donor selection: haploidentical donor. dr. wang yu
TRANSCRIPT
YU WANG, MDBeijing, China
• Assistant Professor, Stem Cell Transplant, Peking University Institute of Hematology
• Dr. Yu Wang obtained her medical degree from Peking University Medical College, China and underwent internal medicine training at Peking University People’s Hospital. Thereafter, she completed training in Hematology at Peking University Institute of Hematology. Dr. Wang has published in numerous peer reviewed journals. She is one of the main prize winners of Second Prize of National Science and Technology Award and Second Prize of Chinese Medical Science and Technology Award. She serves as the vice-president of young commissioner, Beijing Society of Hematology, Beijing Medical Association. Areas of Interest: Risk stratification, management of post- HSCT relapse, haploidentical HSCT
Donor selection for
haploidentical hematopoietic
stem cell transplantation
Yu Wang , Ying-Jun Chang, Xiao-Jun Huang*
Peking University Institute of Hematology
Peking University People’s Hospital
Beijing Key Laboratory of Hematopoietic Stem Cell Transplantation
Questions need to be answered
• ideal donor selection: many aspects
• haploidentical HSCT : unlimited donor and
availabilities of more than one donor
• whether one donor preferred among various
haploidentical donors available
Wang Y, Huang XJ, et al. Cancer 2013;119:978-85
Introduction
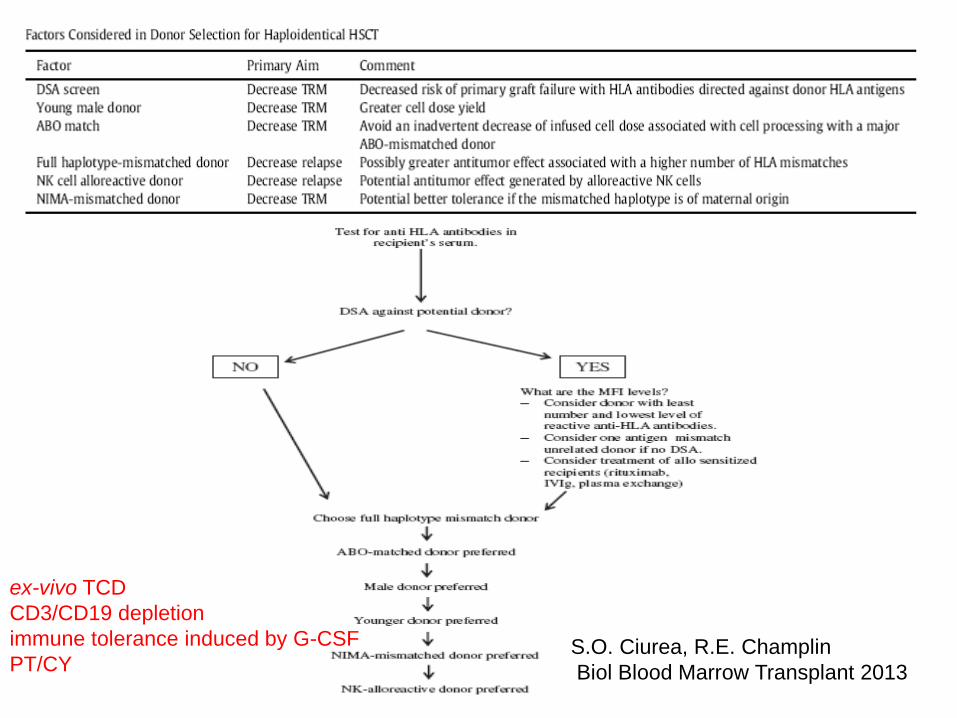
S.O. Ciurea, R.E. Champlin
Biol Blood Marrow Transplant 2013
ex-vivo TCD
CD3/CD19 depletion
immune tolerance induced by G-CSF
PT/CY
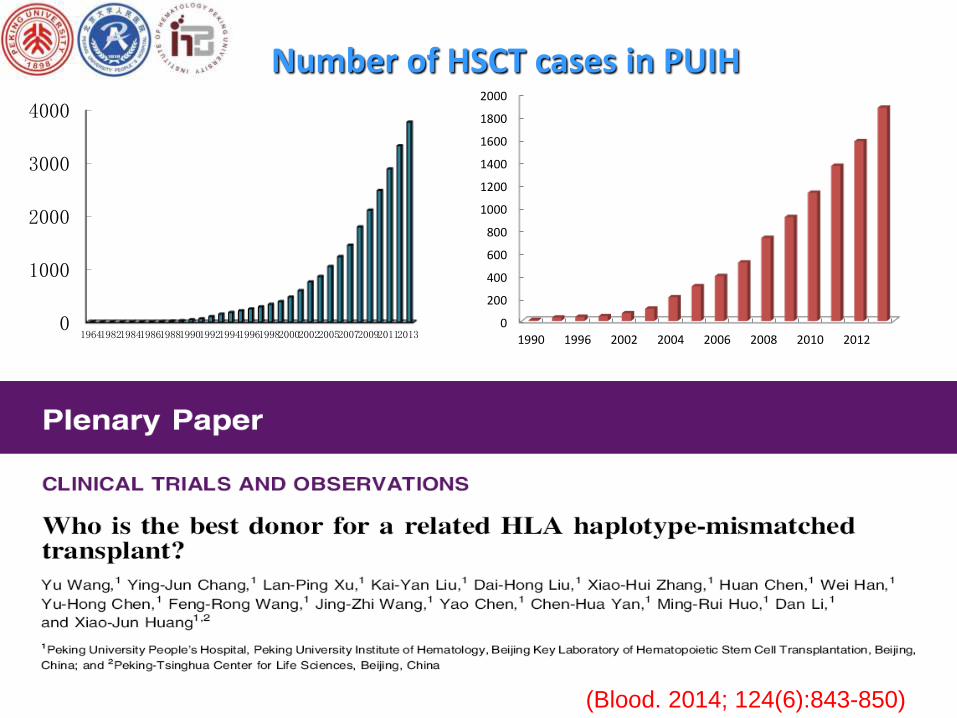
(Blood. 2014; 124(6):843-850)
0
1000
2000
3000
4000
196419821984198619881990199219941996199820002002200520072009201120130
200
400
600
800
1000
1200
1400
1600
1800
2000
1990 1996 2002 2004 2006 2008 2010 2012
Number of HSCT cases in PUIH
Purpose & Design• Really overcome HLA barrier ?
• Which factor impact donor selection?
• Did NIMA rule still play a role?
