depressive symptoms in children and adolescents with cancer: a longitudinal study
TRANSCRIPT

Depressive Symptoms in Children and Adolescents With Cancer:A Longitudinal Study
STUART L. KAPl.AN, M,D" JOAN BUSNFR, PII.D" CHANTAL WEINHOLD, M,A" ANI> PAM LENON, PII,D.
Abstract, Seventeen adolescent oncology patients and ~ I childhood oncology patients were administered aself-report inventory of depression and a self-report psychosocial life events inventory three times at 4-monthintervals over a l-vcar period. The adolescent oncologic sample had a mean level of depressive symptoms that didnot differ from a general population sample of adolescents, The childhood oncologic sample had a mean level ofdepressive symptoms significantly lower than the reported mean of depressive symptoms for a general populationsample of the same age. Depressive symptoms were highly related to psychosocial life events. hut except fornumber of hospitalizations in the childhood oncologic sample, depressive symptoms were unrelated to the courseof the oncologic illness. .1 .uncr.. lead Child Adol. l'svchtat.. IlJX7, ~6, 5:7X~-7X7, Key Words: depression. cancer,psychosocial events.
The 5-year survival rate for childhood cancer has increasedfrom 2X~';, in I%0 to 61 ";, in IlJX2 (National Cancer Institute,19X5), The increase in the effectiveness of treating childhoodcancer is most dramatically illustrated by the survival rates inacute lymphocytic leukemia (ALI,). In 1960, the survival ratefor AlI. was 4";.; as of 19X2, the survival rate was 6X'.';(National Cancer Institute, 19X5). These dramatic increasesin survival rates have led those concerned with the psychological well-being of children and adolescents with cancer andtheir families to redirect their efforts to preparing these families for life with their children rather than preparing them toaccept the inevitability of their child's imminent death (Spineua. 19X2), The increased length of survival time has led tothe longitudinal study of several psychological issues. Spinnctact al, (197X, 19XI) longitudinally studied communicationpatterns and social support in children with cancer and theirfamilies. In general. they found that frequent. tactful. andhonest communication among the child, family, and caregiver promoted the psychological well-being of childhoodcancer patients and their families, whether or not the childsurvived, Koocher ct al. (llJXO), in a series of publicationsbased on a follow-up study of childhood cancer survivors intoearly adulthood, found a high percentage of psychologicaldisturbance in the survivors (Omalley ct al., 1(79). Theamount of psychological disturbance was not related to occultor visible physical disability in the survivors (Omalley ct al.19XO), Another series of investigations has examined cognitivedisability 1(IUnd in survivors as a result of the chemotherapyfor their oncologic illness. These studies have led to thepossibility of modifying chemotherapeutic regimens to optimize the intellectual functioning of childhood cancer survivors(Moss et al., IlJX I: Press, 19X4: Rowland ct al., 19X4).
There have been several studies of the point prevalence ofdepressive disorders in adult cancer patients and one suchstudy in children and adolescent oncology patients. In thelatter study, Kashani and l lakami (19X2), using DSM-1I1
Received Oct :!S, /1)Sf>. aCCI'II/I'd ,\'01' z« IYS(,.Dr. Kaplan is .tssociut« Chnual Protcssor otl'svchiatrv at Colum
hia L'nivcrsu v al/(II:"I'<'CI//l1'1' Director otRorkland Cluldrcn 'v l'svcluatric ('I'II/I'r, SCII' York Stat« OI/icl' ol.\/('//lall/l'l/llh. Dr. 1/111/;('1" il.:l.Isocwl,' I'IrchologlS1 at Rockland Children '.1 l'svchiatric ('I'II/I'rMr-: 11'l'illhold is Research Assistant and Dr. 1.1'1/11/1 is Biostatisticiunat l.oru; island Jewish .\fl'dical ('I'II/I'r. ,\'1'11' l lvdc Park, SI'\I' York.
Reprints I/wr I", rcqucstcd trom Dr. Kaplan. Rocklam! Children '.1
l'svchiutric Center, ('01l1"'11{ Road Orangcburv, N}' IINf>:!.OX9()-X56 7/X7/~6()5-07X~ $()~.()()/()( 19X7 bv the American Acad
cmv of Child and Adolescent Psychiatrv.
criteria and structured psychiatric interviews, found a pointprevalence of 17';;, for major depressive disorders that isgreater than the prevalence of X';;, found by Ruiter in the Isleof Wight Studies, which Kashani and Hakarni used as acomparison group.
We wished to study the levels and fluctuations ofdepressivesymptoms over time in a sample of child and adolescentoncology patients, along with the course of their illness andother life events, to explain the variance in their depressivesymptoms.
Method
POJlII/alion
The sample consisted of all patients between the ages of 7and IX years registered in the pediatric oncology service ofthe l.ong Island Jewish Medical Center, a university-affiliatedtertiary care center in suburban l.ong Island, New York,Children under the age of 7 were excluded because many ofthe measures required the ability to read. There were 41children and adolescents in the sample frame. Three subjectsrefused to participate in the study at its outset and would notgive the reasons for their refusal. This reduced the sample toJX patients. No new subjects were added to the study after itbegan.
