diagnostic radiology and nuclear medicine imaging in...
TRANSCRIPT
Diagnostic Radiology and Nuclear Medicine Imaging in
Hodgkin’s Disease
March 2001
Brett Cox, Harvard Medical School, Year IIIGillian Lieberman, MD
Brett CoxGillian Lieberman, MD
2
Agenda
• Introduction to radiological regions of the mediastinum.• Differential diagnosis of an anterior mediastinal mass.• Brief review of Hodgkin’s disease.• Radiological imaging for Hodgkin’s disease.
– Menu of tests– Diagnostic potential and limitations of tests– Role in treatment monitoring and follow-up– Introduction to gallium scanning
Brett CoxGillian Lieberman, MD
3
Patient Clinical History
• A previously healthy 26-year-old white male was referred to the BIDMC infectious disease department for evaluation of:– Anorexia with weight loss of 173 to 148 pounds over 8 months– Occasional headaches– Nonproductive cough– Prolonged unexplained fevers to 1032
– Worsening drenching night sweats• Entire infectious disease work-up was negative.
Brett CoxGillian Lieberman, MD
4
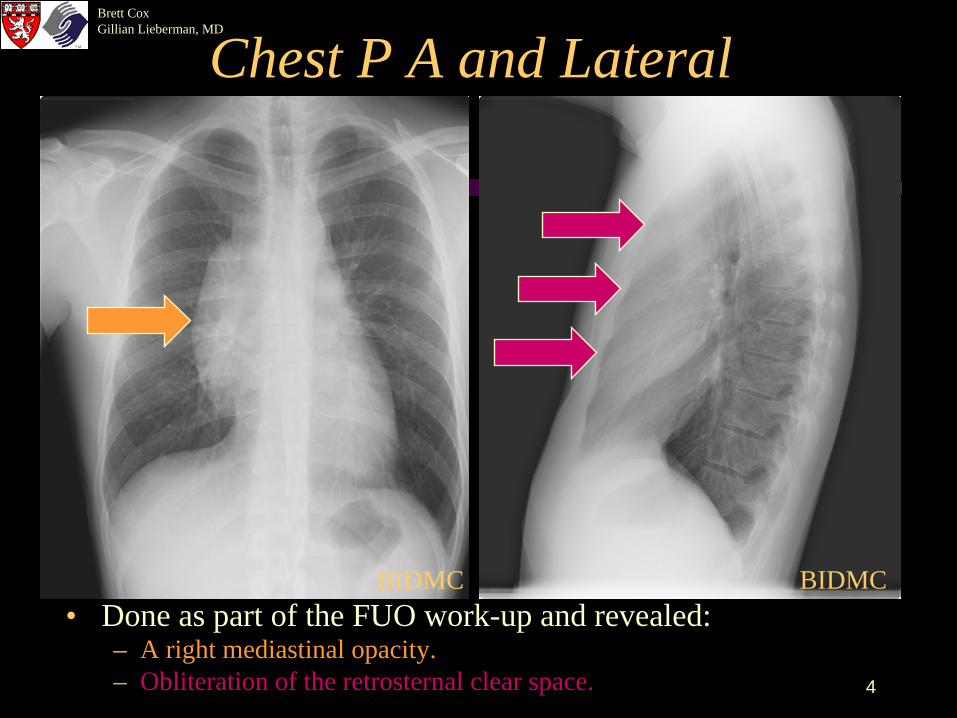
Chest P A and Lateral
• Done as part of the FUO work-up and revealed:
– Obliteration of the retrosternal clear space.– A right mediastinal opacity.
BIDMC BIDMC
Brett CoxGillian Lieberman, MD
5
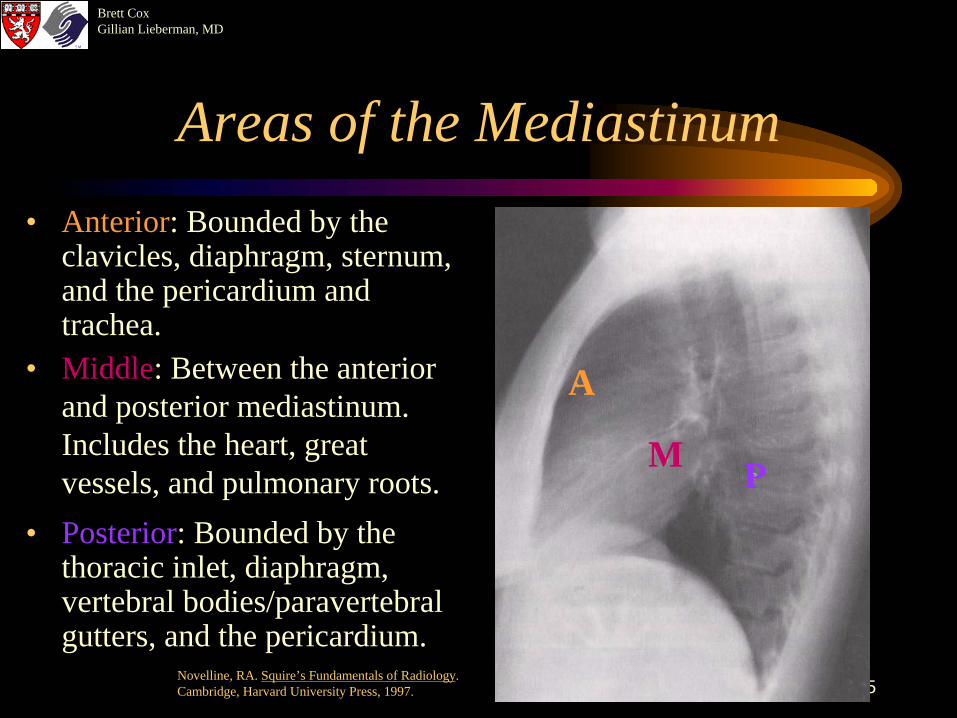
Areas of the Mediastinum
• Middle: Between the anterior and posterior mediastinum. Includes the heart, great vessels, and pulmonary roots.
A
M P
• Anterior: Bounded by the clavicles, diaphragm, sternum, and the pericardium and trachea.
• Posterior: Bounded by the thoracic inlet, diaphragm, vertebral bodies/paravertebral gutters, and the pericardium.
Novelline, RA. Squire’s Fundamentals of Radiology. Cambridge, Harvard University Press, 1997.
