discontinuation of primary and secondary prophylaxis for opportunistic infections in hiv-infected...
TRANSCRIPT
CLINICAL AND EPIDEMIOLOGIC RESEARCH
Discontinuation of Primary and Secondary Prophylaxisfor Opportunistic Infections in HIV-Infected Patients
Who Had CD4 + Cell Count < 200 cells/mm3
But Undetectable Plasma HIV-1 RNA:An Open-Label Randomized Controlled Trial
Romanee Chaiwarith, MD,1 Jutarat Praparattanapan, PhD,1 Nontakan Nuntachit, MD,1
Wilai Kotarathitithum, BS,1 and Khuanchai Supparatpinyo, MD1,2
Abstract
The CDC recommends discontinuing opportunistic infections (OIs) prophylaxis in HIV-infected patients whohave CD4 + cell count > 200 cells/mm3 after receiving combination antiretroviral therapy (cART). A prospectiverandomized controlled trial was conducted at Chiang Mai University Hospital from June 1, 2009 to January 31,2012 in 74 adult HIV-infected patients who had received cART and had CD4 + cell count < 200 cells/mm3 butplasma HIV-1 RNA < 50 copies/ml. Forty-three patients (58.1%) were male and the mean age was 41.8 – 8.1years; 68 (91.9%) and 59 (79.7%) patients were receiving co-trimoxazole and antifungal prophylaxis, respectively.The median CD4 + cell counts at enrollment were 142 (IQR 108, 161) and 158 (IQR 141, 176) cells/mm3 amongpatients who discontinued and continued OIs prophylaxis, respectively (p value = 0.041). One of 37 patients(2.7%) in the discontinuation group developed Pneumocystis jiroveci pneumonia, giving the incidence rate of1.57/1000 person-months. None of the 37 patients in the continuation group developed OIs. The difference in theprevention rates of OIs between groups was - 2.7% (95% CI - 7.9, 2.5). In conclusion, in the setting whereplasma HIV-RNA measurement is available, e.g., Asia-Pacific region, discontinuation of prophylaxis is con-siderably safe in HIV-infected patients receiving cART with undetectable plasma HIV-RNA but incompleteimmune recovery.
Introduction
Currently, combination antiretroviral therapy
(cART) has become the standard of care in the treatmentof HIV infection in many parts of the world. The benefits ofcART as a result of CD4 + cell recovery and suppression ofHIV-1 replication have been reported worldwide, includingThailand.1–3 The National Institutes of Health (NIH), theCenters for Disease Control and Prevention (CDC), and theHIV Medicine Association of the Infectious Diseases Societyof America (HIVMA/IDSA) recommend discontinuing pri-mary and secondary prophylaxis for opportunistic infections(OIs) in HIV-infected adults and adolescents receiving cART,when the CD4 + cell count increases to a certain level for acertain period of time; for instance, prophylaxis for Pneumo-cystis pneumonia (PCP) can be discontinued when the CD4 +
cell count is ‡ 200 cells/mm3 for at least 3 months.4 Severalstudies confirmed that the risk of developing or recurrence ofPCP in these patients was very low, ranging from 0 to 1.9/100person-years for primary prophylaxis,5–12 and 0 to 1.96/100person-years for secondary prophylaxis.9,12–15 However,there may be some patients with incomplete immune recov-ery after receiving an effective cART and, following currentguidelines, may need an indefinite OI prophylaxis. Recently,an observational study reported a low incidence rate of PCPafter discontinuation of prophylaxis among patients who hadCD4 + cell count < 200 cells/mm3 but undetectable plasmaHIV-1 RNA.16 If the discontinuation of OI prophylaxis inpatients with incomplete CD4 + cell recovery is safe, it maylead to reduction of pill burden, drug–drug interactions, anddrug adverse events. This prospective randomized con-trolled study aimed to determine the safety of
1Department of Medicine, Faculty of Medicine, and 2Research Institutes for Health Sciences, Chiang Mai University, Chiang Mai, Thailand.
AIDS PATIENT CARE and STDsVolume 27, Number 2, 2013ª Mary Ann Liebert, Inc.DOI: 10/1089/apc.2012.0303
71

discontinuation of primary or secondary prophylaxis for OIsamong HIV-infected adult patients who had received cARTand had undetectable plasma HIV-1 RNA, but unable toachieve CD4 + cell count ‡ 200 cells/mm3.
