disability, homelessness and social relationships among ... · disability, homelessness and social...
TRANSCRIPT
Carol HarveyHelen Evert
Helen HerrmanTony PinzoneOye Gureje
on behalf of the LPD study group
Disability, homelessness and social relationshipsamong people living with psychosis in Australia
October 2002
Low Prevalence Disorder Component of the NationalStudy of Mental Health and Wellbeing
Bulletin 5
Disability, homelessnessand social relationships
among people living withpsychosis in Australia
A Bulletin of the Low PrevalenceDisorder Study
Carol HarveyHelen Evert
Helen HerrmanTony PinzoneOye Gureje
on behalf of the LPD study group
National Survey of Mental Health and WellbeingBulletin 5
ii Disability, homelessness and social relationships among people living with psychosis in Australia
© Commonwealth of Australia 2002
ISBN 0 642 50340 0
This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no partmay be reproduced by any process without prior written permission from the Commonwealthavailable from Information Services. Requests and inquiries concerning reproduction and rightsshould be addressed to the Manager, Copyright Services, Information Services, GPO Box 1920,Canberra ACT 2601 or by e-mail [email protected].
Publication approval number: 2944
Publications Production Unit (Governance and Business Strategy Branch)Commonwealth Department of Health and AgeingCanberra
Additional copies of the bulletin are available from the Mental Health Branch, CommonwealthDepartment of Health and Ageing, telephone 1800 066 247 or facsimile 1800 634 400.
A copy may also be downloaded from the Mental Health Branch website at:http://www.mentalhealth.gov.au
Copies of other publications produced under the National Mental Health Strategy are alsoavailable at this site.
The opinions expressed in this report are those of the authors and are not necessarily those of theCommonwealth Department of Health & Ageing.
The authors would like to acknowledge the Commonwealth Department of Health and Ageing,Mental Health and Special Programs Branch, for providing the funding to undertake this project.
Disability, homelessness and social relationships among people living with psychosis in Australia iii
This publication is one of a series of publications produced by the Commonwealth Departmentof Health and Ageing under the National Survey of Mental Health and Wellbeing. Otherpublications include:
Low prevalence component of the survey:
People living with psychotic illness: an Australian study 1997-1998
People living with psychotic illness: an overview (Bulletin 1)
Costs of psychosis in urban Australia (Bulletin 2)
Employment and psychosis (Bulletin 3)
The use of psychopharmacological and other treatments by persons with psychosis (Bulletin 4)
Disability, homelessness and social relationships among people living with psychosis inAustralia (Bulletin 5)
Stigma and discrimination (Bulletin 6)
Child and adolescent component of the survey:
The mental health of young people in Australia
Adolescent depression (Leaflet 1)
Conduct disorders (Leaflet 2)
Adolescent suicide (Leaflet 3)
Attention deficit / hyperactivity disorder (Leaflet 4)

iv Disability, homelessness and social relationships among people living with psychosis in Australia
Disability, homelessness and social relationships among people living with psychosis in Australia v
Contents
Acknowledgments viii
Executive summary xi
Functioning and disability - relevant personal and clinical factors for peoplewith psychosis xiDisability, service use and quality of life among people living in different typesof housing across Australia xiiDisability and service use among homeless people living with psychotic disorders inMelbourne xiiiSocial networks and functioning of people with psychosis xiv
1. Disability, homelessness and social relationships - an introduction 1
1.1 The Low Prevalence (Psychotic) Disorders Study 11.2 The importance of functioning and disability of persons with psychosis 11.3 Scope of this bulletin 21.4 The relevance of the attributes of the health condition and personal factors
to functioning 31.5 The relevance of environmental factors to a person’s functioning 41.6 The importance of adequate housing and the problem of homelessness 41.7 The value of social networks 51.8 Summary of aims 6
2. Functioning and disability - relevant personal and clinical factors for peoplewith psychosis 7
2.1 Measures and definitions used in this chapter 92.1.1 Service use 10
2.2 Findings 112.2.1 Socio-demographic characteristics 112.2.2 Work, study, and home duties 112.2.3 Relationships with others, self care and outside interests 122.2.4 Service use 13
2.3 Conclusions 242.4 Recommendations 26
3. Disability, service use and quality of life among people living in differenttypes of housing across Australia 29
3.1 Measures and definitions used in this chapter 303.1.1 Accommodation type 303.1.2 Substance use 323.1.3 Quality of life 32
3.2 Findings 323.2.1 Socio-demographic characteristics 323.2.2 Clinical features 333.2.3 Substance use 33
vi Disability, homelessness and social relationships among people living with psychosis in Australia
3.2.4 Work, study, and home duties 363.2.5 Relationships with others, self care and outside interests 373.2.6 Service use 383.2.7 Quality of life 39
3.3 Conclusions 413.4 Recommendations 42
4. Disability and service use among homeless people living with psychoticdisorders in Melbourne 43
4.1 Definition of homelessness 444.2 Methodology of the nested study of the homeless population with psychosis in
Melbourne 454.2.1 The catchment area for the Melbourne study 454.2.2 Study design 464.2.3 Interviewing and sampling results in marginal accommodation 464.2.4 Interviewing and sampling results in drop-in centres 47
4.3 Findings 484.3.1 Calculating the prevalence of people living with psychosis in marginal
accommodation 484.3.2 Socio-demographic characteristics 484.3.3 Clinical features 494.3.4 Substance use 504.3.5 Relationships with others, home duties, self care and outside interests. 504.3.6 Service use 514.3.7 Quality of life 52
4.4 Conclusions 534.5 Recommendations 54
5. Social networks and functioning of people with psychosis 55
5.1 People with schizophrenia and their social networks 555.2 Measures and definitions used in this chapter 565.3 Findings 56
5.3.1 Socio-demographic characteristics 565.3.2 Clinical features 575.3.3 Work, study, and home duties 585.3.4 Household activities 585.3.5 Relationships with others, self care and outside interests 59
5.4 Conclusions 605.5 Recommendations 61
Appendix 1: The Diagnostic Interview for Psychoses-Disability Module (DIP-DIS) 63
Background and rationale for development of the DIP-DIS 63The Disability Module (DIP-DIS) 63Inter-rater reliability 64Agreement with another measure of disability: Criterion validity 64Sensitivity to differences in disability: Discriminant validity 65Discussion 65

Disability, homelessness and social relationships among people living with psychosis in Australia vii
Appendix 2: Details of the methodology of the systematic case study in Melbourne 67
Instruments 67Compiling the sampling frame for marginal accommodation 67Rationale for number of residents approached for screening 68Ethical procedures 68Sampling results in marginal accommodation 68Compiling the sampling frame for drop-in centres and other non-residentialdisability support agencies 69Sampling results in drop-in centres and other non-residential disability support agencies 69References 71
viii Disability, homelessness and social relationships among people living with psychosis in Australia
Acknowledgments
This bulletin is based on data collected in the framework of the Collaborative Study on Low-Prevalence (Psychotic) Disorders, an epidemiological and clinical investigation which is part ofthe National Survey of Mental Health and Wellbeing, Australia 1997-1998. The members of theLow Prevalence (Psychotic) Disorders Study Group are: Professor Assen Jablensky (ProjectDirector and Team Leader, Western Australia); Professor Vaughan Carr (Adviser); Dr DavidCastle (Deputy Team Leader, Western Australia); Dr Mandy Evans (Team Leader, AustralianCapital Territory); Professor Oye Gureje (Deputy Team Leader, Victoria); Dr Carol Harvey(Deputy Team Leader, Victoria); Professor Helen Herrman (Team Leader, Victoria); Mrs AilsaKorten (Statistician); Associate Professor John McGrath (Team Leader, Queensland); Ms VeraMorgan (Project Database Manager). Other investigators at the four sites included: ScottHenderson, Stephen Rosenman, Jo Medway (Australian Capital Territory); David Chant, SusetteCardy, Chris Young, Ben Chapple (Queensland); Ian Gordon, Tom Trauer, Helen Evert, TonyPinzone (Victoria); Anna Waterreus (Western Australia). A complete list of the investigators isavailable in: Jablensky, A., McGrath, J., Herrman, H., Castle, D., Gureje, O., Morgan, V., &Korten, A. on behalf of the study group (1999) People Living with Psychotic Illness: AnAustralian Study 1997-98. National Survey of Mental Health and Wellbeing - Report 4.Canberra: Australian Mental Health Branch, Commonwealth Department of Health and AgedCare. Ethics approvals for the study were obtained from relevant institutional ethics committees.Full details are available on request. The study was funded by the Commonwealth Department ofHealth and Aged Care for those components carried out in Brisbane, Melbourne and Perth. Thecomponent carried out in Canberra was funded separately by the Australian Capital TerritoryDepartment of Health and Community Care, and The Psychiatric Epidemiology ResearchCentre, Australian National University. This report also acknowledges, with thanks, the hundredsof mental health professionals who assisted in the preparation and conduct of the survey and themany Australians with psychotic disorders who agreed to participate. Without them, this studywould not have seen the light of the day.
Local acknowledgments
Interviewers
Monique DecortisAndrew GreenNaomi HarrisChris HillMaggie McIntoshSusan RobertsRosemary Thomas
Technical Advisory Committee:
Dr John Reilly, St. Vincent’s Mental Health ServiceDr Tom TrauerMs Julie Shaw, VMIACMs Heather MooreAssoc Prof Andrew MacKinnon, Mental Health ResearchInstituteMr Fionn Skiotis, Yarra Community Housing GroupDr Ian Gordon, Statistical Consulting Centre, University ofMelbourneMs Ellie Fossey, La Trobe UniversityMs Margaret Grigg, St. Vincent’s Mental Health Service
Special thanks to all the non-government organisations thatassisted in conducting this study.
Disability, homelessness and social relationships among people living with psychosis in Australia ix
Executive summary
The National Survey of Mental Health and Wellbeing (NSMHWB) was commissioned by theCommonwealth Department of Health and Aged Care and was conducted during 1997 and 1998.As part of the NSMHWB, a two-phase survey of low prevalence (psychotic) disorders (LPD)was undertaken in predominantly urban catchment areas of the Australian Capital Territory,Queensland, Victoria and Western Australia.
The 980 participants were identified using a census and screen, and subsequent sampleinterviews were undertaken using a specially designed instrument (Diagnostic Interview forPsychoses - DIP) covering demographic details, living circumstances, symptoms, and serviceutilisation. The functioning and disability of participants in this survey, which are the coresubject matter of this bulletin, were assessed using the Disability Module of the DiagnosticInterview for Psychoses (DIP-DIS). (Gureje et al. 2001)
This bulletin considers the functioning, housing and social relationships of people living withpsychosis in Australia. Functioning and disability are defined according to those aspects of theInternational Classification of Functioning, Disability and Health (ICF) framework (WorldHealth Organisation 2001) that describe the activity and participation of individuals, and thecontextual factors (personal and environmental), which interact with them in affectingindividuals’ functioning. Within this model, there is a dynamic relationship between healthconditions (in this case, psychosis), these aspects of functioning, and personal and environmentalcontextual factors. In this bulletin, the health condition is categorised by diagnosis and course ofpsychotic disorder. The contextual factors chosen as especially pertinent to the functioning anddisability of people with psychosis are the personal factors of gender and age (Chapter 2)together with the environmental factors of social relationships (Chapter 5) and living conditionsexemplified in housing types (Chapter 3).
The social relationships of people in this survey were classified according to the extent of contactwith relatives and/or friends into: ‘socially isolated’, ‘friends dominated network’, ‘familydominated network’ and ‘socially integrated’ (Chapter 5). With respect to participants’ housing,special emphasis was given to people living in marginal accommodation (Chapter 4), defined asresidential accommodation affordable on a pension, characterised by lack of secure tenure, littleprivacy, and shared kitchen and bathroom facilities.
Functioning and disability - relevant personal and clinical factors forpeople with psychosis
A substantial number of people with psychosis experience activity limitations and participationrestrictions in key life areas. This is particularly so for those men and women with persistingpsychosis. Despite this, less than one-fifth of interviewees participated in rehabilitation programsthat have the potential to address these difficulties through individually tailored pharmacological,psychological, social and occupation-focused therapies. Of concern, mental health services arepredominantly providing pharmacological treatments, with relatively little emphasis on the othertherapies which may be more beneficial in the later stages of illness.
• Given the limited involvement of this population in rehabilitation programs, greater access tosuch programs and/or treatments with a rehabilitation or recovery focus appears to be muchneeded. The National Mental Health Strategy and state planning frameworks should reflectthis need, and federal and state mental health resources should support the development ofsuch programs by mental health services and the psychiatric disability support sector.Rehabilitation should be available at all stages of psychotic illness.
x Disability, homelessness and social relationships among people living with psychosis in Australia
• Like those with physical illness, many people with mental illness or impairments experiencedifficulties in daily living skills. Therefore, to enable them to compensate for their difficulties,they should have equal access to services provided by the joint federal and state program -Home and Community Care (HACC). These include housekeeping, provision of meals andprovision of environmental supports.
• Mental health workers should be fully trained in the range of psychosocial interventionsknown to be effective. Case managers should also be able to call on other clinicians andservice providers with the necessary skills and resources.
• Further research into the effective ingredients of both case management and rehabilitationwould be advantageous to better understand how disability among people with psychosis canbe addressed within the specific and ‘real world’ framework of mental health (and otherservices) in Australia.
Most study participants identified no major occupation, suggesting that boredom and under-activity are likely to be contributing to diminished well-being and quality of life. Even whenoccupied, almost half of those interviewed experienced some occupational dysfunction,suggesting an inadequate fit between motivation, interest, skills and other personal attributes, andthe nature and challenge of the available occupations.
• This under-activity and boredom should be addressed by access to a variety of meaningfuloccupations. A number of systemic changes are necessary, including public educationinitiatives, as well as a review of policies and legislation to ensure that social and financialbarriers to community reintegration do not continue to exist.
• Research into the environmental and personal barriers that prevent people with psychosis fromgaining and retaining meaningful occupation is required.
Only 10% of people with psychosis reported full-time employment and a further 18% were inpart-time employment in the previous 12 months. Much of the considerable psychological,physical and social impact implied by these figures may be avoidable, as experience elsewhere inthe world has shown that many more people with serious mental illness, including psychoticdisorders, can be meaningfully employed.
People with schizophrenia and schizo-affective disorder are less likely to be employed comparedwith others with psychotic disorders.
• Most people with psychosis require assistance, at both the systemic and individual level, eitherto retain or regain employment. More detailed and specific recommendations regardingemployment, vocational training and education are outlined in the companion bulletin (Frost etal. 2002).
Disability, service use and quality of life among people living indifferent types of housing across Australia
The typical resident among those studied in supported, marginal or institutional accommodationis single, male and often diagnosed with schizophrenia. In the marginal and institutional settings,the resident often has less education and less chance of being employed than others who areliving with psychosis. Residents of supported accommodation seem to be doing better than theother two groups: they are more likely to be occupied, including in paid work, they have fewerdifficulties with caring for themselves, and they experience a lower level of social dysfunction.
Under-activity is more common in staffed settings such as institutions, supported housing andhostels. The presence of staff does not of itself address people’s under-occupation, for reasonsthat are likely to be complex.
Disability, homelessness and social relationships among people living with psychosis in Australia xi
Data on everyday living tasks suggest that opportunities are especially limited for people inmarginal and institutional settings. This suggests people’s functioning may be limited throughenvironmental barriers to activity and participation, as well as the effects of the psychosis itselfand associated impairments.
People in institutional settings, and to a lesser degree those in marginal accommodation, lackintimate friendships. So, whilst there are people nearby, there is a lack of intimacy in socialinteractions. Yet there is an expressed desire amongst many residents in these settings for suchintimacy.
• The widespread under-activity and social isolation in institutional settings should beaddressed. This could be done by maximising the use of environmental supports toaccommodate individuals’ functional difficulties, and minimising environmental barriers thatconstrain their opportunities for occupation and relationships. Provision of improved access torehabilitation and disability support could help to address these issues.
The extent of smoking among people living with psychosis is a major public health issue, havingadverse implications for physical health and life expectancy. In comparison to the Australianpopulation, harmful alcohol consumption is more prevalent among people with psychosis livingin all accommodation settings (except for those in supported housing) and is of particularconcern among those living in marginal accommodation where it may contribute to housinginstability. Likewise, heroin use is alarmingly high across all accommodation settings, especiallyin marginal accommodation. In contrast, access to drug and alcohol services among people withpsychosis is extremely low.
• Specially designed programs to help people with psychosis reduce or quit smoking need to bedeveloped and made widely available through agencies such as community health, primarycare and non-government organisations.
• People with psychosis urgently require improved access to drug and alcohol services,particularly services addressing the specific issues arising out of the co-morbidity of mentalillness and substance abuse.
The degree of mismatch between people’s needs (as inferred from the findings with regard tofunctioning) and service use appears to depend on the setting. For example, most people living instaffed settings get little support in managing housing or financial matters even though it couldbe anticipated that many have needs in this area. Particularly striking is the low use of thehousing department by people in marginal accommodation. More encouraging is that the level ofsocial support offered to those in supported accommodation increases as their level of socialdifficulty increases.
• Greater attention should be given to the interaction between personal and environmentalfactors in recovery from psychosis. It is important to assess the individual’s needs rather thanmake assumptions based on his/her current environmental circumstances, and to facilitate theirrecovery by matching their needs with the most appropriate environment.
Disability and service use among homeless people living withpsychotic disorders in Melbourne
A systematic survey detected an unexpectedly high prevalence of people living with psychoticdisorders in marginal accommodation in Melbourne (42%) compared with 21% in a similarstudy in 1989 (Herrman et al. 1989). The decline of low cost housing for people on low incomesin the study area is a linked observation of possible relevance.
Except for people with psychosis in institutional settings, disability in everyday, occupationaland social functioning is higher for those living in marginal accommodation than any other
xii Disability, homelessness and social relationships among people living with psychosis in Australia
group. It is worrying that disability is so prevalent among residents in marginal accommodationbecause these settings are not specifically designed to cater for people with mental-health relatedneeds.
Significant disability and unmet needs are observed among homeless people with psychosisdespite high rates of contact with specialist mental health services, including community mentalhealth services. Even the best clinical services will fail to meet the needs of those with the mostcomplex problems unless there is close co-operation with housing, welfare and disability supportservices, including vocational services, to provide support and assistance to each individual.
• Clinical services, housing services and disability support services, including those provided bynon-government organisations, should be better coordinated in order to more successfullymeet the needs of people with regard to both their mental illness and their housing and livingcircumstances. This is essential for those with complex needs.
• Departments responsible for housing and health should work together to develop a range ofsecure and stable accommodation options, with both flexible and outreach support to meet thevarious and changing needs of people with psychosis.
• Research programs into homelessness and serious mental illness should include longer-termfollow-up studies that focus on how to sustain early gains.
A substantial minority of residents in marginal accommodation feel unsafe in their locality.There are also high levels of dissatisfaction among residents.
• To facilitate service planning, more in-depth analyses of disability and unmet need amonghomeless people with psychosis are required, including the perspective of residents and staff.
Homeless women with psychotic illness have particular characteristics pointing to a differentprofile of needs. Co-morbidity of psychotic illness with substance use is high, although less thanfor homeless men. They are more likely to experience psychotic depression, are more likely to bemarried or have previously been so, and have greater difficulties in their social functioningcompared with homeless men.
• The particular needs of homeless women with psychotic disorders need to be addressed in theprovision of appropriate services, including attention to marital breakdown and wider aspectsof social functioning.
Social networks and functioning of people with psychosis
Relative social isolation amongst people living with psychosis is common. Although the group ofparticipants who were classed as socially integrated had some contacts with friends and family,many were still experiencing some social dysfunction, and almost half wanted more friends. Onethird of these people stated that they had no intimate friend.
• Local, state and national organisations providing social opportunities in the wider communityshould examine whether their policies allow for appropriate access of those with psychoticdisorders. Public education campaigns to combat stigma are required.
• Community mental health services should provide more psychological, social and practicalinput that will assist people with psychosis to re-establish their social networks and alsoprovide support to maintain existing networks to prevent future loss or deterioration inrelationships. People’s preferences should be explored and acknowledged.
• Education and training programs are required to develop specific professional skills that willassist people with psychosis to better improve their social functioning.
People with psychosis who are in contact with relatives (but not friends) may often beexperiencing almost as much social dysfunction as those with virtually no contact with eitherfriends or family.
Disability, homelessness and social relationships among people living with psychosis in Australia xiii
There is a small but nevertheless important minority of those participants who were isolated orhad only family members in their networks that appear to actively reject the need for morefriends.
Those survey participants who had friends in their social networks were rated as having betterself care. The converse association is observed for employment. People with networks dominatedby family were more likely to be employed than those in friends dominated networks. It seemslikely that the nature of people’s social networks, whether primarily composed of friends orfamily members, may have differing relationships to varied aspects of their functioning.
• There should be more quantitative and qualitative research that focuses on the quality ofrelationships of people with psychosis. Further, their expressed needs with regard to socialrelationships should be surveyed and taken into account.
There is an important association between social isolation and socio-economic disadvantage. Themost socially isolated individuals are far less likely to have a job or live in ‘independentaccommodation’ (their own or a family home, or rented accommodation).
The presence of other people in a person’s living arrangement may not truly reflect theiropportunities for, and engagement in, social interactions. For example, many people living ininstitutional settings or marginal accommodation where other people are often around arenevertheless socially isolated. Conversely, one cannot assume that people who are living in rentalproperties (often alone) are without contact with friends and family.
• Community mental health services should review their policies to ensure that they haveeffective outreach procedures to facilitate the access of people with psychosis who areparticularly socially isolated. This will allow assessment of, and effective intervention for,their significant difficulties with regard to daily living skills.

Disability, homelessness and social relationships among people living with psychosis in Australia 1
1. Disability, homelessness and socialrelationships – an introduction
1.1 The Low Prevalence (Psychotic) Disorders StudyThe National Survey of Mental Health and Well-being (NSMHWB) was commissioned by theCommonwealth Department of Health and Aged Care and was conducted during 1997 and 1998.As part of the NSMHWB, a two-phase survey of low prevalence (psychotic) disorders (LPD)was undertaken in predominantly urban catchment areas of the Australian Capital Territory,Queensland, Victoria and Western Australia (Jablensky et al. 1999a; Jablensky et al. 1999b;Jablensky et al. 2000).
The aims of the survey were to:
• establish one-month and one-year prevalence estimates of psychotic disorders among adultsaged 18 to 65 years in Australia
• establish a demographic profile of individuals with psychotic disorders
• quantify the rates of disability associated with psychotic disorders
• determine the pattern of service utilisation by individuals with psychotic disorders
• provide an estimate of unmet needs for individuals with psychotic disorders.
The 980 participants in the LPD were identified using a census and screen, and subsequentsample interviews were undertaken using a specially designed instrument (Diagnostic Interviewfor Psychoses - DIP) covering demographic details, living circumstances, symptoms, level ofdisability and service utilisation. The DIP was designed to be used by trained mental healthprofessionals in this study. An overview of the methods and findings of the study, includingdetailed prevalence estimates, is published as a report and bulletin (Jablensky et al. 1999a;Jablensky et al. 1999b). Additional bulletins present detailed analysis and discussion of findingsfrom the study. Four companion bulletins cover: the employment of persons with psychoticdisorders (Frost et al. 2002); the effects of stigma and discrimination (Carr and Halpin 2002); aneconomic analysis of disability and service costs associated with psychosis (Carr et al. 2002);and, a detailed analysis of the use of psychopharmacological and other treatments by peopleliving with psychosis in Australia (Morgan et al. 2002). This bulletin considers the functioning,housing and social relationships of people living with psychosis in Australia.
1.2 The importance of functioning and disability ofpersons with psychosis
There is increasing recognition of the importance of the functional impact of mental disordersand the need to estimate disability associated with these disorders, as exemplified by the GlobalBurden of Disease study (Murray and Lopez 1997). In considering recovery from psychosis, it isnow acknowledged that improved functioning does not equate with, or automatically followfrom, resolution of psychotic symptoms (Carpenter and Strauss 1991; Harding et al. 1992) andso recovery involves a more complex and varied process than previously thought. Consequently,the pathways to improved functioning and recovery, for individuals or groups of individualsreceiving particular services are likely to be more varied and necessitate a wider range oftreatment approaches from service providers. In Australia, consultation with service providers,
2 Disability, homelessness and social relationships among people living with psychosis in Australia
carer groups and consumer groups has suggested that improved functioning (as contributing todisability) and quality of life are outcomes rated as significantly more important thanimprovement in symptoms or consumer satisfaction (Andrews et al. 1994). This is supported bythe personal stories of people with psychosis. Thus, people living with mental illness (especiallypsychosis) have emphasised the importance of improved functioning, as distinct from symptomresolution, to their experience of recovery (Leete 1989; Davidson and Strauss 1992; Deegan1996). The findings of the LPD study as they relate to functioning and disability of people livingwith psychosis in Australia provide some insight into personal experiences of recovery sincethose experiences are reflected in the ratings made within the semi-structured interview to assessdisability (see Appendix 1). The findings reported here on functioning and disability haveimportant implications for service organisation and delivery.
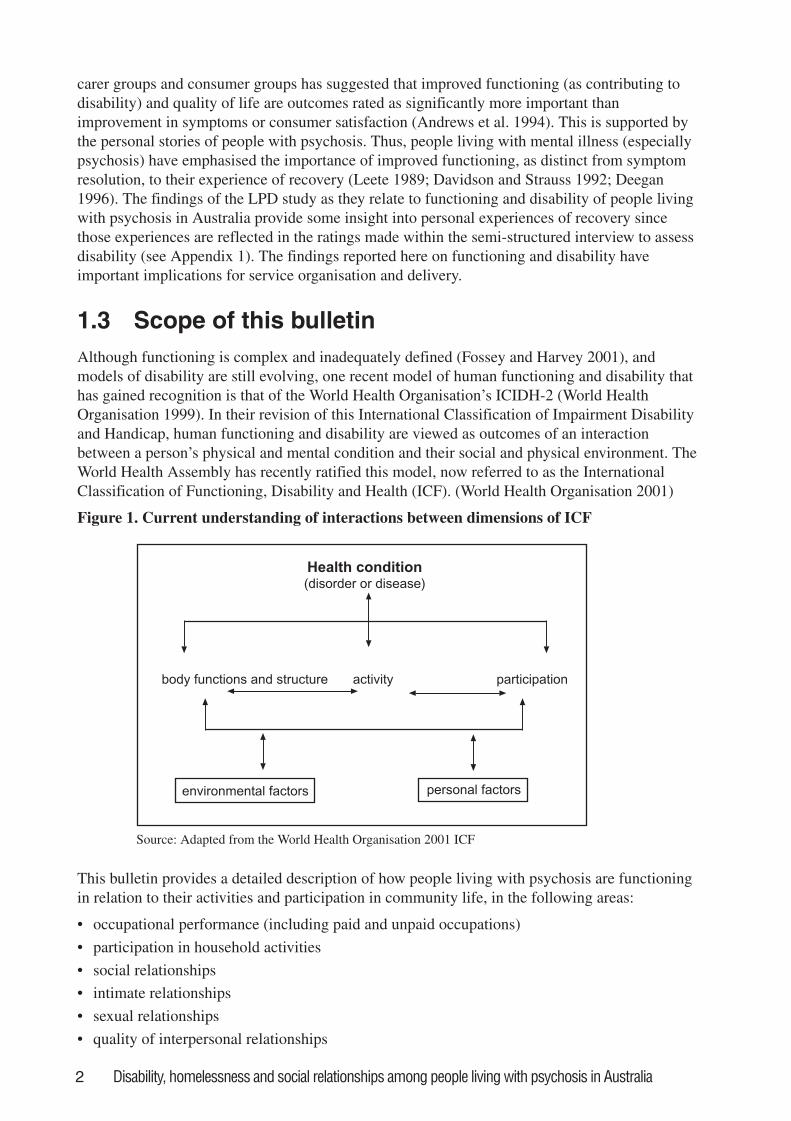
1.3 Scope of this bulletinAlthough functioning is complex and inadequately defined (Fossey and Harvey 2001), andmodels of disability are still evolving, one recent model of human functioning and disability thathas gained recognition is that of the World Health Organisation’s ICIDH-2 (World HealthOrganisation 1999). In their revision of this International Classification of Impairment Disabilityand Handicap, human functioning and disability are viewed as outcomes of an interactionbetween a person’s physical and mental condition and their social and physical environment. TheWorld Health Assembly has recently ratified this model, now referred to as the InternationalClassification of Functioning, Disability and Health (ICF). (World Health Organisation 2001)
Figure 1. Current understanding of interactions between dimensions of ICF
Health condition
(disorder or disease)
body functions and structure activity participation
environmental factors personal factors
Source: Adapted from the World Health Organisation 2001 ICF
This bulletin provides a detailed description of how people living with psychosis are functioningin relation to their activities and participation in community life, in the following areas:
• occupational performance (including paid and unpaid occupations)
• participation in household activities
• social relationships
• intimate relationships
• sexual relationships
• quality of interpersonal relationships
Disability, homelessness and social relationships among people living with psychosis in Australia 3
• self care
• interest in the outside world.
These areas cover performance of activities to meet basic needs (such as caring for oneself) aswell as the nature and extent of their participation in life situations (for example, employment).As summarised in the ICF model (Figure 1), there is a dynamic relationship between healthconditions (in this case, psychosis), these aspects of functioning, and personal and environmentalcontextual factors. In this bulletin, diagnosis and course of psychotic disorder categorise thehealth condition itself. Some personal factors relevant to functioning in general (World HealthOrganisation 1999) as well as to functioning in psychosis in particular (Harding and Keller 1998;Jablensky 2000a) are gender and age. Numerous environmental factors are affected by, and havean effect on people, including those living with psychosis (Jablensky 2000b). These includesocial relationships and living conditions exemplified in people’s housing. These aspects of thehealth condition, and personal and environmental factors will now be elaborated.
1.4 The relevance of the attributes of the healthcondition and personal factors to functioning
Persons with psychosis are generally considered to have a more severe degree of psychiatricsymptomatology and associated poorer functioning than for those without psychosis. Forexample, when psychotic symptoms are part of the picture of affective disorder, the outcome isless positive. Persons with psychotic affective disorders continue to demonstrate functionaldeficits, especially in short-term follow up studies, although improvement is likely over time(Henry and Coster 1996). It has been thought that an even poorer social and occupationalfunctioning is associated with schizophrenia compared with affective psychoses. A majority ofstudies show that the functional difficulties (including in social relationships) in schizo-affectivedisorder are intermediate between those of schizophrenia and affective disorders (Kendler et al.1995).
There is general agreement that the course of the disorder (that is, the pathways or trajectories ofthe disorder) has an impact on social and occupational outcome (Jablensky 2000a). Typically, themore protracted the episodes of illness, the shorter the periods of remission and/or the greater the‘residual symptomatology’, the more substantial the negative impact on social and occupationalfunctioning (Strauss and Carpenter 1977; Henry and Coster 1996).
Age is also important for two main reasons. Firstly, from a developmental perspective, the impactof a psychotic disorder on a person’s functioning depends on the age at which the disorderdevelops and the subsequent impact on developmental tasks-for example, getting a job (EPPIC2001). Secondly, the trajectory of the disorder and thus, its functional impact, may vary with theperson’s age. In the case of schizophrenia, this disorder used to be considered as an intractable,deteriorating illness (Jablensky 2000a). There is now a growing realisation from carefullyconducted long-term follow-up studies that a high proportion of people recover, eithercompletely or with mild residual abnormalities, after decades of severe illness (Harding et al.1987). There is less effect of age on outcome of mood disorders, apart from in the elderly wheredepression, although milder, is often more prolonged and hence may have a more sustainedimpact on everyday and social functioning.
Recent studies of first-episode psychosis suggest that the disorder is less severe and episodes areless frequent in women. In the early stages of the illness, men tend to demonstrate poorer socialand occupational functioning. However, these gender effects seem to diminish over time(Jablensky 2000a). Although both non-psychotic and psychotic depressions are more common inwomen, reports of gender differences in functional outcomes are scarce.
4 Disability, homelessness and social relationships among people living with psychosis in Australia
1.5 The relevance of environmental factors to aperson’s functioning
The Diagnostic Interview for Psychoses - Disability Module (DIP-DIS) was specially designedto assess the functioning and disability of participants in this study (Gureje et al, 2001). SeeAppendix 1 for details. The central core of the DIP-DIS is an abridged and modified version ofthe World Health Organisation. Disability Assessment Schedule (WHO/DAS). (World HealthOrganisation 1988) Consistent with the WHO/DAS, the baseline for rating was provided by theprevalent social norms and expectations about the particular role, since disability can be manifestonly in a social context. When making their ratings, interviewers took into account that there isno single norm that is valid for all ages, for both sexes, and for each social and cultural setting.Beyond this, the LPD was not designed to take account of all environmental circumstances andconditions relevant to an evaluation of the functioning of persons with psychosis. For example, inrelation to social functioning, it has been suggested that ‘the whole person, the illness, and theenvironment must be measured simultaneously if we are to begin to understand these complexand interactive processes’ (Harding and Keller 1998). While this was not possible, informationfrom the LPD is unusually rich in a study of this scope and allows us to describe and begin toexplore the interaction between key environmental features and persons with psychosis. Ourobjective is to explore this interaction as far as the data will allow. Accommodation type andsocial networks are highlighted as these two factors influence each other-each indicate animportant aspect of quality of life and are closely related to the social isolation often experiencedby those living with psychotic disorders (Davidson et al. 1998).
1.6 The importance of adequate housing and theproblem of homelessness
Most persons with psychosis experience significant socio-economic disadvantage as evidencedby the high proportion (85% of the LPD population) living on a government pension or someform of social benefit (Jablensky et al. 1999b). In these circumstances income is less sensitive asan indicator of relative socio-economic disadvantage among persons with psychosis than theirtype of accommodation. Moreover, consumers often identify basic needs such as shelter and adecent home as integral to their experience of satisfactory quality of life in the community(Davidson et al. 1996; Owen et al. 1996; Young and Ensing 1999). The different settings inwhich study participants live are also related to the type of social networks and support availableto them. For these reasons we describe people with psychosis who were interviewed for the LPD,according to the accommodation in which they were living at the time.
We pay special attention to the subgroup of participants who were homeless, or marginallyaccommodated, at the time of the study. Homeless people with mental illness have specific healthand social needs that are often inadequately met by services. Stability of housing is an importantpre-requisite for clinical improvement and episodes of illness may undermine such stability.Public concern about homeless people, and particularly the sub-group of them with mentalillness, is evident in Europe (eg Scott 1993; Craig and Timms 1995; Kovess and Lazarus 1999),the USA (eg Caton 1990) and Australia (Herrman 1996; Teesson et al. 2000). The numbers ofhomeless people, however defined, appear to be growing in several countries (Scott 1993), andthe characteristics of the sub-group with mental illness appear to be changing. The process of de-institutionalisation began over 40 years ago when people with severe mental illness living inlarge psychiatric institutions moved to living in the community. A number of observers haveassumed that de-institutionalisation is the main cause of increased numbers of homeless mentally

Disability, homelessness and social relationships among people living with psychosis in Australia 5
ill people. However, careful studies of the discharge of long stay psychiatric patients, forexample the TAPS (Team for the Assessment of Psychiatric Services) study in London, reportthat few people drifted into homelessness following hospital closure (Leff 1993). Commentatorsemphasise that it is not the policy of de-institutionalisation per se but its inadequateimplementation that is likely to be relevant to the growing number of people who are homelessand mentally ill (Herrman et al. 1989; Thornicroft and Bebbington 1989). Consequently, the lackof appropriate community support services and adequate housing, and poor co-ordination ofthese services for homeless people with mental illness, have been criticised (Thomas andMcCormack 1999). The relevance of these criticisms in Australia is supported by one of themain findings of the National Inquiry into the Human Rights of People with Mental Illness thatthere is a lack of appropriate housing and support to meet each person’s individual needs(Burdekin et al. 1993). We therefore examine the circumstances of people with psychosis whoare homeless or living in marginal accommodation and how these factors may be associated withtheir level of disability, social relationships and use of services.
1.7 The value of social networksNearly everyone wants and benefits from social relationships. People with psychosis are nodifferent (Young and Ensing 1999). Social support and social networks are important factors inhelping most people deal effectively with stress and life challenges. Supportive socialinteractions are associated with recovery from physical illness, emotional well-being and goodwork performance (Sarason et al. 1996). However, social isolation and loneliness is commonamong people with psychosis (Davidson and Stayner 1997).
Living with a psychotic disorder can be stressful in its own right. The recruitment of socialsupport is one coping skill that may moderate the negative effects of stressful life events (Henryand Coster 1996). However, people with psychosis often have marked deficits in socialfunctioning. Social dysfunction interferes with performance at work, within the family and in thewider social environment (Bellack 1997). In turn, social disability is a primary source of stress,and affects quality of life (Bellack 1997).
People with schizophrenia often have fewer social networks than other people and may havefewer opportunities to increase their social network (Albert et al. 1998). How this may be relatedto their functioning is relatively unexamined. In addition, most studies have not distinguishedbetween having friends and having family in defining social networks. Therefore it is difficult todetermine the separate effects of having either friends or family on functioning. The LPD studyoffers an opportunity to explore how contact with friends and/or family is associated with howpeople with psychosis are functioning.
Interactions between several aspects of the lived experience of psychosis are described in thisbulletin. These include the level of functioning in key life areas such as occupation and socialrelationships, and their interaction with a person’s living situation. For example, a person livingin a rooming house who is unemployed and has difficulties with their self care will have fewopportunities to meet new people or participate in recreational activities that open up new socialcontacts. Likewise, if finances are limited, it is harder for people to keep up with old friends. Wewill examine these interactions using the data from the LPD survey. Subsequent chapters of thisbulletin will consider disability, homelessness and social relationships for persons with psychosisin Australia. Recommendations are made concerning the implications for service delivery,training and education, research and public health.