Brett CoxGillian Lieberman, MD
6
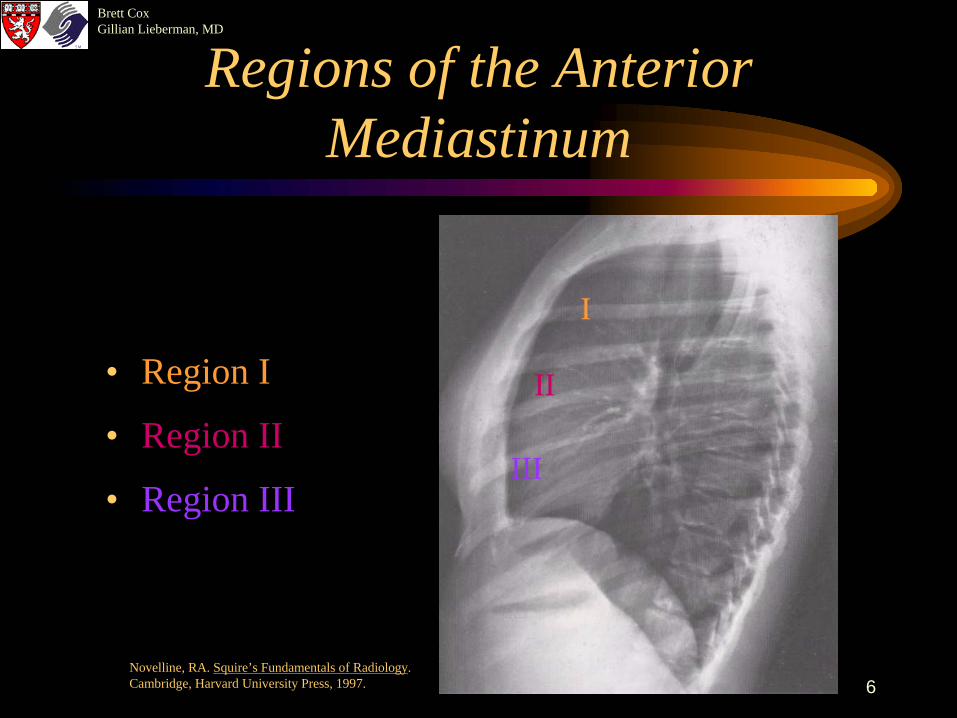
Regions of the Anterior Mediastinum
• Region I
• Region II
• Region III
I
II
III
Novelline, RA. Squire’s Fundamentals of Radiology. Cambridge, Harvard University Press, 1997.
Brett CoxGillian Lieberman, MD
7
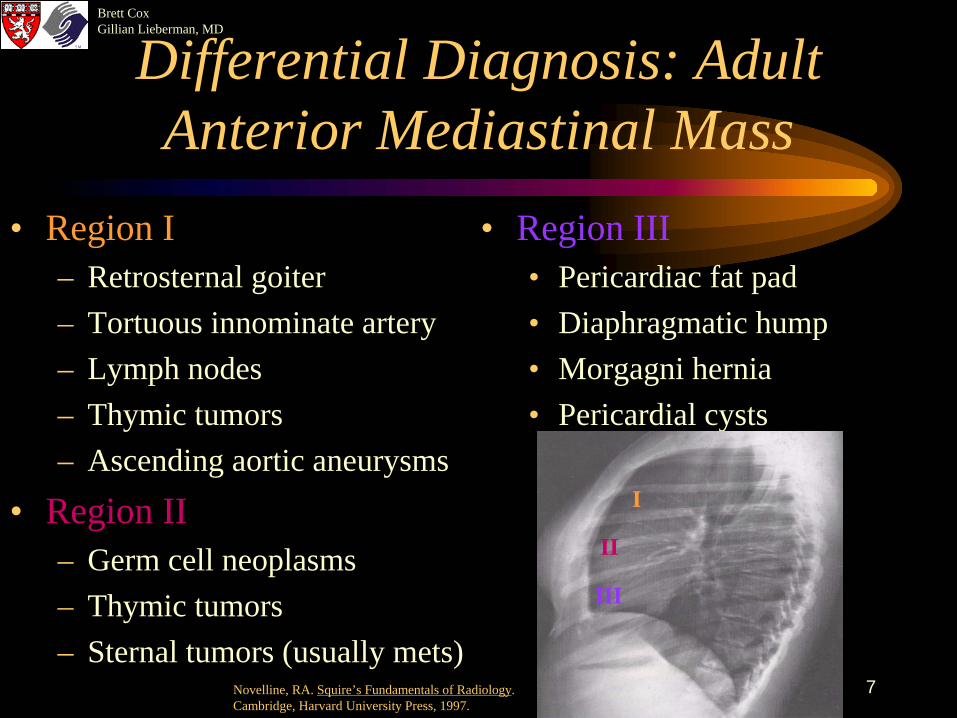
Differential Diagnosis: Adult Anterior Mediastinal Mass
• Region I– Retrosternal goiter– Tortuous innominate artery– Lymph nodes– Thymic tumors– Ascending aortic aneurysms
• Region II– Germ cell neoplasms– Thymic tumors– Sternal tumors (usually mets)
• Region III• Pericardiac fat pad• Diaphragmatic hump• Morgagni hernia• Pericardial cysts
I
II
III
Novelline, RA. Squire’s Fundamentals of Radiology. Cambridge, Harvard University Press, 1997.
Brett CoxGillian Lieberman, MD
8
Definitive Diagnosis
• A Chamberlain procedure (mediastinotomy) was performed.
• Multiple biopsies of the large anterior mediastinal mass were taken.
• Histology and flow cytometry revealed Hodgkin’s Disease, nodular sclerosing type.
Brett CoxGillian Lieberman, MD
9
Hodgkin’s Disease
• 7500 new cases per year.• 20% of all lymphomas.• Mean age of diagnosis is 32.• Arises in a single node and spreads characteristically
to anatomically contiguous nodes.
