diagnosis diagnosis and investigation of chronic kidney ... · ureterolithiasis. recently concerns...
TRANSCRIPT
2 In Practice FOCUS October 2016
Diagnosis and investigation of chronic kidney disease in cats
Martha Cannon
DIAGNOSIS
Chronic kidney disease (CKD) is a common disorder of cats, particularly those in middle to old age. This article describes a practical approach to the diagnosis of CKD in cats and the additional investigations that will then allow an effective treatment plan to be developed, tailored to the needs of the individual cat. A second article in this supplement covers the approaches to treatment of CKD and its associated complications.
IT is estimated that chronic kidney disease (CKD) affects around 30 per cent of cats that are over 12 years of age (Lulich and others 1992), and a recent UK study of 3309 cats treated at first-opinion veterinary practices (O’Neill and others 2015) identified it as the second most common cause of death in cats of five years and older, accounting for 12.1 per cent
Martha Cannon, Oxford Cat Clinic, 78A Westway, Botley,Oxford OX2 9JU, UKe-mail: [email protected]
of cats (trauma was the most common cause, accounting for 12.2 per cent of cats).
Causes of chronic kidney diseaseCKD is the end result of a wide range of primary disorders that cause irreversible damage to nephrons, eventually leading to reduced glomerular filtration rate (GFR). In a minority of cases a specific underlying cause can be identified, for example, neoplasia, polycystic kidney disease, renal amyloidosis, hypercalcaemic nephropathy. However, in
the majority of cases no primary cause can be identified; in these cases tubulointerstitial nephritis and fibrosis are the most common histological changes, likely to be the end result of a degenerative process initiated by factors including, but not limited to, repeated episodes of renal tissue hypoxia, exposure to toxins, glomerulonephritis, pyelonephritis and repeated transient ureteral obstruction due to ureterolithiasis. Recently concerns have been raised regarding an association between CKD and infection with a feline morbillivirus (Woo and others 2012, Furuya and others 2014, 2016), and also the potential for vaccine induced renal auto-antibodies to contribute to the development of CKD in cats receiving lifelong annual vaccinations (Lappin and others 2005, 2006, Finch and others 2016). In a study of 145 elderly pet cats in the UK the only two factors that were identified as being associated with an increased risk of developing CKD were the presence of moderate or severe dental disease and annual or frequent vaccination (Finch and
The International Renal Interest Society (IRIS) has produced a classification system to stage the severity of chronic kidney disease (CKD) in cats and dogs. The system defines four stages of CKD from stage 1, the mildest end of the spectrum, to stage 4 the most severe or end stage disease, and it has been adopted by the International Society of Feline Medicine (ISFM) and other global veterinary bodies.
In addition to providing a framework for diagnosis and investigation of CKD the IRIS staging system provides practical recommendations on appropriate treatment strategies for animals in each stage of disease. For more information visit www.iris-kidney.com and see also the associated article in this supplement on pp 10-13.
CreatinineThe IRIS system uses the serum creatinine level as the principal biomarker for staging renal disease. It is important to note that for staging purposes creatinine must be measured after medical stabilisation of unwell cats, and after correction of any dehydration. Staging should also be based on two separate measurements of creatinine taken several weeks apart to ensure that the measured value is representative of the
glomerular filtration rate (GFR) in stable disease.
StagesStage 1: Asymptomatic, non-azotaemic kidney disease. Creatinine less than 140 μmol/l, but kidney damage or disease is known to be present.
At this stage treatment is aimed at reversing the primary cause of renal disease, if it is known.
Stage 2: Renal disease causing ‘renal insufficiency’, or ‘renal failure’ in previous terminology. Creatinine in the range of 140 to 250 μmol/l, thus including cats with creatinine at the top end of the reference interval through to those with mild to moderate azotaemia.
Treatment is aimed at reversing the primary cause if it is known, and also preventing progression of disease – with particular reference to identifying and managing hyperphosphataemia, proteinuria and systolic hypertension.
Regular monitoring (eg, every three to six months) of key clinical and other parameters is important to allow the treatment plan to
be adjusted as the disease progresses.
Stage 3: Chronic kidney disease with moderate to severe azotaemia. Creatinine in the range 251 to 439 μmol/l.
Treatment is aimed at preventing progression, as in stage 2 disease, but as azotaemia becomes more severe it starts to produce signs in its own right and these need to be addressed too with, for example, protein-restricted diets, subcutaneous fluids, antiemetics, and so on.
Stage 4: Severe to end stage renal failure. Creatinine over 440 μmol/l.
Prevention of progression is less possible, and less relevant, treatment is principally aimed at managing azotaemia and improving quality of life.
Further subclassificationHaving assigned a cat with CKD to IRIS stage 1 to 4, further investigations are required to identify the adverse consequences of CKD which have arisen in the individual cat. In particular the IRIS staging system includes sub-staging based on systolic blood pressure and urine protein content (see main text for more detail).
Box 1: International Renal Interest Society (IRIS) staging system for feline chronic kidney disease
2-9 Cannon.indd 2 16/09/2016 15:05
on 26 April 2019 by guest. P
rotected by copyright.http://inpractice.bm
j.com/
In Practice: first published as 10.1136/inp.i4914 on 7 N
ovember 2016. D
ownloaded from
3In Practice FOCUS October 2016
others 2016). Periodontal disease produces a chronic systemic inflammatory response as well as local inflammation, and it is recognised as a risk factor for the development of CKD in people (Chambrone and others 2013) and dogs (DeBowes and others 1996, Bartlett and others 2010).
Progression of chronic kidney diseaseIn the early stages of kidney disease (Box 1) the loss of nephrons has little or no effect on overall kidney function because the healthy animal has a large functional reserve; that is, has more than twice the number of nephrons needed to maintain adequate GFR. In addition, in the early stages of disease loss of nephrons results in a compensatory increase in glomerular size and function of the remaining nephrons, ‘super-nephrons’, which help to maintain total kidney GFR.
However, whatever the initial cause of the disease, ultimately CKD becomes an irreversible, progressive condition.
Progression due to renal compensationWhile the development of compensatory super-nephrons is initially helpful in maintaining GFR, eventually there is burn-out of the overworked nephrons.
Progression due to the consequences of renal failureCKD results in a number of metabolic changes many of which are themselves damaging to the kidneys; for example, dehydration, hypertension, renal secondary hyperparathyroidism, proteinuria, bacterial urinary tract infection, chronic anaemia, acidosis, and so on.
If CKD is identified early enough, and these metabolic consequences can be prevented or managed, much may be done to limit the progression of disease and maintain a good quality of life. Regular screening of older cats is strongly recommended (Box 2).
