development of an antibody-capture igm-enzyme-linked immunosorbent assay for diagnosis of acute...
TRANSCRIPT
Journal of Virological Methods, 21 (1988) 105-l 15
Elsevier 105
JVM 00766
Development of an antibody-capture &M-enzyme-linked immunosorbent assay for
diagnosis of acute Epstein-Barr virus infections
Frits Wielaard’, Jan Scherdersl, Charles Dagelinckx’, Jaap M. Middeldorp’, Luuk J.M. Sabbe2 and Cees v. Belzen*
‘Organon Scientific Development Group, Oss, The Netherlands, and ‘Streeklaboratorium Zeeland, Goes, The Netherlands
Summary
An anti-EBV IgM-ELISA was developed using the antibody-capture principle, to be used for the diagnosis of acute infectious mononucleosis (IM). The test was based on anti-human IgM-coated microtiter plates; nuclei :,f EBV producer cells were used for antigen; conjugate was prepared by labeling sheep anti-EBV IgG with horseradish peroxidase.
The specificity of the anti-EBV IgM-ELISA was studied with a panel of sera from acute infections with hepatitis A virus, rubella virus, Toxoplasma gondii and cytomegalovirus, and sera positive for rheumatoid factors, positive for antinuclear antibodies, as well as with sera from normal blood donors and pregnant women. Specificity in these panels was 98.4%.
In a clinical study with 449 sera from patients with IM-like symptoms, 109 of 109 confirmed patients were detected by the anti-EBV IgM-ELISA. Specificity of the anti-EBV IgM-ELISA in this clinical study was 99.7%. The anti-EBV IgM-ELISA detected several acute EBV patients who had negative heterophile antibody titers.
Epstein-Barr virus; Diagnosis; IgM detection; Infectious mononucleosis; Enzyme immunoassay
Correspondence to: F. Wielaard, Scientific Development Group, Organon International, P.O. Box 20, 5340 BH Oss. The Netherlands.
0166-0934/88/$03.50 0 1988 Elsevier Science Publishers B.V. (Biomedical Division)
106
Introduction
Diagnosis of acute Epstein-Barr virus (EBV) infections may be based on a va- riety of techniques. For the most common manifestation of a primary acute EBV infection, infectious mononucleosis (IM), diagnosis is performed in the majority of cases by demonstration of heterophile antibodies in the patient’s serum. In ad- dition to the heterophile antibody tests, specific anti-EBV antibodies may be de-
tected by use of immunofluorescent tests (IF). Next to these serologic techniques. differential examination of the numbers of atypical lymphocytes is performed to support the diagnosis.
The limitations of the various heterophile antibody tests are well recognized. Most important of all is the fact that the heterophile antibodies can only be found in about SO-95% of all IM patients (Evans et al., 1975; Nikoskelainen et al., 1974; Klemola et al., 1970) and are absent in the majority of young children with pri- mary EBV infections (Sumaya et al., 1985; Schmitz et al., 1972).
Another drawback of the heterophile antibody tests is connected with the large number of different kinds of tests available for this purpose: many commercially available tests are used next to a myriad of home-made assays, each with their own specific reactivities (Evans et al., 1975; Tilton et al., 1988; Cook et al., 1987;
Fleisher et al., 1983). The immunofluorescence tests used in diagnosis are capable of discriminating
between IgG and IgM class antibodies, and may be used to distinguish antibody responses against various different EBV antigen complexes, such as the viral cap- sid antigen (VCA), early antigens (EA) and nuclear antigens (EBNA). This is of importance for an accurate diagnosis of EBV infections.
The use of these EBV specific IF tests is limited by the ti.me-consuming nature of these tests (especially when large amounts of sera have to be examined) and by the need for specific IF equipment and trained personnel. Moreover, IgM-IF tests may suffer from non-specific reactions when rheumatoid facfors are present in the
serum (Henle et al., 1979). In order to meet the increasing demand for reliable tests t6 diagnose acute EBV
infections, we have started the development of an enzyme-lfnked immunosorbent assay (ELISA) which detects IgM-class antibodies against EBV. This test gives highly specific results, has a high sensitivity and is easy to perform, also when larger amounts of samples have be tested.