Brett CoxGillian Lieberman, MD
10
Hodgkin’s Disease
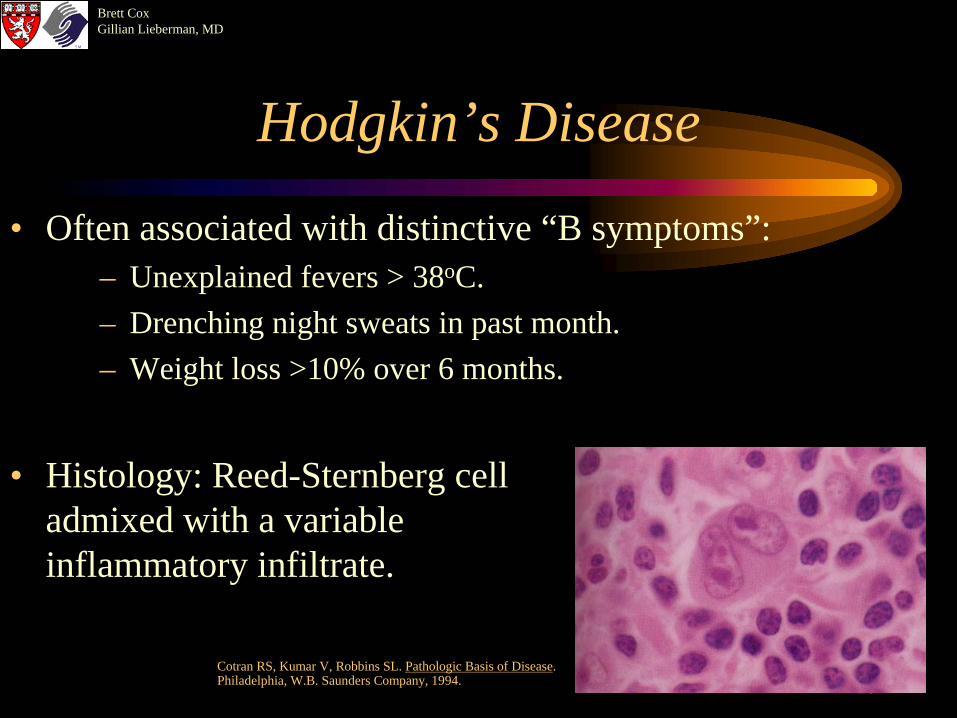
• Often associated with distinctive “B symptoms”:– Unexplained fevers > 38oC.– Drenching night sweats in past month.– Weight loss >10% over 6 months.
• Histology: Reed-Sternberg cell admixed with a variable inflammatory infiltrate.
Cotran RS, Kumar V, Robbins SL. Pathologic Basis of Disease. Philadelphia, W.B. Saunders Company, 1994.
Brett CoxGillian Lieberman, MD
11
Imaging in Hodgkin’s Disease
• Staging is of utmost clinical importance because therapy, prognosis, and clinical course are all intimately related to the distribution of disease.
• Diagnostic radiology and nuclear medicine play a pivotal role in:– Initial staging.– Intra-treatment surveillance.– Post-treatment surveillance.
Brett CoxGillian Lieberman, MD
12
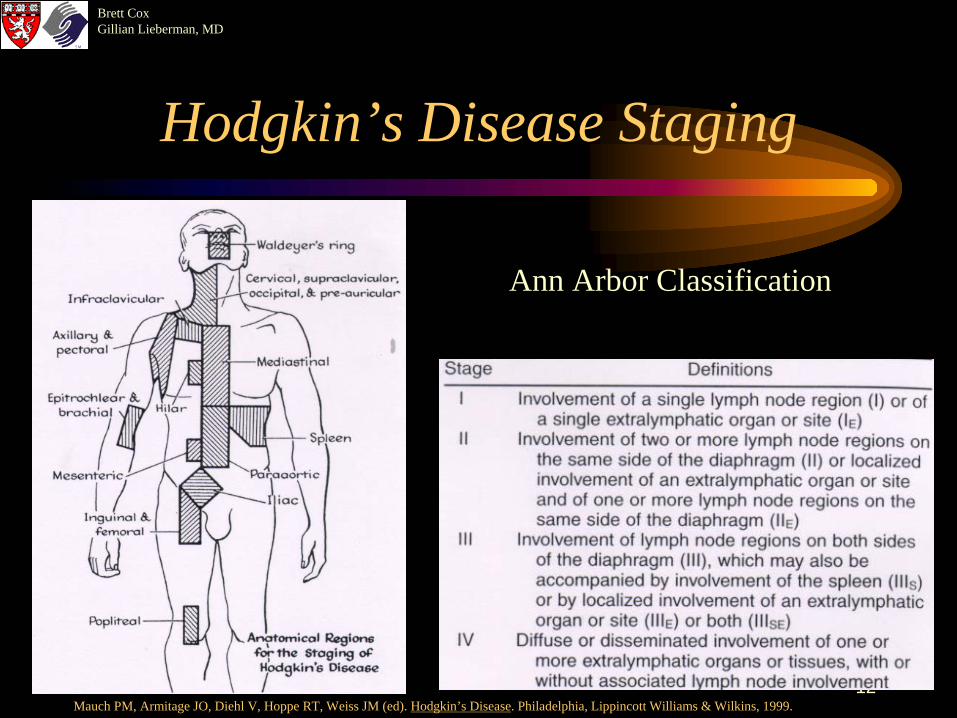
Hodgkin’s Disease Staging
Ann Arbor Classification
Mauch PM, Armitage JO, Diehl V, Hoppe RT, Weiss JM (ed). Hodgkin’s Disease. Philadelphia, Lippincott Williams & Wilkins, 1999.
Brett CoxGillian Lieberman, MD
13
Radiographic work-up in initial staging
• Mandatory radiological work-up includes:– Chest PA/lateral– CT of thorax– CT of abdomen and pelvis ( replaces Bipedal lymphangiogram)
Brett CoxGillian Lieberman, MD
14
CT Scan
– Done with IV contrast, early phase imaging, 1 cm slices.– Detects intrathoracic disease not detected on CXR in 20% of
patients. – Between 10-60% of patients have management change post-CT.– Sensitivity of abdominal node detection equal to bipedal
lymphangiography and is noninvasive and gives added information.
