developing continuous quality improvement...
TRANSCRIPT
�����������������������������������������������������
DEVELOPING
Continuous QualityImprovement Activities
from a quality perspective
Measuring the care you practice provides
Using the quality cycle to continually improve performance
How to get your continuous quality improvement credits

DEVELOPING
Continuous QualityImprovement Activities
from a quality perspective
Measuring the care you practice provides
Using the quality cycle to continually improve performance
How to get your continuous quality improvement credits
�����������������������������������������������������
Acknowledgements
The RNZCGP hopes you will find this resource a useful introduction to the concept of quality improve-
ment. It replaces the Practical Guide to Audit and is the result of feedback from trials and workshops
during 1998/9.
Dr Keith Carey-Smith, Dr Jim Vause, Dr Wellingham, Dr Tony Hanne, Dr Dean Millar-Coote, Maureen
Gillon, Lynn Saul.
ISBN: 0-9582176-1-0
© The Royal New Zealand College of General Practitioners, New Zealand, 2000. Reprinted 2009
The Royal New Zealand College of General Practitioners owns the copyright of this work and has
exclusive rights in accordance with the Copyright Act 1994.
In particular, prior written permission must be obtained from the Royal New Zealand College of General
Practitioners for others (including business entities) to:
• copythework
• issuecopiesofthework,whetherbysaleorotherwise
• showtheworkinpublic
• makeanadaptationofthework
as defined in the Copyright Act 1994.
Contents
This resource is designed for individual GPs, practice staff, IPAs and other primary
care groups. It outlines the RNZCGP framework for designing and undertaking a
College approved quality improvement activity.
Introduction ................................................................................................................. 4
SECTION 1: Quality improvement .............................................................................. 6
1.1 Quality improvement ....................................................................................... 6
1.2 Measuring quality ............................................................................................ 6
1.3 The role of feedback in improving quality ....................................................... 7
1.4 Setting markers for improvement .................................................................... 7
SECTION 2: Introducing the RNZCGP quality cycle .................................................. 9
2.1 A six step guide to designing your own quality improvement process ........ 10
1. Topic selection ................................................................................... 10
2. Plan .................................................................................................... 10
3. Data .................................................................................................... 11
4. Check ................................................................................................. 13
5. Act ...................................................................................................... 14
6. Review ................................................................................................ 15
2.2 Sample quality improvement cycle ............................................................... 16
SECTION 3: Suggested quality improvement topics ............................................... 18
Glossary .................................................................................................................... 24
Appendix 1 ................................................................................................................ 27
Appendix 2 ................................................................................................................ 29
References ................................................................................................................ 30
4 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
Introduction
The Mission statement of the RNZCGP is:
‘To improve the health of all New Zealanders through high quality general practice’
The College has produced this document as another tool to help GPs progress fur-
ther along the path of achieving high quality general practice. The aim of this tool is
to provide a way of taking any aspect of general practice and to formulate a plan to
improve it. It focuses on how you can establish where you are now, where you want
to go and how to get there. It can be used together with the many other tools already
published by the College.
Quality general practice will mean different things to different people depending on
which aspect of a subject is being discussed. However there are two key concepts
that are useful in thinking about improving quality.
Quality can and must be measured. To know where you are now, and how well you •
are making progress towards the goals you want to achieve, a measure of some
sort must be used. Sometimes it is not easy to measure the qualitative aspects of
practice and to improve we must be able to measure that improvement.
Quality is not a static state. Circumstances and parameters change so that what-•
ever you are doing, it can always be done better. This is often called Continuous
Quality Improvement (CQI) and can be expressed in the form of quality cycles.
Therefore, this document is a guide to implementing CQI in general practice.
CQI in general practice is concerned with the assessment of the quality of medical care,
the efforts to improve the provision of care and the procedures to ensure that good
quality is maintained. Undertaking a quality improvement process reflects the desire
and commitment of the team to find out, “Are we doing what we should be doing?”
and, “How can we do better”. In defining where you want to go, it is important that a
process is planned and asks the right questions in order to find the answer.

© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 5
One term for this is a gap analysis. For example:
“Imagine yourself on a yacht in the middle of the Pacific with no engine or modern naviga-
tional equipment. A logical question would be, “Where am I?” Using a sextant allows you
to put a cross on the map. Only then can another cross be marked at where you want to
go before making the next step about how to get there.
“The assumption behind the approach to quality measurement is that unless we learn at
least something about what we are doing, it is highly unlikely that we will know what needs
improving, or how to improve. It is generally agreed that the most effective way to learn is
to ask the right questions. The key is to establish a baseline to enable you to know where
you stand in relation to where you want to go.” (Tony Hanne, Goodfellow Unit, 1999)
6 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
SECTION 1
Quality Improvement
1.1 Quality improvement
Quality improvement in general practice is concerned with the assessment of the quality
of medical care, the efforts to improve the provision of care and the procedures to ensure
that good quality is maintained. Undertaking a quality improvement process reflects
the desire and commitment of the team to find out, “Are we doing what we should be
doing?” and “How can we do better”1, 2. In defining where you want to go, it is important
that a process is planned and asks the right questions in order to find the answer.
1.2 Measuring quality
There are two aspects to improving quality.