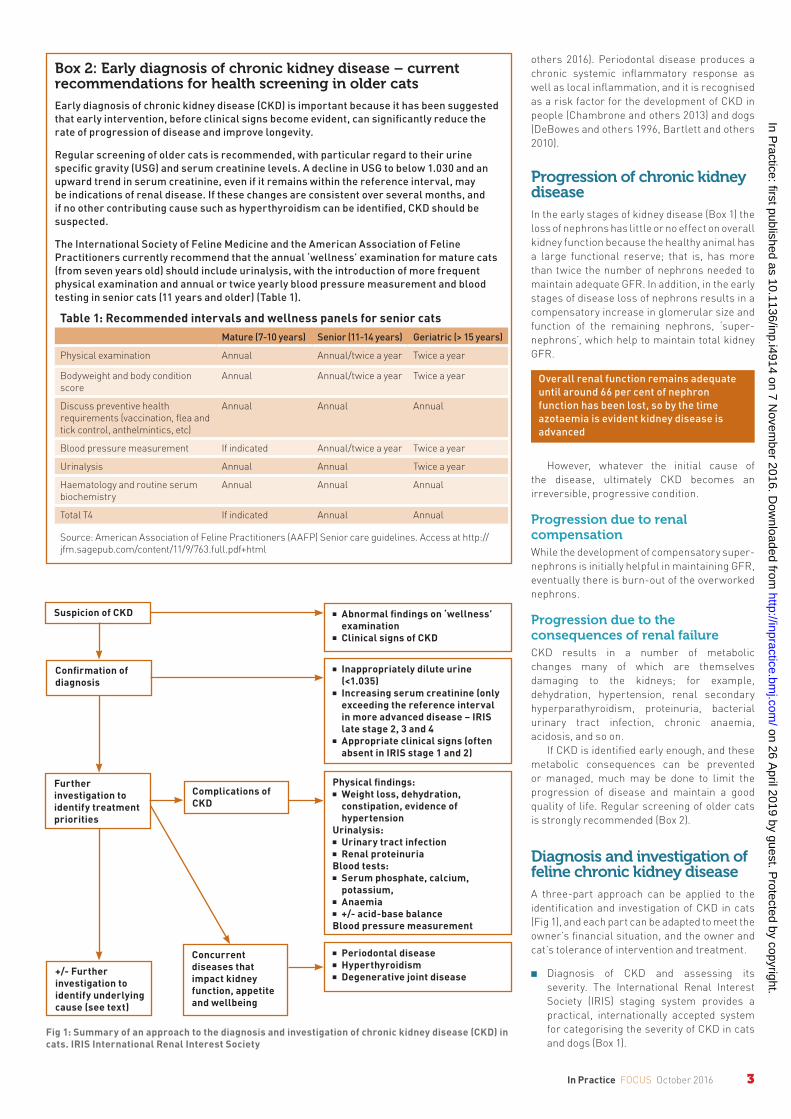
Diagnosis and investigation of feline chronic kidney diseaseA three-part approach can be applied to the identification and investigation of CKD in cats (Fig 1), and each part can be adapted to meet the owner’s financial situation, and the owner and cat’s tolerance of intervention and treatment.
■■ Diagnosis of CKD and assessing its severity. The International Renal Interest Society (IRIS) staging system provides a practical, internationally accepted system for categorising the severity of CKD in cats and dogs (Box 1).
Fig 1: Summary of an approach to the diagnosis and investigation of chronic kidney disease (CKD) in cats. IRIS International Renal Interest Society
Suspicion of CKD
Confirmation of diagnosis
Further investigation to identify treatment priorities
+/- Further investigation to identify underlying cause (see text)
Complications of CKD
Concurrent diseases that impact kidney function, appetite and wellbeing
■ Abnormal findings on ‘wellness’ examination
■ Clinical signs of CKD
■ Inappropriately dilute urine (<1.035)
■ Increasing serum creatinine (only exceeding the reference interval in more advanced disease – IRIS late stage 2, 3 and 4
■ Appropriate clinical signs (often absent in IRIS stage 1 and 2)
Physical findings:■ Weight loss, dehydration,
constipation, evidence of hypertension
Urinalysis:■ Urinary tract infection■ Renal proteinuriaBlood tests:■ Serum phosphate, calcium,
potassium, ■ Anaemia■ +/- acid-base balanceBlood pressure measurement
■ Periodontal disease■ Hyperthyroidism■ Degenerative joint disease
Box 2: Early diagnosis of chronic kidney disease – current recommendations for health screening in older cats
Early diagnosis of chronic kidney disease (CKD) is important because it has been suggested that early intervention, before clinical signs become evident, can significantly reduce the rate of progression of disease and improve longevity.
Regular screening of older cats is recommended, with particular regard to their urine specific gravity (USG) and serum creatinine levels. A decline in USG to below 1.030 and an upward trend in serum creatinine, even if it remains within the reference interval, may be indications of renal disease. If these changes are consistent over several months, and if no other contributing cause such as hyperthyroidism can be identified, CKD should be suspected.
The International Society of Feline Medicine and the American Association of Feline Practitioners currently recommend that the annual ‘wellness’ examination for mature cats (from seven years old) should include urinalysis, with the introduction of more frequent physical examination and annual or twice yearly blood pressure measurement and blood testing in senior cats (11 years and older) (Table 1).
Table 1: Recommended intervals and wellness panels for senior catsMature (7-10 years) Senior (11-14 years) Geriatric (> 15 years)
Physical examination Annual Annual/twice a year Twice a year
Bodyweight and body condition score
Annual Annual/twice a year Twice a year
Discuss preventive health requirements (vaccination, flea and tick control, anthelmintics, etc)
Annual Annual Annual
Blood pressure measurement If indicated Annual/twice a year Twice a year
Urinalysis Annual Annual Twice a year
Haematology and routine serum biochemistry
Annual Annual Annual
Total T4 If indicated Annual Annual
Source: American Association of Feline Practitioners (AAFP) Senior care guidelines. Access at http://jfm.sagepub.com/content/11/9/763.full.pdf+html
Overall renal function remains adequate until around 66 per cent of nephron function has been lost, so by the time azotaemia is evident kidney disease is advanced
2-9 Cannon.indd 3 16/09/2016 15:05
on 26 April 2019 by guest. P
rotected by copyright.http://inpractice.bm
j.com/
In Practice: first published as 10.1136/inp.i4914 on 7 N
ovember 2016. D
ownloaded from
4 In Practice FOCUS October 2016
■■ Wider assessment to identify the adverse consequences of the CKD which will themselves impact on future progression of disease. This allows a treatment plan to be developed to meet the individual cat’s needs.
■■ Consider further investigation into the underlying cause of the CKD.
In addition, identifying and addressing concurrent diseases that impact on the kidneys, the cat’s appetite and/or its overall quality of life is also important and may alter treatment priorities and medication or diet choices.
Diagnosis of chronic kidney disease and applying the IRIS staging systemDiagnosis of CKD is currently based on identifying a combination of:
■■ Compatible clinical signs over a period of months;
■■ Persistently poorly concentrated urine; and
■■ Persistent evidence of reduced GFR, currently by measurement of serum creatinine which is used as an indirect marker of GFR. Serum symmetric dimethylarginine (SDMA) is another indirect marker of GFR which may provide additional information (see below).
Clinical signs of chronic kidney diseaseCKD is a progressive disease and clinical signs become evident as disease becomes more advanced.