6 Disability, homelessness and social relationships among people living with psychosis in Australia
1.8 Summary of aimsOur present aims are to:
• describe the profile of functioning in subgroups of people living with psychosis, as defined bykey demographic and clinical features (chapter two)
• describe the study population of those living with psychosis according to subgroups defined byaccommodation type, presenting a profile of their demographic and clinical characteristics,substance use, daily activities, social participation and quality of life (chapter three)
• present a detailed case study of people with psychosis living in marginal accommodation,based on findings from the Melbourne site (chapter four)
• describe the study population according to their social networks of family and friends, andexplore the relationship between social integration and personal and occupational functioning(chapter five).
Disability, homelessness and social relationships among people living with psychosis in Australia 7
2. Functioning and disability –relevant personal and clinicalfactors for people with psychosis
Over the past few decades the care of people with psychosis, in particular schizophrenia, hasshifted from psychiatric hospitals to community settings. The resulting demands of communityliving have posed additional challenges for those who are attempting to live with their psychosis.Adequate living skills are required for community living but are often lacking among people withpsychosis (Lesage et al. 1991). Hence, how well people are functioning in the community is animportant question, since adequate performance of activities of daily living is a fundamentalaspect of maintaining residential independence (Dickerson et al. 1999). Further, consumersreport that everyday living skills for tasks such as food preparation, maintenance of hygiene, andtaking care of one’s living space are important factors in their recovery process, as areestablishing a routine or taking part in exercise (Young and Ensing 1999). Friendship and socialsupport (Davidson et al. 1998), and having a meaningful occupational role (Mueser et al. 2001)are also highly valued by people with schizophrenia and other psychotic disorders who are livingin the community. Similarly, people with psychiatric disabilities (including those associated withpsychosis) who had lived in institutional care felt that a successful return to the community wasinfluenced by employment and support, as well as a desire to remain out of hospital and apositive sense of identity (Davidson et al. 1996).
The aim of this chapter is to describe the functioning and disability of people with psychosis,with particular reference to those activities that are important for recovery and successfulcommunity living. Functioning and disability have been defined according to those aspects of theICF framework (World Health Organisation 2001) that describe the activity and participation ofindividuals, and the contextual factors (personal and environmental), which interact with them inaffecting individuals’ functioning. The ICF framework encompasses the following components:
• Body functions and structures. These are defined as the physiological and psychologicalfunctions of the body systems, and the anatomical parts (structures) of the body, such asorgans, limbs and their components. Impairment is the term used to refer to problems in any ofthese body functions and structures.
• Activity. This refers to an individual’s execution of tasks or actions associated with activitiesin any area of life (for example, self care, domestic life, work, education, recreation,relationships), ranging from simple activities to complex and composite tasks that incorporateseveral simpler activities. Thus, activity is concerned with the person’s ability to carry outtasks in his or her environment – ie, what the person can do (McLaughlin-Gray 2001). Thus,the term ‘activity limitation’ is used to describe the difficulties a person may have executingtasks or actions in a life area.
• Participation. Participation differs from activity in that it describes the individual’sinvolvement with life situations, that is, what the person does in his or her environment acrossthe range of areas of life. It denotes the individual’s degree of involvement, incorporatingnotions of inclusion, acceptance and access to necessary resources for participation(McLaughlin-Gray 2001). Thus, society’s responses to individuals may be either to facilitateor to hinder participation in any area of life, and problems that individuals may experiencewith participation in life situations are referred to as participation restrictions.
8 Disability, homelessness and social relationships among people living with psychosis in Australia
• Contextual factors. These refer to the various personal and environmental factors that caninterfere with, or promote an individual’s functioning in a given context, reflectingacknowledgment of the significance of person-environment interaction to functioning andhealth (McLaughlin-Gray 2001). Personal factors refer to those aspects of a person’s particularbackground and life experience (for example, age, gender, educational and culturalbackground) that provide a context for current experience and functioning. Environmentalfactors include aspects of the physical, social and attitudinal environment that can act asbarriers or facilitators of a person’s activities and participation.
While functioning reflects the interaction between these components, disability is perhaps mosteasily observed as activity limitations, bearing in mind that impairments (for example, incognitive function) and participation restrictions may be contributing to these activity limitations.In this respect, social disadvantage could be seen as related to the individual (for example, his orher experiences of mental illness, activities and participation) and environmental barriers, such asthose related to stigma and social exclusion. Although this survey was not designed to take fullaccount of either the impairments or environmental factors relevant to functioning and disability,the findings regarding the nature and extent of participants’ activities and participation will bepresented with regard to contextual factors wherever possible. In addition, the public healthimplications of the findings will be explored.
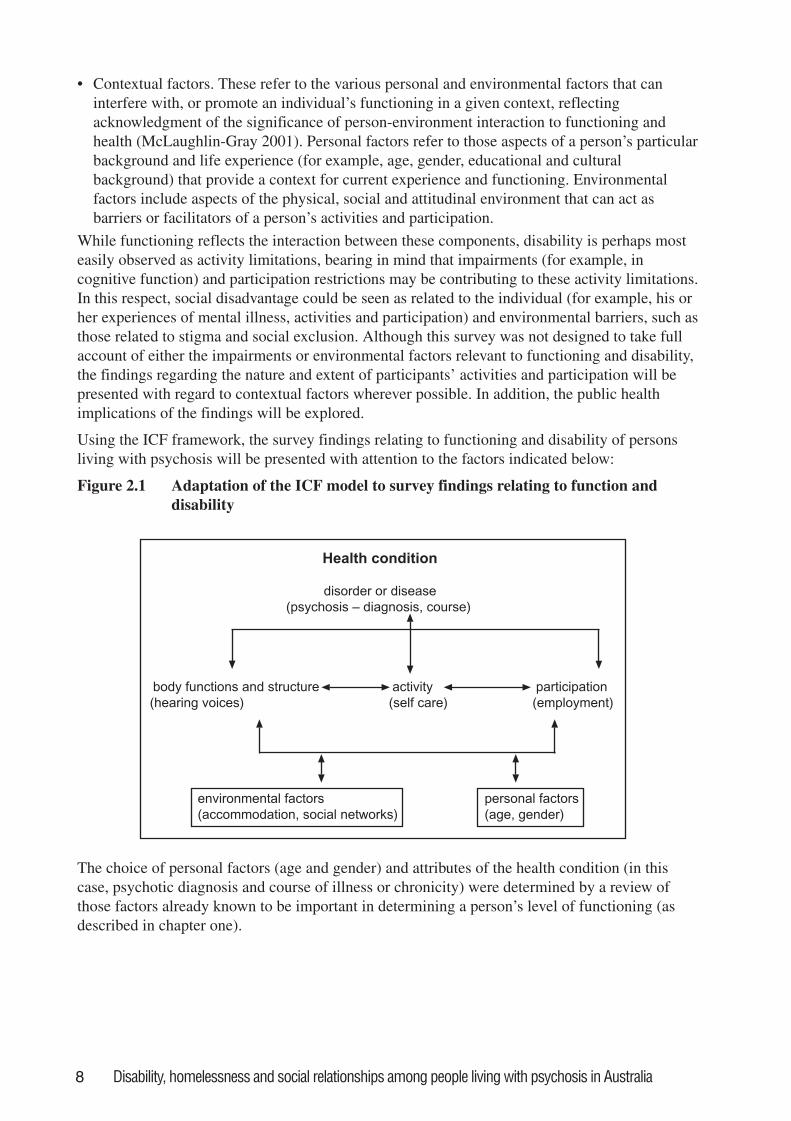
Using the ICF framework, the survey findings relating to functioning and disability of personsliving with psychosis will be presented with attention to the factors indicated below:
Figure 2.1 Adaptation of the ICF model to survey findings relating to function anddisability
Health condition
disorder or disease
(psychosis – diagnosis, course)
body functions and structure activity participation
(hearing voices) (self care) (employment)
environmental factors personal factors
(accommodation, social networks) (age, gender)
The choice of personal factors (age and gender) and attributes of the health condition (in thiscase, psychotic diagnosis and course of illness or chronicity) were determined by a review ofthose factors already known to be important in determining a person’s level of functioning (asdescribed in chapter one).
Disability, homelessness and social relationships among people living with psychosis in Australia 9
2.1 Measures and definitions used in this chapterThe disability questionnaire used in this survey (DIP-DIS) is composed of abridged sections ofthe WHO/DAS (World Health Organisation 1988), the Lancashire Quality of Life Profile (Oliveret al. 1997), and the Social Contact Questionnaire by Tucker (Tucker 1982). Appendix 1describes the development of the DIP-DIS together with its main features and properties,including inter-rater reliability.
The DIP-DIS allows for assessment of functioning over the preceding 12 months in the followingactivities:
• occupational performance – whether the person was less efficient in their work (either paidwork or housework or studies) than they would have liked to be, and whether they have beencriticised by others as a consequence
• household activities – doing things for the family or household that were normally expected ofthe person such as cleaning, washing up or cooking
• socialising – how the person was getting on with other people, including neighbours, membersof the family and people at work. The overall rating reflected the person’s perception of howsuccessful their social interactions were
• social withdrawal – whether the person preferred to be alone; whether the presence of othersbothered them. The overall rating reflected the degree of avoidance of social contacts
• quality of interpersonal relationships – whether the quality of interpersonal relationships hadimproved or deteriorated when compared to previous years. The rating estimated the changeover time in one or both of the previous categories
• intimate relationship* – whether the person had a close friend, that is, someone they could relyon for assistance or support if they needed. This can be taken as a proxy of social support
• sexual relationship* – whether the person was in a sexual relationship and whether they weresatisfied with this relationship.
* These ratings need to be interpreted with caution as these items had lower inter – raterreliability (see Appendix 1)
The following activities were assessed for the preceding month:
• self care – whether the person had put effort into their appearance, and was keeping fit andhealthy
• interests and information – whether the person was keeping up with what was happening inthe world, or with hobbies or interests.
After a series of semi-structured probes to establish relevant life circumstances, opportunities anddetails of functioning (past and current) of the person in each area, the interviewer then made arating that used all of the information.
All items, except ‘quality of interpersonal relationships’ were scored as:
• 0 (no dysfunction)
• 1 (obvious dysfunction)
• 2 (severe dysfunction).
Quality of interpersonal relationships was scored as:
• 0 (no deterioration perceived)
• 1 (deterioration due to subject’s health or loss of interest)
• 2 (deterioration due to other people’s loss of interest)
• 4 (improvement perceived).
10 Disability, homelessness and social relationships among people living with psychosis in Australia
A rating of 8 was made if an item was impossible to assess and 9 if not applicable. For example,8 was used if the rating was still uncertain after detailed questioning and probing, and 9 was usedif the person was not part of a household or was not in a sexual relationship.
Psychotic disorder was sub-divided according to the following diagnostic groupings:
• schizophrenia
• schizo-affective disorder
• delusional and other psychosis (‘other psychosis’ in the tables)
• bipolar disorder with manic episode(s). (For simplicity, referred to as ‘bipolar mania’ in thetext and tables hereafter.)
• psychotic depression
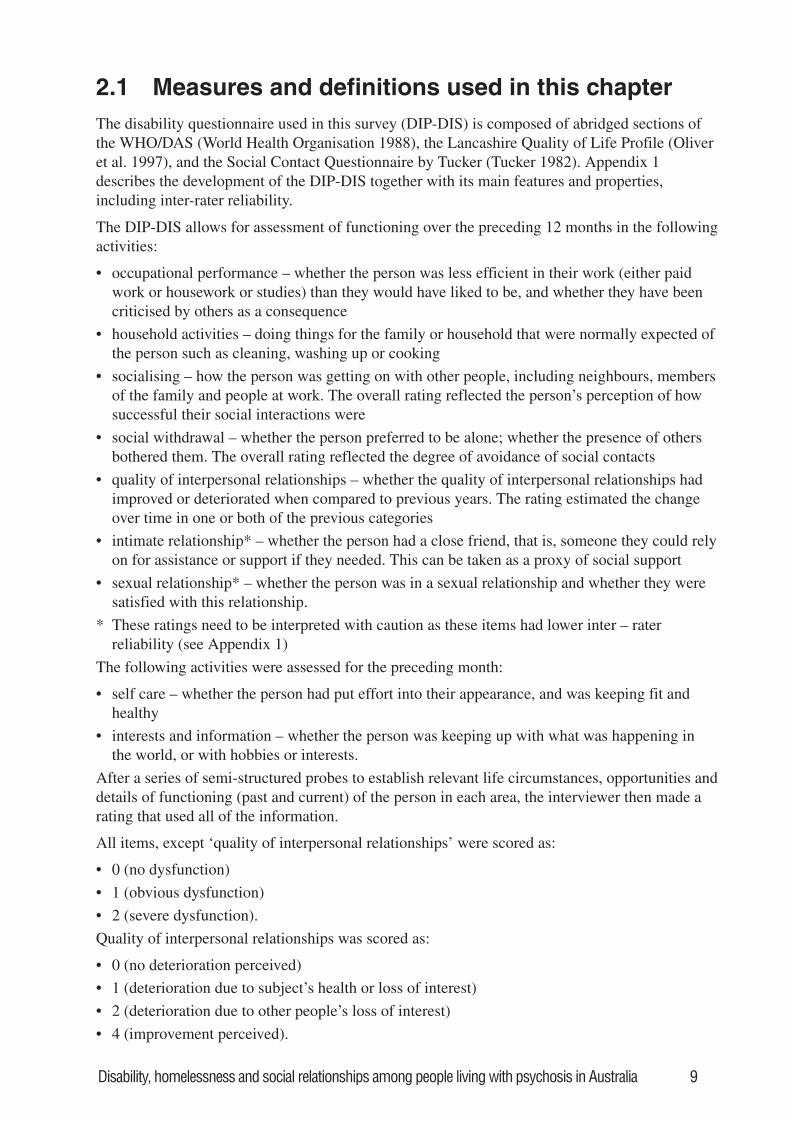
Figure 2.2. Categories used for classifying course of disorder, which also serve as a proxyfor severity of health care condition
Categories used in data collection Categories used in data presentation
Chronic illness little or nodeterioration
Multipleepisodes
Chronicepisodes
Multiple episodes withpartial recovery
Chronic illness withclear deterioration
Single episode goodrecovery
Singleepisode
Multiple episodes withgood recovery
The above categories serve as a proxy for severity of health condition. They were assignedcollaboratively through discussion between participants and interviewers. Diagrammaticrepresentations of these different types of course of disorder were used to guide the assignment.
2.1.1 Service useIn order to begin to understand our findings related to functioning and disability and theirimplications for service organisation and delivery, a summary of participants’ service use isprovided in this chapter. Even without a comprehensive assessment of the participants’ ownviews about their needs for services, this can be useful in beginning to draw inferences about
Disability, homelessness and social relationships among people living with psychosis in Australia 11
possible unmet needs. People were asked if they used the following services in the last 12months:
• medicine prescription
• information about mental illness and about treatment and available services
• psychotherapy, cognitive behavioural therapy, group therapy, counselling
• help to improve your ability to work, or to use your time in other ways
• help to sort out housing or money
• help to improve your ability to look after yourself or your home
• help to meet people for support and company.
These items were scored as:
• 0 (did receive service but needs not adequately met)
• 1 (did receive service and needs were adequately met).
Again, a rating of 8 was made if an item was impossible to assess and 9 if not applicable.
2.2 FindingsAll tables of findings appear at the end of this chapter. Table 2.1 summarises the socio-demographic characteristics of the participants in the LPD. The remaining tables report thepresence of dysfunction (either obvious dysfunction or severe dysfunction) among persons withpsychosis according to:
• age and gender (personal factors)
• diagnosis and course of disorder (aspects of health condition).
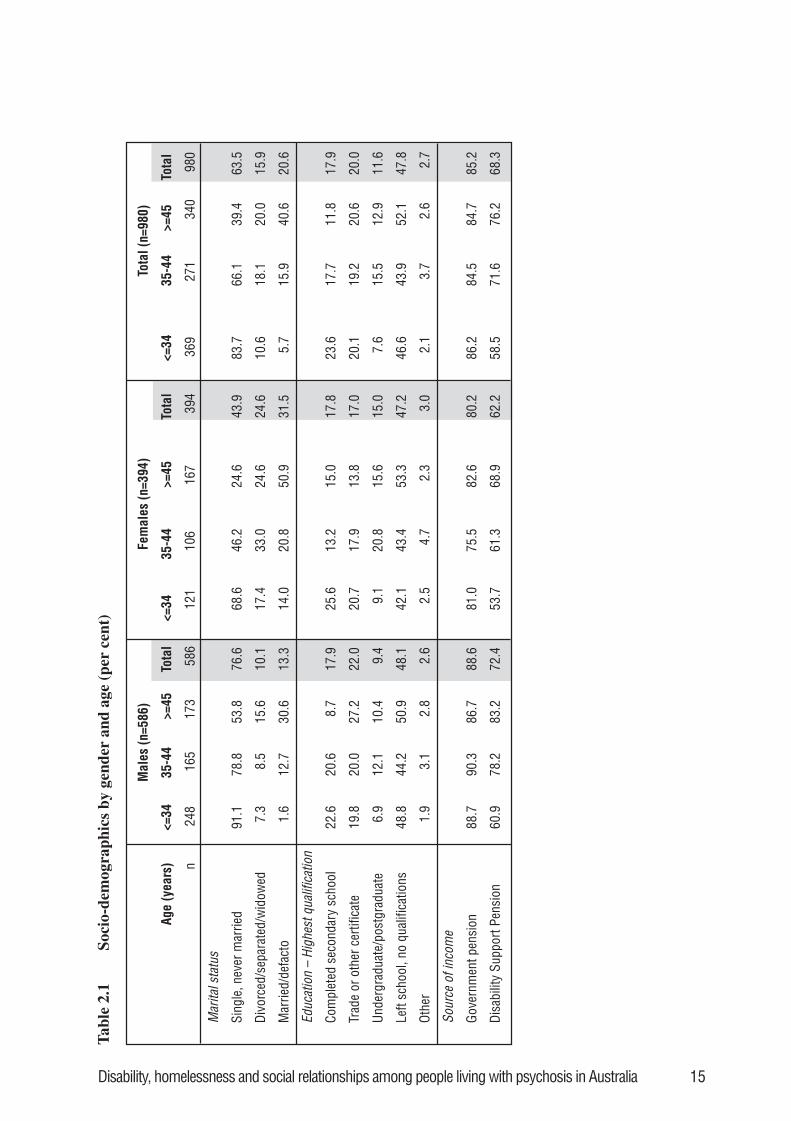
2.2.1 Socio-demographic characteristicsA total of 980 people participated in the study (586 men and 394 women), the overwhelmingmajority of whom met diagnostic criteria for psychosis (Jablensky et al. 1999b). Table 2.1summarises their socio-demographic characteristics. Most were single and had never married(64%); this was particularly so among men aged 34 years or younger (91%). Among femalesaged 45 and above, 51% were married or living in a defacto relationship. Just under half of thepeople interviewed had left school before obtaining qualifications. A somewhat higherproportion of people aged under 35 had completed secondary school (24%), compared withpeople aged 45 and above (12%). More than four out of five people were receiving a governmentpension, and 68% were receiving the Disability Support Pension.
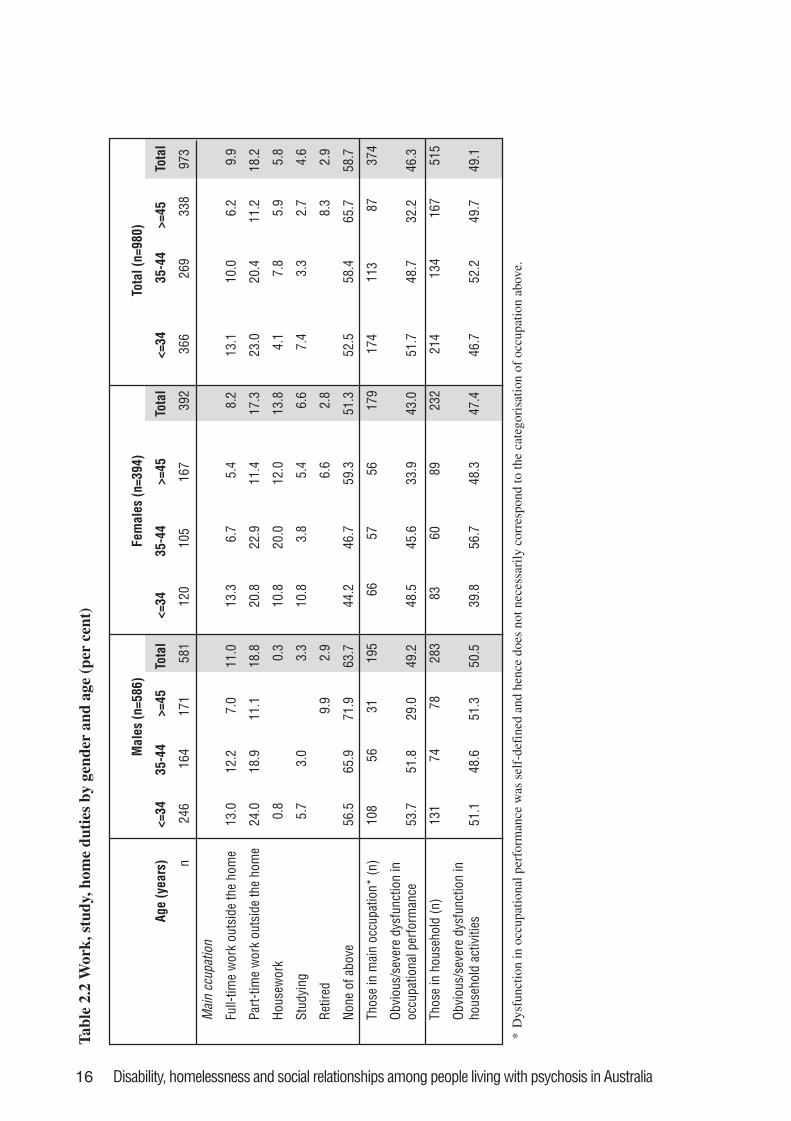
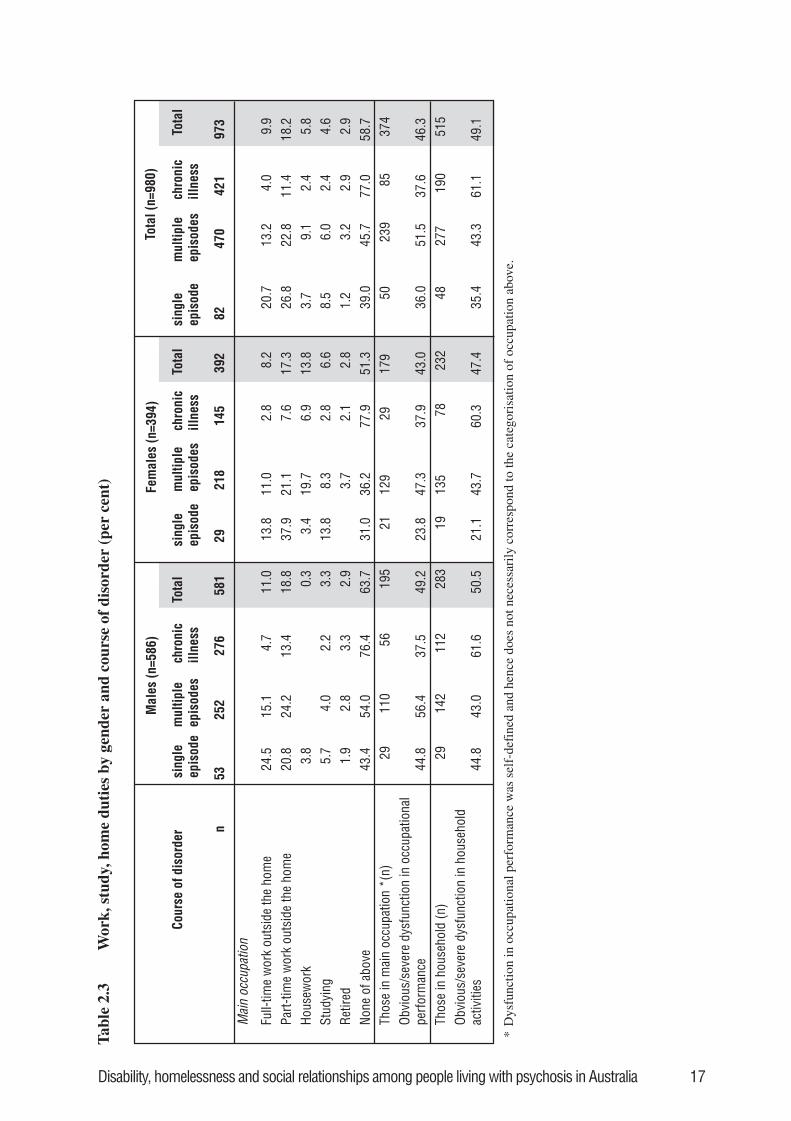
2.2.2 Work, study, and home dutiesTables 2.2, 2.3 and 2.4 describe participation in work, study and home duties. Overall, only 10%were participating in full-time, and 18% in part-time employment during the previous 12 months(Table 2.2). A slightly higher proportion of males was in full-time employment (11%) comparedwith females (8%). There was a progressive decline in the proportion of people engaged in full-time or part-time employment with increasing age. Involvement in employment declined withincreasing severity of psychosis as indicated by course of disorder (Table 2.3). Thus, those with asingle episode of psychosis had the highest levels of full-time and part-time work (21% and 27%,respectively) compared to only 4% and 11%, respectively, of those who had a more chronicillness. A lower proportion of people with a diagnosis of schizo-affective disorder (4%) were infull-time employment than people in other diagnostic groups (Table 2.4).
12 Disability, homelessness and social relationships among people living with psychosis in Australia
Small proportions of persons with psychosis participated in either housework (6%) or study(5%). The main difference between the groups was in gender roles, with a higher proportion offemales engaged in home duties (14%) than males (0.3%) and a higher proportion of femalesstudying (7%) than males (3%). See Table 2.2. People with chronic illness were less likely to beinvolved in either home duties or study (2% in both cases). See Table 2.3.
More than half of the sample was not involved in any work, study or home duties. Of the 374people (38%) who said they had some sort of occupation (paid work, study or home duties), 46%were rated as having activity limitations in this area (Table 2.2). Occupational dysfunction wasdefined as being less efficient in the preceding 12 months in their occupation than they wouldhave liked and receiving criticism about this from others (supervisors, work-mates, members ofthe household). A slightly higher proportion of males reported occupational dysfunction (49%)compared with females (43%). As seen in Table 2.4, those with schizophrenia and schizo-affective disorder reported the most occupational dysfunction among all the diagnostic groups(42% and 44%, respectively).
Household activities
Of those interviewed, 53% described themselves as part of a household. A much higherproportion of females (59%) compared with males (48%) were living in households (Table 2.2).Of the people experiencing a chronic course of illness, 45% were living in a household comparedwith 59% of people with a single episode (Table 2.3).
Those living in a household were asked about their ability to do things normally expected bytheir family or other members of the household (‘household activities’). As seen in Table 2.2, atotal of 49% of those in households said they were unable to do these tasks because of illness orloss of interest in such tasks. A slightly lower proportion of women (47%) reported havingproblems in this area compared with men (51%). Of those with chronic illness, 61% experiencedlimitations in performing household activities compared with 35% of those with a single episodeof illness (Table 2.3). There was no marked difference between the different psychotic diagnoseswhen men and women were considered together (Table 2.4). However, men with either psychoticdepression (67%) or delusional disorder and other psychoses (62%) more frequently reporteddifficulties with household activities than other diagnostic groups, whereas women with bipolarmania reported most limitations (56%), and those with delusional disorder and other psychosesreported least (43%).
2.2.3 Relationships with others, self care and outside interests
Socialising
Table 2.5 shows that the majority of interviewees (59%) were rated as having dysfunction insocialising, that is, they experienced a lack of success in their social interactions. A higherproportion of males (63%) compared with females (53%) was rated as having such difficulties.Increasing age seems to be associated with more disability in this area of functioning (Table 2.5),as does having a more chronic course of illness (Table 2.6). With respect to course of disorder,the group experiencing least success in socialising was males with chronic illness. Almost threeof every four (74%) in this group reported dysfunction in socialising. With respect to diagnosis,difficulties in socialising were most common among those with schizo-affective disorder (67%)and least common among those with bipolar mania (51%). See Table 2.7. The group with mostlimitations was males with psychotic depression (78%).
Social withdrawal
Fifty eight per cent of interviewees were rated as having obvious or severe social withdrawal(Table 2.5). Once again, a higher proportion of males (61%) compared with females (52%) were

Disability, homelessness and social relationships among people living with psychosis in Australia 13
rated as having problems in this area. Among people with chronic illness, 69% reported socialwithdrawal (Table 2.6). Consistent with the features of depression, a higher proportion of peoplewith psychotic depression (73%) reported social withdrawal than any other diagnostic categoryincluding schizophrenia (60%). This was most marked among males with psychotic depression(85%). See Table 2.7.
Intimate relationships
Over the preceding 12 months, 39% of participants lacked an intimate relationship (Table 2.5),with a higher proportion for males (44%) than females (32%). There was little variation acrossage groups, except the figure was considerably higher (38%) for women aged over 44 yearscompared with those under 35 years (28%) or those aged between 35 and 44 (25%). Many morepeople with a chronic course of illness (53%) reported the absence of an intimate relationshipcompared with those experiencing other courses of their disorder (Table 2.6). Table 2.7 indicatesthat a higher proportion of people diagnosed with schizophrenia (48%) did not have a closefriend compared with people with other diagnoses.
Sexual relationships
Nineteen per cent of those surveyed reported that they had no sexual relationship or noopportunity for one in the preceding year (Table 2.5). Of those in sexual relationships, 21%reported they were not satisfied or had problems in their sex life as a result of their illness. Therewere no real differences between men and women. Differences between those with differentcourses of disorder were less marked than for other aspects of social relationships, whilst peoplewith schizophrenia (15%) reported less dysfunction in this area than other diagnostic groups,despite being the least likely to report having intimate relationships (Table 2.7).
Self care
Obvious or severe dysfunction in self care was experienced by 30% of people living withpsychosis (Table 2.5). A higher proportion of males (34%) than females (24%) was rated ashaving dysfunction in this area. People aged 45 years and above were more likely to be rated ashaving difficulties in self care (34%), compared with people aged less than 35 years (27%) andthis was most evident among males (40%). A much higher proportion of people with a chronicillness course (43%) was assessed as having difficulties with self care compared with those witha single episode (17%). See Table 2.6. More people with schizophrenia (35%) had difficulties incaring for themselves than any of the other diagnostic groups (Table 2.7).
Outside interests
Outside interests were rated for the past month. Overall two out of five interviewees had obviousor severe dysfunction in relation to keeping up outside interests (Table 2.5). Men were morelikely to experience these kind of difficulties (42%) compared with women (36%). There wereno striking age differences. Chronicity of illness course had a large impact on people’s interest inthe outside world – 54% of those with a chronic course were not keeping up with eventscompared with 22% of people experiencing a single episode (Table 2.6). As shown in Table 2.7,more people with schizophrenia (45%) had dysfunction in this area than any other diagnosticgroup.
2.2.4 Service use
When discussing the range of disability among people with psychosis it is also important toexamine their service use (see section 2.1). Overall, most people were receiving prescribedmedication (91%), fewer people were receiving therapy or counselling (39%) and even fewerparticipated in rehabilitation or a day program (19%). See Table 2.8. People aged 45 years or

14 Disability, homelessness and social relationships among people living with psychosis in Australia
more were less likely to receive services such as provision of mental health information, therapyor counselling, or help to improve work skills and use of time. This is particularly striking giventhat older people were less likely to be meaningful occupied than their younger peers. Maleswere slightly more likely to receive guidance in housing and financial matters (36%) thanfemales (30%) and females were slightly more likely to receive counselling or therapy (43%)compared with males (37%).
People with a chronic course of illness were less likely to receive mental health information,therapy or counselling, or assistance with work skills or time use than people with a single ormultiple episodes of illness, but were more likely to receive assistance in managing housing andfinancial matters (Table 2.9). They were also less likely than those with multiple illness episodesto attend a rehabilitation or day program (17% and 22%, respectively).
With respect to diagnostic categories, people with psychotic depression and schizo-affectivedisorder were more likely to receive a service to improve their work or time use skills (Table2.10). People with schizophrenia were least likely to receive therapy or counselling (34%).People with psychotic depression (21%) and bipolar mania (24%) were less likely to havereceived services to assist with housing and financial matters. People with a diagnosis of bipolarmania were also less likely to receive assistance with self care compared with their peers withother diagnoses.
Disability, homelessness and social relationships among people living with psychosis in Australia 15
Tab
le 2
.1So
cio-
dem
ogra
phic
s by
gen
der
and
age
(per
cen
t)
Mal
es (n
=586
)Fe
mal
es (n
=394
)To
tal (
n=98
0)
Age
(yea
rs)
<=34
35-4
4>=
45To
tal
<=34
35-4
4>=
45To
tal
<=34
35-4
4>=
45To
tal
n24
816
517
358
612
110
616
739
436
927
134
098
0
Mar
ital s
tatu
s
Sing
le, n
ever
mar
ried
91.1
78.8
53.8
76.6
68.6
46.2
24.6
43.9
83.7
66.1
39.4
63.5
Divo
rced
/sep
arat
ed/w
idow
ed7.
38.
515
.610
.117
.433
.024
.624
.610
.618
.120
.015
.9
Mar
ried/
defa
cto
1.6
12.7
30.6
13.3
14.0
20.8
50.9
31.5
5.7
15.9
40.6
20.6
Educ
atio
n –
High
est q
ualif
icat
ion
Com
plet
ed s
econ
dary
sch
ool
22.6
20.6
8.7
17.9
25.6
13.2
15.0
17.8
23.6
17.7
11.8
17.9
Trad
e or
oth
er c
ertif
icat
e19
.820
.027
.222
.020
.717
.913
.817
.020
.119
.220
.620
.0
Unde
rgra
duat
e/po
stgr
adua
te6.
912
.110
.49.
49.
120
.815
.615
.07.
615
.512
.911
.6
Left
scho
ol, n
o qu
alifi
catio
ns48
.844
.250
.948
.142
.143
.453
.347
.246
.643
.952
.147
.8
Othe
r1.
93.
12.
82.
62.
54.
72.
33.
02.
13.
72.
62.
7
Sour
ce o
f inc
ome
Gove
rnm
ent p
ensi
on88
.790
.386
.788
.681
.075
.582
.680
.286
.284
.584
.785
.2
Disa
bilit
y Su
ppor
t Pen
sion
60.9
78.2
83.2
72.4
53.7
61.3
68.9
62.2
58.5
71.6
76.2
68.3
16 Disability, homelessness and social relationships among people living with psychosis in Australia
*D
ysfu
nctio
n in
occ
upat
iona
l per
form
ance
was
sel
f-de
fine
d an
d he
nce
does
not
nec
essa
rily
cor
resp
ond
to th
e ca
tego
risa
tion
of o
ccup
atio
n ab
ove.
Tabl
e 2.
2 W
ork,
stu
dy, h
ome
duti
es b
y ge
nder
and
age
(pe
r ce
nt)
Mal
es (n
=586
)Fe
mal
es (n
=394
)To
tal (
n=98
0)
Age
(yea
rs)
<=34
35-4
4>=
45To
tal
<=34
35-4
4>=
45To
tal
<=34
35-4
4>=
45To
tal
n24
616
417
158
112
010
516
739
236
626
933
897
3
Mai
n cc
upat
ion
Full-
time
wor
k ou
tsid
e th
e ho
me
13.0
12.2
7.0
11.0
13.3
6.7
5.4
8.2
13.1
10.0
6.2
9.9
Part-
time
wor
k ou
tsid
e th
e ho
me
24.0
18.9
11.1
18.8
20.8
22.9
11.4
17.3
23.0
20.4
11.2
18.2
Hous
ewor
k0.
80.
310
.820
.012
.013
.84.
17.
85.
95.
8
Stud
ying
5.7
3.0
3.3
10.8
3.8
5.4
6.6
7.4
3.3
2.7
4.6
Retir
ed9.
92.
96.
62.
88.
32.
9
None
of a
bove
56.5
65.9
71.9
63.7
44.2
46.7
59.3
51.3
52.5
58.4
65.7
58.7
Thos
e in
mai
n oc
cupa
tion*
(n)
108
5631
195
6657
5617
917
411
387
374
Obvi
ous/
seve
re d
ysfu
nctio
n in
occu
patio
nal p
erfo
rman
ce53
.751
.829
.049
.248
.545
.633
.943
.051
.748
.732
.246
.3
Thos
e in
hou
seho
ld (n
)13
174
7828
383
6089
232
214
134
167
515
Obvi
ous/
seve
re d
ysfu
nctio
n in
hous
ehol
d ac
tiviti
es51
.148
.651
.350
.539
.856
.748
.347
.446
.752
.249
.749
.1
Disability, homelessness and social relationships among people living with psychosis in Australia 17
Tab
le 2
.3W
ork,
stu
dy, h
ome
duti
es b
y ge
nder
and
cou
rse
of d
isor
der
(per
cen
t)
Mal
es (n
=586
)Fe
mal
es (n
=394
)To
tal (
n=98
0)
Cou
rse
of d
isor
der
sing
leep
isod
em
ultip
leep
isod
esch
roni
cill
ness
Tota
lsi
ngle
epis
ode
mul
tiple
epis
odes
chro
nic
illne
ssTo
tal
sing
leep
isod
em
ultip
leep
isod
esch
roni
cill
ness
Tota
l
n
5325
227
658
129
218
145
392
8247
042
197
3
Mai
n oc
cupa
tion
Full-
time
wor
k ou
tsid
e th
e ho
me
24.5
15.1
4.7
11.0
13.8
11.0
2.8
8.2
20.7
13.2
4.0
9.9
Part-
time
wor
k ou
tsid
e th
e ho
me
20.8
24.2
13.4
18.8
37.9
21.1
7.6
17.3
26.8
22.8
11.4
18.2
Hous
ewor
k3.