Brett CoxGillian Lieberman, MD
15
Characteristics CT findings:
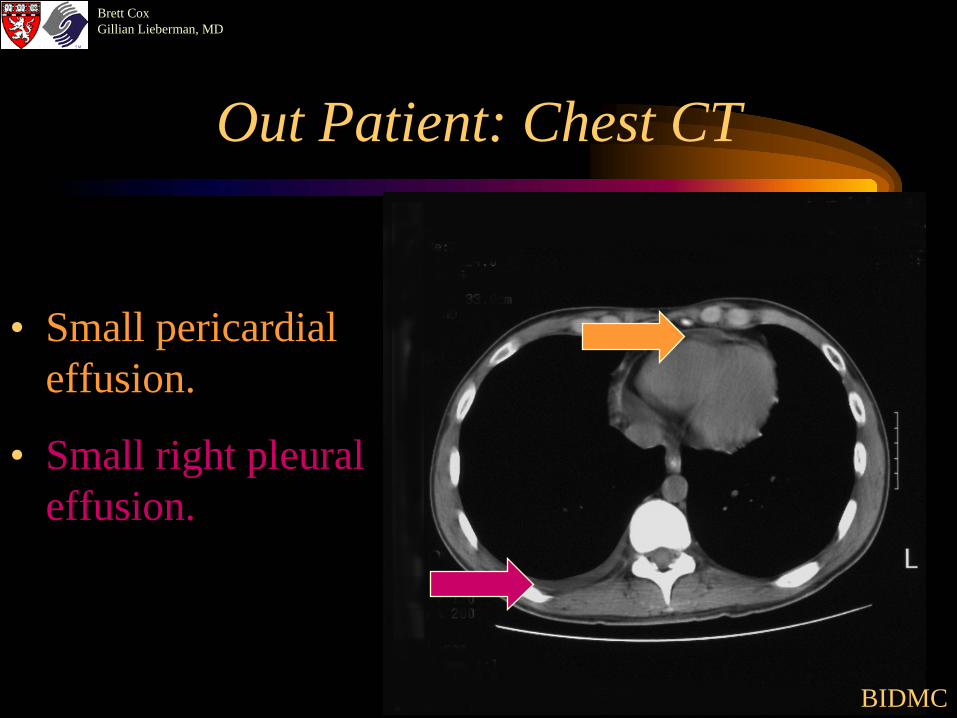
General rule: nodes >1 cm are concerning. – Often see Asymmetric, anterior mediastinal soft tissue mass. – Pleural effusions in 30% of cases (lymphatic/venous obstruction). – Benign pericardial effusions common.
Brett CoxGillian Lieberman, MD
16
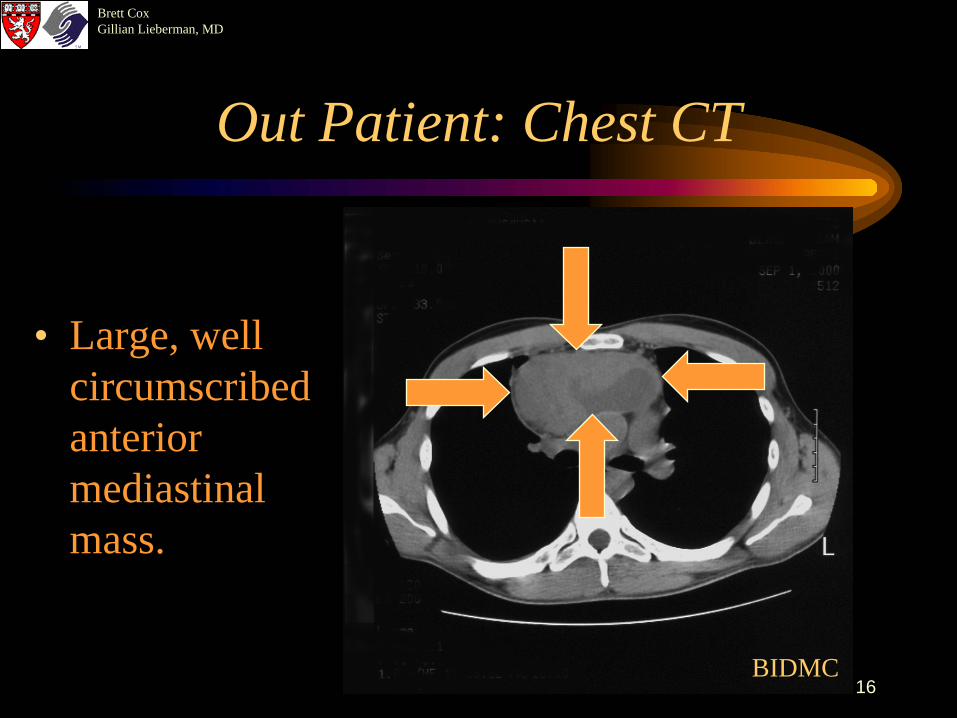
Out Patient: Chest CT
• Large, well circumscribed anterior mediastinal mass.
BIDMC
Brett CoxGillian Lieberman, MD
17
Out Patient: Chest CT
• Small pericardial effusion.
• Small right pleural effusion.
BIDMC
Brett CoxGillian Lieberman, MD
18
Radiographic work-up in initial staging – optional tests
• Liver and spleen ultrasonography– If clinical suspicion for involvement.– Specificity & sensitivity similar to CT or MRI.
• Technetium bone scanning– If bony pain, questionable lesions on other studies.
• MRI– If suspected occult liver, spleen, thymus, bone marrow lesions.– Specificity & sensitivity similar to CT for liver or spleen involvement.
• Gallium scanning– Useful in differentiating scarring from active mediastinal lymphoma.
Brett CoxGillian Lieberman, MD
19
Gallium radionuclide tumor imaging
• Main indication:– Staging of lymphomas, assessment of their response to therapy, and
relapse detection.• Technique:
– 67Ga-citrate administered I.V.– Acquire delayed images.– SPECT = rotation of a photon detector array around the body to
acquire data from multiple angles. – Determines position and concentration of radionuclide distribution.
• Imaging Mechanism– Rough surrogate marker for tumor metabolic activity.– Increased permeability of tumor vessels– Large extracellular fluid space– Tumor up-regulation of iron-binding proteins such as ferritin
Brett CoxGillian Lieberman, MD
20
Gallium radionuclide tumor imaging
• Contraindications: – None.
• Radiopharmaceutical: 67Ga-Gallium citrate – 8-10 mCi, γ−emitter.– Half-life = 78 hours.– Binds to transferrin (in plasma), lactoferrin (in tissue), and ferritin.
• Equipment:– Gamma camera w/ whole body and tomographic abilities, medium
or high energy collimator, imaging computer.
• Patient Preparation:– Bowel regimen may be given after injection to clear activity.
Brett CoxGillian Lieberman, MD
21
Gallium radionuclide tumor imaging
• Images:– Acquired at 48 and 72 hours.– Sensitivity for detecting HD is about 85%, specificity of 90%. – Sensitivity for mediastinal disease is 95%, specificity of 90%.
