diverticulosis, diverticulitis, ischemiccolitis...
TRANSCRIPT

Diverticulosis, diverticulitis,
Ischemic colitis. Irritable bowel
syndromesyndromeDr. Fuszek Péter Phd.
Semmelweis Egyetem Kútvölgyi Klinikai Tömb
2016-10-12

Case Riport • The 55-year-old female patient
(referred by a family doctor)
• History: serious illness is not known. Constipation since childhood.
• Complaints: left upper quadrant • Complaints: left upper quadrant abdominal pain, bloody stool, nausea, dysuria
• temperature: 38,3
• LAB:
• WBC: 14
• CRP: 15
• Urine: normal
UH: thickened sigmoid colonDg: Diverticulitis
Colon cancerHaemorrhoids, Colitis
?

Diverticulosis, diverticulitis
Diverticula are small, bulgingpouches that can form in largebowel. They are found most oftenin the lower part of the largeintestine (colon). Diverticula arecommon, especially after age 40,and seldom cause problems.
Sometimes, however,one or more of thepouches becomeinflamed or infected.That condition isknown as diverticulitis
Epidemiology
The incidence of diverticular disease has increased over the pastcentury. Autopsy studies fromthe early part of the 20th centuryreported colonic diverticula rates of 2% to 10%. This has increaseddramatically over the years. More recent data suggest that up to 50% ofindividuals older than 60 yearsof agehavecolonic diverticula, withindividuals older than 60 yearsof agehavecolonic diverticula, with10% to 25% developing complications such as diverticulitis.Hospitalizations for diverticular disease have also been on the rise.According to an American study evaluating hospitalization ratesbetween 1998 and 2005, rates of admission for diverticular diseaseincreased by 26% during the eight-year study period. Similar trendshave been observed in Canadian and European data over the same timeperiod .
Can J Gastroenterol. 2011 Jul; 25(7): 385–389.

PatogenesisDiverticula are small mucosal herniationsprotruding through the intestinal layers and thesmooth muscle along the natural openingscreated by the vasa recta or nutrient vessels inthe wall of the colon. True diverticulae containall layersof the gastrointestinalwall (mucosa,all layersof the gastrointestinalwall (mucosa,muscularis propria, and adventitia) (eg, Meckeldiverticulum). False diverticulae, or pseudo-diverticulae do not contain the muscular layersor adventitia, and they only involve thesubmucosa and mucosa. The sigmoid colon hasthe highest intraluminal pressures and is mostcommonly affected.

Patogenesis
• The reasonfor diverticula:
• The pathophysiology of diverticular disease is complex andrelates toabnormal colonic motility, changes in the colonic wall, chronic mucosallow-gradeinflammation, imbalancein colonic microflora and viscerallow-gradeinflammation, imbalancein colonic microflora and visceralhypersensitivity. Moreover, there can be genetic factors involved in thedevelopment of colonic diverticula.
• The weakening of the intestinal wall: (Ehlers-Danlos sy, Marfan sy,scleroderma)
• Increased pressure of the bowel wall (manometry demonstrated)..
• Low fiber meal + lack of physical activity is crucial to the role.
•Whiteway J, Morson DC.Elastosis in diverticular disease of the colon.Gut 1985;26:258-66.•Burkitt DP, Walker AR, et al.Effect of dietary fibre on stools and transit times, and its roles in causatios of disease.Lancet 1972;2:1408-12.•Wess L, Eastwood MA, et al.Collagen alteration in animal model of colonic diverticulosis.Gut 1996;8:701-6.

Complicated diverticulitis:Up to 25% of patients with acutediverticulitis develop complicated disease.This includes abscess formation, fistulas,strictures/obstruction and perforation.Abscess occurs with the perforation of adiverticulum that is usually contained. Smallabscesses (smaller than 3 cm) can often betreated with antibiotics alone. Larger
Clinical grounds
Uncomplicated diverticulitis:treated with antibiotics alone. Largerabscesses (larger than 4 cm) may requirecomputed tomography-guided percutaneousdrainage followed by eventual surgery afterresolution of the abscess. Perforatingdiverticular disease may also lead to fistula,with the most common locations beingcolovesicular and colovaginal. Fistulacomplications require surgical management.
Diverticulitis without anysignificant complications accountsfor more than 75% of cases. Thesepatients typically present with leftlower quadrant pain, fever andleukocytosis.
Serologic markers predict histoligical damage in acute diverticulitisJ Clin Gastroenterol 2010: 44(10): 702-6 02December 2010

