diagnostic error reprint plus journal april 2015
TRANSCRIPT

JournalYOUR SOURCE FOR PROFESSIONAL LIABILITY EDUCATION AND NETWORKING
April 2015 Vol. XXVIII Number 4
PLUS Journal ReprintProfessional Liability Underwriting Society5353 Wayzata Blvd., Suite 600Minneapolis, MN 55416-4758phone 800.845.0778 or 952.746.2580www.plusweb.org
As a nonprofit organization that provides industry information, it is the policy of PLUS to strictly adhere to all applicable laws and regulations, including antitrust laws. The PLUS Journal is available free of charge to members of the Professional Liability Underwriting Society. Statements of fact and opinion in this publication are the responsibility of the authors alone and do not imply an opinion on the part of the members, trustees, or staff of PLUS. The PLUS Journal is protected by state and federal copyright law and its contents may not be reproduced without written permission.
April 2015 PLUS Journal 1
Paul A. Greve, Jr., JD, RPLU, is Executive Vice President at Willis Health Care Practices. He can be reached at [email protected].
P. Divya Parikh isDirector of Research& Risk Management atthe PIAA. She can bereached at [email protected].
Diagnostic Error: Pervasive and PersistentBy Paul A. Greve, Jr., JD, RPLU & P. Divya Parikh MPH
$0
$75,000
$150,000
$225,000
$300,000
$375,000
$450,000
0
2,500
5,000
7,500
10,000
12,500
15,000
Improper performance
Errors in diagnosis Failure to supervise or monitor case
Failure to recognize a complica@on of
treatment
Medica@on errors
Avg Inde
mnity
Closed
Claim
s
Closed Claims Avg Indemnity
Diagnostic Error second by number of closed claims; Highest by average indemnity payment.
Exhibit 1
The problem of diagnostic error has gotten more attention than ever over the last ten years in patient safety and medical literature. There are hundreds of articles on a problem that is both pervasive and persistent. The primary care specialties have been principally involved by virtue of the very nature of their practice.
But closed claim studies by the PIAA have shown that the problem occurs at a significant rate in surgical and other specialties as well. For example, in the time frame of 2008-2012, data from
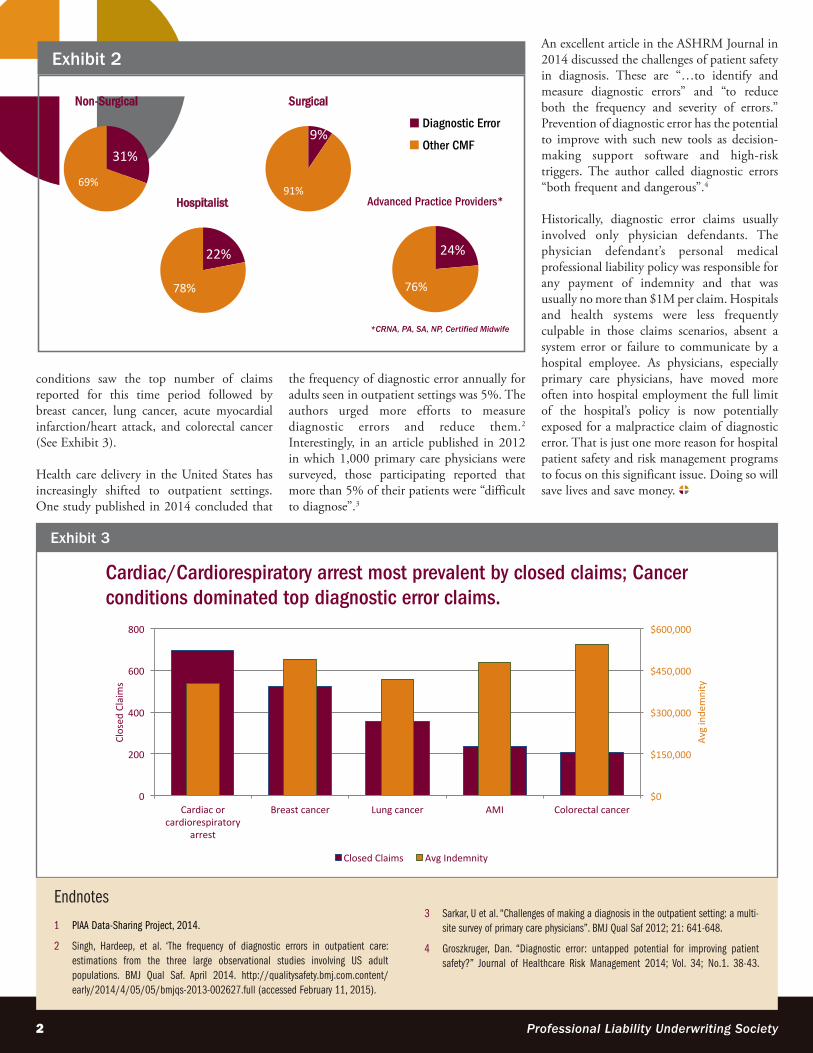
the PIAA Data Sharing Project (DSP) reported that of all the chief medical factors reported, diagnostic errors accounted for the second highest reason for claims and resulted in the highest average indemnity payments (See Exhibit 1). Additionally, surgical specialties were named in 9% of all closed claims reporting diagnostic error; hospitalists’ were named in 22%; advanced practice providers were reported in 24%. Non-surgical specialties (including primary care specialties) were reported in 31% of medical professional liability claims
naming diagnostic error as the chief medical factor in the claim (See Exhibit 2).1
In closer review of the diagnostic error MPL claims reported to the DSP for this five-year period, radiologists were most often named in claims, and claims related to cancer were the top medical conditions (breast, lung, and colorectal cancer specifically). Obstetricians/gynecologists were reported to have the highest indemnity payments reported for diagnostic error. And diagnostic error in cardiac/cardiorespiratory
