LA STORY STEMI 2011
Bill Koenig, MDMedical DirectorLos Angeles County EMS Agency

Establishing a Communitywide System of Care
Designated emergency cardiac care centers
Triage to PCI centers
Data driven quality improvement program
Moyer P. Crit Pathways Cardiol 2004;3:53-61
Boston EMS STEMI
Primary Percutaneous Coronary Intervention (PCI) is one of the most complex, multi-disciplinary, and time-sensitive therapeutic intervention medicine. Our process is measured in Minutes Our outcomes are measured in terms of
Mortality Teamwork and smooth Transitions are
essential
PCI for STEMI
October 30,2010
0930Exercising, CP 0935911 Dispatch 0941ALS Arrives
.October 2006: Chest PainDestination: MAR
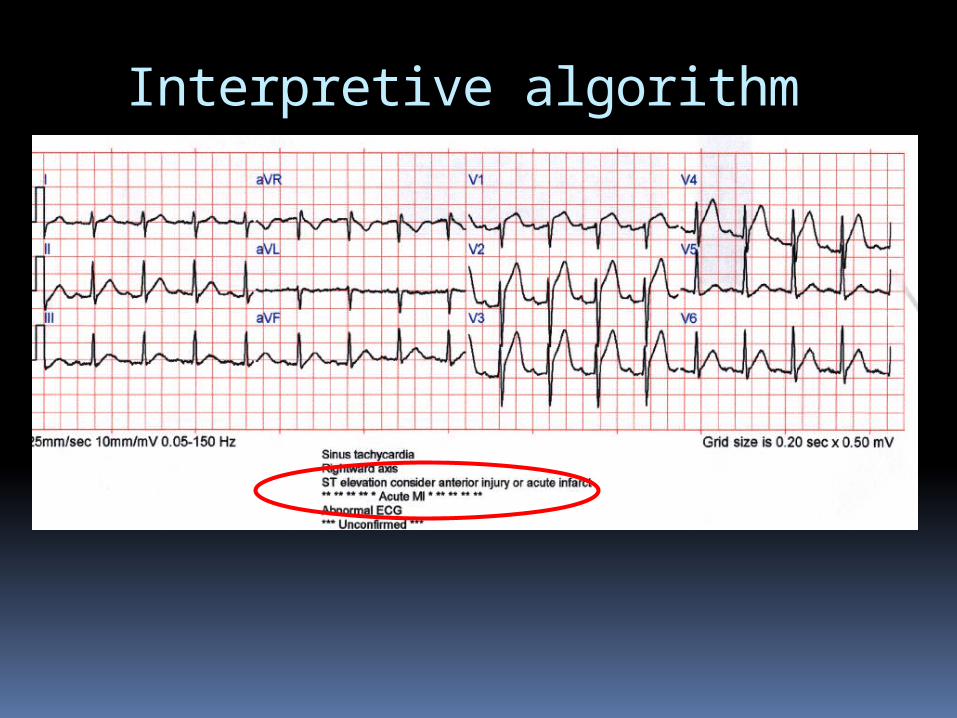
Interpretive algorithm
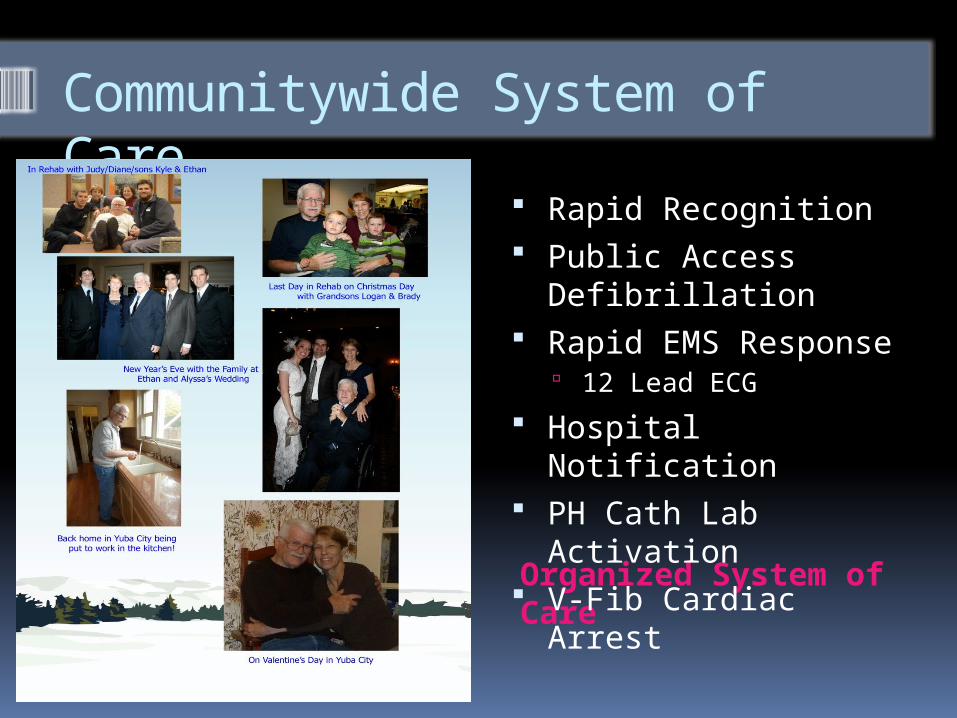
Communitywide System of Care
Organized System of Care
Rapid Recognition Public Access
Defibrillation Rapid EMS Response
12 Lead ECG
Hospital Notification PH Cath Lab
Activation V-Fib Cardiac Arrest

Unique aspects of System
“If you have seen one EMS system…..
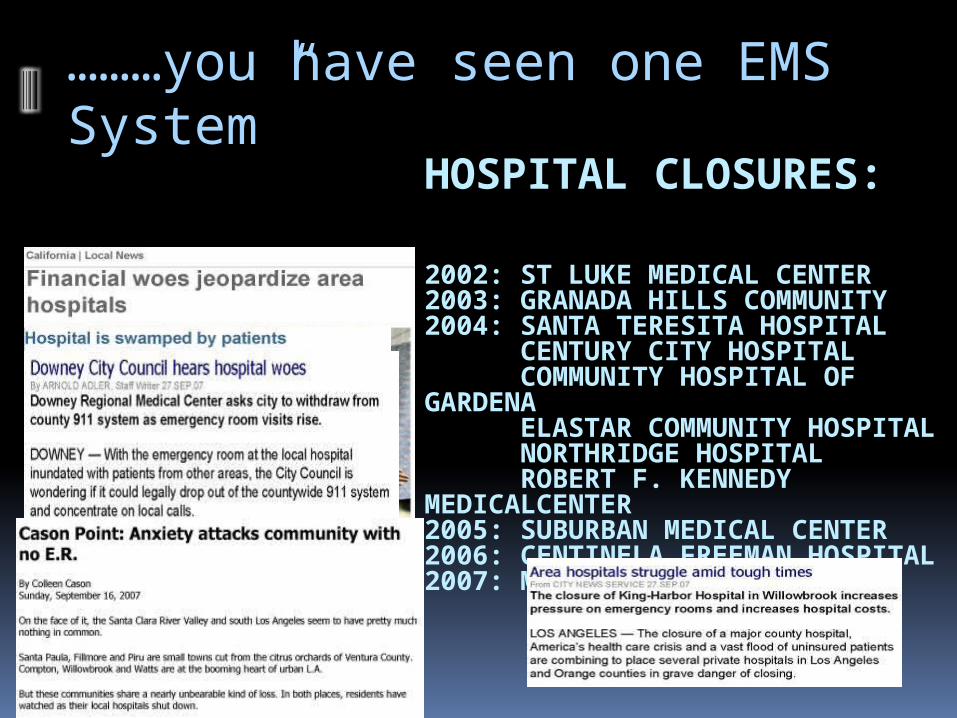
HOSPITAL CLOSURES:
2002: ST LUKE MEDICAL CENTER2003: GRANADA HILLS COMMUNITY 2004: SANTA TERESITA HOSPITAL CENTURY CITY HOSPITAL COMMUNITY HOSPITAL OF GARDENA ELASTAR COMMUNITY HOSPITAL NORTHRIDGE HOSPITAL ROBERT F. KENNEDY MEDICALCENTER2005: SUBURBAN MEDICAL CENTER2006: CENTINELA FREEMAN HOSPITAL2007: MARTIN LUTHER KING JR
………you have seen one EMS System”
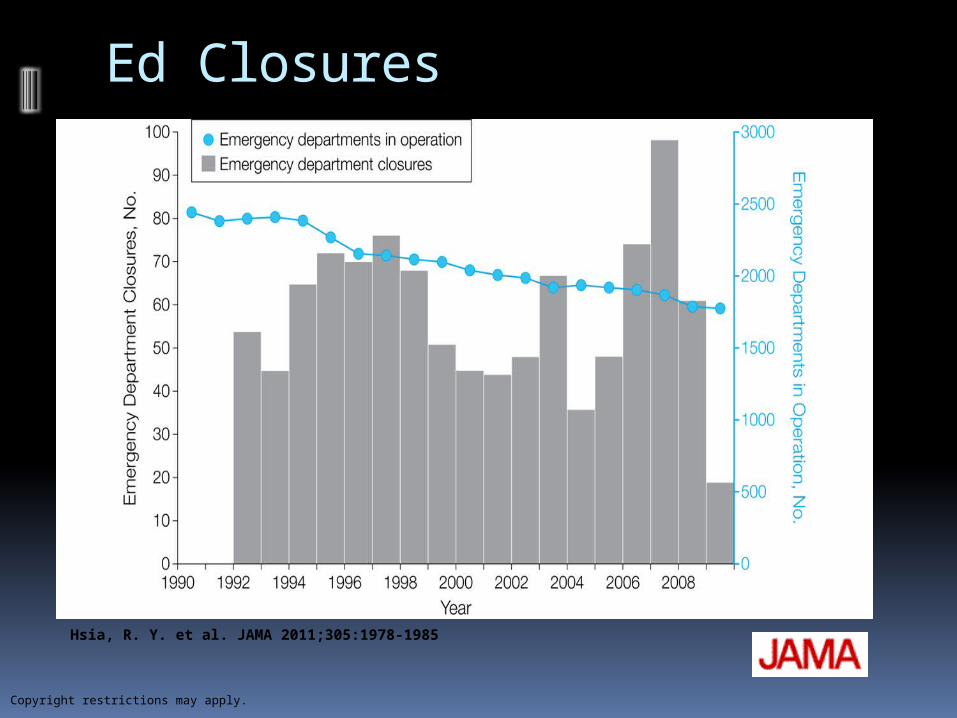
Figure 1. Trends in Emergency Department Operation and Closures in Urban Areas, 1990-2009
Hsia, R. Y. et al. JAMA 2011;305:1978-1985
Copyright restrictions may apply.