80.
33.
419
.76.
913
.83.
79.
12.
45.
8St
udyi
ng5.
74.
02.
23.
313
.88.
32.
86.
68.
56.
02.
44.
6Re
tired
1.9
2.8
3.3
2.9
3.7
2.1
2.8
1.2
3.2
2.9
2.9
None
of a
bove
43.4
54.0
76.4
63.7
31.0
36.2
77.9
51.3
39.0
45.7
77.0
58.7
Thos
e in
mai
n oc
cupa
tion
*(n)
2911
056
195
2112
929
179
5023
985
374
Obvi
ous/
seve
re d
ysfu
nctio
n in
occ
upat
iona
lpe
rfor
man
ce44
.856
.437
.549
.223
.847
.337
.943
.036
.051
.537
.646
.3Th
ose
in h
ouse
hold
(n)
2914
211
228
319
135
7823
248
277
190
515
Obvi
ous/
seve
re d
ysfu
nctio
n in
hou
seho
ldac
tiviti
es44
.843
.061
.650
.521
.143
.760
.347
.435
.443
.361
.149
.1
*D
ysfu
nctio
n in
occ
upat
iona
l per
form
ance
was
sel
f-de
fine
d an
d he
nce
does
not
nec
essa
rily
cor
resp
ond
to th
e ca
tego
risa
tion
of o
ccup
atio
n ab
ove.
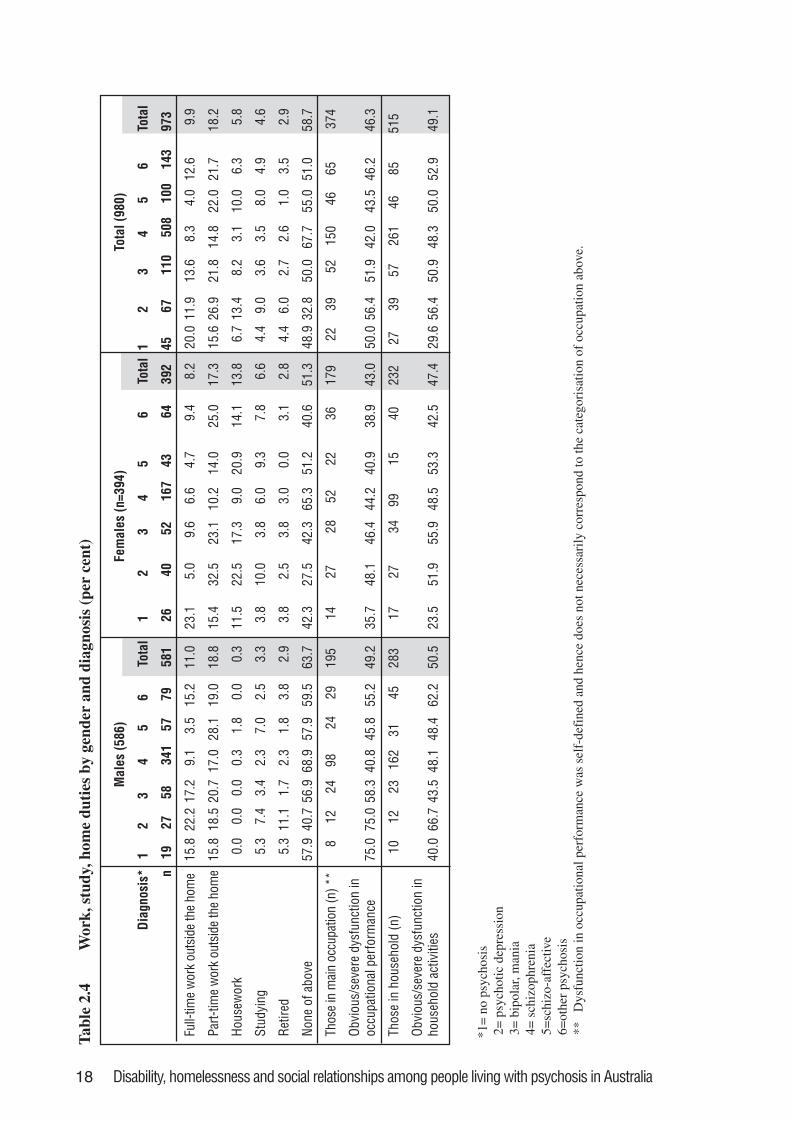
18 Disability, homelessness and social relationships among people living with psychosis in Australia
*1=
no
psyc
hosi
s 2
= p
sych
otic
dep
ress
ion
3=
bip
olar
, man
ia 4
= s
chiz
ophr
enia
5=
schi
zo-a
ffec
tive
6=
othe
r ps
ycho
sis
**
Dys
func
tion
in o
ccup
atio
nal p
erfo
rman
ce w
as s
elf-
defi
ned
and
henc
e do
es n
ot n
eces
sari
ly c
orre
spon
d to
the
cate
gori
satio
n of
occ
upat
ion
abov
e.
Tab
le 2
.4W
ork,
stu
dy, h
ome
duti
es b
y ge
nder
and
dia
gnos
is (
per
cent
)
Mal
es (5
86)
Fem
ales
(n=3
94)
Tota
l (98
0)
Dia
gnos
is*
12
34
56
Tota
l1
23
45
6To
tal
12
34
56
Tota
l
n19
2758
341
5779
581
2640
5216
743
6439
245
6711
050
810
014
397
3
Full-
time
wor
k ou
tsid
e th
e ho
me
15.8
22.2
17.2
9.1
3.5
15.2
11.0
23.1
5.0
9.6
6.6
4.7
9.4
8.2
20.0
11.9
13.6
8.3
4.0
12.6
9.9
Part-
time
wor
k ou
tsid
e th
e ho
me
15.8
18.5
20.7
17.0
28.1
19.0
18.8
15.4
32.5
23.1
10.2
14.0
25.0
17.3
15.6
26.9
21.8
14.8
22.0
21.7
18.2
Hous
ewor
k0.
00.
00.
00.
31.
80.
00.
311
.522
.517
.39.
020
.914
.113
.86.
713
.48.
23.
110
.06.
35.
8
Stud
ying
5.3
7.4
3.4
2.3
7.0
2.5
3.3
3.8
10.0
3.8
6.0
9.3
7.8
6.6
4.4
9.0
3.6
3.5
8.0
4.9
4.6
Retir
ed5.
311
.11.
72.
31.
83.
82.
93.
82.
53.
83.
00.
03.
12.
84.
46.
02.
72.
61.
03.
52.
9
None
of a
bove
57.9
40.7
56.9
68.9
57.9
59.5
63.7
42.3
27.5
42.3
65.3
51.2
40.6
51.3
48.9
32.8
50.0
67.7
55.0
51.0
58.7
Thos
e in
mai
n oc
cupa
tion
(n) *
*8
1224
9824
2919
514
2728
5222
3617
922
3952
150
4665
374
Obvi
ous/
seve
re d
ysfu
nctio
n in
occu
patio
nal p
erfo
rman
ce75
.075
.058
.340
.845
.855
.249
.235
.748
.146
.444
.240
.938
.943
.050
.056
.451
.942
.043
.546
.246
.3
Thos
e in
hou
seho
ld (n
)10
1223
162
3145
283
1727
3499
1540
232
2739
5726
146
8551
5
Obvi
ous/
seve
re d
ysfu
nctio
n in
hous
ehol
d ac
tiviti
es40
.066
.743
.548
.148
.462
.250
.523
.551
.955
.948
.553
.342
.547
.429
.656
.450
.948
.350
.052
.949
.1
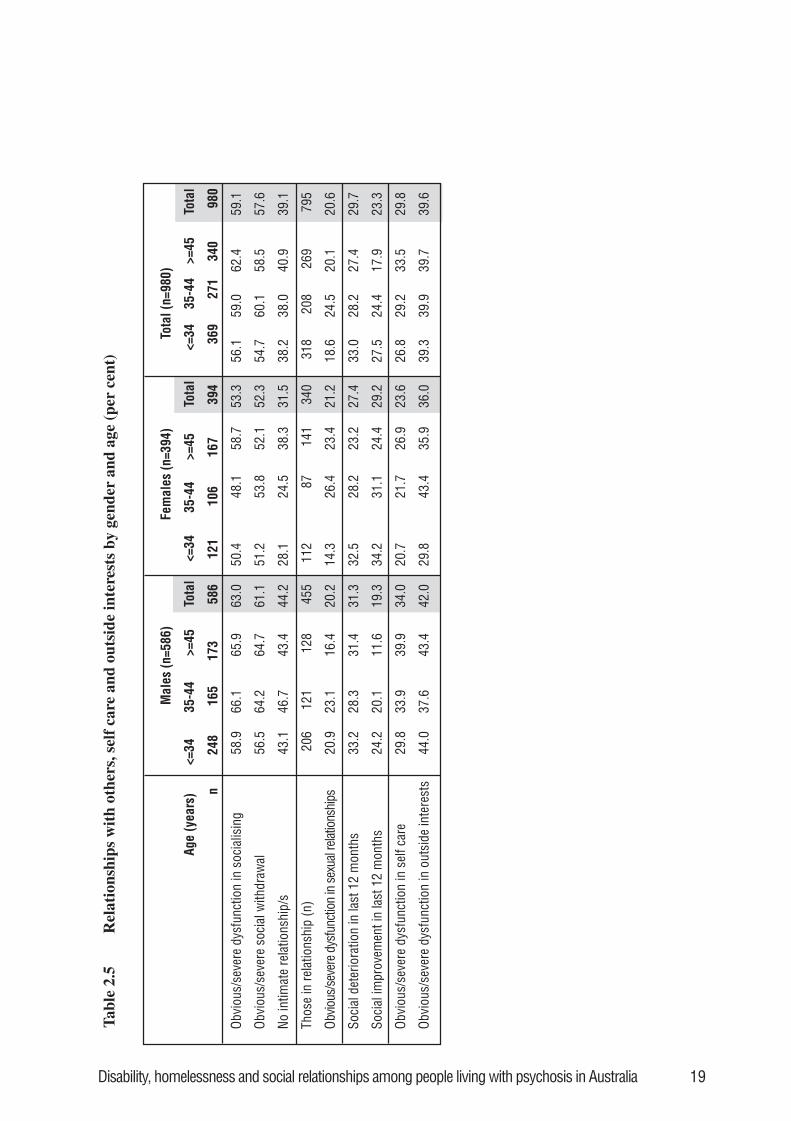
Disability, homelessness and social relationships among people living with psychosis in Australia 19
Tabl
e 2.
5R
elat
ions
hips
wit
h ot
hers
, sel
f ca
re a
nd o
utsi
de in
tere
sts
by g
ende
r an
d ag
e (p
er c
ent)
Mal
es (n
=586
)Fe
mal
es (n
=394
)To
tal (
n=98
0)
Age
(yea
rs)
<=34
35-4
4>=
45To
tal
<=34
35-4
4>=
45To
tal
<=34
35-4
4>=
45To
tal
n24
816
517
358
612
110
616
739
436
927
134
098
0
Obvi
ous/
seve
re d
ysfu
nctio
n in
soc
ialis
ing
58.9
66.1
65.9
63.0
50.4
48.1
58.7
53.3
56.1
59.0
62.4
59.1
Obvi
ous/
seve
re s
ocia
l with
draw
al56
.564
.264
.761
.151
.253
.852
.152
.354
.760
.158
.557
.6
No in
timat
e re
latio
nshi
p/s
43.1
46.7
43.4
44.2
28.1
24.5
38.3
31.5
38.2
38.0
40.9
39.1
Thos
e in
rela
tions
hip
(n)
206
121
128
455
112
8714
134
031
820
826
979
5
Obvio
us/s
ever
e dys
func
tion
in se
xual
relat
ions
hips
20.9
23.1
16.4
20.2
14.3
26.4
23.4
21.2
18.6
24.5
20.1
20.6
Soci
al d
eter
iora
tion
in la
st 1
2 m
onth
s33
.228
.331
.431
.332
.528
.223
.227
.433
.028
.227
.429
.7
Soci
al im
prov
emen
t in
last
12
mon
ths
24.2
20.1
11.6
19.3
34.2
31.1
24.4
29.2
27.5
24.4
17.9
23.3
Obvi
ous/
seve
re d
ysfu
nctio
n in
sel
f car
e29
.833
.939
.934
.020
.721
.726
.923
.626
.829
.233
.529
.8
Obvi
ous/
seve
re d
ysfu
nctio
n in
out
side
inte
rest
s44
.037
.643
.442
.029
.843
.435
.936
.039
.339
.939
.739
.6
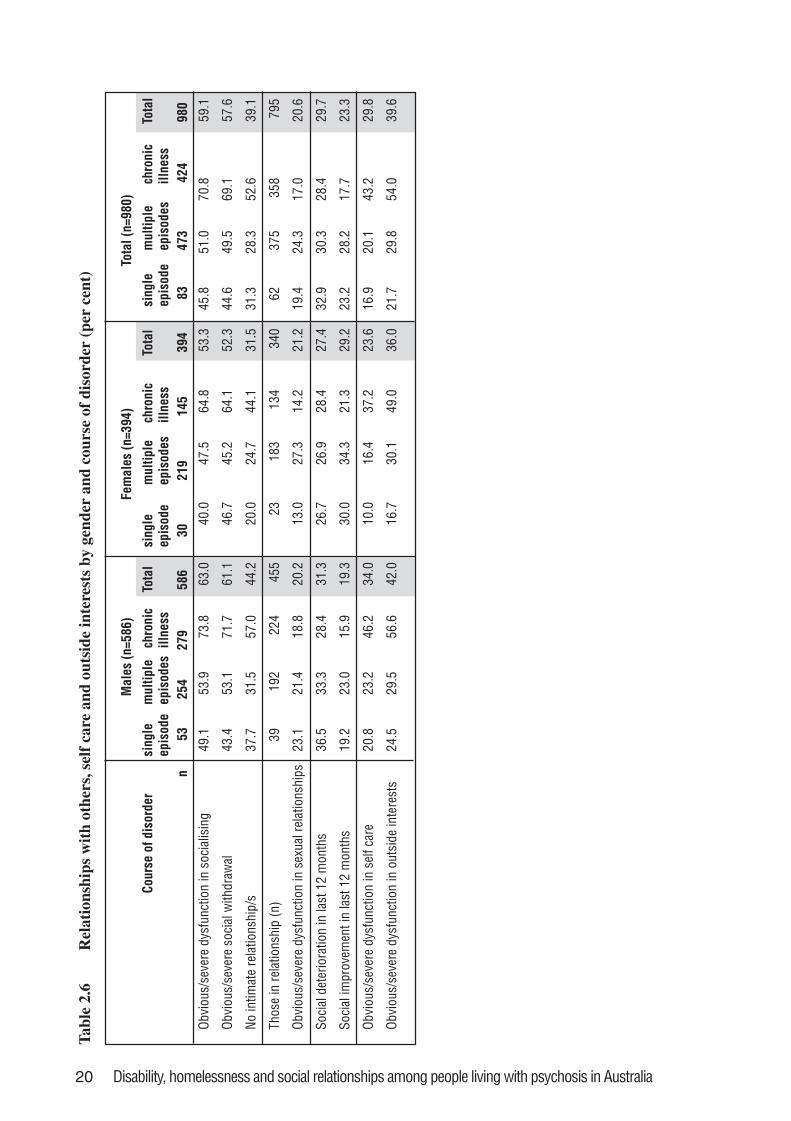
20 Disability, homelessness and social relationships among people living with psychosis in Australia
Tabl
e 2.
6R
elat
ions
hips
wit
h ot
hers
, sel
f ca
re a
nd o
utsi
de in
tere
sts
by g
ende
r an
d co
urse
of
diso
rder
(pe
r ce
nt)
Mal
es (n
=586
)Fe
mal
es (n
=394
)To
tal (
n=98
0)
Cour
se o
f dis
orde
rsi
ngle
epis
ode
mul
tiple
epis
odes
chro
nic
illne
ssTo
tal
sing
leep
isod
em
ultip
leep
isod
esch
roni
cill
ness
Tota
lsi
ngle
epis
ode
mul
tiple
epis
odes
chro
nic
illne
ssTo
tal
n53
254
279
586
3021
914
539
483
473
424
980
Obvi
ous/
seve
re d
ysfu
nctio
n in
soc
ialis
ing
49.1
53.9
73.8
63.0
40.0
47.5
64.8
53.3
45.8
51.0
70.8
59.1
Obvi
ous/
seve
re s
ocia
l with
draw
al43
.453
.171
.761
.146
.745
.264
.152
.344
.649
.569
.157
.6
No in
timat
e re
latio
nshi
p/s
37.7
31.5
57.0
44.2
20.0
24.7
44.1
31.5
31.3
28.3
52.6
39.1
Thos
e in
rela
tions
hip
(n)
3919
222
445
523
183
134
340
6237
535
879
5
Obvi
ous/
seve
re d
ysfu
nctio
n in
sex
ual r
elat
ions
hips
23.1
21.4
18.8
20.2
13.0
27.3
14.2
21.2
19.4
24.3
17.0
20.6
Soci
al d
eter
iora
tion
in la
st 1
2 m
onth
s36
.533
.328
.431
.326
.726
.928
.427
.432
.930
.328
.429
.7
Soci
al im
prov
emen
t in
last
12
mon
ths
19.2
23.0
15.9
19.3
30.0
34.3
21.3
29.2
23.2
28.2
17.7
23.3
Obvi
ous/
seve
re d
ysfu
nctio
n in
sel
f car
e20
.823
.246
.234
.010
.016
.437
.223
.616
.920
.143
.229
.8
Obvi
ous/
seve
re d
ysfu
nctio
n in
out
side
inte
rest
s24
.529
.556
.642
.016
.730
.149
.036
.021
.729
.854
.039
.6
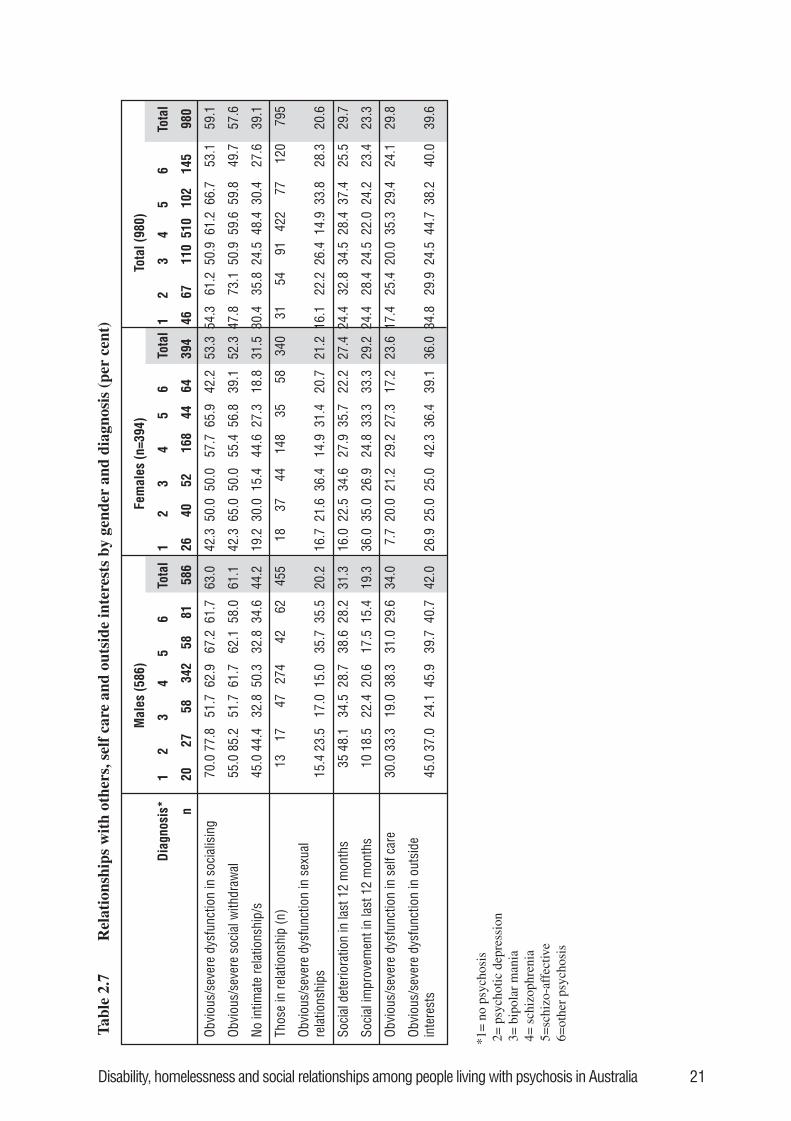
Disability, homelessness and social relationships among people living with psychosis in Australia 21
Tab
le 2
.7R
elat
ions
hips
wit
h ot
hers
, sel
f ca
re a
nd o
utsi
de in
tere
sts
by g
ende
r an
d di
agno
sis
(per
cen
t)
*1=
no
psyc
hosi
s 2
= p
sych
otic
dep
ress
ion
3=
bip
olar
man
ia 4
= s
chiz
ophr
enia
5=
schi
zo-a
ffec
tive
6=
othe
r ps
ycho
sis
Mal
es (5
86)
Fem
ales
(n=3
94)
Tota
l (98
0)
D
iagn
osis
*1
23
45
6To
tal
12
34
56
Tota
l1
23
45
6To
tal
n20
2758
342
5881
586
2640
5216
844
6439
446
6711
051
010
214
598
0
Obvi
ous/
seve
re d
ysfu
nctio
n in
soc
ialis
ing
70.0
77.8
51.7
62.9
67.2
61.7
63.0
42.3
50.0
50.0
57.7
65.9
42.2
53.3
54.3
61.2
50.9
61.2
66.7
53.1
59.1
Obvi
ous/
seve
re s
ocia
l with
draw
al55
.085
.251
.761
.762
.158
.061
.142
.365
.050
.055
.456
.839
.152
.347
.873
.150
.959
.659
.849
.757
.6
No in
timat
e re
latio
nshi
p/s
45.0
44.4
32.8
50.3
32.8
34.6
44.2
19.2
30.0
15.4
44.6
27.3
18.8
31.5
30.4
35.8
24.5
48.4
30.4
27.6
39.1
Thos
e in
rela
tions
hip
(n)
1317
4727
442
6245
518
3744
148
3558
340
3154
9142
277
120
795
Obvi
ous/
seve
re d
ysfu
nctio
n in
sex
ual
rela
tions
hips
15.4
23.5
17.0
15.0
35.7
35.5
20.2
16.7
21.6
36.4
14.9
31.4
20.7
21.2
16.1
22.2
26.4
14.9
33.8
28.3
20.6
Soci
al d
eter
iora
tion
in la
st 1
2 m
onth
s35
48.1
34.5
28.7
38.6
28.2
31.3
16.0
22.5
34.6
27.9
35.7
22.2
27.4
24.4
32.8
34.5
28.4
37.4
25.5
29.7
Soci
al im
prov
emen
t in
last
12
mon
ths
1018
.522
.420
.617
.515
.419
.336
.035
.026
.924
.833
.333
.329
.224
.428
.424
.522
.024
.223
.423
.3
Obvi
ous/
seve
re d
ysfu
nctio
n in
sel
f car
e30
.033
.319
.038
.331
.029
.634
.07.
720
.021
.229
.227
.317
.223
.617
.425
.420
.035
.329
.424
.129
.8
Obvi
ous/
seve
re d
ysfu
nctio
n in
out
side
inte
rest
s45
.037
.024
.145
.939
.740
.742
.026
.925
.025
.042
.336
.439
.136
.034
.829
.924
.544
.738
.240
.039
.6
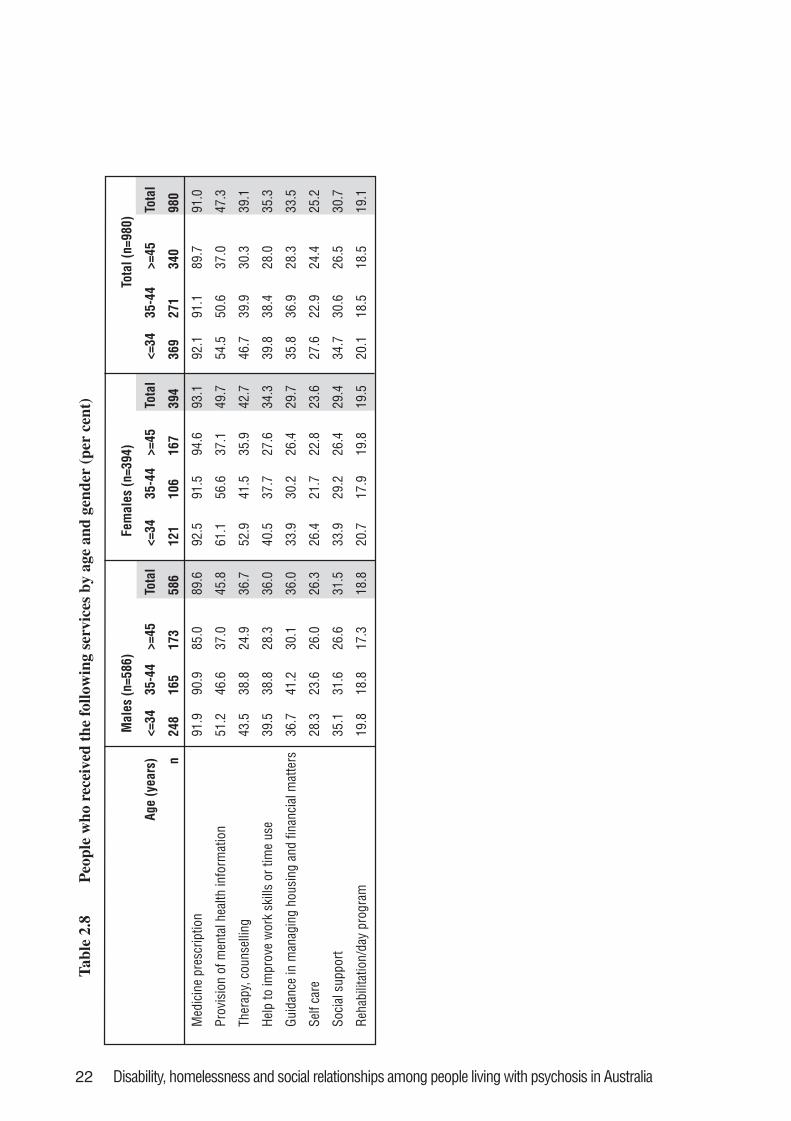
22 Disability, homelessness and social relationships among people living with psychosis in Australia
Tab
le 2
.8P
eopl
e w
ho r
ecei
ved
the
follo
win
g se
rvic
es b
y ag
e an
d ge
nder
(pe
r ce
nt)
Mal
es (n
=586
)Fe
mal
es (n
=394
)To
tal (
n=98
0)
Age
(yea
rs)
<=34
35-4
4>=
45To
tal
<=34
35-4
4>=
45To
tal
<=34
35-4
4>=
45To
tal
n24
816
517
358
612
110
616
739
436
927
134
098
0
Med
icin
e pr
escr
iptio
n91
.990
.985
.089
.692
.591
.594
.693
.192
.191
.189
.791
.0
Prov
isio
n of
men
tal h
ealth
info
rmat
ion
51.2
46.6
37.0
45.8
61.1
56.6
37.1
49.7
54.5
50.6
37.0
47.3
Ther
apy,
cou
nsel
ling
43.5
38.8
24.9
36.7
52.9
41.5
35.9
42.7
46.7
39.9
30.3
39.1
Help
to im
prov
e w
ork
skill
s or
tim
e us
e39
.538
.828
.336
.040
.537
.727
.634
.339
.838
.428
.035
.3
Guid
ance
in m
anag
ing
hous
ing
and
finan
cial
mat
ters
36.7
41.2
30.1
36.0
33.9
30.2
26.4
29.7
35.8
36.9
28.3
33.5
Self
care
28.3
23.6
26.0
26.3
26.4
21.7
22.8
23.6
27.6
22.9
24.4
25.2
Soci
al s
uppo
rt35
.131
.626
.631
.533
.929
.226
.429
.434
.730
.626
.530
.7
Reha
bilit
atio
n/da
y pr
ogra
m19
.818
.817
.318
.820
.717
.919
.819
.520
.118
.518
.519
.1
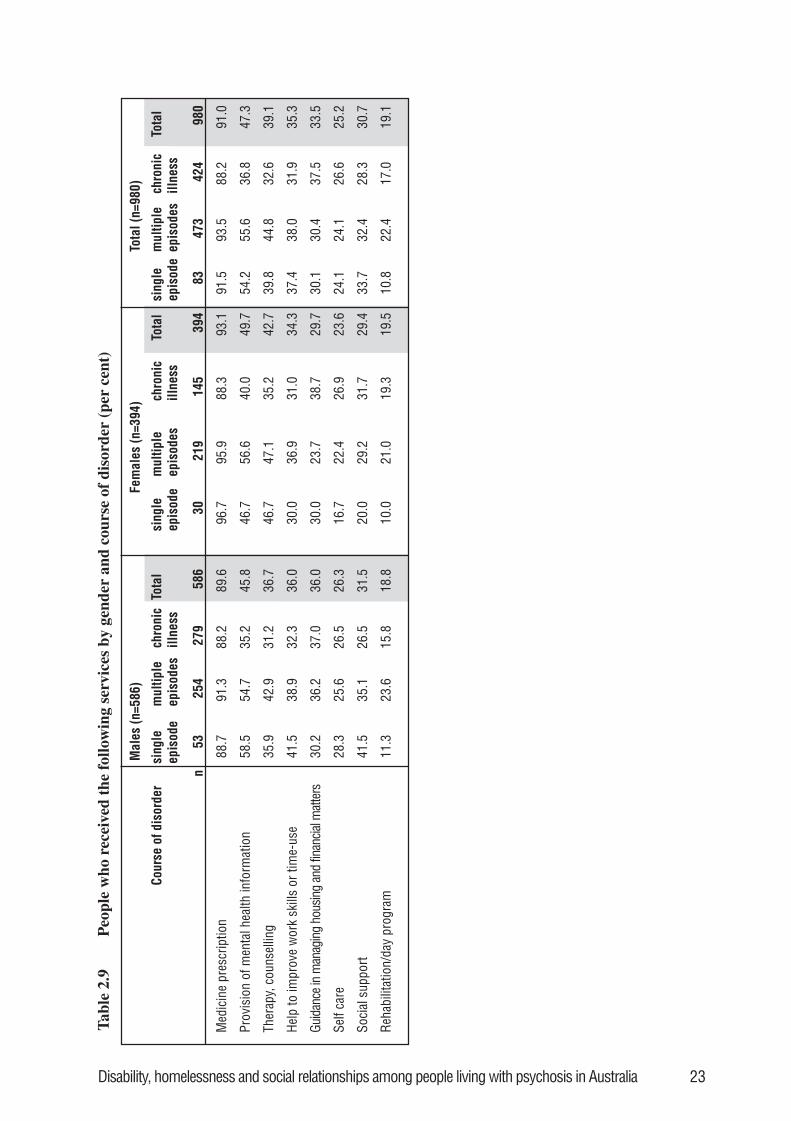
Disability, homelessness and social relationships among people living with psychosis in Australia 23
Tabl
e 2.
9P
eopl
e w
ho r
ecei
ved
the
follo
win
g se
rvic
es b
y ge
nder
and
cou
rse
of d
isor
der
(per
cen
t)
Mal
es (n
=586
)Fe
mal
es (n
=394
)To
tal (
n=98
0) chro
nic
illne
ssTo
tal
n
5325
427
958
630
219
145
394
8347
342
498
0
Med
icin
e pr
escr
iptio
n88
.791
.388
.289
.696
.795
.988
.393
.191
.593
.588
.291
.0
Prov
isio
n of
men
tal h
ealth
info
rmat
ion
58.5
54.7
35.2
45.8
46.7
56.6
40.0
49.7
54.2
55.6
36.8
47.3
Ther
apy,
cou
nsel
ling
35.9
42.9
31.2
36.7
46.7
47.1
35.2
42.7
39.8
44.8
32.6
39.1
Help
to im
prov
e w
ork
skill
s or
tim
e-us
e41
.538
.932
.336
.030
.036
.931
.034
.337
.438
.031
.935
.3
Guid
ance
in m
anag
ing
hous
ing
and
finan
cial m
atte
rs30
.236
.237
.036
.030
.023
.738
.729
.730
.130
.437
.533
.5
Self
care
28.3
25.6
26.5
26.3
16.7
22.4
26.9
23.6
24.1
24.1
26.6
25.2
Soci
al s
uppo
rt41
.535
.126
.531
.520
.029
.231
.729
.433
.732
.428
.330
.7
Reha
bilit
atio
n/da
y pr
ogra
m11
.323
.615
.818
.810
.021
.019
.319
.510
.822
.417
.019
.1
Cour
se o
f dis
orde
rsi
ngle
epis
ode
mul
tiple
epis
odes
chro
nic
illne
ssTo
tal
sing
leep
isod
em
ultip
leep
isod
esch
roni
cill
ness
Tota
lsi
ngle
epis
ode
mul
tiple
epis
odes
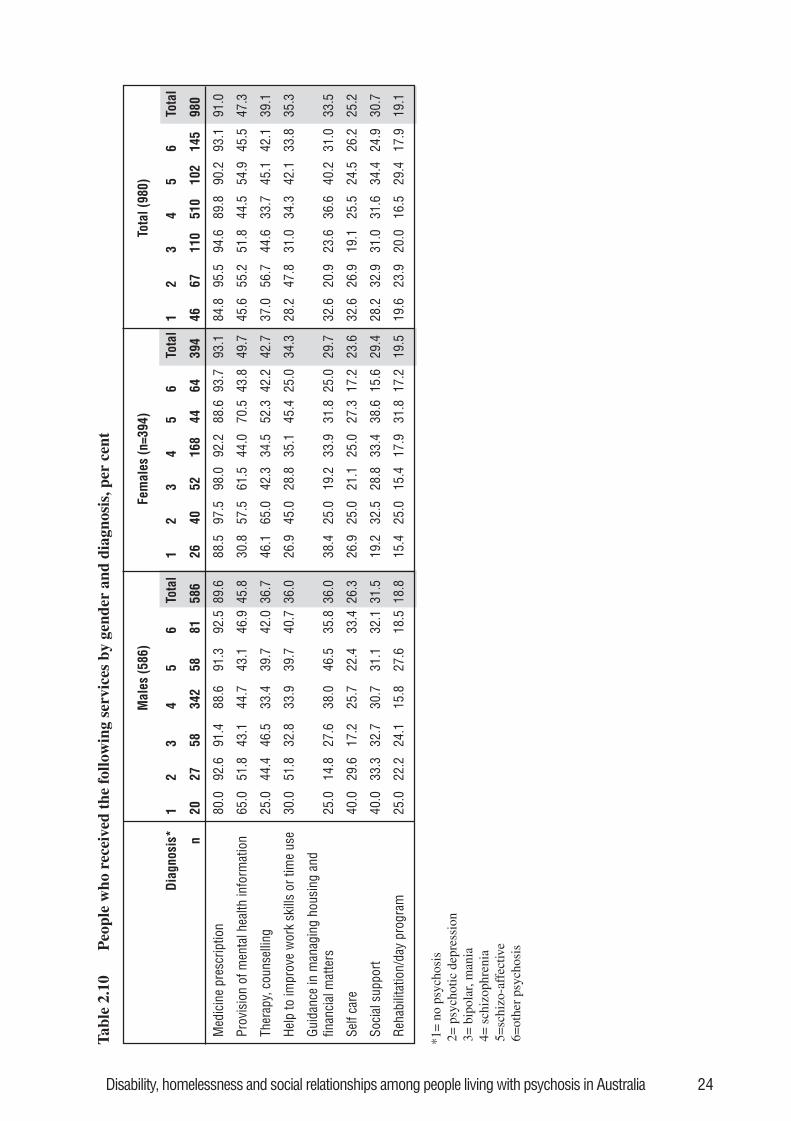
Disability, homelessness and social relationships among people living with psychosis in Australia 24
Tabl
e 2.