The measure: “Look at where you are”.•
The change: “Getting where you want to be”.•
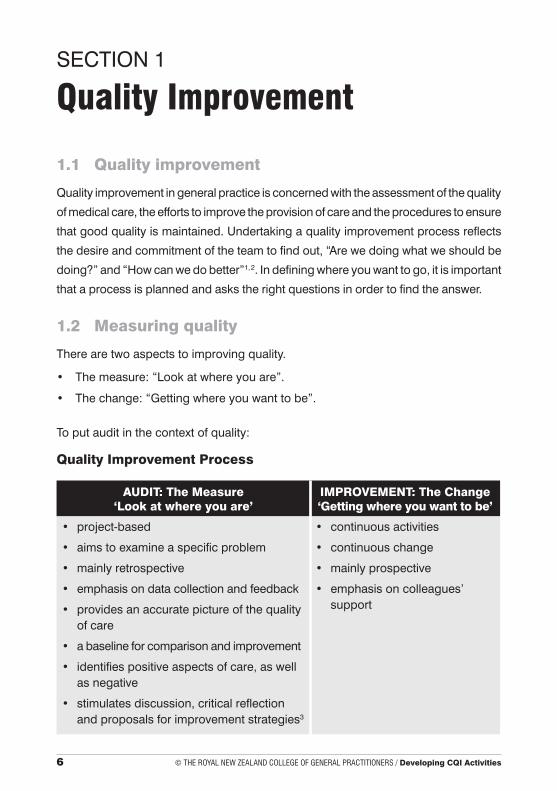
To put audit in the context of quality:
Quality Improvement Process
AUDIT: The Measure ‘Look at where you are’
IMPROVEMENT: The Change ‘Getting where you want to be’
project-based •
aims to examine a specific problem•
mainly retrospective •
emphasis on data collection and feedback•
provides an accurate picture of the quality •of care
a baseline for comparison and improvement•
identifies positive aspects of care, as well •as negative
stimulates discussion, critical reflection •and proposals for improvement strategies3
continuous activities•
continuous change•
mainly prospective•
emphasis on colleagues’ •support
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 7
1.3 The role of feedback in improving quality
Practice staff meetings or peer group discussion provide the best opportunity to dis-
cuss audit results. Planning responses and implementation strategies that are more
likely to produce a change in behaviour then depends on the level of commitment by
the practice team. If used properly, feedback provides a basis for modifying behaviour,
and is fundamental to the learning process3.
1.4 Setting markers for improvement
Identifying ‘where you are’ and setting markers for improvement ‘where you want to
be’ involves three steps:
Choosing indicators1.
Developing criteria2.
Setting the standard 3.
STEP 1: Choosing indicators of best practice from the information available(see Appendix 1 for different ways of classifying evidence)
Indicators are markers that provide points along the way to meeting a standard. They
are measurable elements of practice performance for which there is evidence or con-
sensus that it can be used to assess quality, and produce a change in the quality of
care provided4. The basis for regarding an element of performance, as an indicator
should be explicitly stated, where possible using published evidence e.g.
INDICATOR
The smoking status of adult patients is identified and recorded in the patient notes.
Source: National Health Committee. Guidelines for smoking cessation. NZ: National
Advisory Committee on Health and Disability; July 1999.
Note: The example of smoking status is used throughout this document.
8 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
STEP 2: develop criteria to measure the indicator
Criteria are the elements of care that can be counted or measured in order to assess
the indicator. They are discrete, definable, measurable and explicit. In other words, it
needs to be precisely defined2 e.g.
CRITERIA
• Smokingstatusisrecordedinthenotesofadultpatients.
• Smokingstatusisupdatedregularly.
STEP 3: setting the standard
The standard is essentially a mark of success in achieving an indicator and specifies
the acceptable level of care3. Therefore, the standard is the level of performance that
you want or expect to achieve. It may be a precise target level of performance or that
which you identify e.g.
STANDARD
Smoking status is recorded in 80% of adult patient notes.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 9
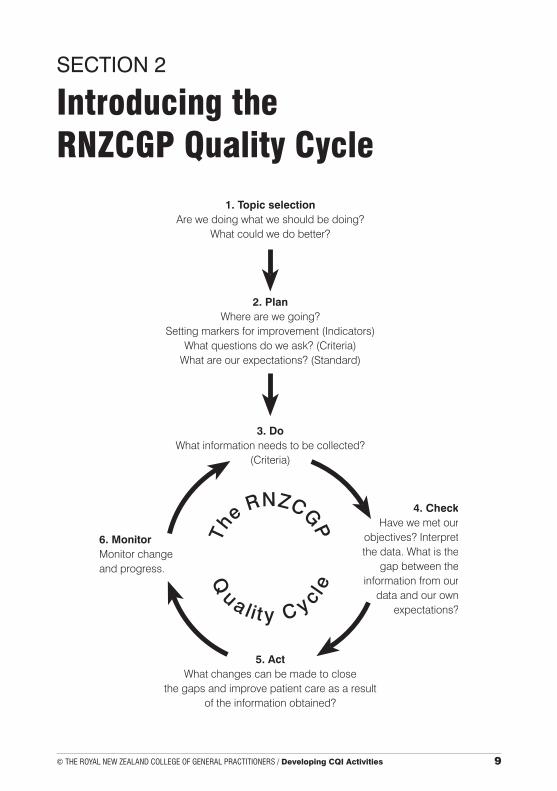
SECTION 2
Introducing the RNZCGP Quality Cycle
10 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
2.1 A six step guide to designing your own quality improvement process
1. TOPIC SELECTION
Are we doing what we should be doing?
e.g. Smoking Cessation
Choosing a topic
What do you want to review?•
Keep it relevant, it should be a practice problem, and/or have common or serious •
consequences.