In this paper we describe the use of this test for diagnosis of acute EBV infec-
tions.
Materials and Methods
Anti-EBV IgM-ELISA Polystyrene microtitre plates were coated with 10 pgiml anti-human IgM im-
munoglobulin G (Organon Teknika, Malvern, Pennsylvania, U.S.A.). Coated plates were stored at 4°C until use.

107
EBV antigen was obtained from culturing the P3HRl cell line HH 514 clone 16
(a kind gift of Dr. G. Miller, Yale University), as described elsewhere (Middel- dorp and Herbrink, 1988). Briefly, TPAbutyrate-induced cells were harvested after six days of culture. Cells were lysed in a hypotonic, detergent containing buffer and the nuclear fraction was isolated by centrifugation through a Ficoll solution. The pellet was sonicated and stored at -20°C until use.
Anti-EBV antibodies, to be used for conjugate, were obtained by immunizing sheep with EBV antigens prepared as described above. IgG was isolated by use of caprylic acid (Steinbuch and Audran, 1969), dialysed against phosphate-buffered saline and stored at -20°C until use.
Anti-EBV conjugate was prepared by coupling sheep anti-EBV IgG antibodies to horseradish peroxidase (Boehringer Mannheim, F.R.G.), using the heterofunc-
tional reagent SPDP (Pharmacia, Uppsala, Sweden) according to the instructions of the manufacturer.
Assay procedure Test sera were diluted 1:lOO in phosphate-buffered saline +0.02% Tween 20
(PBS-tw), and incubated for 1 h at 37°C in the anti-IgM coated wells of a polysty- rene microtiter plate. After emptying and washing the wells, EBV antigen and anti- EBV conjugate were incubated for 1 h at 37°C. Wells were emptied and washed again, and a mixture of tetramethyl-benzidine (TMB) and H202 was added. Any bound enzyme was visualized by this substrate reaction, which was stopped after 30 min by addition of 1 M H$O+ Results were read as optical densities (O.D.) at 450 nm in a Multiskan through-the-plate reader (Organon Teknika, Turnhout, Belgium). The cut-off of the test was defined by the O.D. values of a negative control (N) and a positive control (P) according to the formula 0.5 (O.D., +
O.D.,).
lmmunoj?uorescent tests An immunofluorescent test for detection of anti-EBV VCA IgM was obtained
from Gull Laboratories Inc. (Salt Lake City, Utah, U.S.A.) and was performed as indicated by the manufacturer. Sera which gave discrepant results in the anti- EBV IgM-IF test and anti-EBV IgM-ELISA were retested in the IF test after ab- sorption with anti-IgG serum (Gull Sorb, Gull Laboratories), performed as indi- cated by the manufacturer.
Heterophile untibody tests Heterophile antibodies were determined by the Paul-Bunnell test (PB) (David-
sohn and Lee, 1964). Sera with a PB titer > 1:32 were considered positive.
Specimens A panel of sera from 449 patients with mononucleosis-like symptoms was col-
lected by the Streeklaboratorium Zeeland, The Netherlands. From the majority of those patients who had a positive Paul-Bunnell titer in the
initial specimen, follow-up samples (2-5) were available, as well as from some other
patients. Another panel of sera from 14 patients with a positive heterophile anti- body serology was collected by the Stichting Samenwerkende Delftse Ziekenhui- zen, Delft, The Netherlands. Sera from patients with other acute infections were obtained from various sources. Sera from normal blood donors were kindly sup- plied by the Red Cross Blood Bank, ‘s-Hertogenbosch, The Netherlands. Sera from pregnant women were kindly supplied by the Hopital Cochin, Paris, France.
Western blot analysis Western blot analysis was performed as described elsewhere in this issue (Mid-
deldorp and Herbrink, 1988).