10P
eopl
e w
ho r
ecei
ved
the
follo
win
g se
rvic
es b
y ge
nder
and
dia
gnos
is, p
er c
ent
*1=
no
psyc
hosi
s 2
= p
sych
otic
dep
ress
ion
3=
bip
olar
, man
ia 4
= s
chiz
ophr
enia
5=
schi
zo-a
ffec
tive
6=
othe
r ps
ycho
sis
Mal
es (5
86)
Fem
ales
(n=3
94)
Tota
l (98
0)
Dia
gnos
is*
12
34
56
Tota
l1
23
45
6To
tal
12
34
56
Tota
l
n
2027
5834
258
8158
626
4052
168
4464
394
4667
110
510
102
145
980
Med
icin
e pr
escr
iptio
n80
.092
.691
.488
.691
.392
.589
.688
.597
.598
.092
.288
.693
.793
.184
.895
.594
.689
.890
.293
.191
.0
Prov
isio
n of
men
tal h
ealth
info
rmat
ion
65.0
51.8
43.1
44.7
43.1
46.9
45.8
30.8
57.5
61.5
44.0
70.5
43.8
49.7
45.6
55.2
51.8
44.5
54.9
45.5
47.3
Ther
apy,
cou
nsel
ling
25.0
44.4
46.5
33.4
39.7
42.0
36.7
46.1
65.0
42.3
34.5
52.3
42.2
42.7
37.0
56.7
44.6
33.7
45.1
42.1
39.1
Help
to im
prov
e w
ork
skill
s or
tim
e us
e30
.051
.832
.833
.939
.740
.736
.026
.945
.028
.835
.145
.425
.034
.328
.247
.831
.034
.342
.133
.835
.3
Guid
ance
in m
anag
ing
hous
ing
and
finan
cial
mat
ters
25.0
14.8
27.6
38.0
46.5
35.8
36.0
38.4
25.0
19.2
33.9
31.8
25.0
29.7
32.6
20.9
23.6
36.6
40.2
31.0
33.5
Self
care
40.0
29.6
17.2
25.7
22.4
33.4
26.3
26.9
25.0
21.1
25.0
27.3
17.2
23.6
32.6
26.9
19.1
25.5
24.5
26.2
25.2
Soci
al s
uppo
rt40
.033
.332
.730
.731
.132
.131
.519
.232
.528
.833
.438
.615
.629
.428
.232
.931
.031
.634
.424
.930
.7
Reha
bilit
atio
n/da
y pr
ogra
m25
.022
.224
.115
.827
.618
.518
.815
.425
.015
.417
.931
.817
.219
.519
.623
.920
.016
.529
.417
.919
.1
Disability, homelessness and social relationships among people living with psychosis in Australia 25
2.3 ConclusionsThe LPD study - a prevalence study of psychotic disorders in selected urban areas acrossAustralia - was designed with a particular focus on ‘treated’ point prevalence, that is, on thenumber and characteristics of people using specialised mental health services (Jablensky et al.2000). While sampling for interview was random within each source of recruitment (inpatients,outpatients etc.), inpatients were over-represented and out patients under-represented in the finalinterviewed sample compared to their actual numbers within the population. Thus, theinterviewed sample was somewhat weighted towards those with more severe illness, which needsto be taken into account in the interpretation of the findings that follow (Jablensky et al. 2000).Nevertheless, the LPD study did interview individuals with psychosis who were experiencingless disability, and in many respects had recovered, many of whom were among 173 participantswho were predominantly or exclusively under the care of GPs or private psychiatrists.
Notwithstanding the above caveats, it is clear that a substantial number of people with psychosisexperience activity limitations and participation restrictions in key life areas. This is particularlyso for those men and women with persisting psychosis. Despite this, very few participate inrehabilitation programs that have the potential to address these difficulties through individuallytailored pharmacological, psychological, social and occupation-focused therapies. With respectto schizophrenia, a number of such therapies with substantial evidence of efficacy have beenidentified (Mojtabai et al. 1998) and incorporated into a series of treatment recommendations(Lehman et al. 1998). The first report from this LPD study noted that less than one-fifth ofinterviewees in the LPD survey participated in a rehabilitation or a day hospital program duringthe previous year (Jablensky et al. 1999b). Only 62 people (6% of the sample) had been involvedin such programs for 6-12 months, and only 21 people had been involved in programs run over 5days per week (Jablensky et al. 1999b). As highlighted in that report, mental health services arepredominantly providing pharmacological treatments, with relatively little emphasis on the othertherapies. This is particularly true for those people experiencing persisting illness and this is ofconcern, not only because they generally experience the most disability, but because there issome evidence that psychosocial treatments are more beneficial in the later stages of illness(Mojtabai et al. 1998).
The findings indicate that those with single episodes of psychosis have a higher level offunctioning in nearly all areas compared with people with chronic illness. The trajectories ofrecovery from psychosis are many and varied and it is apparent that substantial recovery orconsiderable improvement is expected in the majority of patients (EPPIC 2001). Nevertheless,between 10% and 20% of people with a first episode of psychosis do not achieve remission ofsymptoms after 12 months (Lieberman et al. 1993; Edwards et al. 1998) with the possibility ofcontinued disruption to social, interpersonal and occupational role functioning (McGlashan1988; EPPIC 2001). At present, rehabilitation programs are considered only when people areexperiencing established difficulties in a number of areas and, as already indicated, relatively fewpeople have access to such programs. There is emerging evidence that effective treatment andspecialised psychosocial interventions should be considered and instituted at an early stage ofillness to improve functioning and minimise further deterioration (EPPIC 2001).
Only 10% of people with psychosis reported full-time employment and a further 18% were inpart-time employment in the last 12 months. Employment is an important component of adultlife and self-identity, providing socially valued roles for most people. The psychological,physical and social impact of unemployment must therefore be considerable, as it is in those whoare not psychotic (Marsden and Duff 1975). Much of this may be avoidable as experienceelsewhere in the world has shown that a much higher proportion of people with serious mentalillness, including psychotic disorders, can be meaningfully employed (Warner 1999; Frost et al.2002).
26 Disability, homelessness and social relationships among people living with psychosis in Australia
The findings indicate that it is less likely that older people who are living with psychosis are inemployment. This may partly reflect the progression or chronicity of the illness and the impact ofsecondary disability. It may also reflect the general experience of those who have periods ofunemployment that, the longer one is unemployed, the less common and perhaps the harder it isto re-enter the workforce.
Other meaningful occupations in which people may participate include study. This could be aviable alternative to work for many people with psychosis, and indeed one which could assistthem to re-enter the workforce in the longer term. However, a low proportion of people withpsychosis was undertaking any course of studies. Indeed, most participants in this studyidentified no major occupation, suggesting that boredom and under-activity are likely to becontributing to diminished well-being and quality of life. This is an under-recognised problem inthe community, although the adverse impact of impoverished social environments in mentalhospitals (providing few opportunities for meaningful activity) was first recognised many yearsago (Wing and Brown 1970). It was assumed that the problem of under-stimulating environmentsin large psychiatric institutions would be solved by de-institutionalisation-when most people withmental illness would continue to live in the community. However, even when occupied, almosthalf of those interviewed experienced some occupational dysfunction, suggesting an inadequatefit between motivation, interest, skills and other personal attributes and the nature and challengeof the available occupations.
People with schizophrenia and schizo-affective disorder are less likely to be employed comparedwith others with psychotic disorders. There are a number of possible explanations for this. Thegreater impact of these disorders on people’s ability to perform in the workplace (for example,with regard to specific symptoms and associated cognitive impairment) may be relevant. Thismay also be due to greater stigma associated with these conditions, meaning their opportunitiesfor participation in work are more restricted.
Women appear to function better than men in caring for themselves, social relationships andmaintaining interest in the outside world. This is consistent with other studies, especially ofpeople with schizophrenia, suggesting that women often experience better functional outcomesthan men.
The association between a person’s diagnosis and level of functioning varies according to thetype of activity in question. Those with bipolar mania and delusional disorder and otherpsychoses generally fared better than those with any other psychotic diagnosis. In areas such asself care and interest in the outside world, people living with affective disorders (both psychoticdepression and bipolar mania) are experiencing fewer difficulties than those with non-affectivedisorders. A different picture emerged for difficulties with participating in household activities.Here, men with psychotic depression and women with bipolar mania were most incapacitated.Thus, it cannot be assumed that people with affective psychoses function uniformly better thanthose with non-affective psychoses, or vice versa.
2.4 Recommendations2.4.1 The extensive disability among people living with psychosis in Australia, reflected in
their activity limitations and restricted participation in many aspects of community life asdocumented here, needs to be addressed. Given the limited involvement of this populationin rehabilitation programs that might address these needs, greater access to such programsand/or treatments with a rehabilitation or recovery focus appears to be much needed. TheNational Mental Health Strategy and state planning frameworks should reflect this need,and federal and state mental health resources should support the development of suchprograms by mental health services and the psychiatric disability support sector.
Disability, homelessness and social relationships among people living with psychosis in Australia 27
2.4.2 Greater consideration should be given to the impact of under-activity and boredom onpeople with psychosis living in the community. Access to a variety of meaningfuloccupations is required. This will necessitate a number of systemic changes. Examplesinclude public education initiatives to ensure that those with psychosis have equal accessto the range of activities available to others in their community. Policies and legislationneed to be reviewed to ensure that financial barriers to meaningful occupation andcommunity re-integration do not continue to exist.
2.4.3 Not enough is known about the mechanisms that underlie people’s difficulties infunctioning in the context of psychotic illness (for example, whether difficulties arerelated to volition, skills or context). Thus, it is not always clear what the focus of theclinical intervention should be (for example, whether improving someone’s socialintegration would assist with his or her daily living skills). Research into these issueswould advance our understanding and assist services to develop more effectiveinterventions.
2.4.4 It should be acknowledged that difficulties in daily living skills might result from mentalas well as physical illness or impairments. People with mental illness therefore shouldhave equal access to services provided by the joint federal and state program, Home andCommunity Care (HACC). These services include housekeeping, the provision of meals,personal care and home nursing services, and provision of environmental supports toenable people to compensate for their difficulties.
2.4.5 Much is already known about what works well in case management and in rehabilitation –specifically about the psychosocial interventions that may alleviate some of these reporteddifficulties in functioning. Such interventions include cognitive behaviour therapy fordepression and the positive symptoms of psychosis, and family interventions in seriousmental illness. Given the prevalence of functional difficulties, more attention should begiven to ensuring that mental health workers are fully trained in the use of treatments thatare known to be effective and that case managers can call on other clinicians and serviceproviders with the necessary skills and resources.
2.4.6 There is further scope for research into the effective ingredients of both case managementand rehabilitation. Since disability among people living with psychosis is relativelywidespread, there is a need for greater understanding about how this can be addressedwithin the specific framework of mental health and other services in Australia. This willrequire research into, and evaluation of, services to understand how best to implementcurrent research evidence about recovery from psychosis in ‘the real world’.
2.4.7 Research that examines relevant environmental and personal barriers is required toexplore the issues that prevent people with psychosis from gaining and retainingmeaningful occupation. Research should aim to increase understanding of lowered self-image/self-esteem, and how it may result from interaction between other personal factors,the illness itself and social factors during the course of illness. Without a fullunderstanding of all relevant barriers to meaningful occupation, it is difficult to designappropriate rehabilitation and vocational programs that facilitate the recovery of self-efficacy, through the acquisition of work and other occupations.
2.4.8 Rehabilitation should be available at all stages of psychotic illness to treat and prevent thedevelopment of functional difficulties. Both adult mental health services and services forearly intervention in psychosis should ensure that prevention of disability andrehabilitation of skills are key priorities for service delivery.
28 Disability, homelessness and social relationships among people living with psychosis in Australia
2.4.9 Most people with psychosis require assistance either to retain or regain employment.Younger people often need assistance to gain skills for employment, especially whenillness disrupts their education. They might also require assistance to retain their jobs inthe face of continuing episodes of disorder. Such assistance might be both at the systemiclevel (such as greater employer awareness of mental health issues or flexible workingpractices) and at the individual level (such as refreshing skills lost during relapse orattention to lowered self-esteem and confidence in one’s abilities). There are specificissues for older people with psychosis – reflected in the higher proportion of unemployedin this age group – who require more targeted interventions. If unemployed for some time,as experienced by the wider community, the obstacles for such people re-entering theworkplace are greater. This is compounded by their (often) more severe disability as aresult of their experience of longer duration of illness. More detailed and specificrecommendations regarding employment, vocational training and education are outlinedin the companion bulletin (Frost et al. 2002).
Disability, homelessness and social relationships among people living with psychosis in Australia 29
3. Disability, service use and quality oflife among people living in differenttypes of housing across Australia
One of the biggest obstacles in the lives of people with mental illness is the absence of adequateaffordable and secure accommodation. Living with a mental illness - or recovering from it - isdifficult even in the best circumstances. Without a decent place to live it is virtually impossible.(Burdekin et al. 1993, p.337)
Adequate housing is widely acknowledged as a fundamental human right. Housing oraccommodation type has been viewed as a variable indicating the level of socio-economicdisadvantage. It is also recognised as an indicator of quality of life (Young and Ensing 1999).Using a prevailing Australian cultural norm about what constitutes desirable housing, mostpeople would prefer to live in a dwelling that has a room to sleep in, a room to live in, one’s ownkitchen and bathroom, and some security of tenure (Chamberlain and Mackenzie 1998). Peoplewith psychosis may be no different in ascribing to this cultural norm, as a recent Australian studyfound that people with psychiatric disabilities preferred living in their own home after whichgovernment subsidised housing was preferred. Interestingly, low cost rooming houseaccommodation was preferred over housing with psychiatric support. Homelessness, long-termhospitalisation and crisis accommodation were the least preferred living arrangements. Featuresof accommodation that were most highly valued in addition to shelter were safety, privacy andthe provision of food (Owen et al. 1996). Furthermore, access to appropriate housing has beenrecognised as an important aspect in the success or failure of a person living with mental illnessremaining in the community. Unsuitable accommodation, or none at all, can erode or destroy thebenefits of treatment or rehabilitation received in hospital (Burdekin et al. 1993). Hence, for allthese reasons, an examination of the profile of people living with psychosis in different types ofaccommodation is very informative.
The purpose of this chapter is to describe the following characteristics of people living withpsychosis grouped according to their main accommodation type in the last 12 months:
• socio-demographic characteristics• clinical features• substance use• disability profile• service use• quality of life.
In chapter 4, special emphasis will be given to people living in marginal accommodation inMelbourne. The reason for highlighting this group is that the methods used in Melbourneinvolved a stratified random clustered sample design. This design allowed us more confidence inestimating the prevalence of people with psychosis living in such accommodation. In addition,and unlike in the original reporting of the LPD (Jablensky et al. 1999b), all those who wereinterviewed and living in these marginal settings in Melbourne are included in this chapter,irrespective of whether they were identified in marginal accommodation or via other agenciesduring the census. This allows a comprehensive account of the level of disability, substance useand service needs of this representative group of people with psychosis living in marginalaccommodation in a part of Melbourne.
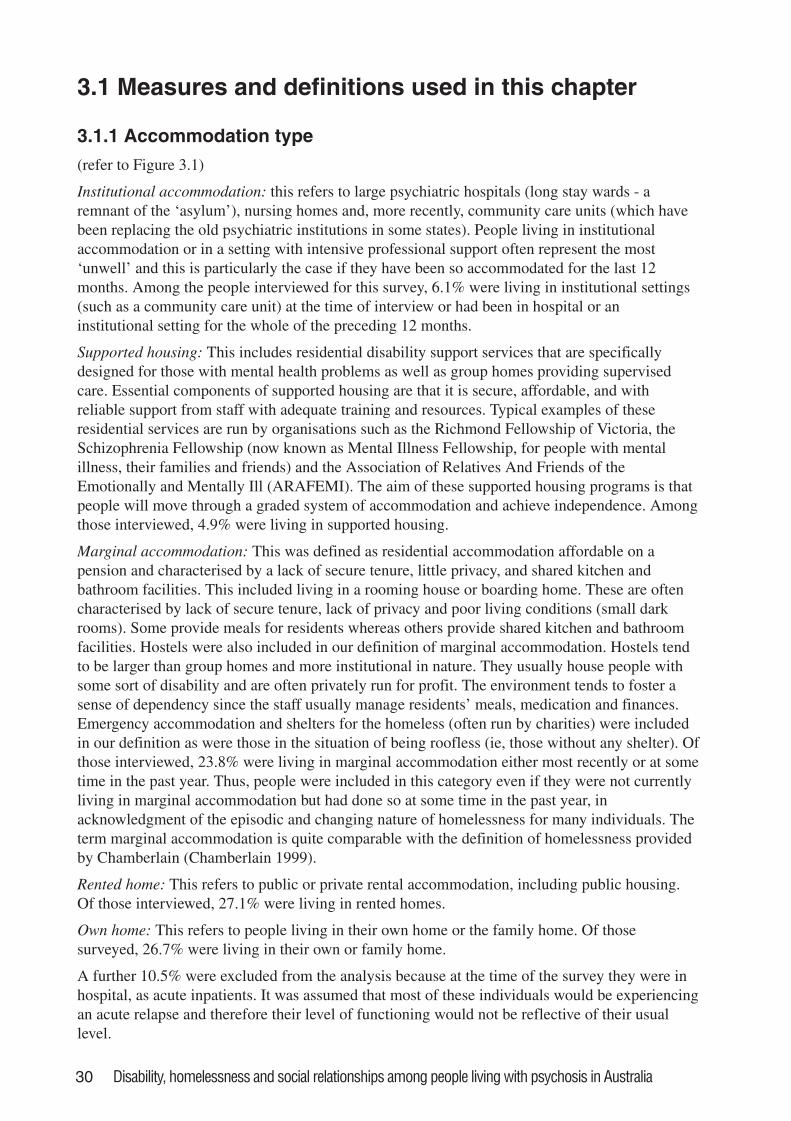
30 Disability, homelessness and social relationships among people living with psychosis in Australia
3.1 Measures and definitions used in this chapter
3.1.1 Accommodation type
(refer to Figure 3.1)
Institutional accommodation: this refers to large psychiatric hospitals (long stay wards - aremnant of the ‘asylum’), nursing homes and, more recently, community care units (which havebeen replacing the old psychiatric institutions in some states). People living in institutionalaccommodation or in a setting with intensive professional support often represent the most‘unwell’ and this is particularly the case if they have been so accommodated for the last 12months. Among the people interviewed for this survey, 6.1% were living in institutional settings(such as a community care unit) at the time of interview or had been in hospital or aninstitutional setting for the whole of the preceding 12 months.
Supported housing: This includes residential disability support services that are specificallydesigned for those with mental health problems as well as group homes providing supervisedcare. Essential components of supported housing are that it is secure, affordable, and withreliable support from staff with adequate training and resources. Typical examples of theseresidential services are run by organisations such as the Richmond Fellowship of Victoria, theSchizophrenia Fellowship (now known as Mental Illness Fellowship, for people with mentalillness, their families and friends) and the Association of Relatives And Friends of theEmotionally and Mentally Ill (ARAFEMI). The aim of these supported housing programs is thatpeople will move through a graded system of accommodation and achieve independence. Amongthose interviewed, 4.9% were living in supported housing.
Marginal accommodation: This was defined as residential accommodation affordable on apension and characterised by a lack of secure tenure, little privacy, and shared kitchen andbathroom facilities. This included living in a rooming house or boarding home. These are oftencharacterised by lack of secure tenure, lack of privacy and poor living conditions (small darkrooms). Some provide meals for residents whereas others provide shared kitchen and bathroomfacilities. Hostels were also included in our definition of marginal accommodation. Hostels tendto be larger than group homes and more institutional in nature. They usually house people withsome sort of disability and are often privately run for profit. The environment tends to foster asense of dependency since the staff usually manage residents’ meals, medication and finances.Emergency accommodation and shelters for the homeless (often run by charities) were includedin our definition as were those in the situation of being roofless (ie, those without any shelter). Ofthose interviewed, 23.8% were living in marginal accommodation either most recently or at sometime in the past year. Thus, people were included in this category even if they were not currentlyliving in marginal accommodation but had done so at some time in the past year, inacknowledgment of the episodic and changing nature of homelessness for many individuals. Theterm marginal accommodation is quite comparable with the definition of homelessness providedby Chamberlain (Chamberlain 1999).
Rented home: This refers to public or private rental accommodation, including public housing.Of those interviewed, 27.1% were living in rented homes.
Own home: This refers to people living in their own home or the family home. Of thosesurveyed, 26.7% were living in their own or family home.
A further 10.5% were excluded from the analysis because at the time of the survey they were inhospital, as acute inpatients. It was assumed that most of these individuals would be experiencingan acute relapse and therefore their level of functioning would not be reflective of their usuallevel.
Disability, homelessness and social relationships among people living with psychosis in Australia 31
Figure 3.1. Categories of accommodation
Categories used in data collection Categories used in data presentation
Own home
Rented
Marginal
Supported
InstitutionalInstitution: hospital
Institution: nursing home, lodge
Supported
Group home
Homeless / no fixed address
Crisis shelter or rooming house
Hostel
Hotel / rented room
Rented home (public)
Rented home (private)
Own home
Family home
32 Disability, homelessness and social relationships among people living with psychosis in Australia
3.1.2 Substance use
Substance use will be described in detail in this chapter. Substance abuse is a common co-morbidproblem among people with psychosis. For people with schizophrenia, cannabis use in particularis recognised as contributing to exacerbation of symptoms and associated poor outcomes. Asimilar pattern of co-morbid substance dependence (especially alcohol) being associated withpoor outcomes has emerged for individuals with mood disorders. A number of studies haveshown that substance use is a risk factor in unstable housing (Lipton et al. 2000; Odell andCommander 2000) and one of the key characteristics that distinguish the homeless mentally illfrom non-homeless mentally ill people (Caton et al. 1994).
All participants were asked about their alcohol consumption during their life-time, how manystandard drinks they had on a typical day when drinking and how often they drank. Intervieweeswere asked how many cigarettes they smoked in the last 12 months. They were also asked aboutillicit drug use. This included substances such as cannabis, amphetamines, tranquillisers, heroin,cocaine, LSD, PCP, and inhalants/solvents. People were asked whether they took these drugs andhow often they took them.
3.1.3 Quality of life
A number of items in the DIP directly or indirectly related to the concept of quality of life. Theseincluded the participant’s own evaluation of their satisfaction with their circumstances as well asindicators of adversity associated with social isolation, marginalisation and socio-economicdeprivation such as victimisation. The following indicators are reported:
• feeling safe in present locality
• being a victim of violence in the last 12 months
• need for police/legal assistance in the last 12 months
• arrested in the last 12 months
• deliberate overdose or self-harm in the last 12 months
• satisfaction with own independence
• satisfaction with life as a whole in the last 12 months.
3.2 Findings
3.2.1 Socio-demographic characteristicsThere was a preponderance of males among residents in supported housing (77%), institutionalsettings (70%), and in marginal accommodation (71%) while the sex distribution was more evenin rented housing (51% males) and among those residing in their own home (54% males). SeeTable 3.1. Institutional accommodation and supported housing shared very high proportions ofpeople who were single and had never married (83% and 88%, respectively). Almost three infour people in marginal accommodation were single, and one in four married or in a defactorelationship. Approximately half of those in their own or rented homes were single and the otherhalf either married, in defacto relationships, divorced, separated or widowed.
Table 3.1 shows that trade or other certificate qualifications were possessed by a lowerproportion of people living in an institutional setting (7%), marginal accommodation (15%) andsupported housing (15%). A similar picture emerged for tertiary qualifications. By comparison,among people who lived in a rented home, 22% had trade qualifications and 14% had tertiaryqualifications. Among people living in their own home, 24% had trade qualifications and 19%had tertiary qualifications.
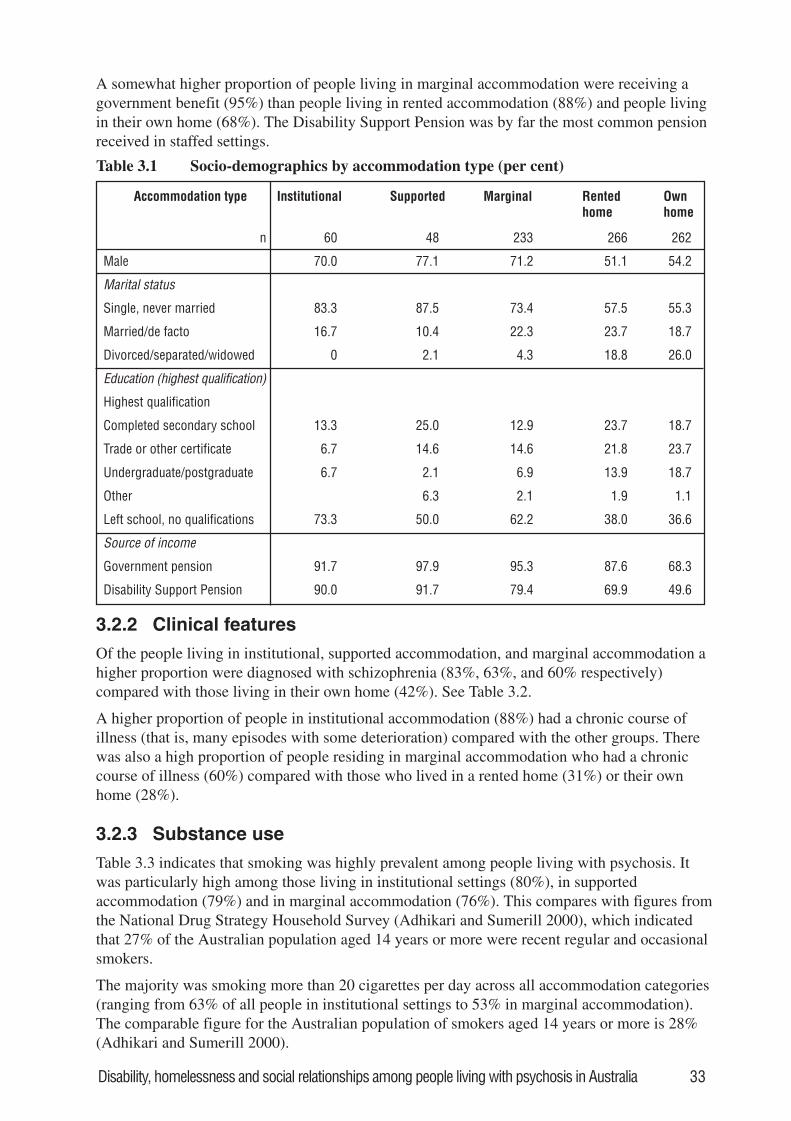
Disability, homelessness and social relationships among people living with psychosis in Australia 33
A somewhat higher proportion of people living in marginal accommodation were receiving agovernment benefit (95%) than people living in rented accommodation (88%) and people livingin their own home (68%). The Disability Support Pension was by far the most common pensionreceived in staffed settings.
Accommodation type Institutional Supported Marginal Rentedhome
Ownhome
n 60 48 233 266 262
Male 70.0 77.1 71.2 51.1 54.2
Marital status
Single, never married 83.3 87.5 73.4 57.5 55.3
Married/de facto 16.7 10.4 22.3 23.7 18.7
Divorced/separated/widowed 0 2.1 4.3 18.8 26.0
Education (highest qualification)
Highest qualification
Completed secondary school 13.3 25.0 12.9 23.7 18.7
Trade or other certificate 6.7 14.6 14.6 21.8 23.7
Undergraduate/postgraduate 6.7 2.1 6.9 13.9 18.7
Other 6.3 2.1 1.9 1.1
Left school, no qualifications 73.3 50.0 62.2 38.0 36.6
Source of income
Government pension 91.7 97.9 95.3 87.6 68.3
Disability Support Pension 90.0 91.7 79.4 69.9 49.6
Table 3.1 Socio-demographics by accommodation type (per cent)
3.2.2 Clinical features
Of the people living in institutional, supported accommodation, and marginal accommodation ahigher proportion were diagnosed with schizophrenia (83%, 63%, and 60% respectively)compared with those living in their own home (42%). See Table 3.2.
A higher proportion of people in institutional accommodation (88%) had a chronic course ofillness (that is, many episodes with some deterioration) compared with the other groups. Therewas also a high proportion of people residing in marginal accommodation who had a chroniccourse of illness (60%) compared with those who lived in a rented home (31%) or their ownhome (28%).
3.2.3 Substance use
Table 3.3 indicates that smoking was highly prevalent among people living with psychosis. Itwas particularly high among those living in institutional settings (80%), in supportedaccommodation (79%) and in marginal accommodation (76%). This compares with figures fromthe National Drug Strategy Household Survey (Adhikari and Sumerill 2000), which indicatedthat 27% of the Australian population aged 14 years or more were recent regular and occasionalsmokers.
The majority was smoking more than 20 cigarettes per day across all accommodation categories(ranging from 63% of all people in institutional settings to 53% in marginal accommodation).The comparable figure for the Australian population of smokers aged 14 years or more is 28%(Adhikari and Sumerill 2000).
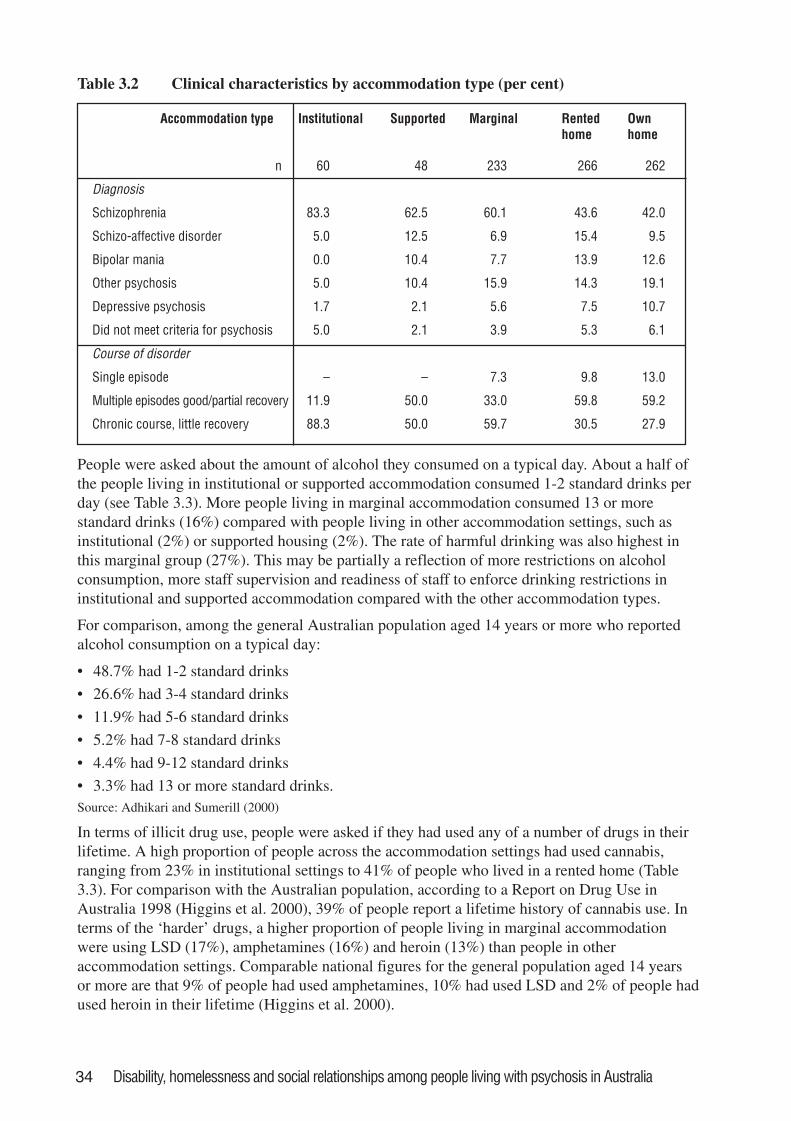
34 Disability, homelessness and social relationships among people living with psychosis in Australia
People were asked about the amount of alcohol they consumed on a typical day. About a half ofthe people living in institutional or supported accommodation consumed 1-2 standard drinks perday (see Table 3.3). More people living in marginal accommodation consumed 13 or morestandard drinks (16%) compared with people living in other accommodation settings, such asinstitutional (2%) or supported housing (2%). The rate of harmful drinking was also highest inthis marginal group (27%). This may be partially a reflection of more restrictions on alcoholconsumption, more staff supervision and readiness of staff to enforce drinking restrictions ininstitutional and supported accommodation compared with the other accommodation types.
For comparison, among the general Australian population aged 14 years or more who reportedalcohol consumption on a typical day:
• 48.7% had 1-2 standard drinks
• 26.6% had 3-4 standard drinks
• 11.9% had 5-6 standard drinks
• 5.2% had 7-8 standard drinks
• 4.4% had 9-12 standard drinks
• 3.3% had 13 or more standard drinks.Source: Adhikari and Sumerill (2000)
In terms of illicit drug use, people were asked if they had used any of a number of drugs in theirlifetime. A high proportion of people across the accommodation settings had used cannabis,ranging from 23% in institutional settings to 41% of people who lived in a rented home (Table3.3). For comparison with the Australian population, according to a Report on Drug Use inAustralia 1998 (Higgins et al. 2000), 39% of people report a lifetime history of cannabis use. Interms of the ‘harder’ drugs, a higher proportion of people living in marginal accommodationwere using LSD (17%), amphetamines (16%) and heroin (13%) than people in otheraccommodation settings. Comparable national figures for the general population aged 14 yearsor more are that 9% of people had used amphetamines, 10% had used LSD and 2% of people hadused heroin in their lifetime (Higgins et al. 2000).
Table 3.2 Clinical characteristics by accommodation type (per cent)
Accommodation type Institutional Supported Marginal Rentedhome
Ownhome
n 60 48 233 266 262
Diagnosis
Schizophrenia 83.3 62.5 60.1 43.6 42.0
Schizo-affective disorder 5.0 12.5 6.9 15.4 9.5
Bipolar mania 0.0 10.4 7.7 13.9 12.6
Other psychosis 5.0 10.4 15.9 14.3 19.1
Depressive psychosis 1.7 2.1 5.6 7.5 10.7
Did not meet criteria for psychosis 5.0 2.1 3.9 5.3 6.1
Course of disorder
Single episode – – 7.3 9.8 13.0
Multiple episodes good/partial recovery 11.9 50.0 33.0 59.8 59.2
Chronic course, little recovery 88.3 50.0 59.7 30.5 27.9
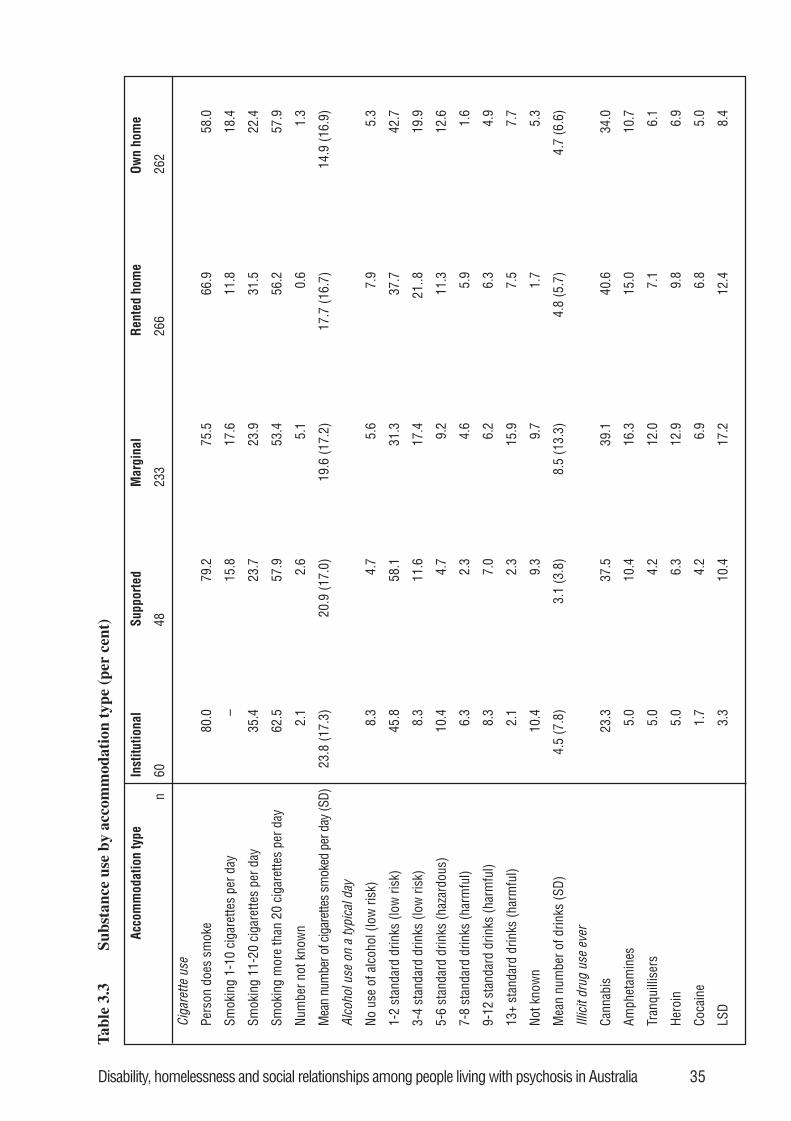
Disability, homelessness and social relationships among people living with psychosis in Australia 35
Acc
omm
odat
ion
type
Inst
itutio
nal
Supp
orte
dM
argi
nal
Rent
ed h
ome
Own
hom
e
n60
4823
326
626
2
Ciga
rette
use
Pers
on d
oes
smok
e80
.079
.275
.566
.958
.0
Smok
ing
1-10
cig
aret
tes
per d
ay–
15.8
17.6
11.8
18.4
Smok
ing
11-2
0 ci
gare
ttes
per d
ay35
.423
.723
.931
.522
.4
Smok
ing
mor
e th
an 2
0 ci
gare
ttes
per d
ay62
.557
.953
.456
.257
.9
Num
ber n
ot k
now
n2.
12.
65.
10.
61.
3
Mea
n nu
mbe
r of c
igar
ette
s sm
oked
per
day
(SD)
23.8
(17.
3)20
.9 (1
7.0)
19.6
(17.
2)17
.7 (1
6.7)
14.9
(16.
9)
Alco
hol u
se o
n a
typi
cal d
ay
No u
se o
f alc
ohol
(low
risk
)8.
34.
75.
67.
95.
3
1-2
stan
dard
drin
ks (l
ow ri
sk)
45.8
58.1
31.3
37.7
42.7
3-4
stan
dard
drin
ks (l
ow ri
sk)
8.3
11.6
17.4
21..8
19.9
5-6
stan
dard
drin
ks (h
azar
dous
)10
.44.
79.
211
.312
.6
7-8
stan
dard
drin
ks (h
arm
ful)
6.3
2.3
4.6
5.9
1.6
9-12
sta
ndar
d dr
inks
(har
mfu
l)8.
37.
06.
26.
34.
9
13+
stan
dard
drin
ks (h
arm
ful)
2.1
2.3
15.9
7.5
7.7
Not k
now
n10
.49.
39.
71.
75.
3
Mea
n nu
mbe
r of d
rinks
(SD)
4.5
(7.8
)3.
1 (3
.8)
8.5
(13.
3)4.
8 (5
.7)
4.7
(6.6
)
Illic
it dr
ug u
se e
ver
Cann
abis
23.3
37.5
39.1
40.6
34.0
Amph
etam
ines
5.0
10.4
16.3
15.0
10.7
Tran
quill
iser
s5.