Introduction
• Haploidentical HSCT without in-vitro TCD
• 2002.5-2013.2 follow-up: 2013-12-1
• Conditioning: Modified Bu/Cy + ATG
• Graft: G-BM+G-PB
• collateral relatives excluded
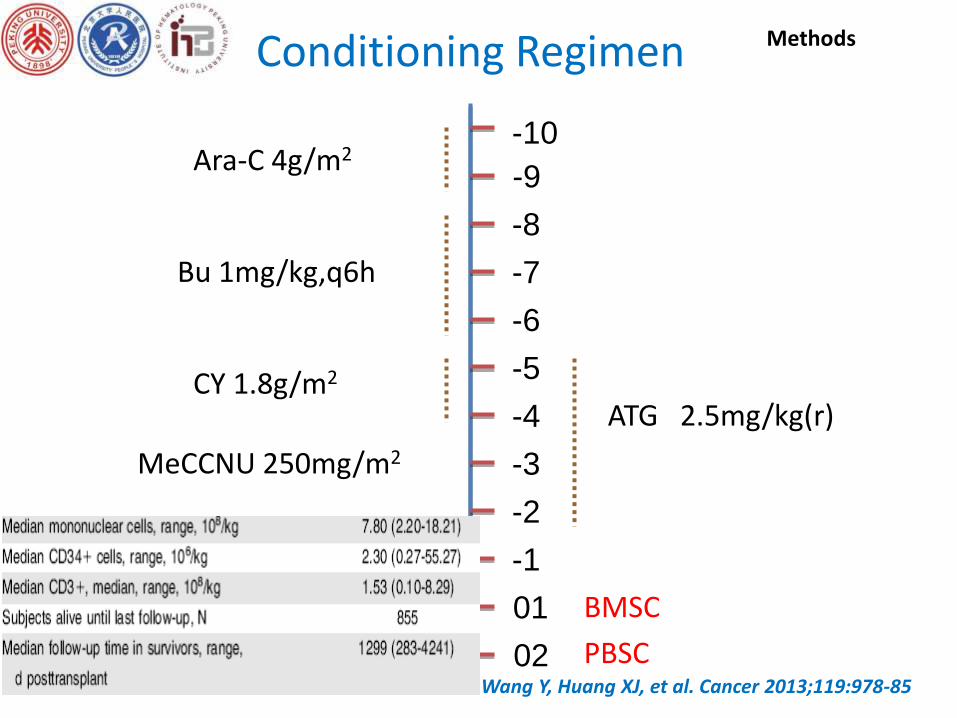
Conditioning Regimen
ATG 2.5mg/kg(r)
-10
-8
-3
-5
-1
01
Ara-C 4g/m2
-6
-9
Bu 1mg/kg,q6h
CY 1.8g/m2
-4
MeCCNU 250mg/m2
-2
-7
BMSC
PBSC02
Methods
Wang Y, Huang XJ, et al. Cancer 2013;119:978-85
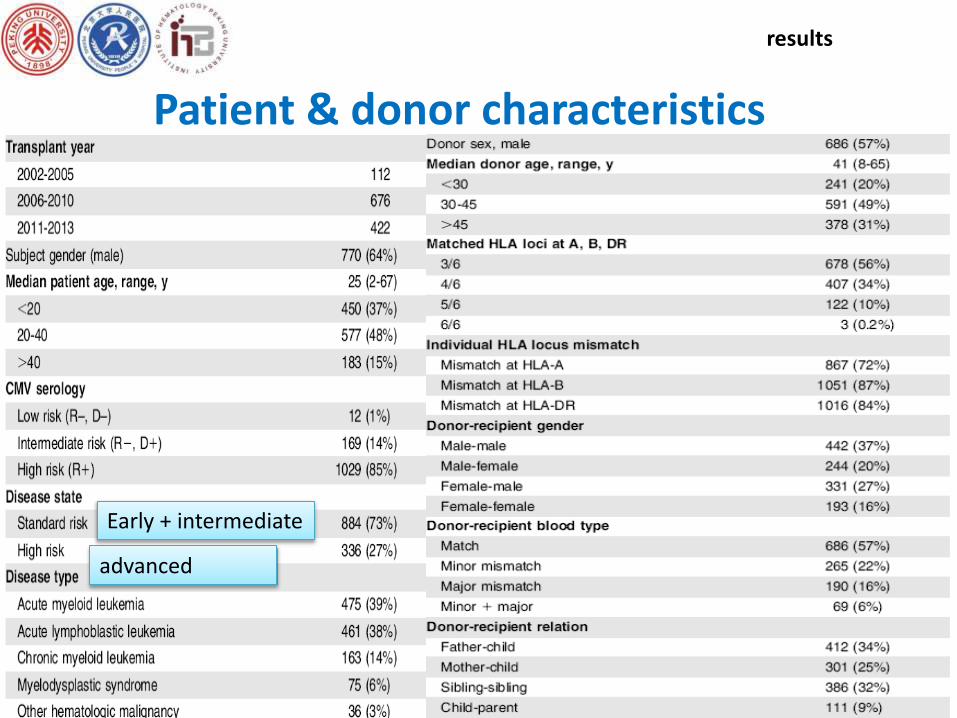
Patient & donor characteristics
results
Early + intermediate
advanced
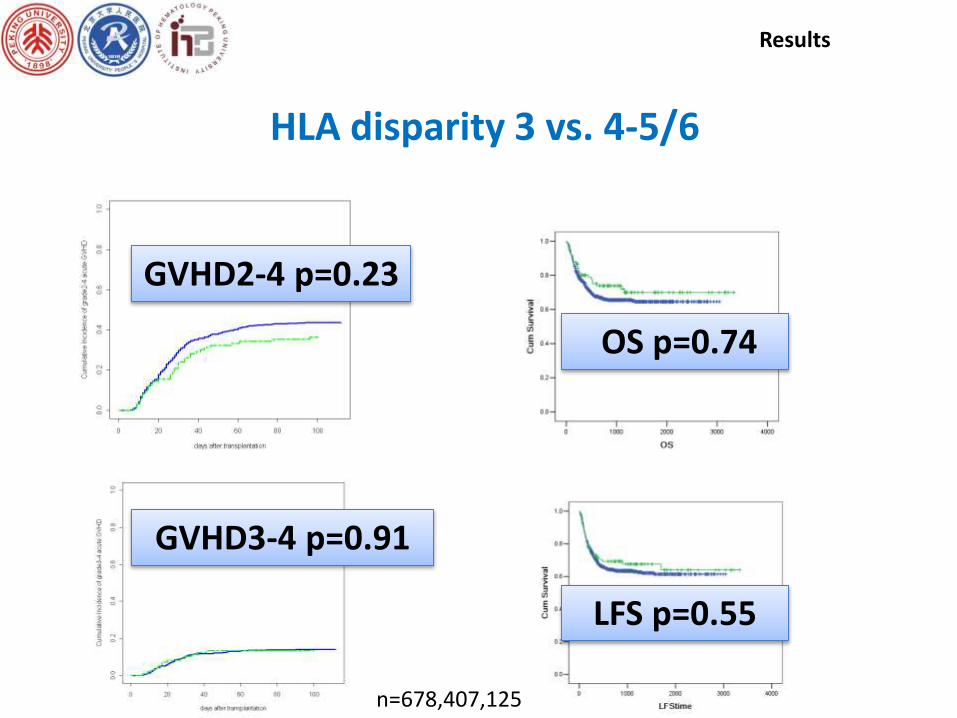
HLA disparity 3 vs. 4-5/6
Results
GVHD
P<0.001
GVHD2-4 p=0.23
GVHD3-4 p=0.91
OS p=0.74
LFS p=0.55
n=678,407,125
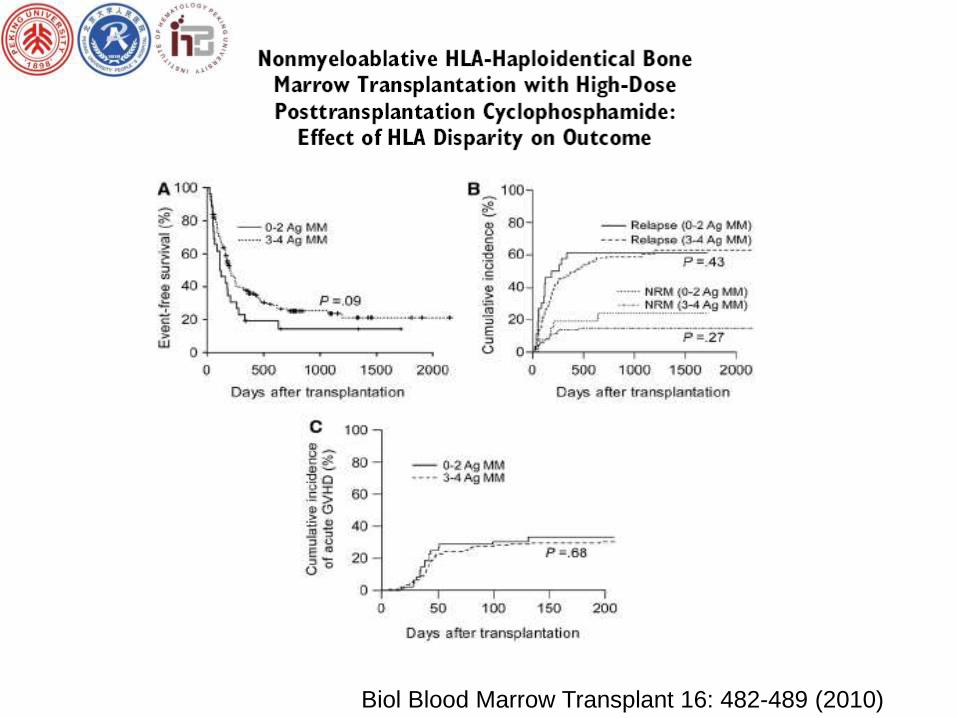
Biol Blood Marrow Transplant 16: 482-489 (2010)