Ed Closures

L.A. Fire Department cuts some rescue vehicles, paramedic supervisorsFacing a $56.5-million budget gap, the department will take 15 fire trucks and six ambulances out of service each day…………
The LA Dilemma: Your Money or Your Life -- What to Cut, Who Will Pay?
911 STEMI Focus Data Base includes all pre-hospital
patients taken to an SRC – regardless of whether cath lab is activated or undergoes PCI
Data Collection is Stemi focused
Los Angeles STEMI system: Inclusion criteria into our data base
is all patients transported by 911 to an SRC as a STEMI patient, including those that never encounter a Cardiologist or the cath lab.
Regulatory Framework Standards and Requirements that are County Based
Hospitals participate in other data bases
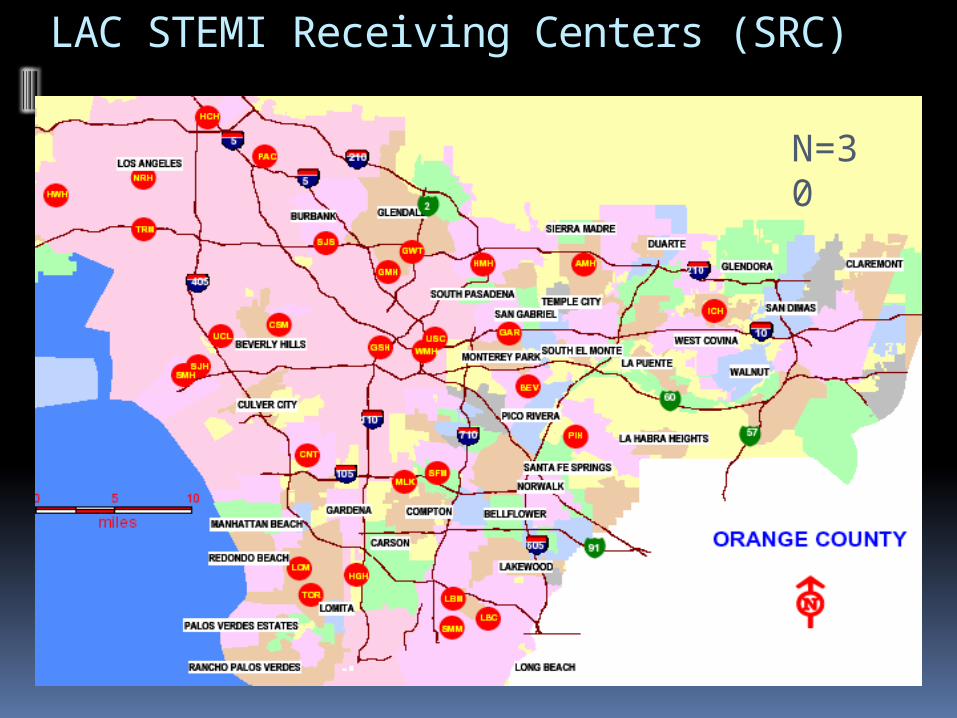
LAC STEMI Receiving Centers (SRC)
N=30
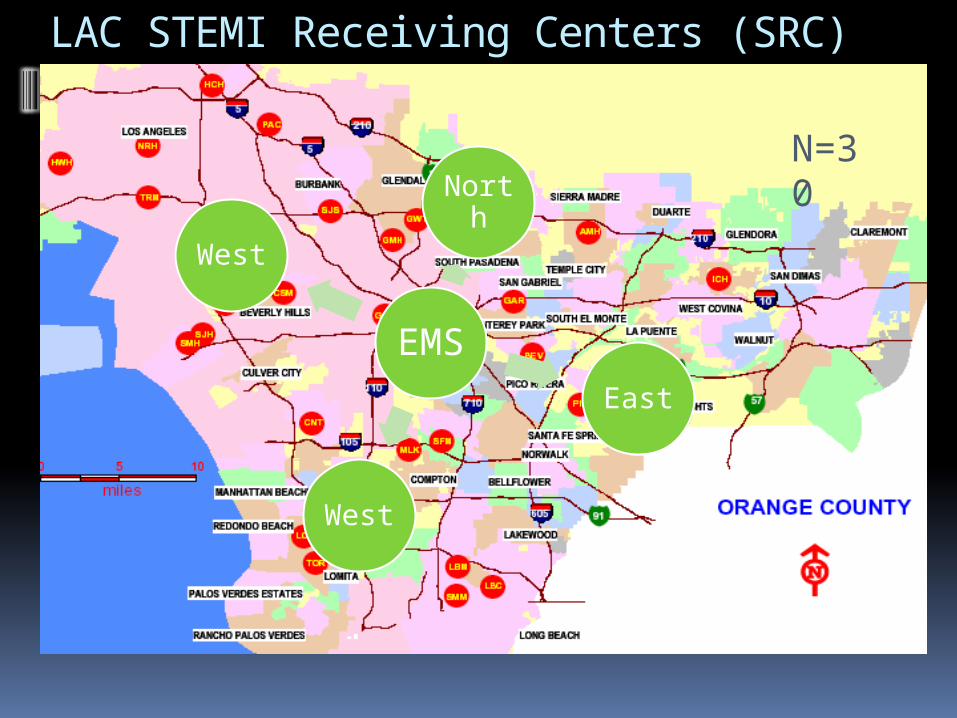
LAC STEMI Receiving Centers (SRC)
N=30
EMS
North
East
West
West
Tipping Points
Medical Literature Community Leaders - AHA
Conceptual framework presented to system participants
Funding AHA and Annenberg Foundation Los Angeles County Board of Supervisors
EMS Agency Reviews
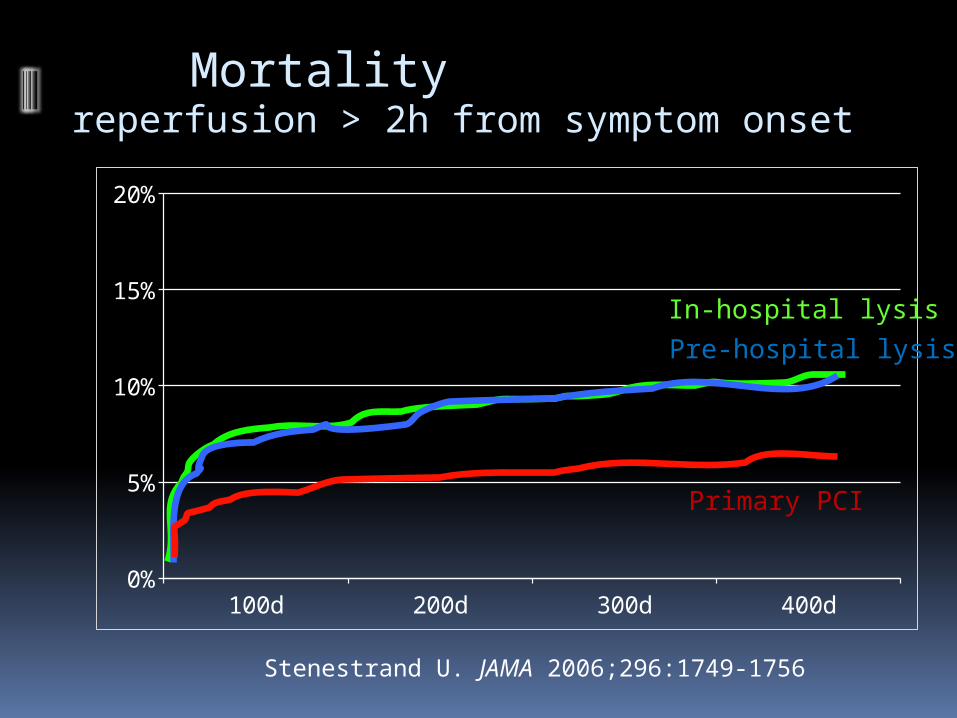
Stenestrand U. JAMA 2006;296:1749-1756
Mortality reperfusion > 2h from symptom onset
100d 200d 300d 400d0%
5%
10%
15%
20%
In-hospital lysis
Pre-hospital lysis
Primary PCI
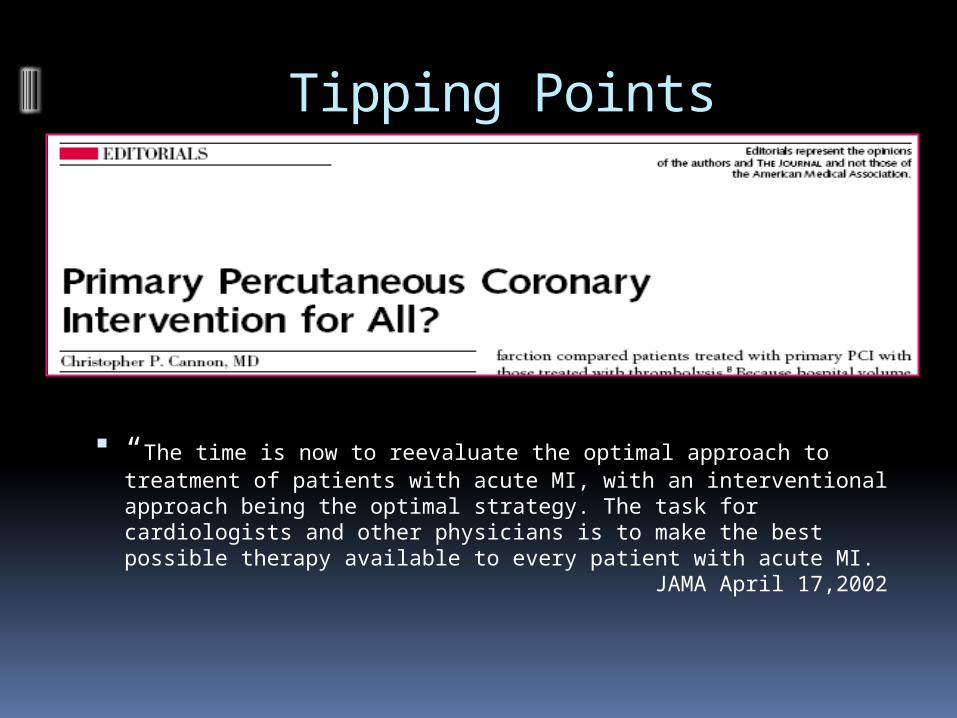
“The time is now to reevaluate the optimal approach to treatment of patients with acute MI, with an interventional approach being the optimal strategy. The task for cardiologists and other physicians is to make the best possible therapy available to every patient with acute MI. JAMA April 17,2002
Tipping Points
Medical Literature
Cannon “Primary PCI for all” (2002 JAMA 287:1987)
Topol “Regionalizaton--a call forSpecialized centers” (2003 Circulation 107:1463)
Williams “Treatment delayed is treatment denied” (2004 Circulation 109:1806)
Henry & Larson “Triage to heart attack centers…is it time for a national policy?”