Materials and Methods
Study design and participants
A prospective randomized controlled trial was conductedamong HIV-infected patients attending the outpatient HIVClinic, Chiang Mai University Hospital, a 1500-bed, tertiary-care Hospital in Northern Thailand, between June 1, 2009and January 31, 2012. All patients who had documented HIVinfection and met the following criteria were included:(1) age ‡ 18 years old, (2) receiving cART, (3) CD4 + cellcount < 200 cells/mm3, (4) plasma HIV-1 RNA < 50 copies/mLfor at least 6 months, (5) receiving primary or secondaryprophylaxis for OIs caused by Pneumocystis jiroveci, Crypto-coccus neoformans, Penicillium marneffei, Histoplasma capsula-tum, Toxoplasma gondii, or Mycobacterium avium complex(MAC), and 6) able to give a written informed consent. Thepatients were excluded if they were pregnant.
Randomization and masking
JP prepared a list for randomization to either discontinue orcontinue primary or secondary prophylaxis in a 1:1 ratio witha block size of 6. Randomization was not stratified by anycharacteristics. Participants, investigators, and statisticianwere not masked to treatment allocation.
Procedures
Eligible and consenting patients were enrolled and random-ized to either discontinue or continue primary or secondaryprophylaxis. Patients were followed up at least every 6 monthsand were censored when they met one of the following criteria:(1) died, (2) developed any of the following OIs: PCP, cerebraltoxoplasmosis, disseminated MAC, disseminated penicilliosismarneffei, disseminated histoplasmosis, and cryptococcal men-ingitis, (3) discontinued primary OI prophylaxis when theirCD4 + cell counts were ‡ 200 cells/mm3 for ‡ 3 months or dis-continued secondary OI prophylaxis when their CD4 + cellcounts were ‡ 100–200 cells/mm3 for ‡ 3–6 months, or (4) whenthe last enrolled patient reached 1 year of follow-up.
Primary endpoint was incidence of patients who died ordeveloped any of the following OIs: PCP, cerebral toxoplas-mosis, disseminated MAC infection, disseminated penicilliosismarneffei, disseminated histoplasmosis, and cryptococcalmeningitis.
Data collection included baseline characteristics (age, gen-der, mode of HIV transmission), clinical data (OIs prior tocART initiation, date of primary or secondary OIs prophy-laxis, OIs prophylaxis medication, date of cART initiation,cART regimen, CD4 + cell count before initiating cART andevery 6 months thereafter, and plasma HIV-1 RNA at 6months after cART and every 6–12 months thereafter), andoutcomes (death, date of death, occurrence of OIs after ran-domization, date of OIs occurrence after randomization).
cART was defined as a combination of a non-nucleosidereverse transcriptase inhibitor (NNRTI) or a protease inhibitor(PI) plus two nucleoside reverse transcriptase inhibitors(NRTI).
The study was approved by the Faculty of Medicine,Chiang Mai University Ethical Committee. This trial wasregistered with ClinicalTrials.gov number, NCT01392430.
Statistical analysis
The analysis was performed on an intention-to-treat basis.The comparisons of baseline characteristics between groupswere performed using Chi-square or Fisher’s exact test forcategorical data and Student’s t-test or Mann-Whitney U testfor continuous data. The incidence rate was calculated by thenumber of events over total person-months of follow-up.
Time to the occurrence of OIs was analyzed using Kaplan-Meier estimates and log rank tests. Cox proportional hazardmodels were used for estimation of hazard ratios (HRs) andconfidence intervals (CIs).
All statistical analyses were performed using Stata sta-tistical software version 10.0 (Stata Statistical Software: Re-lease 10.0, Stata Corporation, College Station, TX, 2007). All pvalues were two-sided. A level of significance of 0.05 wasused to guide interpretation of relationships throughout theanalysis.
Based on the previous studies,8,9,12,17–23 we estimated thatafter 1 year of follow-up the cumulative incidence of OIswould be 10% among patients who continued OIs prophy-laxis giving the assumption of 90% prevention rate of OIs inthis control group. The study was designed to demonstratethat the prevention rate of OIs in the discontinuation groupwas non-inferior to that in the continuation group with amargin of ten percent. A sample of 45 patients was required ineach group, to demonstrate the non-inferiority at the power of80% and the significance level of 5%.
