dermoscopic features of cutaneous rosai-dorfman disease
TRANSCRIPT

S
g
ha-
446 CASES AND RESEARCH LETTER
M.D. Fernández-Ballesteros,a,∗ Á. Vera-Casano,a
J. Escudero-Gómez,b A. Hiraldo-Gameroa
a Servicio de Dermatología, Hospital Materno InfantilCarlos Haya, Málaga, Spainb Servicio de Oftalmología, Hospital Materno InfantilCarlos Haya, Málaga, Spain
∗ Corresponding author.E-mail address: [email protected](M.D. Fernández-Ballesteros).
Dermoscopic Features of CutaneousRosai-Dorfman Disease�
Características dermatoscópicas de la
abnormalities in other organs were observed in the staginstudy.
Rosai-Dorfman disease, or massively enlarged lympnodes with sinus histiocytosis, is a histiocytic prolifer
elya-t
ic
als-y
al
etss-le
ei-hlss-e
r-sd-s-adti-
elynytfs
s-a.3
r-el-rs
ina
m-
s.g-er-th-sdd-see-eg-
enfermedad de Rosai-Dorfman cutánea
To the Editor:
Rosai-Dorfman disease is a benign histiocytic proliferativdisorder of unknown etiology. The presenting sign is usualasymptomatic massive lymphadenopathy. Exclusively cutneous cases of Rosai-Dorfman disease are rare. We presena case report of the disease and describe its dermoscopfeatures.
A 29-year old man with no relevant medical or surgichistory was seen for a lesion that had been growing progresively for several years in the left pectoral region. A biopsreport from another hospital indicated diagnosis of atypicxanthogranuloma.
The physical examination showed an infiltrated plaquwith a heterogeneous surface and well-defined borders. Ilongest diameter was 4.5 × 4 cm and it had an erythematouorange appearance, a central whitish area, and multipyellowish structures at the edges (Fig. 1).
The dermoscopic image showed a milky-red area in thcenter of the lesion, whereas the outer part had multple yellowish homogeneous areas of different sizes witirregular borders, surrounded by large telangiectatic vesseon a red-orange background (Fig. 2). Given the progresive growth of the lesion and the discomfort it caused thpatient, radical excision was performed.
Histologic examination revealed a poorly-defined demal proliferation of large histiocytes. extending downwardinto the subcutaneous adipose tissue. The histiocytes halarge eosinophilic vacuolated cytoplasm and round homogeneous nuclei and some contained intact lymphocyte(Fig. 3). In addition to the histiocytes, there was abundant inflammatory infiltrate composed mainly of plasmcells, with lymphocytes, giant multinucleated cells, anxanthomatous histiocytes with small nuclei. A prominenfibrous stroma was seen with a highly vascularized stor
form pattern. Immunohistochemical staining was positivefor S-100 and CD68 and negative for CD1a. The presence ofemperipolesis and the immunohistochemical profile pointedto diagnosis of a cutaneous variant of Rosai-Dorfman disease.No hematologic abnormalities, lymph node involvement, or� Please cite this article as: Avilés-Izquierdo JA, et al. Caracterís-ticas dermatoscópicas de la enfermedad de Rosai-Dorfman cutánea.Actas Dermosifiliogr. 2012;103:446-8.