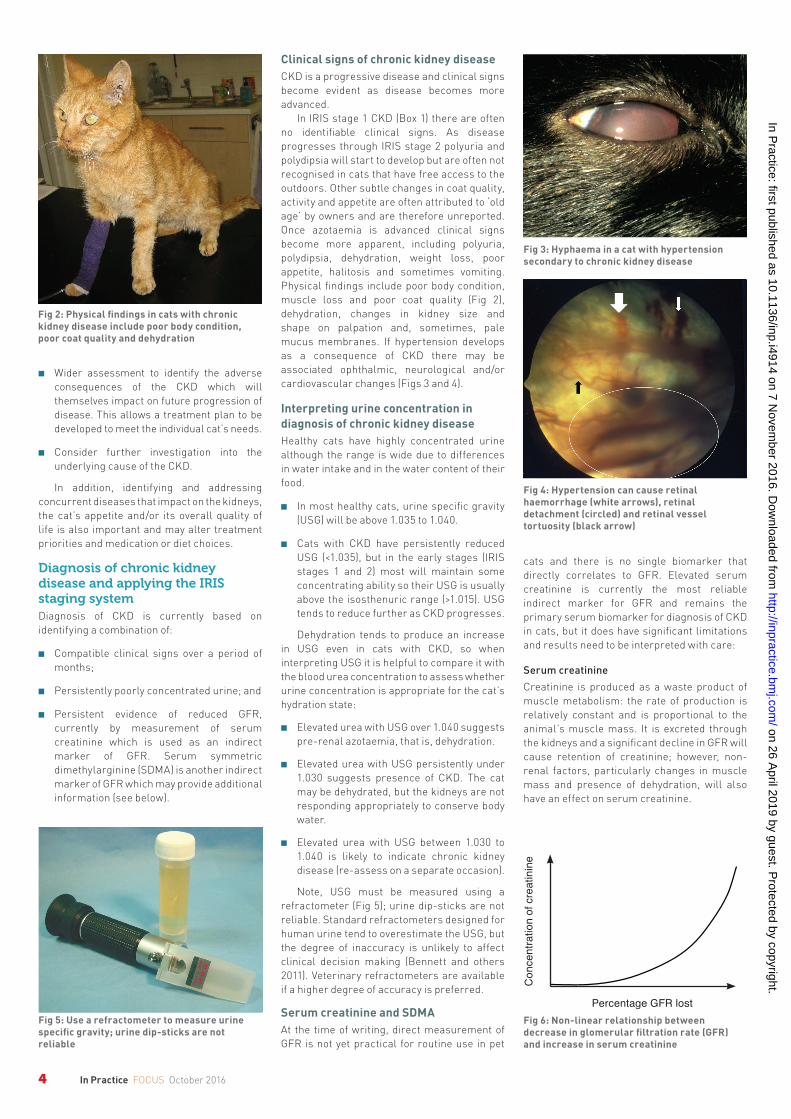
In IRIS stage 1 CKD (Box 1) there are often no identifi able clinical signs. As disease progresses through IRIS stage 2 polyuria and polydipsia will start to develop but are often not recognised in cats that have free access to the outdoors. Other subtle changes in coat quality, activity and appetite are often attributed to ‘old age’ by owners and are therefore unreported. Once azotaemia is advanced clinical signs become more apparent, including polyuria, polydipsia, dehydration, weight loss, poor appetite, halitosis and sometimes vomiting. Physical fi ndings include poor body condition, muscle loss and poor coat quality (Fig 2), dehydration, changes in kidney size and shape on palpation and, sometimes, pale mucus membranes. If hypertension develops as a consequence of CKD there may be associated ophthalmic, neurological and/or cardiovascular changes (Figs 3 and 4).
Interpreting urine concentration in diagnosis of chronic kidney diseaseHealthy cats have highly concentrated urine although the range is wide due to differences in water intake and in the water content of their food.
■■ In most healthy cats, urine specifi c gravity (USG) will be above 1.035 to 1.040.
■■ Cats with CKD have persistently reduced USG (<1.035), but in the early stages (IRIS stages 1 and 2) most will maintain some concentrating ability so their USG is usually above the isosthenuric range (>1.015). USG tends to reduce further as CKD progresses.
Dehydration tends to produce an increase in USG even in cats with CKD, so when interpreting USG it is helpful to compare it with the blood urea concentration to assess whether urine concentration is appropriate for the cat’s hydration state:
■■ Elevated urea with USG over 1.040 suggests pre-renal azotaemia, that is, dehydration.
■■ Elevated urea with USG persistently under 1.030 suggests presence of CKD. The cat may be dehydrated, but the kidneys are not responding appropriately to conserve body water.
■■ Elevated urea with USG between 1.030 to 1.040 is likely to indicate chronic kidney disease (re-assess on a separate occasion).
Note, USG must be measured using a refractometer (Fig 5); urine dip-sticks are not reliable. Standard refractometers designed for human urine tend to overestimate the USG, but the degree of inaccuracy is unlikely to affect clinical decision making (Bennett and others 2011). Veterinary refractometers are available if a higher degree of accuracy is preferred.
Serum creatinine and SDMA At the time of writing, direct measurement of GFR is not yet practical for routine use in pet
cats and there is no single biomarker that directly correlates to GFR. Elevated serum creatinine is currently the most reliable indirect marker for GFR and remains the primary serum biomarker for diagnosis of CKD in cats, but it does have signifi cant limitations and results need to be interpreted with care:
Serum creatinineCreatinine is produced as a waste product of muscle metabolism: the rate of production is relatively constant and is proportional to the animal’s muscle mass. It is excreted through the kidneys and a signifi cant decline in GFR will cause retention of creatinine; however, non-renal factors, particularly changes in muscle mass and presence of dehydration, will also have an effect on serum creatinine.
Fig 4: Hypertension can cause retinal haemorrhage (white arrows), retinal detachment (circled) and retinal vessel tortuosity (black arrow)
Fig 6: Non-linear relationship between decrease in glomerular fi ltration rate (GFR) and increase in serum creatinine
Fig 3: Hyphaema in a cat with hypertension secondary to chronic kidney disease
Fig 2: Physical fi ndings in cats with chronic kidney disease include poor body condition, poor coat quality and dehydration
Fig 5: Use a refractometer to measure urine specifi c gravity; urine dip-sticks are not reliable
Con
cent
ratio
n of
cre
atin
ine
Percentage GFR lost
2-9 Cannon.indd 4 16/09/2016 15:05
on 26 April 2019 by guest. P
rotected by copyright.http://inpractice.bm
j.com/
In Practice: first published as 10.1136/inp.i4914 on 7 N
ovember 2016. D
ownloaded from

5In Practice FOCUS October 2016
The relationship between muscle mass and serum creatinine can be a particular problem when interpreting results in elderly cats with CKD. In these cats, muscle mass may be significantly reduced such that their ‘normal’ range for creatinine may be lower than the population reference interval.
Additionally, the relationship between reduction in GFR and elevation in creatinine is not linear; initially a large drop in GFR produces only a small increase in creatinine, while later in disease a small change in GFR has a much larger effect (Fig 6). This means that for apparently healthy cats (IRIS stage 1 and early stage 2) even a small increase in serum creatinine may indicate a significant deterioration in kidney function. Serial measurements for one animal are therefore more useful than a single measurement and an upward trend in creatinine in an individual cat may reflect deterioration in kidney function even though the creatinine level remains within the population reference interval.
Serum ureaWhile renal azotaemia is a potential cause of elevated serum urea it is a less reliable marker for CKD than creatinine because it is affected by a wide range of non-renal factors.
Urea is produced in the liver during amino acid deamination but the rate of production varies widely with dietary protein intake and
rate of protein catabolism. Urea is excreted by the kidneys but has a functional role in the maintenance of renal urine concentrating ability, so excretion is highly variable depending on body fluid balance. Dehydration stimulates renal reabsorption of urea to allow increased reabsorption of water from the glomerular filtrate.
Urea can be significantly increased due to dehydration, reduced GFR, increased protein catabolism (conditions causing weight loss), a recent high protein meal and the presence of gastrointestinal bleeding. Additionally, as with creatinine the relationship between a decline in GFR and an elevation in urea is non-linear such that small changes in early CKD are more significant than large changes in more advanced disease.
