dimensions of affect modulated by perceived mood regulation ability
TRANSCRIPT

Dimensions of Affect Modulated by Perceived Mood RegulationAbility
Christine A. Hovanitz • Adrienne N. Hursh •
Adam D. Hudepohl
Published online: 22 March 2011
� Springer Science+Business Media, LLC 2011
Abstract The ability to regulate mood is a facet of
emotional intelligence that may contribute to an individ-
ual’s physical and mental health. Precisely what is regu-
lated when mood regulation occurs is dependent on what
‘‘makes up’’ mood. The purpose of this study was to
evaluate whether perceived mood regulation ability can
predict regulation of affect during task engagement and
whether affect regulation is specific to valence or arousal.
Measures of positive affect, negative affect, and frontal
area sEMG (as a measure of arousal) were obtained from a
sample of one hundred twenty-four participants catego-
rized by their self report as possessing low or high mood
regulation ability. Modulation of positive affect, but not
negative affect, was predicted by perceived mood regula-
tion ability. The results of sEMG were mixed. These data
provide some support for the hypothesis that mood regu-
lation ability can predict future efforts to regulate affect, at
least in the context of task engagement.
Keywords Mood regulation � Positive affect � Negative
affect � sEMG
Meta-cognition has been defined as ‘‘thoughts about
thoughts’’ (Metcalfe and Shimamura 1994). A special case
of meta-cognition is mood (or affect) meta-cognition,
which involves thoughts about affective experience; when
so considered, the concept is subsumed under the label of
emotional intelligence. The basic formulation is simple.
When affect is a focus of thought, affect may become a
target of regulation attempts. Because a number of psy-
chological and biological disorders have accompanying
issues of affective disturbance, the ability to regulate affect
may be important to a variety of health-related concerns.
Precisely what is regulated when affect regulation is
attempted may be considered in part a function of what
‘‘makes up’’ affect. This question touches on definitional
issues surrounding distinctions and equivalences between
and among the terms emotion, mood, affect, and subjective
state. A variety of theoretical models have been proposed
that identify different features subsumed by these terms
(Ekman and Davidson 1994; Gross 1998; Russell 2009).
Despite variability in particular formulations, substantial
consensus has been achieved about some of the essential
elements of affective structure (Frijda 2006): Valence and
arousal are considered the primary dimensions. In addition,
emotion is differentiated from other affective states as the
former possesses a specific motivational function, a spe-
cific goal object, and tends to have a clearly demarcated
onset and cessation (Gross 1998). There are exceptions:
Brehm et al. (2009) have shown mood to possess certain
motivational qualities, and the biologically-based moods
(Thayer 1989) tend to accompany if not proceed choice to
engage in energetic behavior.
This paper will deal with what Russell defines as core
affect, which is ‘‘that neurophysiological state consciously
accessible as the simplest raw (non-reflective) feelings
evident in moods and emotions’’ (Russell 2003, p. 148).
Russell’s formulation is similar to what Watson and
Tellegen (1985) have called affect, according to Russell
(2003), although the two differ on some other substantive
but testable elements. For the purposes of the present study,
the terms mood and affect will be used interchangeably as
shorthand terms for core affect. Watson et al. (1988) define
negative affect as a general dimension of subjective
C. A. Hovanitz (&) � A. N. Hursh � A. D. Hudepohl
University of Cincinnati, Cincinnati, OH, USA
e-mail: [email protected]
123
Appl Psychophysiol Biofeedback (2011) 36:113–119
DOI 10.1007/s10484-011-9154-1

distress and unpleasurable engagement, while positive
affect refers to distinctive dimensions in which a person
feels enthusiastic, active and alert. Russell (2003, 2009),
like many, consider valence bipolar. Watson and Tellegen
(1999) believe positive valence to be independent of neg-
ative valence, although bipolarity may appear with some
measures and under some circumstances.
Because core affect is by definition nonreflective, self-
report of what ‘‘makes up’’ affect is not possible by the
experiencing individual. The phenomenon is not subject to
self conscious reflection as experienced. One means of
examining components of core affect, however, may be
through multiple assessments of the affective experience of
the individual. What may be considered the elements of
core affect, the fundamental elements of any affective
experience (valence and arousal), may be assessed simply
by evaluating the individual by multiple instruments that
evaluate potential components, such as positive affect,
negative affect, and arousal.