Results
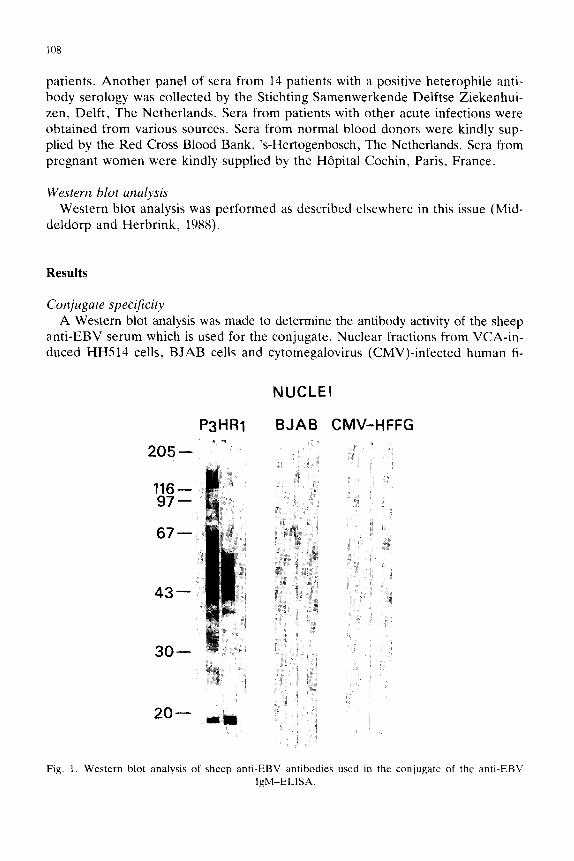
Conjugate spehficity A Western blot analysis was made to determine the antibody activity of the sheep
anti-EBV serum which is used for the conjugate. Nuclear fractions from VCA-in- duced HH514 cells, BJAB cells and cytomegalovirus (CMV)-infected human fi-
P3HRl
205- *”
NUCLEI
BJAB CMV-HFFG
Fig. 1. Western blot analysis of sheep anti-EBV antibodies used in the conjugate of the anti-EBV IgM-ELISA.

109
broblasts (HFFG) were used as antigens. Results are shown in Fig. 1. Broad ac- tivity is seen with the 45-52 kDa band of the EA-complex of the HH514 cells, and with some other EA and VCA polypeptides (e.g. 138, 160 and 18 kDa). Reactivity with BJAB controls and with CMV-infected cells was negligible.
Cut-off value The preliminary cut-off value was defined by 0.5 (O.D.,v + O.D.,), N being the
negative control and P being a positive control serum. Typical O.D. values for N were about 0.200 and typical values for P were 0.700. Hence the cut-off values calculated in each plate were about 0.450, which is well above the mean value of negative sera (O.D.uo = 0.200 * 0.029; data not shown).
Specificity study The specificity of the anti-EBV IgM-ELISA was investigated by testing a num-
ber of sera from different origins (Table 1). Sera (n = 132) from acute stages of infections with Toxoplasma gondii, hepatitis A virus, rubella virus and cytome- galovirus (CMV), as judged by their positivity for the respective IgM antibodies were tested in the anti-EBV IgM-ELISA.
All but one of the anti-CMV IgM positive sera was found negative. In a panel of 30 sera with rheumatoid factors, 26 were negative in the anti-EBV
IgM-ELISA, as were five out of five sera with anti-nuclear antibodies. All sera from pregnant (n = 72) women and all normal blood donor sera (n = 72) were negative.
Based on these results, the overall specificity of the anti-EBV IgM-ELISA was 98.4%.
