desmoplastic supratentorial n euroepithelial tumor … · supratentorial n euroepithelial male...
TRANSCRIPT
Tiirkis/i Neiirosiirgery 11: 69 - 72, 2001 Toliiiiay: Desmop/astic Siipratentorial Neiiroepitlie1ia/ Tl/IIIOr
TumorReport
Supratentorial NeuroepithelialMale Infant: A Cas e
Desmoplasticin A 9-Month-Old
9 Aylik Infanti! Erkekte Desmoplastik SupratentoriyalNöroepitelyal Tümör: Olgu Sunumu
SAHSINE TOLUNA Y, GÜLA YDAN FILIZ, SONER SAHIN, KA YA AKSOY
Uludag Üniversity School of Medicine, Department of Patholoji (ST, GF) Neurosurgery (SS, KA) Bursa, Turkey
Received : 2.8.1999 ~ Accepted : 16.11.1999
Abstract: Desmoplastic infantile neuroepithelial tumors(DINTs) are superficially located supratentorial neoplasmsthat include masses known as "desmoplastic infantilegangliomas" (DIGs) and "desmoplastic infantileastrocytomas" (DIAs). Apart from the presence of ganglioncells in DIGs, these tumors and DIAs share the same features.Traditionally, tumors have been designated as DIAs onlywhen intensiye histological examination has revealed noganglion cells. Some DINTs show no ganglion cells onroutine staining with hematoxylin and eosin (HE), but arepositive for glial fibrillary acidic protein (GFAP), neuronspecific enolases (NSE), neurofilament protein (NF), andsynaptophysine on immunohistochemical staining.Currently, it is generally agreed that DIGs and DIAs arevariants of one type of tumor, and that both these forms ofneoplasia should be labeled DINTs. We deseribe the case ofa 9-month-old male infant who presented with progressivehead enlargement. The baby had a eystic, 8 cm-diameter,space-occupying lesion in his left parietal lobe that wassurrounded by edema. The mass was identified on cranialcomputerized tomography, and the patient underwent totaltumor excision. Microscopic examination of the massrevealed extensive desmoplasia and focal aggregations ofprimitive cells. Sections stained with HE showed no ganglioncells; however, immunohistochemical staining revealedwidespread GFAP positivity, and focal positivity for NSEand synaptophysine. The diagnosis was DINT. This reportdiscusses the clinicopathologic features of the case, andcompares our findings to those documented in previousreports of DIAand DIG attached to the dura.
Özet: Desmoplastik Infantil Nöroepitelyal Tümörler(DINT), Desmoplastik Infantil Gangliogliomalar 'DIG) veDesmoplastik Infantil Astrositomalar (DIA) olaraktabilinen yüzeyel yerlesimli supratentorial tümörlerdir.DIG'larda ganglion hücrelerinin bulunmasinin disinda buikitip neoplazi ayni özellikleri tasir. Bu tömürler dikkatlihistolojik incelemelere ragmen ganglion hücresibulunamaz ise DIA olark isimlendirilir. Bazi DINT'ler
Hematoksilen Eozin (H.E) ile rutin boyamalarda ganglionhücresi göstermez fakat Glial fibriler Acidie Protein(GFAP), Nöron Spesifik Enolaz (NSE), NöroflamentProtein (NF) ve Synaptofizin ile immunohistokimyasalboyamalarda pozitiflik gösterirler. Genelolarak kabuledilen görüs, DIG ve DIA'nin bir tip tümörün varyantiarioldugu ve bunlarin hepsinin DINT terimi altindatoplanmasi gerektigidir.
Key Words: DesmopIasia, embryonal neuroepitheliaItumors, infantile tumors
Anahtar Kelimeler: astrositoma, desmoplastik, infanti!ganglioglioma
69
Turkis/i Neurosurgery 11: 69 - 72, 2001
INTRODUCTION
Desmoplastic infantile neuroepithelial tumor(DINT) is a rare neoplasm of infancy that is typicallyseen in the early months of life (0-18 months). DINTsare usuaiiy solitary and tend to be located in thesupratentorial region, attached to the dura mater.Histopathologicaiiy, these masses are characterized bymarked desmoplasia, and some also have a componentof small, primitive, mitotically active cells. The latterfeature makes it easy to confuse some DINTs withmalignant neoplasms. Accurate diagnosis of DINT isessential because, although these tumors are rare andtend to be large, they take a benign course and this cangreatly? influence treatment decisions.