It should be clearly defined.•
Benefit the health status, well-being or satisfaction of patients.•
Have important cost implications.•
Have relevant scientific findings which show a connection between the process •
and desired outcome5.
Choose a topic where you can change the outcome. If you can’t, don’t try.•
Suggestions
Development/improvement can be done as a peer group activity.•
It may be easier to use an existing resource developed by the RNZCGP.•
KISS Theory• …Keep It Short and Simple.
2. PLAN
Where are we going?
Develop the indicator/marker/area to review.
Where are we going? Are there any evidence-based guidelines or other resources
available that outline best practice e.g.
Guidelines for smoking cessation• 6.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 11
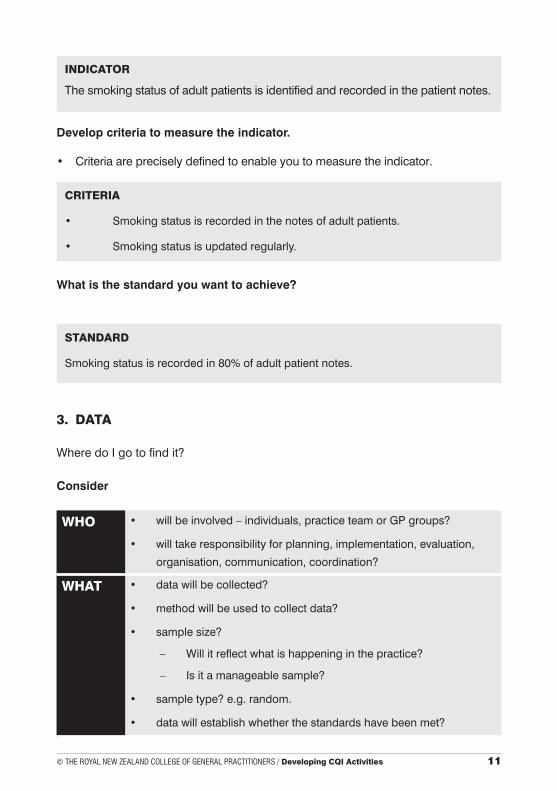
INDICATOR
The smoking status of adult patients is identified and recorded in the patient notes.
Develop criteria to measure the indicator.
Criteria are precisely defined to enable you to measure the indicator.•
CRITERIA
• Smokingstatusisrecordedinthenotesofadultpatients.
• Smokingstatusisupdatedregularly.
What is the standard you want to achieve?
STANDARD
Smoking status is recorded in 80% of adult patient notes.
3. DATA
Where do I go to find it?
Consider
WHO • willbeinvolved–individuals,practiceteamorGPgroups?
• willtakeresponsibilityforplanning,implementation,evaluation,
organisation, communication, coordination?
WHAT • datawillbecollected?
• methodwillbeusedtocollectdata?
• samplesize?
– Willitreflectwhatishappeninginthepractice?
– Isitamanageablesample?
• sampletype?e.g.random.
• datawillestablishwhetherthestandardshavebeenmet?
12 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
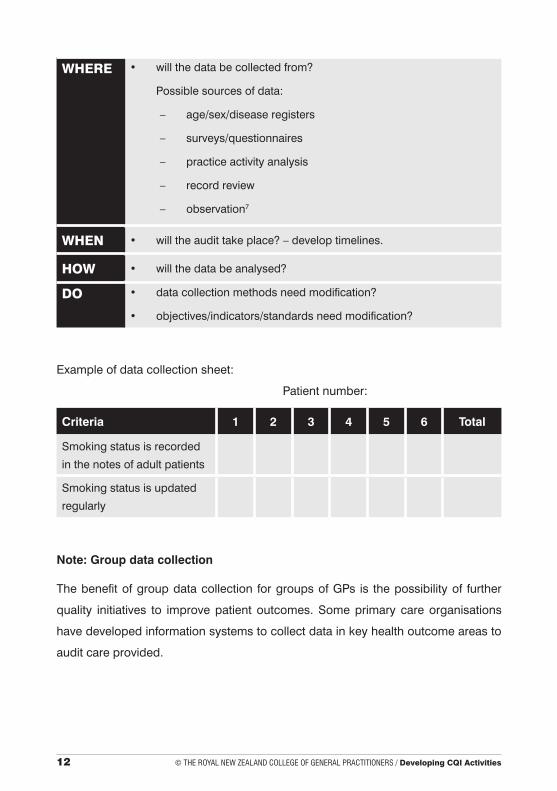
WHERE • willthedatabecollectedfrom?
Possible sources of data:
– age/sex/diseaseregisters
– surveys/questionnaires
– practiceactivityanalysis
– recordreview
– observation7
WHEN • willtheaudittakeplace?–developtimelines.
HOW • willthedatabeanalysed?
DO • datacollectionmethodsneedmodification?
• objectives/indicators/standardsneedmodification?