(2005 JACC)
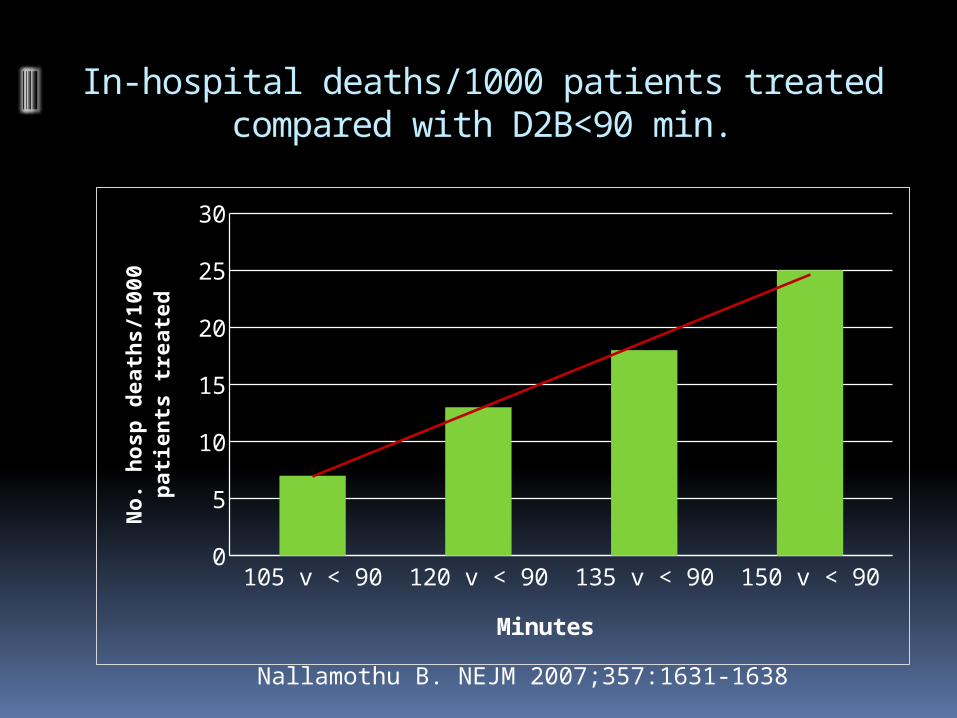
In-hospital deaths/1000 patients treated compared with D2B<90 min.
105 v < 90 120 v < 90 135 v < 90 150 v < 900
5
10
15
20
25
30
Minutes
No.
hosp
death
s/1
00
0 p
ati
en
ts
treate
d
Nallamothu B. NEJM 2007;357:1631-1638
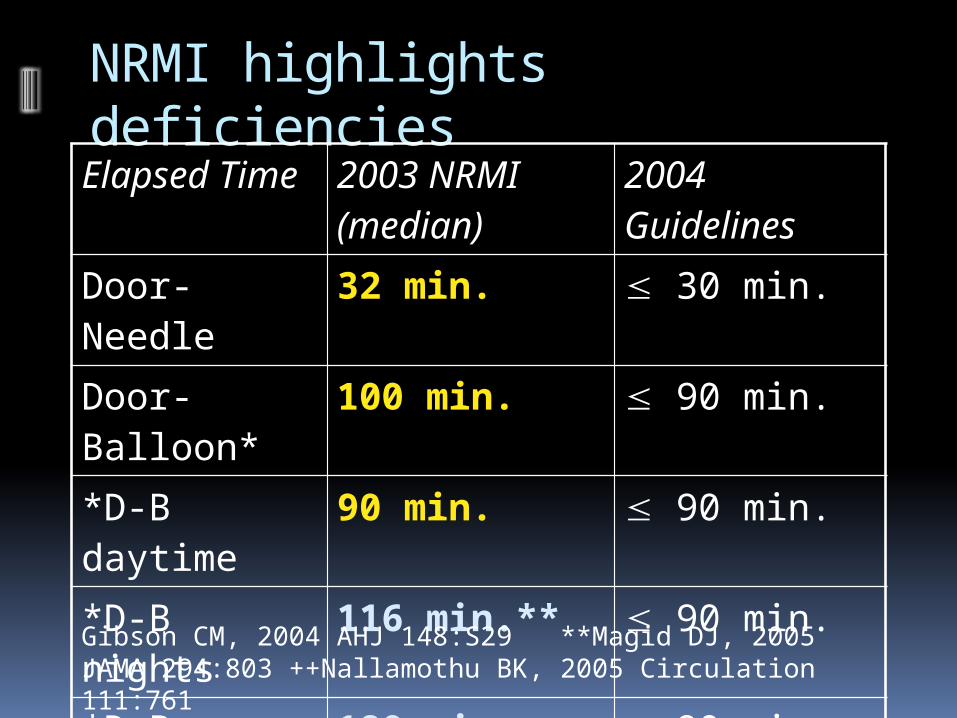
NRMI highlights deficienciesElapsed Time 2003 NRMI
(median)2004 Guidelines
Door-Needle 32 min. 30 min.
Door-Balloon* 100 min. 90 min.
*D-B daytime 90 min. 90 min.
*D-B nights 116 min.** 90 min.
*D-B transfer 180 min.++ 90 min.