The signs and symptoms of diverticulitis• Pain is usually felt in the lower left side of the abdomen: 93–100%.• Fever: > 50%.• Leukocytosis: 75% .• N/V, diarrhea, dysuria, haematochezia.• Physical examination:local tenderness, or tactile resistance, peritoneal
signsof excitementcanbeexperienced.signsof excitementcanbeexperienced.• Rectal examination: tenderness, palpable resistance when the
existence of an abscess.• Differential diagnosis: IBS, CRC, IBD, intestinal obstruction,
appendicitis.• Gynaecological disorders - ovarian cyst rupture, ovarian torsion,
ectopic pregnancy, pelvic inflammatory disease.• Urological diseases.• The elderly population: ischemic colitis.

Diagnosis• The diagnosis of acute diverticulitis can usually be made on the basis of history and
physical examination. Laboratory tests may be of help when the diagnosis is inquestion. A hemogram may reveal leukocytosis and a left shift, indicating infection.However, the absence of leukocytosis does not rule out diverticulitis, as 20-40% ofpatients have a normal white blood cell count. Liver tests and lipase, urine test,pregnancy test may help to exclude other causes of abdominal pain
• Endoscopyis not recommended in the acute settinggiven the risk of worseningdiverticulitis andbowel perforation. After the diverticulitis hassubsided,colonoscopydiverticulitis andbowel perforation. After the diverticulitis hassubsided,colonoscopycan be used to evaluate the extent of diverticulosis or to rule out a malignancymasquerading as a benign postinflammatory stricture.
• Contrast enemais not the imaging modality of choice during an acute episode ofabdominal pain and should only be considered in mild-to-moderate uncomplicatedcases of diverticulitis when the diagnosis is in doubt.
• The diagnosis of diverticulitiscan be made on clinical grounds, but a computedtomography (CT)scan of the abdomen is considered the best imaging method toconfirm the diagnosis. The American College of Radiology (ACR) 2008Appropriateness Criteria for left lower quadrant pain support this recommendationbecause of the specificity and sensitivity of CT scans, which allow for the diagnosis ofcauses of left lower quadrant pain that resembles diverticulitis.

Diagnosis
Medical treatments of diverticulosis• Uncomplicated (no symptoms): It does not require
treatment.
• Recommend: high fiber diet (cellulóz, hemicellulóz,pektinek). Avoid small seed food: (strawberry, raspberry,pappy seed)
• + it shouldbeemphasizedamplefluid intakeaswell.• + it shouldbeemphasizedamplefluid intakeaswell.
• Uncomplicated (with symtoms)The use of non-absorbableantibiotics (Rifamixin) is the mainstay of therapy in patientswith mild to moderate symptoms,
Marlett J, McBurney M, et al.Position of the American Dietetic Assotiation: health implications of dietary fiber.J Am DietAssoc 2002;102:993-1000.Latella G, Pimpo MT, et al. Rifamixin improves symptoms os acquired uncomplicated diverticular disease of the colon. Int JColorectal Dis 2003;18:55-62

Medical treatment of diverticulosis• Uncomplicated diverticulitis: (most patients (94 percent) can be
treated on an outpatient) The decision to hospitalize a patient withuncomplicated diverticulitis depends on several factors, including thepatient's ability to tolerate oral intake, severity of illness,comorbidities, and outpatient support systems.
• Recommended: liquid, fiber-free diet +antibiotics
• Elective resectionof the involved bowel segmentafter 2-3 episodes• Elective resectionof the involved bowel segmentafter 2-3 episodesof uncomplicated diverticulitis to prevent further attacks isgenerally recommended by consensus guidelines.
• In case of acute diverticulitis (immunocompromised patients) muchgreater possibility of complications, so afterthe first diverticulitis isrecommended for elective surgery.
Perkins JD, Shield CF, Chang FC, et al. Acute diverticulitis: Comparison of treatment in immuncompromised and non-immuncompromised patients. Am J Surg 1984;148:745-8.Colorectal Dis 2010: 12(10): e278–e28230 September 2010Int J Colorectal Dis. 2010 Jun;25(6):751-9. Epub 2010 Feb 6. Prospective randomized trial comparing
short-term antibiotic therapy versus standard therapy for acute uncomplicated sigmoid diverticulitis.
Schug-Pass C, Geers P, Hügel O, Lippert H, Köckerling F.