Symmetric dimethylarginine (SDMA)Serum SDMA has recently been validated for use as a biomarker for CKD in cats and dogs (Braff and others 2014, Hall and others 2014), and has now become commercially available in the UK (Idexx).
SDMA is elevated in cats with CKD, with the same non-linear relationship to GFR as creatinine and urea. However, it appears that elevation in SDMA may occur earlier in the course of disease, so it may exceed its reference interval before creatinine, potentially allowing earlier confirmation of the diagnosis of CKD.
A further advantage of SDMA over serum creatinine is that it is not affected by loss of muscle mass, so it may be helpful in supporting a diagnosis of CKD in cats with low muscle mass whose serum creatinine level may be lower than expected. However, in people SDMA is elevated by a number of non-renal diseases such as sepsis, cardiac disease and hepatic disease (Koch and others 2013) and further research is needed into the specificity of raised SDMA in cats.
Based on current evidence the IRIS staging system has recently been adapted to include cautious guidelines on the interpretation of SDMA in cats with CKD (Box 3).
Further investigation of chronic kidney diseaseOnce CKD has been identified it is important to investigate further with the aims of:
■■ Gathering information that will be prognostically useful;
■■ Developing a treatment plan tailored to the individual, aimed at addressing current clinical signs but also, where possible, at slowing down the rate of progression of disease; and
■■ Identifying any concurrent diseases that may need additional treatment.
In all cases further investigations should therefore include the following.
Full physical examinationWith particular reference to common consequences and complications of CKD as well as to identifying comorbidities that may need treatment:
Bodyweight and body condition scoreIdentifying and rectifying loss of muscle mass and body condition is important. Underweight cats with poor appetite may benefit from anti-nausea and appetite stimulant medications. If protein-restricted diets are used close attention will be required to ensure that protein and calorie intake is adequate.
Dehydration Most cats with CKD are subclinically dehydrated due to polyuria with incomplete compensatory polydipsia. If there is physical evidence of dehydration (Table 2), measures to restore fluid balance will be a priority.
Table 2: Physical signs of dehydrationPercentage dehydration
Physical findings
<5 No physical evidence of dehydration, but history suggests reduced fluid intake or increased fluid loss
5 to 6 Dry oral mucous membranes, subtle reduction in skin elasticity
6 to 8 Mild to moderate reduction in skin elasticity, some increase in capillary refill time, dry oral mucous membranes. Possibly eyes sunken in orbits
10 to 12 Marked reduction in skin elasticity, capillary refill time 2-3 seconds, dry mucous membranes, eyes sunken in orbits. Possibly tachycardia, cool extremities, rapid and weak pulses
12 to 15 Severe signs of shock or dehydration, capillary refill time >3 seconds, very severe debilitation
>15 Incompatible with life
A decline in USG to below 1.030 and an upward trend in serum creatinine, even if it remains within the reference interval, may be indicative of renal disease. If these changes are consistent over several months, and if no other contributing cause such as hyperthyroidism can be identified, CKD should be suspected
Box 3: International Renal Interest Society (IRIS) chronic kidney disease guidelines on the interpretation of symmetric dimethylarginine
‘IRIS chronic kidney disease (CKD) staging is based currently on fasting blood creatinine concentrations, but there are indications that symmetric dimethylarginine (SDMA) concentrations in blood plasma or serum may be a more sensitive biomarker of renal function. Accordingly, if blood SDMA concentrations are known, some modification to the guidelines might be considered, as follows:
• A persistent increase in SDMA above 14 μg/dl suggests reduced renal function and may be a reason to consider a . . . cat with creatinine values <1.6 mg/dl as IRIS CKD stage 1.
• In IRIS CKD stage 2 patients with low body condition scores, SDMA ≥25 μg/dl may indicate the degree of renal dysfunction has been underestimated. Consider treatment recommendations listed under IRIS CKD stage 3 for this patient.
• In IRIS CKD stage 3 patients with low body condition scores, SDMA ≥45 μg/dl may indicate the degree of renal dysfunction has been underestimated. Consider treatment recommendations listed under IRIS CKD stage 4 for this patient.
These comments are preliminary and based on early data from the use of SDMA in veterinary patients. We expect them to be updated as the veterinary profession gains further experience using SDMA alongside creatinine, the long-established marker in diagnosis and monitoring of canine and feline CKD.’
Source: www.iris-kidney.com. Accessed August 3, 2016
2-9 Cannon.indd 5 16/09/2016 15:05
on 26 April 2019 by guest. P
rotected by copyright.http://inpractice.bm
j.com/
In Practice: first published as 10.1136/inp.i4914 on 7 N
ovember 2016. D
ownloaded from
6 In Practice FOCUS October 2016
Dental disease Periodontal disease is common in older cats and oral pain can contribute to reduced appetite and weight loss. Additionally, the presence of moderate or severe periodontal disease has been identifi ed as a risk factor for development of CKD in cats (Finch and others 2016), dogs (DeBowes and others 1996, Bartlett and others 2010) and people (Chambrone and others 2013). Treatment of periodontal disease is important and increased age and the presence of CKD should not preclude its treatment, although particular attention to maintaining fl uid balance, body temperature and blood pressure will be required during anaesthesia in these cases.
ConstipationMild, moderate or severe constipation is common in older cats, especially those with CKD. Dehydration, muscle weakness and hindlimb joint pain are common contributing factors that may need treatment, and additional use of stool softeners and laxatives may be required.
Degenerative joint diseaseMore than 65 per cent of cats over 12 years of age have radiographic evidence of osteoarthritis (Hardie and others 2002). Chronic pain contributes to reduced appetite, reduced activity, less frequent use of the litter tray, reduced grooming behaviour and a general decline in quality of life. Cats with stable CKD that are eating and are well hydrated may benefi t from treatment with a low dose of meloxicam (Gowan and others 2011), and where this is contraindicated other treatment modalities such as joint nutraceuticals, pentosan polysulfate injections, acupuncture and analgesics, such as gabapentin, tramadol or buprenorphine, should be considered.
Signs of anaemiaMild to moderate non-regenerative anaemia is a potential complication of advanced CKD which can contribute signifi cantly to reduced activity and reduced wellbeing. Effective management can signifi cantly improve quality of life.
Signs of hyperthyroidismCKD and hyperthyroidism commonly occur concurrently and treatment of both diseases is important to maximise longevity and improve quality of life.
UrinalysisRoutine urinalysis includes measurement of USG (see previously), dip-stick analysis and examination of urine sediment.
Bacterial culture and sensitivity Bacterial culture and sensitivity should also be included whenever possible because while urinary tract infections (UTIs) are rare in healthy cats, they are a common complication of CKD, especially in female cats (Fig 7). One recent study identifi ed positive urine cultures in 30 per cent of cats with CKD (White and others 2013). In some cases these infections produce signs of lower urinary tract discomfort, inappropriate urination, haematuria, urinary incontinence and/or abnormal urine odour, but in the majority of cases, 72 per cent in the previously mentioned study, they are asymptomatic and will only be identifi ed by regular routine screening of urine. UTIs that are causing clinical signs or active urine sediment should be treated in all cases. In elderly human patients treatment for asymptomatic positive urine cultures with inactive sediment is no longer recommended, but whether this approach should be extrapolated to the feline population is currently unknown.