The focus of the current study is the regulation of core
affect. Because the two dimensions of valence and arousal
are considered essential to core affect, affect regulation
may take place with respect to either or both. The ques-
tion is both theoretical and practical in implication;
arousal reduction is targeted in stress-reduction interven-
tions as a goal of many physical health-related psycho-
logical interventions. Improvement in affective valence,
on the other hand, is a goal of therapies targeting mood
disorders. Thus, what is important about affect regulation
ability may depend on the disorder of concern. As little
direct evidence has been obtained to support the idea that
perception of affect regulation ability predicts objectively
measured changes in core affect in a prospective manner,
the intent of this study is to obtain evidence for this
claim. Further, this study will attempt to identify whether
positive or negative affect are similarly modulated. In
addition, an attempt will be made to determine if a
measure of central arousal variability is modulated by
perceived mood regulation.
Method
Participants
Approximately 300 undergraduates completed initial test-
ing in groups ranging in size up to eight. One hundred
twenty-four (66 male, 58 female) agreed to participate in
the second phase and successfully completed the hour-long
experimental protocol conducted approximately one week
later. The second phase included 102 Caucasians, 13
African Americans, and 9 of other ethnicities or who
declined to report ethnicity.
Measures
Self report. The Trait Meta-Mood Scale (TMMS; Salovey
et al. 1995) and the Manifest Anxiety Scale (Taylor 1953)
were administered during an initial screening. The Positive
and Negative Affect Scales (Watson et al. 1988) were
completed during the experimental phase.
The Trait Meta-Mood Scale consists of three subscales,
derived by factor analysis. One subscale, Repair, was
employed in the present study. The Repair score is a sum of
ratings on six items; participants respond to each item on a
5-point scale (1 = strongly agree; 5 = strongly disagree).
Repair was shown to possess good internal consistency and
both convergent and discriminative validity. The items
which make up this scale refer to general beliefs about
habitual thoughts and feelings related to maintaining
optimal mood. The six items that make up the scale are the
following: ‘‘I try to think good thoughts no matter how
badly I feel’’; ‘‘Although I am sometimes sad, I have a
mostly optimistic outlook’’; ‘‘When I am upset I realize
that the ‘good things in life’ are illusions’’ (reverse scored);
‘‘When I become upset I remind myself of all the pleasures
in life.’’; ‘‘Although I am sometimes happy, I have a mostly
pessimistic outlook’’ (reverse scored); and ‘‘No matter how
badly I feel, I try to think about pleasant things)’’. Although
multiple translations and versions of the entire TMMS are
available, and multiple studies have examined the relation
between the subscales of the TMMS and indices of mental
and physical health (Gross and John 2003; Salovey et al.
1995; Thompson et al. 2007), norms or cut-off scores on
the 30-item instrument are not available at this time.
The Manifest Anxiety Scale (MAS) is a 50-item mea-
sure of trait anxiety derived from items present in the
original MMPI. Very widely used, the measure consists of
items that reflect diverse symptoms of anxiety. Included are
cognitive (‘‘I am more sensitive than most other people’’),
behavioral (‘‘I have periods of such great restlessness that I
cannot sit long in a chair’’ and physiological (‘‘I sweat very
easily even on cool days’’) items. Participants respond by
indicating whether an item is true or false as it applies to
them; scores range from 0 to 50. Standard scoring of the
instruments was employed, with the sum of the keyed items
analyzed as a continuous variable. Among university stu-
dents, a median score of 13 was cited in the manuscript
covering the initial construction of the test; this can be
compared to the median of 34 obtained from psychiatric
inpatients. Reasonable psychometric properties are also
reported, given the heterogeneity of the item content. Test
retest reliability over a 4 week period was found to be .88
among nonpsychiatric patients, while Kuder-Richardson
internal consistency estimates have ranged from .78 to .84.
The MAS was included in this study to evaluate the
independence of negative affect from anxiety (Tellegen
114 Appl Psychophysiol Biofeedback (2011) 36:113–119
123

1985), and the independence of arousal from anxiety
(Hazlett et al. 1994; Hoehn-Saric and McLeod 2000).