Gibson CM, 2004 AHJ 148:S29 **Magid DJ, 2005 JAMA 294:803 ++Nallamothu BK, 2005 Circulation 111:761
Tipping Points
Medical Literature
Circulation June 2007
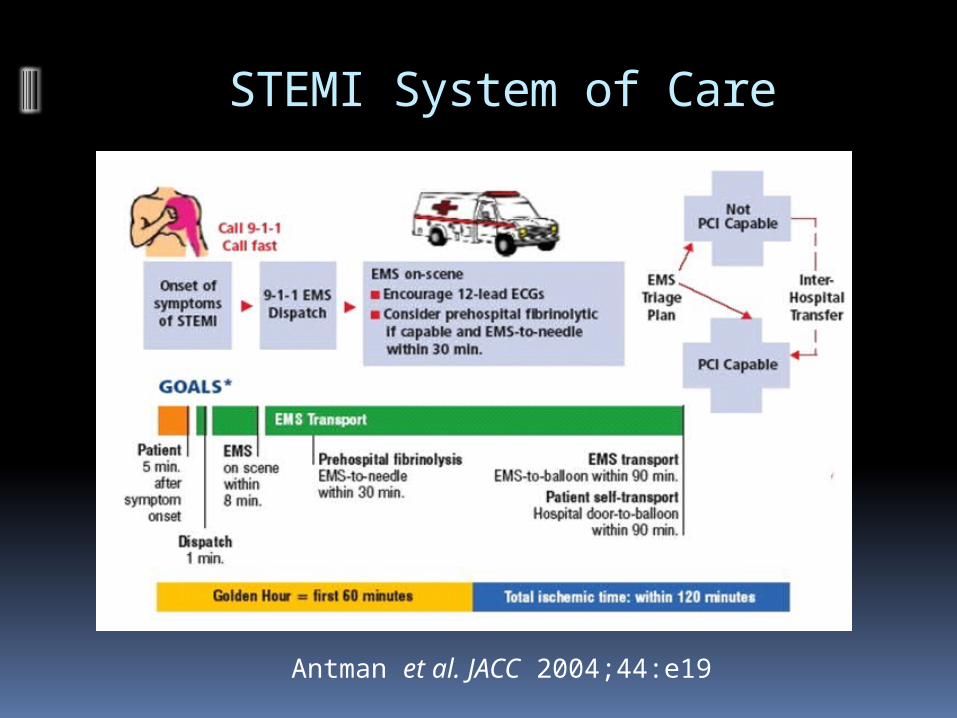
Antman et al. JACC 2004;44:e19
STEMI System of Care
30 >> 30 >> 30 Rule
EMS >> ED >> Cath lab
Tipping Points
Hospital Best Practices Develop

Hospital-Based Strategies Associated with Shorter Door-to-Balloon Time and Potential Tools
to Implement Them
Nallamothu B et al. N Engl J Med 2007;357:1631-1638
Prehospital ECG Activation Expected interval between page and arrival Single Call from ED to Cath Lab Activation
Single Call Panel Physician
Real time Feedback to EMS, ED Fire Department removes rig from service for cath
Cardiologist in hospital 24/7 Senior Management commitment
CEO Required to attend agency reviews
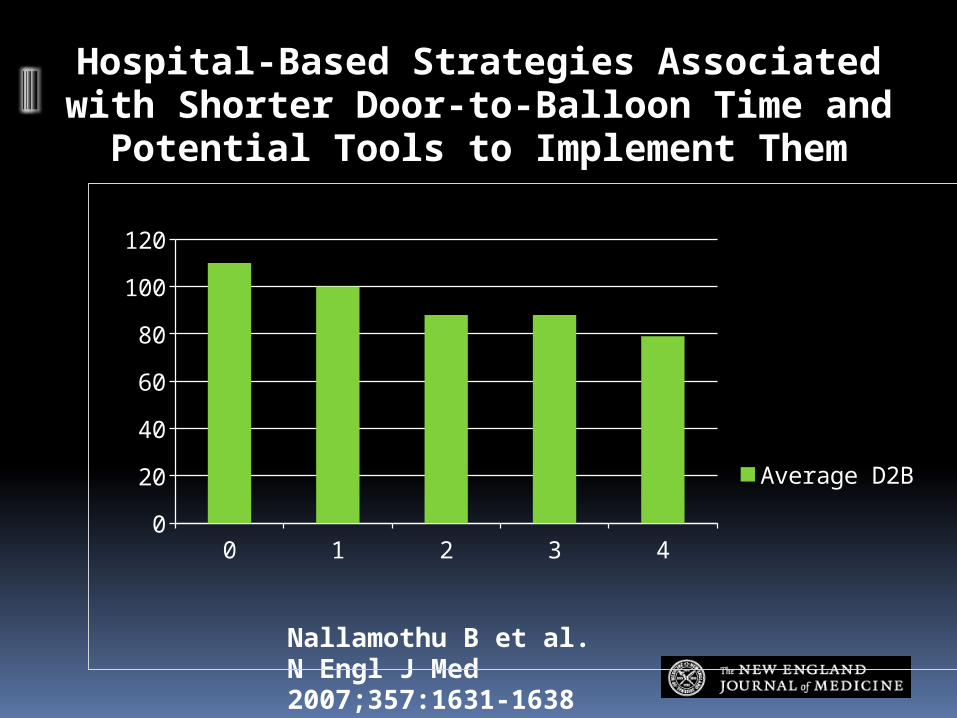
Hospital-Based Strategies Associated with Shorter Door-to-Balloon Time and Potential Tools