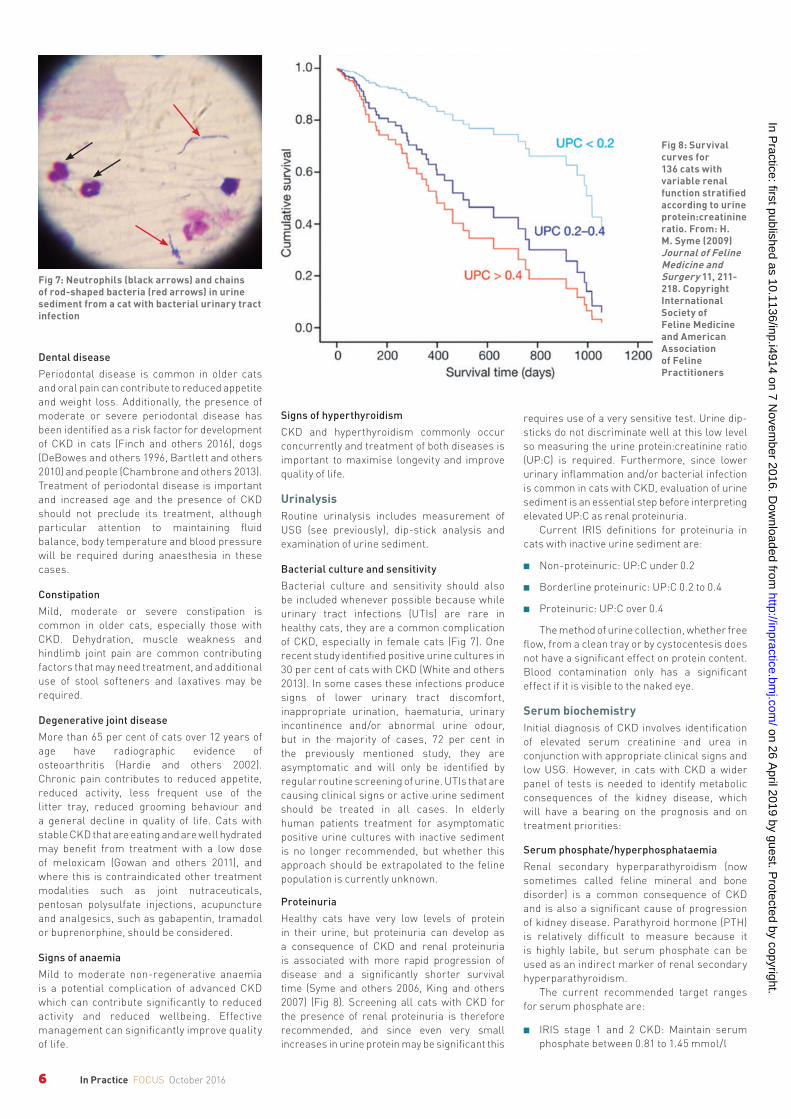
ProteinuriaHealthy cats have very low levels of protein in their urine, but proteinuria can develop as a consequence of CKD and renal proteinuria is associated with more rapid progression of disease and a signifi cantly shorter survival time (Syme and others 2006, King and others 2007) (Fig 8). Screening all cats with CKD for the presence of renal proteinuria is therefore recommended, and since even very small increases in urine protein may be signifi cant this
requires use of a very sensitive test. Urine dip-sticks do not discriminate well at this low level so measuring the urine protein:creatinine ratio (UP:C) is required. Furthermore, since lower urinary infl ammation and/or bacterial infection is common in cats with CKD, evaluation of urine sediment is an essential step before interpreting elevated UP:C as renal proteinuria.
Current IRIS defi nitions for proteinuria in cats with inactive urine sediment are:
■■ Non-proteinuric: UP:C under 0.2
■■ Borderline proteinuric: UP:C 0.2 to 0.4
■■ Proteinuric: UP:C over 0.4
The method of urine collection, whether free fl ow, from a clean tray or by cystocentesis does not have a signifi cant effect on protein content. Blood contamination only has a signifi cant effect if it is visible to the naked eye.
Serum biochemistryInitial diagnosis of CKD involves identifi cation of elevated serum creatinine and urea in conjunction with appropriate clinical signs and low USG. However, in cats with CKD a wider panel of tests is needed to identify metabolic consequences of the kidney disease, which will have a bearing on the prognosis and on treatment priorities:
Serum phosphate/hyperphosphataemiaRenal secondary hyperparathyroidism (now sometimes called feline mineral and bone disorder) is a common consequence of CKD and is also a signifi cant cause of progression of kidney disease. Parathyroid hormone (PTH) is relatively diffi cult to measure because it is highly labile, but serum phosphate can be used as an indirect marker of renal secondary hyperparathyroidism.
The current recommended target ranges for serum phosphate are:
■■ IRIS stage 1 and 2 CKD: Maintain serum phosphate between 0.81 to 1.45 mmol/l
Fig 8: Survival curves for 136 cats with variable renal function stratifi ed according to urine protein:creatinine ratio. From: H. M. Syme (2009) Journal of Feline Medicine and Surgery 11, 211-218. Copyright International Society of Feline Medicine and American Association of Feline Practitioners
Fig 7: Neutrophils (black arrows) and chains of rod-shaped bacteria (red arrows) in urine sediment from a cat with bacterial urinary tract infection
2-9 Cannon.indd 6 16/09/2016 15:05
on 26 April 2019 by guest. P
rotected by copyright.http://inpractice.bm
j.com/
In Practice: first published as 10.1136/inp.i4914 on 7 N
ovember 2016. D
ownloaded from
7In Practice FOCUS October 2016
■■ IRIS stage 3 CKD: Maintain serum phosphate between 0.81 to 1.61 mmol/l
■■ IRIS stage 4 CKD: Maintain serum phosphate between 0.81 to 1.94 mmol/l
Note, these levels of phosphate fall within most laboratories reference intervals.
Calcium Serum calcium may be normal, subnormal or elevated in cats with CKD. Hypercalcaemia is a potential cause of kidney damage but can also occur as a consequence of CKD. In addition, restricting phosphate intake to manage renal secondary hyperparathyroidism causes hypercalcaemia in a small proportion of cats. Serum calcium should therefore be monitored, ideally using an ionised calcium assay since some cats with normal total calcium have significantly elevated ionised calcium.
PotassiumIn CKD there is both increased urinary loss of potassium and reduced oral intake if appetite is poor. Metabolic acidosis also contributes to serum hypokalaemia due to H+/K+ ion exchange which drives acidifying H+ ions intracellularly. Hypokalaemia is therefore common in affected cats and may cause muscle weakness and a stilted gait, which may in turn contribute to constipation and lethargy. Conversely in advanced (stage 4) CKD potassium may be elevated due to failure of renal excretion.
Routine haematologyAnaemia is a common complication of advanced CKD, caused by a number of factors:
■■ Uraemia damages red blood cells reducing their circulating life span;
■■ Uraemia may also lead to gastrointestinal ulcers, causing bleeding. Initially the lost red blood cells are replaced but in the longer term iron deficiency can develop, especially if the cat has poor food intake;
■■ Reduced erythropoietin secretion from the damaged kidney leads to an inability to replace red blood cells as they reach the end of the end of their life span; and
■■ Poor food intake, leading to a negative protein and energy balance contributes to the problem.
The anaemia is usually non-regenerative and slowly progressive. If there is concurrent iron deficiency there may be microcytosis and hypochromia.
Treatment of anaemia can produce a marked improvement in attitude, appetite and activity, improving both quality of life and longevity.