Results
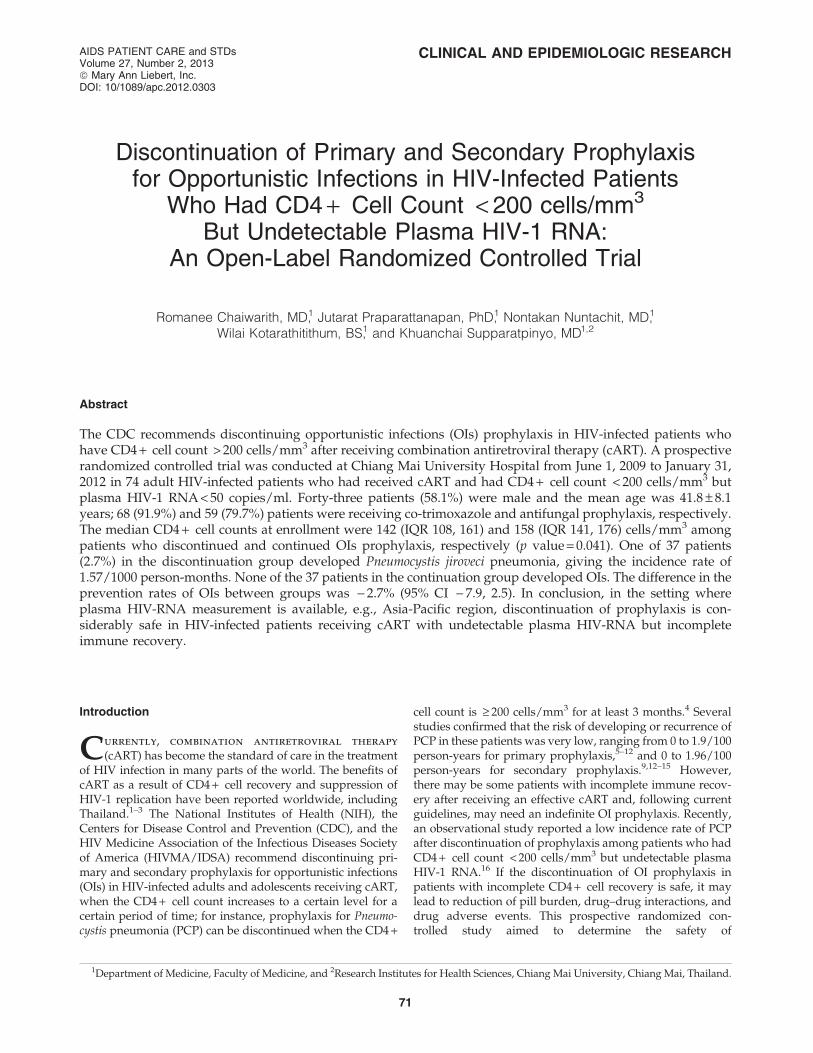
From June 1, 2009 to January 31, 2011, 74 HIV-infectedpatients attending the outpatient HIV Clinic at Chiang MaiUniversity Hospital who fulfilled the inclusion criteria wereenrolled to the study (Fig. 1). The enrollment rate was slowingdown through the end of study period due to the increase innumber of HIV-infected individuals who accessed to cART athigher CD4 + cell counts in the region. After the enrollment ofthe 74th participant on January 13, 2011, no participant wasenrolled during the 12-month period until January 2012. Thestudy team considered that it was unlikely to enroll additional16 participants to meet the enrollment target; therefore, thestudy team decided to end the study on January 31, 2012 dueto the futility reason. No patient died during the total follow-up of 1210.5 person-months and median duration of 16.6months. Twenty-eight patients discontinued primary OI pro-phylaxis when their CD4 + cell counts were ‡ 200 cells/mm3
for ‡ 3 months, and 29 discontinued secondary OI prophy-laxis when their CD4 + cell counts were ‡ 100–200 cells/mm3
for ‡ 3–6 months. Sixteen patients (7 in the discontinuationgroup and 9 in the continuation group) were followed up untilthe end of study period.