• Aftercare:– None.
• Complications:– None.
• Cost:– The cost of SPECT imaging is around $700.
Brett CoxGillian Lieberman, MD
22
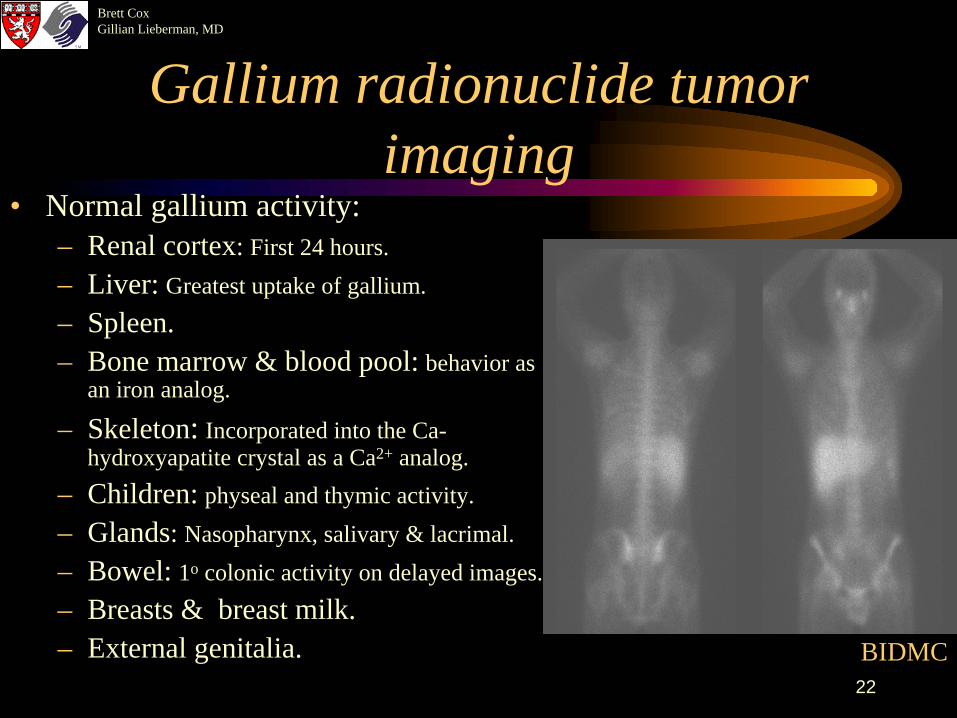
Gallium radionuclide tumor imaging
• Normal gallium activity:– Renal cortex: First 24 hours.– Liver: Greatest uptake of gallium.– Spleen.– Bone marrow & blood pool: behavior as
an iron analog.
– Skeleton: Incorporated into the Ca- hydroxyapatite crystal as a Ca2+ analog.
– Children: physeal and thymic activity.– Glands: Nasopharynx, salivary & lacrimal.– Bowel: 1o colonic activity on delayed images.– Breasts & breast milk.– External genitalia. BIDMC
Brett CoxGillian Lieberman, MD
23
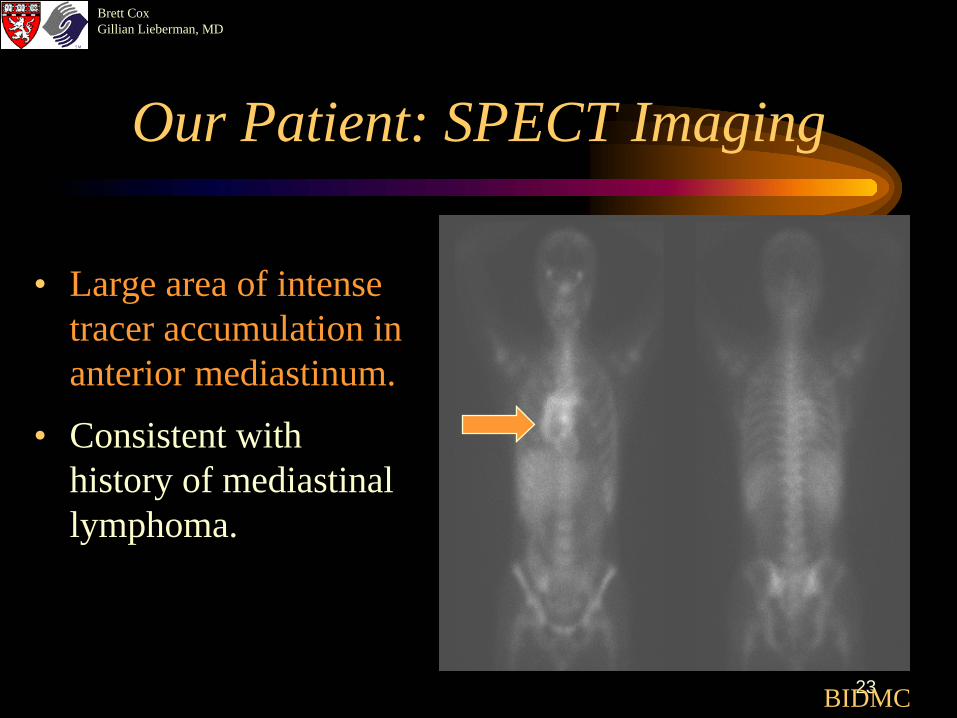
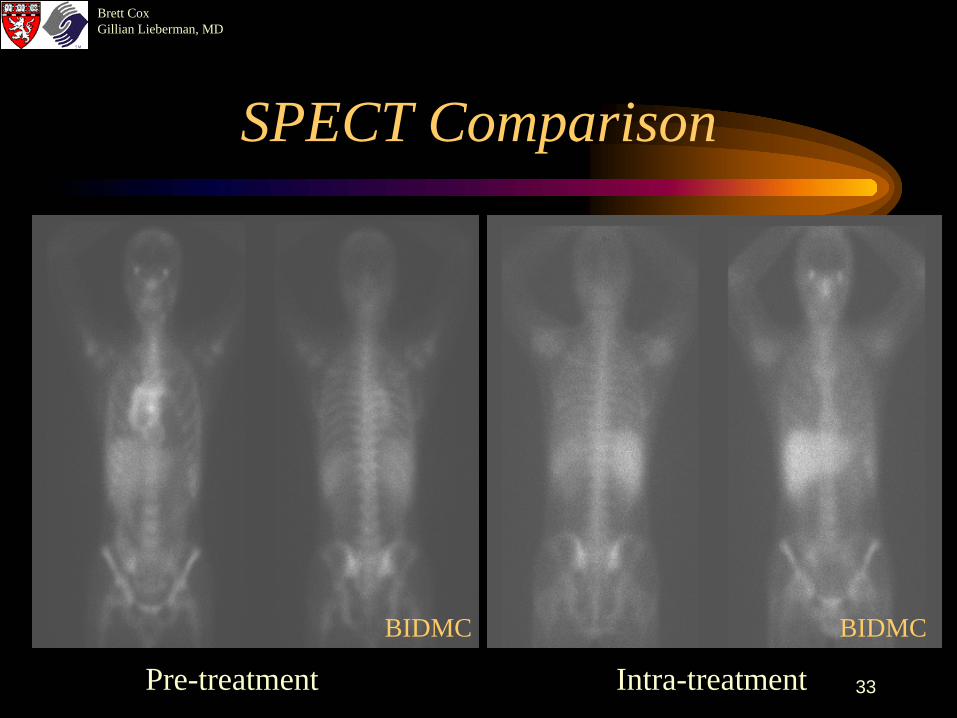
Our Patient: SPECT Imaging
• Large area of intense tracer accumulation in anterior mediastinum.