04.
212
.07.
16.
1
Hero
in5.
06.
312
.99.
86.
9
Coca
ine
1.7
4.2
6.9
6.8
5.0
LSD
3.3
10.4
17.2
12.4
8.4
Tab
le 3
.3Su
bsta
nce
use
by a
ccom
mod
atio
n ty
pe (
per
cent
)
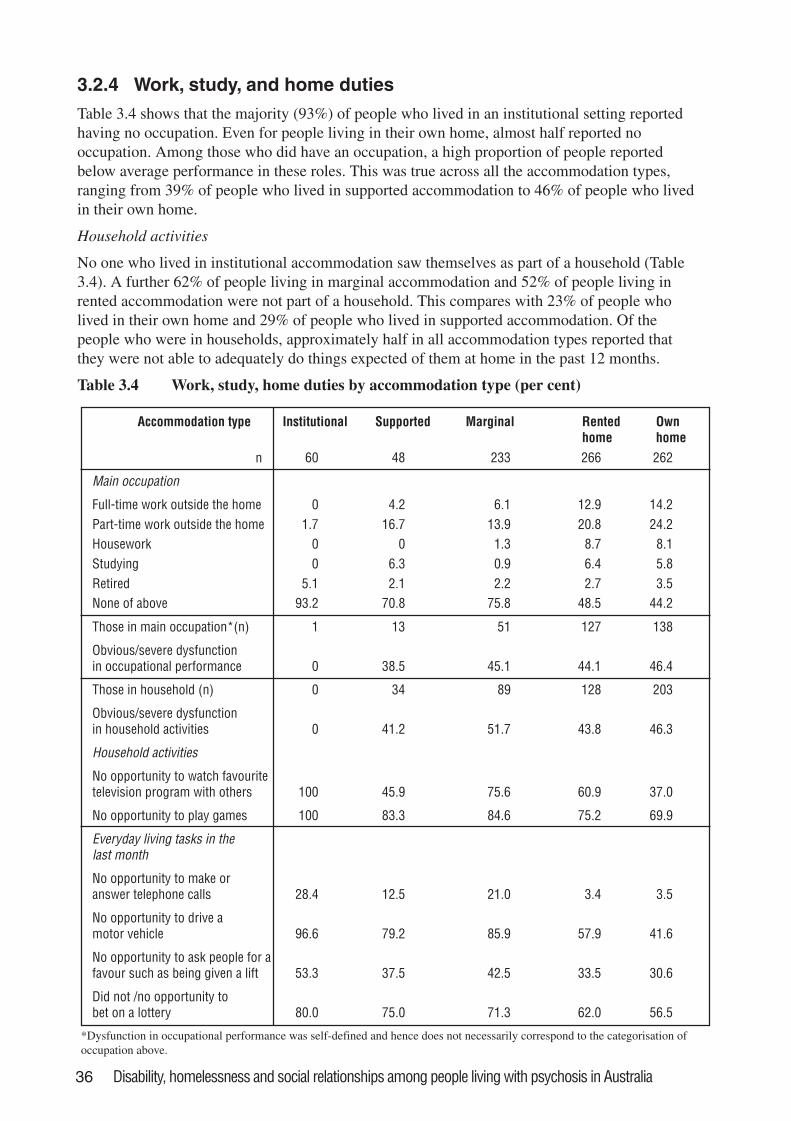
36 Disability, homelessness and social relationships among people living with psychosis in Australia
3.2.4 Work, study, and home duties
Table 3.4 shows that the majority (93%) of people who lived in an institutional setting reportedhaving no occupation. Even for people living in their own home, almost half reported nooccupation. Among those who did have an occupation, a high proportion of people reportedbelow average performance in these roles. This was true across all the accommodation types,ranging from 39% of people who lived in supported accommodation to 46% of people who livedin their own home.
Household activities
No one who lived in institutional accommodation saw themselves as part of a household (Table3.4). A further 62% of people living in marginal accommodation and 52% of people living inrented accommodation were not part of a household. This compares with 23% of people wholived in their own home and 29% of people who lived in supported accommodation. Of thepeople who were in households, approximately half in all accommodation types reported thatthey were not able to adequately do things expected of them at home in the past 12 months.
Table 3.4 Work, study, home duties by accommodation type (per cent)
Accommodation type Institutional Supported Marginal Rentedhome
Ownhome
60 48 233 266 262
Main occupation
Full-time work outside the home 0 4.2 6.1 12.9 14.2Part-time work outside the home 1.7 16.7 13.9 20.8 24.2Housework 0 0 1.3 8.7 8.1Studying 0 6.3 0.9 6.4 5.8Retired 5.1 2.1 2.2 2.7 3.5None of above 93.2 70.8 75.8 48.5 44.2
Those in main occupation*(n) 1 13 51 127 138
Obvious/severe dysfunctionin occupational performance 0 38.5 45.1 44.1 46.4
Those in household (n) 0 34 89 128 203
Obvious/severe dysfunctionin household activities 0 41.2 51.7 43.8 46.3
Household activities
No opportunity to watch favouritetelevision program with others 100 45.9 75.6 60.9 37.0
No opportunity to play games 100 83.3 84.6 75.2 69.9
Everyday living tasks in thelast month
No opportunity to make oranswer telephone calls 28.4 12.5 21.0 3.4 3.5
No opportunity to drive amotor vehicle 96.6 79.2 85.9 57.9 41.6
No opportunity to ask people for afavour such as being given a lift 53.3 37.5 42.5 33.5 30.6
Did not /no opportunity tobet on a lottery 80.0 75.0 71.3 62.0 56.5
n
*Dysfunction in occupational performance was self-defined and hence does not necessarily correspond to the categorisation ofoccupation above.
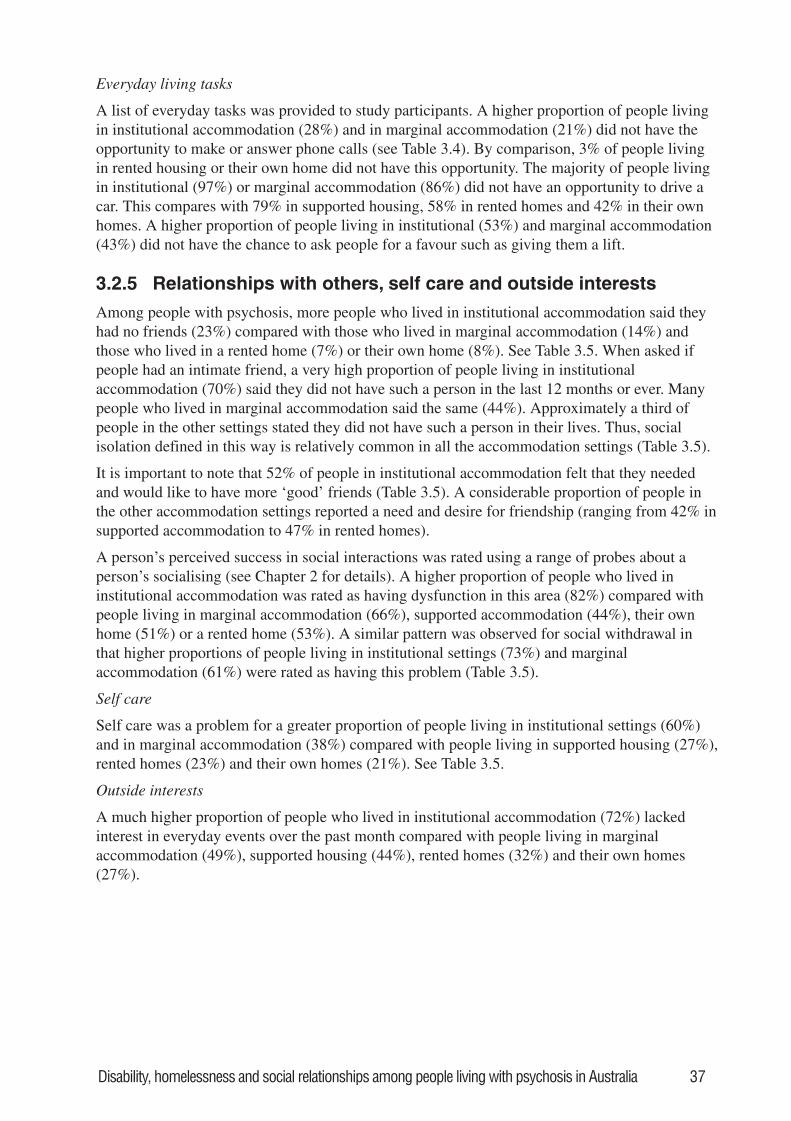
Disability, homelessness and social relationships among people living with psychosis in Australia 37
Everyday living tasks
A list of everyday tasks was provided to study participants. A higher proportion of people livingin institutional accommodation (28%) and in marginal accommodation (21%) did not have theopportunity to make or answer phone calls (see Table 3.4). By comparison, 3% of people livingin rented housing or their own home did not have this opportunity. The majority of people livingin institutional (97%) or marginal accommodation (86%) did not have an opportunity to drive acar. This compares with 79% in supported housing, 58% in rented homes and 42% in their ownhomes. A higher proportion of people living in institutional (53%) and marginal accommodation(43%) did not have the chance to ask people for a favour such as giving them a lift.
3.2.5 Relationships with others, self care and outside interests
Among people with psychosis, more people who lived in institutional accommodation said theyhad no friends (23%) compared with those who lived in marginal accommodation (14%) andthose who lived in a rented home (7%) or their own home (8%). See Table 3.5. When asked ifpeople had an intimate friend, a very high proportion of people living in institutionalaccommodation (70%) said they did not have such a person in the last 12 months or ever. Manypeople who lived in marginal accommodation said the same (44%). Approximately a third ofpeople in the other settings stated they did not have such a person in their lives. Thus, socialisolation defined in this way is relatively common in all the accommodation settings (Table 3.5).
It is important to note that 52% of people in institutional accommodation felt that they neededand would like to have more ‘good’ friends (Table 3.5). A considerable proportion of people inthe other accommodation settings reported a need and desire for friendship (ranging from 42% insupported accommodation to 47% in rented homes).
A person’s perceived success in social interactions was rated using a range of probes about aperson’s socialising (see Chapter 2 for details). A higher proportion of people who lived ininstitutional accommodation was rated as having dysfunction in this area (82%) compared withpeople living in marginal accommodation (66%), supported accommodation (44%), their ownhome (51%) or a rented home (53%). A similar pattern was observed for social withdrawal inthat higher proportions of people living in institutional settings (73%) and marginalaccommodation (61%) were rated as having this problem (Table 3.5).
Self care
Self care was a problem for a greater proportion of people living in institutional settings (60%)and in marginal accommodation (38%) compared with people living in supported housing (27%),rented homes (23%) and their own homes (21%). See Table 3.5.
Outside interests
A much higher proportion of people who lived in institutional accommodation (72%) lackedinterest in everyday events over the past month compared with people living in marginalaccommodation (49%), supported housing (44%), rented homes (32%) and their own homes(27%).
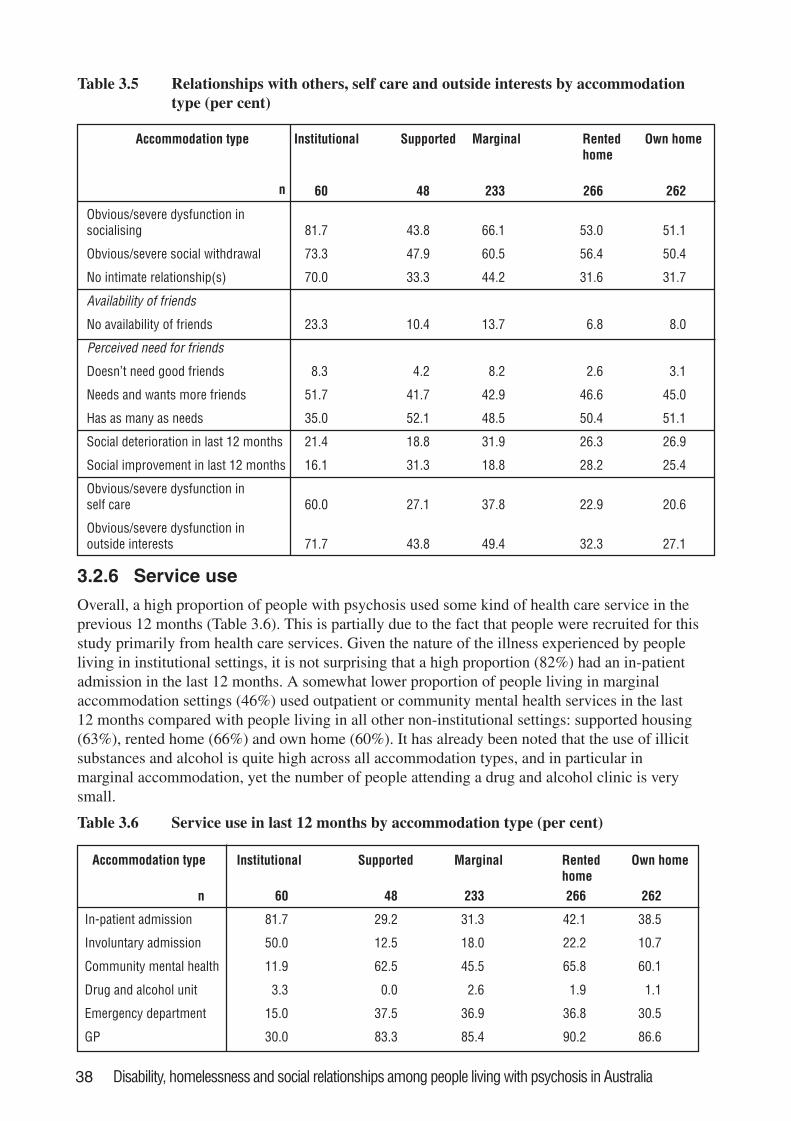
38 Disability, homelessness and social relationships among people living with psychosis in Australia
Table 3.5 Relationships with others, self care and outside interests by accommodationtype (per cent)
Accommodation type Institutional Supported Marginal Rentedhome
Own home
60 48 233 266 262
Obvious/severe dysfunction insocialising 81.7 43.8 66.1 53.0 51.1
Obvious/severe social withdrawal 73.3 47.9 60.5 56.4 50.4
No intimate relationship(s) 70.0 33.3 44.2 31.6 31.7
Availability of friends
No availability of friends 23.3 10.4 13.7 6.8 8.0
Perceived need for friends
Doesn’t need good friends 8.3 4.2 8.2 2.6 3.1
Needs and wants more friends 51.7 41.7 42.9 46.6 45.0
Has as many as needs 35.0 52.1 48.5 50.4 51.1
Social deterioration in last 12 months 21.4 18.8 31.9 26.3 26.9
Social improvement in last 12 months 16.1 31.3 18.8 28.2 25.4
Obvious/severe dysfunction inself care 60.0 27.1 37.8 22.9 20.6
Obvious/severe dysfunction inoutside interests 71.7 43.8 49.4 32.3 27.1
n
3.2.6 Service use
Overall, a high proportion of people with psychosis used some kind of health care service in theprevious 12 months (Table 3.6). This is partially due to the fact that people were recruited for thisstudy primarily from health care services. Given the nature of the illness experienced by peopleliving in institutional settings, it is not surprising that a high proportion (82%) had an in-patientadmission in the last 12 months. A somewhat lower proportion of people living in marginalaccommodation settings (46%) used outpatient or community mental health services in the last12 months compared with people living in all other non-institutional settings: supported housing(63%), rented home (66%) and own home (60%). It has already been noted that the use of illicitsubstances and alcohol is quite high across all accommodation types, and in particular inmarginal accommodation, yet the number of people attending a drug and alcohol clinic is verysmall.
Accommodation type Institutional Supported Marginal Rentedhome
Own home
n 60 48 233 266 262
In-patient admission 81.7 29.2 31.3 42.1 38.5
Involuntary admission 50.0 12.5 18.0 22.2 10.7
Community mental health 11.9 62.5 45.5 65.8 60.1
Drug and alcohol unit 3.3 0.0 2.6 1.9 1.1
Emergency department 15.0 37.5 36.9 36.8 30.5
GP 30.0 83.3 85.4 90.2 86.6
Table 3.6 Service use in last 12 months by accommodation type (per cent)

Disability, homelessness and social relationships among people living with psychosis in Australia 39
People were asked about other services received in the last twelve months and whether they weresatisfied with the service they received. Most people with psychosis received prescribedmedication across all accommodation types and most stated that they were satisfied with thisservice. With respect to receiving mental health information, the proportions varied acrossaccommodation types, the lowest (surprisingly) being for people living in institutional settingsand (not surprisingly) for those in marginal accommodation (38% in each case). Less than half ofpeople living in any setting received therapy or counselling. The figures were especially low forthose in institutional (28%) and marginal accommodation (32%).
Across all accommodation types, the proportions of those receiving a service designed toimprove work skills or use of time differ – usually markedly – from the proportions that areunoccupied. For instance, of people living in:
• institutional accommodation, 93% were unoccupied and only 42% were receiving a service toimprove work or time use
• supported accommodation, 71% were unoccupied and only 35% were using such a service
• marginal accommodation, 76% were unoccupied and only 36% were using such a service
• rented home, 49% were unoccupied and 32% were using such a service
• their own home, 44% were unoccupied and 38% were using such a service.
It is not surprising that people living in stable housing received fewer services to help themmanage their housing or financial matters. Nevertheless, the proportion of people in less stableaccommodation using such a service is not as high as one might expect: for example, only 46%of people in marginal accommodation. While it is unclear what proportion of this represents anunmet need or an absence of need, that many people living in inadequate accommodation arenevertheless not in receipt of help relating to housing is a striking observation.
People were asked if they received a service directed at social support in the last 12 months, andtheir answers contrast with the level of dysfunction in their socialising.
Of people living in:
• institutional accommodation, 82% had dysfunction in socialising and only 40% were receivinga service to improve their social support
• supported accommodation, 44% had dysfunction in socialising and 33% were using such aservice
• marginal accommodation, 66% had dysfunction in socialising and only 34% were using such aservice
• rented home, 53% had dysfunction in socialising and only 29% were using such a service
• their own home, 51% had dysfunction in socialising and 27% were using such a service.
In general, fewer people in marginal accommodation were satisfied with services received.
The level of use of services provided by government and non-government agencies varied amongthe different accommodation types. Perhaps the most striking difference is found among peoplewho used the government department for housing. Given that marginal accommodation may beregarded as the least stable accommodation type, only 18% of people in this setting had accessedthis service. This contrasts with 47% of people who lived in a rented home.
3.2.7 Quality of life
Among people living in different accommodation types, a higher proportion of people inmarginal accommodation reported being a victim of violence (26%) compared with people livingin their own home (8%) or in supported accommodation (10%). See Table 3.7. It is also
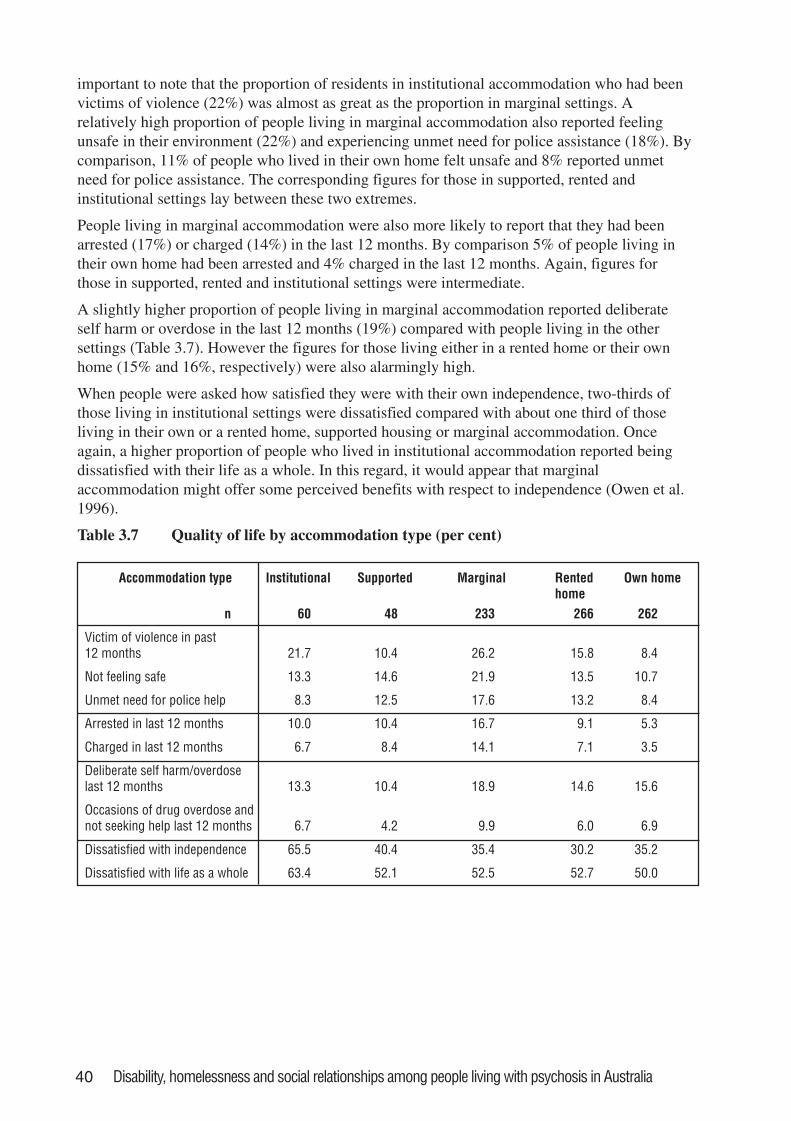
40 Disability, homelessness and social relationships among people living with psychosis in Australia
important to note that the proportion of residents in institutional accommodation who had beenvictims of violence (22%) was almost as great as the proportion in marginal settings. Arelatively high proportion of people living in marginal accommodation also reported feelingunsafe in their environment (22%) and experiencing unmet need for police assistance (18%). Bycomparison, 11% of people who lived in their own home felt unsafe and 8% reported unmetneed for police assistance. The corresponding figures for those in supported, rented andinstitutional settings lay between these two extremes.
People living in marginal accommodation were also more likely to report that they had beenarrested (17%) or charged (14%) in the last 12 months. By comparison 5% of people living intheir own home had been arrested and 4% charged in the last 12 months. Again, figures forthose in supported, rented and institutional settings were intermediate.
A slightly higher proportion of people living in marginal accommodation reported deliberateself harm or overdose in the last 12 months (19%) compared with people living in the othersettings (Table 3.7). However the figures for those living either in a rented home or their ownhome (15% and 16%, respectively) were also alarmingly high.
When people were asked how satisfied they were with their own independence, two-thirds ofthose living in institutional settings were dissatisfied compared with about one third of thoseliving in their own or a rented home, supported housing or marginal accommodation. Onceagain, a higher proportion of people who lived in institutional accommodation reported beingdissatisfied with their life as a whole. In this regard, it would appear that marginalaccommodation might offer some perceived benefits with respect to independence (Owen et al.1996).
Table 3.7 Quality of life by accommodation type (per cent)
Accommodation type Institutional Supported Marginal Rentedhome
Own home
n 60 48 233 266 262
Victim of violence in past12 months 21.7 10.4 26.2 15.8 8.4
Not feeling safe 13.3 14.6 21.9 13.5 10.7
Unmet need for police help 8.3 12.5 17.6 13.2 8.4
Arrested in last 12 months 10.0 10.4 16.7 9.1 5.3
Charged in last 12 months 6.7 8.4 14.1 7.1 3.5
Deliberate self harm/overdoselast 12 months 13.3 10.4 18.9 14.6 15.6
Occasions of drug overdose andnot seeking help last 12 months 6.7 4.2 9.9 6.0 6.9
Dissatisfied with independence 65.5 40.4 35.4 30.2 35.2
Dissatisfied with life as a whole 63.4 52.1 52.5 52.7 50.0
Disability, homelessness and social relationships among people living with psychosis in Australia 41
3.3 ConclusionsThere is an emerging picture of a typical resident among those studied in supported, marginal orinstitutional accommodation being single, male and often diagnosed with schizophrenia. In thecase of the marginal and institutional settings, the resident often has less education than otherswho are living with psychosis, and has a smaller chance of being employed. With respect toemployment prospects, the situation for residents of supported housing is slightly better.
The extent of smoking among people living with psychosis is a major public health issue. It haslong been known that the physical health of those with psychosis is worse than for comparablegroups in the general population (Brugha et al. 1989). Further, among people with schizophrenia,life expectancy is reduced compared with the general population, even after accounting for theirhigher suicide rate (Newman and Bland 1991; Mortensen and Juel 1993). These observations arevery likely to be linked.
In comparison to the Australian population, harmful alcohol consumption is more prevalentamong people with psychosis living in all accommodation settings except for those in supportedhousing. This rate is of particular concern among those living in marginal accommodation asalcohol and drug use are known risk factors for housing instability (Rickards et al. 1999; Odelland Commander 2000; Sullivan et al. 2000). In contrast, access to drug and alcohol servicesamong people with psychosis is extremely low.
Heroin use among people living with psychosis is alarmingly high across all accommodationsettings, but especially in marginal accommodation.
Under-activity is more common in staffed settings such as institutions, supported housing andhostels. It seems clear that the presence of staff does not of itself address people’s under-occupation, for reasons that are likely to be complex. Greater attention to facilitating meaningfulactivity within and outside of these settings would be likely to enhance residents’ well-being andquality of life.
Data on everyday living tasks suggest that opportunities are especially limited for people inmarginal and institutional settings. This suggests people’s functioning may be limited throughenvironmental barriers to activity and participation, as well as the effects of the psychosis itselfand associated impairments.
In general, the greatest disability exists among people with psychosis living in settings wheresome staff input is available. Whilst this is reassuring in the sense that such disability providesone of the rationales for placement of people in institutional and supported settings, it isworrying that disability and other problems such as substance misuse are so prevalent amongresidents in marginal accommodation. This is because marginal settings are not specificallydesigned to cater for people with mental-health related needs. In the case of residents ofsupported accommodation, there are some ways in which they seem to be doing better than theother two aforementioned groups. For example, there is a greater chance that they will beoccupied (including in paid work), they have fewer difficulties with caring for themselves andthey experience a lower level of social dysfunction. Indeed, with regard to social dysfunction,people living in ‘independent accommodation’ (rented or own home) may be more incapacitatedthan people living in supported accommodation.
People in institutional settings, and to a lesser degree those in marginal accommodation, lackintimate friendships. So, whilst there are people nearby, there is a lack of intimacy in socialinteractions. Yet there is an expressed desire amongst many residents in these settings for suchintimacy.
42 Disability, homelessness and social relationships among people living with psychosis in Australia
The degree of mismatch between people’s needs (as inferred from the findings with regard tofunctioning) and service use appears to depend on the setting. For instance, more people living inindependent accommodation and in need of occupational assistance receive help in this area.Although this may be due to the perception that people in other settings are too ill or unmotivatedto benefit from such input, the success of programs overseas cautions us to avoid thisassumption. Most people living in staffed settings get little support in managing housing orfinancial matters even though it could be anticipated that many have needs in this area.Particularly striking is the low use of the housing department by people in marginal settings.More encouraging is that there is a closer fit between level of social difficulties and assistanceoffered with social support for those in supported accommodation. This may be one of thestrengths of this type of service.
3.4 Recommendations3.4.1 Specially designed programs to help people with psychosis reduce or quit smoking, such
as the recently established SANE Australia Smoke Free Kit, need to be developed andmade widely available through agencies such as community health, primary care and non-government organisations.
3.4.2 People with psychosis urgently require improved access to drug and alcohol services.There should be greater availability of specially targeted drug and alcohol programs (suchas the SUMITT program in North Western Melbourne) for this subgroup, sincespecialised input is required to deal with the co-morbidity of mental illness and substancemisuse.
3.4.3 Institutional settings such as long-stay wards, community care units and nursing homescare for those with the greatest disability. While acknowledging this, it is crucial that thewidespread under-activity and social isolation in these settings are addressed. To improveindividuals’ participation in meaningful activities and intimate relationships requires bothmaximising the use of environmental supports to accommodate individuals’ functionaldifficulties, and minimising environmental barriers that constrain their opportunities foroccupations and relationships. Provision of improved access to rehabilitation anddisability support could help to address these issues.
3.4.4 It is clear that there are differences between the level and types of disability experiencedby people with psychosis living in different settings. Greater attention should be given tothe interaction between personal and environmental factors in recovery from psychosis. Itis important to assess the individual’s needs rather than make assumptions based on his/her current environmental circumstances, and to facilitate their recovery by matching theirneeds with the most appropriate environment.
3.4.5 Clinical services, housing services and disability support services, including thoseprovided by non-government organisations, should be better coordinated in order to moresuccessfully meet the needs of people with regard to both their mental illness and theirliving circumstances (Victorian Homelessness Strategy Ministerial Advisory Committee2001). Implementing the co-ordination of housing supply and community support hasproved to be very difficult and it has been proposed that a co-ordinating body is required(Thomas and McCormack 1999).
3.4.6 At a government level, the Departments of Housing and Health should work together todevelop a range of secure and stable accommodation options, with flexible support tomeet the range and changing needs of people with psychosis. Support options shouldinclude assertive outreach responses, since these are recognised as effective in reducinghomelessness (Mueser et al. 1998).
Disability, homelessness and social relationships among people living with psychosis in Australia 43
4. Disability and service use amonghomeless people living withpsychotic disorders in Melbourne
P is a 45 year old male who lives in a rooming house in inner Melbourne. He feelsunsafe in his neighbourhood and was beaten up recently. The police came but saidhe was drunk and took him down to the station. He saw his brother five years agoand basically lives alone with little or no contact with friends or family. He firstbecame unwell after the death of his wife. This was 10 years ago. He hears voicesthat continually tell him that he is no good and that people are out to get him. Hebelieves he is the prince of darkness. He drinks everyday, usually two litres of wine.This stops him hearing the voices. He doesn’t attend any mental health services.He might visit the local doctor and front up to the hospital emergency departmentif he has injured himself while drunk. He says he is mostly satisfied with his lifeand would like to stop drinking but it is very hard.
This chapter provides a detailed description of people with psychosis who are homeless. Thisgroup is doubly disadvantaged and therefore particularly vulnerable. A number of reports havedocumented that their needs are not fully understood or met by either the mental health system orthe housing sector (Victorian Homelessness Strategy Ministerial Advisory Committee 2001).
As has already been mentioned (Chapter 1), public concern about homeless mentally ill people,and reports of the growing number of this subgroup in various countries, have sometimes beenlinked with the process of de-institutionalisation. Indeed, an apparent dilemma arises whenhomelessness and psychiatric disability are found among people even where relatively goodcommunity psychiatric and health services exist. The popular response to this recognition is acall to slow down the process of dismantling the institutions, or even to bring back the asylums.Yet large-scale institutional care has mostly failed and is no longer acceptable (Singh 1992).
The growing number of mentally ill homeless people is not a uniform finding. Contradictoryfindings may be partially explained by the use of different methods for defining and identifyingthis group of people (see below), and are not necessarily linked to de-institutionalisation. Forexample, the prevalence of schizophrenia among hostel residents in Edinburgh was lower in 1992than in 1966 even after taking into account potential confounding factors, and despite a largereduction in the number of occupied psychiatric beds (Geddes et al. 1994). The relatively lowprevalence of schizophrenia among homeless people in Edinburgh could be explained bydevelopments in the provision of health, housing and welfare services. Even so, as the authorsemphasise, the prevalence of 9% is several times higher than in the general population.
Within the Australian context, the prevalence of psychosis in general, and schizophrenia inparticular, among the homeless population has increased over time. In 1985, Doutney et al.(1985) reported the prevalence of schizophrenia among men living in a homeless refugee inSydney as 15%. In 1987, a Melbourne study found a life-time prevalence of 21% for psychoticdisorders among people living in marginal accommodation (Herrman et al. 1989). More recently,in Sydney, the prevalence of schizophrenia found in hostel users was 29% (Hodder et al. 1998).
It is important to define and delimit the scope of the mentally ill homeless population especiallywhen studies in different settings report different rates of mental illness among the homeless
44 Disability, homelessness and social relationships among people living with psychosis in Australia
(Bachrach 1995). Homeless mentally ill people differ widely in their diagnosis, treatmenthistories, disabilities and service needs. Even though mentally ill homeless people are diverse inso many ways, and share many characteristics with the majority of homeless people (who are notmentally ill), they possess unique service requirements that may be overlooked. By and large,they require mental health services in addition to social support, housing, and economic securityto alter their life circumstances (Bachrach 1995). Homeless mentally ill people with psychoticdisorders tend to have high rates of previous contact with traditional psychiatric services, buttypically have limited current contact and low rates of psychotropic medication use (Herrman etal. 1992; Hamid et al. 1995a; Hamid et al. 1995b; Marshall 1996). On the other hand, accessibleand relevant specialist services for homeless people, including outreach services, can encouragehelpful service contact (Geddes et al. 1994; Buhrich and Teesson 1996), and homeless mentallyill people will use accessible primary health care (Herrman et al. 1992). There is a need forfurther studies to assess the needs of homeless people and help direct the policy and resources tomeet their needs.
The different rates of psychosis among homeless populations in various countries have alreadybeen highlighted. In this respect, it is crucial to estimate the extent of the problem in Australia.However, an understanding of the rate of disorder does not in itself give a good indication of theneed for services. Few of the hostel workers in Edinburgh had formal training in caring forpeople with such disorders, and contact with psychiatric services does not necessarily imply thathealth needs are being met. To illustrate, there was still considerable unmet need among mentallyill hostel residents in Oxford, as measured by the MRC Needs for Care Schedule, despite aspecialised GP service and weekly visits from a psychiatric registrar (Hogg and Marshall 1992).A sub-group of hostel residents in any city will have significant mental disorder and relateddisability (Hamid et al. 1995a; Hamid et al. 1995b). The social disability of these residents canbe reduced with adequate psychiatric treatment (Marshall 1996), but without an in-depthassessment of their disabilities and needs, including the views of residents and staff (Hogg andMarshall 1992), it is not possible to plan accurately for community based services.
4.1 Definition of homelessnessOverseas, the definition of homelessness has narrowed over time. For example, several decadesago in the United States, homelessness encompassed people living in substandard housing,whereas today the term refers to people who are roofless or living in public and private sheltersand institutions providing temporary accommodation (Daly 1996).
The general consensus among researchers is that the term homeless refers to something morethan just ‘house-less-ness’ (Baum and Burnes 1993; Daly 1996). This is reflected in thefollowing excerpt:
The term ‘homeless’ is actually a catch word, a misnomer that focuses our attention on only oneaspect of the individual’s plight: his lack of residence or housing. In reality, the homeless often haveno job, no function, no role within the community; they generally have few social supports. They arejobless, penniless, functionless, and supportless as well as homeless. (Lipton and Sabatini 1984,p.156)
An important aspect of ‘homelessness’ is the person’s alienation from society. This is reflected inthe definition provided by the Council of Homeless Persons, Victoria.
A homeless person is without a conventional home. She/he is often cut off from support of relatives andfriends, she/he has few independent resources and often has no immediate means and in some cases,little future prospects of self-support.
People may be transiently, episodically or chronically homeless and homeless people may,according to this definition, be roofless, or moving about between refuges, shelters, hostels or
Disability, homelessness and social relationships among people living with psychosis in Australia 45
relatives and friends, or living in rooming houses or cheap hotels (Arce and Vergare 1984). Inother words, homelessness is a series of states that exist along the continuum of time and thecontinuum of place, and entry to, or exit from, the homeless state is usually part of a processrather than a single jump.
Within the Australian context the definition of homelessness has remained broad, taking intoaccount various states of homelessness as described in the definition below:
Primary homelessness: people without conventional accommodation such as those who ‘sleep out’, oruse derelict buildings, cars, railway stations, for shelter.
Secondary homelessness: people who frequently move from temporary accommodation such asemergency accommodation, refuges, temporary shelters. People may use boarding houses or familyaccommodation but on a temporary basis.
Tertiary homelessness: people who live in rooming houses or boarding houses on a medium or long-term basis, where they do not have their own bathroom and kitchen facilities and tenure is not securedby a lease.
(Chamberlain 1999)
This chapter reports on a nested study within the Melbourne catchment area (an inner-city andsuburban site) of the main LPD survey. The Melbourne site added to the core a systematic surveyof an at-risk population group: residents of marginal accommodation and users of ‘drop-in’disability support services in the catchment area. This allowed the estimation of the prevalence ofpsychotic illness among homeless people in inner Melbourne, a decade after a previous study(Herrman et al. 1989). A broad definition of homelessness was used, including a definition ofmarginal accommodation as residential accommodation affordable on a pension characterised bya lack of secure tenure, little privacy, and shared kitchen and bathroom facilities (see Chapter 3).This nested study also extended the identification of the homeless by including drop-in centresand other non-residential disability support agencies in the scope of the systematic survey. Theseagencies included charitable organisations that provide emergency relief, food parcels or mealsfor people who are homeless or economically and socially disadvantaged, as well as that givepeer support to people living with mental illness. Some of the agencies offer independent livingskills training, using both centre-based and outreach approaches. The disability and service useare described in this group of homeless people in order to define their needs for care.
4.2 Methodology of the nested study of the homelesspopulation with psychosis in Melbourne
The nested study was designed to screen a representative sample of ‘at risk people’ who wereusing marginal accommodation places and day facilities in the Melbourne catchment area. Weused the same age and diagnostic criteria for inclusion of participants, as well as instruments forscreening and interviews, as in the main LPD survey (Jablensky et al. 1999b; Jablensky 2000).However, the methodology of this nested study has not been previously described, so a briefdescription will be provided here, with further details available in Appendix 2.
