing of the inner ear structures. Some unsteadiness may persist for a few days postoperatively. On rare occasions dizziness is prolonged.
34015-56111-110 BOOK Facial Nerve Problems.indd 9 2/13/18 10:09 AM

10
Related to Middle Fossa ApproachThe middle fossa approach to the facial nerve, nec-essary in some cases, is a more serious operation. Hearing and balance disturbances are more likely following this surgery. Permanent impairment is, nonetheless, uncommon.
A hematoma (collection of blood under the skin incision) develops in a small percentage of cases, prolonging hospitalization and healing. Reoperation to remove the clot may be necessary if this compli-cation occurs.
A cerebrospinal fluid leak (leak of fluids surrounding the brain) – develops in an occasional case. Reoperation may be necessary to stop the leak.
Infection is a rare occurrence following facial nerve surgery. Should an infection develop after a middle fossa it could lead to meningitis, an infection in the fluid surrounding the brain. Fortunately, this compli-cation is very rare.
Temporary paralysis of half of the body has occurred following middle fossa operation, due to brain swelling. This complication is extremely rare.
Related to AnesthesiaOperations on the facial nerve usually are performed under general anesthesia. There are risks involved with any anesthesia and you should discuss this with the anesthesiologist.
INJURIES OF THE FACIAL NERVE
A common cause of facial nerve injury is a skull fracture. This injury may occur immediately or may develop some days later due to nerve swelling. Injury to the facial nerve may occur in the course of operations on the ear. This complication, fortunately, is very uncommon. It may occur, however, when
34015-56111-110 BOOK Facial Nerve Problems.indd 10 2/13/18 10:09 AM

11
the nerve is not in its normal anatomical position (congenital abnormality) or when the nerve is so distorted by the mastoid or middle ear disease that is not identifiable. In rare cases it may be necessary to remove a portion of the nerve in order to eradicate the disease.
Treatment Treatment of an injured facial nerve may be medi-cal or surgical, depending on the extent of the nerve damage.
Medical TreatmentMedical treatment is the same as described for Bell’s palsy.
Surgical Treatment¨ Mastoid Decompression of the facial nerve. (Refer to page 8.) ¨ Middle fossa facial nerve decompression (Refer to page 9.) ¨ Facial nerve graft A facial nerve graft is necessary at times if facial nerve damage is extensive. A skin sensa-tion nerve is removed from the neck and transplanted into the ear bone to replace the diseased portion of the facial nerve. Total paralysis will be present until the nerve re-grows through the graft. This usually takes 6 to 15 months. Some facial weakness may be permanent.
TUMORS Acoustic Tumors The most common tumor to involve the facial nerve is a nonmalignant fibroid tumor of the hearing and balance nerve, the acoustic tumor. Although there is rarely any weakness of the face before surgery, tumor removal sometimes results in weakness or paralysis. This weakness usually subsides in several months without treatment, occasionally it will be permanent.
34015-56111-110 BOOK Facial Nerve Problems.indd 11 2/13/18 10:09 AM

12
It may may be necessary to remove a portion of the facial nerve in order to remove the acoustic tumor. Rarely, it may be possible to sew the nerve ends to-gether at the time of surgery or to insert a nerve graft. At times a nerve anastomosis procedure is necessary later, connecting a tongue nerve to the facial nerve (hypoglossal facial anastomosis page 13 ). In either case the face is totally paralyzed until the nerve re-grows which takes from (6 to 15 months).
Facial Nerve NeuromaA nonmalignant fibroid growth may grow in the facial nerve itself. This tumor may or may not produce a gradually progressive facial nerve paraly-sis. Removal of this facial nerve neuroma requires removing that portion of the facial nerve invaded by the tumor. Usually it is possible to graft it at the time with a skin sensation nerve from the neck. Total paralysis will last until the nerve regrows through the graft, usually requiring a period of 6 to 15 months. There will be some permanent facial weakness.
When the portion of the facial nerve nearest the brain is destroyed by the tumor, a facial reanimation procedure may be necessary (see below).
Removal of a facial nerve neuroma may necessi-tate removal of the inner ear structure. If this were necessary, it would result in a total loss of hearing in the operated ear and temporary severe dizziness. Persistent unsteadiness is uncommon.
FACIAL REANIMATION There are a number of surgical procedures that are helpful with facial paralysis. In some cases, repairing or decompressing an injured nerve is an important consideration. There are variety of other procedures that may be helpful to prevent drying or injury of the eye and assist in improving symmetry or even movement of the face although none of these procedures can create a perfectly normal appearance of the face.
34015-56111-110 BOOK Facial Nerve Problems.indd 12 2/13/18 10:09 AM

