data collection guide direct data submission...
TRANSCRIPT
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 1
DATA COLLECTION GUIDE
Direct Data Submission
Depression Care Measures 2014 (02/01/2013 to 01/31/2014 Dates of Service)
Changes from Draft Data Collection Guide: 1. Updated Evaluation & Management CPT Codes found on Page 19. Please note: These are optional codes
that can be used to identify visits.
2. Depression PHQ-9 Follow-up Assessment at 6-months and 12-months measures are publicly reported as of September 2013. These measure results have been available privately to medical groups via the MNCM Data Portal since the inception of Depression Care data collection (2009). They are two of 10 available Depression Care measures and revisions have been made to Appendix F to indicate they are publicly reported measures.
3. Medical groups can upload denominator counts and information OR they can enter information directly into the data portal. See pages 34-35 for more information.
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 2
Table of Contents
Overview of the Process and Timeline ............................................ 3
Measure Specifications .................................................................. 4
Major Depression and Dysthymia Diagnosis Codes .....................................................................................6 Table 1: ICD-9 Diagnosis Codes for Identifying Major Depression or Dysthymia ............................................................... 6
Codes Used to Identify Patients who Meet Exclusion Criteria ......................................................................7 Table 2: ICD-9 Diagnosis Codes for Identifying Patients Meeting Exclusion Criteria ......................................................... 7
Measure Logic/Flow Charts ........................................................................................................................9
Data Collection and Submission Instructions ................................ 12
Data Collection and Submission Preparations and Considerations: ............................................................ 13 Section A: Identifying the Patient Population (Denominator) .................................................................... 16 Section B: Clinic Level Population Counts .................................................................................................. 21 Section C: Data Collection ........................................................................................................................ 23
Data Elements and Field Specifications ............................................................................................................................ 26 Section D: Patient Data File Creation ........................................................................................................ 32 Section E: Patient Data File Submission .................................................................................................... 34 Section F: MNCM Validation ..................................................................................................................... 38
Appendices .................................................................................. 40