At the time of the initial data collection, the adolescentsample consisted of 17 adolescents ranging in age from IJ toIlJ (X = 15.4 S.D. = I.X2). There were seven male and 10female subjects: the mean Hollingshead two-factor index ofsocial position (Hollingshead and Redlich, 195X) for the adolescent sample was 2.9 (S.D. = 0.75). Ten adolescents hadacute lymphocytic leukemia, three were in relapse, and sevenwere in remission, The seven in remission had had no relapses.Of the three subjects in relapse, two were having their firstrelapse and one was having his second relapse. The diagnosesof the remaining seven adolescents were: one malignant histiocytic tumor, one metastatic ovarian tumor, one stage IVmetastatic neuroblastoma, one stage I Hodgkins disease, onestage IIA Hodgkins disease, and one stage III Hodgkins disease. One adolescent's diagnosis could not be obtained. Theaverage number of hospitalizations was 5.0 (S.D. = J.O). Themean number of years since diagnosis for the adolescentsample was 2.07 years (S.D, = O.XO).
The childhood sample consisted of 21 children with a meanage of I}. 7 1 (S. D. = I. 52), rangi ng from 7 to I2 years. Therewere I I male and to female subjects, and the mean Hollings-
DI'PRI:SSIVI' SYMPTOMS AND CANCleR
TAIlI.I' 2. .ldole,IH'IIIS' 1',ITc!loSO(,{III/.tle 1"1'1'1/1 1I,'IIlS
Psychosocial events. ;\ vcrsive or negative life events arcsignificantly related to depression in physically healthy adultwomen, adolescents, children, and in physically ill adolescents(Finlay-Jones and Brown, Il./X I: Cirant ct al., Il./X I: Kaplan ctal., !l./X6: Lloyd, Il./XO: Paykcl ct al., 1l)6l./: Vinokur and Seller.1lJ75). The greater the number of aversive or negative lifeevents, the more likely the subject is depressed. Thus, ourstudy of the vicissitudes of depression in children and adolescent oncology patients required a life event measure to explaina portion of the variance of depressive symptoms. The Coddington Life Event Survey, the most widely reported measureof life events for children and adolescents, relics heavily onrarely occurring events such as parental death and divorce(Coddington, 1l./72: Heisel ct al., 1l./7.1). To assess the relationship between life events and fluctuations in depressive symptoms over short time spans. we were interested in events thatmight occur repeatedly during the l-ycar time span of ourstudy. Thus, we created an adolescent and a children's instrument that contained a variety of frequently occurring events(c.g .. argument with parents). From the 24 life event items ofour adolescent inventory, 10 items were retained for the dataanalysis on the basis of their high alpha coefficients: from the2l./ items of our children's inventory, seven items were similarly retained for the data analysis (sec Tables 2 and .1 foradolescents and children, rcspcctivelv.) The high internalcoherence of the items used made it statistically permissibleto combine them to ohtain a single life event score for each
head two-factor index of social position of the childhoodsample was .1.0 (S.D. = .7l./5), ranging from socioeconomicclass 2 to 4.
The average length of time since initial diagnosis was 2.4.1years (S.D. = 1.6l./). The average number of hospitalizationswas 5.1 (S.D. = .1.46).
Of the 21 children, 1X had acute lymphocytic leukemia:one was in relapse and the remaining 17 were in remission.The diagnoses of the remaining three patients were: om- acutemylcogcnous leukemia, one stage IV non-Hodgkins malignant lymphoma, and one malignant rncscnchyoma with metastasis.
The sample sill' at the three time periods and the reasonsfor the change in the sample size over the year of the studyare summarized in Table I.
lnstrumcnts
Beck Depression lnvcntorv The BOI (Beck ct al., I% I) isa widely used and well-studied clinical and research selfadministered measure of depression. It consists of 21 questions, and each question provides for a response of 0-\. Theo response means that the depressive symptom is not present:I means the symptom is present. and a 2 or .1 means thesymptom is severe. The total BDI score is the sum of theindividual items. ;\ total BDI score of 16+ has been validatedto he a cutoff score for major depressive disorder in adults(Burnbcrry ct al., 1l./7X) and adolescents (Strober et al., Il./X I).The BDI has been used in the study of depression in adultcancer patients (Plumb and Holland, 1l./77), in an epidemiological study of depressive symptoms in a general adolescentsample (Kaplan ct al., IlJX4), and in a study of depression inmedically ill hospitalized adolescents (Kaplan ct al., Il./X6).
Children's Depression lnvcntorv. The Children's Depression Inventory (CDI) (Kovacs and Beck, 1l./77) is a selfadministered measure of depression, based on the BDI anddesigned fix children aged X to 1.1.
It consists of 27 items, each rated on a scale from 0- 2: thehigher the rating, the more severe the symptom. Total scoresrange from 0-54. In a sample of X- to 1.1-year-old childrenwith major depressive disorder, the mean CDI score was 1.1.<1.1(S.D. = 6.6l./) (Kovacs, Il./X.1). The mean and S.D. from ageneral sample of third through sixth graders was X.67 (S.D.= 7.(2) (Smucker ct al., Il./X6). The instrument's test-retestreliability and internal consistency reliability arc reported tohe good (Smucker et al., Il./X6).