13
Eyelid SurgeryImplantation of gold into the upper eyelid can be helpful in counter balancing the lifting eyelid muscle. This helps to prevent dryness and irritation of the eye and helps to improve the appearance. Shortening of the lower lid or corners of the eyelid are sometimes performed at the same operation. Complications of these procedures are rare and may include bleeding, infection, droopy eyelid, extrusion of the implant and visual loss.
Hypoglossal-Facial Nerve AnastomosisConnecting a portion or all of the tongue nerve to the facial nerve may provide good tone to the face. Facial movements can also be obtained by attempt-ing to move the tongue to the involved side when a smile is desired. Some degree of tongue weakness is expected which may affect speech or swallowing.
Temporalis Muscle TranspositionTransferring one of the jaw muscles to the corner of the mouth can provide improvement of facial sym-metry. Smiling is relearned by attempting to bite at the same time. Unlike hypoglossal-facial anastomo-sis, no tongue weakness is expected and chewing problems are rare. The surgeon always attempts to over correct the pull at the corner of the mouth. This over-correction and the significant face swelling usu-ally resolve in 4-6 weeks. Rarely a very thick muscle may result in a bulge.
While facial reanimation surgery cannot provide a return to normal facial function, the improvement in eye protection and appearance is usually gratifying. Not infrequently, secondary procedures or revisions may be required to obtain the best results or modify results because of the passage of time.
34015-56111-110 BOOK Facial Nerve Problems.indd 13 2/13/18 10:09 AM

14
MiscellaneousThere are a variety of other operations that are some-times performed by themselves or in combination with the above procedures. Such procedures may include a face lift or removal of excess skin at the brow or cheek. For patients who have some faulty return of facial function, selective cutting of facial nerve branches or facial muscles may be of benefit and are sometimes combined with other procedures to correct some of the anticipated weakness.
OTHER FACIAL NERVE DISORDERS
Facial SpasmSurgery to correct this problem may involve 1) inten-tional weakening of the nerve through an incision on the face which may also require a gold weight eyelid implant, or 2) relieving pressure on the nerve adjacent to the brain. This operation includes risks of facial paralysis, hearing loss, dizziness, spinal fluid leak and stroke. 3) An injection of Botox can give temporary relief. As always, you should discuss your proposed surgery in detail with your doctor.
Mastoid InfectionAcute or chronic middle ear infections occasion-ally cause a weakness of the face due to swelling or direct pressure on the nerve. In acute infections the weakness usually subsides as the infection is con-trolled and the swelling around the nerve subsides.
Facial nerve weakness occurring in chronically infected ears is usually due to pressure from a cholesteatoma (skin-lined cyst). Mastoid surgery is performed to eradicate the infection and relieve nerve pressure. Some permanent facial weakness may remain.
34015-56111-110 BOOK Facial Nerve Problems.indd 14 2/13/18 10:09 AM

15
Postoperative Facial Nerve WeaknessDelayed weakness or paralysis of the face following reconstructive middle ear surgery (myringoplasty, tympanoplasty, stapedectomy) is uncommon, but oc-curs at times due to swelling of the nerve during the healing period.
Fortunately this type of facial nerve weakness usually subsides spontaneously in several weeks and rarely requires further surgery.
Hemifacial SpasmHemifacial spasm is an uncommon disease of unknown cause which results in spasmodic contrac-tions of one side of the face. Extensive investigation is necessary at times to establish the diagnosis cor-rectly. In some cases, a hemifacial spasm is caused by irritation of the facial nerve near the brain. Exami-nation of the nerve and correction of the irritation, if present, is possible by the retrolabryrinthine or retrosigmoid surgical approach. Facial nerve decom-pression (see Bell’s palsy) may be beneficial.
In this operation the area between the brain and the inner ear is exposed by removing the mastoid bone behind the inner ear. The complications related to this surgery are the same as those for the middle fossa approach (Pages 9 and 10) .
Brain DiseaseTumors and circulatory disturbances of the nervous system may cause facial nerve paralysis. The most common example of this is a stroke.
As opposed to other conditions listed in this book-let, in brain diseases there are usually many other symptoms which indicate the cause of the problem. Treatment is managed by the internist, neurologist or neurosurgeon.
34015-56111-110 BOOK Facial Nerve Problems.indd 15 2/13/18 10:09 AM

