dimitrios farmakiotis, md1,2 , alyssa r. letourneau, md
TRANSCRIPT
Limitations of our study are stratification of infection control
practices by institution, retrospective data collection, and the fact
that it was conducted at two hospitals in the same healthcare
network, potentially limiting the generalizability of our results.
Antibiotic prophylaxis after LVAD implantation was associated with
increased rates of antibacterial resistance without decreased rates
of infectious complications.
As we gain more knowledge regarding the effects of antibiotic
administration on cutaneous microbiota, sampling of the driveline
exit site to analyze its microbiome could help elucidate the
complex microbial dynamics of LVAD-associated infections.
Prospective studies of LVAD-infections, using standardized
definitions to analyze patient-level clinical and microbiologic data
are needed.
Dimitrios Farmakiotis, MD1,2 , Alyssa R. Letourneau, MD, MPH3, Alicia Galar, Pharm D, PhD1,
Sophia Koo, MD1, James H. Maguire, MD1, Michael M. Givertz, MD4, Lindsey R. Baden, MD1
Patients and Methods
Printed by
We retrospectively studied patients with continuous flow-LVADs placed at Brigham and Women’s Hospital (BWH) and Massachusetts General Hospital (MGH), between 1/1/2007 and 11/30/2014.
We compared two different strategies after implantation, with sterile dressings and: (1) topical care alone: chlorhexidine skin cleanser (BWH), or (2) antimicrobial prophylaxis: oral doxycycline with topical polymyxin-trimethoprim drops (MGH). We assessed LVAD-specific or related infection rates, according to the ISHLT criteria, identified factors associated with LVAD-infections, and analyzed pathogen susceptibilities during first episodes of infection.
A new “episode” of LVAD-infection was defined as an infection event prompting modification of management, such as change of antibiotic regimen or hospital admission, if they were caused by a different organism, or by the same organism, but with evidence of clinical resolution of the initial episode, at least 30 days apart and, for bacteremia, with documented negative blood cultures in between.
Conclusions and Limitations
• We studied 191 patients. More patients in the prophylaxis
group received an LVAD as bridge to transplant (p=0.01) and
had a HeartWare HVAD device (p<0.01).
• Independent predictors of LVAD-infection included male sex
(Rate ratio [RR] 1.8, p=0.04; sub-distribution hazard ratio
[sHR, after adjustment for death or transplant as competing
events] 2.8, p=0.02) and diabetes (RR 1.7, p<0.01; sHR 1.9,
p=0.02), but not antibiotic prophylaxis.
• While there were no inter-institutional differences in
antibiogram susceptibility rates of Staphylococci to
tetracycline or trimethoprim/sulfamethoxazole, antibiotic
prophylaxis was associated with increased rates of resistance
to both agents (p<0.01 and p=0.05, respectively).
• All-cause mortality was not affected by infection or
prophylaxis.
• Among patients with bridge-LVADs, there were no differences
in transplant rates between patients with and without LVAD-
infection, or between those who received antibiotic
prophylaxis and those who did not.
• Infection as a time-varying parameter was associated with
shorter time to transplant in all transplant candidates (HR 1.7,
95% CI 1-2.9, p=0.04), and after exclusion of those who died
before transplant (HR 1.8, 95% CI 1.1-3.1, p=0.02).
In heart failure patients with left ventricular-assist devices (LVADs),
infections cause significant morbidity and frequent hospitalizations.
The marked heterogeneity in methods and results across different
studies of LVAD infections led the International Society for Heart
and Lung Transplantation (ISHLT) to propose uniform definitions
for infections in patients with LVADs.
There are few studies describing the epidemiology, risk factors for
and outcomes of continuous-flow (CF)-LVAD-(associated)
infections, by application of these standardized criteria. Also, the
effects of prolonged antibiotic prophylaxis after LVAD implantation
on the incidence of LVAD-associated infection and antibacterial
resistance have not been adequately described.
• Aims of the present study were to:
1.Describe the spectrum of LVAD-infections and pathogen species
distribution, using the ISHLT definitions, in a contemporary cohort
of patients with CF-LVADs
2.Identify predictors of infection and its impact on clinical outcomes
3.Assess the effects of prolonged antibiotic prophylaxis after
device implantation on LVAD-infection rates, outcomes and
antibacterial resistance.
