douglas m. kerr, ph.d. washington state psychological...
TRANSCRIPT
Douglas M. Kerr, Ph.D.Washington State Psychological Association
October 18, 2014
Only one, but it has to want to change.
Motivational Interviewing looks for motivation in the person’s most deeply held values and in the chemistry of the relationship with the provider.
20 to 45% of the prescriptions written are never filled.
Slightly over half of the prescriptions that are filled are taken (more or less) as prescribed.
This is a shadow that hangs over treatment efficacy research where patients are dropped from the study if they do not comply.
A treatment that is not implemented is not going to be effective.
Brunton, SA (2011) Improving medication adherence in chronic disease management. J. Family Practice, 60(4), S1.
Assumptions about why clients don’t change and what to do about it:
Lack critical information for reasoned choice = EDUCATELack behavior change skills = TRAINLack “will power” or character strength = EXHORTFail to appreciate the seriousness of the situation = CONFRONT
Inappropriate lack of concern or motivation = GIVE UP
Resistance occurs when the patient has not yet decided that the change under discussion is currently in his/her best interest or worth the effort required (but the provider does).
Resistance occurs when the provider and patient have not yet found a way to collaborate effectively.
Resistance is no longer a term used in MI3. Two new terms cover the “resistance” concept:◦ Discord is the friction or confrontational aspect of the
pt/provider interaction.◦ Sustain talk is the verbal expression of unwillingness or
reluctance.
Feel listened to and understood
Sense of self-efficacy and empowerment
Hope and positive expectations
Change consistent w/larger goals & values
Make a commitment
Collaborate with patient at her/his currentstage of change
Express empathy, be nonjudgmental
Explore and articulate ambivalence aboutthe behavior change
Evoke client’s resources, motivations, & strengths
Elicit “change talk” (i.e., desire, intention, or commitment to change)
Roll with resistance and avoid argumentation
Support self-efficacy and personal choice
Person Centered: People change when they are accepted non-judgmentally with accurate empathy.
Self Perception: When clients argue for change, change is more likely.
Values: Clients change when the status quo violates their closely held values.
Motivation is the product of an interaction, not a personality trait.
Collaboration with the patient yields greater change than confrontation.
Resistance occurs when the provider has not yet figured out how to collaborate effectively.
Almost all patients are ambivalent about changeto some extent.
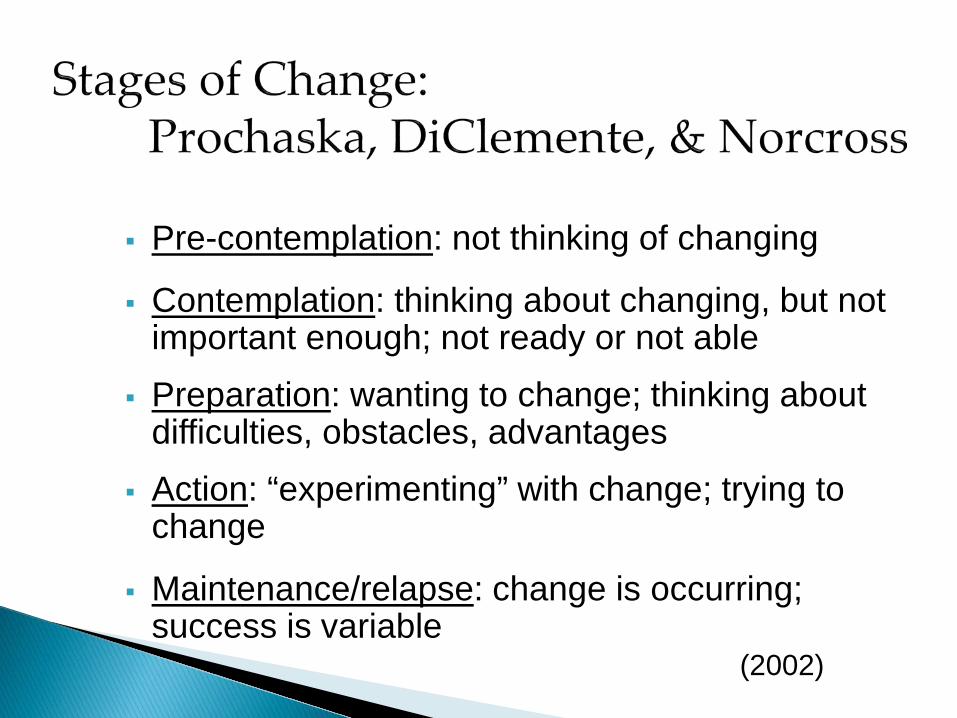
Pre-contemplation: not thinking of changing
Contemplation: thinking about changing, but not important enough; not ready or not able
Preparation: wanting to change; thinking about difficulties, obstacles, advantages
Action: “experimenting” with change; trying to change
Maintenance/relapse: change is occurring; success is variable
(2002)
“I know I should quit smoking, but I’ve got a big exam coming up and I know it will be a pack a day for thenext two weeks.”