Items
My school grades have improvedI've failed to achieve something I've really
wantedI spend as much time with my friends as I
always haveMy boyfriend/girlfriend and I broke upMy best friend and I arc as dose as we've
always beenMy parents have had a hig argument1argue with my parents oftenMy family goes out as much as they always
have1go to as many parties as 1always haveI'm not as pleased with my appearance as I
used to he
Alpha Coefficients
Time I. (UnTime 2. 0,74Time 3. 0,:'1
TAIlI.I I. SIIIIl!lle Si :« ol( '11Ihl IIl1d .·ldole,lcelll Sample» III theThree IJIIIII Collection Points otth« Studv
"One child did not return questionnaire mailed to home: didcomplete the questionnaire tin time 3.
I< One adolescent moved and never returned questionnaire,'Two children died and two never returned mailed questionnaires."One adolescent died: three did not return mailed questionnaires:
one who did not return questionnaire was having a hone marrowtransplant. hut there is no known reason for the failure of the othertwo adolescents to return the questionnaire.
Item
Children': l'svchosocia! l.ik: Event Items
Alpha Coefficients
lime I. 0.70
Time 2. «.nTime 3. D.hl
TAIlII' 3.
I have failed a subject in school
I spend as much time with my friends as Ialways have
I'm as dose to my best friend as I've alwaysheen
I am aware that my parents have had a big
argumentMy family and I go out as much as we
always haveI go to as many parties as I always haveI'm not as pleased with rnv appearance as I
used to be
Adolescents
2120"17'
Children
Time ITime 2Time 3

KAPLAN LT AI..
TABU 5. Correlations of!Jef'!'('.\s/OI/ (rota! (DI Scores) JI'ithTotal l'svchosocial lrir F\'('II/s bv lillie 1/1 thildrcn
l.i1e Events
TABI I 4. Correlations otDcprcssion tlotal UIJI Scores) II 'ithrota! I'svrhosocial Lite F\'e/II Scor('.\ h.l' Time 1/1 Adolcscrnt»
Life l.vcnts
time I with life events at time 3. ,. = 0.73. fJ< 0.0 I: life eventsat time 2 with life events at time 3. ,. = 0.28. NS.) In children.only life events at times 2 and 3 were correlated significantly(r = 0.50. fJ < (l.(l5).
In adolescents. depressive symptoms as measured hy theBDt were highly related at all three points in time (BOI attime I with BOI at time 2. r = 0.X3. fJ < 0.0 I: BDt at time Iwith BDt at time 3. r = 0.86. fJ < 0.0 I: BDt at time 2 withBDt at time 3. ,. = 0.75. IJ < 0.(1). The data suggest that theBDt is a remarkably stable measure over time in this sample.
In children. depressive symptoms as measured by the CDtcorrelated significantly over the l-ycar span of the study. Theintercorrclations were weaker than the intcrcorrclations of theBOI in adolescents (COl at time I with COl at time 2. r =(),3X. NS: CDI at time I with CDt at time 3. ,. = 0.57. fJ <0.05: COl at time 2 with COl at time 3. ,. = 0.74. fJ < (l.OI).
In adolescents. BDt and life events were highly correlatedover the l-ycar period of the study. For adolescents. the largerthe number of negative life events and the smaller the numberof positive life events, the greater the depressive symptoms orthe higher the total BOI score (see Table 4). In children thecorrelational relationships between life event scores and theCDt were much weaker than the correlational relationshipbetween the BDt and life events in adolescents (see Table 5).In children only one of the nine possible correlations wassignificant. whereas in adolescents. seven of the nine possiblecorrelations were significant (see Tables 4 and 5).
The data analysis to this point entailed the use of total lifeevent scores. which were the algebraic sum of positive andnegative lite events for each subject at each time point. Tofurther assess the relationship between life events and BOIand life events and COl. two life event scores were calculatedfor each subject: a positive life event score and a negative lifeevent score. In both children and adolescents. depressivesymptoms were directly or positively related to negative liteevents and inversely or negatively related to positive lifeevents. Although this relationship was more powerful in theadolescent sample than in the child sample, the significantcorrelations in the child sample suggest that this relationship
subject. which could then he correlated with subjects' totaldepression score.
Positive. negative. or neutral valence was assigned to eachitem a priori. Each item required only a yes or no responseand inquired about the 4 months before the administrationof the questionnaire. As can he seen from Tables 2 and 3. theinventory asked about psychosocial lite events such as parental arguments. relationships with friends and parents. andsocial activity. Although these items can he influenced bycancer and its treatment. they seemed to he the type of eventsthat would lead to pleasant feelings or dysphoria in mostchildren and adolescents.
1/11/1'1\ ('I'('//{\, In contrast to psychosocial lite events. illnesslifi- events are lite events directly related to the illness and itsmedical treatment. They include: number of hospitalizations.rclap«: or remission status. length of time since diagnosis.number of weeks of treatment until remission fix those inremission. and number of relapses. To assess the amount ofvariance in depressive symptoms these events explained. weconsidered these lite events to he a distinct subgroup of liteevents.