Baseline characteristics
Among the 74 patients enrolled to the study, 37 patientseach were randomly assigned to the discontinuation andcontinuation groups. Forty-three patients (58.1%) were maleand the mean age was 41.8 – 8.1years. Thirty-five patients
72 CHAIWARITH ET AL.
(47.3%) received primary prophylaxis. Thirty-nine patients(52.7%) received secondary prophylaxis: 20 patients for PCP,5 for penicilliosis marneffei, 5 for cryptococcal meningitis, 4for PCP and cryptococcal meningitis, 2 for histoplasmosis, 1for cerebral toxoplasmosis, 1 for PCP and penicilliosis mar-neffei, and 1 for PCP, cryptoccocal meningitis, and cerebraltoxoplasmosis. Sixty-eight patients (91.8%) received co-trimoxazole, 49 patients (66.2%) received fluconazole, 11patients (14.9%) received azithromycin, 10 patients (13.5%)
received itraconazole, and 9 patients (12.2%) received dap-sone. The median CD4 + cell counts at enrollment were 158(IQR 141, 176) and 142 (IQR 108, 161) cells/mm3 among dis-continuation and continuation groups, respectively. Thecomparisons of baseline characteristics between groups areshown in Table 1. Overall, the baseline characteristics weresimilar between groups, except the discontinuation group hadslightly but significantly lower CD4 + cell counts and shorterduration on cART at baseline.
FIG. 1. Flow chart of the study participants.
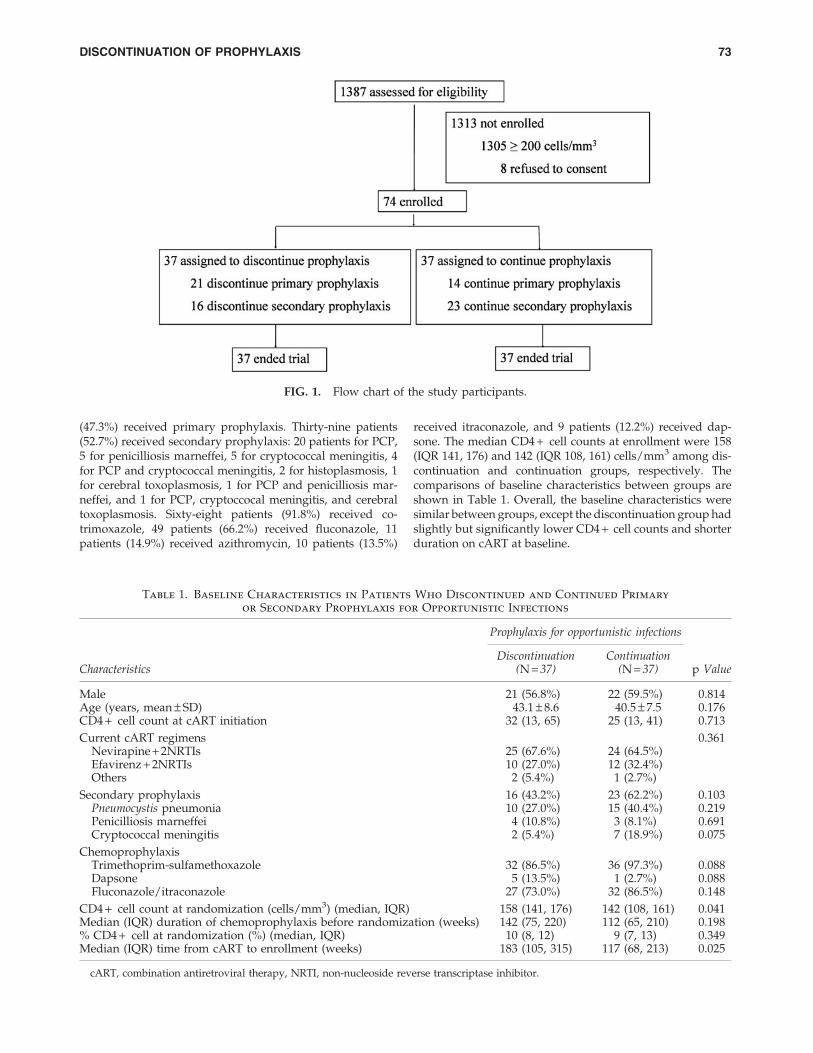
Table 1. Baseline Characteristics in Patients Who Discontinued and Continued Primary
or Secondary Prophylaxis for Opportunistic Infections
Prophylaxis for opportunistic infections
Discontinuation ContinuationCharacteristics (N = 37) (N = 37) p Value
Male 21 (56.8%) 22 (59.5%) 0.814Age (years, mean – SD) 43.1 – 8.6 40.5 – 7.5 0.176CD4 + cell count at cART initiation 32 (13, 65) 25 (13, 41) 0.713
Current cART regimens 0.361Nevirapine + 2NRTIs 25 (67.6%) 24 (64.5%)Efavirenz + 2NRTIs 10 (27.0%) 12 (32.4%)Others 2 (5.4%) 1 (2.7%)
Secondary prophylaxis 16 (43.2%) 23 (62.2%) 0.103Pneumocystis pneumonia 10 (27.0%) 15 (40.4%) 0.219Penicilliosis marneffei 4 (10.8%) 3 (8.1%) 0.691Cryptococcal meningitis 2 (5.4%) 7 (18.9%) 0.075
ChemoprophylaxisTrimethoprim-sulfamethoxazole 32 (86.5%) 36 (97.3%) 0.088Dapsone 5 (13.5%) 1 (2.7%) 0.088Fluconazole/itraconazole 27 (73.0%) 32 (86.5%) 0.148
CD4 + cell count at randomization (cells/mm3) (median, IQR) 158 (141, 176) 142 (108, 161) 0.041Median (IQR) duration of chemoprophylaxis before randomization (weeks) 142 (75, 220) 112 (65, 210) 0.198% CD4 + cell at randomization (%) (median, IQR) 10 (8, 12) 9 (7, 13) 0.349Median (IQR) time from cART to enrollment (weeks) 183 (105, 315) 117 (68, 213) 0.025
cART, combination antiretroviral therapy, NRTI, non-nucleoside reverse transcriptase inhibitor.