4.2.1 The catchment area for the Melbourne study
The area comprises two local government areas in Melbourne, the inner city of Yarra(incorporating the former cities of Fitzroy, Collingwood and Richmond), and the contiguousmore affluent suburban city of Boroondara (former cities of Kew, Hawthorn and Camberwell).The total adult population of Yarra in the 1996 mid-term Census estimates was 65,000, and ofBoroondara 145,000. The City of Yarra has traditionally been a working class area with asignificant proportion of people who are economically disadvantaged and socially isolated, and it
46 Disability, homelessness and social relationships among people living with psychosis in Australia
is an area settled by people arriving from many non-English speaking backgrounds over severaldecades. There is a high rate of illicit drug use and alcohol abuse. The area has large publichousing estates and a number of rooming and boarding houses. In recent times, artists andprofessionals wishing to live close to the city have settled this area. In contrast, the City ofBoroondara is predominantly a middle-class area without any large-scale public housing,although still containing a number of large properties functioning as rooming and boardinghouses.
4.2.2 Study design
The study design had three components. Firstly, the sampling frame of accommodation and dayfacilities in the catchment area was established. This required compiling a list of allaccommodation facilities, drop-in centres, soup kitchens and specialised disability supportprograms in the designated catchment areas. In the course of this exercise it became evident thata number of houses previously in use as marginal accommodation were no longer in existence, orhad been converted into apartments (see Appendix 2).
Secondly, a stratified sampling frame was constructed for accommodation places. Housesmeeting the criterion definition of marginal accommodation were stratified by local governmentarea (City of Yarra, and Boroondara) and number of beds (fewer than 20; 20 to 49; 50 andabove). From this sampling frame a random list of houses was produced for each of the six strata.
Using a stratified random cluster sample design gave an equal chance of inclusion to each personliving in a particular stratum (defined by city and size of house), while giving different weights toeach stratum to allow inclusion of a minimum number of people from a variety of differentsettings. Women were over-sampled because they were a small minority in the population. Inother words, all women from the few women-only dwellings were included (there were 4 housesfor women who agreed to take part, all in the fewer than 20 bed range in the City of Yarra with atotal of 61 beds; an additional house of 12 beds in the same bed range in Yarra declined).
A target of 500 residents was used as a basis for obtaining 360 screens and in-depth interviewswith up to 90 residents who were screened as positive (see Appendix 2 for more detailedrationale for these numbers). This target of 500 was divided between the strata as describedabove; the number of houses required to provide the estimated number of respondents weredrawn from the randomly ordered list of all houses in that cluster. If the proprietor of a selectedhouse did not agree to the study proceeding, the next rooming house on the list was contacted. Ofthe 80 houses in the final list, a total of 13 did not respond to inquiries about taking part in thesurvey, 17 refused, and 13 were agreeable to taking part but ultimately were not required assufficient numbers were obtained from the final sample of 37 houses.
Thirdly, conducting the census and interviewing participants took place over a six-week period,including the study census, in winter 1997. Interviewers had backgrounds in clinical psychology,social work, and psychiatric nursing, and were trained according to procedures established forthe national study and supervised by Oye Gureje locally. Various homeless outreach workers,including staff from the local mental health service and the Royal District Nursing Service, gavethem advice.
4.2.3 Interviewing and sampling results in marginal accommodation
In a number of the houses, the management informed the residents of the intent to conduct thesurvey. Trained interviewers went in pairs to the randomly selected houses and knocked on alldoors in each house. Three separate attempts were made to contact a person in each room withthe interviewers visiting on different and pre-determined days and times. When a resident
Disability, homelessness and social relationships among people living with psychosis in Australia 47
answered the door, the interviewer introduced her/himself, explained the purpose of the visit,described the study, and administered the screening questionnaire to those who gave verbalconsent.
Apart from a number of people who did not meet the study criteria because they were over theage limit, had insufficient English language skills to answer the questions or had an intellectualdisability, all those who screened positive were invited by the interviewer to take part in the in-depth interview. As some people living in these places move in and out of accommodationfrequently, the interview was booked with as little time lag between screening and interview aspossible. As many interviews as possible were done concurrently with the screening. Of the 597beds that met study criteria, 348 people (58.3%) residing there were screened and 164 people(47.1%) had a positive screen. Details of the houses and facilities together with other samplingresults appear in Appendix 2, including Table B1.1.
4.2.4 Interviewing and sampling results in drop-in centres
People were sampled from drop-in centres to supplement the sampling frame of accommodationhouses for the following reasons:
1. People who lived in the sampled rooming house could be attending a local drop-in centreduring the day. Sampling in drop-in centres was therefore used as an additional strategy inlocating people who were not home when interviewers called on the selected rooming house.
2. People who are sleeping rough or are shelterless often attend drop-in centres to receive meals,clothing or participate in social activities. Sampling in drop-in centres was a way of accessingthese roofless individuals.
3. People living in other types of accommodation who attend drop-in centres for emergencyrelief, food, or clothing were deemed eligible for inclusion in a study of marginal populationssince their attendance at drop-in centres indicated a high level of poverty and socialdisadvantage.
After compiling the sampling frame of relevant agencies in the catchment area (see Appendix 2),leaflets giving information about the study were distributed to program participants. Participationin the study was voluntary and only those people who wished to participate were screened. Theinterviewers approached the program participants, discussed the study and conducted the screen.
Details of sampling results appear in Appendix 2. In summary, the estimated overall number ofparticipants in the 10 agencies on an average day was 570. Of those, 150 were screened (26%),among whom 65 (43%) screened positive. See Table B1.1, Appendix 2. As people werescreened, those identified as positive for psychosis and fulfilling the other inclusion criteria wereinvited for interview, or listed for later approach. The quota for interview in this segment of thestudy was 25. Initially, arrangements were made for interview the same day. However, in view ofa greater than expected proportion of screens with positive results, the procedure was changedmid-way through the study period. The names of people eligible for interview were listed, and arandom sample of individuals generated for sequential approach requesting agreement to the in-depth interview. If an individual screened positive but was intoxicated, behaved in an aggressivemanner, or was severely agitated, then the interviewer neither invited that person for interviewnor put their name on the list.
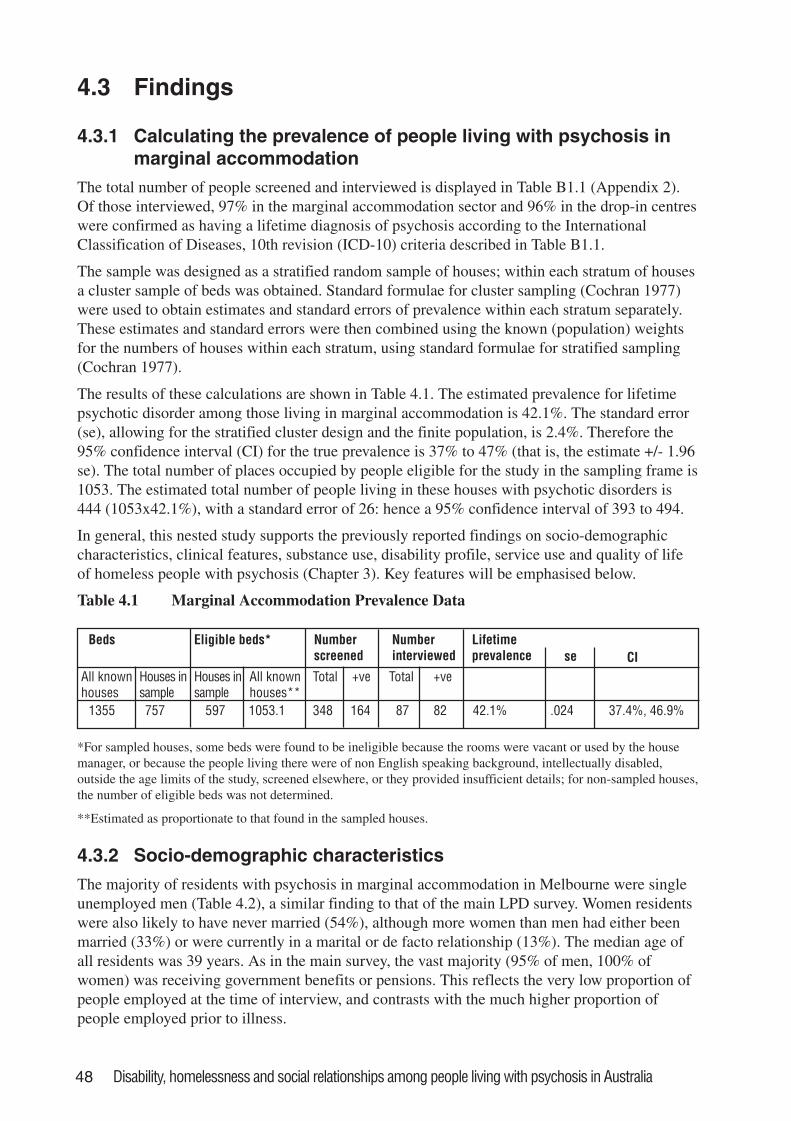
48 Disability, homelessness and social relationships among people living with psychosis in Australia
4.3 Findings
4.3.1 Calculating the prevalence of people living with psychosis inmarginal accommodation
The total number of people screened and interviewed is displayed in Table B1.1 (Appendix 2).Of those interviewed, 97% in the marginal accommodation sector and 96% in the drop-in centreswere confirmed as having a lifetime diagnosis of psychosis according to the InternationalClassification of Diseases, 10th revision (ICD-10) criteria described in Table B1.1.
The sample was designed as a stratified random sample of houses; within each stratum of housesa cluster sample of beds was obtained. Standard formulae for cluster sampling (Cochran 1977)were used to obtain estimates and standard errors of prevalence within each stratum separately.These estimates and standard errors were then combined using the known (population) weightsfor the numbers of houses within each stratum, using standard formulae for stratified sampling(Cochran 1977).
The results of these calculations are shown in Table 4.1. The estimated prevalence for lifetimepsychotic disorder among those living in marginal accommodation is 42.1%. The standard error(se), allowing for the stratified cluster design and the finite population, is 2.4%. Therefore the95% confidence interval (CI) for the true prevalence is 37% to 47% (that is, the estimate +/- 1.96se). The total number of places occupied by people eligible for the study in the sampling frame is1053. The estimated total number of people living in these houses with psychotic disorders is444 (1053x42.1%), with a standard error of 26: hence a 95% confidence interval of 393 to 494.
In general, this nested study supports the previously reported findings on socio-demographiccharacteristics, clinical features, substance use, disability profile, service use and quality of lifeof homeless people with psychosis (Chapter 3). Key features will be emphasised below.
Table 4.1 Marginal Accommodation Prevalence Data
Beds Eligible beds* Numberscreened
Numberinterviewed
Lifetimeprevalence CI
All knownhouses
Houses insample
Houses insample
All knownhouses**
Total +ve Total +ve
1355 757 597 1053.1 348 164 87 82 42.1% .024 37.4%, 46.9%
se
*For sampled houses, some beds were found to be ineligible because the rooms were vacant or used by the housemanager, or because the people living there were of non English speaking background, intellectually disabled,outside the age limits of the study, screened elsewhere, or they provided insufficient details; for non-sampled houses,the number of eligible beds was not determined.
**Estimated as proportionate to that found in the sampled houses.
4.3.2 Socio-demographic characteristics
The majority of residents with psychosis in marginal accommodation in Melbourne were singleunemployed men (Table 4.2), a similar finding to that of the main LPD survey. Women residentswere also likely to have never married (54%), although more women than men had either beenmarried (33%) or were currently in a marital or de facto relationship (13%). The median age ofall residents was 39 years. As in the main survey, the vast majority (95% of men, 100% ofwomen) was receiving government benefits or pensions. This reflects the very low proportion ofpeople employed at the time of interview, and contrasts with the much higher proportion ofpeople employed prior to illness.
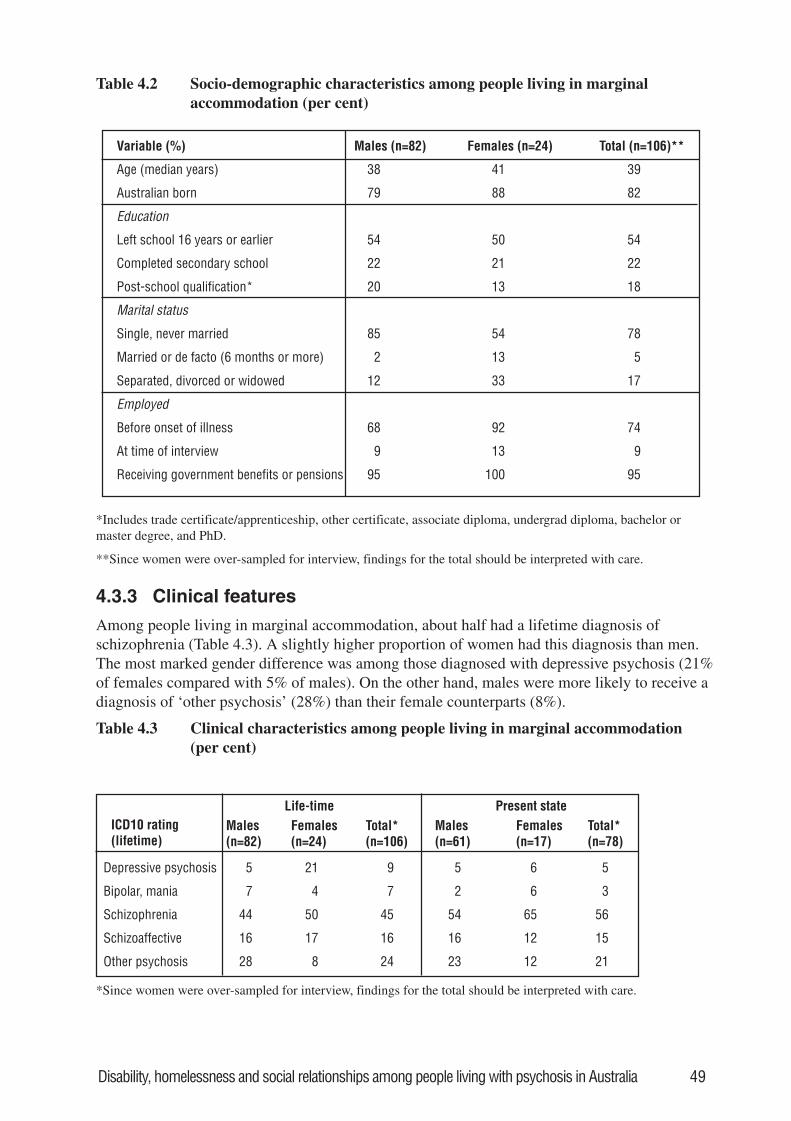
Disability, homelessness and social relationships among people living with psychosis in Australia 49
Table 4.2 Socio-demographic characteristics among people living in marginalaccommodation (per cent)
Variable (%) Males (n=82) Females (n=24) Total (n=106)**
Age (median years) 38 41 39
Australian born 79 88 82
Education
Left school 16 years or earlier 54 50 54
Completed secondary school 22 21 22
Post-school qualification* 20 13 18
Marital status
Single, never married 85 54 78
Married or de facto (6 months or more) 2 13 5
Separated, divorced or widowed 12 33 17
Employed
Before onset of illness 68 92 74
At time of interview 9 13 9
Receiving government benefits or pensions 95 100 95
*Includes trade certificate/apprenticeship, other certificate, associate diploma, undergrad diploma, bachelor ormaster degree, and PhD.
**Since women were over-sampled for interview, findings for the total should be interpreted with care.
4.3.3 Clinical features
Among people living in marginal accommodation, about half had a lifetime diagnosis ofschizophrenia (Table 4.3). A slightly higher proportion of women had this diagnosis than men.The most marked gender difference was among those diagnosed with depressive psychosis (21%of females compared with 5% of males). On the other hand, males were more likely to receive adiagnosis of ‘other psychosis’ (28%) than their female counterparts (8%).
Table 4.3 Clinical characteristics among people living in marginal accommodation(per cent)
Life-time Present stateICD10 rating(lifetime)
Males(n=82)
Females(n=24)
Total*(n=106)
Males(n=61)
Females(n=17)
Total*(n=78)
Depressive psychosis 5 21 9 5 6 5
Bipolar, mania 7 4 7 2 6 3
Schizophrenia 44 50 45 54 65 56
Schizoaffective 16 17 16 16 12 15
Other psychosis 28 8 24 23 12 21
*Since women were over-sampled for interview, findings for the total should be interpreted with care.
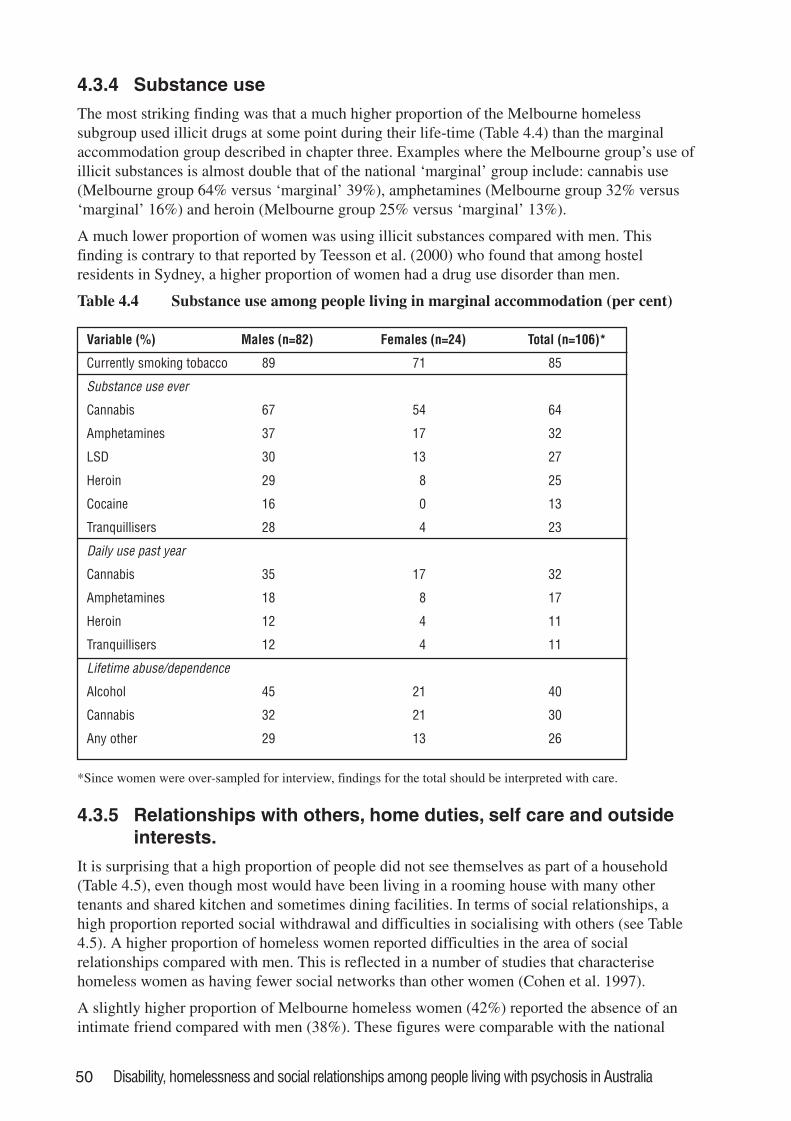
50 Disability, homelessness and social relationships among people living with psychosis in Australia
4.3.4 Substance use
The most striking finding was that a much higher proportion of the Melbourne homelesssubgroup used illicit drugs at some point during their life-time (Table 4.4) than the marginalaccommodation group described in chapter three. Examples where the Melbourne group’s use ofillicit substances is almost double that of the national ‘marginal’ group include: cannabis use(Melbourne group 64% versus ‘marginal’ 39%), amphetamines (Melbourne group 32% versus‘marginal’ 16%) and heroin (Melbourne group 25% versus ‘marginal’ 13%).
A much lower proportion of women was using illicit substances compared with men. Thisfinding is contrary to that reported by Teesson et al. (2000) who found that among hostelresidents in Sydney, a higher proportion of women had a drug use disorder than men.
Table 4.4 Substance use among people living in marginal accommodation (per cent)
Variable (%) Males (n=82) Females (n=24) Total (n=106)*
Currently smoking tobacco 89 71 85
Substance use ever
Cannabis 67 54 64
Amphetamines 37 17 32
LSD 30 13 27
Heroin 29 8 25
Cocaine 16 0 13
Tranquillisers 28 4 23
Daily use past year
Cannabis 35 17 32
Amphetamines 18 8 17
Heroin 12 4 11
Tranquillisers 12 4 11
Lifetime abuse/dependence
Alcohol 45 21 40
Cannabis 32 21 30
Any other 29 13 26
*Since women were over-sampled for interview, findings for the total should be interpreted with care.
4.3.5 Relationships with others, home duties, self care and outsideinterests.
It is surprising that a high proportion of people did not see themselves as part of a household(Table 4.5), even though most would have been living in a rooming house with many othertenants and shared kitchen and sometimes dining facilities. In terms of social relationships, ahigh proportion reported social withdrawal and difficulties in socialising with others (see Table4.5). A higher proportion of homeless women reported difficulties in the area of socialrelationships compared with men. This is reflected in a number of studies that characterisehomeless women as having fewer social networks than other women (Cohen et al. 1997).
A slightly higher proportion of Melbourne homeless women (42%) reported the absence of anintimate friend compared with men (38%). These figures were comparable with the national
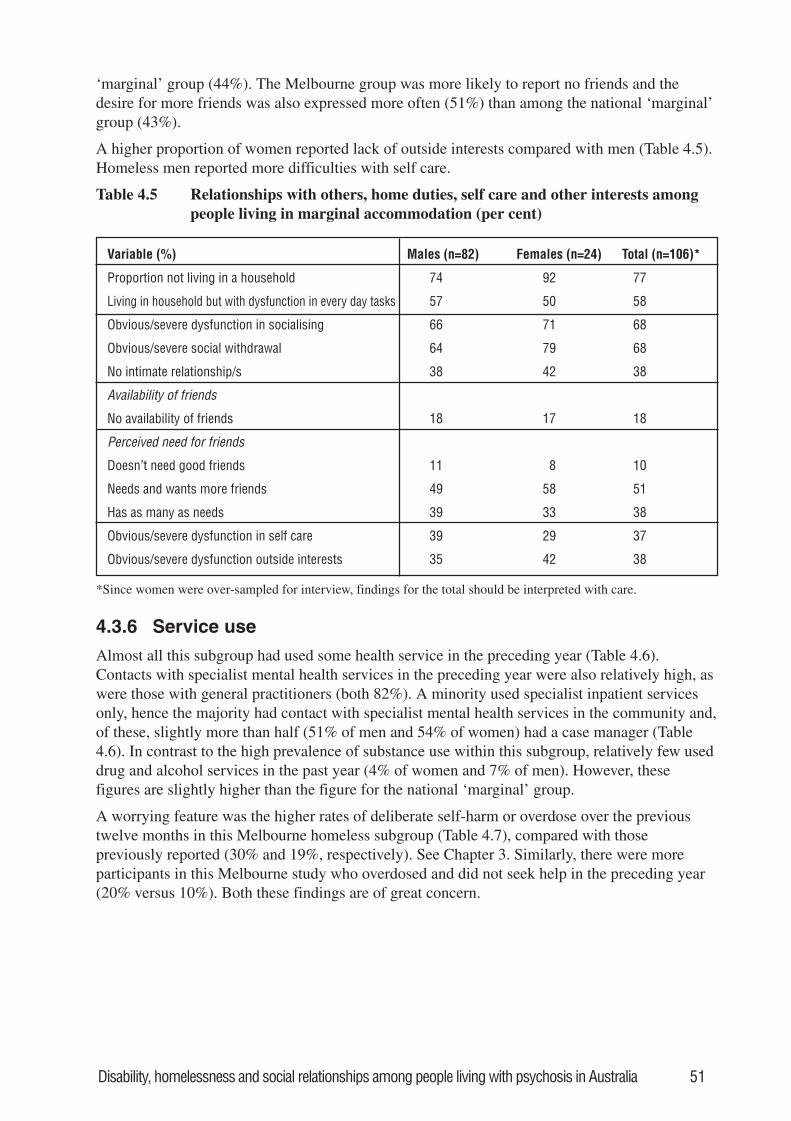
Disability, homelessness and social relationships among people living with psychosis in Australia 51
‘marginal’ group (44%). The Melbourne group was more likely to report no friends and thedesire for more friends was also expressed more often (51%) than among the national ‘marginal’group (43%).
A higher proportion of women reported lack of outside interests compared with men (Table 4.5).Homeless men reported more difficulties with self care.
Table 4.5 Relationships with others, home duties, self care and other interests amongpeople living in marginal accommodation (per cent)
Variable (%) Males (n=82) Females (n=24) Total (n=106)*
Proportion not living in a household 74 92 77
Living in household but with dysfunction in every day tasks 57 50 58
Obvious/severe dysfunction in socialising 66 71 68
Obvious/severe social withdrawal 64 79 68
No intimate relationship/s 38 42 38
Availability of friends
No availability of friends 18 17 18
Perceived need for friends
Doesn’t need good friends 11 8 10
Needs and wants more friends 49 58 51
Has as many as needs 39 33 38
Obvious/severe dysfunction in self care 39 29 37
Obvious/severe dysfunction outside interests 35 42 38
*Since women were over-sampled for interview, findings for the total should be interpreted with care.
4.3.6 Service use
Almost all this subgroup had used some health service in the preceding year (Table 4.6).Contacts with specialist mental health services in the preceding year were also relatively high, aswere those with general practitioners (both 82%). A minority used specialist inpatient servicesonly, hence the majority had contact with specialist mental health services in the community and,of these, slightly more than half (51% of men and 54% of women) had a case manager (Table4.6). In contrast to the high prevalence of substance use within this subgroup, relatively few useddrug and alcohol services in the past year (4% of women and 7% of men). However, thesefigures are slightly higher than the figure for the national ‘marginal’ group.
A worrying feature was the higher rates of deliberate self-harm or overdose over the previoustwelve months in this Melbourne homeless subgroup (Table 4.7), compared with thosepreviously reported (30% and 19%, respectively). See Chapter 3. Similarly, there were moreparticipants in this Melbourne study who overdosed and did not seek help in the preceding year(20% versus 10%). Both these findings are of great concern.
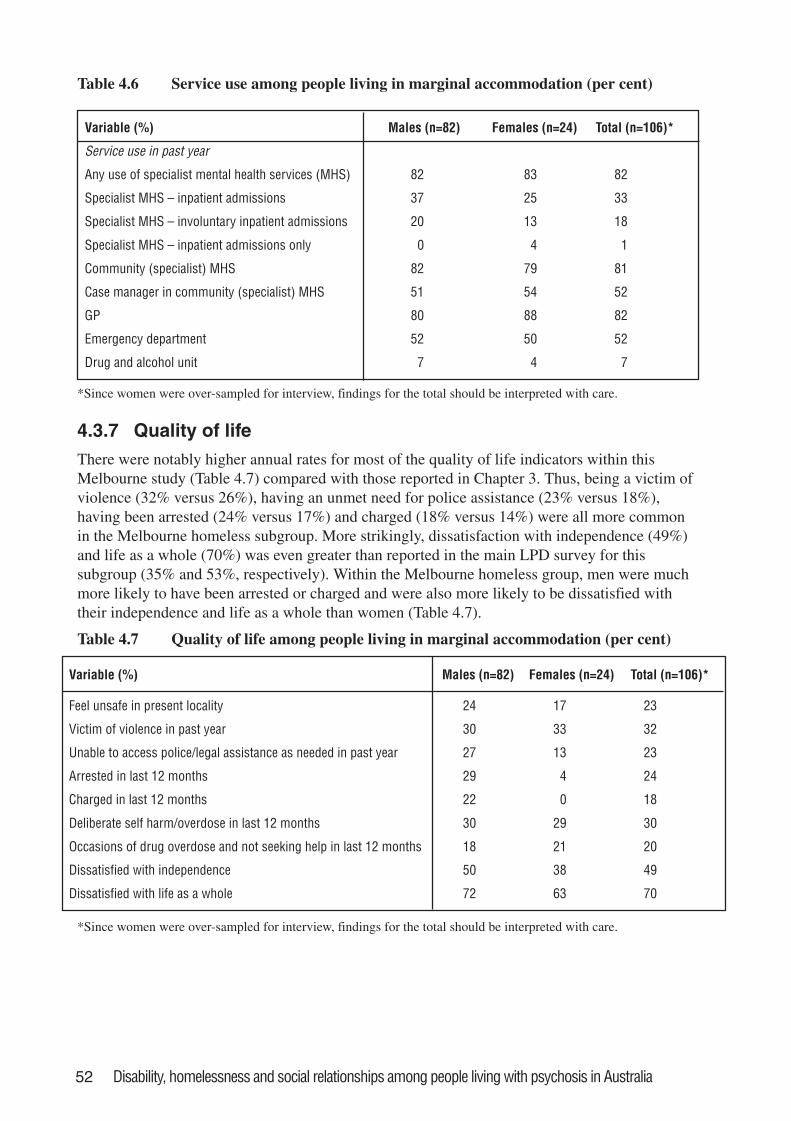
52 Disability, homelessness and social relationships among people living with psychosis in Australia
Table 4.6 Service use among people living in marginal accommodation (per cent)
Variable (%) Males (n=82) Females (n=24) Total (n=106)*
Service use in past year
Any use of specialist mental health services (MHS) 82 83 82
Specialist MHS – inpatient admissions 37 25 33
Specialist MHS – involuntary inpatient admissions 20 13 18
Specialist MHS – inpatient admissions only 0 4 1
Community (specialist) MHS 82 79 81
Case manager in community (specialist) MHS 51 54 52
GP 80 88 82
Emergency department 52 50 52
Drug and alcohol unit 7 4 7
*Since women were over-sampled for interview, findings for the total should be interpreted with care.
4.3.7 Quality of lifeThere were notably higher annual rates for most of the quality of life indicators within thisMelbourne study (Table 4.7) compared with those reported in Chapter 3. Thus, being a victim ofviolence (32% versus 26%), having an unmet need for police assistance (23% versus 18%),having been arrested (24% versus 17%) and charged (18% versus 14%) were all more commonin the Melbourne homeless subgroup. More strikingly, dissatisfaction with independence (49%)and life as a whole (70%) was even greater than reported in the main LPD survey for thissubgroup (35% and 53%, respectively). Within the Melbourne homeless group, men were muchmore likely to have been arrested or charged and were also more likely to be dissatisfied withtheir independence and life as a whole than women (Table 4.7).
Table 4.7 Quality of life among people living in marginal accommodation (per cent)
Variable (%) Males (n=82) Females (n=24) Total (n=106)*
Feel unsafe in present locality 24 17 23
Victim of violence in past year 30 33 32
Unable to access police/legal assistance as needed in past year 27 13 23
Arrested in last 12 months 29 4 24
Charged in last 12 months 22 0 18
Deliberate self harm/overdose in last 12 months 30 29 30
Occasions of drug overdose and not seeking help in last 12 months 18 21 20
Dissatisfied with independence 50 38 49
Dissatisfied with life as a whole 72 63 70
*Since women were over-sampled for interview, findings for the total should be interpreted with care.
Disability, homelessness and social relationships among people living with psychosis in Australia 53
4.4 ConclusionsThere is an unexpectedly high prevalence of people living with psychotic disorders in marginalaccommodation in Melbourne (42%). This compares with findings in 1989 whereby 21% ofpeople living in marginal settings in Melbourne had a lifetime diagnosis of psychosis (Herrmanet al. 1989).
Housing for people on low incomes in the two cities had become much scarcer over several yearsbefore the study. For instance, in the City of Boroondara in 1987 there were 53 houses (786beds); in 1995 there were 22 houses (486 beds) [source: Inner Eastern Regional Housing NeedsAssessment, 1995]; and in 1997 there were 20 houses (419 beds) [field work for this study].
There is a possible link between these two observations above – that is, as housing for people onlow incomes becomes scarcer, it may be increasingly occupied by those who are particularlydisabled or disadvantaged, of whom people with psychosis are an important subgroup.
Except for those people with psychosis in institutional settings, disability in everyday,occupational and social functioning is higher for those living in marginal accommodation thanany other group. See Chapter 3. The high level of unemployment and the frequency ofdifficulties with social relationships (both the perceived success of social interactions as well asthe degree of avoidance of the same) are particularly striking.
The degree to which residents are experiencing a lack of safety in their day-to-day environmentalso deserves comment. As already noted, safety is a valued attribute of people’saccommodation. This relative lack of safety together with other adverse features of theenvironment may be contributing to the high levels of dissatisfaction observed amongst residents.
The frequent use of illicit substances of all types as well as high rates of lifetime abuse anddependence in this homeless subgroup of people with psychosis has enormous implications. Thisis especially so given the low rate of use of drug and alcohol services. Previous studies in Sydneyand Melbourne (Herrman et al. 1989; Teesson et al. 2000), and in other countries, havedocumented similar high rates of overlap in individual homeless respondents between substancedependence and mood and psychotic disorders. Such co-morbidity of substance use with mentaldisorders is probably an important factor in the genesis of homelessness. Co-morbidity is also aproblem in homeless women, although the rates of disorder reported here are less than those inmen. The needs of those with dual diagnosis are especially complex. However, work in the US inparticular has shown that flexible, coordinated and adequately resourced services can make adifference to most people, even those with severe disabilities. Both early intervention andrehabilitation or maintenance in adequate housing with opportunities for social contact andactivity are useful and appropriate.
Homeless women with psychotic illness have some particular characteristics pointing to adifferent profile of needs. Co-morbidity of psychotic illness with substance use is high, althoughless than for homeless men, as already indicated. Homeless women in Melbourne have adifferent profile of psychotic diagnoses compared with men, with more experiencing psychoticdepression. Furthermore, more homeless women than men are married or have previously beenso, indicating a possible role of marital breakdown in their progression to homelessness. Finally,the women in this study had greater difficulties in their social functioning and were less likely tohave an intimate relationship compared with men.
The findings raise the question: is this the best we can do? This study was undertaken in acatchment area with an organised, sectorised, specialist mental health service. There were highrates of contact with specialist mental health services, including community mental healthservices, among those interviewed. There were also high rates of contact with general
54 Disability, homelessness and social relationships among people living with psychosis in Australia
practitioners and hospital emergency services. However, we do not know the focus of thesecontacts with services, whether they were addressing mental health issues and associateddisabilities (as documented above) and indeed, whether these services were in contact with eachother. It has been previously reported that people, when they have access to specialist services,do make contact with them (Herrman et al. 1989). However, at the same time they have highlevels of disability and unmet needs. As previously argued, existing methods of assessingdisability are not especially good, and a more intensive analysis of needs is required (Hogg andMarshall 1992). Furthermore, the low use of rehabilitation and vocational services has alreadybeen noted. Even the best clinical services will fail to meet the needs of those with the mostcomplex problems unless there is close co-operation with housing, welfare and disability supportservices (including vocational services) to provide support and assistance to each individual.
4.5 Recommendations4.5.1 More in-depth analyses of disability and unmet need among homeless people with
psychosis are required, including the perspective of residents and staff. The results will becrucial information for planning future services.
4.5.2 Service systems must be linked at all levels to remove barriers and promote efficient useof services; this includes psychiatric services with housing, social services, substanceabuse treatment, and the criminal justice system. In particular, coordinated serviceprovision is essential for those with complex needs.
4.5.3 Substance abuse treatment must be an integral part of comprehensive psychiatric servicesfor people with severe mental illnesses.
4.5.4 While wider factors are involved, attention to risk factors at the individual level mayreverse or prevent a drift towards homelessness. Thus, good management of severe mentalillness is required and is similar in principle whether or not the patients are homeless, andis likely to contribute to the prevention of homelessness. At the same time serviceproviders need to be aware of factors particular to the management of homeless people.The provision of a decent place to live is a primary need, complemented by access toappropriate treatment and support.
4.5.5 A range of housing options is required. Independent living with the availability of supportservices is both possible and preferred by most people with mental illnesses. Because thisdoes not meet the needs or preferences of everyone, however, other choices may have tobe considered. Negotiation of the role, resources and service links of the various sectorsproviding housing support will be necessary for this to be successful.
4.5.6 Preventive health care and education are critical, especially relating to the risks of HIV/AIDS, tuberculosis and smoking. This is most likely to be effective if provided within theframework of accessible and relevant primary health care.
4.5.7 The needs of families and the factors that may enhance the ability and willingness offamilies to provide care have often been disregarded. The breakdown of family links mayincrease the chances of homelessness for an individual with severe mental illness.Therefore, continuing attention to the needs for family and individual support to helpprevent homelessness and its persistence among those with mental illness is required.
4.5.8 The particular needs of homeless women with psychotic disorders need to be addressed inthe provision of appropriate services. These will include attention to marital breakdownand wider aspects of social functioning.
4.5.9 Research programs into homelessness and serious mental illness should include longer-term follow-up studies that focus on how to sustain early gains.
Disability, homelessness and social relationships among people living with psychosis in Australia 55
5. Social networks and functioning ofpeople with psychosis
S is a 33 year old female who lives in her own home with her husband and threechildren. She felt very sad after having her last child. She was very lonely and didnot have any family support as her parents live in the country. Her friends werehelpful but there was only so much she could ask. She started to develop thoughtsthat she was very important. Everything that was said to her took on specialsignificance; it was like people were talking in metaphors. She saw herself beingtalked about on the television and in newspaper headlines. Things came to a crisiswhen she thought that she and her children were dead. She stayed in hospital for afew weeks and was discharged into the care of a private psychiatrist. Her husbandhas been very supportive and took time off work to spend time with her and thefamily. She is mostly satisfied with the future and believes it is important to havemore support services.