16
GENERAL COMMENTS
During the period of recovery of facial function, exercises may be recommended. Exercising the muscles by wrinkling the forehead, closing the eyes tightly and smiling forcefully may be beneficial.
Electrical stimulation of the facial muscles may be of some benefit.
As recovery of facial nerve function begins exercises may be recommended by your otologist.
Excerpt from materials prepared by the Otologic Medical Group Inc., Los Angeles, CA.
34015-56111-110 BOOK Facial Nerve Problems.indd 16 2/13/18 10:09 AM
17
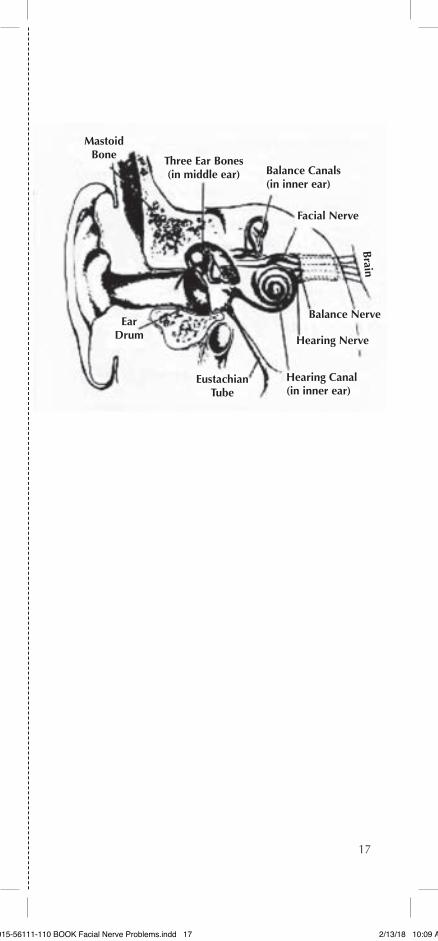
Mastoid Bone Three Ear Bones
(in middle ear) Balance Canals (in inner ear)
Facial Nerve
Balance Nerve
Hearing Nerve
Hearing Canal (in inner ear)
Eustachian Tube
Ear Drum
Brain
34015-56111-110 BOOK Facial Nerve Problems.indd 17 2/13/18 10:09 AM

19
Mic
higa
n Ea
r In
stitu
te
Received by
Patient Signature
Date
Facial Nerve Problems
34015-56111-110 BOOK Facial Nerve Problems.indd 19 2/13/18 10:09 AM

22
For more information on the services and staff of the Michigan Ear Institute, call us at (248) 865-4444 or visit our web site at www.michiganear.com
Michigan Ear InstituteProvidence Medical Building30055 Northwestern Highway #101Farmington Hills, MI 48334 (248) 865-4444 phone (248) 865-6161 fax
34015-56111-110 REV 2/7/18
NOTICE
St. John Providence complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex.
ATTENTION: If you speak a language other than English, language assistance services, free of charge, are available to you. Call 1-586-753-1888 (TTY: 1-313-343-3126).
ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística. Llame al 1-586-753-1888 (TTY: 1-313-343-3126).
(رقم ھاتف 1888-753-586-1كنت تتحدث اذكر اللغة، فإن خدمات المساعدة اللغویة تتوافر لك بالمجان. اتصل برقم ملحوظة: إذا ).3126-343-313-1الصم والبكم:
34015-56111-110 BOOK Facial Nerve Problems.indd 22 2/13/18 10:09 AM