to Implement Them
Nallamothu B et al. N Engl J Med 2007;357:1631-1638
0 1 2 3 40
20
40
60
80
100
120
Average D2B
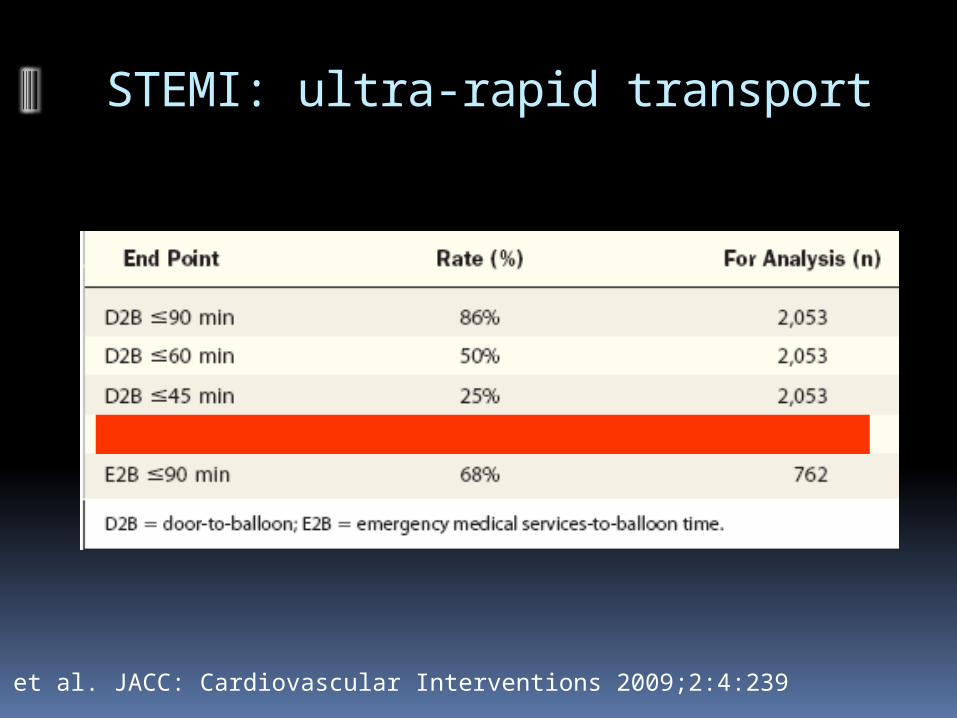
STEMI: ultra-rapid transport
Rokos et al. JACC: Cardiovascular Interventions 2009;2:4:239

Tipping Points Hospitals Systems change
Placeholder Placeholder Placeholder for data from study Placeholder for data from study Placeholder Placeholder
Implementation of 12 lead studied prior to Stemi Center Designation Reduced D2B
Funded by AHA/Annenberg Foundation
Tipping Point: Funding
American Heart Association and Annenberg Foundation – $3 million
Los Angeles County Board of Supervisors Conceptual Framework was important
Retrospect scope :Uniform EquipmentUniform Transmission Interface
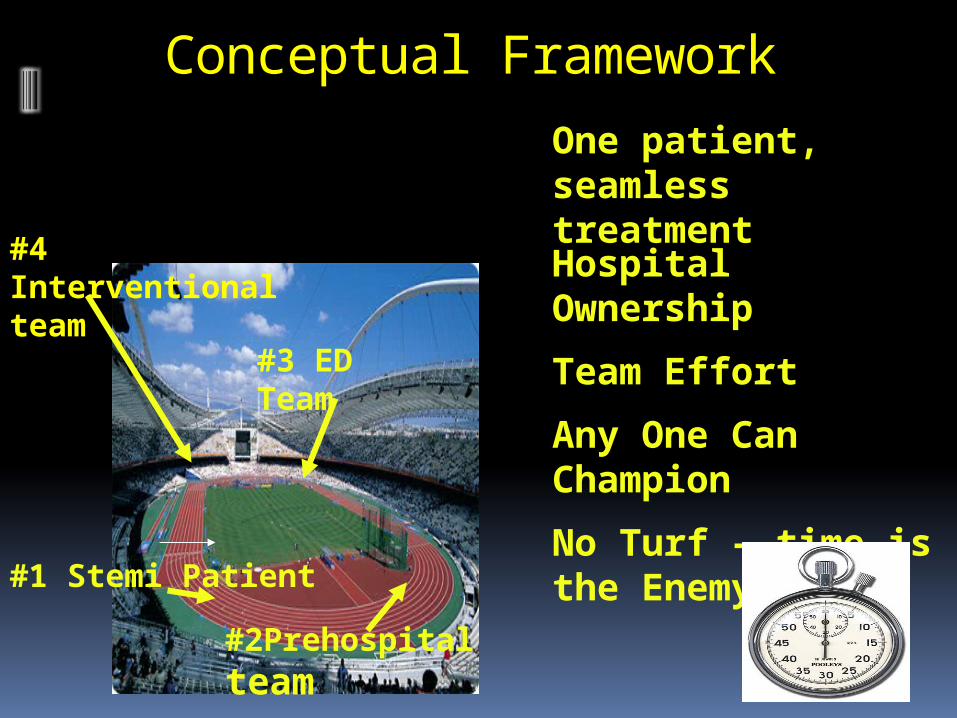
Conceptual Framework
#1 Stemi Patient
#2Prehospital team
#3 ED Team
#4 Interventional team
One patient, seamless treatment