Example of data collection sheet:
Patient number:
Criteria 1 2 3 4 5 6 Total
Smoking status is recorded
in the notes of adult patients
Smoking status is updated
regularly
Note: Group data collection
The benefit of group data collection for groups of GPs is the possibility of further
quality initiatives to improve patient outcomes. Some primary care organisations
have developed information systems to collect data in key health outcome areas to
audit care provided.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 13
4. CHECK (COMPARE)
What is the gap between data results and your own expectations?
Analysing the results
This step involves comparing data with the standards set for the indicators and crite-
ria, (although some may be doing better than expected, it is more common for most
practices to find that their audit results are not as good as expected8).
Review the data and compare with your expectations (the standard you set)
Where are the gaps between your expectations and your data results?•
Where are the gaps small, i.e. where are you doing well?•
Where are the gaps large, i.e. where is there room for improvement?•
Which gaps do we want to close?•
Note: Before developing an action plan, prioritise the problem to solve and choose
solutions.
EXAMPLE
• If the standard for recording the smoking status was set at 80% and
you achieved 40%, then you would have a baseline for identifying improvement.
• Theremightbeanumberofareasthatyoucouldidentifyasbeingpotentialsources
for improvement e.g.
– Routinelyaskingpatientsaboutsmoking.
– Developingawarningiconforthecomputer.
– Usingcolouredstickersforsmokingstatus.
• Oncethelistisdevelopedthebestoptionscanbechosenbythepracticestaff.
14 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
5. ACT
What changes can be made to improve patient care?
Taking action
Once the team has identified priorities for change, the next step is to ensure everyone
knows what needs to be done, by whom, and by when. Include the practice team in
the planning and decision making.
Problem solving process
What is the problem or underlying problem(s)?•
Change it to an aim.•
What are the solutions or options?•
What are the barriers? How can you overcome them?•
Overcoming barriers
Identifying barriers can provide a basis for change3.
Whatisachievable–findoutwhattheexternalpressuresonthepracticeareand•
discuss ways of dealing with them in the practice setting.
Identify the barriers? •
Develop a priority list. •
Choose one or two achievable goals e.g.•
Barriers list Options Selected options
1.
2.
3.
Effective interventions3
No single strategy or intervention is more effective than another, and sometimes •
a variety of methods are needed to bring about lasting change.
Interventions should be directed at existing barriers or problems, knowledge, skills •
and attitudes, as well as performance and behaviour.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 15
Action – A framework for change
Below is an example of an action plan for identifying and organising change:9
Action plan for improving the recording rate of patients who smoke
Action required
Person responsible
Resources required
Establish timeline
Priority Procedure
PRESENT THE RESULTS – PLAN CHANGES
Develop ways to change the result to a more positive solution15.
• Whatistheunderlyingproblem?–Doesthepracticeseeanyareasitwishes to improve?
• Whatareyouaimingtoachieve?–Prioritisethegapswhichthepracticewishestoclose and choose one, two or three topics.
• Whatoptionsarethereforachievingtheaims?–Developactionplans.
• Whichoptionswouldbebest?–Useproblemsolvingtechniques.
• Whatbarrierswillpreventyouachievingthese?–Howwillthepracticeensureplansare carried out?
• Howwillyougetpastthebarriers?–Who/what/how/when?
• Whenwillyoureviewthisagaintoseehowfaryouhavegot?–diaryit!
• Planafeedbacksessionusingafacilitator.
6. REVIEW
Were the goals for improvement achieved?
Monitoring change and progress
Review the action plan, e.g. 3/12, 6/12, 9/12, 12/12 against the timeline.•
Evaluatetheoutcome–istheprocessworking?•
Were the goals for improvement achieved?•
Have the goals changed as a result?•
Do you need to develop new tools to achieve the goals that have been set?•
Determine whether a second audit should be done.•
16 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
Undertaking a second cycle
It is recommended that the second cycle be commenced at stage 3 (Data).
Was the information you collected appropriate for the questions asked?•
Did you meet the expectations as outlined in the first cycle?•
Was the whole process beneficial?•
Keeptheworkloadmanageable!•
Gaining credits
MOPS (Maintenance of Professional Standards) credits may be gained from complet-
ing continuous quality improvement activities that have been endorsed by the College
(see Appendix 2).
2.2 Sample Quality Improvement Cycle – Smoking Cessation6
This activity was developed using the Guidelines for Smoking Cessation.
TOPIC SMOKING CESSATION
Consider are we doing what we should be doing?
PLAN Where are we going?
Are there any evidence-based guidelines or other resources avail-
able that outline best practice?
National Health Committee. Guidelines for smoking cessation. NZ: National
Advisory Committee on Health & Disability; July, 1999.
1. Which indicators will you choose from the information available?
The smoking status of adult patients is identified and recorded in the
patient notes.
2. Identify the criteria to measure the indicator.
• Smokingstatusisrecordedinthenotesofadultpatients.
• Smokingstatusisupdatedregularly.
3. What is the standard you want to achieve?
Smoking status is recorded in 80% of adult patient notes.