Uncomplicated diverticulitis
• Trimethoprim/sulfamethoxazole :DS, 160/800 mg orally every 12 hoursorevery 12 hoursor
• Ciprofloxacin (Cipro), 750 mg orally every 12 hours, • Levofloxacin (Levaquin), 750 mg orally every 24 hours,+
+ Metronidazole(Flagyl), 500 mg orally every six hours• Amoxicillin/clavulanateextended release (Augmentin XR),
two 1,000/62.5-mg tablets orally every 12 hoursor• Moxifloxacin (Avelox), 400 mg orally every 24 hours

DiverticulitisHospitalization should be considered if patients have signs of
peritonitis or there is suspicion of complicated diverticulitis.
Inpatient management includes no food or drink by mouth,
intravenous fluid resuscitation (normal saline or lactated Ringer
Perkins JD, Shield CF, Chang FC, et al. Acute diverticulitis: Comparison of treatment in immuncompromised andnon-immuncompromised patients. Am J Surg 1984;148:745-8.Colorectal Dis 2010: 12(10): e278–e28230 September 2010
solution), and intravenous antibiotics.
Clinical improvement is expected within two to four days and
includes decreasing fever, leukocytosis, and pain.
Fifteen to 30 percent of patients admitted with acute diverticulitis
require surgicalintervention during that admission.

Patients with a localized abscess
• Patients with a localized abscess maybe candidates for CT-guidedpercutaneous drainage, a procedure thatdoes not increase the risk of recurrentdiverticulitis.diverticulitis.
• Patients at increased risk of colonicperforation includeimmunocompromised patients andpatients taking nonsteroidal anti-inflammatory drugs, corticosteroids, orchronic opioid analgesics.

Can J Gastroenterol. 2011 Jul; 25(7): 385–389.

Diverticular colitis
• Diverticular colitis is the termused to describe a particular pattern ofactive chronic inflammation in the sigmoid colon affected bydiverticular disease.
• The pathogenesis remains uncertain but is almost certainlymultifactorial.
• Symptomsandendoscopicfindingsarediverse.• Symptomsandendoscopicfindingsarediverse.
• Histologically, the disease closely mimicking chronic inflammatorybowel disease, especially ulcerative colitis, butit is not IBD .
• Diverticular colitis may respond well to treatment similar to that usedfor chronic inflammatory bowel disease.
Evens LP, Cooper J, et al. Diverticular colitis – therapeutic and aetiological consideration. Colorectal disease 2002;5:208-12.Ludemann L, Stepherd NA. What is diverticular colitis? Pathology 2002;34(6):568-72
Case riport 2 • A 75-year-old woman comes to the
office because of a 1 day hystoryand abdominal pain.
• Past Hx: not serious illness
• Havy smoker. She has constipationsince childhood.
• Complaints: suddenly developed• Complaints: suddenly developedumbilical crampy abdominal pain,nausea, haematochezia urgent.
• Fever: 37,9
• LAB:
• Leukocytosis: 11, CRP: 10
• LDH: 500, pH: 7,2
UH: normal ? Colono, angio CT angio. Dx: ??


Epidemiology
• The exact incidence of ischemic colitis isdifficult to estimate, as many patients withmild ischemia may not seek medical attention.Ischemiccolitis is responsiblefor about 1 inIschemiccolitis is responsiblefor about 1 in2000 hospital admissions, and is seen on about1 in 100 endoscopies.
• Men and women are affected equally; ischemiccolitis is a disease of the elderly, with morethan 90% of cases occurring in people over theage of 60.