DISCONTINUATION OF PROPHYLAXIS 73
Incidence of opportunistic infections
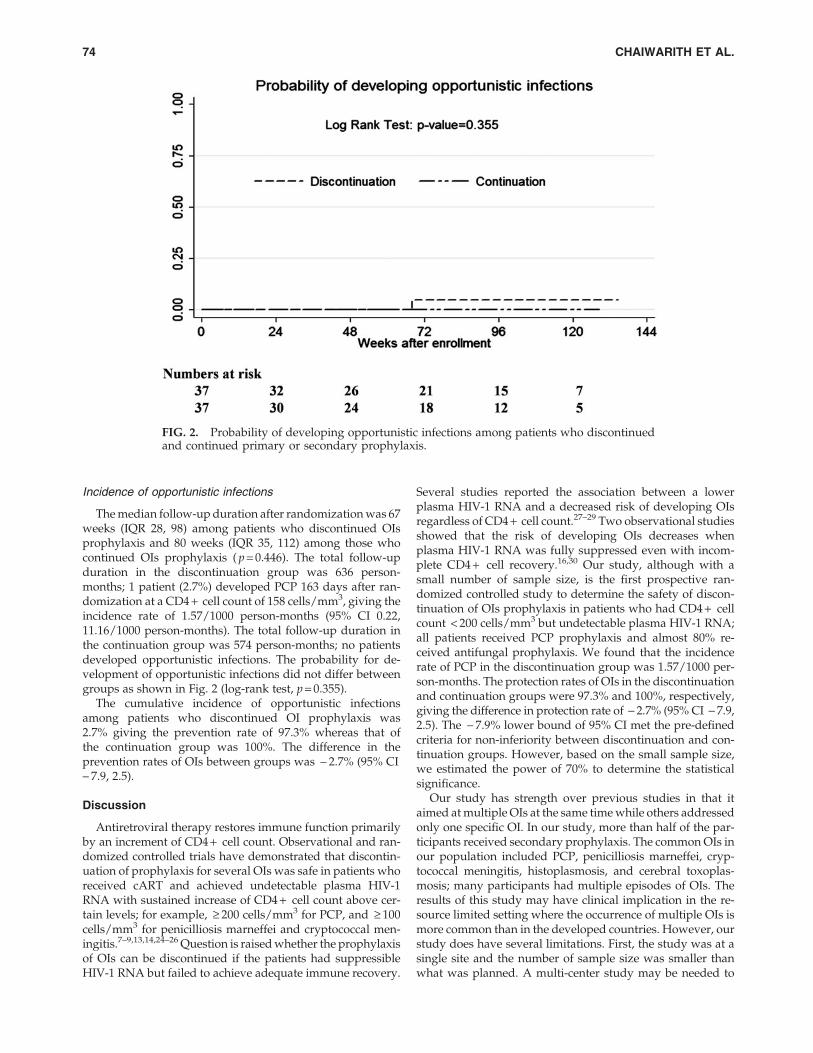
The median follow-up duration after randomization was 67weeks (IQR 28, 98) among patients who discontinued OIsprophylaxis and 80 weeks (IQR 35, 112) among those whocontinued OIs prophylaxis ( p = 0.446). The total follow-upduration in the discontinuation group was 636 person-months; 1 patient (2.7%) developed PCP 163 days after ran-domization at a CD4 + cell count of 158 cells/mm3, giving theincidence rate of 1.57/1000 person-months (95% CI 0.22,11.16/1000 person-months). The total follow-up duration inthe continuation group was 574 person-months; no patientsdeveloped opportunistic infections. The probability for de-velopment of opportunistic infections did not differ betweengroups as shown in Fig. 2 (log-rank test, p = 0.355).