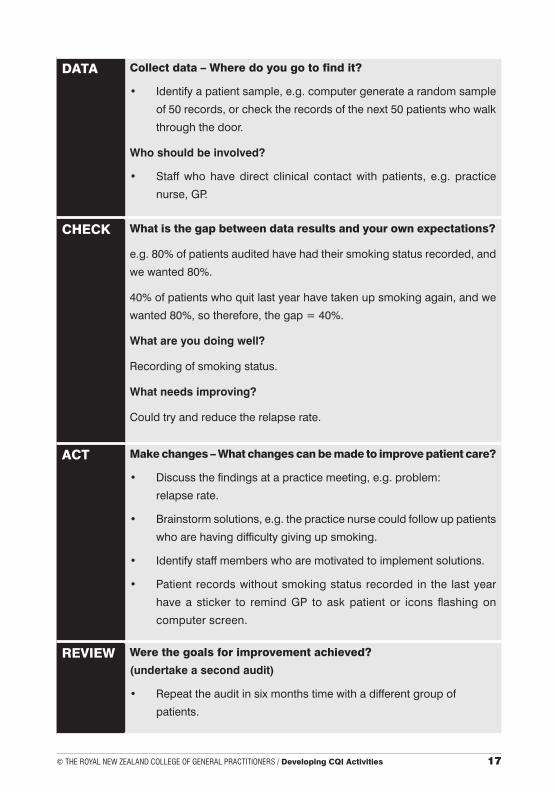
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 17
DATA Collect data – Where do you go to find it?
• Identifyapatientsample,e.g.computergeneratearandomsample
of 50 records, or check the records of the next 50 patients who walk
through the door.
Who should be involved?
• Staffwhohavedirect clinical contactwith patients, e.g. practice
nurse, GP.
CHECK What is the gap between data results and your own expectations?
e.g. 80% of patients audited have had their smoking status recorded, and
we wanted 80%.
40% of patients who quit last year have taken up smoking again, and we
wanted 80%, so therefore, the gap = 40%.
What are you doing well?
Recording of smoking status.
What needs improving?
Could try and reduce the relapse rate.
ACT Make changes – What changes can be made to improve patient care?
• Discussthefindingsatapracticemeeting,e.g.problem:
relapse rate.
• Brainstormsolutions,e.g.thepracticenursecouldfollowuppatients
who are having difficulty giving up smoking.
• Identifystaffmemberswhoaremotivatedtoimplementsolutions.
• Patient recordswithoutsmokingstatusrecorded in the lastyear
have a sticker to remind GP to ask patient or icons flashing on
computer screen.
REVIEW Were the goals for improvement achieved?
(undertake a second audit)
• Repeattheauditinsixmonthstimewithadifferentgroupof
patients.
18 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
SECTION 3
Suggested Quality Improvement Topics
There are two frequently used classifications that describe the functions of a
practice:
Structure, process, outcome• 10.
Patient, professional and management quality• 11.
The most difficult part of a quality improvement activity can be choosing the topic.
Below is a list of suggested topics under the above classifications.
Structure (management quality)
The buildings, personnel, equipment and protocols that facilitate the process
of care.
Patient confidentiality in public parts of the practice is often difficult. Does the prac-
tice layout enhance patient privacy in the reception and waiting rooms12?
Are there adequate safeguards in the reception area to ensure confidentiality of •
information?
Do arrangements exist for private discussion with patients?•
Can phone calls in the reception area be heard by patients in the waiting room?•
Can reception staff observe patients in the waiting room whilst maintaining privacy •
of interactions and information?
Is there a phone available for private patient telephone conversations when •
needed?
Does your practice have a vision? Strategic planning is a participative process that
includes the whole practice team9. Successful planning is based on practical ex-
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 19
periences and contributions from all staff. Their ideas and opinions can contribute
in a practical way. For example, the reception staff may have noticed that patients
are distressed at the time they have to wait to see the GPs and have suggested a
better appointment system. The practice team can work together to develop the
best approach for all concerned.
What is the problem?•
Where is the practice now?•
Where do you want to be in the future?•
How will you get there?•
What are the goal posts?•
Good practice systems are important to the smooth functioning of the practice. Are
patient records and documents filed safely and securely12?
Are patient records and documents visible in public areas?•
Are patient records and documents visible in occupied consulting rooms?•
Are non-lockable files in staff areas only?•
Are practice staff aware of the practice policy on the storage and safety of documents?•
Are files secure or password protected when not in use?•
Emergency work is an important part of GP work. They must be ready and equipped
to administer first line treatment for medical emergencies. Therefore, it is important
that the contents of the doctors bag are current and complete12 .
Are you aware of the standard for a doctors bag?•
Do you have a list of the contents?•
Who is the person responsible for updating the contents of the bag?•
How regularly is the bag checked?•
Is there a system for checking?•
Is the bag kept in a place that is secure?•
Does each doctor have their own bag?•
20 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
Process (professional quality)
Concerned with the technical aspects of medical care, activities of a health system
or practitioner in the provision of care.
Do the records in your practice contain enough information to identify the
patient and to document the assessment, management, progress and out-
comes sufficiently for another doctor to carry on management12?
Is there sufficient information to identify the patient?•
Was the last consultation recorded adequately?•
Was the doctor making the entry easily identified?•
Are all current medications listed?•
Are problems and risk factors identified?•
Is there an adequate record of preventive services and options given?•
Coordinating care for patients who require cardiac rehabilitation13 – the primary
care setting often means GPs have to communicate with other health professionals
to ensure their patients have access to the care they need.
Can you identify the team members for coordinating cardiac care?•
Do each of the team members have a defined role that is understood by others?•
Is there a plan for care?•
How are the reporting structures defined?•
How does the feedback loop work?•
The incidence of tuberculosis in New Zealand is increasing14. Are you familiar with
the management principles for the treatment of tuberculosis?
