diagnosing and monitoring ventilator- associated...
TRANSCRIPT
Diagnosing and monitoring ventilator-associated pneumonia
BSAC spring meeting 23/3/2010
Mihye Lee Microbiology StR
Queen Alexandra Hospital, Portsmouth Hospitals NHS Trust
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Introduction
• Saving Lives. DoH High impact intervention No.5 : Care bundle for ventilated patients Care bundle compliance reported to IPC
• Does good care bundle compliance translate into good outcomes?
A way to measure outcome Discussion of VAP pathway
Commissioners attempting to use VAP rate as a quality performance indicator
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Controversies
• Controversies with definition and diagnosis of VAP
• Non-controversial: VAP increases mortality and length of stay
“The definition of VAP is perhaps the most subjective of the common device-related healthcare-associated
infection” The society for healthcare epidemiology of America (SHEA) and infectious diseases society of America
(IDSA), 2008
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Definitions American Thoracic Society (ATS)+IDSA, 2005:
“ VAP refers to pneumonia that arises more than 48–72 hours after endotracheal intubation.”
National Institute for Health and Clinical Excellence (NICE), 2008 : “There is no generally accepted definition of VAP in mechanically ventilated patients, but it is often defined as pneumonia that develops 48hours or more after intubation with an endotracheal or tracheostomy tube and that was, not present before intubation”
Centers for Disease Control and Prevention (CDC) : “Pneumonia that occurs in a patient who was intubated and ventilated at the time of or within 48 hours before the onset of the pneumonia.”
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Diagnostic criteria • VAP has been diagnosed by the clinical criteria
published by Johanson et al. 1972
• Sensitivity 69%a, Specificity 75%a aAlvaro Rea-Neto et al, Critical Care 2008
Presence of new or persistent infiltrates on CXR and any 2 of: - Febrile > 38.3 -leukocytosis or leucopenia (>11 or < 3.5) -Purulent tracheobronchial secretions
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Diagnostic criteria VAP can be accurately diagnosed by any one of several standard criteriab: • histopathologic examination of lung tissue either on lung biopsy or at