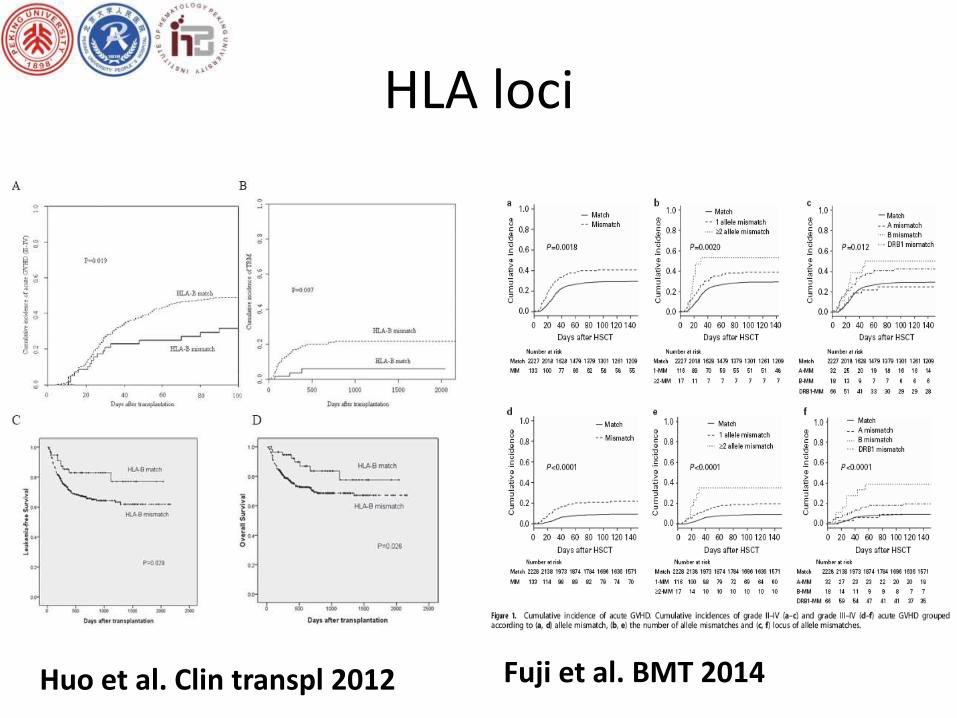
HLA loci
Huo et al. Clin transpl 2012 Fuji et al. BMT 2014
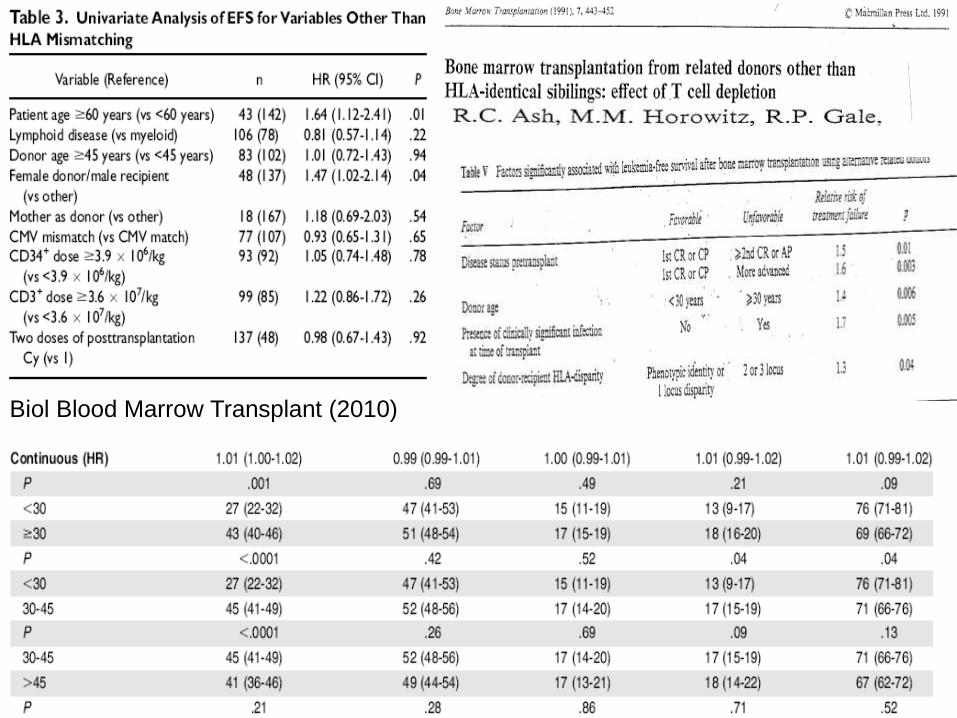
Biol Blood Marrow Transplant (2010)
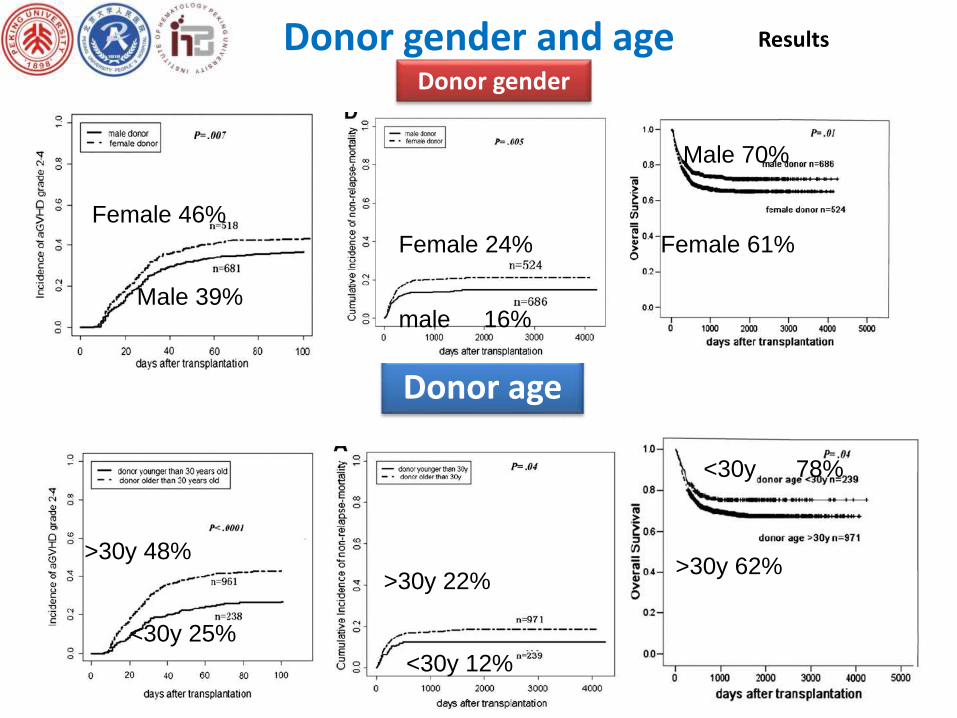
Donor gender and age Results
Donor gender
Donor age
Female 46%
Male 39%
>30y 48%
<30y 25%
Female 24%
male 16%
>30y 22%
<30y 12%
Male 70%
Female 61%
<30y 78%
>30y 62%
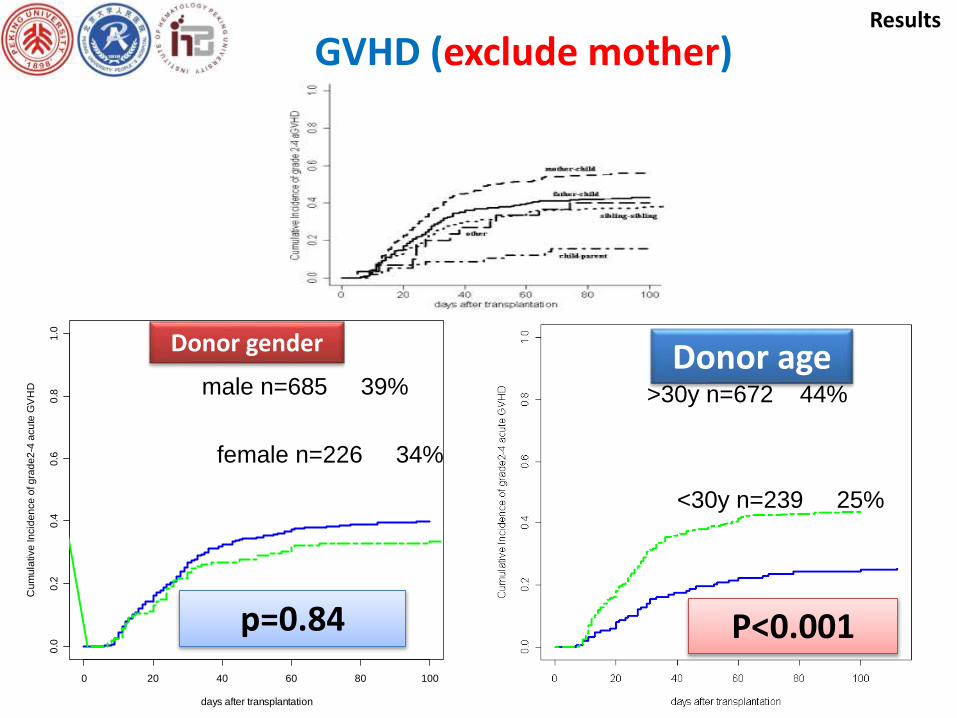
Donor sex
Results
Donor age
>30y n=590 48%
<30y n=159 25%<30y n=239 25%
>30y n=672 44%
0 20 40 60 80 100
0.0
0.2
0.4
0.6
0.8
1.0
days after transplantation
Cu
mu
lative
In
cid
en
ce
of g
rad
e2
-4 a
cu
te G
VH
D
female n=226 34%
p=0.84
male n=685 39%Donor ageDonor gender
GVHD (exclude mother)
P<0.001
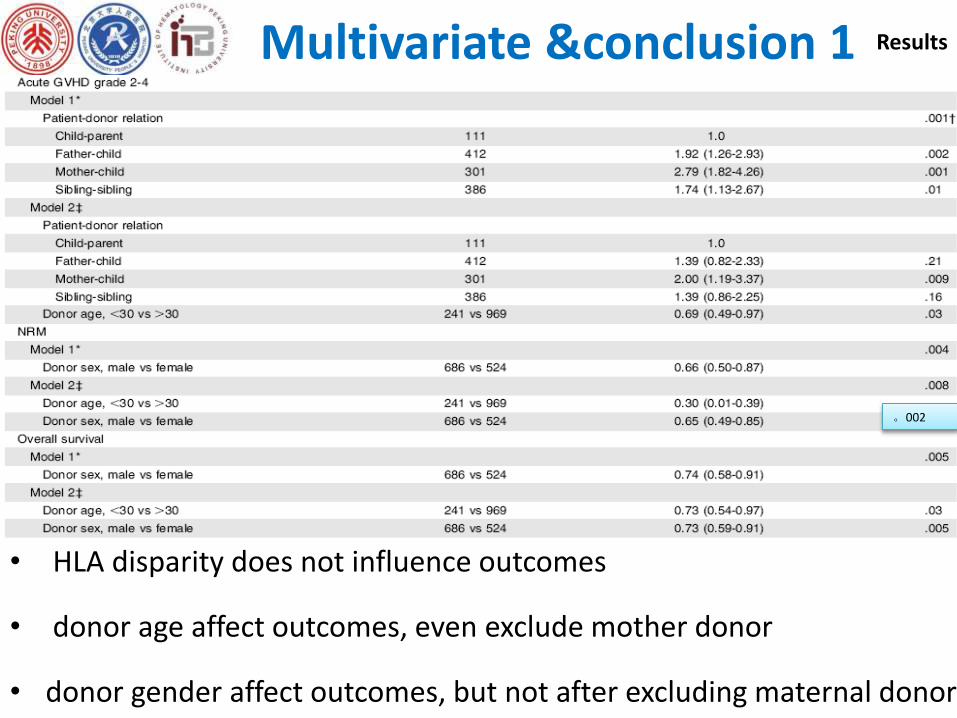