The cumulative incidence of opportunistic infectionsamong patients who discontinued OI prophylaxis was2.7% giving the prevention rate of 97.3% whereas that ofthe continuation group was 100%. The difference in theprevention rates of OIs between groups was - 2.7% (95% CI- 7.9, 2.5).
Discussion
Antiretroviral therapy restores immune function primarilyby an increment of CD4 + cell count. Observational and ran-domized controlled trials have demonstrated that discontin-uation of prophylaxis for several OIs was safe in patients whoreceived cART and achieved undetectable plasma HIV-1RNA with sustained increase of CD4 + cell count above cer-tain levels; for example, ‡ 200 cells/mm3 for PCP, and ‡ 100cells/mm3 for penicilliosis marneffei and cryptococcal men-ingitis.7–9,13,14,24–26 Question is raised whether the prophylaxisof OIs can be discontinued if the patients had suppressibleHIV-1 RNA but failed to achieve adequate immune recovery.
Several studies reported the association between a lowerplasma HIV-1 RNA and a decreased risk of developing OIsregardless of CD4 + cell count.27–29 Two observational studiesshowed that the risk of developing OIs decreases whenplasma HIV-1 RNA was fully suppressed even with incom-plete CD4 + cell recovery.16,30 Our study, although with asmall number of sample size, is the first prospective ran-domized controlled study to determine the safety of discon-tinuation of OIs prophylaxis in patients who had CD4 + cellcount < 200 cells/mm3 but undetectable plasma HIV-1 RNA;all patients received PCP prophylaxis and almost 80% re-ceived antifungal prophylaxis. We found that the incidencerate of PCP in the discontinuation group was 1.57/1000 per-son-months. The protection rates of OIs in the discontinuationand continuation groups were 97.3% and 100%, respectively,giving the difference in protection rate of - 2.7% (95% CI - 7.9,2.5). The - 7.9% lower bound of 95% CI met the pre-definedcriteria for non-inferiority between discontinuation and con-tinuation groups. However, based on the small sample size,we estimated the power of 70% to determine the statisticalsignificance.
Our study has strength over previous studies in that itaimed at multiple OIs at the same time while others addressedonly one specific OI. In our study, more than half of the par-ticipants received secondary prophylaxis. The common OIs inour population included PCP, penicilliosis marneffei, cryp-tococcal meningitis, histoplasmosis, and cerebral toxoplas-mosis; many participants had multiple episodes of OIs. Theresults of this study may have clinical implication in the re-source limited setting where the occurrence of multiple OIs ismore common than in the developed countries. However, ourstudy does have several limitations. First, the study was at asingle site and the number of sample size was smaller thanwhat was planned. A multi-center study may be needed to
FIG. 2. Probability of developing opportunistic infections among patients who discontinuedand continued primary or secondary prophylaxis.
74 CHAIWARITH ET AL.

ensure an adequate sample size for the non-inferiority trial.Second, there were slight but significant imbalances betweengroups in our study. Patients who discontinued prophylaxishad lower CD4 + cell count ( p = 0.04) and shorter durationon cART before randomization ( p = 0.025) than those whocontinued prophylaxis. This is most likely by chance partic-ularly with a small sample size. However, these imbalancesfavor the control group thus having no effect on the finalinterpretation. Again, a multi-center study may be necessaryto adequately address a statistical power and significance aswell as a strong evidence to confidently change the practiceguidelines.
In conclusion, our study, in addition to the previousobservational studies, supports that in the setting whereplasma HIV-RNA measurement is available (e.g., Asia-Pacific region), discontinuation of OI prophylaxis is con-siderably safe in HIV-infected patients receiving cART withundetectable plasma HIV-RNA but incomplete immune re-covery. However, the power to detect the statistical differ-ence might be low due to the small sample size and smallnumber of events.