autopsy • rapid cavitation of a pulmonary infiltrate in the absence of cancer or
tuberculosis on CT • positive pleural fluid culture • same species with same antibiogram isolated from blood and respiratory
secretions without another identifiable source of bacteremia
bC. Glen Mayhall, Emerging Infectious Diseases, 2001
Invasive procedures Uncommon manifestations or complications of VAP Different approach is needed for the definitive diagnosis of VAP
C. Glen Mayhall, Emerging Infectious Diseases, 2001
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Diagnostic criteria
• Different strategies for diagnosing VAP • Variable sensitivities and specificities • Clinical : e.g. CPIS (sens: 72- 93%, spec: 42-85 %)
• Semi-quantitative microbiology
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
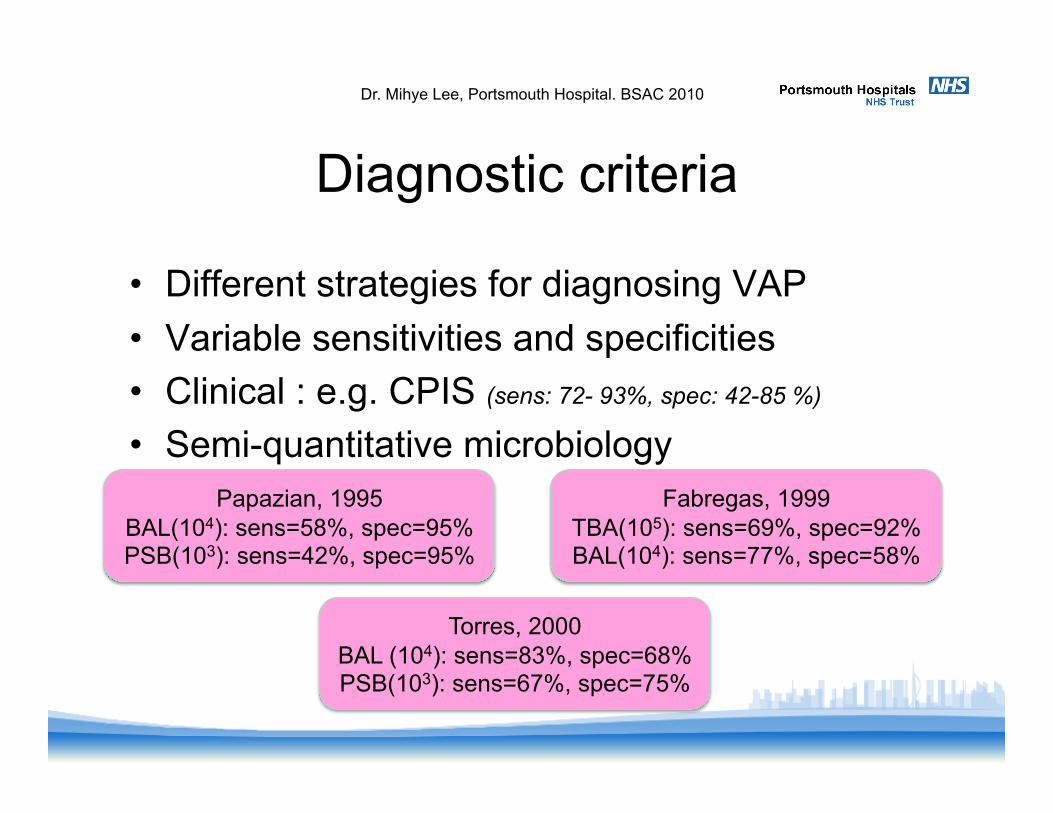
Diagnostic criteria
• Different strategies for diagnosing VAP • Variable sensitivities and specificities • Clinical : e.g. CPIS (sens: 72- 93%, spec: 42-85 %)
• Semi-quantitative microbiology
Torres, 2000 BAL (104): sens=83%, spec=68% PSB(103): sens=67%, spec=75%