in,9
ss
tion in which approximately 40% of the patients havextranodal involvement.1,2 The skin is the most frequentaffected organ. Purely cutaneous forms of Rosai-Dorfmadisease are rare. Skin lesions are nonspecific and matake the form of solitary or multiple lesions of differensizes and morphologies. They can present on any part othe body and the clinical differential diagnosis includea broad range of conditions including panniculitis, vaculitis, acne vulgaris, suppurative hidradenitis, granulomannulare, and sarcoidosis, as well as other histiocytosesKong et al.4 proposed a classification based on the mophologic features of 39 lesions. Papulonodular lesions werthe most common form (accounting for almost 80%) folowed by the infiltrated plaque type (12.5%) and the tumotype (7.7%). The histologic findings in cutaneous lesionare similar to those found in lymph tissue. The mafinding is a dense infiltrate of large histiocytes and
large pale cytoplasm with rounded nuclei. The cytoplascontains intact leukocytes, usually lymphocytes, a phenomenon known as lymphophagocytosis or emperipolesiTypically, these histiocytes are positive for S-100 and neative for CD1a, and can be either positive or negativfor CD68. The immunohistochemical profile is essential fohistologic diagnosis, as fibrosis, vascular proliferation, lymphoid clusters, foam cells, and multinucleated Touton giancells may or may not be present, and so confusion witother histiocytic processes, and with juvenile xanthogranuloma in particular, is possible.The dermoscopic featureof Rosai-Dorfman disease have not been widely reportein the literature.5,6 Rodríguez Blanco et al.6 reportea case of Rosai-Dorfman disease on the sole, characterized by cotton-like ovoid structures on an erythematoubackground in the dermoscopic image. In contrast, thdermoscopic features in our case were similar to thosdescribed for juvenile xanthogranuloma, that is, a yelloworange homogeneous central area and a somewhat morerythematous peripheral area. This is known as the settinsun feature.7 The presence of clouds of pale yellow globules is considered indicative of xanthomatous histiocytes
the superficial dermis.8 The presence of comma vesselsarborizing telangiectasia,10 and whitish linear projectionhas also been reported, particularly in advanced case
of juvenile xanthogranuloma. The differential dermoscopicdiagnosis should be performed with solitary yellow lesions,such as juvenile xanthogranuloma, organoid nevus or seba-ceous nevus, xanthomatous dermatofibroma, and solitaryreticulohistiocytoma.9---11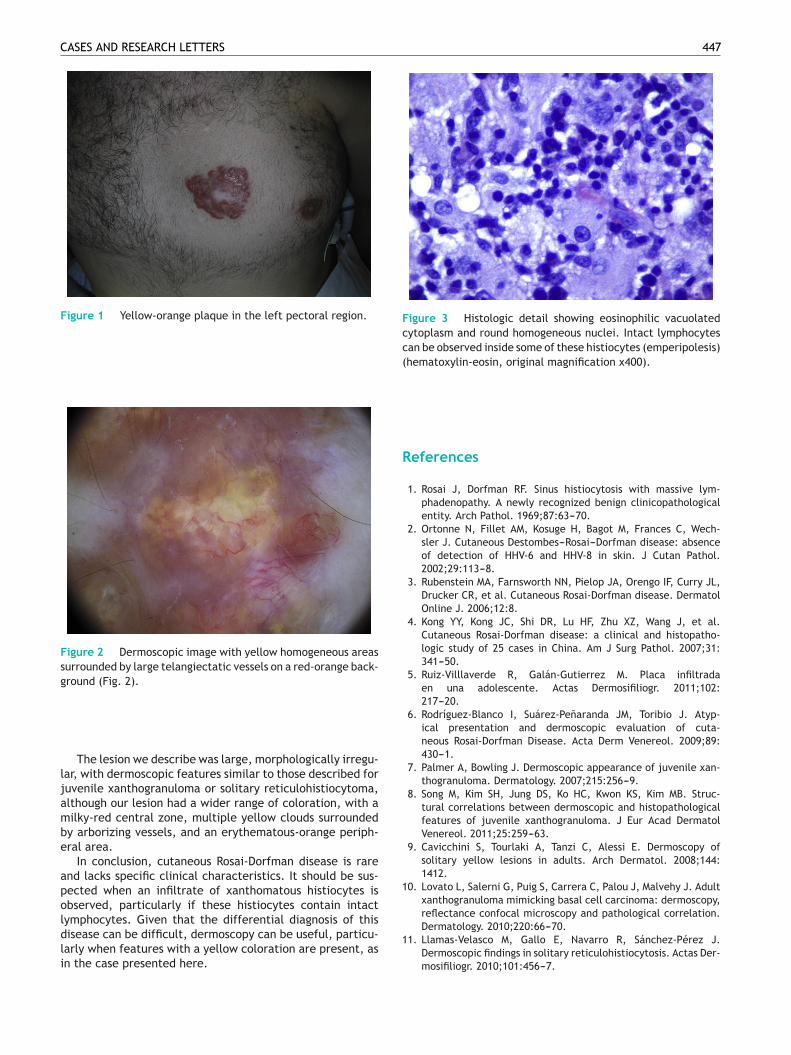
CASES AND RESEARCH LETTERS 447
Figure 1 Yellow-orange plaque in the left pectoral region.
Figsurgro
larjuvaltmibyera
anpeoblymdislarin
Figure 3 Histologic detail showing eosinophilic vacuolatedcytoplasm and round homogeneous nuclei. Intact lymphocytescan be observed inside some of these histiocytes (emperipolesis)(hematoxylin-eosin, original magnification x400).
Re
1.
ure 2 Dermoscopic image with yellow homogeneous areasrounded by large telangiectatic vessels on a red-orange back-und (Fig. 2).