Pn I( HIII,.('
Data were collected three times. at 4-month intervals. overthe course of a year. Outpatient subjects were approached inthe waiting room of the oncology clinic as they awaited theirmedical appointments. Informed consent was obtained fromthe parents and adolescents, and assent was obtained fromthe children. Subjects were brought individually to a quietroom where they completed the questionnaires. A femaleresearch assistant was present to answer any questions. Inpatient subject» were administered the questionnaires at theirbedsides. Occasionally. when no scheduled appointments fellclose to our -l-rnonth measurement interval. the questionnaires were mailed to subjects' homes.
Results
The HDI means of the adolescent sample at times I. 2. and3 were 7.1 (S.D. = 6.0. N = 16): 4.2 (S.D. = 3.X. S = 15):and 3.9 (S.D. = 4.0. i\' = 10): respectively. There were nosignificant differences between these scores and the mean BDIscore of 6.13 (S.D. = 5.72) of a control sample of 344adolescents drawn from high school students surrounding thehospital (Kaplan ct al., IllX4).
The CDI means of the child sample at times I. 2. and 3were 6.2 (S.D. = 4.6. N = 21): 5.9 (S.D. = 5.1. S = 20): and5.X (S.D. = 3.X. N = 17). respectively. We did not draw acomparison sample for this experiment group. However. eachof the three means is significantly lower ( I' < 0.(5) than thepublished mean CDI score of X.67 (S.D. = 7.(2) obtainedfrom an age-comparable general sample of 615 third throughsixth graders (Smucker ct al., 19X6).