Multivariate &conclusion 1 Results
。002
• HLA disparity does not influence outcomes
• donor age affect outcomes, even exclude mother donor
• donor gender affect outcomes, but not after excluding maternal donor
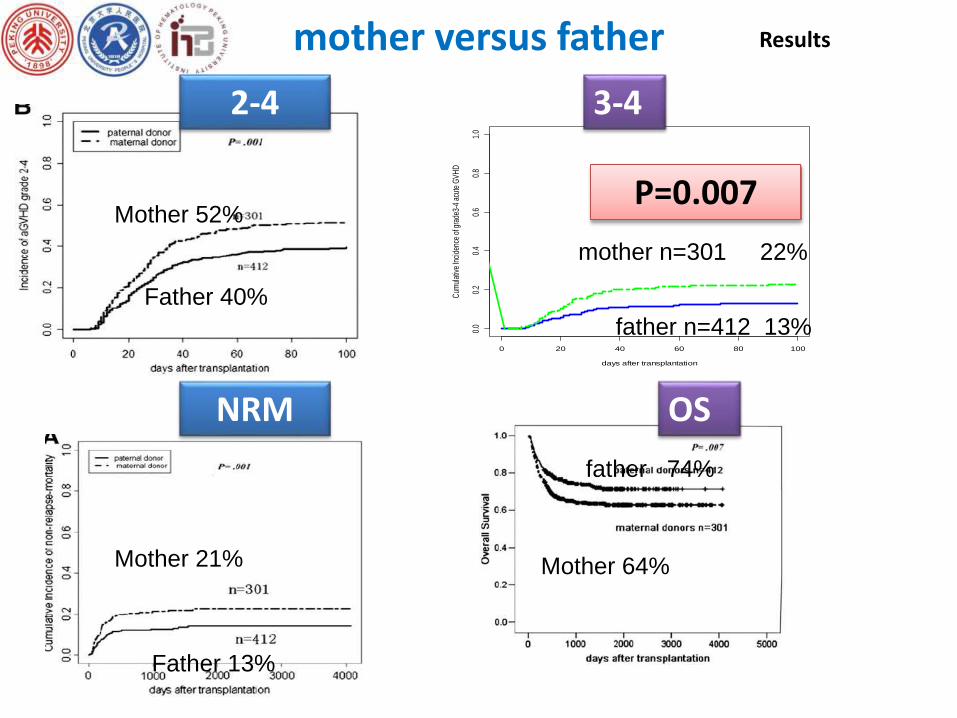
Results
P=0.007
0 20 40 60 80 100
0.0
0.2
0.4
0.6
0.8
1.0
days after transplantation
Cum
ulat
ive
Inci
denc
e of
gra
de3-
4 ac
ute
GV
HD
mother versus father
3-42-4
Mother 52%
Father 40%
mother n=301 22%
father n=412 13%
Mother 21%
Father 13%
NRM
father 74%
Mother 64%
OS
Results
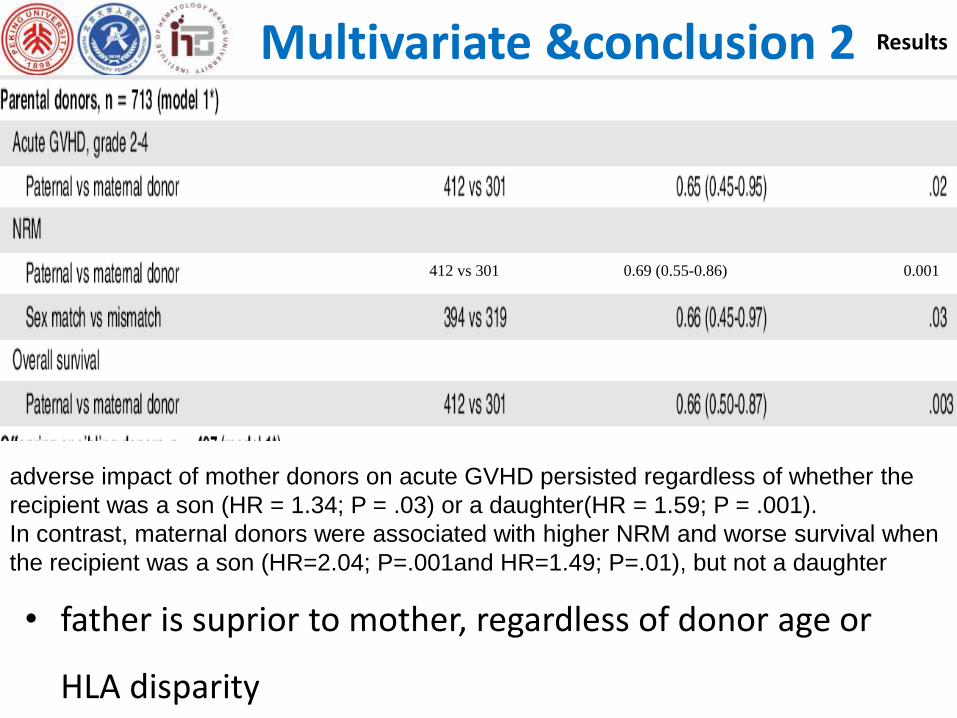
412 vs 301 0.69 (0.55-0.86) 0.001
adverse impact of mother donors on acute GVHD persisted regardless of whether the
recipient was a son (HR = 1.34; P = .03) or a daughter(HR = 1.59; P = .001).