Ischemic colitis• Colonic blood supply.
• Pink - supply from superiormesenteric artery (SMA) and itsbranches: middle colic, right colic,ileocolic arteries.
• Blue - supply from inferior• Blue - supply from inferiormesenteric artery (IMA) and itsbranches: left colic, sigmoid,superior rectal artery.
• 7 is for so-called Cannon-Böhmpoint (the border between the areasof SMA and IMA supplies), whichlies at the splenic flexure
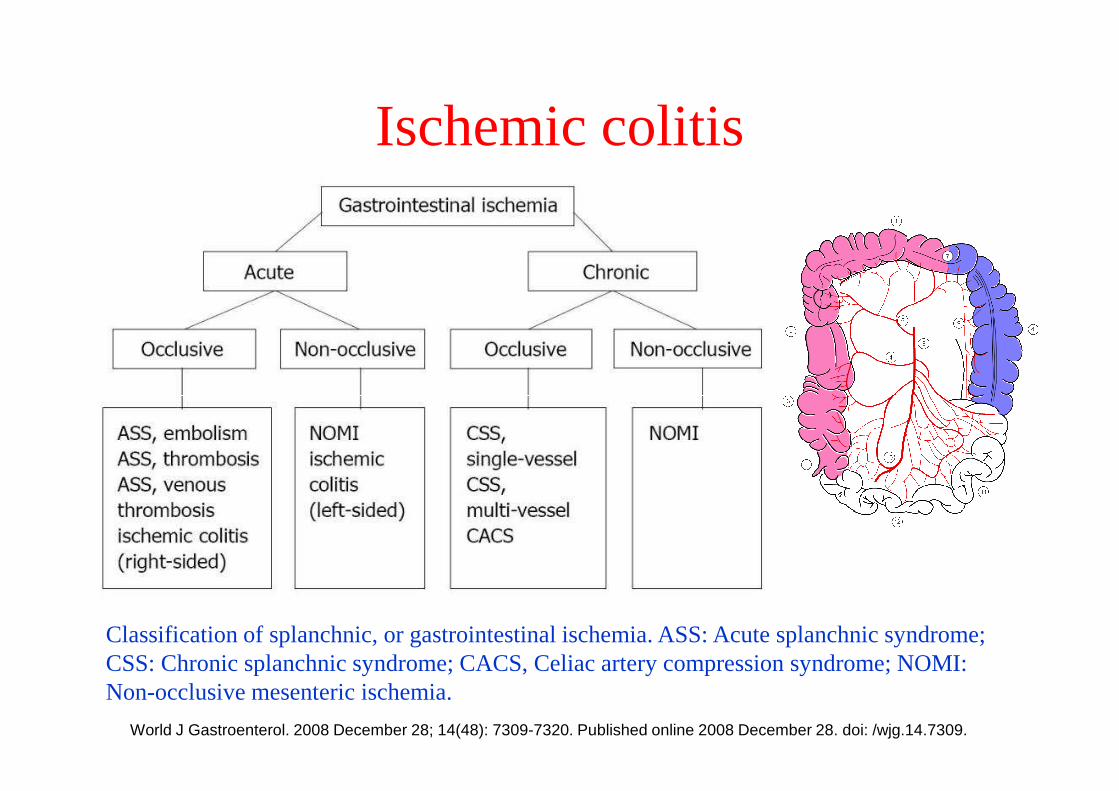
Ischemic colitis
Classification of splanchnic, or gastrointestinal ischemia. ASS: Acute splanchnic syndrome; CSS: Chronic splanchnic syndrome; CACS, Celiac artery compression syndrome; NOMI: Non-occlusive mesenteric ischemia.
World J Gastroenterol. 2008 December 28; 14(48): 7309-7320. Published online 2008 December 28. doi: /wjg.14.7309.

Diagnostic approach• Clinicians must maintain a high index of suspicion for ischaemic
bowel disease,because the signs and symptoms are relatively non-
specific yet the condition has significant morbidity and mortality.
Early recognition, appropriate diagnostic studies, and
aggressivetreatment are necessaryto improve outcome.aggressivetreatment are necessaryto improve outcome.
• In the absence of highly specific or definitive signs and symptoms,
a history and physical examination alone are generally not
sufficient to make the diagnosis; usually some formof imaging is
required. However, when fulminant ischaemic bowel disease is
present, extensive diagnostic testing may not be appropriate in
order that surgical intervention can proceed without delay.