The lesion we describe was large, morphologically irregu-, with dermoscopic features similar to those described forenile xanthogranuloma or solitary reticulohistiocytoma,hough our lesion had a wider range of coloration, with alky-red central zone, multiple yellow clouds surrounded
arborizing vessels, and an erythematous-orange periph-l area.In conclusion, cutaneous Rosai-Dorfman disease is rare
d lacks specific clinical characteristics. It should be sus-cted when an infiltrate of xanthomatous histiocytes isserved, particularly if these histiocytes contain intactphocytes. Given that the differential diagnosis of this
ease can be difficult, dermoscopy can be useful, particu-ly when features with a yellow coloration are present, asthe case presented here.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
ferences
Rosai J, Dorfman RF. Sinus histiocytosis with massive lym-
phadenopathy. A newly recognized benign clinicopathologicalentity. Arch Pathol. 1969;87:63---70.Ortonne N, Fillet AM, Kosuge H, Bagot M, Frances C, Wech-sler J. Cutaneous Destombes---Rosai---Dorfman disease: absenceof detection of HHV-6 and HHV-8 in skin. J Cutan Pathol.2002;29:113---8.
Rubenstein MA, Farnsworth NN, Pielop JA, Orengo IF, Curry JL,Drucker CR, et al. Cutaneous Rosai-Dorfman disease. DermatolOnline J. 2006;12:8.
Kong YY, Kong JC, Shi DR, Lu HF, Zhu XZ, Wang J, et al.Cutaneous Rosai-Dorfman disease: a clinical and histopatho-logic study of 25 cases in China. Am J Surg Pathol. 2007;31:341---50.
Ruiz-Villlaverde R, Galán-Gutierrez M. Placa infiltradaen una adolescente. Actas Dermosifiliogr. 2011;102:217---20.
Rodríguez-Blanco I, Suárez-Penaranda JM, Toribio J. Atyp-ical presentation and dermoscopic evaluation of cuta-neous Rosai-Dorfman Disease. Acta Derm Venereol. 2009;89:430---1.
Palmer A, Bowling J. Dermoscopic appearance of juvenile xan-thogranuloma. Dermatology. 2007;215:256---9.
Song M, Kim SH, Jung DS, Ko HC, Kwon KS, Kim MB. Struc-tural correlations between dermoscopic and histopathologicalfeatures of juvenile xanthogranuloma. J Eur Acad DermatolVenereol. 2011;25:259---63.
Cavicchini S, Tourlaki A, Tanzi C, Alessi E. Dermoscopy ofsolitary yellow lesions in adults. Arch Dermatol. 2008;144:1412.
Lovato L, Salerni G, Puig S, Carrera C, Palou J, Malvehy J. Adultxanthogranuloma mimicking basal cell carcinoma: dermoscopy,reflectance confocal microscopy and pathological correlation.Dermatology. 2010;220:66---70.Llamas-Velasco M, Gallo E, Navarro R, Sánchez-Pérez J.Dermoscopic findings in solitary reticulohistiocytosis. Actas Der-mosifiliogr. 2010;101:456---7.
S
ct
din
448 CASES AND RESEARCH LETTER
J.A. Avilés-Izquierdo,a,∗ V. Parra Blanco,b
F. Alfageme Roldána
a Servicio de Dermatología, Hospital General UniversitarioGregorio Maranón, Madrid, Spainb Servicio de Anatomía Patológica, Hospital GeneralUniversitario Gregorio Maranón’, Madrid, Spain
∗ Corresponding author.E-mail address: [email protected](J.A. Avilés-Izquierdo).
Erosive Palmoplantar Lichen Planus�
Liquen plano erosivo plantar
To the Editor:
Erosive palmoplantar lichen planus (LP), also known as ulcer-ative or bullous LP, was first described by Cram et al.1 in 1966as a rare variant of LP that can affect mucous membranes,palms, and soles. It presents clinically as erythematous,ulcerated plaques that run an extremely chronic course andare resistant to all types of treatment.
The patient was an 84-year-old woman with a per-sonal history of hypertension, aortic valve fibrosclerosis,and polyarthritis who had been receiving treatmentwith paracetamol, acetylsalicylic acid, atorvastatin, andcandesartan-hydrochlorothiazide for several years. She pre-sented with a very painful ulcerated lesion on her rightfoot that had appeared 6 months earlier and made walk-ing difficult. Physical examination revealed an ulceratedplaque, measuring 4 × 5 cm, on the medial aspect of theright heel. The base of the lesion was filled with granula-tion tissue, which in some areas was covered with whitish,macerated epithelium. Another ulcer with the same char-acteristics was present on the dorsal aspect of the firsttoe (Figs. 1 and 2). The dermatological examination alsorevealed the presence of whitish reticulated areas on thebuccal mucosa and pterygium on several fingernails. In addi-tion, the patient had total scalp alopecia, having lost herhair, as well as all 10 toenails, 6 years earlier. She didnot have alopecia of the eyebrows, eyelashes, axilla, orpubic area, or any other cutaneous abnormalities. Bloodtests, including liver function tests, hepatitis B serology, andhepatitis C serology, were normal or negative. Skin biopsyrevealed marked orthokeratotic hyperkeratosis, acanthosis,and a band-like lymphocytic infiltrate in the upper der-mis, without melanophages. Also present were spiculateddermal papillae and vacuolar degeneration at the dermal-epidermal junction. The findings were consistent with LP(Fig. 3).