In contrast, maternal donors were associated with higher NRM and worse survival when
the recipient was a son (HR=2.04; P=.001and HR=1.49; P=.01), but not a daughter
• father is suprior to mother, regardless of donor age or
HLA disparity
Multivariate &conclusion 2
children vs. sibling
Results
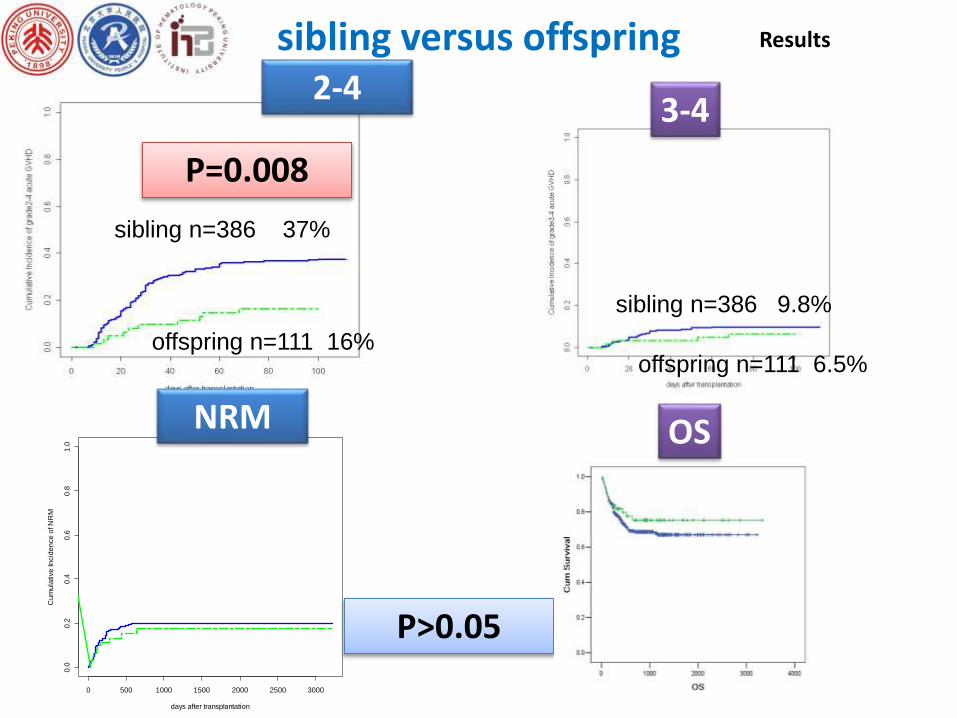
P>0.05
sibling versus offspring 2-4
3-4
sibling n=386 37%
offspring n=111 16%
P=0.008
sibling n=386 9.8%
offspring n=111 6.5%
0 500 1000 1500 2000 2500 3000
0.0
0.2
0.4
0.6
0.8
1.0
days after transplantation
Cu
mu
lative
In
cid
en
ce
of N
RM
NRM OS
Results
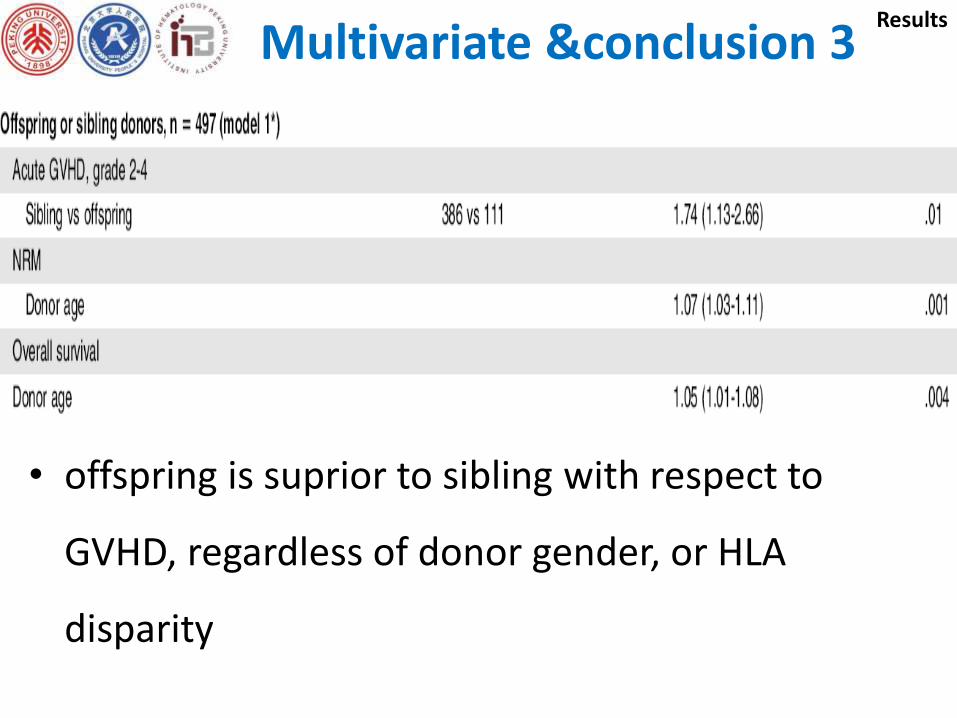
• offspring is suprior to sibling with respect to
GVHD, regardless of donor gender, or HLA
disparity
Multivariate &conclusion 3
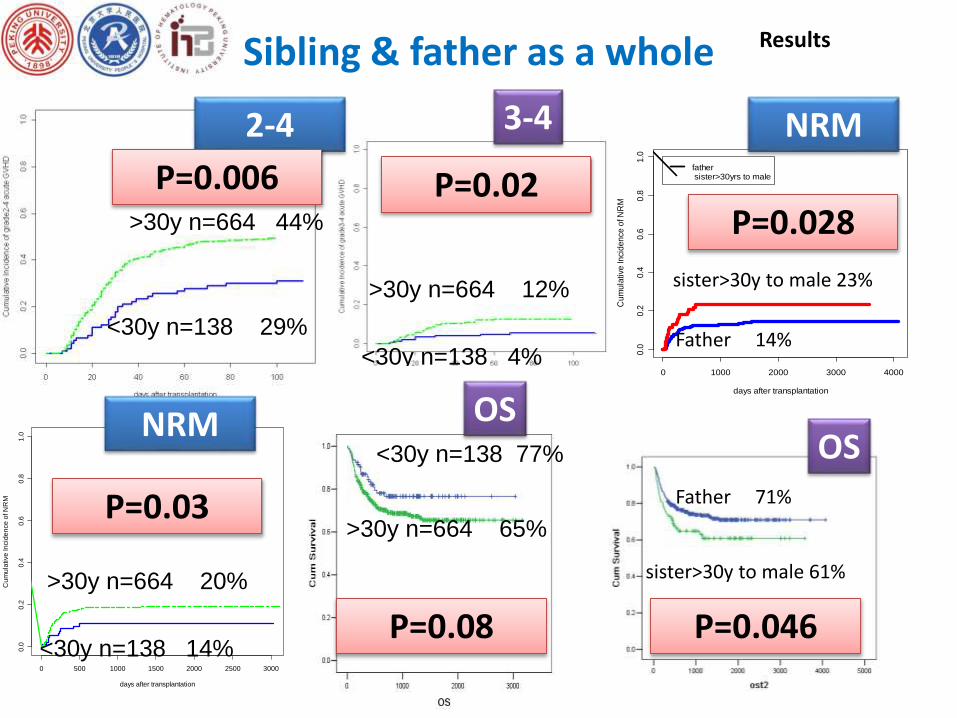
Father & sibling
ResultsSibling & father as a whole