“I’ve tried to give up sweets for 20 years and failed. Nowmy doctor says my diabetes is getting worse and startingto affect my eyes.”
“I’m a confirmed couch potato. My doctor says if I don’tget moving, I’ll die an early death. I don’t know if I believehim or if I care.”
“I’ve had two ‘spells’ in the last 2 weeks. I keep forgettingto take my pills. I’ve never been good with pills.”
Importance: What are the advantages? Is it worth the effort? Will it really help?
Confidence: Can I change if I try? How hard will it be? What if I fail?
Readiness: Is this the best time to try? What else must I do to prepare?
“I know I should stop drinking, but it will turn my worldupside down and I might not be able to keep it up.”
—I should, but I don’t want to and I’m not sure I could if I tried.
“I actually like to exercise, but I just don’t have timewith my mom in the hospital and all.”
—I want to, but I’m not sure I can and this is a really bad time to try.
“They don’t call them ‘cancer sticks’ for nothing. I know it will kill me, but I’ve tried to stop a dozen times and I don’t usually last even a week.”
—I should, but I can’t and I doubt I ever will.
“I know I can stop drinking, but not right before my21st birthday!”
—I should and I could, but I’m not ready yet.
“I need to go on a low-fat, low-cholesterol, low-enjoyment diet now that I’ve had a second heart attack, but I haven’t even started yet and I’m already dreaming about cheese-burgers and French fries.”
—I should and I’m ready, but I’m not sure I can.
“I’ve taken these psych meds off and on for a year now and you want me to take them everyday! I don’t do anything every day except ___ and ___, man. Give me a break!”
—Maybe I could, but I’m not going to and you can’t make me.
Elicit from patient his/her own “change talk”
Articulate the patient’s ambivalence re: change
Selective focus on pt’s own reasons for change
“It is the patient and not the counselor whoshould be making the arguments for change ….The counselor’s job is to find and connect with those reasons, with the co-healer inside the patient.”
—William Miller, 2004
Directing implies a top down interaction where one party is acknowledged to have more expertise and sets the agenda.
Guiding represents an approach which positions the provider as a consultant who helps the pt to clarify and carry out their goals. Agenda setting is collaborative.
Following indicates a “good listener” who prioritizes the pt’s experience and exercises minimal influence over the agenda.
There is a time and place for each. None is wrong or bad, but may be more or less effective in a given situation.
When the leading communication style is not working effectively, guiding can be a viable option.
Collaborative agenda setting consistent with Patient-centered medicine.
“We usually check in on your blood sugars, your eating, and exercise. There may be something else you want to discuss today too. What would be most important to you for us to talk about today?”
“Your blood pressure is high again today, so we will need to talk about that. What else do we need to talk about today?”
“I need to check your feet and eyes as we always do, but last time you mentioned that you have been feeling depressed and we didn’t have time to discuss it. Should we talk about that today?”
“For your exercise, you have been trying to walk around three blocks every day, but you have only been able to do it about half of the time. What else could you do on the days that you don’t walk?”
“You want to cut down on your drinking, but you aren’t sure you are ready to stop. Some of my pts find that it helps to have designated non-drinking days and days when you can drink if you want to. Do you think that might help you?”
“Which of these options (collaboratively brainstormed) would you like to try first?”
Open Questions: genuinely curious questions inviting elaboration by the patient
Affirmations: encouraging, appreciation of patient’s efforts and intentions
Reflective Statements: empathic articulation of the patient’s experience
Summaries: review of patient’s main concerns, focus on ambivalence
Invite the patient to elaborate on thoughts, feelings, experiences, and motivations
Elicit from the patient personal strengths, knowledge, experience, and resources
Allow the therapist to introduce topics or change direction of the interview (selective attention)
Begin with How? What? Who? When? or Why?
NOT with Do you? Does it? Are you? or Is it?
Identify and articulate personal strengths:“I bet there were many times when you were readyto give up on your chemo, but you were able to hang on when the going was rough.”
Focus on demonstrated character traits and stated intentions, not on accomplishments per se:
“Other people doubted you could do it and that just made you more determined.”
Appreciation of client attributes:“You care more about your sobriety than the opinions of those idiots.”
Empathy, sensitivity, creativity, ability to “seethe flowers among the weeds” is required
NOT cheerleading
Simple Reflection: paraphrase or restatement including emotional tone
Complex Reflection: adds context and dimensionto rephrasing, articulates the unsaid
Double-Sided Reflection: both sides of ambivalence about change juxtaposed
Amplified Reflection: rephrase ‘goes further’ than patient’s expression
-
Simple: “You think they ganged up on you and you are angry and hurt.”