The Positive and Negative Affect Scales (PANAS) is a
brief questionnaire consisting of 20 words that assess the
constructs of positive affect (POS) and negative affect
(NEG). Each adjective is rated on a 5-point scale (1 = very
slightly or not at all to 5 = extremely) in response to the
instructions ‘‘indicate to what extent you feel this way right
now, that is, at the present moment’’. Examples of the
10 items which assess positive affect (valence) include
‘‘interested’’ and ‘‘excited’’. Some of the 10 items which
assess negative affect include ‘‘distressed’’ and ‘‘nervous’’.
Cronbach’s coefficient alpha for positive affect as a state,
i.e., assessed under the instructions ‘‘at the present moment’’
is .89; for negative affect, this is .85. Test–retest reliability
over an 8-week interval is .54 for positive affect and .45 for
negative affect when mood is rated as a state; higher test–
retest reliability is reported when the participant is asked to
rate ‘‘typical mood’’, or mood as a trait. These scales have
been used extensively as measures of the two dimensional
models of self report affect. The positive and negative scales
are not significantly correlated according to studies reported
in Watson et al. (1988); others have found these scales to
correlate under some conditions.
Physiological Measure
An Autogenics Biolab module M130 was used to assess
frontal area EMG. The EMG signal was obtained with a
band pass filter at 100–250 HZ. The RMS method was used
to process the signal. Electrodes with a diameter of 12.5
were attached horizontally approximately � inch above
each eyebrow on a vertical line above each pupil. The
ground was attached horizontally between the two active
electrodes.
Signals were sampled at the rate of 10 per second.
Means were collected over 2� min intervals before and
after administration of the Free Choice Protocol, and dur-
ing completion of each of the 7 math problem trials. This
instrument and these filter settings were employed by
Hoehn-Saric et al. (1997), who found evidence that fron-
talis area sEMG reflected central nervous system arousal.
However, means in the present study were obtained over a
2� min interval as opposed to the 5 min interval employed
in that study. Further, as the present study focused on
reactivity as opposed to tonic measures, analysis involving
sEMG controlled for baseline measure by entering the
baseline sEMG as a covariate in relevant analyses.
Experimental Procedure
After the purpose of the study was presented and consent
to participate received, some demographic data (sex,
ethnicity, age) and information on consumption of caffeine
within the past 4 h were obtained.
The ‘‘Free Choice’’ protocol consists of series of trials
during which math problems are presented (Hovanitz et al.
2002). Ten levels of math problem difficulty were created.
The levels of difficulty are differentiated by number of
digits, simplicity of mathematical computation by number
(e.g., by difficulty of operation and by complexity of
numbers operated on, for instance, ‘‘5’’ or ‘‘0’’ vs. ‘‘137’’
and ‘‘263’’).
For this study, 7 trials of math problems were presented
manually to the participant. Each trial involved 15 indi-
vidually-presented problems. Participants chose the diffi-
culty of math problems they wished to work on prior to the
administration of each trial. Their choice was informed:
Before the participants’ initial selection of a trial difficulty,
participants were shown an example problem from each of
the 10 difficulty levels. Participants were told that their
goal was to achieve as high a score as possible, that points
were given for correct answers and that achievement at
higher levels of math difficulty was awarded with more
points. Each problem in a trial was displayed for 5 s, and
then removed from sight. The participant was to provide an
answer within 10 s after the problem was removed. Access
to paper or a calculator was not provided. Any failure to
produce a correct response in this time frame, regardless of
cause (i.e., sneezing, inattention, incorrect answer or no
answer) was considered an incorrect response.
After completion of the first math trial, the participant
was administered the PANAS. The participant was asked
for the math problem difficulty level s/he wished to work
on next, and, following completion of the trial, was again
administered the PANAS. The process was repeated for a
total of 7 trials.
Analysis
Groups reporting high and low mood regulation were
constructed by identifying participants through a mean split
(mean Repair = 22.80). Participants obtaining a score of
22 or 23 were not placed in a low or high mood regulation
group, given the ambiguity of such an assignment. The low
Repair group consisted of 25 males and 17 females; the
high Repair group, 36 males and 35 females.