Fabregas, 1999 TBA(105): sens=69%, spec=92% BAL(104): sens=77%, spec=58%
Papazian, 1995 BAL(104): sens=58%, spec=95% PSB(103): sens=42%, spec=95%
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Diagnostic criteria
• Different strategies for diagnosing VAP • Variable sensitivities and specificities • Clinical : e.g. CPIS (sens: 72- 93%, spec: 42-85 %)
• Semi-quantitative microbiology
Modified CPIS > 6, positive semi-quantitative microbiology and MDT
VAP forum
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
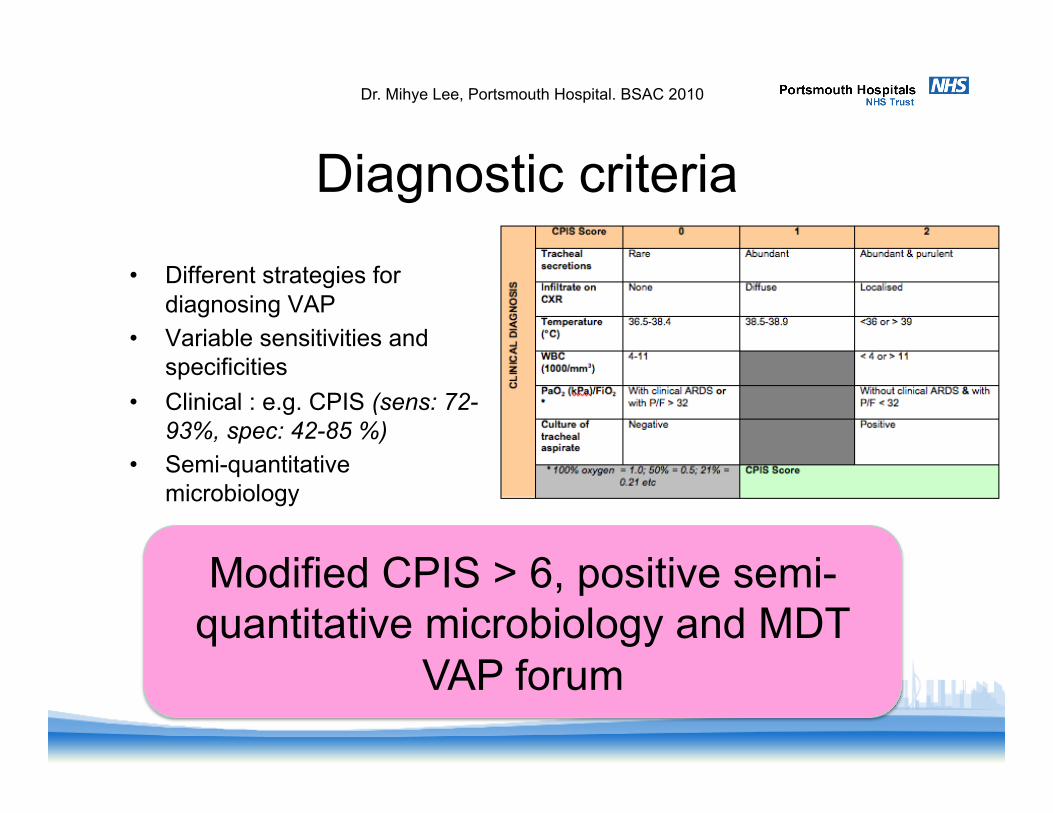
Diagnostic criteria
• Different strategies for diagnosing VAP
• Variable sensitivities and specificities
• Clinical : e.g. CPIS (sens: 72- 93%, spec: 42-85 %)
• Semi-quantitative microbiology
Modified CPIS > 6, positive semi-quantitative microbiology and MDT
VAP forum
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Methods
• Audit period: 116 days from 2009 to 2010 • Data collection: ventilated for > 48hrs + clinical
deterioration suspected to be due to respiratory infection were included in proforma
• Multidisciplinary team (MDT) VAP forum: attended by Microbiologists and Intensivists to discuss and finalise VAP cases