One adolescent and two children died during the study.The adolescent had the following HDI score: time I. 9: time2. X. The two children who died had CDls at time I of 4 and6. and at time 2. 3 and 6. respectively.
In adolescents. lite events at time I were significantlyrelated to life events at time 2 and time 3. (I .ifc events at timeI with life events at time 2. ,. = 0.71. II < 0.0 I: life events at
BDI
Time ITime ::!rime 3
** I' < 0.01.
CDI
Timl'lTime ::!Time .1
"" n < 0.01.
Time I
-O.XO**-0.X1**-0.09""
Time I
-0..19-0.19-0.:\7
Time ::!
-0.4::!-0.59""-0.::!4
Time ::!
-0.05""-OAO-0.43
Time 1
-0.71""-0.7::!""-o.n""
Time 1
-0.::!90.11
-0.15
DEPR ESSIVE SYMPTOMS AN D rA NrER 7R5
TAIl 1.1' 7. Corrclatinn ofl 'ositivc and Negative /.iii' 1:' \'( ,tI!J WirhDepression 0,'('1' Time: Children
T A111.1 ' 6 . Corrctation lII'Positive 1I1ld Negative /.iii' I:" 'CIII.I ll 'i/IiJ) 1'11rI -JJillll Over Time: ..rd ll/I'J('('IIIJ
is found in the child sample as well as in the ado lescent sample(see Tables 6 and 7).
Cross-lagged Panel Correlation
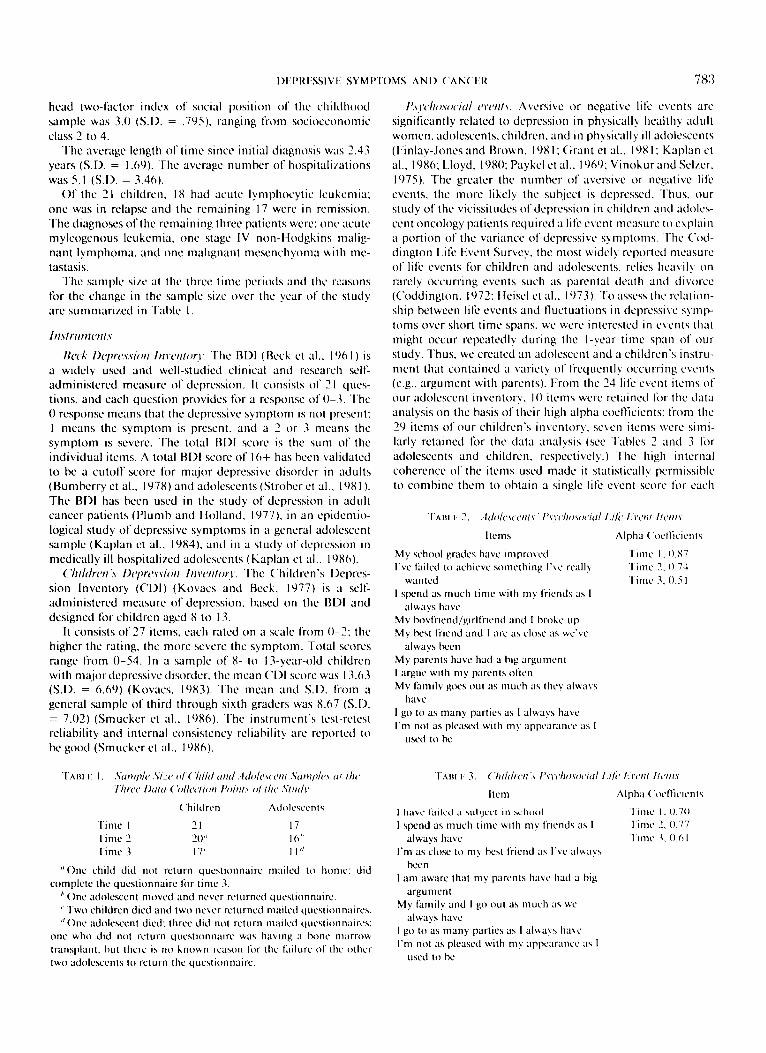
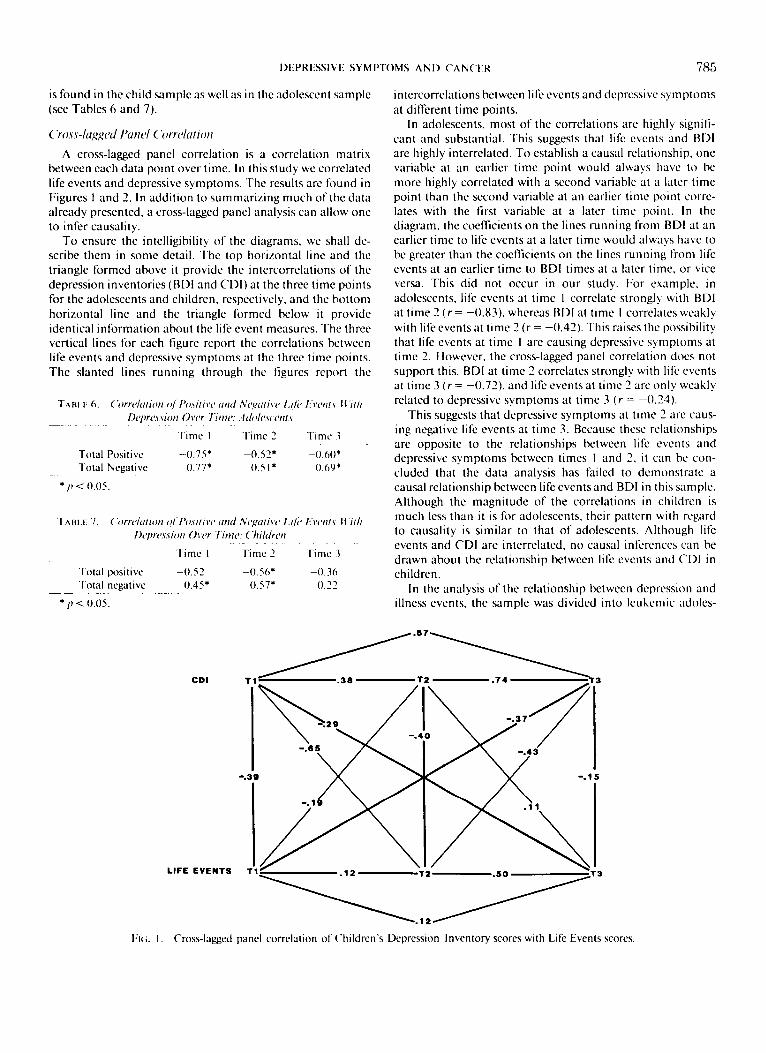
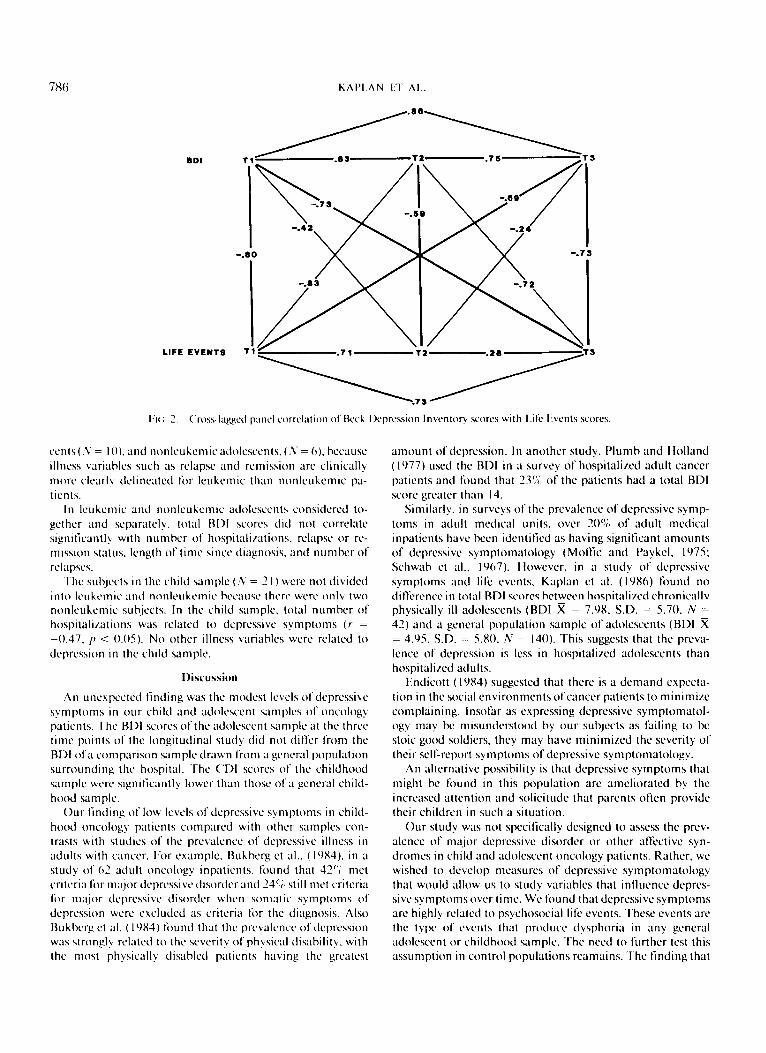
A cross -lagged panel co rrelation is a co rrelation matrixbetween each data point over tim e. In th is study we correlatedlife events and depressi ve sympto ms . Th e results are found inFigures I and 2. In addit ion to sum ma rizing much of the dataalready presented. a cross-lagged pan el ana lysis can allow oneto infer ca usa lity.