2-4 3-4
<30y n=138 29%
>30y n=664 44%
P=0.006 P=0.02
>30y n=664 12%
<30y n=138 4%
0 500 1000 1500 2000 2500 3000
0.0
0.2
0.4
0.6
0.8
1.0
days after transplantation
Cu
mu
lative
In
cid
en
ce
of N
RM
NRM
>30y n=664 20%
<30y n=138 14%
P=0.03
OS<30y n=138 77%
>30y n=664 65%
0 1000 2000 3000 4000
0.0
0.2
0.4
0.6
0.8
1.0
days after transplantation
Cu
mu
lativ
e In
cid
en
ce o
f NR
M
father sister>30yrs to male
Father 71%
sister>30y to male 61%
P=0.046
OS
P=0.028
NRM
sister>30y to male 23%
Father 14%
P=0.08
Results
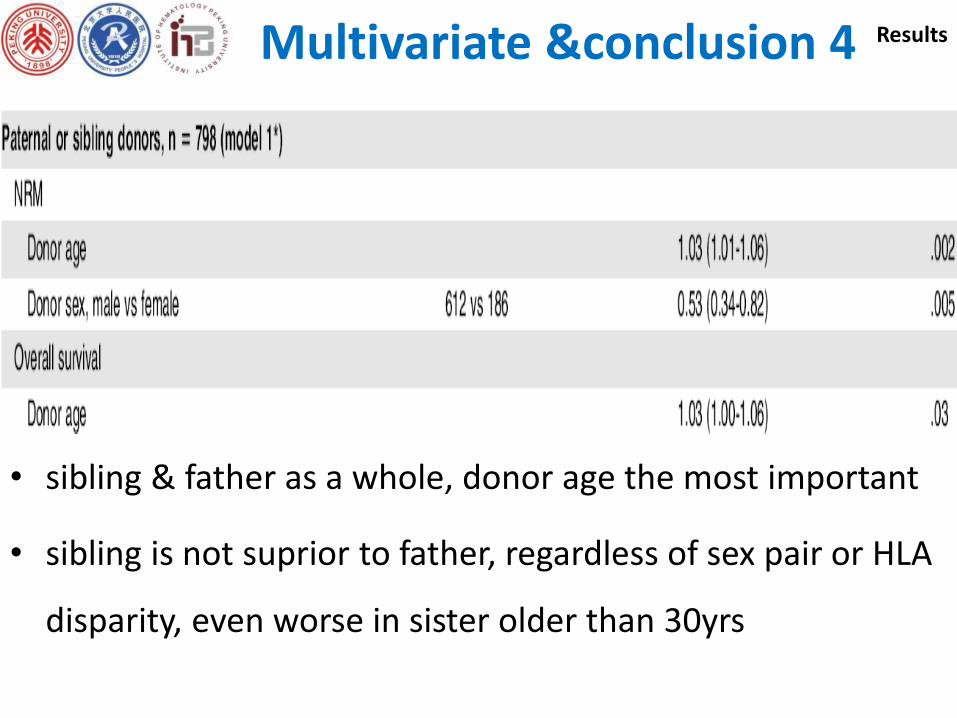
• sibling & father as a whole, donor age the most important
• sibling is not suprior to father, regardless of sex pair or HLA
disparity, even worse in sister older than 30yrs
Multivariate &conclusion 4
Father & sibling
Results
Results
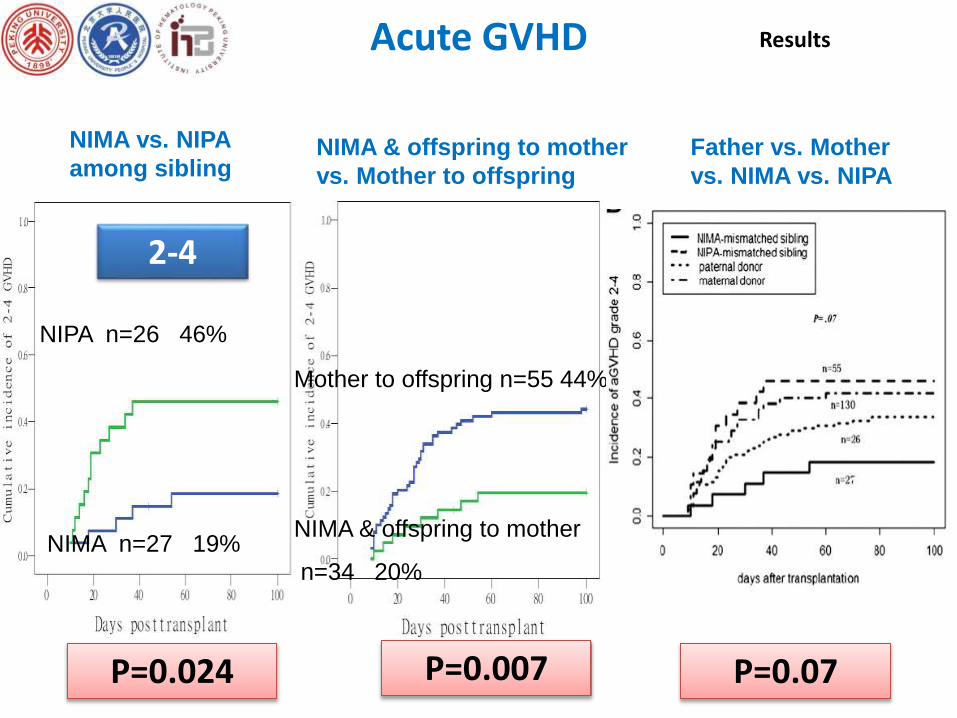
P=0.024
Acute GVHD
2-4