Gross specimen of dead bowel.


Management• Patients with chronic mesenteric ischemia have traditionally
been treated with mesenteric vascular surgicalrevascularization.
• Overall, the operative mortality remains high (approximately7.5%–10%).
• There are several surgical revascularization strategies,• There are several surgical revascularization strategies,including visceral endarterectomy, antegrade supraceliac aortato visceral bypass, and retrograde infrarenal aorta to visceralbypass.
• Before surgical revascularization, the patient may benefit fromtotal parenteral nutrition (TPN).

Management Angioplasty and stenting
• Angioplasty is technically difficult because of the anatomy ofthe SMA.
• Mesenteric angioplasty has a good technical success rate but ahigh rate of restenosis, (restenosis rates are 20-50%. ) androutine stenting is recommended.
Successful endovascularstenting of superiormesenteric artery stenosisfor chronic mesentericischemia. (a) Pre-stenting; (b) Post-stenting. (Figure courtesyof Deepak L Bhatt, MD.)
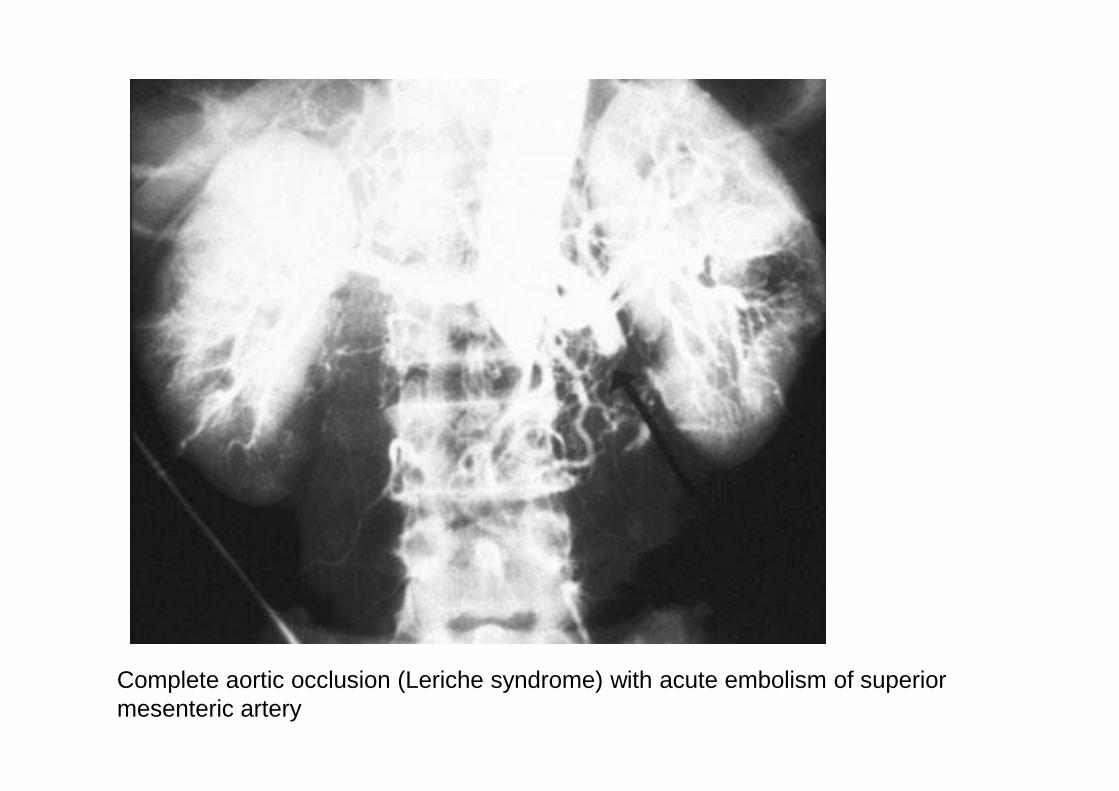
Complete aortic occlusion (Leriche syndrome) with acute embolism of superior mesenteric artery





Prognosis
• Most patients with ischemic colitis recover fully, although theprognosis depends on the severity of the ischemia. Patientswith pre-existing peripheral vascular disease or ischemia of theascending (right) colon may be at increased risk forcomplicationsor death.complicationsor death.
• Non-gangrenous ischemic colitis, which comprises the vastmajority of cases, is associated with a mortality rate ofapproximately 6%. However, the minority of patients whodevelop gangrene as a result of colonic ischemia have amortality rate of 50-75% with surgical treatment; the mortalityrate is almost 100% without surgical intervention.