CASE REPORT
A 9-month-old male infant had been underobservation for pulmonary stenosis since birth at theUludag University School of Medicine pediatricclinic. The baby' s head had become noticeablyenlarged over a l-month period, and the parentsreported that he was vomiting and had developed afever. On admission, a physical examination revealedpurulent material the right ear, widespreadmaculopapular ski n eruptions, and an ejectionmurmur (2/6) in the pulmonary valve region. Aneurological examination showed somnolence, andincreased musele tone in both right limbs.
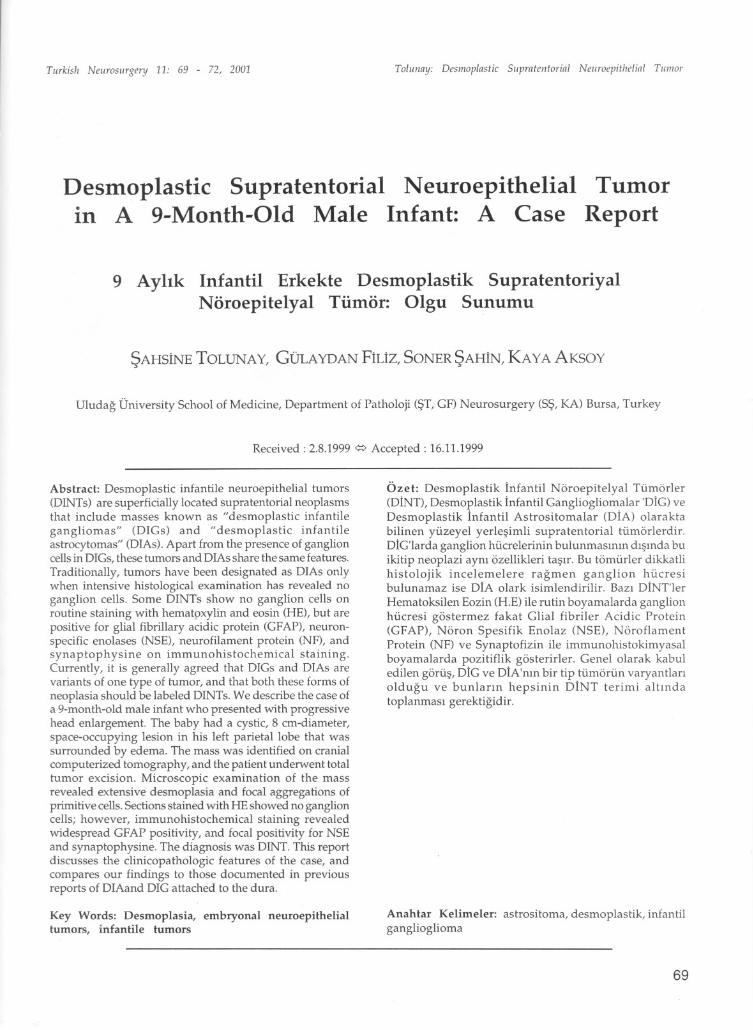
The only abnormal laboratory finding was awhite blood ceii (WBC) count of lS,OOO/pL.Cranialmagnetic resonance imaging (MRI) revealed a largeeystic mass with septae and peripheral edema. Thelesion was located in the left temporoparietal cortexand measured 8 cm in diamet~r (Figure 1). it wascompressing the left lateral ventriele, resulting in adisplacement of midline structures to the right andcausing hydrocephalus.
Based on clinical and MRI findings, and atentative diagnosis of brain abscess, we performedan emergency_burr hole aspiration with a 3 mmdiameter brain cannula for the diagnosis anddecompressive effect, was taken approximately 40ml eloudy, hemmorhagic, odorless fluid. Since thematerial did not match that expected with an abscess,5 days later we placed the patient under generalanesthesia and performed surgery through a leftfronto-temporal surgial approach. On opening thedura in this region, we found a firm mass attached.The neoplasm was easily separated from thesurrounding brain tissue and was totaiiy excised.