The evaluation of moment by moment change in
direction of affect valence was made by identifying the
number of times a drop in the quality of affective valence
(report of lower positive affect, higher negative affect, or
higher EMG) was not corrected after choice of the next
level of task difficulty. This technique of assessing a failure
of homeostasis was introduced in the research on baro-
ceptor control of fluctuations in blood pressure (Reyes del
Paso 1994). For example, consider a trial (T ? 1) where a
Appl Psychophysiol Biofeedback (2011) 36:113–119 115
123
participant’s self reported mood declined from the trial
previous (T). If the subsequent trial (T ? 2) also resulted in
a decline in mood quality, then that participant would be
considered to have produced a ‘‘ramp’’, serving here as a
measure of failure to regulate. Simply put, a ramp was
produced by two consecutive drops in positive affect, two
consecutive rises in negative affect, or two consecutive
increases in EMG; the lower the number of ramps, the
better the regulation. The seven trials of math problems
created the opportunity for 5 ramps (trials assessing mood
were allowed to overlap; e.g., the second trial for the first
‘‘ramp’’ was the first trial for the second ‘‘ramp,’’ and the
third trial was the first trial for the third ‘‘ramp,’’ etc.). The
number of ‘‘ramps’’, then, served as a dependent variable
assessing objective mood regulation.
Results
Descriptive Data
A significant difference was not found on ethnicity
between low and high scorers on Repair, however, caffeine
consumption did significantly differ [F(1,122) = 9.06,
p \ .005]. Drinking caffeine prior to the experimental
phase was associated with having reported a higher ability
to regulate mood on Repair (23.55 vs. 21.11). The possible
confounding effect of this variable was addressed by
including this variable as a covariate.
Gender differences were also calculated among these
variables. Significant differences in mood regulation ability
were not found [F(1,122) = .61, ns]; however, as typically
found, trait anxiety showed a significant gender difference
[F(1,120) = 7.94, p \ .01; mean for males = 16.70 (8.10);
females, 20.86 (8.15)]. Significant gender differences were
not found on the summed mean scores across the 7 trials
for positive affect, negative affect, or sEMG.
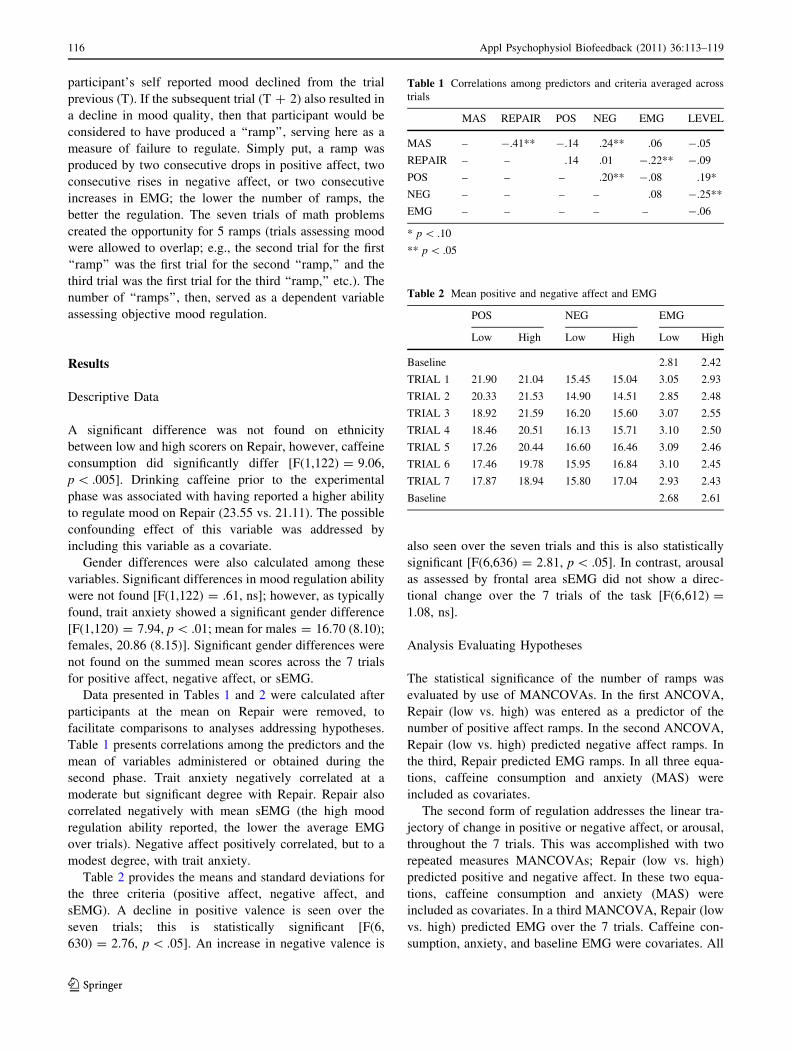
Data presented in Tables 1 and 2 were calculated after
participants at the mean on Repair were removed, to
facilitate comparisons to analyses addressing hypotheses.