Complex: “You think they ganged up on you and you areso mad that you are not going to forgive them for it this time.”
Simple: “You feel like you have failed and let everybody down.”
Complex: “You feel like you have let everyone down, yourself included, and this has happened so many times before that you are not sure it is any
use even trying.”
“You know there are lots of good reasons to try to bringyour weight down, but your life is centered around foodand it seems like you would have to change everything.”
“The psych meds you have been taking have had some side effects that you don’t like and some therapeutic effects that help you.”
“On one hand, you want to live to see your grandchildren grow up, and on the other, you don’t know if it’s worth it to go through another series of chemo. It’s so much suffering and there seems to be no end to it.”
“You have tried everything and nothing has helped at all.”
“Even with your doctor’s help, you’re sure that you can’t stop smoking and you never will.”
“You are not going to do it. NO WAY. You don’t even carewhat they do to you.”
“You’re sick of thinking about it. If you are going to die young, so be it!”
“You are so frustrated that you are ready to give up.”
In conversations, people tend to self-correct to a middle position, e.g. if the provider takes a strong abstinence position, the pt will argue that such a strong position is overboard, but if the provider were to take a strong position on the other side, the pt would argue with that position as well. This would cause the pt to argue for more self control.
Example: Provider: “Cholesterol is not going to kill you anytime soon. Maybe you don’t want to concern yourself with it now.” Patient: “I don’t want to wait until it is too late!”
Selectively organize threads of the conversation
Focus on ambivalence
Reinforce change talk
Link current concerns to previous statements
Opportunity to transition to new topics
Often followed by an open question
“You have told me in detail about the many times you have tried to stop smoking, how hard you have tried, and all the problems that you have run into. Now youare discouraged, but you still want to keep trying despite everything. You told me, ‘I refuse to be addicted.’”
Follow-up question:
“What does that say about you?”
“You have explained to me how much you don’t like getting shots. You start to worry a week before and lose sleep thinking about it. You worry you might faint or embarrass yourself somehow, even though this has never happened. Sometimes you think it is silly to make such a big deal out of a shot. You have skipped some of your scheduled injections when you backed out at the last minute. You know you need these shots, but that doesn’t keep you from hating every one of them, and even skipping out on a few.”
Follow-up question:
“What makes the difference between being ableto make yourself go to the injections or just stay home?”
Change talk involves self-motivational statements about change.
Change talk refers to specific behavior or set of behaviors.
Change talk expresses the desire or ability to change, the benefits of change, or commitments and/or actions to change.
Sustain talk expresses the reasons or desire not to change
Motivational Interviewing (MI) is the only therapy that explicitly focuses on eliciting change talk.
Desire for change (but no commitment):“I wish… I hope… I’m not the person I want to be.”
Ability or optimism about change:“I’m going to have to do it someday; I’m going to prove them wrong.”
Reasons or benefits of change:“If I don’t, I’ll lose my license; If I do, maybe she’ll get off my back!”
Need for change or problems with the status quo“I need to …. I have to …. It can’t stay like this.”
DARN statements are moderately related to behavior change.
Use verbs that communicate the intention to act:“I’m going to …. I’ve already started to ….”
Client asserts that the goal is take action:“I know I have to bite the bullet and start now.”
Taking steps:“I told him I would leave if he didn’t stop; I madea healthy choice.”
Commitment and mobilizing language is strongly related to behavior change.
OARS:
Open questions, Affirmations, Reflective Statements, Summaries
Evocative Questions:
“What is the thing you most want out of this?”
Elaboration:
“When things were better, what was happening?”
Extremes:
“How bad would it get if this all falls apart?”
Time Shifts:
“When you got married, what kind of a life did you think you would have now? Five years from now, what do you think will be happening with this?”
Re-visit Goals:“How does this fit in with what you told me youwant for yourself?”
Assessment Feedback: Personalized (either normative or related to client goals); permission asked; Elicit—Provide—Elicit
Scaling Questions
Elicit: Inquire if the patient wants feedback: “What kind of feedback would be helpful?”“What conclusions has pt. already drawn?”
Provide feedback stated in neutral terms:“People in your situation … at your level of use …generally need these services … experience thesekinds of problems ….”
Elicit: Inquire what pt. made of feedback: “What does this mean to you?”“How does this change how you see the problem?” “Would some other feedback be more helpful?”
Format:
“On a scale of 0 to 10, how important is it for you to make this change?”
Meaning:
“What made you choose a 7?”“What made you choose a 7 rather than a 5?”“What kept you from choosing a 9?”
Change:“Last time, you chose a 5. What moved it to an 8?”“What would it take to move it to a 9?”