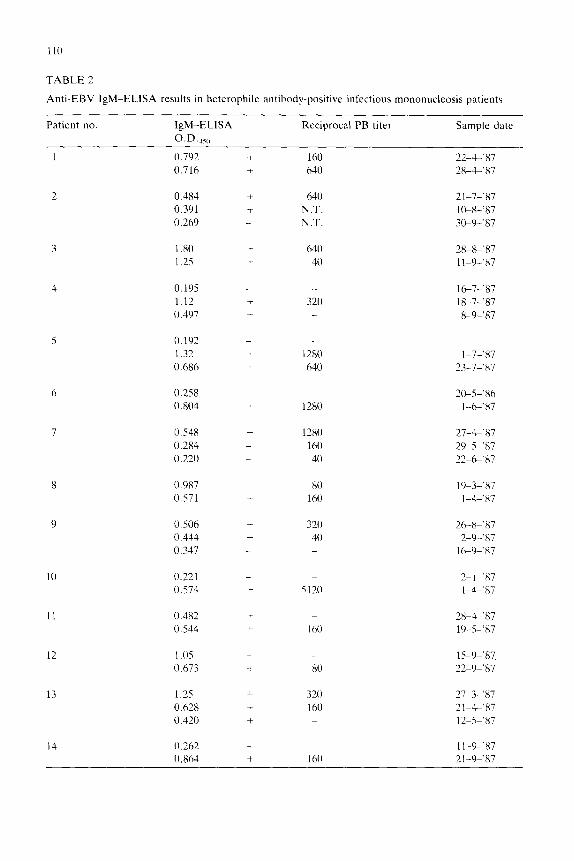
Serial specimens of selected EBV mononucleosis patients A panel of serial serum samples from fourteen patients with IM-like symptoms
and positive heterophile antibody serology was tested in the anti-EBV IgM-ELISA. Results are shown in Table 2. In all patients a clear IgM-response was detected;
in two patients the anti-EBV IgM-ELISA was positive earlier than the PB test.
TABLE 1
Specificity of the anti-EBV IgM-ELISA tested with different types of sera
Type of serum No. tested No. positive
anti-HAV IgM positive 18 0
anti-toxoplasma IgM positive 50 0 anti-rubella IgM positive 36 0
anti-CMV IgM positive 28 1
rheumatoid factor positive 30 4
anti-nuclear antibodies positive 5 0
normal blood donors 72 0 pregnant women 72 0
110
TABLE 2
Anti-EBV IgM-ELISA results in heterophile antibody-positive infectious mononucleosis patients
Patient no. IgM-ELISA
O.D.,,,,
Reciprocal PB titer Sample date
1 0.792 f 160 22-J-%87
0.716 + 640 2%,-c’87
2 0.4X4 + 640 21-7-%X7 0.391 + N.T. I O-X-‘87
0.269 _ N.T. 3&9-‘87
1.80 c 640 2X-X-‘87
1.25 1. 40 11-9-.x7
0.195
1.12
0.397
_ _ i 320 +
l&7-‘87 1%7-‘87
X-9-,87
0.192 _ 1.32 + 1280
0.686 + 640 1-7-x7
23-7-‘87
0.258 0.804
_ _ + 1280
2&5-.X6
l-G.87
0.548 + 1280 27-4-.x7
0.284 _ 160 29-5-W
0.220 _ 40 72-f%‘87
0.987 + 80 19-3-.x7
0.571 + 160 l--k’87
0.506
0.444
0.347
+ 320 26-X-,87 + 40 2-9-.x7 _ _ I GO-‘87
10 0.221
O.S74
_ _ + 5120
2-I-‘87
l-G.87
11 0.482 + _ 2X-4-.x7
0.544 + 160 1%s-‘87
12 1 .os + _ 15-9-x7
0.673 + 80 22-9-*X7
13 1.25 c 320 27-3-‘87
0.628 160 21-;1-‘X7
0.420 + _ 12-5-X7
14 0 262 _ 1 I-9-.X7
0.864 + 160 2 l-9-%7

111
TABLE 3
Correlations between the anti-EBV IgM-ELISA and the anti-EBV IgM-IF before and after absorp-
tion of discrepant sera with anti-IgG and subsequent retesting in the IgM-IF test
ELISA
IF before absorption
+ _ ELISAb
IF after absorption
+
+ 145 2 + 146 1
_ 9 293 _ 2 300
Clinical study The use of the anti-EBV IgM-ELISA for diagnosis of acute infectious mono-
nucleosis was evaluated in a study where sera from 449 patients with IM-like symptoms had been collected. All sera were tested in the PB test, the anti-EBV IgM-immunofluorescence test (IgM-IF) and in the anti-EBV IgM-ELISA. From most PB-positive patients follow-up specimens were available.
In order to assess the clinical sensitivity of the anti-EBV IgM-ELISA, we de- fined confirmed IM patients as patients with both positive PB titers and positive
IgM-IF results. A total of 109 confirmed patients could be defined; the anti-EBV IgM-ELISA was positive in the initial specimens of 1091109 (100%) of these pa- tients.