Blood pressure measurement and ophthalmic examinationHypertension is a common problem in cats with CKD, although the reported incidence varies widely between different studies ranging from 19 per cent to 65 per cent (Stiles and others 1994, Syme and others 2002). The
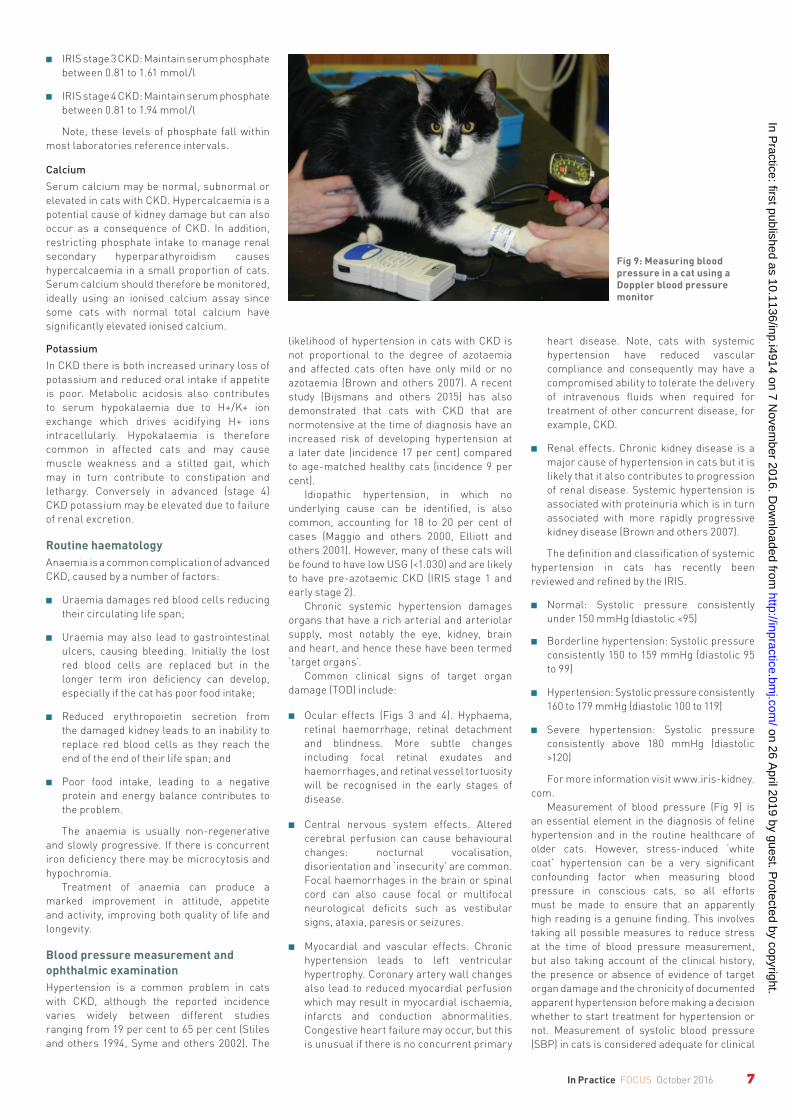
Fig 9: Measuring blood pressure in a cat using a Doppler blood pressure monitor
likelihood of hypertension in cats with CKD is not proportional to the degree of azotaemia and affected cats often have only mild or no azotaemia (Brown and others 2007). A recent study (Bijsmans and others 2015) has also demonstrated that cats with CKD that are normotensive at the time of diagnosis have an increased risk of developing hypertension at a later date (incidence 17 per cent) compared to age-matched healthy cats (incidence 9 per cent).
Idiopathic hypertension, in which no underlying cause can be identified, is also common, accounting for 18 to 20 per cent of cases (Maggio and others 2000, Elliott and others 2001). However, many of these cats will be found to have low USG (<1.030) and are likely to have pre-azotaemic CKD (IRIS stage 1 and early stage 2).
Chronic systemic hypertension damages organs that have a rich arterial and arteriolar supply, most notably the eye, kidney, brain and heart, and hence these have been termed ‘target organs’.
Common clinical signs of target organ damage (TOD) include:
■■ Ocular effects (Figs 3 and 4). Hyphaema, retinal haemorrhage, retinal detachment and blindness. More subtle changes including focal retinal exudates and haemorrhages, and retinal vessel tortuosity will be recognised in the early stages of disease.
■■ Central nervous system effects. Altered cerebral perfusion can cause behavioural changes: nocturnal vocalisation, disorientation and ‘insecurity’ are common. Focal haemorrhages in the brain or spinal cord can also cause focal or multifocal neurological deficits such as vestibular signs, ataxia, paresis or seizures.
■■ Myocardial and vascular effects. Chronic hypertension leads to left ventricular hypertrophy. Coronary artery wall changes also lead to reduced myocardial perfusion which may result in myocardial ischaemia, infarcts and conduction abnormalities. Congestive heart failure may occur, but this is unusual if there is no concurrent primary
heart disease. Note, cats with systemic hypertension have reduced vascular compliance and consequently may have a compromised ability to tolerate the delivery of intravenous fluids when required for treatment of other concurrent disease, for example, CKD.
■■ Renal effects. Chronic kidney disease is a major cause of hypertension in cats but it is likely that it also contributes to progression of renal disease. Systemic hypertension is associated with proteinuria which is in turn associated with more rapidly progressive kidney disease (Brown and others 2007).
The definition and classification of systemic hypertension in cats has recently been reviewed and refined by the IRIS.
■■ Normal: Systolic pressure consistently under 150 mmHg (diastolic <95)
■■ Borderline hypertension: Systolic pressure consistently 150 to 159 mmHg (diastolic 95 to 99)
■■ Hypertension: Systolic pressure consistently 160 to 179 mmHg (diastolic 100 to 119)
■■ Severe hypertension: Systolic pressure consistently above 180 mmHg (diastolic >120)
For more information visit www.iris-kidney.com.
Measurement of blood pressure (Fig 9) is an essential element in the diagnosis of feline hypertension and in the routine healthcare of older cats. However, stress-induced ‘white coat’ hypertension can be a very significant confounding factor when measuring blood pressure in conscious cats, so all efforts must be made to ensure that an apparently high reading is a genuine finding. This involves taking all possible measures to reduce stress at the time of blood pressure measurement, but also taking account of the clinical history, the presence or absence of evidence of target organ damage and the chronicity of documented apparent hypertension before making a decision whether to start treatment for hypertension or not. Measurement of systolic blood pressure (SBP) in cats is considered adequate for clinical
2-9 Cannon.indd 7 16/09/2016 15:05
on 26 April 2019 by guest. P
rotected by copyright.http://inpractice.bm
j.com/
In Practice: first published as 10.1136/inp.i4914 on 7 N
ovember 2016. D
ownloaded from
8 In Practice FOCUS October 2016
assessment, as isolated diastolic hypertension appears to be rare.
The International Society of Feline medicine (ISFM), in association with Ceva Animal Health, has recently published a set of ‘Practical Recommendations on the Indirect Measurement of Blood Pressure in Conscious Cats’ (see Useful resources). These recommendations provide a wealth of practical information aimed at making blood pressure measurement in cats achievable and reliable.
Blood gas analysisIf available, blood gas analysis to determine acid-base status is recommended in cats with more advanced CKD (IRIS stages 3 and 4) as metabolic acidosis is common in these cases.
Concurrent diseaseAdditional blood tests may be needed to identify concurrent disease depending on the presenting signs, for example, total T4, serum folate and cobalamin, retrovirus testing, and so on.