Case Riport 3• 35-year-old female patient,• History: illness was not
serious. (Smokers),Constipation and abdominalpain often since childhood.
• Complaints: suddenumbilical• Complaints: suddenumbilicalcrampy abdominal pain (aftereating), nausea. She will bebetter after a bowelmovement.
• Fever: 36,3• LAB: • Leukocytosis: 8 , CRP: 3• LDH: 15, pH: 7,4
UH: normal, colono: neg, Gynecologyst: neg, Stool culture: negDx:??
Irritable bowelsyndrome(IBS)syndrome(IBS)

Irritable bowel syndrome(Classification)
• IBS is a chronic functional disorder of the gastrointestinalsystem. Patients experience abdominal pain and altered bowelhabit, with either predominantly:
• Symptoms:
• (IBS-D) diarrhea Mild• (IBS-C) constipation
• (IBS-M) or both
• There is nodefinitive investigationasno biomarkerhas beenfound, so IBS is diagnosed clinically.
• Monoclonal Anti-Vinculin antibody A Serologic Test for Irritable Bowel
Syndrome????
MildModerateSerious

Epidemiology• IBS disease of primarily young women.
(Female / male = 2/1, 4/1)
• The visit to the doctor on femalepredominanceof the diseasethe real one ispredominanceof the diseasethe real one iseven more significant - and often easier forwomen to seek medical advice, (female / maleratio = 2/1).
• Studies showthat women are 20% of men atsome point in life has 12% of the symptomscaused by irritable syndrome.

Worldwide prevalence of irritable bowel syndrome, as reported by country
Clin Epidemiol. 2014; 6: 71–80. Published online 2014 Feb 4. doi : 10.2147/CLEP.S40245

Irritable bowel syndrome frequency in different countries

The causes of IBS

The causes of IBS • While the causes of IBS are still unknown, it is believed thatthe entire gut–brain
axis is affected.
• Post-infectious:The risk of developing IBS increases six-fold afteracute gastrointestinal infection. (IBS-PI) „postinfectious IBS„ (Insome individuals, IBS may have an acute onset and develop after aninfectious illness characterized by two or more of: fever, vomiting,diarrhea,or positivestoolculture.)diarrhea,or positivestoolculture.)
• Stress: childhood physical and psychological abuse is oftenassociated with the development of IBS
• Bacteria, Fungus, ProtozoaSmall intestinal bacterial overgrowthoccurs with greater frequency in patients who have been diagnosedwith IBS compared to healthy controls. (SIBO)
• Genetic, environmental, and psychologicalfactors seemto beimportant in the development of IBS.

Monoclonal Anti-Vinculin antibody A Serologic Test for Irritable Bowel Syndrome
Measurement of anti-vinculin antibodies in serumdemonstrated higher levels of these autoantibodies in IBSpatients, compared with those without the disorder, withpositive predictive values between 90% and 100% dependingon the cutoff values used, reportedMark Pimentel, MD, ofCedars-SinaiMedicalCenterin LosAngeles,andcolleagues.Cedars-SinaiMedicalCenterin LosAngeles,andcolleagues.
Novel Research Suggests Efficacy of Diagnostic Blood Test for IrritableBowel Syndrome(IBS); Psychological Factors Like Anxiety, Depression May be Central Drivers of IBSRather than Inflammation 2013- SanDiegoAmerican College of Gastroenterology (ACG)
Vinculin is a cell migration and adherence protein foundpredominantly onnerves and epithelium. A series of studiesleading up to this result suggests that acute gastroenteritiscauses antibodies to be formed to vinculin and is associatedwith IBS development.
IBS, possibly of the post-infectious type
higher levels of plasma IL-6
“cytoskeletal protein”,
Vinculin