Hospital Ownership
Team Effort
Any One Can Champion
No Turf – time is the Enemy

DATA
Inclusion Criteria
All patients identified as STEMI patients in field and transported to an SRC All Patients Triaged from field – even
when cath lab not activated All 911 inter-facility transfers for
STEMI Independent Base Hospital Data
Base Hospital Bordering LA County
Included

Data Collection Web Based

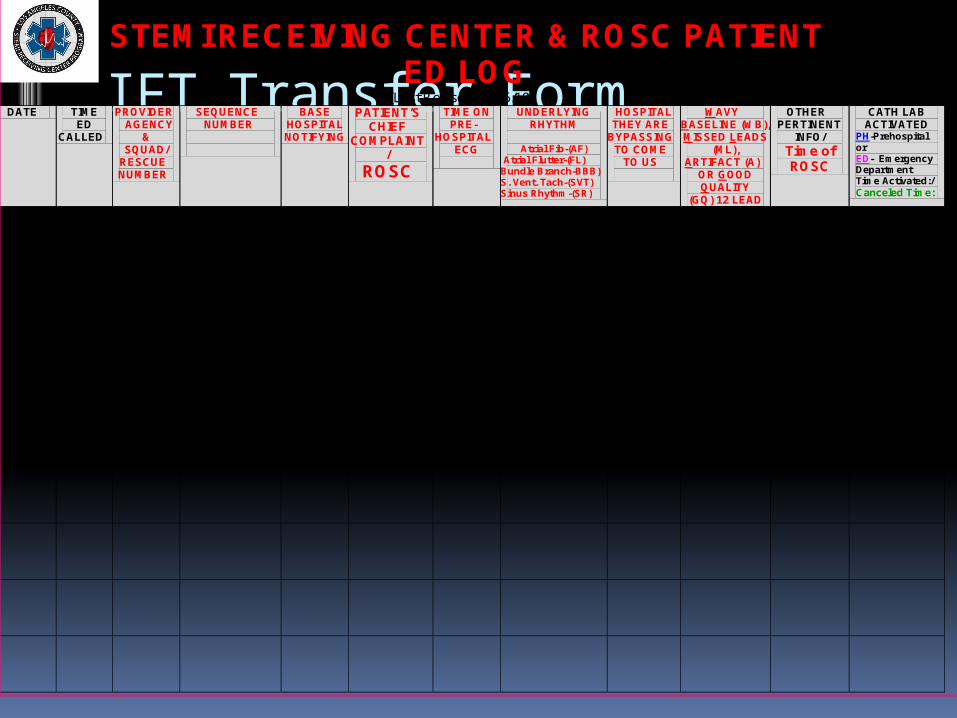
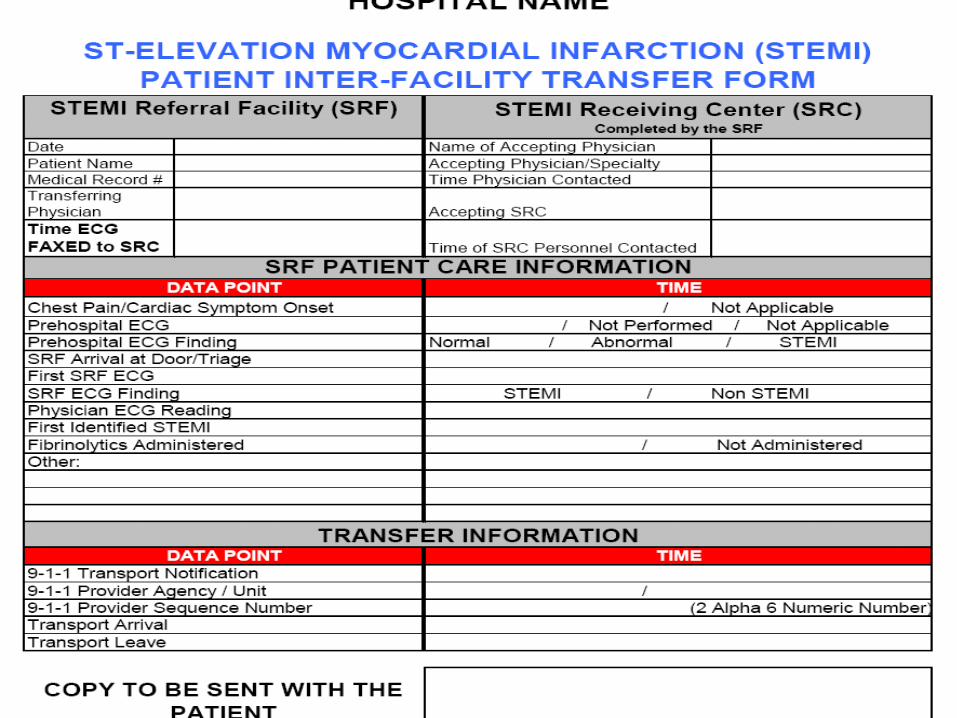
IFT Transfer Form STEMI RECEIVING CENTER & ROSC PATIENT
ED LOG (Last Revised 10/26/10)
DATE TIME ED
CALLED
PROVIDER AGENCY
& SQUAD/
RESCUE NUMBER
SEQUENCE NUMBER
BASE HOSPITAL NOTIFYING
PATIENT’S CHIEF
COMPLAINT/
ROSC
TIME ON PRE-
HOSPITAL ECG
UNDERLYING RHYTHM
Atrial Fib-(AF)
Atrial Flutter-(FL) Bundle Branch-BBB) S. Vent. Tach-(SVT) Sinus Rhythm-(SR)
HOSPITAL THEY ARE
BYPASSING TO COME
TO US
WAVY BASELINE (WB), MISSED LEADS