Consider further investigation into the primary cause of kidney diseaseIn the majority of elderly cats with CKD the primary cause of the problem cannot be identified. However, in selected cases further investigation may identify the underlying cause of CKD, which may be helpful to owners and in some cases may open avenues of treatment to address the primary problem. In general, seeking a primary cause is more likely to be rewarding in younger cats and in cats with enlargement of one or both kidneys.
In younger cats presenting with CKD the clinical history and/or further investigations may suggest:
■■ An inherited cause, for example, polycystic kidney disease in Persian and related breeds or renal amyloidosis in Siamese cats.
■■ Chronic kidney disease secondary to previous acute kidney injury (AKI), for example, previous access to toxins such
as lily plants, previous episodes of urethral obstruction or previous blunt abdominal trauma.
■■ Nephropathy secondary to hypercalcaemia.
In cats with unilateral or bilateral kidney enlargement kidney ultrasound is often rewarding and may indicate:
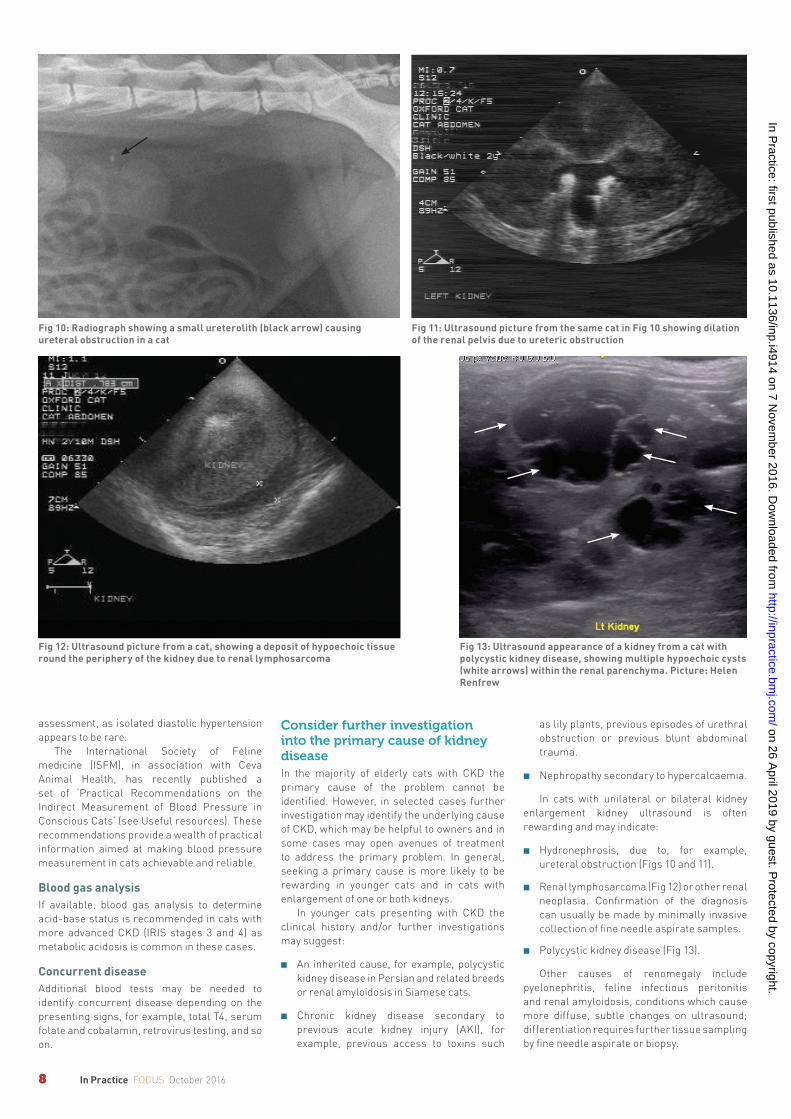
■■ Hydronephrosis, due to, for example, ureteral obstruction (Figs 10 and 11).
■■ Renal lymphosarcoma (Fig 12) or other renal neoplasia. Confirmation of the diagnosis can usually be made by minimally invasive collection of fine needle aspirate samples.
■■ Polycystic kidney disease (Fig 13).
Other causes of renomegaly include pyelonephritis, feline infectious peritonitis and renal amyloidosis, conditions which cause more diffuse, subtle changes on ultrasound; differentiation requires further tissue sampling by fine needle aspirate or biopsy.
Fig 13: Ultrasound appearance of a kidney from a cat with polycystic kidney disease, showing multiple hypoechoic cysts (white arrows) within the renal parenchyma. Picture: Helen Renfrew
Fig 12: Ultrasound picture from a cat, showing a deposit of hypoechoic tissue round the periphery of the kidney due to renal lymphosarcoma
Fig 11: Ultrasound picture from the same cat in Fig 10 showing dilation of the renal pelvis due to ureteric obstruction
Fig 10: Radiograph showing a small ureterolith (black arrow) causing ureteral obstruction in a cat
2-9 Cannon.indd 8 16/09/2016 15:05
on 26 April 2019 by guest. P
rotected by copyright.http://inpractice.bm
j.com/
In Practice: first published as 10.1136/inp.i4914 on 7 N
ovember 2016. D
ownloaded from

9In Practice FOCUS October 2016
ConclusionChronic kidney disease is a very common problem in older cats. In most cases the primary cause is unknown, and in all cases pre-existing kidney damage at the time of diagnosis will be irreversible. Nevertheless, early diagnosis and appropriate treatment can have a very significant positive effect on both quality of life and longevity. Recent improvements in our understanding of the pathophysiology of CKD have led to the development of clear and practical, evidence-based advice and guidelines on the diagnosis, investigation and management of CKD in all its stages.
Key points
■■ Chronic kidney disease is estimated to affect around 30 per cent of cats that are over 12 years of age (Lulich and others 1992).
■■ Early diagnosis and management of CKD can slow down the progression of disease.
■■ Reduction in USG (<1.035) usually precedes azotaemia and is an important early indicator of CKD.
■■ Once CKD has been identified, further investigations are required and will identify the current treatment needs of the individual cat.