One cause of IBS is having a previous gut infection which oftentriggers small intestinal bacterial overgrowth (SIBO).The idea behind this study is that a bacterial toxin called cytolethaldistending toxin B (CdtB) produced by gramnegativeProteobacteria (such as Shigella sp. and E. coli), triggersgastroenteritis by molecular mimicry which stimulates auto-antibodiesto vinculin. This processmay be involved eventual
Could IBS be an autoimmune condition?
antibodiesto vinculin. This processmay be involved eventualdevelopment of IBS, though the details of howthis happens are farfrom clear. Studying antibody titers to vinculin in IBS patients canestablish the role of gastroenteritis in IBS and help determine theextent to which autoimmune processes are involved.
Posted onFebruary 19, 2014by Norm Robillard
J Cell Biol. 2006 Nov 6;175(3):465-75. Shigella applies
molecular mimicry to subvert vinculin and invade host cells.
Izard T1, Tran Van Nhieu G, Bois PR.

It is believed that the entire gut–brain axis is affected
Dr. Papp János (IBS-2000)

Altered sensation

Altered motility

The pressure conditions of the colon in healthy humans/ IBS patients

The GastrocolicReflex & Irritable Bowel Syndrome

Diagnosis of IBS: Rome III (2006)
Irritable bowel syndrome has been a diagnosis of exclusion, to help this process, researchers have developed of diagnostic criteria for IBS.(Rome diagnostic criteria):
At least 3 days per month in past 12 weeks of continuous or recurrent abdominal pain or discomfort.abdominal pain or discomfort.
With at least 2 of the following:
-Relief with defecation-Altered stool frequency-Altered stool form
Onset of symptoms more than 6 months before diagnosis.

Diagnosis of IBS• (Romediagnosticcriteria)
• Except
• Some red flag signs and symptoms that suggest need foradditional tests:additional tests:
• New onset, after age 50, weight loss, rectal bleeding, fever,nausea or recurrent vomiting, abdominal pain, especially ifit's not completely relieved by a bowel movement, oroccurs at night, diarrhea that is persistent or awakens youfrom sleep, anemia related to lowiron.

Differential diagnosis

Treatments and drugs
TREATMENTS
Because it's not clear what causes irritable bowel syndrome, treatment
focuses on the relief of symptoms. (Symptom-oriented treatment)
In most cases, you can successfully control mild signs and symptoms
of irritable bowel syndrome by learning to manage stress and making
changes in your diet and lifestyle. Try to avoid foods that trigger your
symptoms. Also try to get enough exercise, drink plenty of fluids and
get enough sleep.

Diet
• Dietary changes:
• Eliminating high-gas foods: especiallycabbage, broccoli and cauliflower — and rawfruits.fruits.
• Eliminating gluten:
• Eliminating FODMAPs: (fermentable oligo-,di-, and monosaccharides and polyols).FODMAPs are found in certain grains,vegetables, fruits and dairy products.