5.1 People with schizophrenia and their socialnetworks
Most studies of the association between people’s social relationships and their overall well-beinghave looked at people’s social networks – defined as the organisation of people’s ties to oneanother, the frequency of their contact with various network members, and in particular thenumber of relationships or social roles a person has (Thoits 1995). Social support, on the otherhand, is a subjective assessment of the affective or emotional value of the network interactions(Albert et al. 1998). It has been concluded that social networks and social support have benefitsfor the individual by either acting as a buffer against stress, assisting in recovery from physicalillness, or having positive effects on general well-being (Henderson 1988). In the field of mentalillness, most studies have concentrated on people with schizophrenia and the evidence for abeneficial effect of wider social networks and greater social support in those with psychosis(especially schizophrenia) is still accumulating (Buchanan 1995). Indeed, it has been noted thatcertain types of social interaction are too stressful for some people with psychosis (Buchanan1995). Nevertheless, positive benefits of social support include a role in preventing homelessnessamong people with psychotic disorders (Odell and Commander 2000). It is certainly the case thatpeople with schizophrenia are more likely to have smaller social networks and their network islikely to decrease as duration of illness increases. Also, their network is more likely to comprisefamily members and to be made up of more dependent relationships than for people from thegeneral community (Hammer et al. 1978; Buchanan 1995; Albert et al. 1998; Becker et al. 1998).
Among members of the general population, an intimate psychosocial network consists of about25 people. In contrast, people with severe mental illness report between 5 and 13 people in theirsocial network (Albert et al. 1998). It appears that the most dramatic reduction in social networksoccurs after the first hospitalisation. People with schizophrenia assessed during their firstadmission reported larger social networks than those assessed after a number of hospitaladmissions (Lipton et al. 1981). The latter were more likely to have family contacts andproportionally fewer friendship or acquaintance contacts; indeed, one third did not have a closefriend (Lipton et al. 1981). Thus, it seems likely that the family network declines less rapidlythan friendship networks in the course of a schizophrenic illness.
56 Disability, homelessness and social relationships among people living with psychosis in Australia
The interactions between persons with severe mental illness and their families are complex andthe impact of having family in one’s network may be mixed. For instance, several studies havereported that persons whose social networks are composed primarily of friends, neighbours andothers who were not kin, tended to demonstrate better occupational functioning, bettersymptomatic recovery and lower relapse rates than those whose social networks were composedprimarily of relatives (Henry and Coster 1996). A number of researchers (Brown et al. 1972;Vaughn and Leff 1976; Lukoff et al. 1984) have found that people with schizophrenia were morelikely to relapse if their family members expressed negative emotions towards them. Thesenegative emotions (which could be viewed as less adaptive coping responses) included highlevels of criticism, over-involvement and hostility directed towards the person by a familymember (either a parent or spouse). Erickson et al. (1998) found that non-family social resourceswere correlated with good prognosis in schizophrenia and affective psychosis, while involvementof family members predicted good prognosis among people with affective psychosis but pooroutcomes among people with schizophrenia. However, a Finnish study indicated that people withschizophrenia who were living outside of their family, particularly men, were less likely to havegood recovery of their functioning over a five year period (Salokangas 1997). These various andcontradictory findings suggest a need to look more carefully at the possible impact of bothfamily and friends in the network of people with psychosis. This is particularly relevant giventhat current models of mental health service delivery do not seem to be very effective inimproving people’s social functioning (Mueser et al. 1998). This chapter aims to describe theLPD participants in terms of their social networks and associated life circumstances.
5.2 Measures and definitions used in this chapter• A ‘social network’ is defined as having face-to-face contact with family and friends in the last
12 months.
• ‘Socially isolated’ refers to no contact or very minimal contact with one family member andno friends or just one friend.
• ‘Friends dominated network’ refers to a few or many friends and no or minimal familycontact.
• ‘Family dominated network’ refers to frequent family contact and one or no friends.
• ‘Socially integrated’ refers to a few or many friends and frequent family contact.
Of the 980 people in the survey, 968 had complete data for the above variables allowing them tobe categorised accordingly.
5.3 FindingsA total of 66 people (7%) were identified as socially isolated. While 112 people (11%) wereidentified as having friends dominated networks, 143 (15%) had family dominated networks.Finally, the majority of participants were classified as socially integrated (647, or 66%).
5.3.1 Socio-demographic characteristicsWhen examining the characteristics of people across these four groups defined by their socialnetworks, there was a higher proportion of males in the socially isolated group (73%) comparedwith that in the socially integrated group (57%). In terms of marital status there were no obviousdifferences between the groups (Table 5.1). Those without family contact in their network wereolder than those with relatives in their network.
A higher proportion of people who were socially isolated was living in marginal accommodation
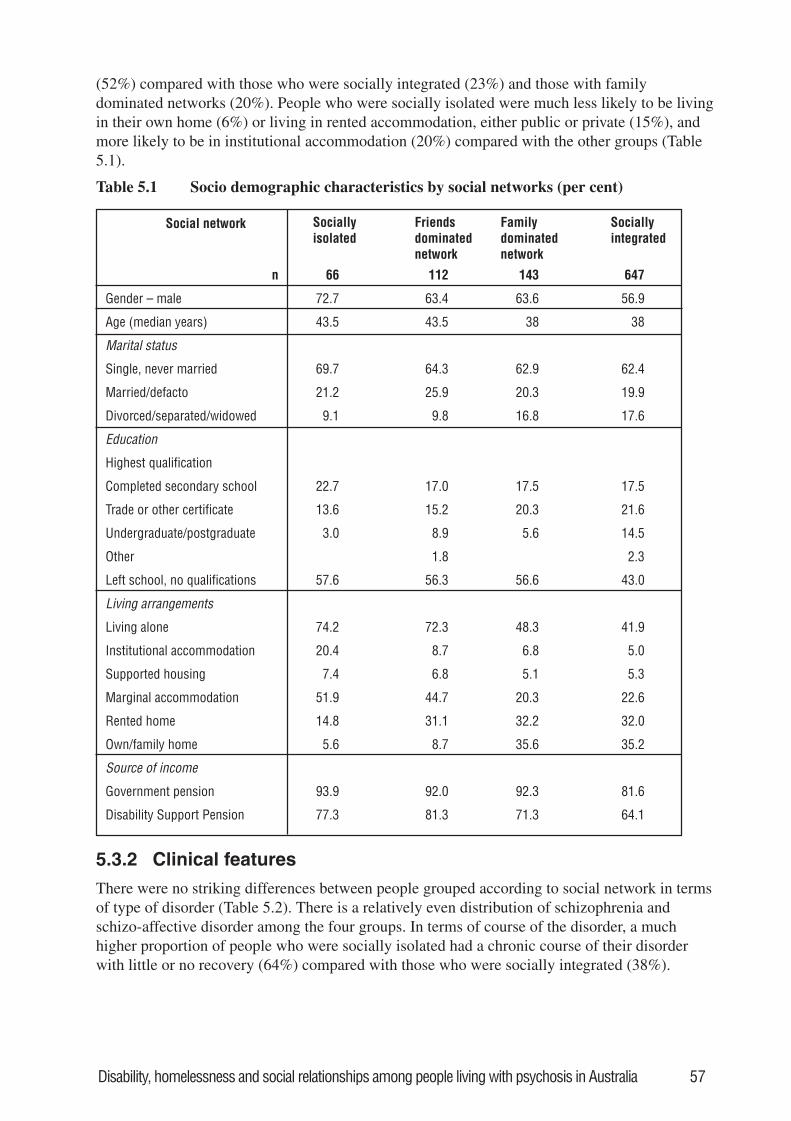
Disability, homelessness and social relationships among people living with psychosis in Australia 57
(52%) compared with those who were socially integrated (23%) and those with familydominated networks (20%). People who were socially isolated were much less likely to be livingin their own home (6%) or living in rented accommodation, either public or private (15%), andmore likely to be in institutional accommodation (20%) compared with the other groups (Table5.1).
Table 5.1 Socio demographic characteristics by social networks (per cent)
Social network Sociallyisolated
Friendsdominatednetwork
Familydominatednetwork
Sociallyintegrated
n 66 112 143 647
Gender – male 72.7 63.4 63.6 56.9
Age (median years) 43.5 43.5 38 38
Marital status
Single, never married 69.7 64.3 62.9 62.4
Married/defacto 21.2 25.9 20.3 19.9
Divorced/separated/widowed 9.1 9.8 16.8 17.6
Education
Highest qualification
Completed secondary school 22.7 17.0 17.5 17.5
Trade or other certificate 13.6 15.2 20.3 21.6
Undergraduate/postgraduate 3.0 8.9 5.6 14.5
Other 1.8 2.3
Left school, no qualifications 57.6 56.3 56.6 43.0
Living arrangements
Living alone 74.2 72.3 48.3 41.9
Institutional accommodation 20.4 8.7 6.8 5.0
Supported housing 7.4 6.8 5.1 5.3
Marginal accommodation 51.9 44.7 20.3 22.6
Rented home 14.8 31.1 32.2 32.0
Own/family home 5.6 8.7 35.6 35.2
Source of income
Government pension 93.9 92.0 92.3 81.6
Disability Support Pension 77.3 81.3 71.3 64.1
5.3.2 Clinical features
There were no striking differences between people grouped according to social network in termsof type of disorder (Table 5.2). There is a relatively even distribution of schizophrenia andschizo-affective disorder among the four groups. In terms of course of the disorder, a muchhigher proportion of people who were socially isolated had a chronic course of their disorderwith little or no recovery (64%) compared with those who were socially integrated (38%).
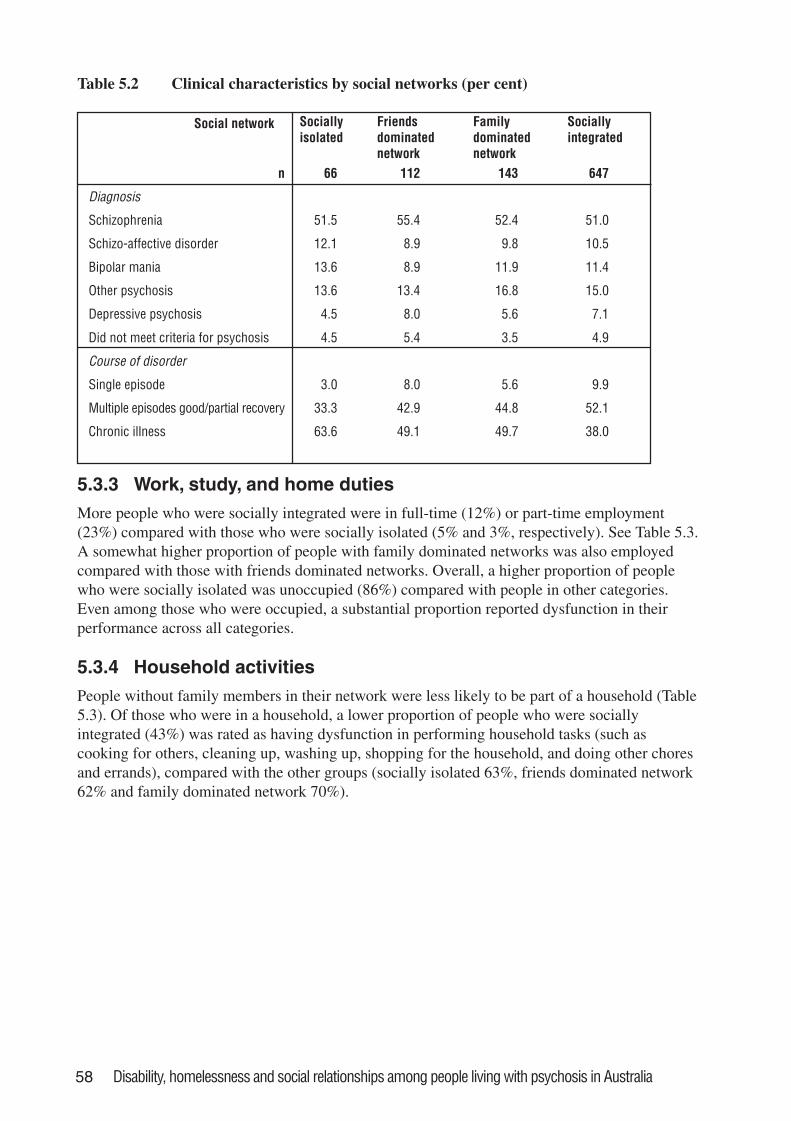
58 Disability, homelessness and social relationships among people living with psychosis in Australia
Table 5.2 Clinical characteristics by social networks (per cent)
Social network Sociallyisolated
Friendsdominatednetwork
Familydominatednetwork
Sociallyintegrated
n 66 112 143 647
Diagnosis
Schizophrenia 51.5 55.4 52.4 51.0
Schizo-affective disorder 12.1 8.9 9.8 10.5
Bipolar mania 13.6 8.9 11.9 11.4
Other psychosis 13.6 13.4 16.8 15.0
Depressive psychosis 4.5 8.0 5.6 7.1
Did not meet criteria for psychosis 4.5 5.4 3.5 4.9
Course of disorder
Single episode 3.0 8.0 5.6 9.9
Multiple episodes good/partial recovery 33.3 42.9 44.8 52.1
Chronic illness 63.6 49.1 49.7 38.0
5.3.3 Work, study, and home dutiesMore people who were socially integrated were in full-time (12%) or part-time employment(23%) compared with those who were socially isolated (5% and 3%, respectively). See Table 5.3.A somewhat higher proportion of people with family dominated networks was also employedcompared with those with friends dominated networks. Overall, a higher proportion of peoplewho were socially isolated was unoccupied (86%) compared with people in other categories.Even among those who were occupied, a substantial proportion reported dysfunction in theirperformance across all categories.
5.3.4 Household activitiesPeople without family members in their network were less likely to be part of a household (Table5.3). Of those who were in a household, a lower proportion of people who were sociallyintegrated (43%) was rated as having dysfunction in performing household tasks (such ascooking for others, cleaning up, washing up, shopping for the household, and doing other choresand errands), compared with the other groups (socially isolated 63%, friends dominated network62% and family dominated network 70%).
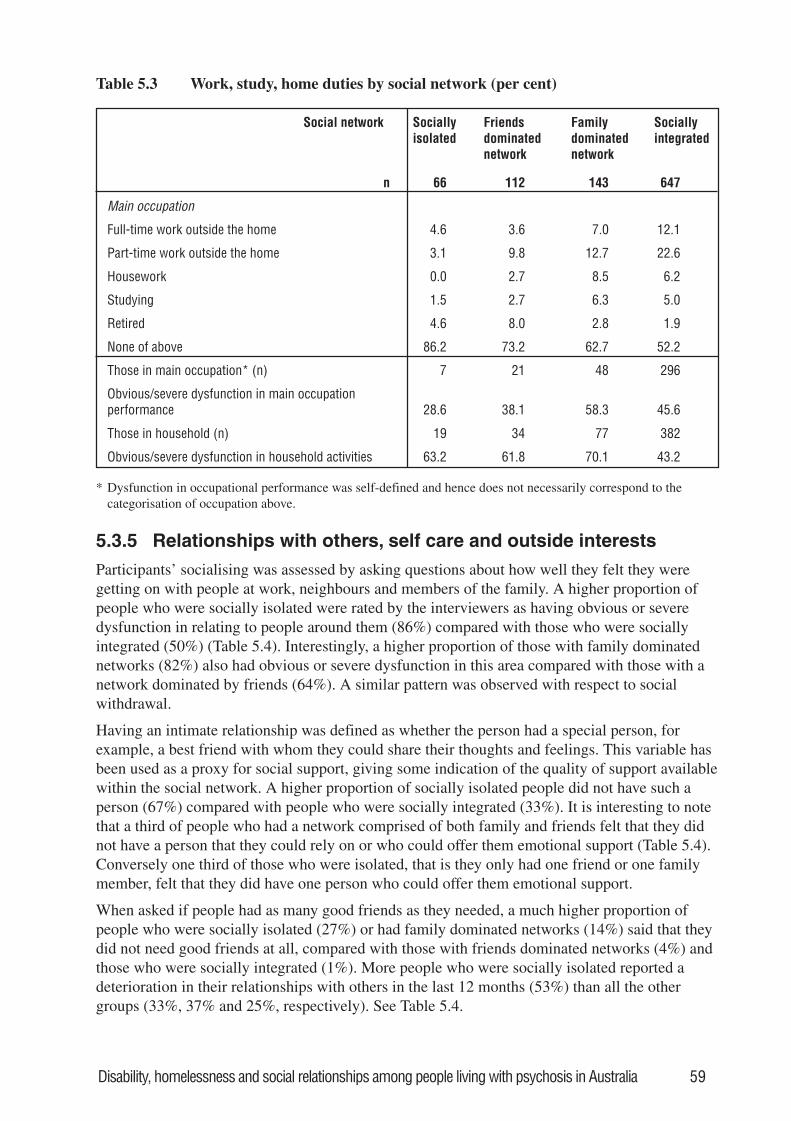
Disability, homelessness and social relationships among people living with psychosis in Australia 59
Table 5.3 Work, study, home duties by social network (per cent)
Social network Sociallyisolated
Friendsdominatednetwork
Familydominatednetwork
Sociallyintegrated
n 66 112 143 647
Main occupation
Full-time work outside the home 4.6 3.6 7.0 12.1
Part-time work outside the home 3.1 9.8 12.7 22.6
Housework 0.0 2.7 8.5 6.2
Studying 1.5 2.7 6.3 5.0
Retired 4.6 8.0 2.8 1.9
None of above 86.2 73.2 62.7 52.2
Those in main occupation* (n) 7 21 48 296
Obvious/severe dysfunction in main occupationperformance 28.6 38.1 58.3 45.6
Those in household (n) 19 34 77 382
Obvious/severe dysfunction in household activities 63.2 61.8 70.1 43.2
* Dysfunction in occupational performance was self-defined and hence does not necessarily correspond to thecategorisation of occupation above.
5.3.5 Relationships with others, self care and outside interests
Participants’ socialising was assessed by asking questions about how well they felt they weregetting on with people at work, neighbours and members of the family. A higher proportion ofpeople who were socially isolated were rated by the interviewers as having obvious or severedysfunction in relating to people around them (86%) compared with those who were sociallyintegrated (50%) (Table 5.4). Interestingly, a higher proportion of those with family dominatednetworks (82%) also had obvious or severe dysfunction in this area compared with those with anetwork dominated by friends (64%). A similar pattern was observed with respect to socialwithdrawal.
Having an intimate relationship was defined as whether the person had a special person, forexample, a best friend with whom they could share their thoughts and feelings. This variable hasbeen used as a proxy for social support, giving some indication of the quality of support availablewithin the social network. A higher proportion of socially isolated people did not have such aperson (67%) compared with people who were socially integrated (33%). It is interesting to notethat a third of people who had a network comprised of both family and friends felt that they didnot have a person that they could rely on or who could offer them emotional support (Table 5.4).Conversely one third of those who were isolated, that is they only had one friend or one familymember, felt that they did have one person who could offer them emotional support.
When asked if people had as many good friends as they needed, a much higher proportion ofpeople who were socially isolated (27%) or had family dominated networks (14%) said that theydid not need good friends at all, compared with those with friends dominated networks (4%) andthose who were socially integrated (1%). More people who were socially isolated reported adeterioration in their relationships with others in the last 12 months (53%) than all the othergroups (33%, 37% and 25%, respectively). See Table 5.4.
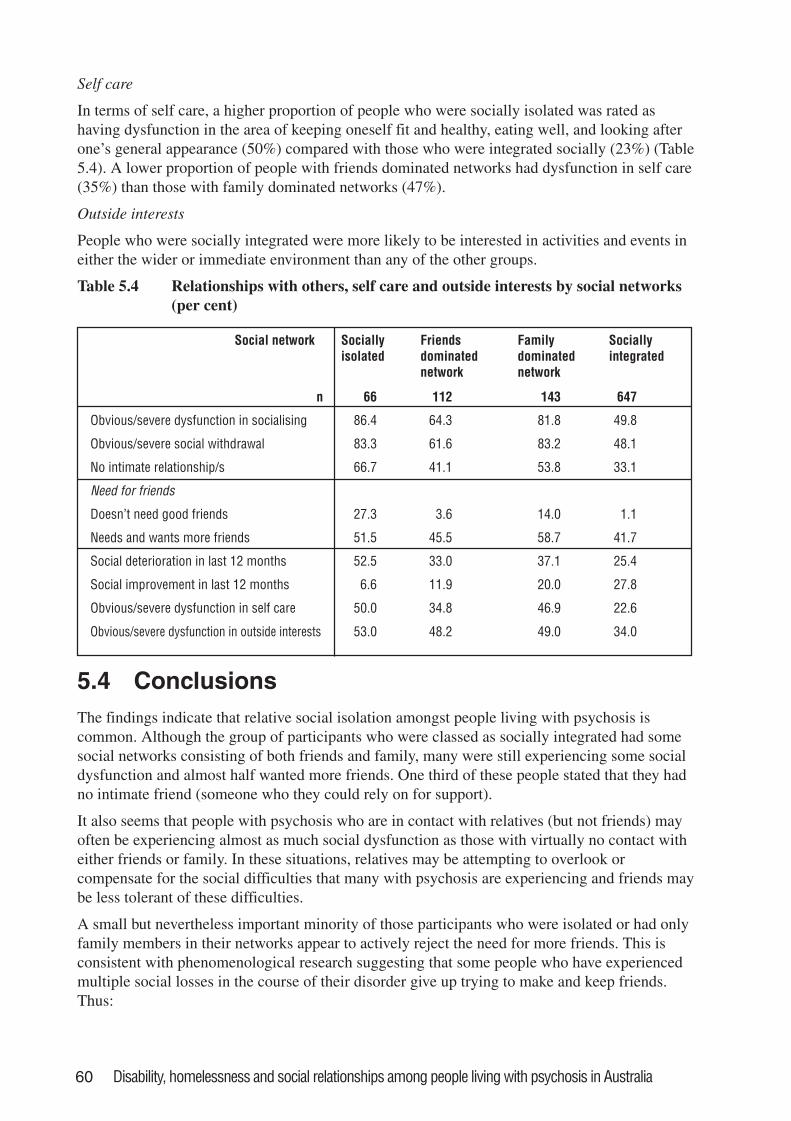
60 Disability, homelessness and social relationships among people living with psychosis in Australia
Self care
In terms of self care, a higher proportion of people who were socially isolated was rated ashaving dysfunction in the area of keeping oneself fit and healthy, eating well, and looking afterone’s general appearance (50%) compared with those who were integrated socially (23%) (Table5.4). A lower proportion of people with friends dominated networks had dysfunction in self care(35%) than those with family dominated networks (47%).
Outside interests
People who were socially integrated were more likely to be interested in activities and events ineither the wider or immediate environment than any of the other groups.
Table 5.4 Relationships with others, self care and outside interests by social networks(per cent)
Social network Sociallyisolated
Friendsdominatednetwork
Familydominatednetwork
Sociallyintegrated
n 66 112 143 647
Obvious/severe dysfunction in socialising 86.4 64.3 81.8 49.8
Obvious/severe social withdrawal 83.3 61.6 83.2 48.1
No intimate relationship/s 66.7 41.1 53.8 33.1
Need for friends
Doesn’t need good friends 27.3 3.6 14.0 1.1
Needs and wants more friends 51.5 45.5 58.7 41.7
Social deterioration in last 12 months 52.5 33.0 37.1 25.4
Social improvement in last 12 months 6.6 11.9 20.0 27.8
Obvious/severe dysfunction in self care 50.0 34.8 46.9 22.6
Obvious/severe dysfunction in outside interests 53.0 48.2 49.0 34.0
5.4 ConclusionsThe findings indicate that relative social isolation amongst people living with psychosis iscommon. Although the group of participants who were classed as socially integrated had somesocial networks consisting of both friends and family, many were still experiencing some socialdysfunction and almost half wanted more friends. One third of these people stated that they hadno intimate friend (someone who they could rely on for support).
It also seems that people with psychosis who are in contact with relatives (but not friends) mayoften be experiencing almost as much social dysfunction as those with virtually no contact witheither friends or family. In these situations, relatives may be attempting to overlook orcompensate for the social difficulties that many with psychosis are experiencing and friends maybe less tolerant of these difficulties.
A small but nevertheless important minority of those participants who were isolated or had onlyfamily members in their networks appear to actively reject the need for more friends. This isconsistent with phenomenological research suggesting that some people who have experiencedmultiple social losses in the course of their disorder give up trying to make and keep friends.Thus:
Disability, homelessness and social relationships among people living with psychosis in Australia 61
For us giving up was a way of surviving. Giving up, refusing to hope. Not trying. Notcaring: all of these were ways of trying to protect the last fragile traces of our spiritand our selfhood from undergoing another crushing. (Davidson and Stayner 1997,p.10).
Nevertheless, there may be underlying needs and desires for social relationships –‘despite theiroutward appearance at times suggesting the contrary’ (Davidson et al. 2001, p.276).
There is an important association between social isolation and socio-economic disadvantage,such as lack of employment and inadequate housing. The most socially isolated individuals arefar less likely to have a job or live in ‘independent accommodation’ (own or family home orrented accommodation). It is possible that stigma, lack of employment and poverty as indicatedby sub-standard accommodation may limit a person’s opportunity for social participation, whichin turn may limit their ability to meet new people and retain old friendships. Some of theexplanation for this association may also be afforded by the more chronic course of illnessexperienced by the socially isolated, which allows little respite from symptoms during which topursue a social life. However, it is also possible that social isolation leads to greater apparent‘chronicity’ of illness.
The presence of other people in a person’s living arrangement may not truly reflect theiropportunities for, and engagement in, social interactions. For example, many people living ininstitutional settings or marginal accommodation where other people are often around arenevertheless socially isolated. Conversely, one cannot assume that people who are living in rentalproperties (often alone) are without contact with friends and family. This is consistent withresearch by Brown (1996) indicating that when people were compared across living situations(living alone, in a group home, with family) there was no difference in reported loneliness.
It has already been noted that the ability to care for oneself is an important goal for consumersand a valued contributor to quality of life. It is striking that those survey participants who hadfriends in their social networks were rated as having better self care. It is possible that friendshipsserve as a greater incentive for those with mental illness to look after themselves, via interactionsand activities that promote self-esteem. Alternatively, it may be that families are more tolerantthan friends and acquaintances of people’s difficulties in this area. The converse association isobserved for employment. People with networks dominated by family were more likely to beemployed than those in friends dominated networks. It seems likely that the nature of people’ssocial networks, whether primarily composed of friends or family members, may have differingrelationships to varied aspects of their functioning.
Consistent with the literature on social networks, the type of psychotic disorder (diagnosis) bearslittle relationship to people’s social networks. However, the course of the psychotic disorder isimportant, since those people experiencing little or no recovery are more likely to be isolated.
5.5 Recommendations5.5.1 Community mental health services should broaden their focus to provide psychological,
social and practical input that will assist people with psychosis to establish and re-establish their social networks and also provide support to maintain existing networks toprevent future loss or deterioration in relationships. In this regard, people’s preferencesshould be taken into account, since some people actively reject more friends: theunderlying causes of this require exploration.
62 Disability, homelessness and social relationships among people living with psychosis in Australia
5.5.2 Public education campaigns are required to combat stigma and minimise the possibilitythat friendships and family relationships will be disrupted by the experience of psychoticillness. In addition, local, state and national organisations providing social opportunitiesin the broader community should examine whether their policies allow for appropriateaccess by those with psychotic disorders. Significant differences in overall social outcomehave been shown to be associated with differences in mental health policy (de Sisto et al.1995).
5.5.3 People with psychosis who are more socially isolated require greater rehabilitation inputto perform their activities of daily living, including assistance to regain (and learn, ifnecessary) relevant skills. Community mental health services should review their policiesto ensure that they have effective outreach procedures to facilitate their access by peoplewith psychosis who are particularly socially isolated. In addition, this subgroup of peopleshould be specifically targeted by services for assessment of, and effective interventionfor, their difficulties with regard to daily living skills.
5.5.4 Education and training programs are required to develop specific professional skills thatwill assist people with psychosis to improve their social functioning more effectively.
5.5.5 To date, most research has concentrated on the size of a person’s social networks and littleattention has been paid to the quality of existing relationships, that is, how supported theperson feels emotionally and instrumentally. There should be more quantitative andqualitative research that focuses on the quality of relationships of people with psychosis.Further, the expressed needs of consumers with regard to social relationships should besurveyed and taken into account.
5.5.6 Most research studies are designed from the perspective that social dysfunction is aninevitable consequence of the experience of psychotic disorder. Insufficient attention isgiven to the person’s social context and especially to the identified obstacles to socialrelationships that are not directly to do with the disorder (Harding and Keller 1998).These should be considered in future research programs.
Disability, homelessness and social relationships among people living with psychosis in Australia 63
Appendix 1: The Diagnostic Interview forPsychoses-Disability Module (DIP-DIS)
Background and rationale for development of theDIP-DISIn order to assist with service planning, the Study of Low Prevalence Disorders (LPD) aimed toprovide data on the degree of disability associated with the experience of psychosis. This wasdone by assessing those aspects of objective circumstances and subjective experience that have abearing on the quality of life of persons experiencing psychosis (Lehman 1983; Jenkins 1998).The conceptual framework for this assessment of the impact of psychotic disorder was therehabilitation model (Anthony et al. 1990) with its emphasis on disability as restriction or lack ofability in role performance. However, this framework was deliberately broadened to incorporatemore recent notions of the consequences of mental illness embodied in the recovery model(Deegan 1988; Anthony 1993) and in particular, to include more subjective outcomes (Kaiser etal. 1997; Orley et al. 1998).
Existing tools for the assessment of role performance, including social adjustment and quality oflife of persons with mental illness (Weissman et al. 1981; Lehman 1996), were judged to beinappropriate for this survey since they are often specific to particular disorders (for example,schizophrenia) or limited in scope to, for example, social roles (Weissman 1975). Thus, aworking group of the LPD investigators identified qualities that were required in a measure ofdisability. These included:
1) acceptability to largely community-dwelling respondents
2) applicability to persons with psychosis
3) relative comprehensiveness to cover the main areas of disability experienced by people withpsychosis
4) inclusion of the perspective of the patient and clinician
5) brevity (could be administered in 10 - 15 minutes).
The objective was to have an instrument that would measure performance in the areas of personaland social activities and manifest behaviour that could be attributable to illness and not to lack ofpersonal or social opportunities.
The Disability Module (DIP-DIS)As explained in Chapter 2, the DIP-Disability Module (DIP-DIS) consists of a core made up ofan abridged and modified version of the WHO/DAS (World Health Organisation 1988). This wassupplemented by sections of the Lancashire Quality of Life Profile (Oliver et al. 1997) and theCurrent Social Contacts Scale described by Tucker (1982). Items were selected from thesesources to reflect the range of disabilities associated with the experience of psychosis, asidentified during consultative meetings with consumers and mental health professionals. TheDIP-DIS assesses functioning in the areas of participation in household activities, socialising,social withdrawal, quality of interpersonal relationships, occupational performance, interests andinformation, intimate relationships, sexual relationships, and self care. These items are rated byresearch interviewers using all information gathered with a series of open-ended questions to
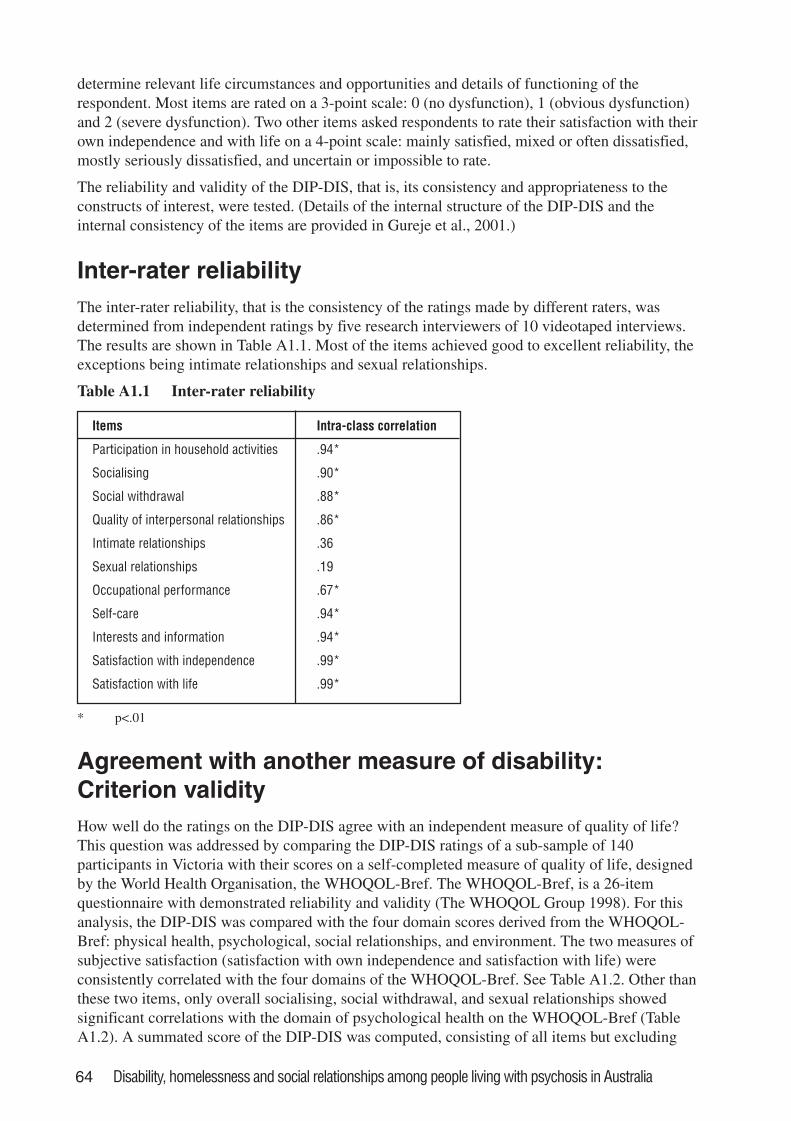
64 Disability, homelessness and social relationships among people living with psychosis in Australia
determine relevant life circumstances and opportunities and details of functioning of therespondent. Most items are rated on a 3-point scale: 0 (no dysfunction), 1 (obvious dysfunction)and 2 (severe dysfunction). Two other items asked respondents to rate their satisfaction with theirown independence and with life on a 4-point scale: mainly satisfied, mixed or often dissatisfied,mostly seriously dissatisfied, and uncertain or impossible to rate.
The reliability and validity of the DIP-DIS, that is, its consistency and appropriateness to theconstructs of interest, were tested. (Details of the internal structure of the DIP-DIS and theinternal consistency of the items are provided in Gureje et al., 2001.)
Inter-rater reliabilityThe inter-rater reliability, that is the consistency of the ratings made by different raters, wasdetermined from independent ratings by five research interviewers of 10 videotaped interviews.The results are shown in Table A1.1. Most of the items achieved good to excellent reliability, theexceptions being intimate relationships and sexual relationships.
Table A1.1 Inter-rater reliability
Items Intra-class correlation
Participation in household activities .94*
Socialising .90*
Social withdrawal .88*
Quality of interpersonal relationships .86*
Intimate relationships .36
Sexual relationships .19
Occupational performance .67*
Self-care .94*
Interests and information .94*
Satisfaction with independence .99*
Satisfaction with life .99*
* p<.01
Agreement with another measure of disability:Criterion validityHow well do the ratings on the DIP-DIS agree with an independent measure of quality of life?This question was addressed by comparing the DIP-DIS ratings of a sub-sample of 140participants in Victoria with their scores on a self-completed measure of quality of life, designedby the World Health Organisation, the WHOQOL-Bref. The WHOQOL-Bref, is a 26-itemquestionnaire with demonstrated reliability and validity (The WHOQOL Group 1998). For thisanalysis, the DIP-DIS was compared with the four domain scores derived from the WHOQOL-Bref: physical health, psychological, social relationships, and environment. The two measures ofsubjective satisfaction (satisfaction with own independence and satisfaction with life) wereconsistently correlated with the four domains of the WHOQOL-Bref. See Table A1.2. Other thanthese two items, only overall socialising, social withdrawal, and sexual relationships showedsignificant correlations with the domain of psychological health on the WHOQOL-Bref (TableA1.2). A summated score of the DIP-DIS was computed, consisting of all items but excluding
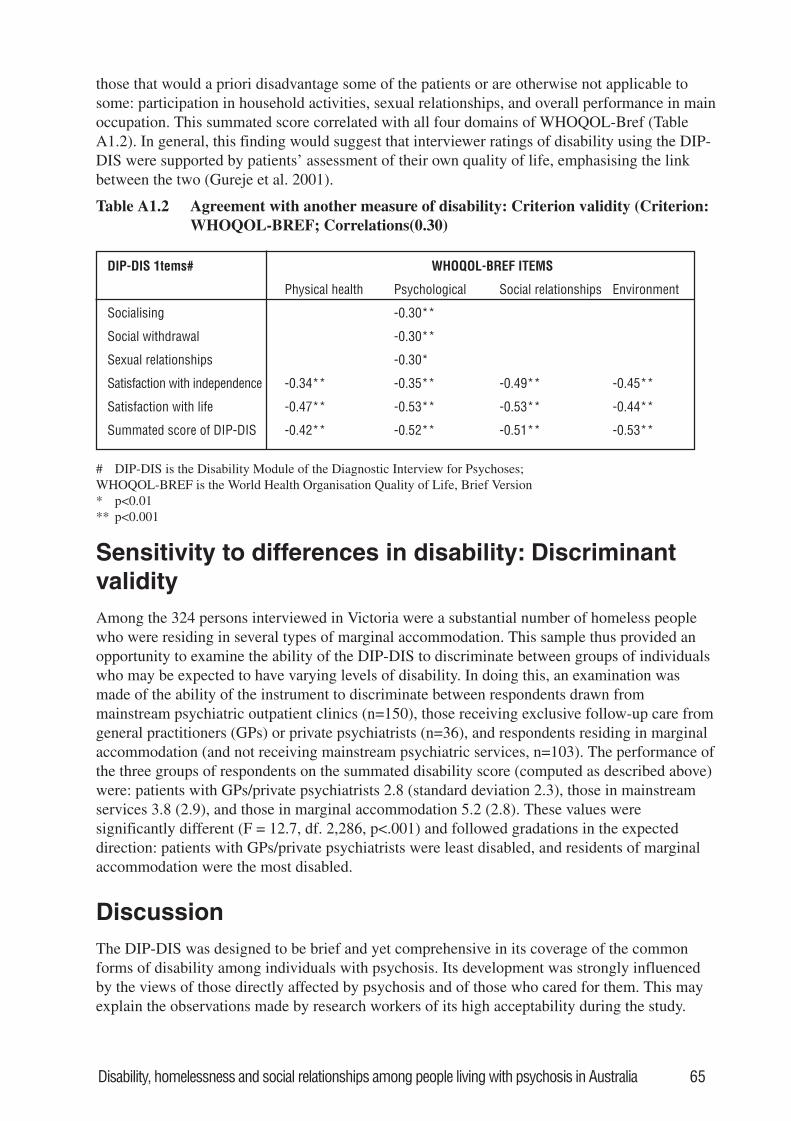
Disability, homelessness and social relationships among people living with psychosis in Australia 65
those that would a priori disadvantage some of the patients or are otherwise not applicable tosome: participation in household activities, sexual relationships, and overall performance in mainoccupation. This summated score correlated with all four domains of WHOQOL-Bref (TableA1.2). In general, this finding would suggest that interviewer ratings of disability using the DIP-DIS were supported by patients’ assessment of their own quality of life, emphasising the linkbetween the two (Gureje et al. 2001).