Acknowledgments
We wish to thank the National Research University Projectunder Thailand’s Office of the Higher Education Commis-sion for financial support. The sponsor did not have a role instudy design, data analysis, data interpretation, or draftingthe article.
The corresponding author had full access to all the data inthe study and had final responsibility for the decision tosubmit for publication. RC participated in trial design, dataanalysis, data interpretation, and drafted the article. JP par-ticipated in patient randomization and data collection. NNand WK participated in patient recruitment. KS participatedin trial design, data interpretation, and revised article criti-cally for important intellectual content. All authors read andapproved the final article.
Author Disclosure Statement
No competing financial interests exist.
References
1. Chaovavanich A, Chottanapund S, Ausavapipit J, Adulya-wat N, Ubonsai W. Survival time of AIDS patients inBamrasnaradura Institute. J Med Assoc Thai 2006;89:1859–1863.
2. Getahun A, Tansuphasawadikul S, Desakorn V, Dhitavat J,Pitisuttithum P. Efficacy and safety of generic fixed-dosecombination of stavudine, lamivudine and nevirapine(GPO-vir) in advanced HIV infection. J Med Assoc Thai2006;89:1472–1478.
3. Kiertiburanakul S, Khongnorasat S, Rattanasiri S, Sungka-nuparph S. Efficacy of a generic fixed-dose combination ofstavudine, lamivudine and nevirapine (GPO-VIR) in ThaiHIV-infected patients. J Med Assoc Thai 2007;90:237–243.
4. Guidelines for Prevention and Treatment of OpportunisticInfections in HIV-Infected Adults and Adolescents. Avail-able from http://www.aidsinfo.nih.gov/guidelines [Cited2011 Feb 11].
5. Kirk O, Lundgren JD, Pedersen C, Nielsen H, Gerstoft J. Canchemoprophylaxis against opportunistic infections be dis-
continued after an increase in CD4 cells induced by highlyactive antiretroviral therapy? AIDS 1999;13:1647–1651.
6. Dworkin MS, Hanson DL, Kaplan JE, Jones JL, Ward JW.Risk for preventable opportunistic infections in persons withAIDS after antiretroviral therapy increases CD4 + T lym-phocyte counts above prophylaxis thresholds. J Infect Dis2000;182:611–615.
7. Schneider MM, Borleffs JC, Stolk RP, Jaspers CA, HoepelmanAI. Discontinuation of prophylaxis for Pneumocystis cariniipneumonia in HIV-1-infected patients treated with highlyactive antiretroviral therapy. Lancet 1999;353:201–203.
8. Furrer H, Egger M, Opravil M, et al. Discontinuation ofprimary prophylaxis against Pneumocystis carinii pneumo-nia in HIV-1-infected adults treated with combination anti-retroviral therapy. Swiss HIV Cohort Study. N Engl J Med1999;340:1301–1306.
9. Lopez Bernaldo de Quiros JC, Miro JM, Pena JM, et al. Arandomized trial of the discontinuation of primary andsecondary prophylaxis against Pneumocystis carinii pneu-monia after highly active antiretroviral therapy in patientswith HIV infection. Grupo de Estudio del SIDA 04/98. NEngl J Med 2001;344:159–167.
10. Weverling GJ, Mocroft A, Ledergerber B, et al. Dis-continuation of Pneumocystis carinii pneumonia prophy-laxis after start of highly active antiretroviral therapy inHIV-1 infection. EuroSIDA Study Group. Lancet 1999;353:1293–1298.
11. Mussini C, Pezzotti P, Govoni A, et al. Discontinuation ofprimary prophylaxis for Pneumocystis carinii pneumoniaand toxoplasmic encephalitis in human immunodeficiencyvirus type I-infected patients: The changes in opportunisticprophylaxis study. J Infect Dis 2000;181:1635–1642.
12. Koletar SL, Heald AE, Finkelstein D, et al. A prospectivestudy of discontinuing primary and secondary Pneumo-cystis carinii pneumonia prophylaxis after CD4 cell countincrease to > 200 · 106 /l. AIDS 2001;15:1509–1515.
13. Mussini C, Pezzotti P, Antinori A, et al. Discontinuation ofsecondary prophylaxis for Pneumocystis carinii pneumoniain human immunodeficiency virus-infected patients: A ran-domized trial by the CIOP Study Group. Clin Infect Dis2003;36:645–651.
14. Soriano V, Dona C, Rodriguez-Rosado R, Barreiro P, Gonzalez-Lahoz J. Discontinuation of secondary prophylaxis for oppor-tunistic infections in HIV-infected patients receiving highlyactive antiretroviral therapy. AIDS 2000;14:383–386.