To ensure the intelligibility of the diagram s. we shall describe them in some det ail. Th e top hor izontal line and thetr iangle formed abo ve it pro vide the inte rcorrelat ion s of thedepression inventories (BOI and C Ol ) at the three time pointsfor the adolescents and children. respectively . and the hottomhorizontal line and the triangle formed below it provideident ical information about the life event measures. The threevert ical lines for each figure report the correlations betweenlife events and depressive symptom s at the three time points.Th e slanted lines running th rou gh the figures report the
intercorrela tions between life eve nts and de pressive sympto msat d ifferent time point s.
In ado lescents. most of the correla tio ns are highly significant and substantial. Thi s suggests that life events and BOIare highly interrelated. To establish a causa l relati on ship . onevariab le at an earlier tim e point would always have to hemore highly correlated with a seco nd variable at a later tim epoint than the second variable at an earlier t ime point co rrelates with the first variable at a later tim e point. In thed iagram . the coe ffic ients on the lines runn ing from BOI at a nearl ier time to life events at a later time would always have tobe greater than the coefficient s on the lines runn ing from lifeevents at an earlier tim e to BOI tim es at a later time. or viceversa. This did not occur in our study. For example. inado lescents. life events at time I correlate strongly with BOIat time 2 (r = -0.83). whereas BOI at time I correlates weakl ywith life events at time 2 (r = -0.42). This raises the possihil itythat life events at time I arc causing depressive symptoms attime 2. However. the cross-lagged panel correlation does notsuppo rt thi s. BOI at time 2 correlates strongly with life eve ntsat time 3 (r = -0.72 ). and life eve nts at tim e 2 are only weaklyrelated to depressive symptoms at time 3 ( r = - 0.24).
T his suggests that depressive sym pto ms at time 2 are ca using negati ve life events at time 3. Becau se these relation shipsarc opposi te to the relat ion shi ps between lite events anddepressive sym ptoms between times I and 2. it can he con cluded that the data ana lysis has failed to dem on strate acausal relati on ship between life eve nts and BOI in this sam ple.Although the magnitude of the correlations in children ismu ch less than it is for adolescen ts. their pattern with regardto causality is similar to that of adolescent s. Although lifeevents and COl are interrela ted. no ca usal inferences can bedrawn about the relationship betwee n life events and C Ol inchild ren.
In the analysis of the relat ion shi p between depression a ndillness event s. the sample was di vided int o leukemic ado lcs-
- O.J 60.22
- 0 .60"0 .69"
T ime .\
Ti me :I
- 0.56*0 .57*
Ti me 2
- 0.52"0.5 1*
Time 2
- 0.75"0 .77*
Time I
- 0.52OA5"
T ime I
To tal PositiveTo tal Negative
* I' < 0.05.
To tal posit iveTo tal negat ive
" fI < 0.05 .
CD'
LIFE EVENTS
-.311 -.15
------:::,'T3
rl( ;. I. Cro ss-lagged panel co rrelation of Children 's Dep ression Inventory scores with Life Events scores.
7!i1i KAPLAN IT AI..
BDI T1 .83
~"-.42
-.80 -.73
-.83
~LIFE EVENTS T1 .71 T3
.73
1:)(;.2. Cross-lagged panel correlation of Beck Depression Inventory scores with l.ife Events scores.
cents (S = 10), and non leukemic adolescents, (S = 6), becauseillness variables such as relapse and remission are clinicallymore clearly delineated for leukemic than non leukemic patients.
In leukemic and non leukemic adolescents considered together and separately, total BDI scores did not correlatesignificantly with number of hospitalizations. relapse or remission status, length of time since diagnosis, and number ofrelapses.
The subjects in the child sample (S = 21) were not dividedinto leukemic and nonlcukcmic because there were only twonon leukemic subjects. In the child sample, total number ofhospitalizations was related to depressive symptoms (,. =-OA7, II < 0.(5). No other illness variables were related todepression in the child sample.