Table A1.2 Agreement with another measure of disability: Criterion validity (Criterion:WHOQOL-BREF; Correlations(0.30)
DIP-DIS 1tems# WHOQOL-BREF ITEMS
Physical health Psychological Social relationships Environment
Socialising -0.30**
Social withdrawal -0.30**
Sexual relationships -0.30*
Satisfaction with independence -0.34** -0.35** -0.49** -0.45**
Satisfaction with life -0.47** -0.53** -0.53** -0.44**
Summated score of DIP-DIS -0.42** -0.52** -0.51** -0.53**
# DIP-DIS is the Disability Module of the Diagnostic Interview for Psychoses;WHOQOL-BREF is the World Health Organisation Quality of Life, Brief Version* p<0.01** p<0.001
Sensitivity to differences in disability: DiscriminantvalidityAmong the 324 persons interviewed in Victoria were a substantial number of homeless peoplewho were residing in several types of marginal accommodation. This sample thus provided anopportunity to examine the ability of the DIP-DIS to discriminate between groups of individualswho may be expected to have varying levels of disability. In doing this, an examination wasmade of the ability of the instrument to discriminate between respondents drawn frommainstream psychiatric outpatient clinics (n=150), those receiving exclusive follow-up care fromgeneral practitioners (GPs) or private psychiatrists (n=36), and respondents residing in marginalaccommodation (and not receiving mainstream psychiatric services, n=103). The performance ofthe three groups of respondents on the summated disability score (computed as described above)were: patients with GPs/private psychiatrists 2.8 (standard deviation 2.3), those in mainstreamservices 3.8 (2.9), and those in marginal accommodation 5.2 (2.8). These values weresignificantly different (F = 12.7, df. 2,286, p<.001) and followed gradations in the expecteddirection: patients with GPs/private psychiatrists were least disabled, and residents of marginalaccommodation were the most disabled.
DiscussionThe DIP-DIS was designed to be brief and yet comprehensive in its coverage of the commonforms of disability among individuals with psychosis. Its development was strongly influencedby the views of those directly affected by psychosis and of those who cared for them. This mayexplain the observations made by research workers of its high acceptability during the study.
66 Disability, homelessness and social relationships among people living with psychosis in Australia
The result of the inter-rater exercise, while encouraging, shows that items relating to sexual andintimate relationships may be too personal to rate reliably among respondents with experience ofpsychosis.
In the assessment of the relationship of the DIP-DIS to an independent measure of quality of life,it was revealing that the items that most strongly correlated with the four domains of theWHOQOL-Bref were those dealing with respondents’ subjective assessment of satisfaction withown independence and with life. These observations suggest that while the concept of quality oflife is integral to that of disability, the latter is nevertheless broader than the former. The resultsof the discriminant analysis provided an indication that the DIP-DIS is sensitive to differences inthe levels of disability. However, future studies should provide a more direct assessment of itssensitivity to change.
Overall, the DIP-DIS seems an appropriate and valid measure of disability among persons withthe experience of psychosis. Its rating of disability may however be improved and enriched bysupplementary longitudinal assessment of functioning together with information supplied by keyinformants and observational assessments of functioning.
Disability, homelessness and social relationships among people living with psychosis in Australia 67
Appendix 2: Details of the methodologyof the systematic case study inMelbourne
InstrumentsThe screening protocol was developed for the national LPD study (Jablensky et al. 2000). ThePsychosis Screen (PS), includes a set of five questions about specific psychotic symptoms(current or at any time in the past) and a sixth question asking whether a doctor had ever told theperson he/she may have schizophrenia, schizo-affective disorder or bipolar disorder (manicdepression). It also has an item recording the clinical judgement of the key worker administeringthe PS (where applicable; or the trained clinician conducting the screen as in this nested study) asto whether, on the basis of all information available, psychotic symptoms were present. Scoringtwo or more items as positive was selected as the criterion for a positive screen after pilot testingthe instrument before the national survey (Jablensky et al. 1999b). With sensitivity andspecificity at 0.67 and 0.84, respectively, the positive predictive value of the screen was 0.70 andthe negative predictive value 0.80. The clinicians administering the screen were instructed toscore the screen positive rather than negative in cases of doubt, and doubtful instances werereviewed with the fieldwork supervisor and trainer [Helen Evert (HE) and Oye Gureje (OG) inthe nested study reported here].
Compiling the sampling frame for marginalaccommodationA list of all marginal facilities in the catchment area was compiled from various sources. Thestate government Department of Housing, local councils, non-government community andreligious agencies and other researchers (Bryan Speed, Project Epidemiologist, InfectiousDiseases Physician, Austin & Repatriation Medical Centre, who conducted a study into theprevalence of TB among people living in rooming houses; Source: Reid et al. 1998) all assisted.Information was collected about the number of rooms, the ‘turn over’ of residents, and staffingand support in each facility identified. The original list of appropriate houses and establishments(‘houses’) obtained from these sources was amended to exclude houses with insufficient contactdetails or bed numbers. This list was further reduced when interviewers contacted houses anddiscovered that they were no longer in existence, or had been converted into apartments orstudent accommodation (32 houses in Yarra, 38 houses in Boroondara).
In preparation for the study, HE contacted a number of key non-government agencies. Theseincluded Yarra Community Housing Co-operative (300 residents living in 21 properties), Fitzroy,Richmond and Collingwood Accommodation Service, the Inner Urban Regional HousingCouncil, The Rooming House Tenant’s Association, The Royal District Nursing Service (RDNS)Homeless Persons Program, Bedford Street Outreach service, and Hawthorn Project run by theSalvation Army. Religious organisations also have a number of properties that provide long-termand short-term accommodation, and The Catholic Homeless Network provided a forum forCatholic welfare agencies to discuss common issues. The Mental Health Issues Group is anotherimportant forum where key non-government agencies discuss issues and concerns about mentalhealth services. HE discussed the study and methodology with both of these groups.
68 Disability, homelessness and social relationships among people living with psychosis in Australia
A number of the organisations were concerned about privacy for tenants and specifically aboutthe possibility of information about people’s mental health being available to the manager orproprietor of the rooming house. Meetings were held to assure various groups that the censuswould be conducted in a sensitive manner. A focus group was convened through consumerconsultants from the Victorian Mental Illness Awareness Council (VMIAC) who invited peopleliving in rooming houses to discuss their views on the best ways to conduct the study. Fivepeople attended the session, and unanimously expressed a strong view that screening beconducted by direct contact between interviewers and residents. Confidentiality, privacy andinformation were critical considerations for residents. People felt it was important to informoccupants about the study in advance, giving them the option of not participating in the census,and that this could be accomplished by approaching residents directly to conduct the screen.
The interviewers promoted the study to proprietors and residents through working closely withthe non-government agencies and St. Vincent’s Mental Health Service (SVMHS), specifically theoutreach service to homeless people. Residents were informed about the study in a number ofways: articles in the local newspaper, posters on rooming houses’ notice boards and individualleaflets under people’s doors. Each resident in Yarra Community Housing received a letter fromthe manager describing and endorsing the study.
A number of meetings were held between the interviewers and staff from SVMHS, the RoyalDistrict Nursing Service and the Yarra Community Housing Group to advise the interviewersabout safety issues. Interviewers went into the houses in pairs, with a mobile phone, and theiritineraries were logged and monitored.
Rationale for number of residents approached forscreeningWe had the resources to locate and conduct the in-depth interviews with up to 90 residents whowere screened as positive. The pilot data on the screening instrument suggested a positivepredictive value of 70% for current psychotic disorder. Based on a presumed prevalence forpsychotic disorder of 30% among homeless people, we calculated that we would need to screenabout 360 people to identify 110 to 120 people with positive screens (of whom we expected 90 toconsent to and attend an interview). Since we expected a sizeable number of residents to declinescreening, a target of 500 residents was used as a basis for obtaining 360 screens.
Ethical proceduresDuring initial approach for screening, all residents were informed about the study andspecifically told that it was a random selection of accommodation settings, they were free not toparticipate, and information collected was confidential and would be used in an aggregate form.They were also informed that they could be asked to participate in a longer interview. Afterindividuals agreed to participate in the latter, they were informed that they would be reimbursedfor their time. All interviewed residents signed a consent form.
Sampling results in marginal accommodationThe final list contained a total of 80 houses or other facilities (‘houses’) with 1355 beds. 37houses with a total of 757 beds were randomly selected and participated in the study. 28 of thesewere in the City of Yarra from a list of 61 houses, and 9 were selected in Boroondara from 19houses. 27 selected houses (with 322 beds) had less than 20 beds, 8 houses (with 272 beds) had
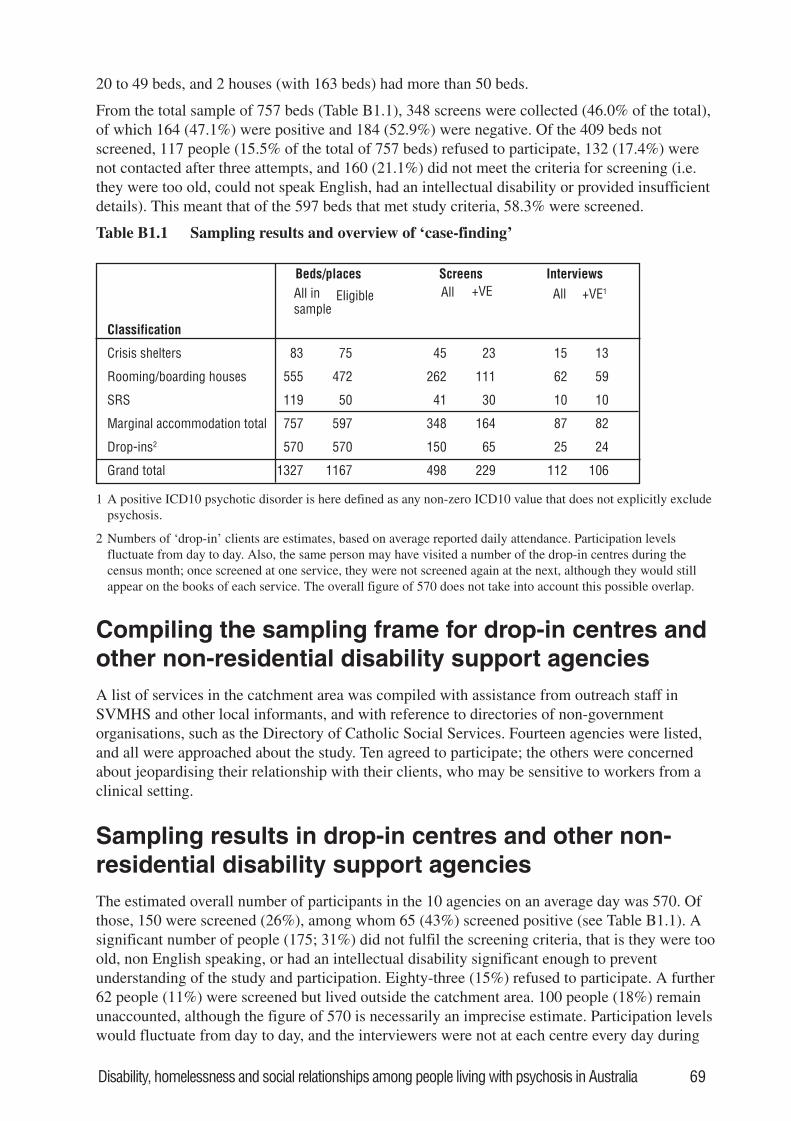
Disability, homelessness and social relationships among people living with psychosis in Australia 69
20 to 49 beds, and 2 houses (with 163 beds) had more than 50 beds.
From the total sample of 757 beds (Table B1.1), 348 screens were collected (46.0% of the total),of which 164 (47.1%) were positive and 184 (52.9%) were negative. Of the 409 beds notscreened, 117 people (15.5% of the total of 757 beds) refused to participate, 132 (17.4%) werenot contacted after three attempts, and 160 (21.1%) did not meet the criteria for screening (i.e.they were too old, could not speak English, had an intellectual disability or provided insufficientdetails). This meant that of the 597 beds that met study criteria, 58.3% were screened.
Table B1.1 Sampling results and overview of ‘case-finding’
Beds/places Screens InterviewsAll insample
Eligible All +VE All +VE1
Classification
Crisis shelters 83 75 45 23 15 13
Rooming/boarding houses 555 472 262 111 62 59
SRS 119 50 41 30 10 10
Marginal accommodation total 757 597 348 164 87 82
Drop-ins2 570 570 150 65 25 24
Grand total 1327 1167 498 229 112 106
1 A positive ICD10 psychotic disorder is here defined as any non-zero ICD10 value that does not explicitly excludepsychosis.
2 Numbers of ‘drop-in’ clients are estimates, based on average reported daily attendance. Participation levelsfluctuate from day to day. Also, the same person may have visited a number of the drop-in centres during thecensus month; once screened at one service, they were not screened again at the next, although they would stillappear on the books of each service. The overall figure of 570 does not take into account this possible overlap.
Compiling the sampling frame for drop-in centres andother non-residential disability support agenciesA list of services in the catchment area was compiled with assistance from outreach staff inSVMHS and other local informants, and with reference to directories of non-governmentorganisations, such as the Directory of Catholic Social Services. Fourteen agencies were listed,and all were approached about the study. Ten agreed to participate; the others were concernedabout jeopardising their relationship with their clients, who may be sensitive to workers from aclinical setting.
Sampling results in drop-in centres and other non-residential disability support agenciesThe estimated overall number of participants in the 10 agencies on an average day was 570. Ofthose, 150 were screened (26%), among whom 65 (43%) screened positive (see Table B1.1). Asignificant number of people (175; 31%) did not fulfil the screening criteria, that is they were tooold, non English speaking, or had an intellectual disability significant enough to preventunderstanding of the study and participation. Eighty-three (15%) refused to participate. A further62 people (11%) were screened but lived outside the catchment area. 100 people (18%) remainunaccounted, although the figure of 570 is necessarily an imprecise estimate. Participation levelswould fluctuate from day to day, and the interviewers were not at each centre every day during
70 Disability, homelessness and social relationships among people living with psychosis in Australia
the study period of one month. In addition, the same person may have visited a number of thedrop-in centres; once screened at one service, they were not screened again at the next. Theoverall estimate of 570 did not take into account this possible overlap in attendance acrossagencies by the same individuals. If an individual screened at a drop-in centre reported living inone of the houses selected for screening in the study we transferred the screen to the marginalaccommodation category.
Disability, homelessness and social relationships among people living with psychosis in Australia 71
References
Adhikari P, Sumerill A 2000, 1998 National Drug Strategy Household Survey Detailed Findings.Canberra: Australian Institute of Health and Welfare (Drug Statistic Series).
Albert M, Becker T, McCrone P, Thornicroft G 1998, Social networks and mental health serviceutilisation - a literature review. International Journal of Social Psychiatry; 44:248-266.
Andrews G, Peters L, Teesson M 1994, Measurement of consumer outcome in mental health: Areport to the National Mental Health Information Strategy Committee. Sydney: Clinical ResearchUnit for Anxiety Disorders.
Anthony WA 1993, Recovery from mental illness: The guiding vision of the mental healthservice system in the 1990s. Psychosocial Rehabilitation Journal; 16:11-23.
Anthony WA, Cohen MR, Farkas MD 1990, Psychiatric Rehabilitation. Boston: BostonUniversity, Center for Psychiatric Rehabilitation.
Arce AA, Vergare MJ 1984, Identifying and characterizing the mentally ill among the homeless.In: Lamb HR, ed. The Homeless Mentally Ill: A Task Force Report of the American PsychiatricAssociation. Washington: American Psychiatric Association: 75-89.
Bachrach LL 1995, “Boundary Busting” and the mentally ill homeless population. PsychiatricServices; 46:875-889.
Baum AS, Burnes DW 1993, A Nation in Denial: The Truth About Homelessness. Boulder:Westview Press.
Becker T, Leese M, Clarkson P, Taylor RE, Turner D, Kleckham J, Thornicroft G 1998, Linksbetween social networks and quality of life: an epidemiologically representive study of psychoticpatients in South London. Social Psychiatry and Psychiatric Epidemiology; 33:299-304.
Bellack AS 1997, Social Skills Deficits and Social Skills Training: New Developments andTrends. In: Brenner HD, Böker W, Genner R, eds. Towards a Comprehensive Therapy forSchizophrenia. Seattle: Hogrefe & Huber Publishers.
Brown C 1996, A comparison of living situation and loneliness for people with mental illness.Psychiatric Rehabilitation Journal; 20:59-63.
Brown GW, Birley JLT, Wing JK 1972, Influence of family life on the course of schizophrenicdisorders: a replication. British Journal of Psychiatry; 121:241-258.
Brugha TS, Wing JK, Smith BL 1989, Physical health of the long-term mentally ill in thecommunity. Is there unmet need? British Journal of Psychiatry; 155:777-781.
Buchanan J 1995, Social support and schizophrenia: A review of the literature. Archives ofPsychiatric Nursing; 9:68-76.
Buhrich N, Teesson M 1996, Impact of a psychiatric outreach service for homeless persons withschizophrenia. Psychiatric Services; 47:644-646.
Burdekin B, Guilfoyle M, Hall D 1993, Human Rights & Mental Illness : Report of the NationalInquiry into the Human Rights of People with Mental Illness. Canberra: Australian GovernmentPublishing Service.
Carpenter WT, Strauss JS 1991, The prediction of outcome in schizophrenia IV: Eleven-yearfollow-up of the Washington IPSS cohort. The Journal of Nervous and Mental Disease; 179:517-525.
72 Disability, homelessness and social relationships among people living with psychosis in Australia
Carr V, Halpin S 2002 (on behalf of the Low Prevalence Disorders Study Group), Stigma anddiscrimination. National Survey of Mental Health and Wellbeing, Bulletin 6.
Carr V, Neil A, Halpin S, Holmes S 2002 (on behalf of the Low Prevalence Disorders StudyGroup), Costs of psychosis in urban Australia. National Survey of Mental Health and Wellbeing,Bulletin 2.
Caton CL 1990, Solutions to the homeless problems. In: Caton CL, ed. Homeless in America.Oxford: Oxford University Press: 174-190.
Caton CLM, Shrout PE, Eagle PF, Opler LA, Felix A, Dominguez B 1994, Risk factors forhomelessness among Schizophrenic Men: A Case-Control Study. American Journal of PublicHealth; 84:265-270.
Chamberlain C 1999, Counting the Homeless: Implications for Policy Development 1996.Canberra: Australian Bureau of Statistics.
Chamberlain C, Mackenzie D 1998, Youth Homelessness: Early Intervention & Prevention.Sydney: Australian Centre for Equity through Education.
Cochran WG 1977, Sampling Techniques. New York: Wiley.
Cohen C, Ramirez M, Teresi J, Gallagher M, Sokolovsky J 1997, Predictors of becomingredomiciled among older homeless women. The Gerontologist; 37:67-74.
Craig TKJ, Timms PW 1995, Homelessness and schizophrenia. In: Hirsch S, Weinberger D, eds.Schizophrenia. Oxford: Blackwell Science: 664-684.
Daly G 1996, Homeless: Policies, strategies, and lives on the street. London: Routledge.
Davidson L, Haglund KE, Stayner DA, Rakfeldt J, Chinman MJ, Tebes JK 2001, “It was justrealizing...that life isn’t one big horror”: A Qualitative Study of Supported Socialization.Psychiatric Rehabilitation Journal; 24:275-291.
Davidson L, Hoge M, Godleski L, Rakfeldt J, Griffith E 1996, Hospital or community living?Examining consumer perspectives on deinstitutionalisation. Psychiatric Rehabilitation Journal;19:49-58.
Davidson L, Stayner D 1997, Loss, Loneliness, and the Desire for Love: Perspectives on theSocial Lives of People with Schizophrenia. Psychiatric Rehabilitation Journal; 20:3-12.
Davidson L, Stayner D, Haglund KE 1998, Phenomenological perspective on the socialfunctioning of people with schizophrenia. In: Mueser KT, Tarrier N, eds. Handbook of socialfunctioning in schizophrenia. Boston: Allyn and Bacon: 97-120.
Davidson L, Strauss JS 1992, Sense of self in recovery from severe mental illness. BritishJournal of Psychiatry; 65:131-145.
Deegan P 1996, Recovery as a journey of the heart. Psychiatric Rehabilitation Journal; 19:91-97.
Deegan PE 1988, Recovery: The lived experience of rehabilitation. Psychosocial RehabilitationJournal; 11:11-19.
de Sisto MJ, Harding CM, McCormick RV, Ashikaga T, Brooks GW 1995, The Maine andVermont three-decade studies of serious mental illness. British Journal of Psychiatry; 167:331-342.
Dickerson FB, Ringel N, Parente F 1999, Predictors of Residential Independence AmongOutpatients With Schizophrenia. Psychiatric Services; 50:515-519.
Disability, homelessness and social relationships among people living with psychosis in Australia 73
Doutney CP, Buhrich N, Virgona A, Cohen A, Daniels P 1985, The prevalence of schizophreniain a refuge for homeless men. Australian and New Zealand Journal of Psychiatry; 19:233-238.
Edwards J, Maude D, McGorry PD, Harrigan S, Cocks JP 1998, Prolonged recovery in first-episode psychosis. British Journal of Psychiatry; 172:107-116.
EPPIC 2001, Case management in early psychosis: a handbook. Melbourne: EPPIC.
Erickson DH, Beiser M, Iacono W 1998, Social support predicts 5 year outcome in first-episodeSchizophrenia. Journal of Abnormal Psychology; 107:681-685.
Fossey E, Harvey CA 2001, A conceptual review of functioning: Implications for thedevelopment of consumer outcome measures. Australian and New Zealand Journal ofPsychiatry; 35:91-98.
Frost B, Carr V, Halpin S 2002 (on behalf of the Low Prevalence Disorders Study Group),Employment and Psychosis. National Survey of Mental Health and Wellbeing, Bulletin 3.
Geddes J, Newton R, Young G, Bailey S, Freeman C, Priest R 1994, Comparison of prevalenceof schizophrenia among residents of hostels for homeless people in 1966 and 1992. BritishMedical Journal; 308:816-819.
Gureje O, Herrman H, Harvey C, Trauer T, Jablensky A 2001, Defining disability in psychosis:performance of the diagnostic interview for psychoses-disability module (DIP-DIS) in theAustralian National Survey of Psychotic Disorders. Australian and New Zealand Journal ofPsychiatry; 35:846-851.
Hamid WA, Wykes T, Stansfield S 1995a, The social disablement of men in hostels for homelesspeople; I. reliability and prevalence. British Journal of Psychiatry; 166:806-808.
Hamid WA, Wykes T, Stansfield S 1995b, The social disablement of men in hostels for homelesspeople; II. A comparison of patients from long-stay wards. British Journal of Psychiatry;166:806-808.
Hammer M, Makiesky-Barrow, Gutwirth L 1978, Social networks and schizophrenia.Schizophrenia Bulletin; 4:522-545.
Harding C, Keller A 1998, Long-term outcome of social functioning. In: Mueser, Tarrier, eds.Handbook of Social Functioning in Schizophrenia. Boston: Allyn & Bacon: 134-148.
Harding CM, Brooks GW, Ashikaga T, Strauss JS, Breier A 1987, The Vermont longitudinalstudy of persons with severe mental illness, II: Long-term outcome of subjects whoretrospectively met DSM-III criteria for schizophrenia. American Journal of Psychiatry;144:727-735.
Harding CM, Zubin J, Strauss JS 1992, Chronicity in Schizophrenia: Revisited. British Journalof Psychiatry; 161:27-37.
Henderson AS 1988, An Introduction to Social Psychiatry. Oxford: Oxford University Press.
Henry AD, Coster WJ 1996, Predictors of Functional Outcome Among Adolescents and YoungAdults With Psychotic Disorders. The American Journal of Occupational Therapy; 50:171-181.
Herrman H, McGorry P, Bennett P, van Riel R, Singh B 1989, Prevalence of severe mentaldisorders in disaffiliated and homeless people in inner Melbourne. American Journal ofPsychiatry; 146:1179-1184.
Herrman H, McGorry P, Bennett P, Varnavides K, Singh B 1992, Use of services by homelessand disaffiliated individuals with severe mental disorders: A study in Melbourne. In: Cooper B,Eastwood R, eds. Primary Health Care & Psychiatric Epidemiology: 142-159.
74 Disability, homelessness and social relationships among people living with psychosis in Australia
Herrman HE 1996, Hard times for homeless people. Medical Journal of Australia; 165:629.
Higgins K, Cooper-Stanbury M, Williams P 2000, Statistics on Drug Use in Australia 1998.Canberra: Australian Institute of Health and Welfare (Drug Statistic Series).
Hodder T, Teeson M, Buhrich N 1998, Down and Out in Sydney, Prevalence of mental disorders,disability and health service use among homeless people in inner Sydney. Sydney: ResearchGroup in Mental Health and Homelessness: Sydney City Mission.
Hogg LI, Marshall M 1992, Can we measure need in the homeless mentally ill? Using the MRCneeds for care assessment in hostels for the homeless. Psychological Medicine; 22:1027-1034.
Jablensky A 2000a, Course and outcome of schizophrenia and their prediction. In: Gelder MG,Lopez-Ibor J, Andreasen NC, eds. New Oxford Textbook of Psychiatry. Oxford: OxfordUniversity Press: 612-621.
Jablensky A 2000b, Epidemiology of schizophrenia. In: Gelder MG, Lopez-Ibor J, AndreasenNC, eds. New Oxford Textbook of Psychiatry. Oxford: Oxford University Press: 585-599..
Jablensky A, McGrath J, Herrman H, Castle D, Gureje O, Evans M, Carr V, Morgan V, Korten A,Harvey C 2000, Psychotic disorders in urban areas: an overview of the Study on Low PrevalenceDisorders. Australian and New Zealand Journal of Psychiatry; 34:221-236.
Jablensky A, McGrath J, Herrman H, Castle D, Gureje O, Morgan V, Korten A 1999a (on behalfof the study group), People Living with Psychotic Illness: An Australian Study 1997-98. AnOverview (National Survey of Mental Health and Wellbeing - Bulletin 1). Canberra: AustralianMental Health Branch, Commonwealth Department of Health and Aged Care.
Jablensky A, McGrath J, Herrman H, Castle D, Gureje O, Morgan V, Korten A 1999b (on behalfof the study group), People Living with Psychotic Illness: An Australian Study 1997-98.(National Survey of Mental Health and Wellbeing - Report 4). Canberra: Australian MentalHealth Branch, Commonwealth Department of Health and Aged Care.
Jenkins R 1998, Linking epidemiology and disability measurement with mental health servicepolicy and planning. Epidemiologia E Psichiatria Sociale; 7:120-126.
Kaiser W, Priebe S, Barr W, Hoffmann K, Isermann M, Roder-Wanner U, Huxley P 1997,Profiles of subjective quality of life in schizophrenic in- and outpatient samples. Psychiatry;66:153-166.
Kendler KS, McGuire M, Gurneberg AM, Walsh D 1995, Examining the validity of DSM-III-Rschizoaffective disorder and its putative subtypes in the Roscommon family study. AmericanJournal of Psychiatry; 152:755-764.
Kovess V, Lazarus CM 1999, The prevalence of psychiatric disorders and use of care byhomeless people in Paris. Social Psychiatry & Psychiatric Epidemiology; 34:580-587.
Leete E 1989, How I perceive and manage my illness. Schizophrenia Bulletin; 15:197-200.
Leff JP 1993, The TAPS Project: evaluating community placement of long-stay psychiatricpatients. British Journal of Psychiatry; 162:1-56.
Lehman AF 1983, The well-being of chronic mental patients. Archives of General Psychiatry;40:369-373.
Lehman AF 1996, Measures of quality of life among persons with severe and persistent mentaldisorders. Social Psychiatry and Psychiatric Epidemiology; 31:78-88.
Disability, homelessness and social relationships among people living with psychosis in Australia 75
Lehman AF, Steinwachs DM, Dixon LB, Goldman HH, Osher F, Postrado L, Scott JE,Thompson JW, Fahey M, Fischer P, Kasper JA, Lyles A, Skinner EA, Buchanan R, CarpenterWT, Jr., Levine J, McGlynn EA, Rosenheck R, Zito J 1998, Translating research into practice:The Schizophrenia Patient Outcomes Research Team (PORT) Treatment Recommendations.Schizophrenia Bulletin; 24:1-10.
Lesage AD, Mignolli G, Faccincani C, Tansella M 1991, Standardized assessment of the needsfor care in a cohort of patients with schizophrenic psychoses. Psychological Medicine;Monograph supplement 19:27-33.
Lieberman JA, Jody D, Geisler S, Alfir J, Loebel A, Szymanski S, Woerner M, Borenstein M1993, Time course and biological correlates of treatment response in first episode schizophrenia.Archives of General Psychiatry; 50.
Lipton FR, Cohen C, Fischer E, Katz S 1981, Schizophrenia: A network crisis. SchizophreniaBulletin; 7:144-151.
Lipton FR, Sabatini A 1984, Constructing Support Systems for Homeless Chronic Patients. In:Lamb HR, ed. The Homeless Mentally Ill: A Task Force Report of the American PsychiatricAssociation. Washington: American Psychiatric Association.
Lipton FR, Siegel C, Hannigan A, Samuels J, Baker S 2000, Tenure in supportive housing forhomeless persons with severe mental illness. Psychiatric Services; 51:479-486.
Lukoff D, Snyder K, Ventura J, Nuechterlein KH 1984, Life events, familial stress, and coping inthe developmental course of schizophrenia. Schizophrenia Bulletin; 10:258-292.
Marsden D, Duff E 1975, Workless: some unemployed men and their families. Baltimore:Penguin.
Marshall M 1996, Evaluating services for homeless people with mental disorders: Theoreticaland practical issues. In: Bhugra D, ed. Homelessness and mental health. Studies in social andcommunity psychiatry. Cambridge, England UK: Cambridge University Press: 280-296.
McGlashan TH 1988, A selective review of recent North American long-term followup studies ofschizophrenia. Schizophrenia Bulletin; 14:515-542.
McLaughlin-Gray J 2001, Discussion of the ICIDH-2 in relation to occupational therapy andoccupational science. Scandinavian Journal of Occupational Therapy; 8:19-30.
Mojtabai R, Nicholson RA, Carpenter BN 1998, Role of psychosocial treatments in managementof schizophrenia: A meta-analytic review of controlled outcome studies. Schizophrenia Bulletin;24:569-587.
Morgan V, Castle D, Jablensky A 2002 (on behalf of the Low Prevalence Disorders StudyGroup), The use of psychopharmacological and other treatments by persons with psychosis: Self-reported data from the National Study of Low Prevalence (Psychotic) Disorders. National Surveyof Mental Health and Wellbeing, Bulletin 4.
Mortensen PB, Juel K 1993, Mortality and causes of death in first admitted schizophrenicpatients. British Journal of Psychiatry; 163:183-189.
Mueser KT, Bond GR, Drake RE, Resnick SG 1998, Models of community care for severemental illness: A review of research on case management. Schizophrenia Bulletin; 24:37-74.
Mueser KT, Salyers MP, Mueser PR 2001, A prospective analysis of work in schizophrenia.Schizophrenia Bulletin; 27:281-296.
Murray CJL, Lopez AD 1997, Regional patterns of disability-free life expectancy and disability-adjustetd life expectancy: global burden of disease study. The Lancet; 349:1347-1352.
76 Disability, homelessness and social relationships among people living with psychosis in Australia
Newman S, Bland RC 1991, Mortality in a cohort of patients with schizophrenia: A recordlinkage study. Canadian Journal of Psychiatry; 36:239-245.
Odell SM, Commander MJ 2000, Risk factors for homelessness among people with psychoticdisorders. Social Psychiatry and Psychiatric Epidemiology; 35:396-401.
Oliver JP, Huxley PJ, Priebe S, Kaiser W 1997, Measuring the quality of life of severely mentallyill people using the Lancashire Quality of Life Profile. Social Psychiatry and PsychiatricEpidemiology; 32:76-83.
Orley J, Saxena S, Herrman H 1998, Quality of life and mental illness. Reflections from theperspective of the WHOQOL. British Journal of Psychiatry; 172:291-293.
Owen C, Rutherford V, Jones M, Wright C, Tennant C, Smallman A 1996, HousingAccommodation Preferences of People With Psychiatric Disabilities. Psychiatric Services;47:628-632.
Reid G, Speed B, Miller P, Cooke F, Crofts N 1998, A methodology for sampling and accessinghomeless individuals in Melbourne, 1995-96. Australian and New Zealand Journal of PublicHealth; 22:568-572.
Rickards LD, Leginski W, Randolph FL, Oakley D, Herrell JM, Gallagher C 1999, Cooperativeagreements for CMHS/CSAT collaborative program to prevent homelessness: an overview.Alcoholism Treatment Quarterly; 17:1-15.
Salokangas RKR 1997, Living situation, social network and out come in schizophrenia: a five-year prospective follow-up study. Acta Psychiatrica Scandinavica; 96:459-486.
Sarason IG, Sarason BR, Brock DM, Pierce GR 1996, Social Support: Current Status, CurrentIssues. In: Spielberger CD, Sarason IG, Brebner JMT, Greenglass E, Laungani P, O’Roark AM,eds. Stress and Emotion: Anxiety, Anger, and Curiosity. Washington: Taylor & Francis.
Scott J 1993, Homelessness and mental illness. British Journal of Psychiatry; 162:314-324.
Singh BS 1992, Mainstreaming psychiatric services. The Medical Journal of Australia; 156:373-374.
Strauss JS, Carpenter WT 1977, Prediction of outcome in schizophrenia III: Five-year outcomeand its predictors. Archives of General Psychiatry; 34:159-163.
Sullivan G, Burnam A, Koegel P 2000, Pathways to homelessness among the mentally ill. SocialPsychiatry and Psychiatric Epidemiology; 35:444-450.
Teesson M, Hodder T, Buhrich 2000, Substance use disorders among homeless people in innerSydney. Social Psychiatry and Psychiatric Epidemiology; 35:451-456.
The WHOQOL Group 1998, Development of the World Health Organization WHOQOL-Brefquality of life assessment. Psychological Medicine; 28:551-558.
Thoits PA 1995, Stress, coping, and social support processes: Where are we? What Next?Journal of Health and Social Behavior (Extra Issue): 53-79.
Thomas KL, McCormack C 1999, Adequate housing for people with a serious mental illness:Policy obstacles and practice solutions. Australasian Psychiatry; 7:81-84.
Thornicroft G, Bebbington P 1989, Deinstitutionalisation - from hospital closure to servicedevelopment. British Journal of Psychiatry; 155:739-753.
Tucker MB 1982, Social support and coping: applications for the study of female drug abuse.Journal of Social Issues; 38:117-137.

Disability, homelessness and social relationships among people living with psychosis in Australia 77
Vaughn CE, Leff JP 1976, The influence of family and social factors on the course of psychiatricillness. British Journal of Psychiatry; 129:125-137.
Victorian Homelessness Strategy Ministerial Advisory Committee 2001, Building Solutions forIndividuals and Families Who Experience Homelessness - Working Report of the VictorianHomelessness Strategy. Melbourne: Victorian Government Department of Human Services.
Warner R 1999, Schizopohrenia and the environment: Speculative interventions. EpidemiologiaE Psichiatria Sociale; 8:19-34.
Weissman MM 1975, The assessment of social adjustment: a review of techniques. Archives ofGeneral Psychiatry; 32:357-365.
Weissman MM, Shalomskas D, John K 1981, The assessment of social adjustment: an update.Archives of General Psychiatry; 38:1250-1258.
Wing JK, Brown GW 1970, Institutionalism and schizophrenia: A comparative study of threemental hospitals 1960-1968. London: Cambridge University Press.
World Health Organisation 1988, WHO Psychiatric Disability Assessment Schedule (WHO/DAS). Geneva: World Health Organisation.
World Health Organisation 1999, International Classification of Functioning and Disability Beta-2 Draft Short Version July 1999. Geneva: World Health Organisation.
World Health Organisation 2001, International Classification of Functioning, Disability andHealth. Geneva: World Health Organisation.
Young SL, Ensing DS 1999, Exploring Recovery from the Perspective of People with PsychiatricDisabilities. Psychiatric Rehabilitation Journal; 22:219-231.