15. Ledergerber B, Mocroft A, Reiss P, et al. Discontinuation ofsecondary prophylaxis against Pneumocystis carinii pneu-monia in patients with HIV infection who have a response toantiretroviral therapy. Eight European Study Groups. NEngl J Med 2001;344:168–174.
16. Cheng CY, Chen MY, Hsieh SM, et al. Risk of pneumocys-tosis after early discontinuation of prophylaxis among HIV-infected patients receiving highly active antiretroviral therapy.BMC Infect Dis 2010;10:126.
17. Bozzette SA, Finkelstein DM, Spector SA, et al. A ran-domized trial of three antipneumocystis agents in patientswith advanced human immunodeficiency virus infection.NIAID AIDS Clinical Trials Group. N Engl J Med 1995;332:693–699.
18. Chariyalertsak S, Supparatpinyo K, Sirisanthana T, NelsonKE. A controlled trial of itraconazole as primary prophylaxisfor systemic fungal infections in patients with advancedhuman immunodeficiency virus infection in Thailand. ClinInfect Dis 2002;34:277–284.
DISCONTINUATION OF PROPHYLAXIS 75

19. Havlir DV, Dube MP, McCutchan JA, et al. Prophylaxis withweekly versus daily fluconazole for fungal infections inpatients with AIDS. Clin Infect Dis 1998;27:1369–1375.
20. McKinsey DS, Wheat LJ, Cloud GA, et al. Itraconazoleprophylaxis for fungal infections in patients with advancedhuman immunodeficiency virus infection: Randomized,placebo-controlled, double-blind study. National Institute ofAllergy and Infectious Diseases Mycoses Study Group. ClinInfect Dis 1999;28:1049–1056.
21. Nightingale SD, Cal SX, Peterson DM, et al. Primary pro-phylaxis with fluconazole against systemic fungal infectionsin HIV-positive patients. AIDS 1992;6:191–194.
22. Powderly WG, Finkelstein D, Feinberg J, et al. A random-ized trial comparing fluconazole with clotrimazole trochesfor the prevention of fungal infections in patients with ad-vanced human immunodeficiency virus infection. NIAIDAIDS Clinical Trials Group. N Engl J Med 1995;332:700–705.
23. Singh N, Barnish MJ, Berman S, et al. Low-dose fluconazoleas primary prophylaxis for cryptococcal infection in AIDSpatients with CD4 cell counts of < or = 100/mm3: Demon-stration of efficacy in a positive, multicenter trial. Clin InfectDis 1996;23:1282–1286.
24. Chaiwarith R, Charoenyos N, Sirisanthana T, SupparatpinyoK. Discontinuation of secondary prophylaxis against peni-cilliosis marneffei in AIDS patients after HAART. AIDS2007;21:365–367.
25. Vibhagool A, Sungkanuparph S, Mootsikapun P, et al. Dis-continuation of secondary prophylaxis for cryptococcalmeningitis in human immunodeficiency virus-infected pa-tients treated with highly active antiretroviral therapy: A
prospective, multicenter, randomized study. Clin Infect Dis2003;36:1329–1331.
26. Mussini C, Pezzotti P, Miro JM, et al. Discontinuation ofmaintenance therapy for cryptococcal meningitis in patientswith AIDS treated with highly active antiretroviral therapy:an international observational study. Clin Infect Dis 2004;38:565–571.
27. Lyles RH, Chu C, Mellors JW, et al. Prognostic value ofplasma HIV RNA in the natural history of Pneumocystiscarinii pneumonia, cytomegalovirus and Mycobacteriumavium complex. Multicenter AIDS Cohort Study. AIDS 1999;13:341–349.
28. Kaplan JE, Hanson DL, Jones JL, Dworkin MS. Viral load asan independent risk factor for opportunistic infections inHIV-infected adults and adolescents. AIDS 2001;15:1831–1836.
29. Williams PL, Currier JS, Swindells S. Joint effects of HIV-1RNA levels and CD4 lymphocyte cells on the risk of specificopportunistic infections. AIDS 1999;13:1035–1044.
Address correspondence to:Dr. Romanee ChaiwarithDepartment of Medicine
Faculty of MedicineChiang Mai University
Chiang Mai 50200Thailand
E-mail: [email protected]
76 CHAIWARITH ET AL.