Table 1 presents correlations among the predictors and the
mean of variables administered or obtained during the
second phase. Trait anxiety negatively correlated at a
moderate but significant degree with Repair. Repair also
correlated negatively with mean sEMG (the high mood
regulation ability reported, the lower the average EMG
over trials). Negative affect positively correlated, but to a
modest degree, with trait anxiety.
Table 2 provides the means and standard deviations for
the three criteria (positive affect, negative affect, and
sEMG). A decline in positive valence is seen over the
seven trials; this is statistically significant [F(6,
630) = 2.76, p \ .05]. An increase in negative valence is
also seen over the seven trials and this is also statistically
significant [F(6,636) = 2.81, p \ .05]. In contrast, arousal
as assessed by frontal area sEMG did not show a direc-
tional change over the 7 trials of the task [F(6,612) =
1.08, ns].
Analysis Evaluating Hypotheses
The statistical significance of the number of ramps was
evaluated by use of MANCOVAs. In the first ANCOVA,
Repair (low vs. high) was entered as a predictor of the
number of positive affect ramps. In the second ANCOVA,
Repair (low vs. high) predicted negative affect ramps. In
the third, Repair predicted EMG ramps. In all three equa-
tions, caffeine consumption and anxiety (MAS) were
included as covariates.
The second form of regulation addresses the linear tra-
jectory of change in positive or negative affect, or arousal,
throughout the 7 trials. This was accomplished with two
repeated measures MANCOVAs; Repair (low vs. high)
predicted positive and negative affect. In these two equa-
tions, caffeine consumption and anxiety (MAS) were
included as covariates. In a third MANCOVA, Repair (low
vs. high) predicted EMG over the 7 trials. Caffeine con-
sumption, anxiety, and baseline EMG were covariates. All
Table 1 Correlations among predictors and criteria averaged across
trials
MAS REPAIR POS NEG EMG LEVEL
MAS – -.41** -.14 .24** .06 -.05
REPAIR – – .14 .01 -.22** -.09
POS – – – .20** -.08 .19*
NEG – – – – .08 -.25**
EMG – – – – – -.06
* p \ .10
** p \ .05
Table 2 Mean positive and negative affect and EMG
POS NEG EMG
Low High Low High Low High
Baseline 2.81 2.42
TRIAL 1 21.90 21.04 15.45 15.04 3.05 2.93
TRIAL 2 20.33 21.53 14.90 14.51 2.85 2.48
TRIAL 3 18.92 21.59 16.20 15.60 3.07 2.55
TRIAL 4 18.46 20.51 16.13 15.71 3.10 2.50
TRIAL 5 17.26 20.44 16.60 16.46 3.09 2.46
TRIAL 6 17.46 19.78 15.95 16.84 3.10 2.45
TRIAL 7 17.87 18.94 15.80 17.04 2.93 2.43
Baseline 2.68 2.61
116 Appl Psychophysiol Biofeedback (2011) 36:113–119
123

repeated measures MANCOVAs controlled sphericity by
the use of the Huynh–Feldt Epsilon.
Missing data points resulted in the elimination of that
measure from the relevant analysis.
Positive Affect
Repair [F(1,107) = 9.42, p \ .005] predicted the number
of ramps (reflecting decline in positive valence). Partici-
pants reporting low mood regulation ability on Repair
produced a mean of 3.48 (STD = 1.15) ramps whereas
those reporting high Repair obtained a mean of 2.80 ramps
(STD = 1.21). In other words, participants who reported
low levels of mood regulation ability were less able to
correct declining positive affect valence than those who
reported high ability.