Discussion
An unexpected finding was the modest levels of depressivesymptoms in our child and adolescent samples of oncologypatients. The RDI scores of the adolescent sample at the threetime points of the longitudinal study did not differ from theBDI of a comparison sample drawn from a general populationsurrounding the hospital. The CDI scores of the childhoodsample were significantly lower than those of a general childhood sample.
Our finding of low levels of depressive symptoms in childhood oncology patients compared with other samples contrasts with studies of the prevalence of depressive illness inadults with cancer. For example, Bukbcrg et al., ( 19X4), in astudy of 62 adult oncology inpatients, found that 42"; metcriteria for major depressive disorder and 24"; still met criteriafor major depressive disorder when somatic symptoms ofdepression were excluded as criteria for the diagnosis. AlsoBukbcrg ct al. ( 19X4) found that the prevalence of depressionwas strongly related to the severity of physical disability. withthe most physically disabled patients having the greatest
amount of depression. In another study, Plumh and Holland(1977) used the ADI in a survey of hospitalized adult cancerpatients and found that 23'};, of the patients had a total BDIscore greater than 14.
Similarly, in surveys of the prevalence of depressive symptoms in adult medical units, over 20'/;, of adult medicalinpatients have been identified as having significant amountsof depressive symptomatology (Moffic and Paykcl, 1975:Schwab ct al., 19(7). However, in a study of depressivesymptoms and lite events, Kaplan ct al. (19X6) found nodifference in total RDI scores between hospitalized chronicallyphysically ill adolescents (BDI X = 7.9X, S.D. = 5.70, N =42) and a general population sample of adolescents (ADI X= 4.95, S.D. = 5.XO, N = 140). This suggests that the prevalence of depression is less in hospitalized adolescents thanhospitalized adults.
Endicott ( 19X4) suggested that there is a demand expectation in the social environments of cancer patients to minimizecomplaining. Insofar as expressing depressive symptomatology may he misunderstood hy our subjects as failing to hestoic good soldiers, they may have minimized the severity oftheir self-report symptoms of depressive symptomatology.
An alternative possihility is that depressive symptoms thatmight be found in this population are ameliorated hy theincreased attention and solicitude that parents often providetheir children in such a situation.
Our study WaS not specifically designed to assess the prevalence of major depressive disorder or other affective syndromes in child and adolescent oncology patients. Rather, wewished to develop measures of depressive symptomatologythat would allow us to study variables that influence depressive symptoms over time. We found that depressive symptomsare highly related to psychosocial life events. These events arethe type of events that produce dysphoria in any generaladolescent or childhood sample. The need to further test thisassumption in control populations rcarnains, The finding that

DEPRESSIVI SYMPTOMS AND CANCER 787
the CDt in the childhood sample was also related to psychosocial events, although less strongly than in the adolescentsample, lends support to the concept that psychosicial liteevents are an important source of variance of depressivesymptoms in child and adolescent oncologic populations. Ourstudy provides evidence for this in two different-aged samples,using two different sets of instruments.
Our finding that illness events are unrelated to depressivesymptoms is much more tentative. First, the finding is counterintuitive. Health care providers of these patients understandahly regard the patient's health status such as relapseand remission or need for further hospitalization as crucialissues, and they seem to assume that these variahles wouldhave a major influence on the patients' morale or levels ofdysphoria. Our findings do not support this reasonable assumption in children and adolescents. This finding againseems discrepant from clinical experience and must he replicated. Rather. children and adolescent oncology patients seemto he dysphoric ahout the same issues as other children andadolescents.
The finding that psychosocial life events account for animportant part of the variance of depressive symptoms inchildren and adolescents supports the importance of psychosocial interventions in these samples. Because psychosocialevents are strongly related to depressive symptoms. dysphoriain these samples is not at the mercy of biological fate, hutrather might he able to he influenced by appropriate psychotherapeutic intervention.
References
Beck, A. '1'., Ward. C. II., Mendelsohn, M., Mock, J. & l.rbaugh, J.(1911 I). An inventory for measuring depression . ..trch. Gen. Psvchial.4:561-571.
Bukbcrg, J .. Penman, D. & Holland. J. C. (19X4), Depression inhospitalized cancer patients. Psvchosom Mcd.. 46: 199-212.
Burnbcrry, W., Oliver, J. M. & McClure. J. N. (197X), Beck Deprcssion Inventory in a university population using psychiatric estimateas the criterion . .I. COlIsIIII. Clin. l'svchol.. 46: 150-155.
Coddington, R. D. (1972). The significance of life events as etiologicfactors in the diseases of children, II: a study of a normal population. l'svchosom. Rl'I .. 16:205-211.
Endicott. J. (May 15, 19X4). Measurement of depression in patientswith cancer. Cancer, (Suppl.:2241-2249.
Hnlay-Joncs. R. & Brown, (;. W. ( 19Xl ). Types of stressful life eventsand the onset of anxiety and depressive disorders. l'sychol. .l/cd.II :XOJ-X 15.
Grant. I.. Swcctwood, II. 1.., Yager, J. & Gerst, M. ( 19XI ). Quality oflife events in relation to psychiatric symptoms...Ink (jm. I'srchiat.. 1X:115-119.