• Consistent with history of mediastinal lymphoma.
BIDMC
Brett CoxGillian Lieberman, MD
24
Patient Treatment
• Chemotherapy: 5 cycles of ABVD• Radiation therapy: Modified mantle
Brett CoxGillian Lieberman, MD
25
Radiographic intra-treatment surveillance
• Repeat studies with detectable lesions at presentation.• Determines therapeutic response, therapy modification.• Follow:
– Tumor volume decrease.– New lesions.– Therapy-induced lesions.
Brett CoxGillian Lieberman, MD
26
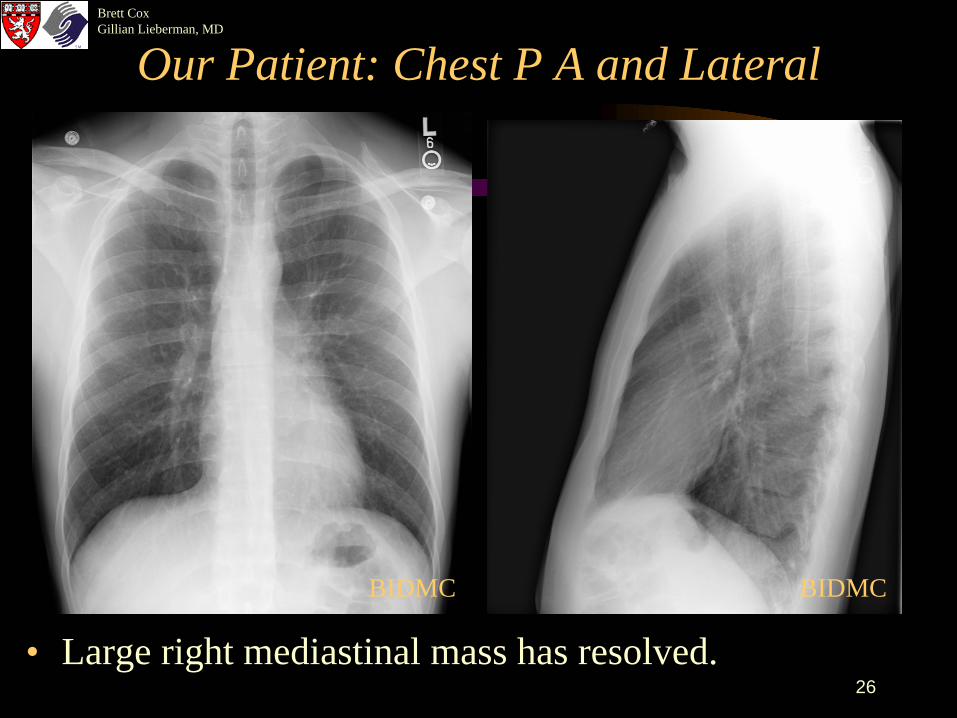
Our Patient: Chest P A and Lateral
• Large right mediastinal mass has resolved.
BIDMCBIDMC
Brett CoxGillian Lieberman, MD
27
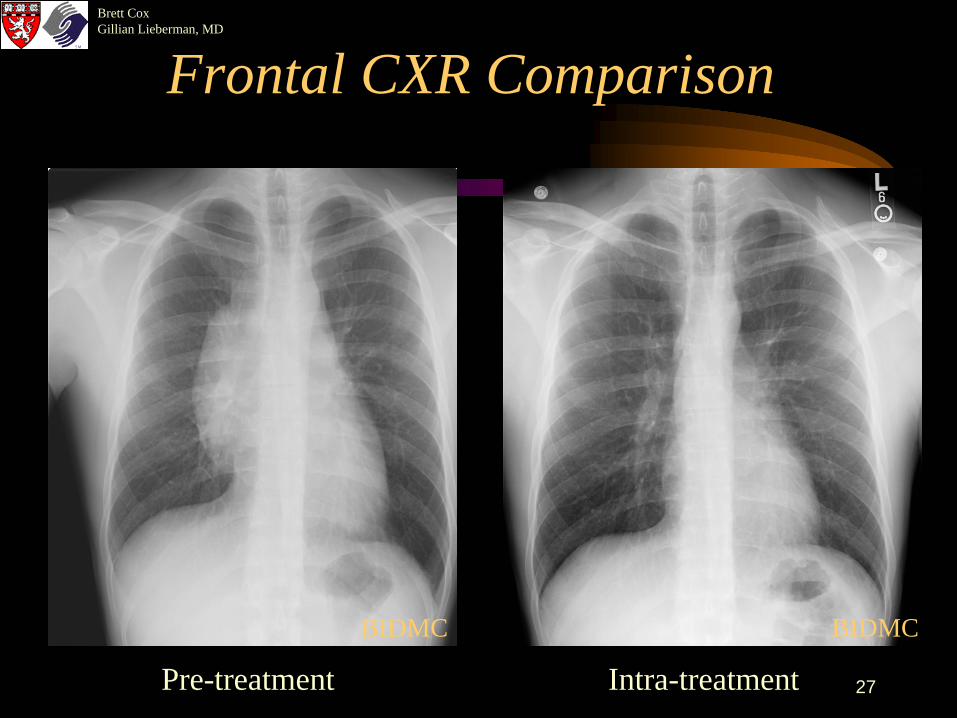
Frontal CXR Comparison
Pre-treatment Intra-treatment
BIDMCBIDMC
Brett CoxGillian Lieberman, MD