What are the investigations needed to identify the organism and its sensitivity pattern?•
Can you identify patient compliance with medications?•
What is the treatment for suspected poor compliance or multi-drug resistance?•
Are you familiar with drug treatment regimes?•
What are the processes used to notify infectious diseases?•
How are infectious cases of tuberculosis isolated?•
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 21
The clinical management of diabetic patients should include appropriate observa-
tions that are recorded annually15.
Have you recorded:
weight•
smoking history•
fundoscopy (two yearly)•
foot examination•
cardiac risk•
BP•
lipids•
renal function•
HbA1c•
Falls are common amongst the elderly. By systematically taking into account the
following areas when seeing a patient after a fall, it may be possible to break the
falls/immobility cycle16 .
Did you identify and treat the cause of the fall?•
Is medication a reason for the fall?•
What are the environmental issues?•
Did you identify preventive aspects e.g. spectacles, walking aids?•
Will increased physical exercise make a difference?•
Outcome (patient quality)
A change in patient’s current or future health status (including; physical, psychological,
social health and behavioural), that can be attributed to previous care.
Communicating with patients – how good are your communication skills17?
Patient feedback is the best way to understand patient perceptions of your
communication skills.
Do patients think that you listen well?•
Do you avoid medical jargon?•
22 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
Do patients understand your explanations?•
Do your patients feel reassured?•
Are patients able to express their fears or concerns?•
Patient feedback is also a way of determining satisfaction with the level of service your
practice provides. How do patients perceive the service provided in your practice17 ?
How comfortable is the waiting room?•
Are staff trained to handle telephone queries in a discreet manner?•
Do patients have to wait long before they see a doctor?•
What are patient perceptions of the reception staff?•
Do patients know the cost of your service?•
Improving patient outcomes may depend on the way you interact or interpret patient
cues. Some patients have multifactors that are the cause of their ongoing problems.
Their situation or illness may be attributable to factors beyond their control, and
yours. However, there are ways of identifying and developing different strategies
for care to improve outcomes – even if they are not clinical outcomes18.
Can you identify criteria for patients in the practice who have challenging health •
issues or circumstances beyond their control?
Who and how many of these patients can you identify?•
Do these patients have common characteristics?•
Can you develop new strategies for managing patients e.g. developing better •
communication skills, improving your knowledge of health conditions?
Will referral to another service be more beneficial to an outcome?•
Can you link patients to community organisations that provide extra support?•
GP Audits
Self Care
To provide good patient care a GP should consider their own state of wellness, or
otherwise. Burnout is a common cause of many GPs losing control of a situation and
affects their personal and professional lives19.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 23
How do you rate your lifestyle? – Some studies found that GPs who felt in control of
their lives had developed coping strategies that worked19.
Can you identify imbalance in your life?•
Where are you in control?•
Where do you feel a loss of control?•
Do you participate in activities outside the practice?•
How much energy is spent on work activity by comparison with your own time?•
Self-prescribing19 – a study in the UK in 1993 found that 83% of GPs have
self prescribed their own medications. It is a practice that is easy to adopt
and can have harmful effects.
Are you aware of the dangers of self-prescribing?•
Can you describe your limits for self-prescribing?•
Do you discuss self-prescribing in a peer group situation?•
Do you have your own GP?•
24 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
Glossary
Aquickguidetoqualityjargon–thesedefinitionshavebeendraftedbytheRNZCGP
for use in quality related documents.
Acceptability
The profession as a whole regards the indicator and assessment method as acceptable20.
Accessibility
Services should be reasonably accessible when clinically needed. Necessary services
should be accessible to people regardless of age, sex, ethnicity, disability or health
status21.
Achievability
A set of minimum entry indicator standards must be achievable by general practice20.
Benchmark
Reference standards against which to compare results. These may be your own results
or another comparable population or national standard.
Clinical Audit
The measurement of an aspect of clinical care carried out by the practice team.
Continuous Quality Improvement
A culture that seeks never ending improvement of the whole system as part of normal
daily activity:
CQI Cycle: Topic ➙ Plan ➙ Data ➙ Check ➙ Action ➙ Review
Criteria
A discrete, definable, measurable and relevant component of a standard2.
Efficiency
Primary care services should be based on evidence of clinical effectiveness and resources
used efficiently21.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 25
Data Collection
The availability and accessibility of the required data elements; the cost and effort required
to extract or collect data22.
Fairness
Services should not vary widely in range or quality in different parts of the country21.
Feasibility
The process of practice assessment must be feasible in terms of its implementation and
the time and effort required20.
Guidelines
Systematically developed statements, which assist doctors and patients in making deci-
sions about appropriate treatment for specific conditions.
IPA
Independent Practitioners Associations.
Indicators
Measurable elements of performance selected (by evidence or by consensus) for as-
sessment of quality (and change in quality) of care provided.
Key performance indicator
Criteria against which achievement of goals is measured.
Minimum standard
The standard required to satisfy an authority, e.g. Medical Council, Accreditation.
Outcome
A change in patient’s current or future health status (including; physical, psychological,
social health and behavioural), that can be attributed to previous care.
Process
Concerned with the technical aspects of medical care, activities of a health system or
practitioner in the provision of care23.
Protocol
A detailed account of the planned process for a specific situation or condition.