Avoid argumentation
Emphasize personal choice
Approach resistance with empathy
Be aware of types of resistance:
Complete rejection of problem Oppositional attitude (counter-control) Reluctance (often not voiced)
Review and revise patient’s stage of change
Complete Rejection of Problem: “I don’t go along with any of this.”“This is all a bunch of s---.”“I do not think I have a problem and you are trying to tell me I do. Who the hell are you anyway? God?”
Oppositional Attitude (Counter-Control): “I don’t let anybody tell me what to do.”“Push me about this and see where it gets you.”“Anybody who gets between me and my cigarettesis dog meat.”
Reluctance (Often Not Voiced):“I don’t know how that would work out.”“That might cause a lot of complications, but I’m not sure what exactly.”
Behavior:Distracted, eye rolling, looking at the floor or out the window, grunts, etc.
Yes, buts ….:“That’s a good idea, but it would never work.”“You know I want to quit, but not right now.”
Empathize, empathize, empathize
Use reflective statements to articulate resistance
Avoid taking the pro-change position
Emphasize personal choice
Amplify no-change position to invite the “righting reflex”
Change the topic to something both can agree on
Agree (with a twist)
“This is like some kind of nightmare. You don’t know why you have to be here or what this is all about or what you have to do. You just know you don’t like it.”
“You don’t know what the all the fuss is about. You are overweight and you always have been. So what. It never slowed you down. Until now….”
“You don’t want to take your Lithium because it makes you gain weight. You are sick of being fat and you can’t do anything about it when you are taking this drug. You just keep ballooning up and that makes you feel out of control. It starts you wondering if was really so bad when you were off your meds.
How was it?”
T: You feel like you’re between a rock and a hard place with this Court order. You think it’s stupid and unnecessary and you hate to be told what to do. What will you do now?
C: I guess I have to do it. I don’t have any choice!T: You know what will happen if you don’t—back to jail.
But you do have a choice. If you decide not to goalong with treatment, you can refuse, as long as youare willing to do some more time.
C: This is so f---ing stupid! I can’t believe it!
T: You hate this, but you are the only one who can decide if you are going to treatment.
T: You have been told that you need to go on dialysis, but you don’t know yet if you are going to. No one seems to be recognizing that it is your decision to make.
C: That’s right. I just don’t know if it’s worth it. I don’t want to be dependent on a machine to live and I don’t like people telling me what to do. Everybody tells me I have to do it.
T: You want people to listen to you and acknowledge that it is your choice to make. You know they have your best interests at heart, but…
C: Who the hell are you? Why do I have to talk to another shrink? Don’t you guys have something better to do than harass me?
T: You don’t want to be here and you think I’m goingto make you do something you don’t want to do.
C: That’s right. Another know-it-all asshole telling mewhat to do.
T: I know you’re in control of what you do and don’t do. I can’t make you do anything, and I’m not going to try. Tellme about how you got such a high opinion of shrinks.
Transition Indicators: Increased change talk, esp. mobilizing and commitment language; questions about what and how to make change.
Therapist Key Questions: What’s next? What doyou want to do now? What is the next step?
Revisit Goals: How do you want your life to be different? What change would really make a difference for you? What is the most important thing you want to get out of this?
Key Questions:
“What’s next?”“What do you want to do now?”“What is the next step?”
Revisit Goals:
“How do you want your life to be different?”“What change would really make a difference for you?” “What is the most important thing you want to get out of this?”
Brainstorm a plan and organize best ideas
Advise on the elements of the plan (e.g., feasibility):“May I share with you some of the things my other patients have done that worked for them?”
Write the plan down (or not):“Would it help you to have a written copy of the thingsyou are deciding to do now?”
Reaffirm commitment to specific plan:“Is this plan in line with the kind of changes you want for yourself? If you succeed at this plan, will it really make a difference?”
Summarize the current motivation to change and check for accuracy.
Specify steps patient is willing to take and when.
Designate resources needed for each step.
Emphasize self-efficacy and personal control.
Review and Reassess confidence specifically for this plan.
Bem’s (1967) self-perception theory contradicted Festinger’s (1957) cognitive dissonance theory.
Bem said there is no innate drive to maintain consonance of beliefs, attitudes, and behaviors.
Instead, people observe their own behavior to determine their attitudes.
But only when the behavior is not coerced.
When the person is unsure and not coerced, attitudes shift toward the arguments.
We come to believe in that for which we freely argue.
Arkowitz, H., Westra, H., Miller, W.A., & Rollnick, S. (2008). Motivational interviewing in the treatment of psychological problems. New York: Guilford.
Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change (3rd ed.) New York: Guilford.
Prochaska, J. O., Norcross, J. C., & DiClemente, C. C.. (1994). Changing for good. New York: Avon Books.
Rollnick, S., Miller, W.M. & C. Butler, (2008). Motivational interviewing in health care. New York: Guilford.
Rosengren, D. (2009). Building motivational interviewing skills: A practitioner’s workbook. New York: Guilford.
www.motivationalinterview.org