28
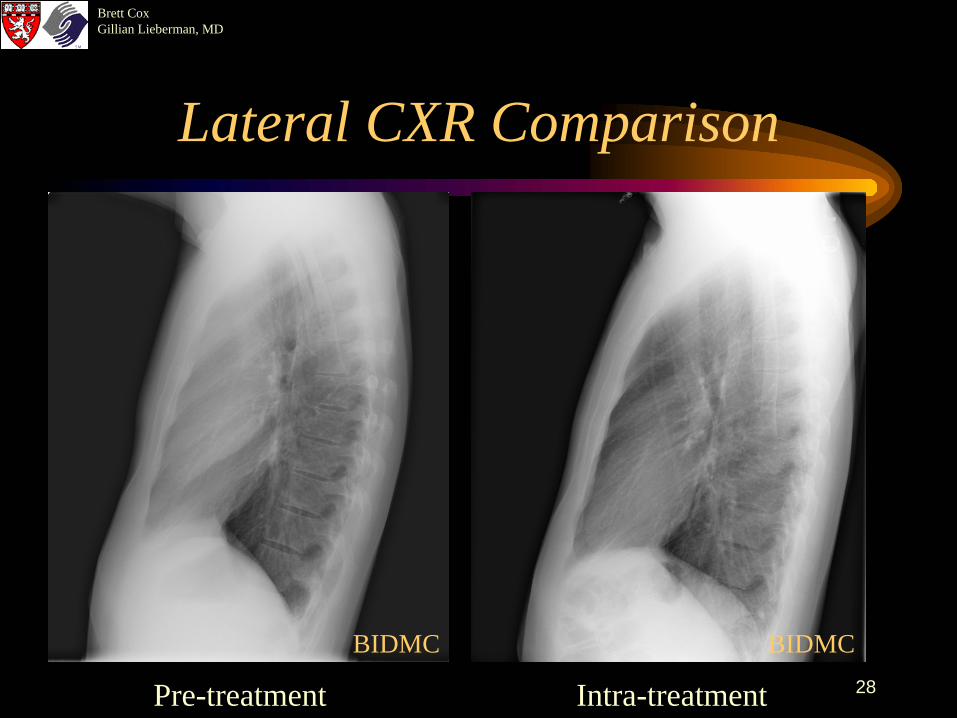
Lateral CXR Comparison
Pre-treatment Intra-treatment
BIDMCBIDMC
Brett CoxGillian Lieberman, MD
29
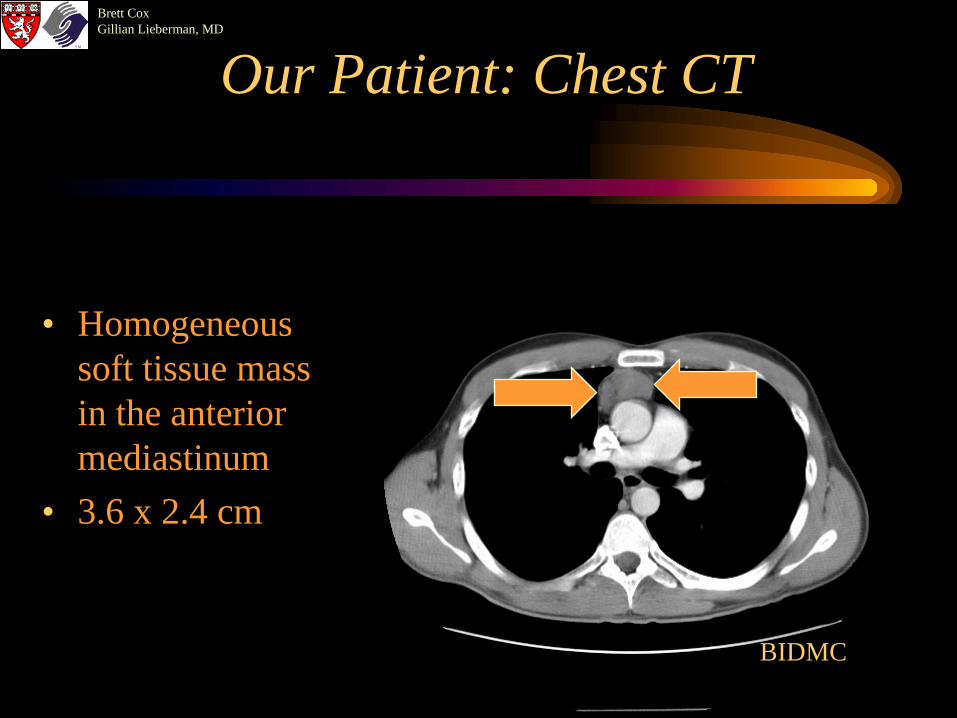
Our Patient: Chest CT
• Homogeneous soft tissue mass in the anterior mediastinum
• 3.6 x 2.4 cm
BIDMC
Brett CoxGillian Lieberman, MD
30
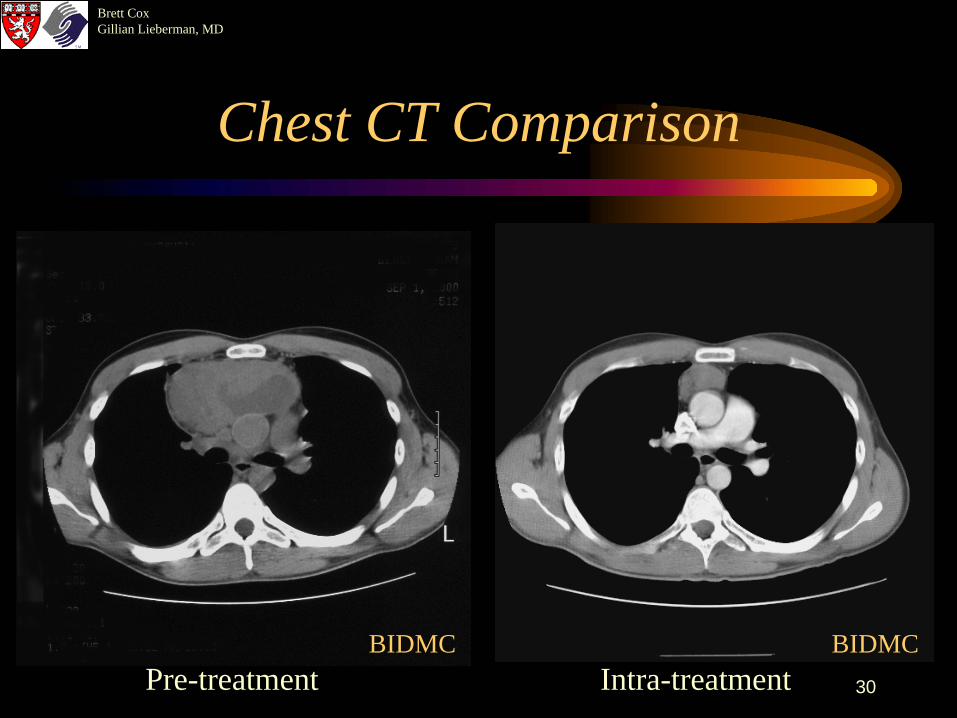
Chest CT Comparison
Pre-treatment Intra-treatmentBIDMCBIDMC
Brett CoxGillian Lieberman, MD
31
Radiographic intra-treatment surveillance
• Residual fibrotic mass often visible on CXR and CT.• Further investigations determine nature of residual
abnormality.• Gallium imaging after 3 cycles of chemotherapy is an
excellent prognostic indicator of clinical outcome. • A complete response is achieved in 70% of patients.