Heisel, J. S.. Ream, S., Raitz, R., Rappaport, M. & Coddington. R.D. (197:1). The significance of IiIi: events as etiologic factors in thediseases of children. III: a study of pediatric patients. J l'cdiut,X1:119-12.l
Hollingshead. A. B. & Redlich, F. C. (195Xl. Social Class and MCII/alI/II1CSS. New York: Wiley.
Kaplan, S. 1.., Grossman. P., Landa. B., Shenker. I. R. & Weinhold.C. (19X6). Depressive symptoms and life events in physically illhospitalized adolescents. .I. . Idol. II/Ih. Care. 7: 107-II I.
-- Hong, G. K. & Weinhold. C. (19X4), Epidemiology of depressivesymptomatology in adolescents. This Journal, 21:91-9X.
Kashani. J. & l lakarni, N. (19X2), Depression in children and adolescents with malignancy. CWIlIl/. Psvchiat .. D:474-477.
Koochcr, G. P., Omalley, J. L, Gogan. J. I.. & roster. D. J. (19XO),Psychological adjustment among pediatric cancer survivors. .I.Child Psvchol. l'svchiat., 21: 161-171.
Kovacs, M. (19X1). The Children 's Depression Invcntorv a sclt-ratcddepression scale jill'. school-uged .l'lIIl/1gsICT,I. U npublished manuscript. University of Pittsburgh School of Medicine.
-- Beck, A. T. (1977). An empirical clinical approach towards adefinition of childhood depression. In: Depression ill Children. cd.J.G. Schultebrant & A. Raskin. New York: Raven Press. PI'. 1-25.
Lloyd, C. (19XO), Life events and depressive disorders reviewed, II,events as precipitating factors . Arch. (jm l'svchiut.. 17:541-54X.
Mollic, II. & Paykel, E, S. (1975), Depression in medical inpatients.u-« .I. l'svchiat. 126:146~.151.
Moss, II, A., Nannis, E, D. & Poplack. D. G. (19X I). The effects ofprophylactic treatment of the central nervous system on the intellectual functioning of children with acute lymphocytic leukemia.Amcr]. st.«. 1:119-1211.
National Cancer Institute, Surveillance and Operations ResearchBranch (19X5). Annual CawCT Stutistics RI'I'/CII' (National Institutcs of Health Publication #X6-DX9). Rockville, Md.: Author.
Omalley, J. E., Foster, D., Koocher. G. & Slavin. I.. (19XO). Visiblephysical impairment and psychological adjustment among pediatric cancer survivors. ..1I11CT. l'svchiat .. 117:94-96.
-- Koochcr, G. Foster, D. & Slavin, I.. (1979), Psychiatric sequelaeof surviving childhood cancer. .'tmcr J Orlhop.ITchial .. 49:60X6111.
Paykel, L J.. Myers, J. K., Dicncit. M. N., Klcrrnan. C. 1.., Lindenthai, J. J. & Pepper, M. P. (1969), l.ifc events and depression: acontrolled study... Ink (jcll l'svchiut, 21 :751-760.
Plumb, M. J. & Holland. J. (1977). Comparative studies of psychological function in patients with advanced cancer. I. self-reporteddepressive symptoms. Psvchosom. sted., 19:264-D6.
Press, M. (19X4), Damage to the developing brain and subtle psychiatric consequences: the case of Milton. In: Childhood Cancer:Impact Oil the Family. cd, A.L Christ & K. Flomcnhaft. NewYork: Plenum Press.
Rowland. J. H., Glidewell. O. J.. Sibley, R, F., ct al. (19X4), Ellectsof different forms of central nervous system prophylaxis on ncuropsychologic function in childhood leukemia. Clin Oneal..2:UD-IJJ5.
Schwab, J. J.. Bialow, M., Brown, J. M. & 1I01zer, C. L (1967).Diagnosing depression in medical inpatients, .:11111. 1111. ,\fcd..67:695-707.
Smucker, M. R., Craighead. W. E., Craighead, I.. W. & Green, B. J.( 19X6). Normative and reliability data for the children" DepressionInventory, .I. ..11>1101'.111. Child 1'.ITChol., 14:25-19.
Spinctta, J. J. (19X2), Behavioral and psychological research in childhood cancer: an overview. Cancer. 50: 1919~ 194.l
-- Deasy-Spinctta. P. ed. (19X I). Living with Childhood Cancer.SI. Louis, Mo.: C.V. Mosby.
-- Maloney. I.. J. (197X). The child with cancer: patterns ofcommunication and denial. .I. ('(//1.11111 Clin. l'sychol.. 4X:15401541.
-- Swasncr, J, A. & Shcposh, J. P. (19X I), Effective parental copingfollowing the death of a child from cancer. .I. Pcdiut l'svchol..6:251-261.
Strober, M.. Green, J. & Carlson, G. (19X I), Utility of the BeckDepression Inventory with psychiatrically hospitalized adolescents..I. COIISIIII. CIiIl Psycho!.. 49:4X2-4X1.
Vinokur, A. & Selzer, M. I.. (1975), Desirable versus undesirable lifeevents: their relationship to stress and mental distress. .I. Pcrs. Socl'svchol.. 12:129-JJ7.