Repeated Measures
The mean differences between Repair groups over time are
not statistically different when family wise error rates are
controlled using the simulate option for general mixed and
repeated measures models from the Statistical Analysis
Software (SAS). Table 2 provides the mean data for all
trials.
Negative Affect
Repair did not significantly predict the number of negative
valence ramps [F(1, 109) = .01, ns] nor the linear pro-
gression of negative affect over the 7 trials [F(6,612) =
.91, ns].
sEMG
Repair predicted sEMG ramps at a trend level of signifi-
cance [F(1,107) = 3.79, p = .054]. However, the mean
number of ramps are not in the predicted direction (low
mood regulation produced a mean of 2.19 and std of 1.23,
whereas high mood regulation obtained a mean of 2.55 and
a std of 1.00).
Repair did not significantly predict linear change in
sEMG over the 7 trials [F(6,582) = .40, ns]. It should be
noted that Repair had previously been found to negatively
correlate with the mean sEMG across trials.
Trait Anxiety
When employed as a covariate in the equations evaluating
repeated measures hypotheses, trait anxiety (MAS) exerted
a significant main effect on negative valence [F(1,102) =
6.62, p \ .05] and a trend level main effect on sEMG
[F(1,97) = 2.97, p = .08].
Caffeine
When employed as a covariate in the equation evaluating
the repeated measures hypothesis caffeine exerted a posi-
tive main effect with positive affect [F(1,101) = 4.33,
p \ .05).
Discussion
The purpose of this study was to obtain evidence that
perception of affect regulation ability predicted objectively
measured changes in core affect. Findings demonstrated
that low scores on the TMMS—Repair scale predicted less
ability to alter declining positive affect when participants
engaged in a task that permitted substantial moment by
moment control over task difficulty. The mood regulation
ability was apparent when analyzed in a nonlinear fashion;
more successive trials of decreasing positive affect were
found among those reporting low mood regulation ability.
Interestingly, Repair did not predict ability to avoid
increasing negative affect. Perhaps the most remarkable
aspect of this failure to find a significant effect is that most
items on the TMMS—Repair scale refer to the regulation
of a negative mood state, as opposed to the maintenance of
a positive one. A possible contributor to the failure to find
an effect may be observed in a close examination of the
mean data in Table 2. Whereas the mean positive affect
scores declines, for both low and high mood regulation
ability groups, in a clear linear fashion, a simple linear
increase is not observed for both groups with respect to
negative affect. A post hoc analysis was performed to
determine if the covariate MAS was responsible for the
absence of a regulation effect. The covariate was not found
to account for the absence of the hypothesized findings.
Two other aspects of descriptive information shed some
additional light on interpretation of results, however. First,
whereas math problems are perhaps the most common
laboratory stressor employed, the math problem protocol
used here may be the only one employed where the par-
ticipants choose the difficulty of the problems they work
on. The intent, of course, is to formally structure a means
of behavioral regulation for the participants. However, that
freedom fundamentally alters the task—it may no longer be
a laboratory stress task. As seen in Table 1, negative affect
is correlated with the level of math problems chosen—but
in a negative direction. In other words, the higher the
average level of difficulty chosen, the lower the average
Appl Psychophysiol Biofeedback (2011) 36:113–119 117
123

negative affect. It would seem that average level chosen is
more like a measure of positive engagement than a measure
of stress. Some data support this interpretation. In Table 1,
a positive correlation is found between chosen level and
positive affect (at a trend level of significance). If this is the
proper interpretation, then at least in part, these participants
were not first and foremost regulating stress, but instead
regulating their interest or engagement with the task.
The mood regulation scale Repair significantly predicted
changes in sEMG, as hypothesized, but not in the predicted
direction when analyzed nonlinearly. The low regulation
group produced fewer ramps (made more adjustments) than
the high regulation group. Repair did not predict linear
change over the course of the 7 trials. However, Repair
significantly although modestly predicted average sEMG
(as shown in Table 1) in the expected direction; examina-
tion of Table 2 reveals an ‘‘eyeball’’ view. Clearly these
findings are complex; interpretation of these data can be
only tentative. The sEMG as a measure is very difficult; the
very high noise to signal ratio creates difficulties in the
simple collection of valid data. Even if one assumes that
the presence of statistically significant data is an indicator
of valid data, other problems exist. Another ‘‘problem’’
may be that the sEMG may assess a general factor and be
relevant to many constructs. The frontal area sEMG cor-
relates with anxiety, headache, and depression (Hovanitz
et al. 2002), to name but a few. In this particular study,
sEMG could even have tapped into the arousal necessary
for successful task engagement. These variables may be in
active competition. Having made note of the possibilities,
there are no analyses here that suggest task performance
was improved by heightened sEMG. One point that is
perhaps important to note is that the temporal window of
reactivity for sEMG, as it relates to the kind of arousal that
was intended to be assessed here, may be rather long.