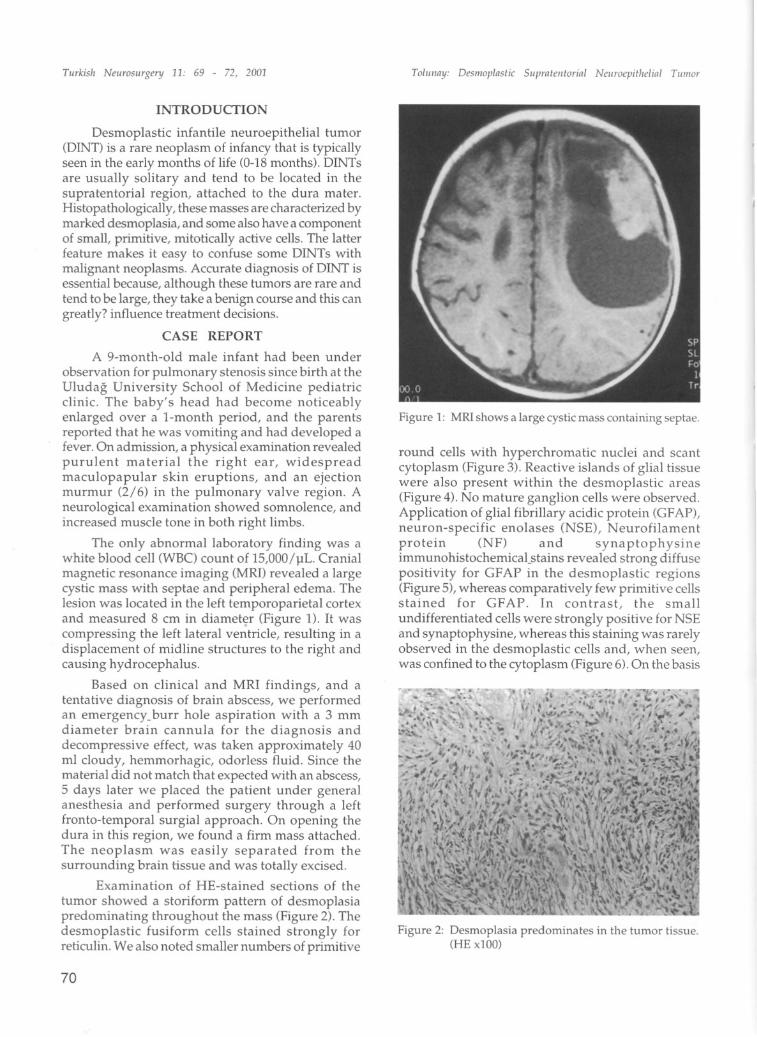
Examination of HE-stained sections of thetumor showed a storiform pattem of desmoplasiapredominating throughout the mass (Figure 2). Thedesmoplastic fusiform ceiis stained strongly forreticulin. We also noted smaller numbers of primitive
70
To/iiiiay: Desniop/nstic Suprateiitorin/ Neiiroepitlielin/ TimlOr
Figu re 1: MRI shows a large cystic mass con ta ining septae.
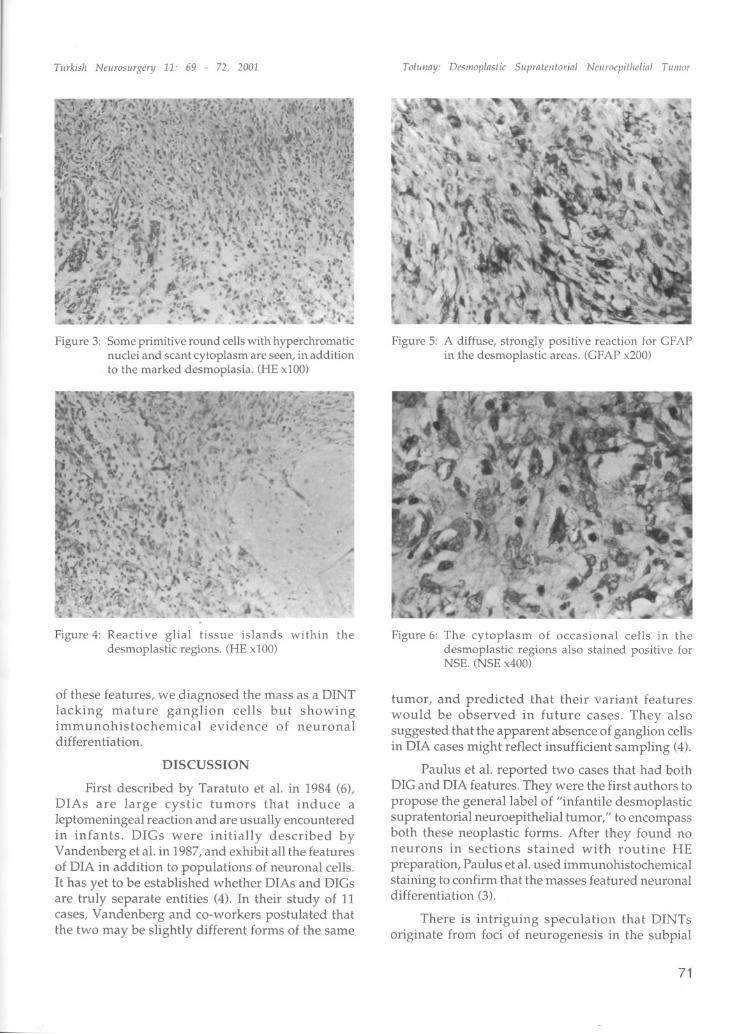
round cells with hyperchromatic nuelei and scantcytoplasm (Figure 3). Reactive islands of glial tissuewere also present within the desmoplastic areas(Figure 4). No mature ganglion ceiis were observed.Application of glial fibrillary acidie protein (GFAP),neuron-specific enolases (NSE), Neurofilamentprotein (NF) and synaptophysineimmunohistochemicatstains revealed strong diffusepositivity for GFAP in the desmoplastic regions(Figure S),whereas comparatively few primitive cellsstained for GFAP. In contrast, the smallundifferentiated ceiis were strongly positive for NSEand synaptophysine, whereas this staining was rarelyobserved in the desmoplastic cells and, when seen,was confined to the cytoplasm (Figure 6).On the basis
Figure 2: Desmoplasia predominates in the tumor tissue.(HE x100)
TiirkisJi Neurosiirgen) 11: 69 - 72, 2001
Figure 3: Some primitive round cells with hyperchromaticnuclei and scant eytopla sm are seen, in additionto the marked desmoplasia. (HE x100)
Figure 4: Reacti ve glial tissue islands within thedesmoplastic regions. (HE x100)
of these features, we diagnosed the mass as a DINTlacking mature ganglion cells but showingimmunohistochemical evidence of neuronaldifferentiation.
DISCVSSION
First described by Taratuto et aL. in 1984 (6),DIAs are large cystic tumors that induce aleptomeningeal reaction and are usually encounteredin infants. DIGs were initially described byVandenberg et aL.in 1987, and exhibit all the featuresof DiA in addition to populations of neuronal cells.it has yet to be established whether DlAs and DlGsare truly separate entities (4). In their study of 11cases, Vandenberg and co-workers postulated thatthe two may be slightly different forms of the same