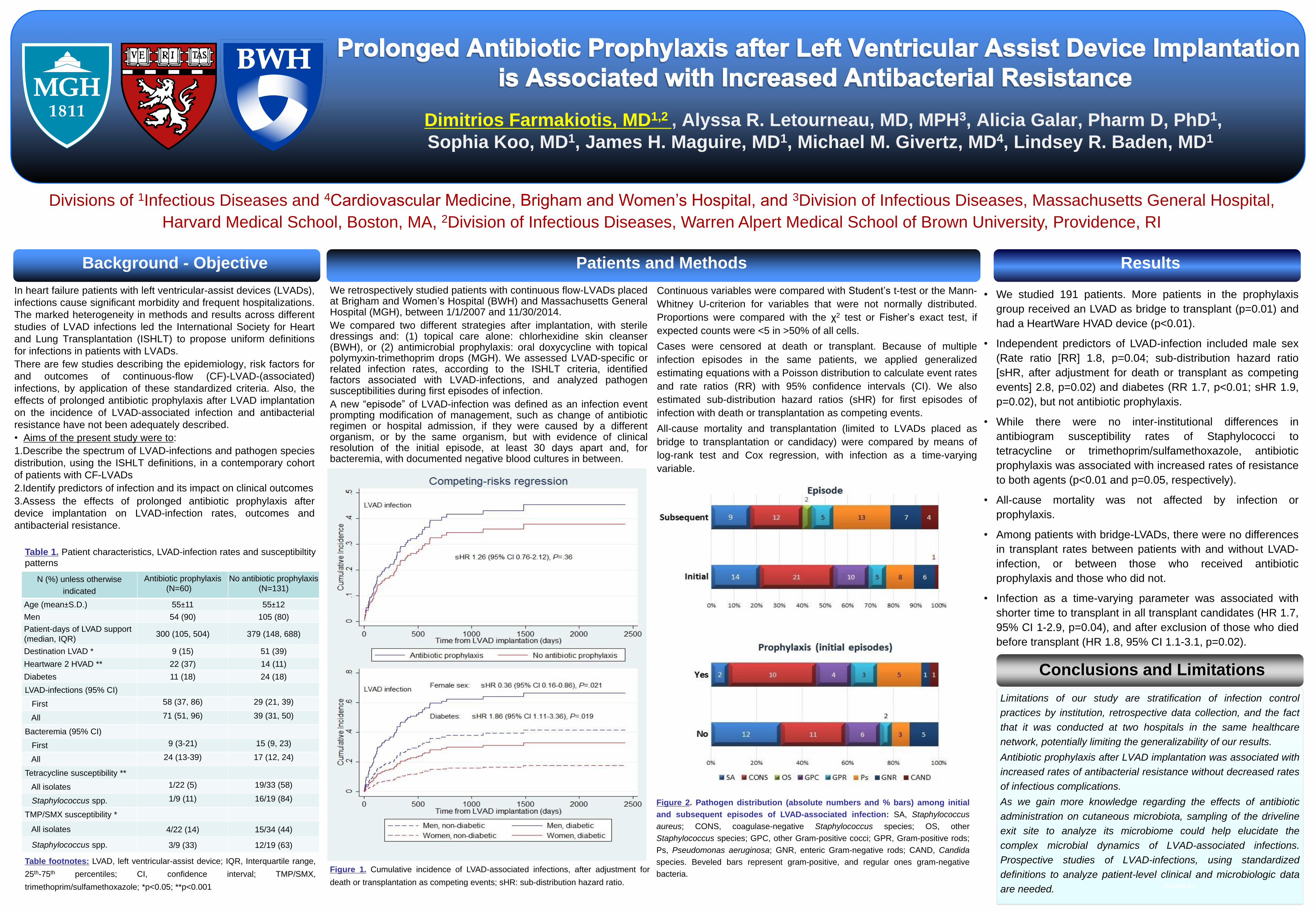
Figure 1. Cumulative incidence of LVAD-associated infections, after adjustment for
death or transplantation as competing events; sHR: sub-distribution hazard ratio.
Divisions of 1Infectious Diseases and 4Cardiovascular Medicine, Brigham and Women’s Hospital, and 3Division of Infectious Diseases, Massachusetts General Hospital,
Harvard Medical School, Boston, MA, 2Division of Infectious Diseases, Warren Alpert Medical School of Brown University, Providence, RI
Continuous variables were compared with Student’s t-test or the Mann-
Whitney U-criterion for variables that were not normally distributed.
Proportions were compared with the χ2 test or Fisher’s exact test, if
expected counts were <5 in >50% of all cells.
Cases were censored at death or transplant. Because of multiple
infection episodes in the same patients, we applied generalized
estimating equations with a Poisson distribution to calculate event rates
and rate ratios (RR) with 95% confidence intervals (CI). We also
estimated sub-distribution hazard ratios (sHR) for first episodes of
infection with death or transplantation as competing events.
All-cause mortality and transplantation (limited to LVADs placed as
bridge to transplantation or candidacy) were compared by means of
log-rank test and Cox regression, with infection as a time-varying
variable.
Figure 2. Pathogen distribution (absolute numbers and % bars) among initial
and subsequent episodes of LVAD-associated infection: SA, Staphylococcus
aureus; CONS, coagulase-negative Staphylococcus species; OS, other
Staphylococcus species; GPC, other Gram-positive cocci; GPR, Gram-positive rods;
Ps, Pseudomonas aeruginosa; GNR, enteric Gram-negative rods; CAND, Candida
species. Beveled bars represent gram-positive, and regular ones gram-negative
bacteria.
Background - Objective Results
N (%) unless otherwise
indicated
Antibiotic prophylaxis
(N=60)
No antibiotic prophylaxis
(N=131)
Age (mean±S.D.) 55±11 55±12
Men 54 (90) 105 (80)
Patient-days of LVAD support
(median, IQR) 300 (105, 504) 379 (148, 688)
Destination LVAD * 9 (15) 51 (39)
Heartware 2 HVAD ** 22 (37) 14 (11)
Diabetes 11 (18) 24 (18)
LVAD-infections (95% CI)
First 58 (37, 86) 29 (21, 39)
All 71 (51, 96) 39 (31, 50)
Bacteremia (95% CI)
First 9 (3-21) 15 (9, 23)
All 24 (13-39) 17 (12, 24)
Tetracycline susceptibility **
All isolates 1/22 (5) 19/33 (58)
Staphylococcus spp. 1/9 (11) 16/19 (84)
TMP/SMX susceptibility *
All isolates 4/22 (14) 15/34 (44)
Staphylococcus spp. 3/9 (33) 12/19 (63)
Table footnotes: LVAD, left ventricular-assist device; IQR, Interquartile range,
25th-75th percentiles; CI, confidence interval; TMP/SMX,
trimethoprim/sulfamethoxazole; *p<0.05; **p<0.001
Table 1. Patient characteristics, LVAD-infection rates and susceptibiltity
patterns