(ML), ARTIFACT (A)
OR GOOD QUALITY
(GQ) 12 LEAD
OTHER PERTINENT
INFO/ Time of ROSC
CATH LAB ACTIVATED
PH-Prehospital or ED- Emergency Department Time Activated:/ Canceled Time:
1/10/09 (Example)
0900
RB 61
ZZ999999
LCM
Chest Pain
0852
BBB
None
1ST ECG with WB 2nd GQ
Nrsg Hm On vent Altered
ED- 0921/ 0958
1/11/09 (Example)
2034
ES 31
ZZ888888
LCM
Chest Pain ROSC
2027
SR
Gardena
GQ
Previous Stent 1/09 ROSC @ 2040
PH- 2039/ 2103

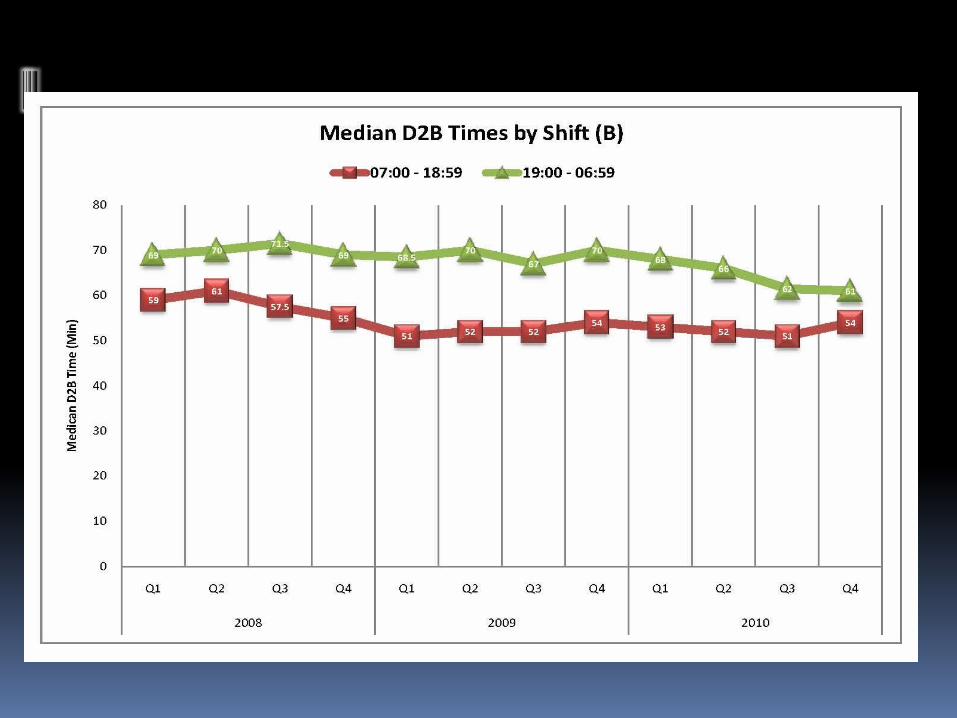
median times
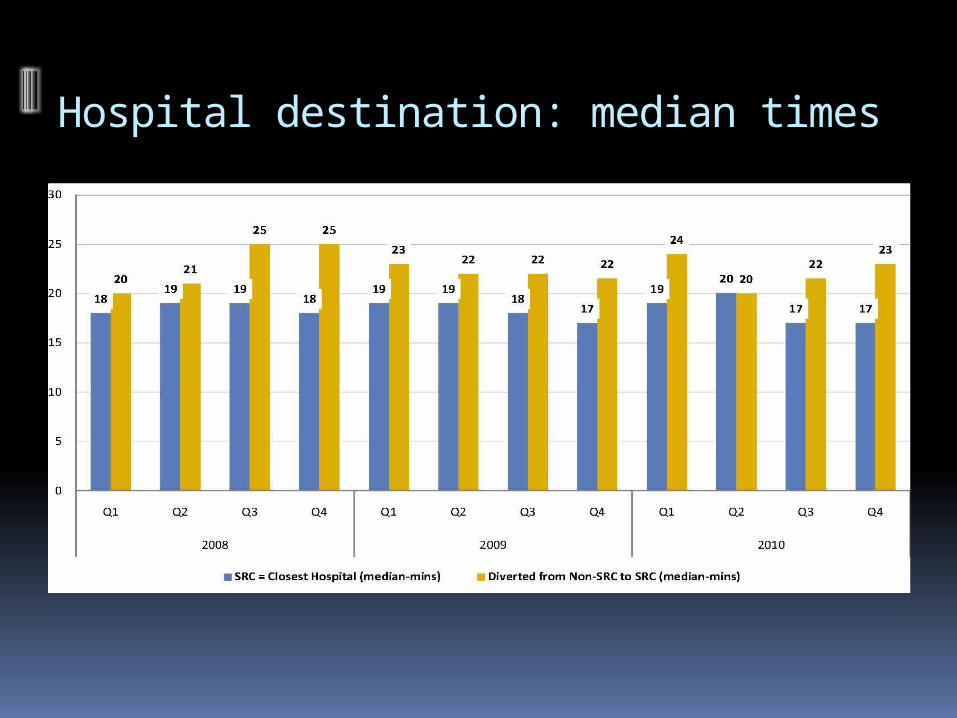
Hospital destination: median times
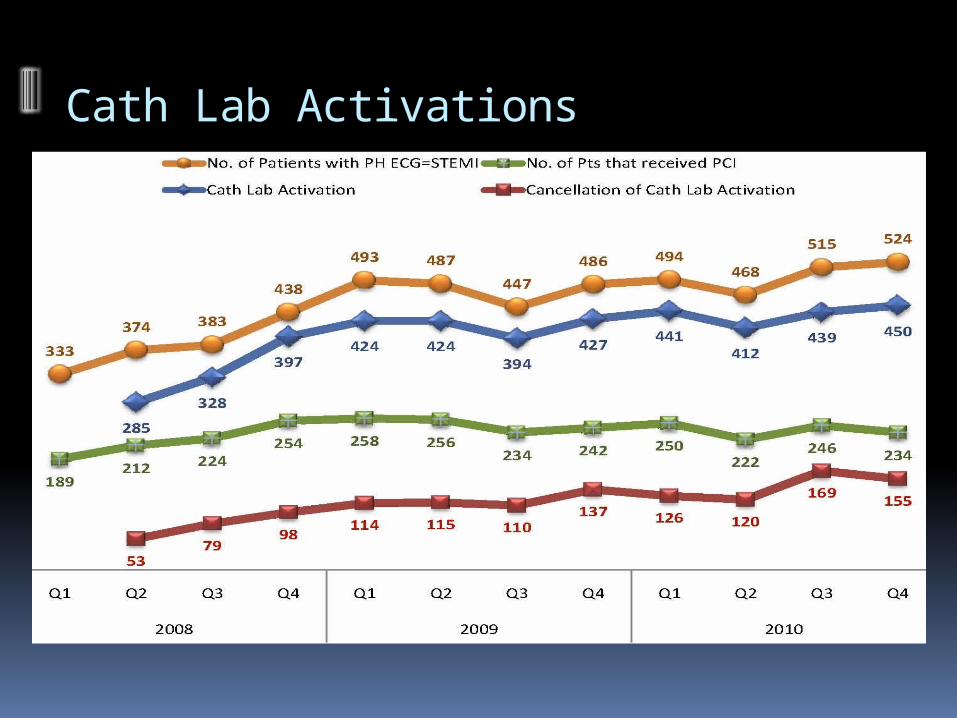
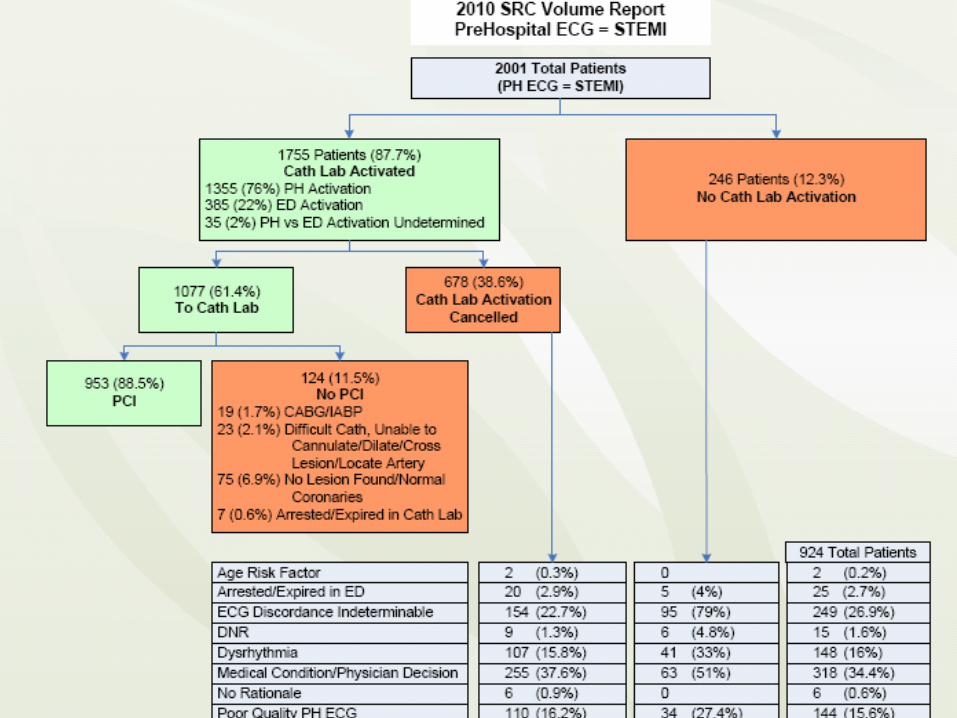
Cath Lab Activations
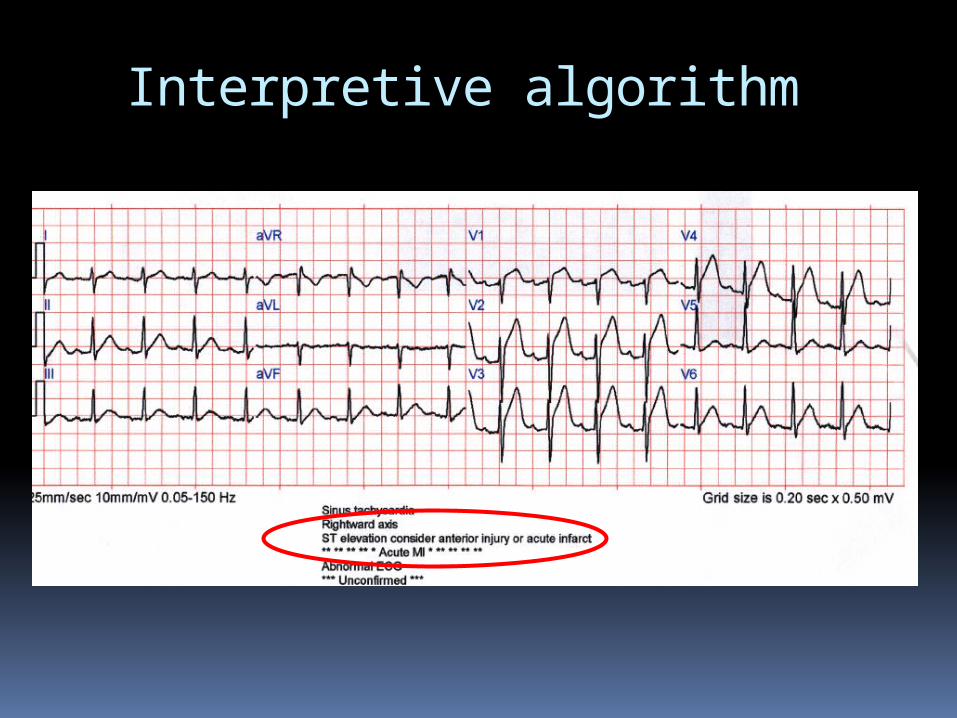
Interpretive algorithm
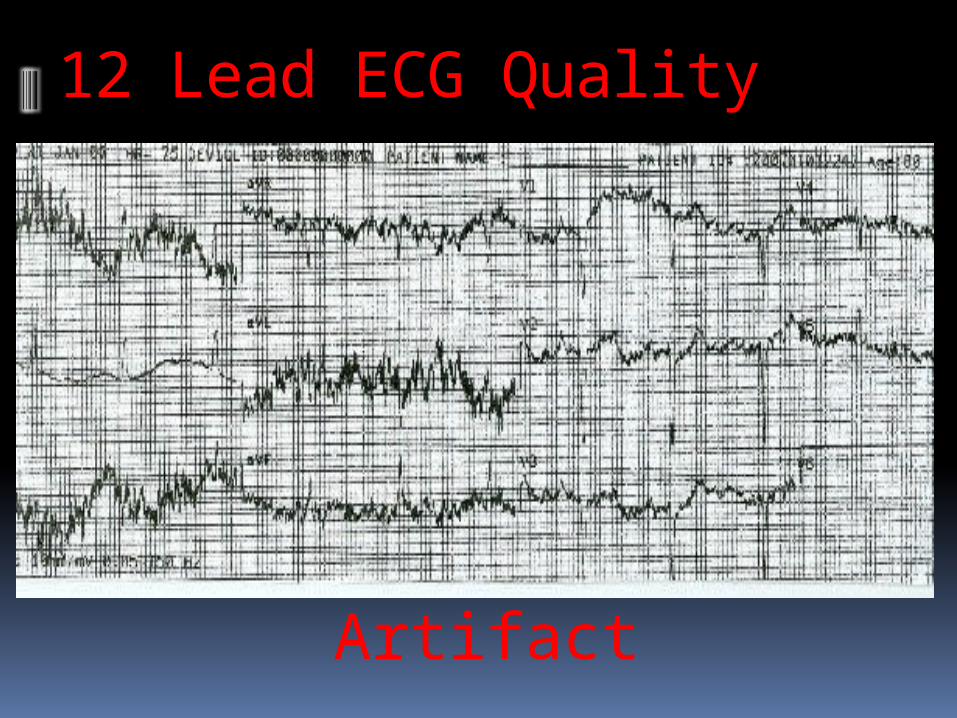
12 Lead ECG Quality
Artifact
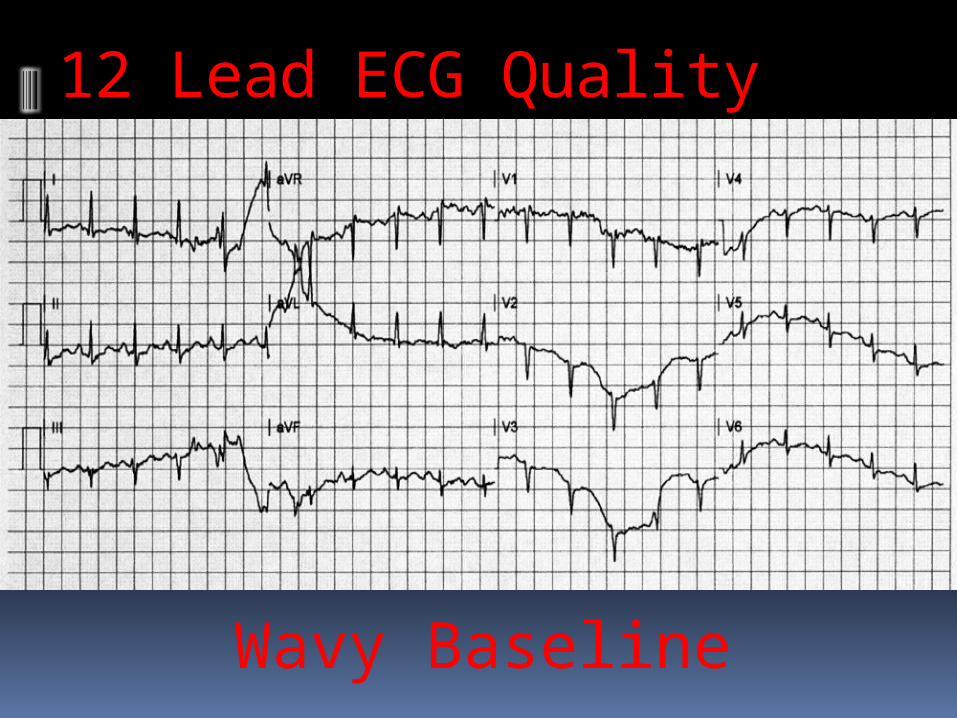
12 Lead ECG Quality
Wavy Baseline
Evolving role of Medical Control when ***AMI*** doesn’t fit