ReferencesBARTLETT, P. C., VAN BUREN, J. W., BARTLETT, A. D. & ZHOU, C. (2010) Case-control study of risk factors associated with feline and canine chronic kidney disease. Veterinary Medicine International doi: 10.4061/2010/957570BENNETT, A. D., MCKNIGHT, G. E., DODKIN, S. J., SIMPSON, K. E., SCHWARTZ, A. M. & GUNN-MOORE, D. A. (2011) Comparison of digital and optical hand-held refractometers for the measurement of feline urine specific gravity. Journal of Feline Medicine and Surgery 13, 152-154BIJSMANS, E. S., JEPSON, R. E., CHANG, Y. M., SYME, H. M. & ELLIOTT, J. (2015) Changes in systolic blood pressure over time in healthy cats and cats with chronic kidney disease. Journal of Veterinary Internal Medicine 29, 855-861BRAFF, J., OBARE, E., YERRAMILLI, M., ELLIOTT, J. & YERRAMILLI, M. (2014) Relationship between serum symmetric dimethylarginine concentration and glomerular filtration rate in cats. Journal of Veterinary Internal Medicine 28, 1699-1701BROWN, S., ATKINS, C., BAGLEY, R., CARR, A., COWGILL, L., DAVIDSON, M. & OTHERS (2007) Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. Journal of Veterinary Internal Medicine 21, 542-558 CHAMBRONE, L., FOZ, A. M., GUGLIELMETTI, M. R., PANNUTI, C. M., ARTESE, H. P., FERES, M. & ROMITO, G. A. (2013) Periodontitis and chronic kidney disease: a systematic review of the association of diseases and the effect of periodontal
treatment on estimated glomerular filtration rate. Journal of Clinical Periodontology 40, 443-456 DEBOWES, L. J., MOSIER, D., LOGAN, E., HARVEY, C. E., LOWRY, S. & RICHARDSON, D. C. (1996) Association of periodontal disease and histologic lesions in multiple organs from 45 dogs. Journal of Veterinary Dentistry 13, 57-60ELLIOTT, J., BARBER, P. J., SYME, H. M., RAWLINGS, J. M. & MARKWELL, P. J. (2001) Feline hypertension: clinical findings and response to antihypertensive treatment in 30 cases. Journal of Small Animal Practice 42, 122-129FINCH, N. C., SYME, H. M. & ELLIOTT, J. (2016) Risk factors for development of chronic kidney disease in cats. Journal of Veterinary Internal Medicine 30, 602-610 FURUYA, T., SASSA, Y., OMATSU, T., NAGAI, M., FUKUSHIMA, R., SHIBUTANI, M., YAMAGUCHI, T., UEMATSU, Y., SHIROTA, K. & MIZUTANI, T. (2014) Existence of feline morbillivirus infection in Japanese cat populations. Archives of Virology 159, 371-373FURUYA, T., WACHI, A., SASSA, Y., OMATSU, T., NAGAI, M., FUKUSHIMA, R. & OTHERS (2016) Quantitative PCR detection of feline morbillivirus in cat urine samples. Journal of Veterinary Medical Science 77, 1701-1703GOWAN, R. A., LINGARD, A. E., JOHNSTON, L., STANSEN, W., BROWN, S. A. & MALIK, R. (2011) Retrospective case-control study of the effects of long-term dosing with meloxicam on renal function in aged cats with degenerative joint disease. Journal of Feline Medicine and Surgery 13, 752-761HALL, J. A., YERRAMILLI, M., OBARE, E., YERRAMILLI, M. & JEWELL, D. E. (2014) Comparison of serum concentrations of symmetric dimethylarginine and creatinine as kidney function biomarkers in cats with chronic kidney disease. Journal of Veterinary Internal Medicine 28, 1676-1683HARDIE, E. M., ROE, S. C. & MARTIN, F. R. (2002) Radiographic evidence of degenerative joint disease in geriatric cats: 100 cases (1994-1997). Journal of the American Veterinary Medical Association 220, 628-632KING, J. N., TASKER, S., GUNN-MOORE, D. A., STREHLAU, G. & BENRIC (BENAZEPRIL IN RENAL INSUFFICIENCY IN CATS) STUDY GROUP (2007) Prognostic factors in cats with chronic kidney disease. Journal of Veterinary Internal Medicine 21, 906-916 KOCH, A., WEISKIRCHEN, R., BRUENSING, J., DÜCKERS, H., BUENDGENS, L., KUNZE, J., MATTHES, M., LUEDDE, T., TRAUTWEIN, C. & TACKE, F. (2013) Regulation and prognostic relevance of symmetric dimethylarginine serum concentrations in critical illness and sepsis. Mediators of Inflammation doi: 10.1155/2013/413826LAPPIN, M. R., BASARABA, R. J. & JENSEN, W. A. (2006) Interstitial nephritis in cats inoculated with Crandell Rees feline kidney cell lysates. Journal of Feline Medicine and Surgery 8, 353-356LAPPIN, M. R., JENSEN, W. A., JENSEN, T. D., BASARABA, R. J., BROWN, C. A., RADECKI, S. V. & HAWLEY, J. R. (2005) Investigation of the induction of antibodies against Crandell-Rees feline kidney cell lysates and feline renal cell lysates after parenteral administration of vaccines against feline viral rhinotracheitis, calicivirus, and panleukopenia in
cats. American Journal of Veterinary Research 66, 506-511LULICH, J. P. OSBORNE, C. A., O’BRIEN, T. D. & POLZIN, D. J. (1992) Feline renal failure: questions, answers, questions. Compendium on Continuing Education for the Practising Veterinarian 14, 127-152MAGGIO, F., DEFRANCESCO, T. C., ATKINS, C. E., PIZZIRANI, S., GILGER, B. C. & DAVIDSON, M. G. (2000) Ocular lesions associated with systemic hypertension in cats: 69 cases (1985-1998). Journal of the American Veterinary Medical Association 217, 695-702O’NEILL, D. G., CHURCH, D. B., MCGREEVY, P. D., THOMSON, P. C. & BRODBELT, D. C.(2015) Longevity and mortality of cats attending primary care veterinary practices in England. Journal of Feline Medicine and Surgery 17, 125-133STILES, J., POLZIN, D. J. & BISTNER, S. I. (1994) The prevalence of retinopathy in cats with systemic hypertension and chronic renal failure or hyperthyroidism. Journal of the American Animal Hospital Association 30, 564-572SYME, H. M., BARBER, P. J., MARKWELL, P. J. & ELLIOTT, J. (2002) Prevalence of systolic hypertension in cats with chronic renal failure at initial evaluation. Journal of the American Veterinary Medical Association 220, 1799-1804SYME, H. M., MARKWELL, P. J., PFEIFFER, D. & ELLIOTT, J. (2006) Survival of cats with naturally occurring chronic renal failure is related to severity of proteinuria. Journal of Veterinary Internal Medicine 20, 528-535WHITE, J. D., STEVENSON, M., MALIK, R., SNOW, D. & NORRIS, J. M. (2013) Urinary tract infections in cats with chronic kidney disease. Journal of Feline Medicine and Surgery 15, 459-465WOO, P. C., LAU, S. K., WONG, B. H., FAN, R. Y., WONG, A. Y., ZHANG, A. J. & OTHERS (2012) Feline morbillivirus, a previously undescribed paramyxovirus associated with tubulointerstitial nephritis in domestic cats. Proceedings of the National Academy of Sciences of the United States of America 109, 5435-5440
Useful resourcesAMERICAN ASSOCIATION OF FELINE PRACTITIONERS (AAFP) Senior care guidelines. http://jfm.sagepub.com/content/11/9/763.full.pdf+html. Accessed September 9, 2016INTERNATIONAL RENAL INTEREST SOCIETY (IRIS) Website www.iris-kidney.comISFM Practical recommendations on the measurement of indirect blood pressure in cats. http://icatcare.org/sites/default/files/PDF/CEVA-BP-Booklets/ISFM%20BP%20recommendations%20English.pdf. Accessed September 9, 2016SPARKES, A. H., CANEY, S., CHALHOUB, S., ELLIOTT, J., FINCH, N., GAJANAYAKE, I. & OTHERS (2016) ISFM consensus guidelines on the diagnosis and management of feline chronic kidney disease. http://jfm.sagepub.com/site/Guidelines/Guidelines.xhtml. Accessed September 9, 2016
Competing interests No competing interests declared.
doi: 10.1136/inp.i4914
2-9 Cannon.indd 9 16/09/2016 15:05
on 26 April 2019 by guest. P
rotected by copyright.http://inpractice.bm
j.com/
In Practice: first published as 10.1136/inp.i4914 on 7 N
ovember 2016. D
ownloaded from