According to the same procedure, we defined non-EBV patients to be those with neither a positive PB titer nor a positive IgM-IF result in the initial specimen. In 293 non-EBV patients, the specificity of the anti-EBV IgM-ELISA was 99.7%
(2921293). The correlation of the anti-EBV IgM-ELISA with the standard IgM-IF test was
determined using initial sera of all 449 patients, and was found to be 97.6% (Table 3). When the discrepant sera were retested in the IgM-IF using the anti-IgG ab- sorption step, the correlation improved till 99.3% (Table 3). Seven out of 9 IgM-IF- positive sera which were IgM-ELISA negative and PB negative became IgM-IF negative after absorption; one of two IgM-IF negative sera which were IgM-ELISA
TABLE 4
Effect of absorption with anti-IgG serum on test results in the anti-EBV IgM-IF test
Serum no. Reciprocal PB titer Results
IgM-ELISA IgM-IF
before absorption after absorption
17.1 16 _ + _
65.1 + _
108.1 _ _ + _
168.1 _ + _
269.1 _ + _
287.1 _ _ +
393.1 _ _ +
380.1 512 + _ +
112
PATIENT 92 PATIENT 95
A450 IQM-ELISA RECIPROCAL PB TITER
0~5
0 4 8 WEEKS
512
128
-32
NEG.
Ads IgM-ELISA RECtPROCAL PB TITER
- 2048
0 4 8
WEEKS
PATIENT 102
A&SQ I&-EL&A mmacAt. PB TITER
147
f - 2048
I,(?- 512
-128
” 32
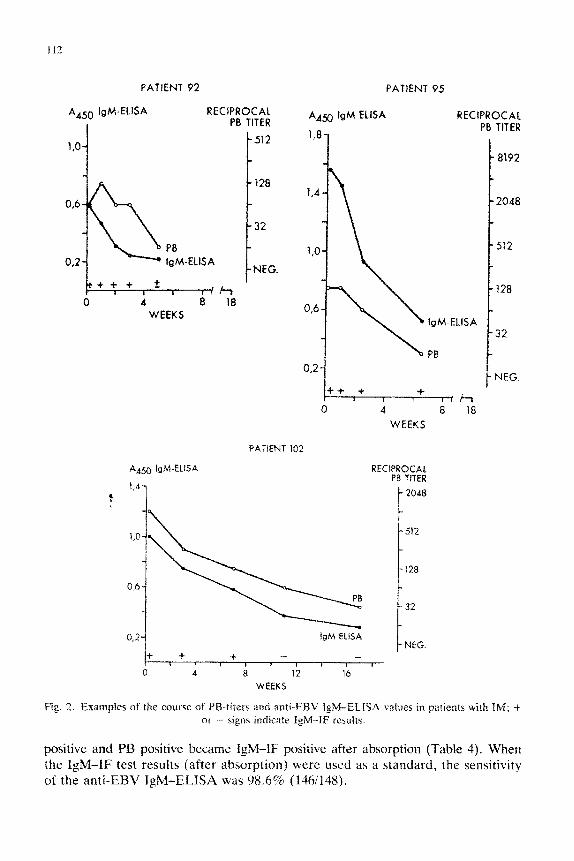
Fig. 2. Examples of the cburse of PW-titers md anti-EBV IgK43_iSA values in patients with IM: i or -- signs indicate f&l-IF rcsutts.
positive and PB positive became IgM-IF positive after absorption (Table 4). When the IgM-IF test results (after absorption) were used as a standard, the sensitivity of the anti-EBV IgM-ELISA was 98.6% (1361148).

113
The specificity calculated in this way was 99.7% (3001301). The course of the
anti-EBV IgM-antibodies as determined by the ELISA was studied in IM-patients from which serial specimens were available. A wide variation in the rate of decline was found; IgM antibodies disappeared between one and three months after onset of illness.