On the basis of the clinical and histopathologic findings,the patient was diagnosed with erosive palmoplantar LP and
Figure 1 Absence of 5 toenails and ulcer on the dorsal aspeof the first toe similar to the ulcers on the heel.
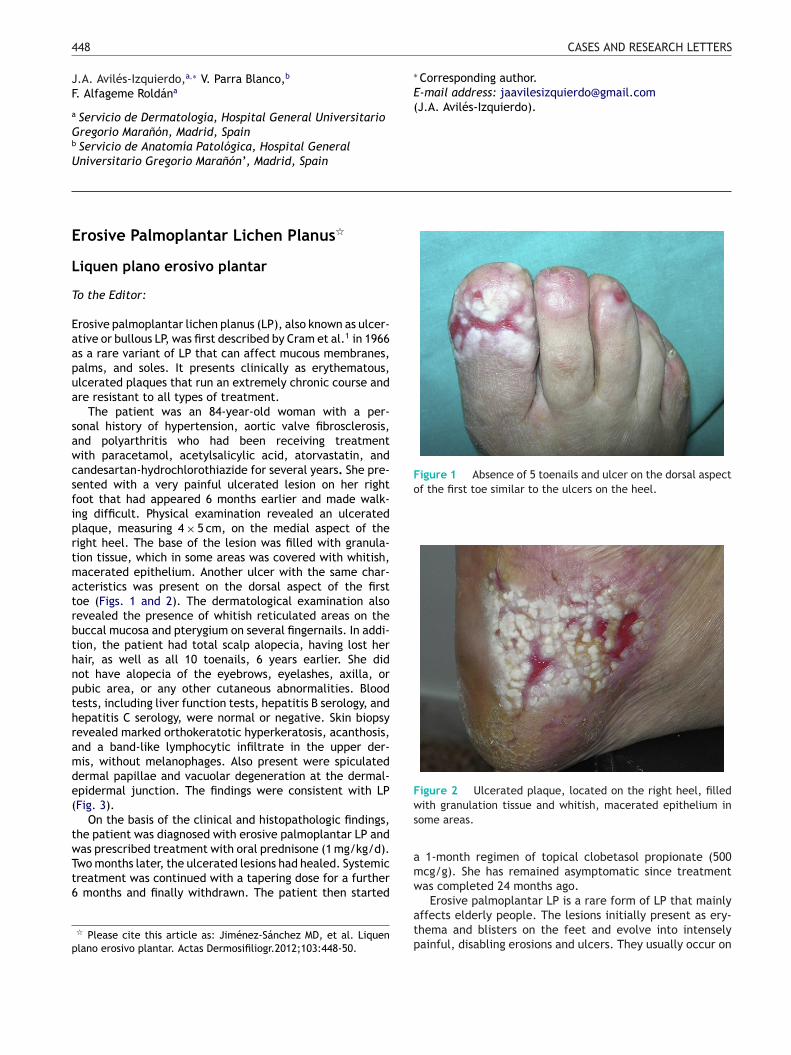
Figure 2 Ulcerated plaque, located on the right heel, fillewith granulation tissue and whitish, macerated epithelium
some areas.
was prescribed treatment with oral prednisone (1 mg/kg/d).Two months later, the ulcerated lesions had healed. Systemictreatment was continued with a tapering dose for a further6 months and finally withdrawn. The patient then started
� Please cite this article as: Jiménez-Sánchez MD, et al. Liquenplano erosivo plantar. Actas Dermosifiliogr.2012;103:448-50.
0t
a 1-month regimen of topical clobetasol propionate (50mcg/g). She has remained asymptomatic since treatmenwas completed 24 months ago.
Erosive palmoplantar LP is a rare form of LP that mainlyaffects elderly people. The lesions initially present as ery-thema and blisters on the feet and evolve into intenselypainful, disabling erosions and ulcers. They usually occur on