Symptom-oriented treatmentSymptom-oriented treatment
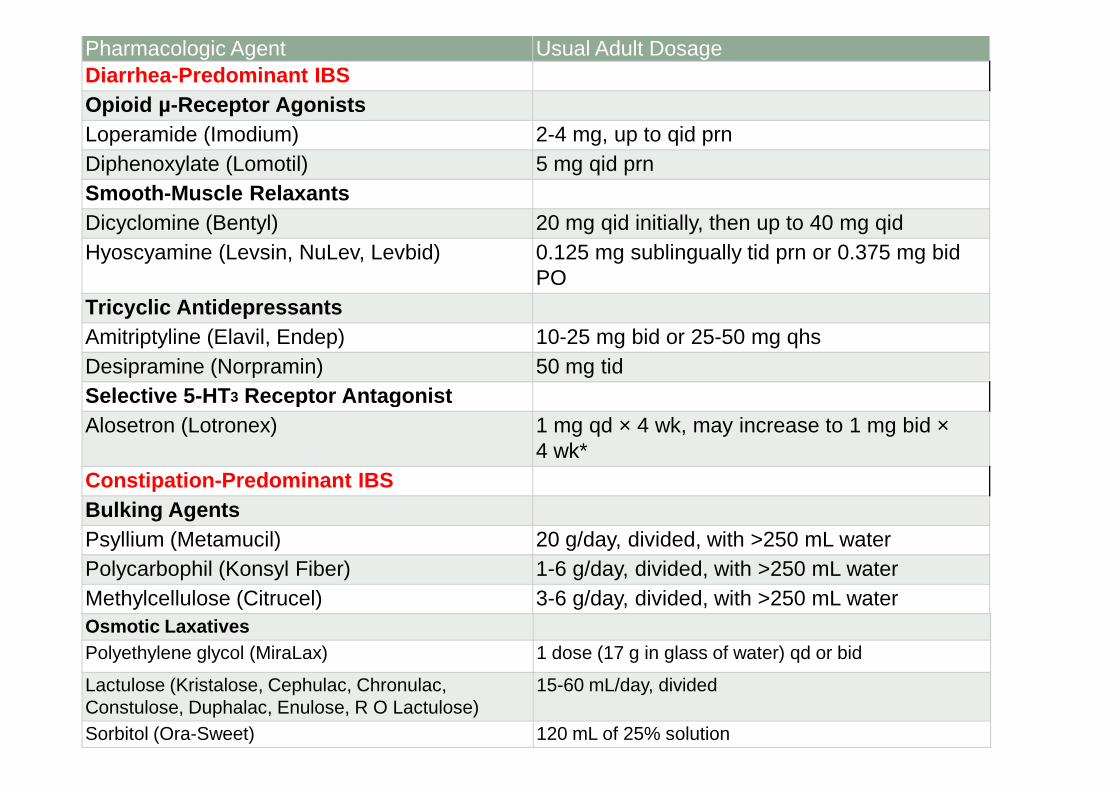
Pharmacologic Agent Usual Adult DosageDiarrhea-Predominant IBSOpioid µ-Receptor AgonistsLoperamide (Imodium) 2-4 mg, up to qid prnDiphenoxylate (Lomotil) 5 mg qid prnSmooth-Muscle RelaxantsDicyclomine (Bentyl) 20 mg qid initially, then up to 40 mg qidHyoscyamine (Levsin, NuLev, Levbid) 0.125 mg sublingually tid prn or 0.375 mg bid
POTricyclic AntidepressantsAmitriptyline (Elavil, Endep) 10-25 mg bid or 25-50 mg qhsDesipramine (Norpramin) 50 mg tidSelective 5-HT3 Receptor AntagonistSelective 5-HT3 Receptor AntagonistAlosetron (Lotronex) 1 mg qd × 4 wk, may increase to 1 mg bid ×
4 wk*Constipation-Predominant IBSBulking AgentsPsyllium (Metamucil) 20 g/day, divided, with >250 mL waterPolycarbophil (Konsyl Fiber) 1-6 g/day, divided, with >250 mL waterMethylcellulose (Citrucel) 3-6 g/day, divided, with >250 mL waterOsmotic LaxativesPolyethylene glycol (MiraLax) 1 dose (17 g in glass of water) qd or bid
Lactulose (Kristalose, Cephulac, Chronulac, Constulose, Duphalac, Enulose, R O Lactulose)
15-60 mL/day, divided
Sorbitol (Ora-Sweet) 120 mL of 25% solution

Pain
Smooth-muscle relaxants
Dicyclomine (Bentyl) 20 mg qid initially, then up to 40 mg qid
Hyoscamine (Levsin, NuLev, Levbid) 0.125 mg sublingually tid prn or 0.375 mg bid PO
Pharmacologic Agent Usual Adult Dosage
bid PO
Tricyclic Antidepressants
Amitriptyline (Elavil, Paregoric) 10-25 mg bid or 25-50 mg qhs
Desipramine (Norpramin) 50 mg tid

Treatment of IBS
Psychological factorsPsychological factors

• You have to explain that the complaint doesnot depend on the quality of food consumed,butalsocausesthemealitself.butalsocausesthemealitself.
• The symptoms due to non-normal gastrocolicreflex occurred.

The hypnotic effect of the colon pressure

Thank you for your attention!Thank you for your attention!