Examples are shown in Fig. 2. In general, the decline of the IgM-ELISA values coincided with the decline of the IgM-IF positivity, and both patients whom either
IgM-IF antibodies or IgM-ELISA antibodies persisted longer were observed. Among the 449 initial sera, 27 sera were found negative in the PB test, and po-
sitive in both the anti-EBV IgM-ELISA and the IgM-IF test. Based on data from
follow-up specimens, 7 of these patients could be defined as true acute EBV in- fections. From the remaining subset of 20 sera, we could retest 14 sera in the IgM-IF after anti-IgG absorption. Thirteen of these remained positive, and were therefore considered to represent true acute EBV infections. One serum gave an inconclusive result, the six remaining sera could not be retested. Altogether, we
could indicate 20 patients with an incorrectly negative PB test result in the initial
specimen.
Discussion
The results presented in this study confirm the value of the antibody-capture anti- EBV IgM-ELISA for the diagnosis of infectious mononucleosis.
For development of the IgM-ELISA the antibody-capture principle was chosen in view of the high sensitivity and specificity inherent to this principle. The advan-
tages of antibody-capture systems for the detection of specific IgM antibodies are well documented (Champsaur et al., 1988).
The low sensitivity for rheumatoid factor interference of the antibody-capture tests as compared with IgM-assays using anti-IgM conjugates is clearly demon- strated in this study: seven PB-negative sera were found which were positive in the IgM-IF test and negative in the anti-EBV IgM-ELISA; after absorption with anti- human IgG, the IgM-IF results became negative as well. Presumably, the false positivity of the IgM-IF was caused by rheumatoid factors; the anti-EBV IgM-ELISA yielded correct results with these sera.
The problem of rheumatoid factor interference in the IgM-IF test has been de- scribed by others (Henle et al., 1979) and various methods to solve the problem have been developed, such as column separation of sera (Sumaya et al., 1984) and Staphylococcus aureus absorption (Sumaya et al., 1982; Harnett et al., 1985), or IgG precipitation (Hekker et al., 1979).
False negative results in IgM-IF assays due to competition of specific IgG have been described as well (Sumaya et al., 1982). In the initial serum specimens in our study we have found one example, being the serum no. 380.1 in Table 4. In the follow-up specimens, more examples were seen (data not shown). The antibody- capture IgM-ELISA is not sensitive for IgG competition, and yielded correct re- sults.

11-l
The high sensitivity of the IgM-ELISA described here may partly be attributed to the broad and strong reactivity of the sheep anti-EBV hyperimmune serum used for conjugate preparation. The Western blot shows strong bands with a variety of
antigenic polypeptides (Fig. 1). The most prominent activity is directed against the 45-52 kDa protein of the EBV EA complex. The important role of the EA anti-
gens in detection of acute-stage IgM is becoming clearer (Middeldorp and Her-
brink, 1988). The anti-VCA IgM response as observed in IgM-IF assays may very well in-
clude an anti-EA IgM response, since these EA antigens are invariably present in the cell preparations used for preparing anti-VCA IgM-IF slides.
The specificity of the anti-EBV IgM-ELISA was assessed with sera from pa-
tients with various acute infections. Only in the group of 30 sera which were po- sitive for anti-CMV IgM antibodies one serum was positive in the anti-EBV IgM-ELISA as well. We have not been able to assess whether this result was a true false positive or reflected a double infection of CMV and EBV. In the group of sera positive for rheumatoid factors four positive results were found; it was con- cluded that these were false positives in view of the negative results found in the
IgM-IF test after absorption of IgG. Sera from normal blood donors and pregnant women were all negative. Altogether, the specificity of the anti-EBV IgM-ELISA
in this specificity study was 98.4%. In order to assess the value of the anti-EBV IgM-ELISA in a real clinical set-
ting, a clinical study was performed in collaboration with a regional laboratory which performs routine EBV testing on sera of patients with IM-like symptoms.
Sera from 449 patients were collected, and tested in the PB test, IgM-IF test and the anti-EBV IgM-ELISA. The presence of both PB positivity and IgM-IF positivity in the initial specimens was used to define true EBV patients. Using this definition, the sensitivity of the ELISA was found to be 100%. When compared with the IgM-IF test on these sera, the sensitivity was 98.6%. The specificity of the ELISA in this clinical setting was found to be 99.7%.