Tolimny: Des/lloplnstic 511prnteiitorinl NeJlroepitJielinl Tli/IIor
Figure 5: A diffuse, strongly positive reaction for GFAPin the desmoplastic areas. (GFAP x200)
Figure 6: The cytoplasm of occasional cells in thedesmoplastic regions also stained positive forNSE. (NSE x400)
tumor, and predicted that their variant featureswould be observed in future cases. They alsosuggested that the apparent absence of ganglion cellsin DiA cases might reflect insufficient sampling (4).
Paulus et aL. reported two cases that had bothDIG and DiA features. They were the first authors topropose the generallabel of "infantile desmoplasticsupratentorial neuroepithelial tumor," to encompassboth these neoplastic forms. Af ter they found noneurons in sections stained with routine HE
preparation, Paulus et aL.used immunohistochemicalstaining to confirm that the masses featured neuronaldifferentiation (3).
There is intriguing speculation that DINTsoriginate from foci of neurogenesis in the subpial
71

Tiirkis/i Neiirosiirgery 11: 69 - 72, 2001
granular layer of the cerebral hemispheres. Inhumans, this celllayer starts to disappear at 8 monthsof gestation, but remnants of it have been found in thefrontallobes even at 6 months after birth. Due to their
large size, their pre-perinatal development, and theirundifferentiated nature, DINTs are considered
embryonal tUlllOrs (3,4). Unlike other poorlydifferentiated embryonal tumors of the central nervoussystem, the behavior of this tumor is not aggressive,and DINTs are generally seen in the first 18 months oflife. Grossly, the masses have a multiple eystic structureand are firm in consistency. Their significantmicroscopic features are the pres en ce of populationsof neuroepithelial cells and desmoplasia (1,2,3,4).