2 Professional Liability Underwriting Society
conditions saw the top number of claims reported for this time period followed by breast cancer, lung cancer, acute myocardial infarction/heart attack, and colorectal cancer (See Exhibit 3).
Health care delivery in the United States has increasingly shifted to outpatient settings. One study published in 2014 concluded that
the frequency of diagnostic error annually for adults seen in outpatient settings was 5%. The authors urged more efforts to measure diagnostic errors and reduce them.2 Interestingly, in an article published in 2012 in which 1,000 primary care physicians were surveyed, those participating reported that more than 5% of their patients were “difficult to diagnose”.3
An excellent article in the ASHRM Journal in 2014 discussed the challenges of patient safety in diagnosis. These are “…to identify and measure diagnostic errors” and “to reduce both the frequency and severity of errors.” Prevention of diagnostic error has the potential to improve with such new tools as decision-making support software and high-risk triggers. The author called diagnostic errors “both frequent and dangerous”.4
Historically, diagnostic error claims usually involved only physician defendants. The physician defendant’s personal medical professional liability policy was responsible for any payment of indemnity and that was usually no more than $1M per claim. Hospitals and health systems were less frequently culpable in those claims scenarios, absent a system error or failure to communicate by a hospital employee. As physicians, especially primary care physicians, have moved more often into hospital employment the full limit of the hospital’s policy is now potentially exposed for a malpractice claim of diagnostic error. That is just one more reason for hospital patient safety and risk management programs to focus on this significant issue. Doing so will save lives and save money.
31%
69%
Non-Surgical
9%
91%
Surgical
22%
78%
Hospitalist
24%
76%
Advanced Practice Providers*
*CRNA, PA, SA, NP, Certified Midwife
Diagnostic Error
Other CMF
Exhibit 2
$0
$150,000
$300,000
$450,000
$600,000
0
200
400
600
800
Cardiac or cardiorespiratory
arrest
Breast cancer Lung cancer AMI Colorectal cancer
Avg inde
mnity
Closed
Claim
s
Closed Claims Avg Indemnity
Cardiac/Cardiorespiratory arrest most prevalent by closed claims; Cancer conditions dominated top diagnostic error claims.
Exhibit 3
Endnotes
1 PIAA Data-Sharing Project, 2014.
2 Singh, Hardeep, et al. ‘The frequency of diagnostic errors in outpatient care: estimations from the three large observational studies involving US adult populations. BMJ Qual Saf. April 2014. http://qualitysafety.bmj.com.content/early/2014/4/05/05/bmjqs-2013-002627.full (accessed February 11, 2015).
3 Sarkar, U et al. “Challenges of making a diagnosis in the outpatient setting: a multi-site survey of primary care physicians”. BMJ Qual Saf 2012; 21: 641-648.
4 Groszkruger, Dan. “Diagnostic error: untapped potential for improving patient safety?” Journal of Healthcare Risk Management 2014; Vol. 34; No.1. 38-43.