26 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
Quality
The measurement and judgement of the technical and interpersonal aspects of care
(“excellence”, “fitness for purpose”, “minimal defects”). Is a commitment to a process
of continuous improvement.
Quality assessment
Systematic collection and analysis of data about a service, including content, process
(delivery) and outcomes.
Quality assurance
Planned activities based on performance review with the aim of continually improving
standards of care3.
Relevance
The applicability and/or pertinence of the indicator to its users and customers22.
Reliability
Behaves similarly under different circumstances20.
Responsiveness
Services that reflect the needs and preferences of the individuals using them and the
health demographic and social needs of the area they serve21.
Standard
Essentially a mark of success in achieving the criterion and specifies the acceptable
level of care3.
Strategic Plan
An organisation-wide plan establishing overall objectives.
Structure
The buildings, personnel, equipment and protocols that facilitate the process of care23.
TQM – Total Quality Management
An overall organisational culture and strategy for engendering and sustaining CQI.
Validity
The indicators adequately measured what they purport to measure – good practice?22.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 27
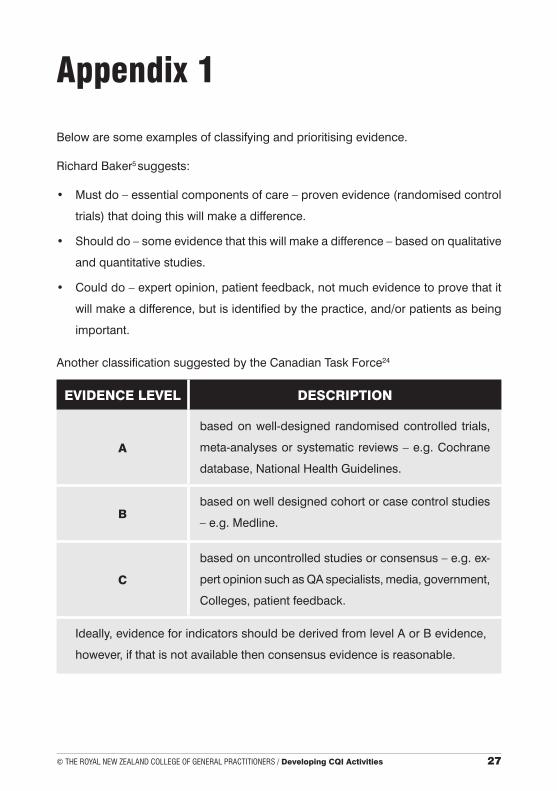
Appendix 1
Below are some examples of classifying and prioritising evidence.
Richard Baker5 suggests:
Mustdo–essentialcomponentsofcare–provenevidence(randomisedcontrol•
trials) that doing this will make a difference.
Shoulddo–someevidencethatthiswillmakeadifference–basedonqualitative•
and quantitative studies.
Coulddo–expertopinion,patientfeedback,notmuchevidencetoprovethatit•
will make a difference, but is identified by the practice, and/or patients as being
important.
Another classification suggested by the Canadian Task Force24
EVIDENCE LEVEL DESCRIPTION
A
based on well-designed randomised controlled trials,
meta-analysesorsystematicreviews–e.g.Cochrane
database, National Health Guidelines.
Bbased on well designed cohort or case control studies
–e.g.Medline.
C
basedonuncontrolledstudiesorconsensus–e.g.ex-
pert opinion such as QA specialists, media, government,
Colleges, patient feedback.
Ideally, evidence for indicators should be derived from level A or B evidence,
however, if that is not available then consensus evidence is reasonable.
28 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
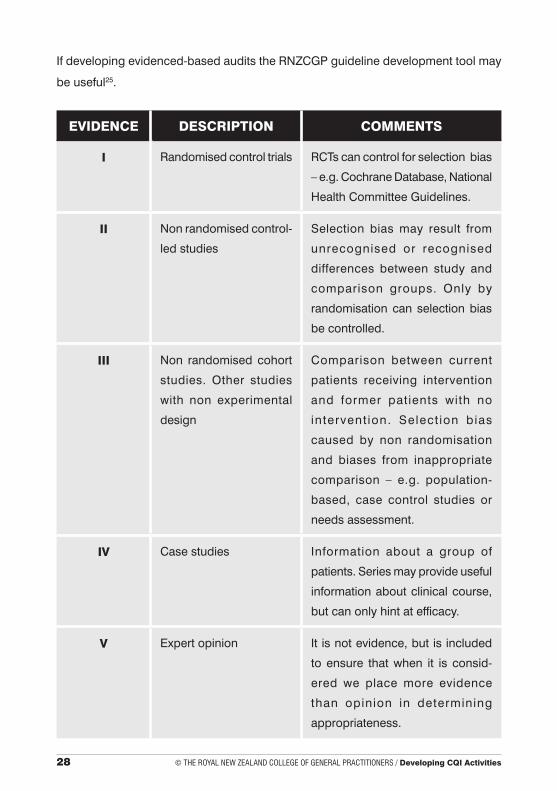
If developing evidenced-based audits the RNZCGP guideline development tool may
be useful25.
EVIDENCE DESCRIPTION COMMENTS
I Randomised control trials RCTs can control for selection bias
–e.g.CochraneDatabase,National
Health Committee Guidelines.
II Non randomised control-
led studies
Selection bias may result from
unrecognised or recognised
differences between study and
comparison groups. Only by
randomisation can selection bias
be controlled.