In addition to immature neuronal ce lls, some
reports on DIG have noted the presence of matureganglion cells. As Vandenburg et aL. proposed, thelack of neuronal differentiation in other cases maybe due to insufficient sampling and the paucity ofneoplastic neuronal components (2,4). However,another opinion is that the undifferentiated cells'potential for transformation may stop at the astrocyticline. This fits with the hypothesis that the neoplasticchange may begin in the fetal stages. if there isenough undifferentiated cellular material, this maylead to diffuse proliferation of desmoplastic cells andspread of the tumor to the leptomeninges. Spread tothe leptomeninges is seen in almost all patients, andis an important feature. As well, it is a trait commonto other desmoplastic tumorso The extensive fibroustissue may specifically originate from meningealfibroblasts, and may reflect the neoplasm's invasionof the leptomeninges.
A different theory concerning the origin of thisneoplasm is that aberrant metaplasia in the neoplasticglial cells may trigger the development of the fibroustissue. However, to date it has not been proven thatextracellular matrix material is produced in centralneuroepithelial tumors such as DIGs (1,2,3,4). Furtherstudy is needed in this regard.
The key issue in cases of DINT is accuratediagnosis. These tumors must be distinguished frommalignant neoplasms. In the past, DINTs have beenerroneously diagnosed as gliosarcoma, anaplasticastrocytoma, malignant meningioma, andleptomeningeal fibrosareoma (4). Information onpatient age, radiological features, histologicalfindings of marked desmoplastic and primitive cellcomponents, and immunohistochemical stainingtraits for GFAP, NSE, NF, and synaptophysineshould be assessed as a who le when attempting todifferentiate DINTs from malignant neoplasms.
72
To/iil1ny: Desl/iop!nstic Siiprnteiitorin! Neiiroepit/ielin! Tiil/lor
In general, DINT carries a good prognosis.However, the tumor's considerable bulk relative to
the small size of the infant brain can make surgicalintervention difficult, and this is the basis for the
considerable mortality risk (2,4). Apart from surgicalcomplications, the patient may develop seriousproblems with hydrocephalus, or brain edema andhemiation. if the mass can be totally excised,radiation and chemotherapy are not indicated.Postoperative disease-free survival of 14 years hasbeen report ed in excision cases (4).
CONCLUSION
DINT is a benign embryonal tumor that issuspiciously large and of ten appears malignant onhistopathological examination. Accurate diagnosis ofDINT is crucial in terms of treatment and prognosis,as these neoplasms can be easily confused withmalignancies. This case marks the first diagnosis ofthis type of tumor in our pathology department. Weview this description as a significant contribution tothe current literature on the basis of the rarity ofDINTs and the need for further information on their
clinical, radiological, and histopathological features.
Correspondence: Sahsine Tolunay
Uludag University Faeulty of MedicinePathology Department16059 Görükle
Bursa/TurkeyTel: 0.224- 4428850
0.224-4428400-1181Fax: 0.224-4428018
E-mail: [email protected]
REFERENCES
1. ChadarevianJP, Pattisapu JV, Faerber EN: Desmoplastieeerebral astroeytoma of infaney. Caneer 66: 173-179,1990
2. Duffner PK, Burger PC, Cohen ME, et al.: Desmoplastieinfantile gangliogliomas: An approaeh to therapy.Neurosurg 34: 583-589, 1994
3. Paulus W, Seholate W, Perentes E, et al: Desmoplastiesupratentorial neuroepithelial tumors of infaney.Histopathology 21: 43-49, 1992
4. Vandenberg SR, May EE, et al: Desmoplastiesupratentorial neuroepithelial tumors of infaney withdivergent differentiation potential (desmoplastieinfantile gangliogliomas). J. Neurosurg 66: 58-71, 1987
5. Serra A, Strain J, Stephanie R: Desmoplastie eerebra!astroeytoma of infaney. Report and review of theimaging eharaeteristies. AJR 166: 1459-1461, 1996
6. Taratuto AL, Monges J, Lylk P, et al: Superfieial eerebralastroeytoma attaehed to the dura. Report of six eases ininfants. Caneer 54 (ll): 2505-12, 1984