Repair correlated with sEMG in the expected direction
when assessed over about a 30 min window.
These data addressing the hypotheses needs to be placed
in the larger context of the descriptive data. In terms of the
analyses of linear patterns, positive affect declined, negative
affect rose, and arousal did not show significant change for
both low and high mood regulation ability groups. Thus,
while there was evidence of ability to regulate positive affect
among those claiming mood regulation ability while the task
was underway, and there was a difference favoring the high
regulation group overall, the successful efforts were not
sufficient to sustain the degree of positive affect present at the
start of the protocol. Statistically speaking, negative affect
declined overall as well. In addition, those claiming good
mood regulation ability did not, at the completion of the
protocol, report a significantly more optimal mood state
(more positive or less negative) than those reporting low
mood regulation ability. Thus, although evidence was found
that those reporting mood regulation ability were able to
engage in mood valence trajectory corrections, the magni-
tude or persistence of these corrections was not large.
A look at recent reflections on the nature of the PANAS
positive and negative affect scales and what they measure,
beyond perhaps the intended valence, may provide more
insights. Positive affect as assessed by the PANAS is now
described as related to approach motivation (Watson 2000)
and the PANAS scales have been renamed by the author to
reflect interest in approach/avoidance motivation models.
More recent descriptions for what the positive affect PANAS
scale measures, by the author of the scale, reflect a change
from the original formulation that may explain why this scale
was more susceptible to mood regulation efforts: ‘‘Positive
affect is composed of positively valenced mood states,
including enthusiasm, energy, interest, pleasure, confi-
dence’’ (Gray and Watson 2007, p. 173), and some have
suggested that the scale measures approach motivation that
may even be negative in nature (Harmon-Jones et al. 2009).
Indeed, some kind of an explanation like this might account
for why the positive and negative PANAS scales not only
failed to demonstrate a bipolar relation, as would have been
evidenced by a negative correlation, but were in fact posi-
tively (albeit weakly) correlated in the present study.
This study provided some preliminary data suggesting
that perceived mood regulation ability can predict objec-
tively measured affect regulation in a laboratory setting. It
appears that the type of affect modulated concerned positive
task engagement, in a protocol designed to study the self
regulation of affect and behavior (Carver 2004). However,
the methodology employed here limited what kind of regu-
lation could be found; the protocol optimized the partici-
pant’s ability to regulate mood through positive task
engagement. Future studies should consider use of other
measures of affect, and might benefit from considering a
multisession or longitudinal design employing protocols that
include passive coping tasks of a long duration. Assessment
of the consumption of other substances, such as nicotine or
prescription medications, would also eliminate other sources
of unintended variability in mood. Alternative methods of
assessing arousal may be attempted as well. While some
success has been achieved, as of yet, mood regulation ability
has not been demonstrated to be a generalized skill that
allows modulation of affect by means other than positive task
engagement, by populations other than college students, and
by other measures of affect.
References
Brehm, J. W., Miron, A. M., & Miller, K. (2009). Affect as a
motivational state. Cognition & Emotion, 23, 1069–1089.
Carver, C. S. (2004). Self-regulation of action and affect.
In R. F. Baumeister & K. D. Vohs (Eds.), Handbook of
118 Appl Psychophysiol Biofeedback (2011) 36:113–119
123

self-regulation: Research, theory and applications. New York,
NY: Guilford Press.
Ekman, P., & Davidson, R. J. (Eds.). (1994). The nature of emotion:Fundamental questions. New York: Oxford University Press.
Frijda, N. H. (2006). The laws of emotion. Mahwah, NJ: Erlbaum.