As compared to the PB test, the ELISA detected more IM patients. In our study we found 27 patients with*initial PB titers of =z 1:32 and positive IgM-ELISA re-
sults, which were confirmed by the IgM-IF test. In 20 of these 27 patients, strong evidence was available to confirm that these
were true acute EBV infections. These findings are in agreement with the well de- scribed low sensitivity of heterophile antibody tests for diagnosis of IM (Fleisher et al., 1983; Nikoskelainen et al.. 1974; Swanston et al., 1986).
Acknowledgement
The supply of serial specimens from IM-patients by Dr. P. Herbrink (SSDZ) is gratefully acknowledged.
115
References
Cook, L., Midget, J., Willis, D.. Clinton, B. and Folds. J.D. (1987) Evaluation of latex-based heter- ophile antibody assay for diagnosis of acute infectious mononucleosis. J. Clin. Microbial. 25.
2391-2394.
Champsaur, H., Fattal-German, M. and Arranhado, R. (1988) Sensitivity and specificity of viral im-
munoglobulin M determination by indirect enzyme-linked immunosorbent assay. J. Clin. Micro-
biol. 26, 328332.
Davidsohn, I. and Lee, C.L. (1964) Serologic diagnosis of infectious mononucleosis. Am. J. Clin. Pa-
thol. 41, 115-125.
Evans, A.S., Niedermann, J.C., Cenabre, L.C., West, B. and Richards. V.A. (1975) A prospective
evaluation of heterophile and EBV specific IgM antibody tests in clinical and subclinical infectious
mononucleosis. J. Infect. Dis. 132, 54&554.
Fleisher, G.R., Collins, M. and S. Fager (1983) Limitations of available tests for diagnosis of infectious
mononucleosis. J. Clin. Microbial. 17, 619-624.
Harnett, G.B., Palmer, C.A. and Bucens. M.C. (1985) A modified IF test for EBV specific IgM an-
tibody. J. Virol. Methods 12, 25-30.
Hekker, A.C.. Brand-Saathof, B., Vis, J. and Meijers, R.C. (1979) Indirect IF test for detection of
IgM antibodies to CMV. J. Infect. Dis. 140, 596600.
Henle, G., Lenette, E.T.. Alspangh, M.A. and Heule, W. (1979) Rheumatoid factor as a cause of
positive reactions in tests for EBV specific IgM. Clin. Exp. Immunol. 36. 415-422.
Klemola, E.. von Essen, R., Heule, G. and Heule. W. (1970) IM-like disease with negative hetero-
phile agglutination test. J. Infect. Dis. 121, 608-614.
Middeldorp, J.M. and Herbrink, P. (1988) J. Virol. Methods, 21, 133-146.
Nikoskelainen, J., Leikola, J. and Leikola, E. (1974) IgM antibodies specific for EBV in IM without heterophile antibodies. Br. Med. J. 4, 72-75.
Schmitz, I-I., Volz, D., Krainiek-Richert, Ch. and Schrere. M. (1972) Acute EBV infections in chil-
dren. Med. Microbial. Immunol. 158. 58-63.
Steinbuch, M. and Audran, R. (1969) The isolation of IgG from mammalian sera with aid of caprylic
acid. Arch. Biochem. Biophys. 134, 279-284.
Sumaya, C.V., Erich. Y. and Pope, R.M. (1982) Improved tests for IgM antibody to EBV. J. Infect.
Dis. 146, 518-521.
Sumaya, C.V.. Erich, Y., Carillo, M.A. and Pope, R.M. (1984) Use of a simple separation column in detection of IgM antibody to EBV. J. Clin. Microbial. 20, 298299.
Sumaya, C.V. and Erich, Y. (1985) EBV mononucleosis in children. II. Pediatrics 75, 1011-1019.
Swanston, W., Mahony, J., McLaughlin, B. and Chernesky, M. (1986) Assessment of serologic mark- ers for EBV. Diagn. Microbial. Infect. Dis. 5, 235-244.
Tilton, R.C., Dias, F. and Ryan. R.W. (1988) Comparative evaluation of three commercial tests for
detection of heterophile antibody in patients with IM. J. Clin. Microbial. 26, 275-278.