– Longer disease free survival.– Lower mortality.
Brett CoxGillian Lieberman, MD
32
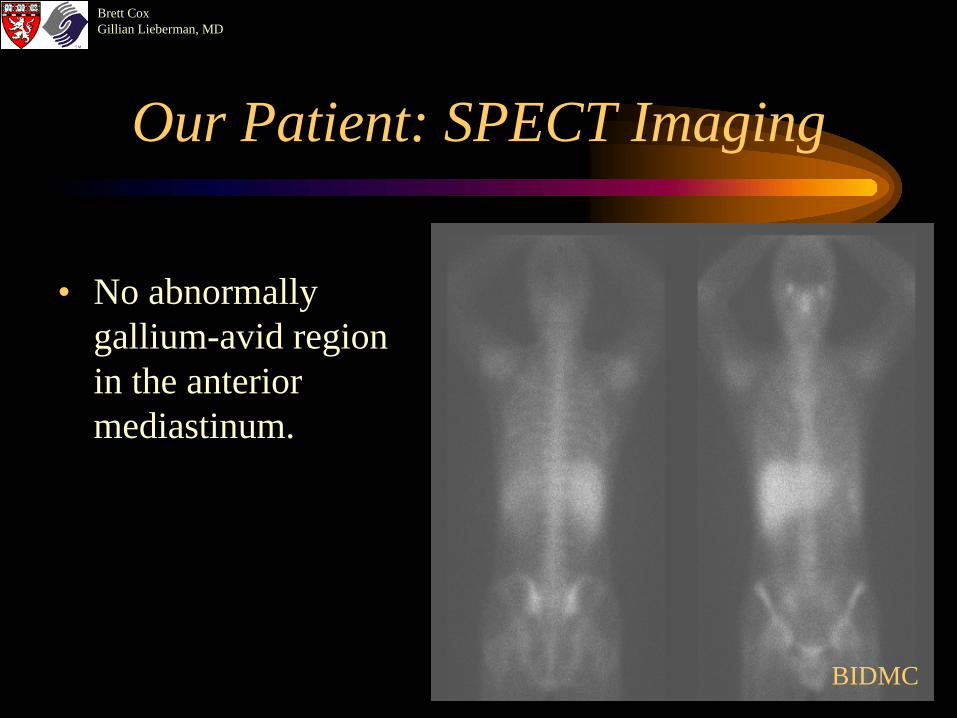
Our Patient: SPECT Imaging
• No abnormally gallium-avid region in the anterior mediastinum.
BIDMC
Brett CoxGillian Lieberman, MD
33
SPECT Comparison
Pre-treatment Intra-treatment
BIDMCBIDMC
Brett CoxGillian Lieberman, MD
34
Radiographic post-treatment surveillance
• Repeat investigations that were abnormal at presentation.• 25% of relapses occur at new sites.• Regression of disease may be slow.• Residual fibrotic mass may still be visible on chest
radiograph and CT.• Further investigations may be necessary to define nature
of residual abnormality, can also follow over time.
Brett CoxGillian Lieberman, MD
35
References
• Castellino RA. 1992. Diagnostic imaging studies in patients with newly diagnosed Hodgkin's disease. Annals of Oncology. 3 Suppl 4:45-7.
• Chapman S, Nakielny R. Aids to Radiological Differential Diagnosis, 3rd edition. Philadelphia, W.B. Saunders Company, 1995, 166-177.
• Chapman S, Nakielny R. A Guide to Radiological Procedures. Philadelphia, W.B. Saunders Company, 1993, 298-299.
• Cotran RS, Kumar V, Robbins SL. Pathologic Basis of Disease. Philadelphia, W.B. Saunders Company, 1994, 643-648.
• Front D, Israel O. 1995. The role of Ga-67 scintigraphy in evaluating the results of therapy of lymphoma patients. Seminars in Nuclear Medicine. 25(1): 60-71.
• Kramer EL, Sanger JJ (ed). Clinical SPECT imaging. New York, Raven Press, 1995, 7-38, 129-135, 197-201.
• Mauch PM, Armitage JO, Diehl V, Hoppe RT, Weiss JM (ed). Hodgkin’s Disease. Philadelphia, Lippincott Williams & Wilkins, 1999, 223-261.
• McLaughlin AF, Magee MA, Greenough R, Allman KC, Southee AE, Meikle SR, Hutton BF, Joshua DE, Bautovich GJ, Morris JG. 1990. Current role of gallium scanning in the management of lymphoma. European Journal of Nuclear Medicine. 16(8-10):755-71.
• Novelline, RA. Squire’s Fundamentals of Radiology. Cambridge, Harvard University Press, 1997.
Brett CoxGillian Lieberman, MD
36
The End!
Brett CoxGillian Lieberman, MD
37
Acknowledgements
• Beverlee Turner for her support and PowerPoint expertise• Larry Barbaras and Ben Crandall our Web Masters