Paced LBBB Atrial
flutter Artifact

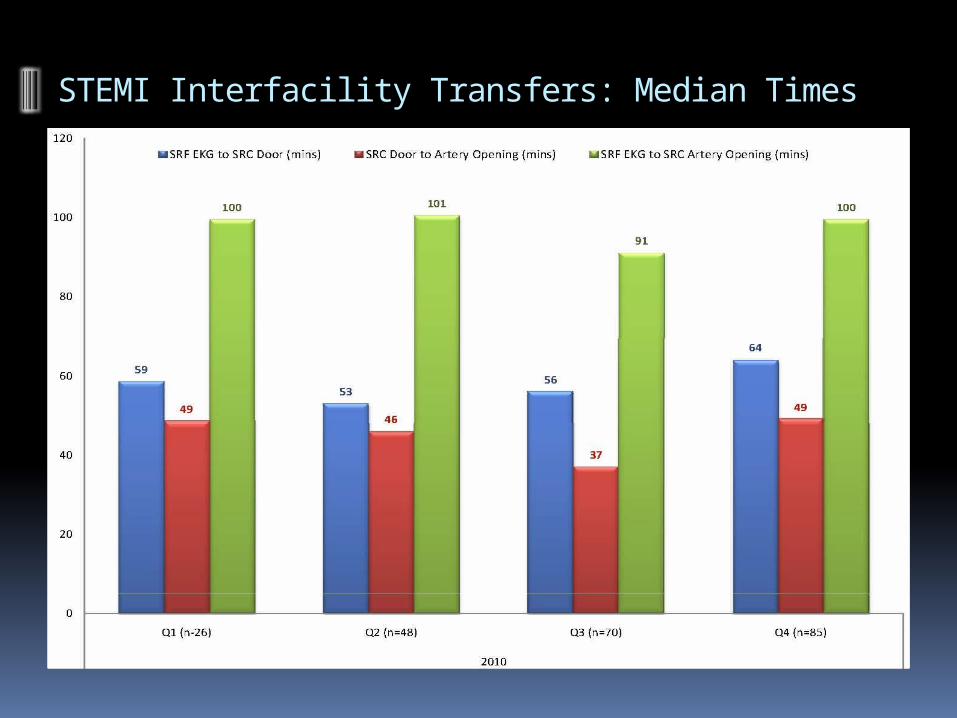
STEMI Interfacility Transfers: Median Times
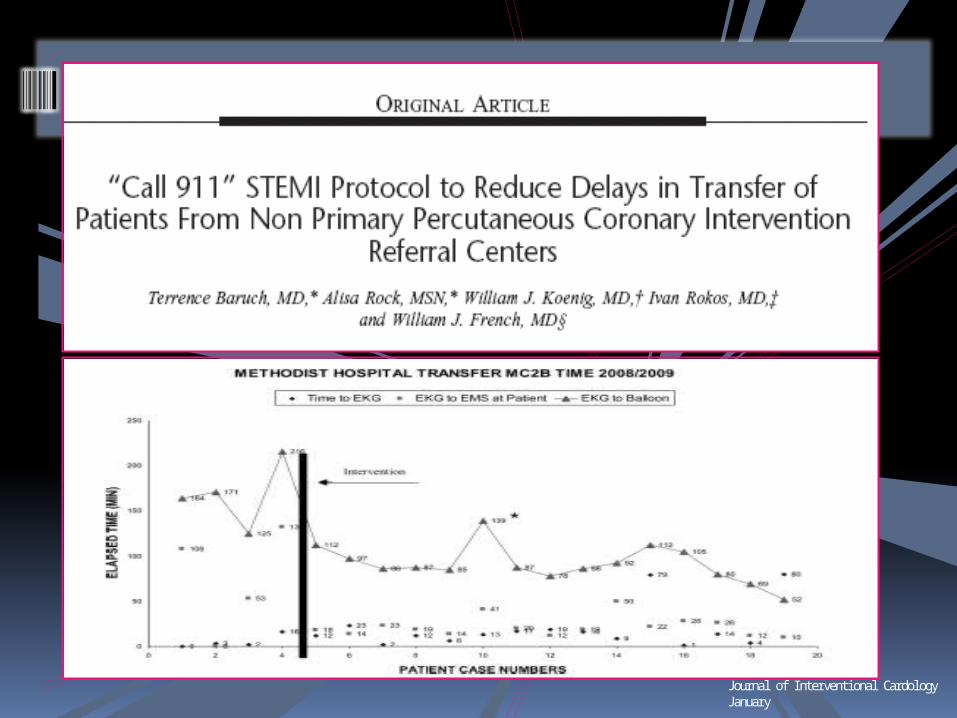
Journal of Interventional CardologyJanuary
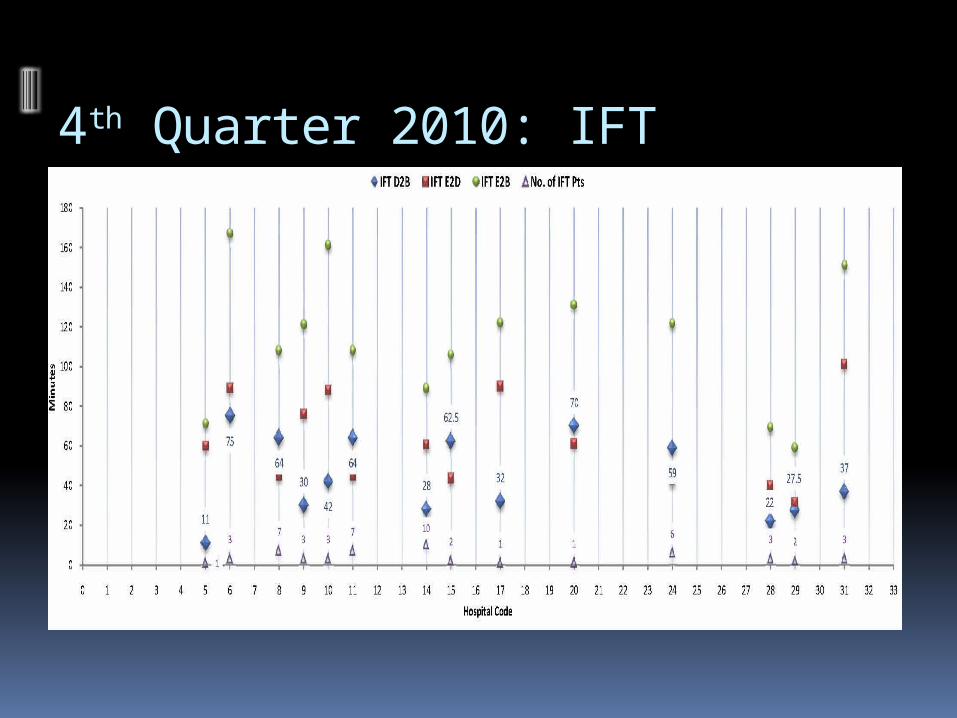
4th Quarter 2010: IFT

JACC CV Interventions, April 2009; 2:339-46
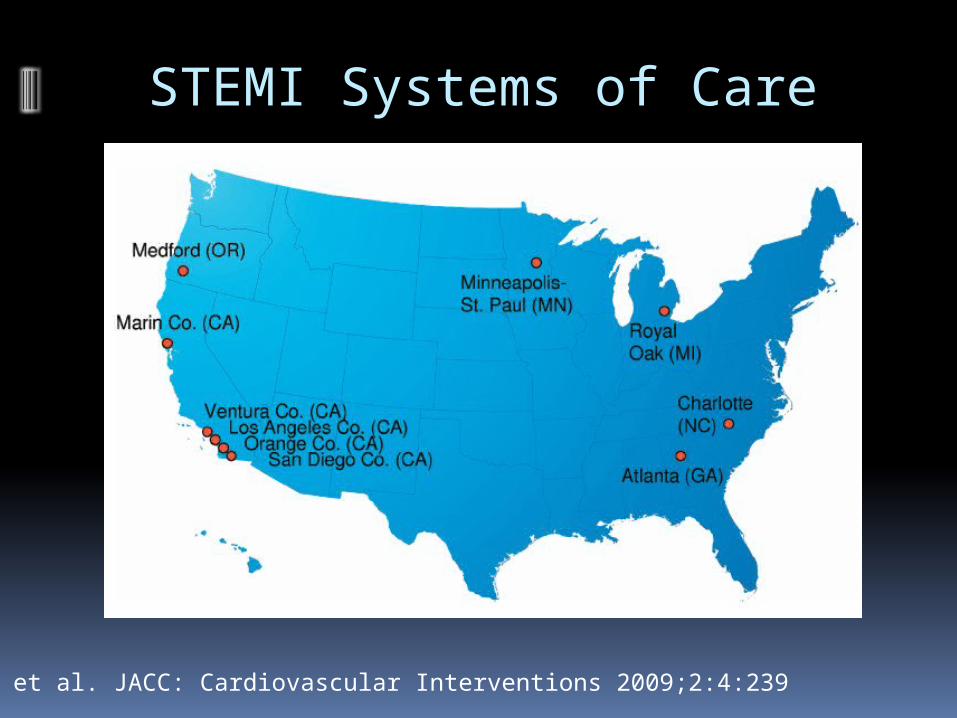
Rokos et al. JACC: Cardiovascular Interventions 2009;2:4:239
STEMI Systems of Care
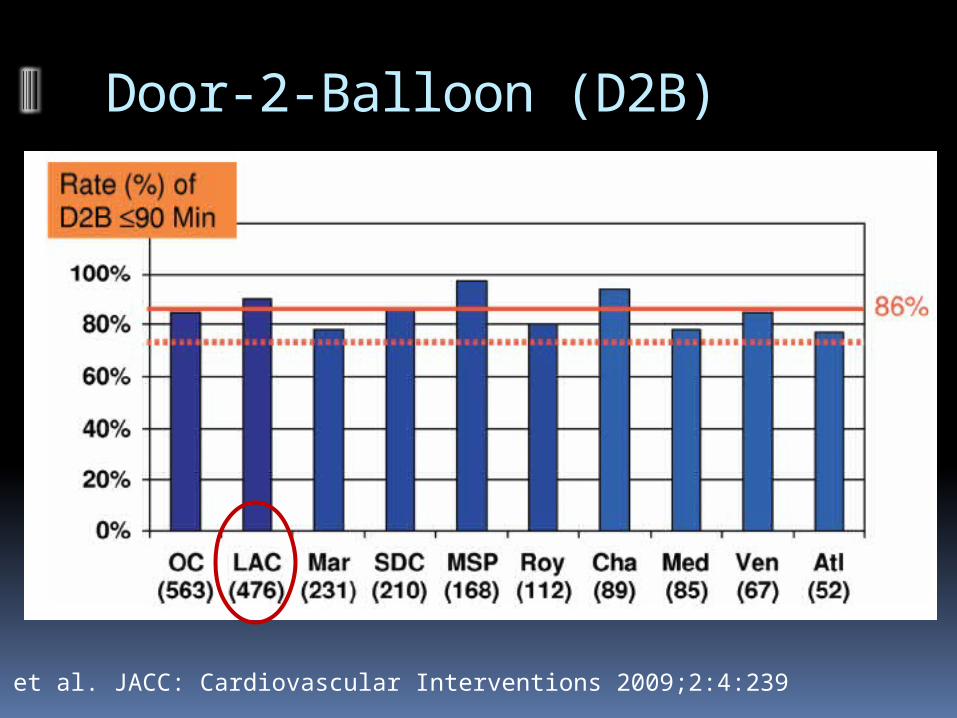
Door-2-Balloon (D2B)
Rokos et al. JACC: Cardiovascular Interventions 2009;2:4:239
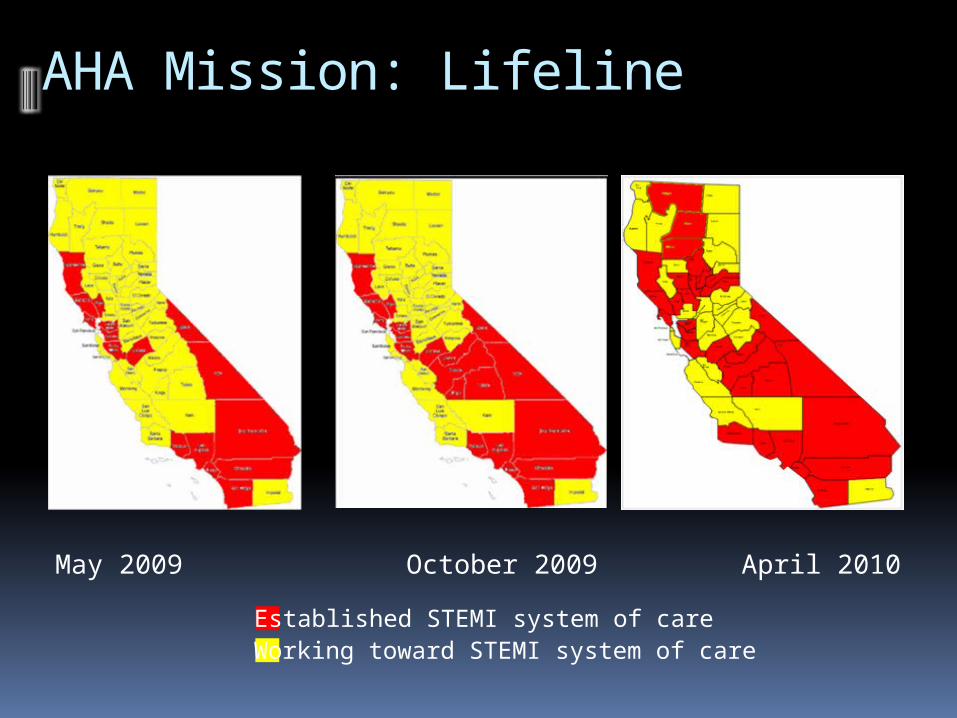
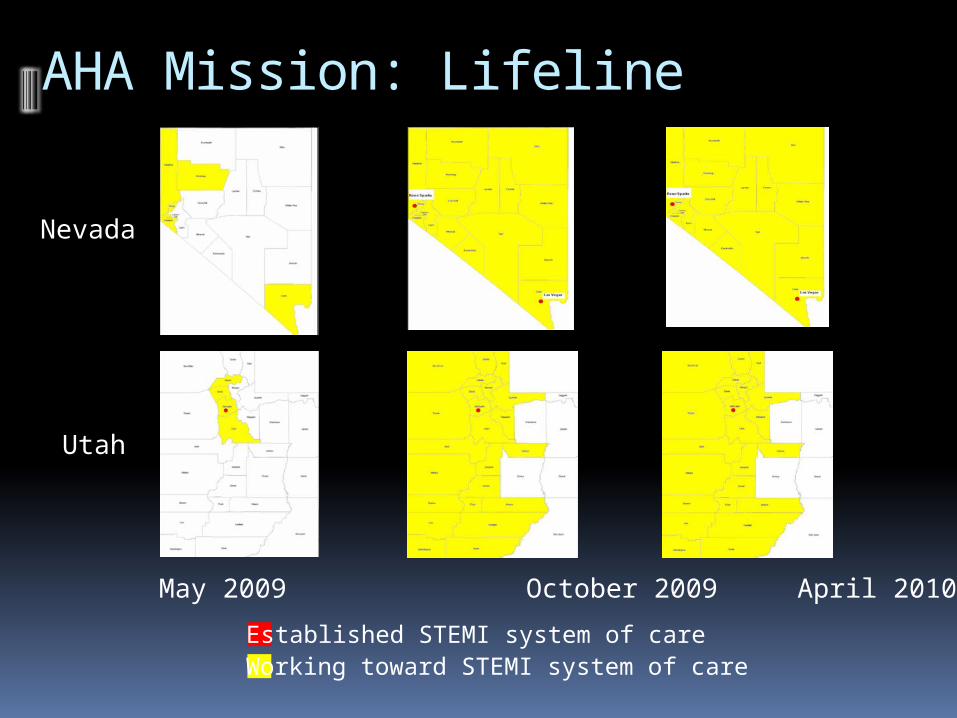
AHA Mission: Lifeline
May 2009 October 2009 April 2010
Established STEMI system of care Working toward STEMI system of care
AHA Mission: Lifeline
May 2009 October 2009 April 2010
Established STEMI system of care Working toward STEMI system of care
Nevada
Utah
End