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
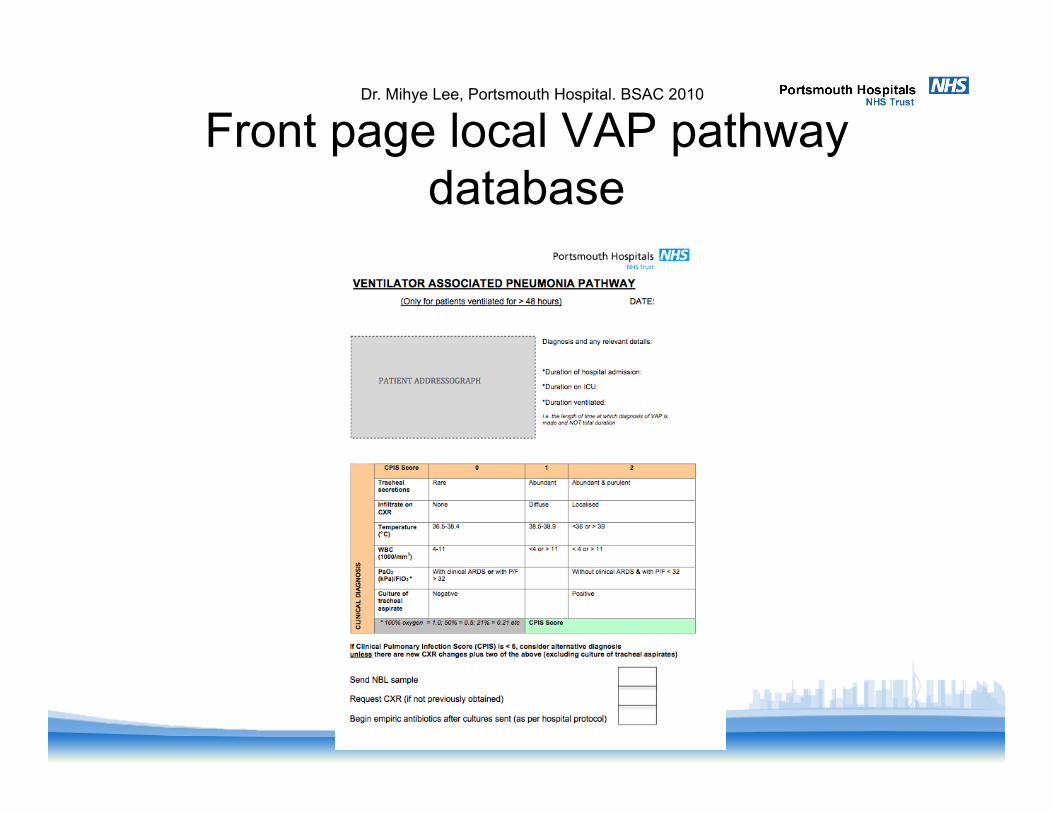
Front page local VAP pathway database
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
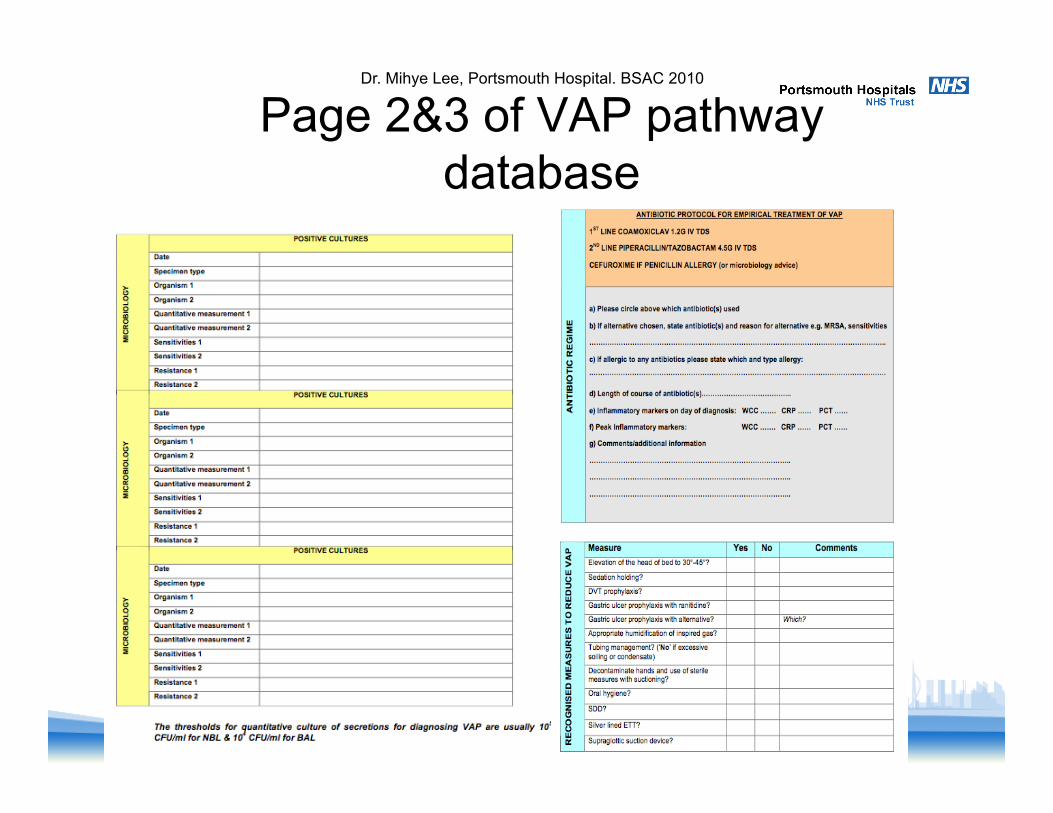
Page 2&3 of VAP pathway database
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
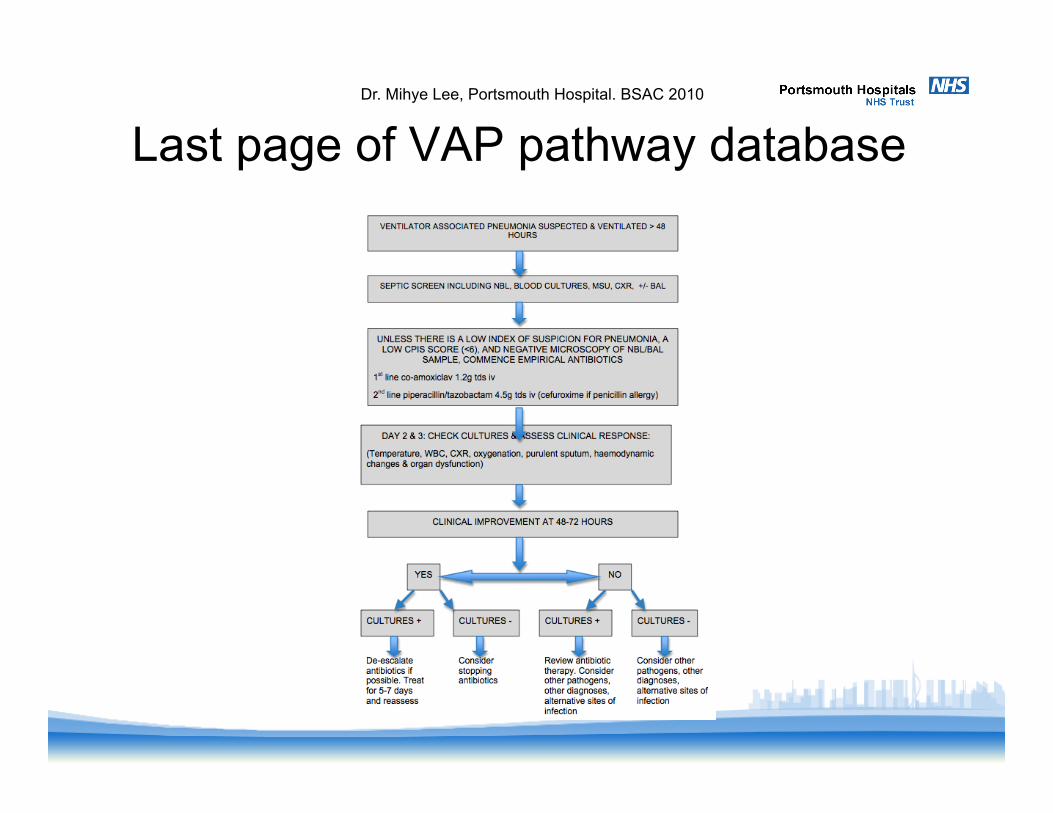
Last page of VAP pathway database Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
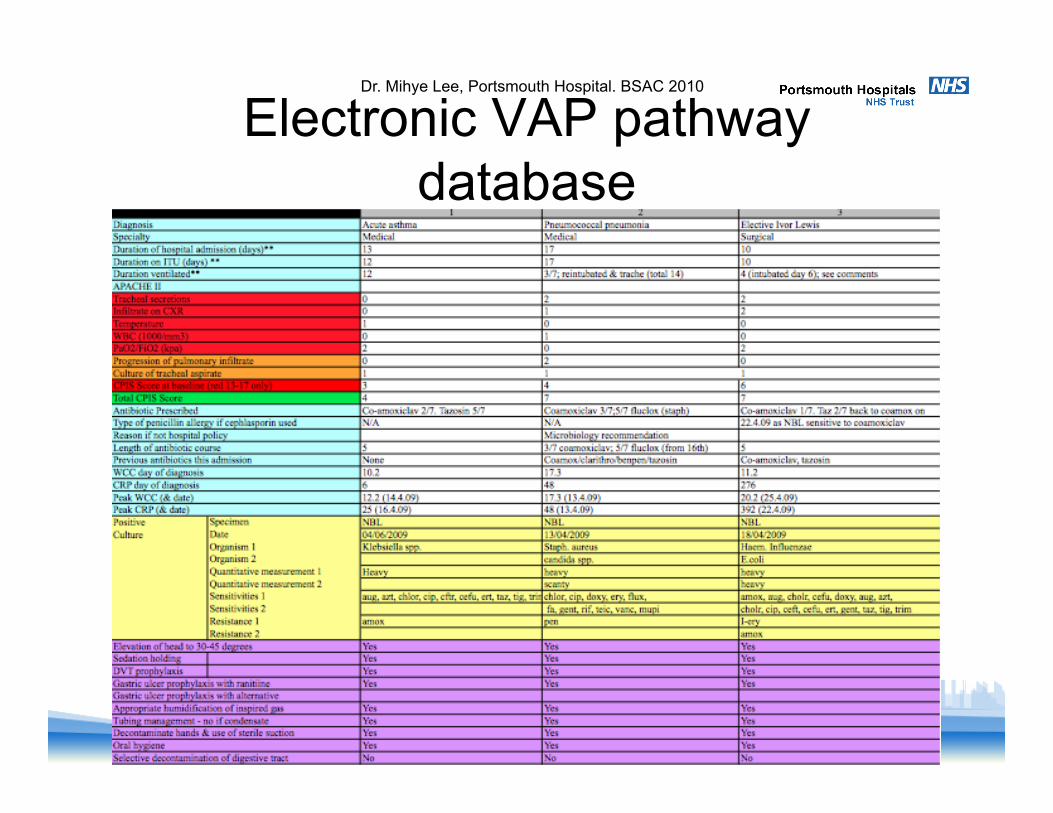
Electronic VAP pathway database
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Results
• 12 episodes were collected on proforma
• 2 long stay patients included twice suspected episodes at two different points during the stay
• MDT VAP forum
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
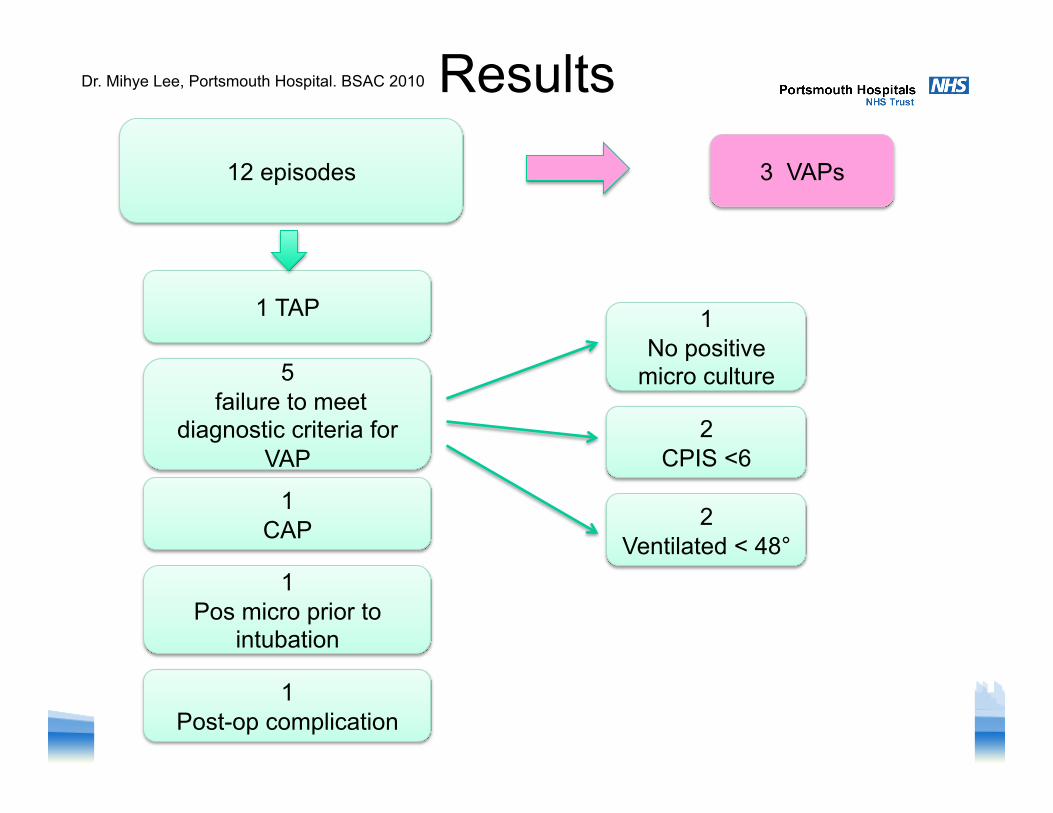
Results 12 episodes 3 VAPs
5 failure to meet
diagnostic criteria for VAP
2 CPIS <6
2 Ventilated < 48°
1 No positive
micro culture
1 CAP
1 Post-op complication
1 TAP
1 Pos micro prior to
intubation
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Results
• Denominator data over 116 days:-
No. patients admitted : 366 patients No. patient ventilated : 199 patients (54%) No. of total ventilated days : 759 days
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010

Results
• No. of patients diagnosed with VAP: 3 patients 4 in 1000 ventilated days
• One patient diagnosed with TAP (tube-associated pneumonia)
• Pilot audit over 61 days:- 12 in 1000 ventilated days
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Conclusions
• Developed Comprehensive process to diagnose VAP
• Implemented an agreed pathway in order to monitor VAP rate
• Audit outcome from stepwise changes in the care bundle ongoing measure of quality of care
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Continued controversies
• Monitoring other healthcare-associated pneumonia that do not fit the VAP definition? eg. TAP
• Necessity to establish national standards to diagnose and monitor VAPs?
• Should VAP be a quality performance indicator for critical care?
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010
Acknowledgements
S Wyllie : Microbiology consultant M Williams : Critical Care consultant S Mathieu, C Allan, J Coakes : Critical care SpR
Dr. Mihye Lee, Portsmouth Hospital. BSAC 2010