NIPA n=26 46%
NIMA n=27 19%
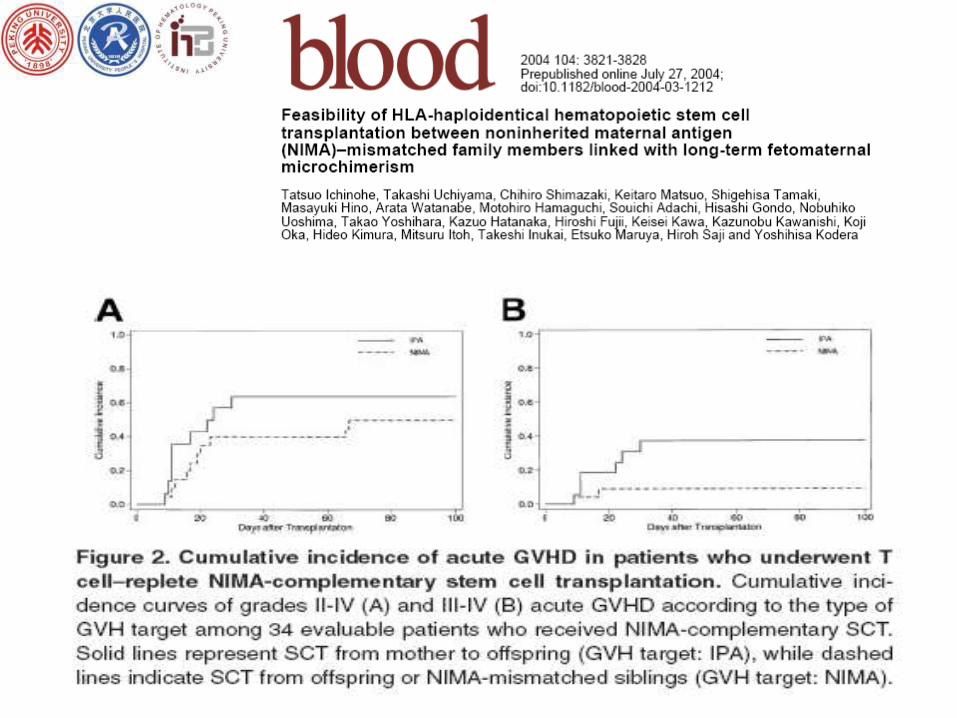
NIMA vs. NIPA
among sibling
P=0.007
Mother to offspring n=55 44%
NIMA & offspring to mother
n=34 20%
NIMA & offspring to mother
vs. Mother to offspring
P=0.07
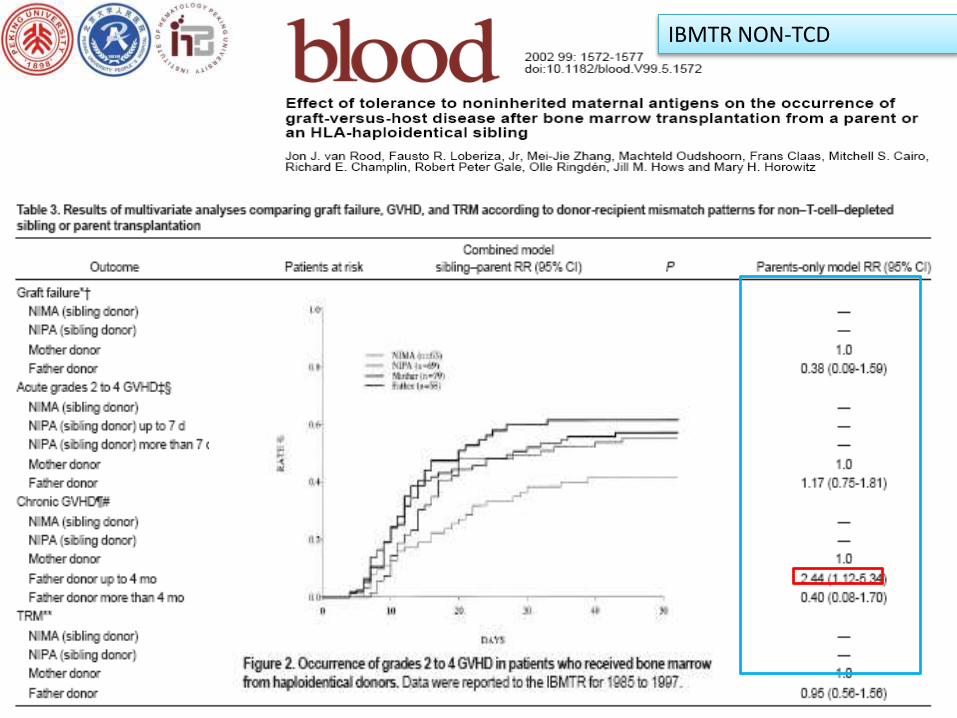
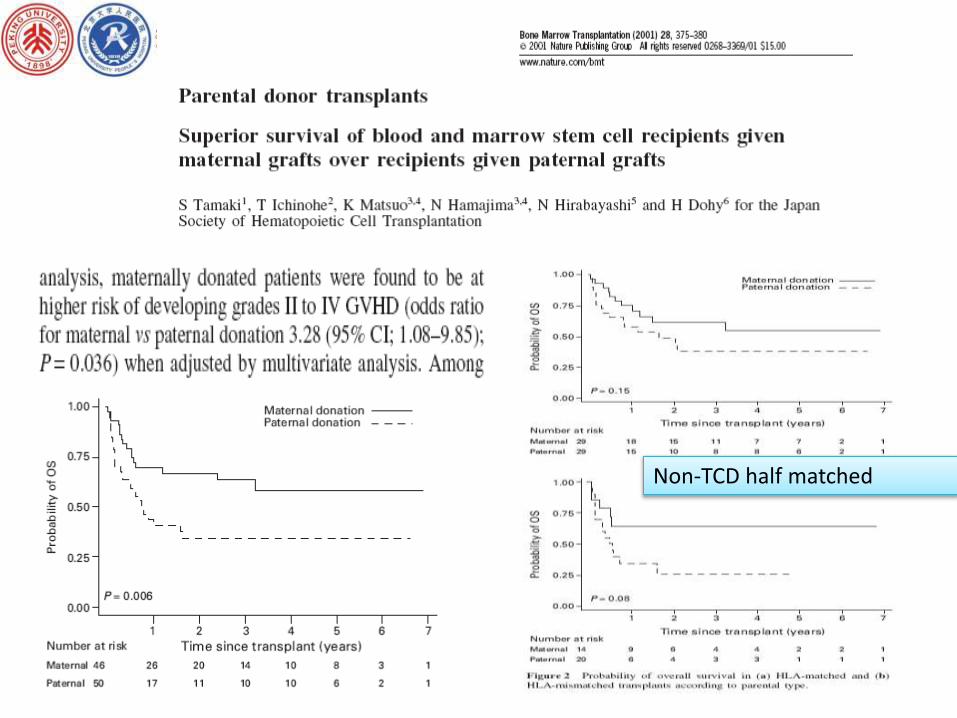
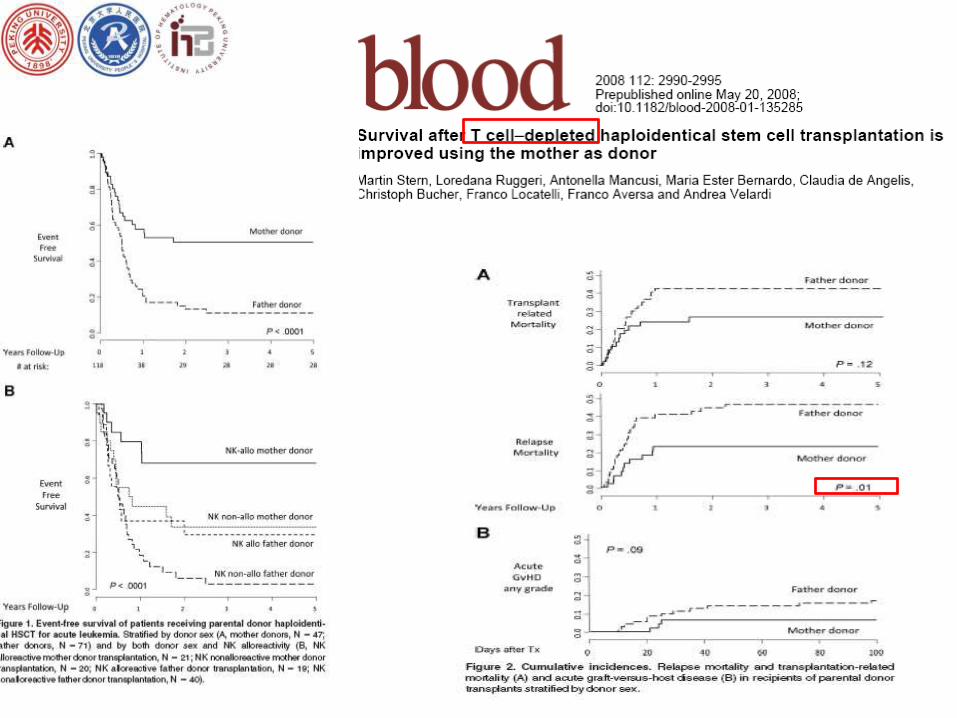
Father vs. Mother
vs. NIMA vs. NIPA
ResultsMultivariate &conclusion 5
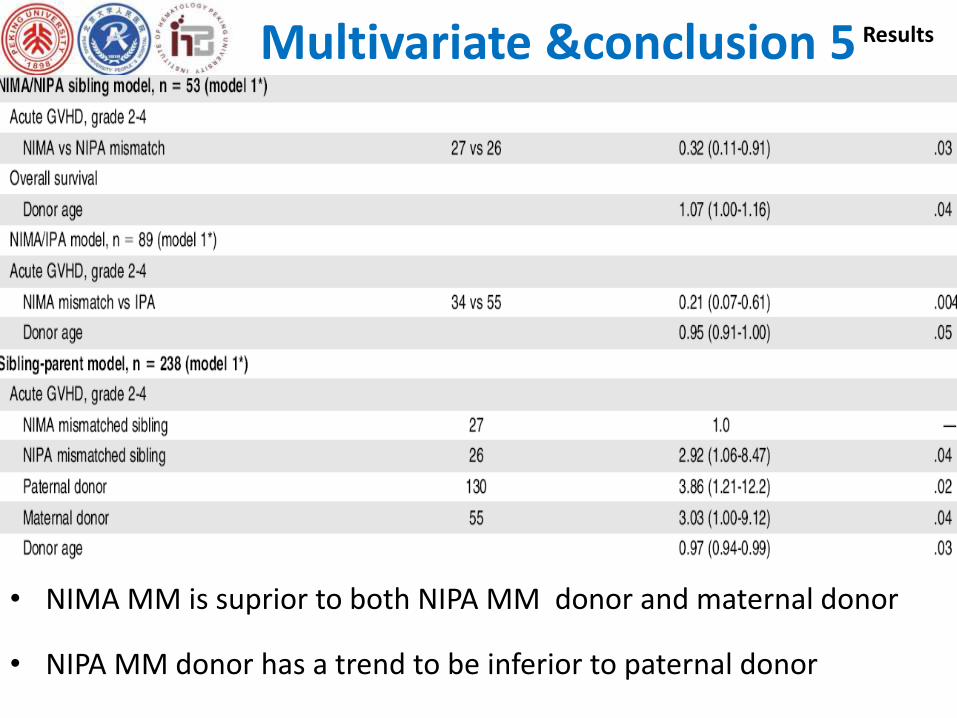
• NIMA MM is suprior to both NIPA MM donor and maternal donor
• NIPA MM donor has a trend to be inferior to paternal donor
Father & sibling
ResultsIBMTR NON-TCD
Father & sibling
Results
Non-TCD half matched
Father & sibling
Results
Father & sibling
Results
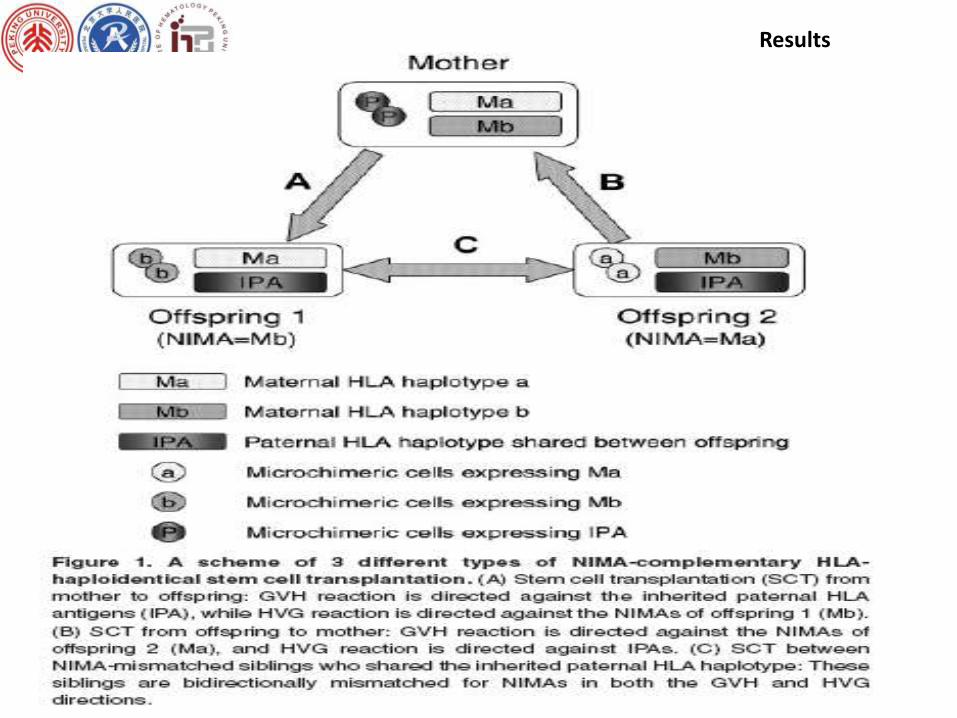
Mechanism
Unclear & complicated, possible:
• materno-fetal microchemerism result in either tolerance or immunity