III Non randomised cohort
studies. Other studies
with non experimental
design
Comparison between current
patients receiving intervention
and former patients with no
intervent ion. Select ion bias
caused by non randomisation
and biases from inappropriate
comparison – e.g. population-
based, case control studies or
needs assessment.
IV Case studies Information about a group of
patients. Series may provide useful
information about clinical course,
but can only hint at efficacy.
V Expert opinion It is not evidence, but is included
to ensure that when it is consid-
ered we place more evidence
than opinion in determining
appropriateness.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 29
Appendix 2
Maintenance of Professional Standards (MOPS) Programme
MOPS credits
Credits
GPs can claim the following Continuous Quality Improvement (CQI) Activity credits
towards the Maintenance of Professional Standards programme (MOPS) once each
cycle has been completed.
Note: A cycle is defined as completing data, check, act and monitor stages. When
applying for credits each cycle can be treated as a separate exercise so it possible
to complete the first cycle in one triennium and the second in the next. However, it is
strongly recommended that you complete the whole cycle.
Claiming credits
In order to claim credits towards MOPS for completing these activities you are required
to write a summary of each activity completed.
Endorsement of CQI activities for the MOPS programme
If you have designed your own Continuous Quality Improvement Activity, you must
apply to the College for endorsement. For further information, you may contact the
Maintenance of Professional Standards Unit at the RNZCGP (04) 496 5999. When
applying for MOPS credits for an individually designed audit you must use the Re-
cording Sheet provided.
CQI Activity (completing the second audit)
Credits for a complete second audit may be claimed under the Continuous Quality
Improvement Activites section of the MOPS programme.
It is important that the whole process of check, action, monitoring progress in the first
audit has been undertaken as well as the second audit.
30 © THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities
References
1 Royal College of General Practitioners. Audit in practice, the 24 packages from
the working well in Tamar programme. Southampton, UK: RCGP; 1996.
2 Grol R, Lawrence M. Quality improvement by peer review: Oxford General Practice
Series 32. Oxford, UK: Oxford University Press; 1995.
3 Marwick J, Grol R, Borgiel A. Quality assurance for family doctors, report of the
QA working party. Wellington, NZ: World Organisation of Family Doctors, George
Jeffery & Co; 1992.
4 Lawrence M, Olesen F. Indicators of quality in health care, Equip working party
on indicators. European Journal of General Practice 1997 September; 3.
5 Baker R. Clinical audit in primary health care: towards quality assurance. British
MedicalJournal1995;310–413.
6 National Health Committee. Guidelines for smoking cessation. NZ: National Ad-
visory Committee on Health and Disability; July 1999.
7 Turner N. Medical audit workbook. Wellington, NZ: The Royal New Zealand Col-
lege of General Practitioners; 1994.
8 Baker R. Audit and quality. Notes from lecture tour of New Zealand. UK:University
of Leicester, 1996.
9 Smith D. Guidelines for strategic planning and goal setting in general practice.
Wellington, NZ: RNZCGP; 1994.
10 Donabedian A. Explorations in quality assessment and monitoring Vol 1, the
definition of quality and its approaches to its assessment. Ann Arbor, Michigan:
Health Administration Press, University of Michigan; 1980.
11 Øvretveit J. Health service quality, an introduction to quality methods for health
services. Oxford, UK: Blackwell Scientific Publications; 1992.
© THe Royal New ZealaNd College of geNeRal PRaCTiTioNeRs / Developing CQI Activities 31
12 The Royal New Zealand College of General Practitioners. Standards for general practice,
aiming for excellence in general practice. Wellington, NZ: RNZCGP; January 2000.
13 The Royal New Zealand College of General Practitioners. Cardiac rehabilitation.
Welllington, NZ: RNZCGP; 1998.
14 Ministry of Health. Guidelines for tuberculosis control in New Zealand. Wellington,
NZ: Public Health Group, MOH; 1996.
15 The Royal New Zealand College of General Practitioners. Diabetes pack. Wel-
lington, NZ: RNZCGP; 1993.
16 The Royal New Zealand College of General Practitioners. Care of the elderly. Wel-
lington, NZ: RNZCGP; 1996.
17 Client Focussed Evaluation Programme. Doctor’s interpersonal skills questionnaire
and better practice patient questionnaire. Australia: CFEP, Griffiths University; 1995.
18 The Royal New Zealand College of General Practitioners. Practical guide to audit.
Wellington, NZ: RNZCGP; 1997.
19 The Royal New Zealand College of General Practitioners. Self care for GPs. Wel-
lington, NZ: RNZCGP; 1998.
20 Royal Australian College of General Practitioners. Entry standards for general
practice accreditation. Australia: RACGP; 1996.
21 Department of Health. White paper, primary care: delivering the future. UK: Depart-
ment of Health; Dec 1996.
22 The Joint Commission of Accreditation of Health Care Organisations (JCAHO) in
the USA. National library of health indicators (NLHI), USA.
23 DonabedianA.Explorationsinqualityassessmentandmonitoring,Vols1–111.
Ann Arbor: Health Administration Press; 1985.
24 Lawrence M, et al. Canadian task force on indicators of general practice. Canadian
MedicalAssociationJournal1979;121:193–254.
25 The Royal New Zealand College of General Practitioners. Guideline package.
Wellington, NZ: RNZCGP; 1997.