Gray, E. K., & Watson, D. (2007). Assessing positive and negative
affect via self-report. In J. A. Coan & J. J. B. Allen (Eds.),
Handbook of emotional elicitation and assessment (pp. 171–183).
New York: Oxford Press.
Gross, J. J. (1998). The emerging field of emotion regulation: An
integrative review. Review of General Psychology, 2, 271–299.
Gross, J. J., & John, O. P. (2003). Individual differences in two
emotion regulation processes: Implications for affect, relation-
ships, and well-being. Journal of Personality and SocialPsychology, 85, 348–362.
Harmon-Jones, E., Hormon-Jone, C., Abramson, L., & Peterson, C. K.
(2009). PANAS positive activation is associated with anger.
Emotion, 9, 183–196.
Hazlett, R. L., HcLeod, D. R., & Hoehn-Saric, R. (1994). Muscle
tension in generalized anxiety disorder: Elevated muscle tonus or
agitated movement? Psychophysiology, 31, 189–195.
Hoehn-Saric, R., Hazlett, R. L., Pourmotabbed, R., & McLeod, D. R.
(1997). Does muscle tension reflect arousal? Relationship
between electromyographic and electroencephalographic record-
ings. Psychiatry Research, 71, 49–55.
Hoehn-Saric, R., & McLeod, D. R. (2000). Anxiety and arousal:
Physiological changes and their perception. Journal of AffectiveDisorders, 61, 217–224.
Hovanitz, C. A., Christianson, A. L., Stokes-Crowe, L., & Scheff, J.
(2002a). Effects of headache-state and headache-proneness on
objective and perceived performance. Headache, 42, 603–611.
Hovanitz, C. A., Filippides, M., Lindsay, D., & Scheff, J. (2002b).
Muscle tension and physiologic hyperarousal, performance and
state affectivity: Assessing the independence of effects in
frequent headache and depression. Applied Psychophysiologyand Biofeedback, 27, 29–44.
Metcalfe, J., & Shimamura, A. P. (1994). Metacognition: Knowingabout knowing. Cambridge, MA: MIT Press.
Reyes del Paso, G. A. (1994). A program to assess baroreceptor
cardiac reflex function. Research Methods, Instruments, andComputers, 26, 62–64.
Russell, J. A. (2003). Core affect and the psychological construction
of emotion. Psychological Review, 110, 145–175.
Russell, J. A. (2009). Emotion, core affect, and psychological
construction. Cognition & Emotion, 23, 1259–1283.
Salovey, P., Mayer, J. D., Goldman, S. L., Turvey, C., & Palfai, T. P.
(1995). Emotional attention, clarity, and repair: Exploring
emotional intelligence using the trait meta-mood scale. In
J. W. Pennebaker (Ed.), Emotion, disclosure, and health(pp. 125–154). Washington, D.C.: APA.
Taylor, J. A. (1953). A personality scale of manifest anxiety. TheJournal of Abnormal and Social Psychology, 48, 285–290.
Tellegen, A. (1985). Structures of mood and personality and their
relevance to assessing anxiety, with an emphasis on self-report.
In A. H. Tuma & J. D. Maser (Eds.), Anxiety and the anxietydisorders (pp. 681–706). Hillsdale, NJ: Erlbaum.
Thayer, R. E. (1989). The biopsychology of mood and arousal. New
York: Oxford University Press.
Thayer, R. E. (1996). The origin of everyday moods: Managingenergy, tension, and stress. New York: Oxford University Press.
Thompson, B. L., Waltz, J., Croyle, K., & Pepper, A. C. (2007). Trait
meta-mood and affect as predictors of somatic symptoms and
life satisfaction. Personality and Individual Differences, 43,
1786–1795.
Watson, D. (2000). Mood and temperament. New York: Guilford
Press.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and
validation of brief measures of positive and negative affect: The
PANAS scales. Journal of Personality and Social Psychology,54, 1063–1070.
Watson, D., & Tellegen, A. (1985). Toward a consensual structure of
mood. Psychological Bulletin, 98, 219–235.
Watson, D., & Tellegen, A. (1999). Issues in the dimensional
structure of affect—effects of descriptors, measurement error,
and response formats: Comment on Russell and Carroll (1999).
Psychological Bulletin, 125, 601–610.
Appl Psychophysiol Biofeedback (2011) 36:113–119 119
123