depending on the immunologic maturity of the host and the
antigenic disparity
• partial tolerance to the paternal HLA antigens might be counteracted
by reactivity to paternal minor histocompatibility antigens (mHA)
• mother exposure to IPA may develop anti-HLA Ab towards paternal
HLA molecules
• allo-reactivity towards H-Y antigen in mother-to-son
• NK allo-reactivity
summary
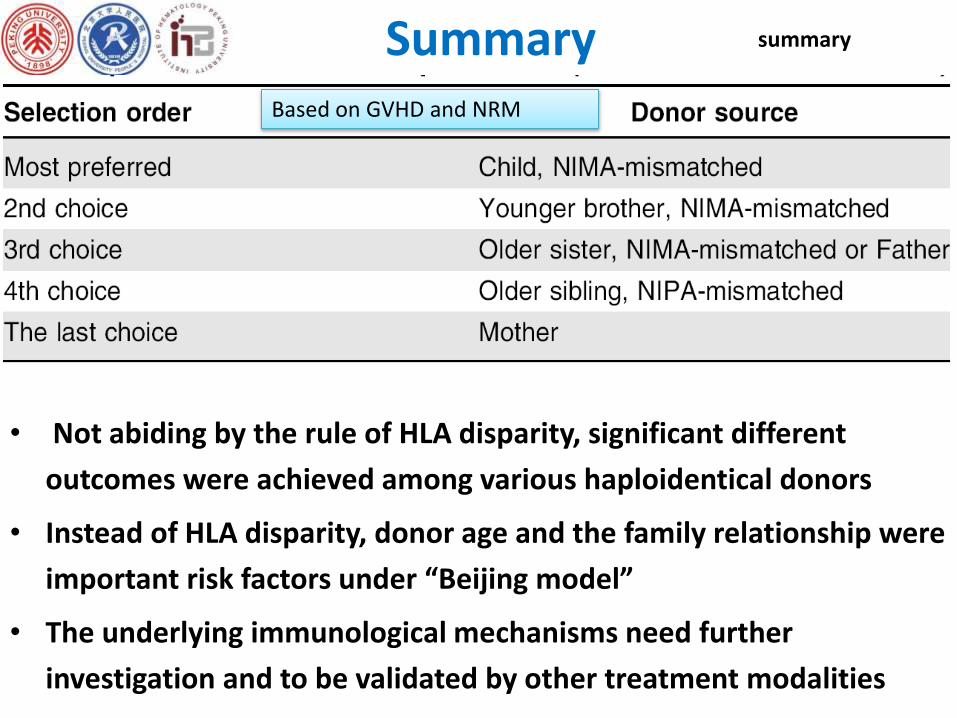
Summary
• Not abiding by the rule of HLA disparity, significant different
outcomes were achieved among various haploidentical donors
• Instead of HLA disparity, donor age and the family relationship were
important risk factors under “Beijing model”
• The underlying immunological mechanisms need further
investigation and to be validated by other treatment modalities
summary
Based on GVHD and NRM

Acknowledgements