Appendix A: Registration on the MNCM Data Portal ................................................................................. 41 Appendix B: Resources to Help You Get Started ........................................................................................ 42 Appendix C: Timelines for Data Submission and Public Reporting .............................................................. 43 Appendix D: Notes about the PHQ-9 Test ................................................................................................. 45 Appendix E: Explaining the Depression Measures to Providers and Clinical Staff ........................................ 46 Appendix F: Suite of Available Depression Care Measures ......................................................................... 47 Appendix G: About MN Community Measurement and Measure Development ......................................... 51 Appendix H:About Direct Data Submission ....................................................... Error! Bookmark not defined.
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 3
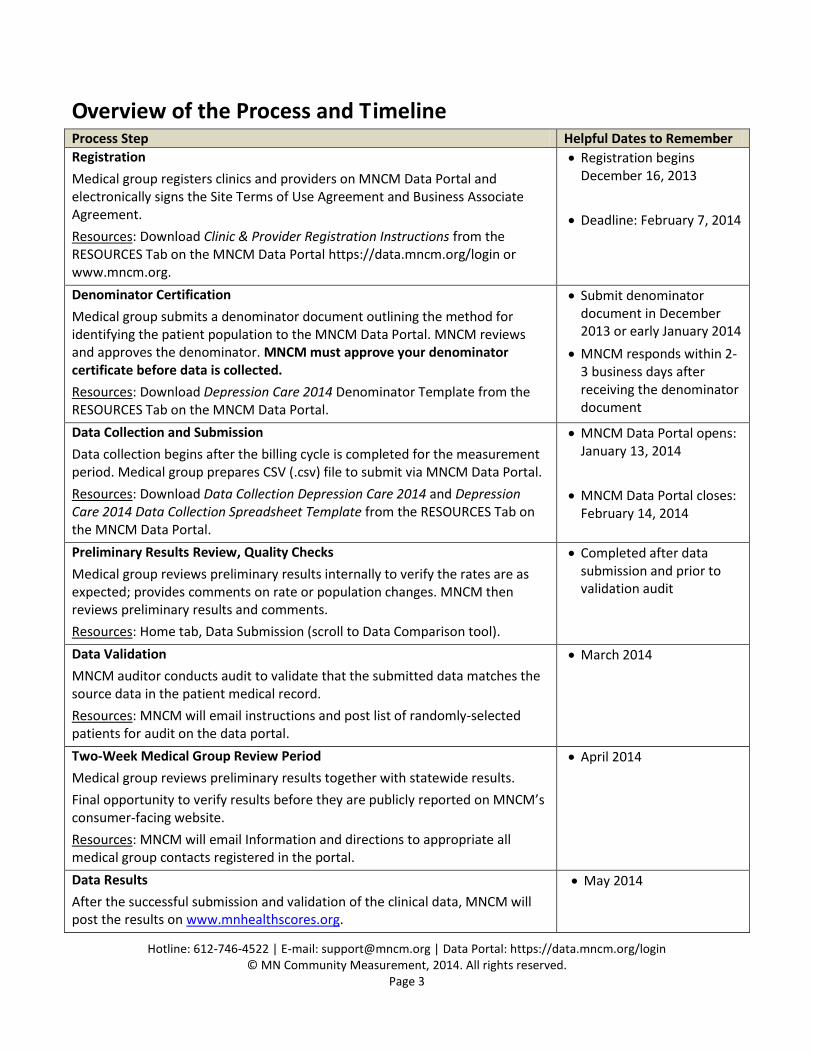
Overview of the Process and Timeline Process Step Helpful Dates to Remember
Registration
Medical group registers clinics and providers on MNCM Data Portal and electronically signs the Site Terms of Use Agreement and Business Associate Agreement.
Resources: Download Clinic & Provider Registration Instructions from the RESOURCES Tab on the MNCM Data Portal https://data.mncm.org/login or www.mncm.org.
Registration begins December 16, 2013
Deadline: February 7, 2014
Denominator Certification
Medical group submits a denominator document outlining the method for identifying the patient population to the MNCM Data Portal. MNCM reviews and approves the denominator. MNCM must approve your denominator certificate before data is collected.
Resources: Download Depression Care 2014 Denominator Template from the RESOURCES Tab on the MNCM Data Portal.
Submit denominator document in December 2013 or early January 2014
MNCM responds within 2-3 business days after receiving the denominator document
Data Collection and Submission
Data collection begins after the billing cycle is completed for the measurement period. Medical group prepares CSV (.csv) file to submit via MNCM Data Portal.
Resources: Download Data Collection Depression Care 2014 and Depression Care 2014 Data Collection Spreadsheet Template from the RESOURCES Tab on the MNCM Data Portal.
MNCM Data Portal opens: January 13, 2014
MNCM Data Portal closes: February 14, 2014
Preliminary Results Review, Quality Checks
Medical group reviews preliminary results internally to verify the rates are as expected; provides comments on rate or population changes. MNCM then reviews preliminary results and comments.
Resources: Home tab, Data Submission (scroll to Data Comparison tool).
Completed after data submission and prior to validation audit
Data Validation
MNCM auditor conducts audit to validate that the submitted data matches the source data in the patient medical record.
Resources: MNCM will email instructions and post list of randomly-selected patients for audit on the data portal.
March 2014
Two-Week Medical Group Review Period
Medical group reviews preliminary results together with statewide results.
Final opportunity to verify results before they are publicly reported on MNCM’s consumer-facing website.
Resources: MNCM will email Information and directions to appropriate all medical group contacts registered in the portal.
April 2014
Data Results
After the successful submission and validation of the clinical data, MNCM will post the results on www.mnhealthscores.org.
May 2014
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 4
Depression Care Measures 2014
Direct Data Submission (02/01/2013 to 01/31/2014 Dates of Service)
Measure Specifications
Depression Care Measures 2014 Direct Data Submission
Measurement Specifications
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 5
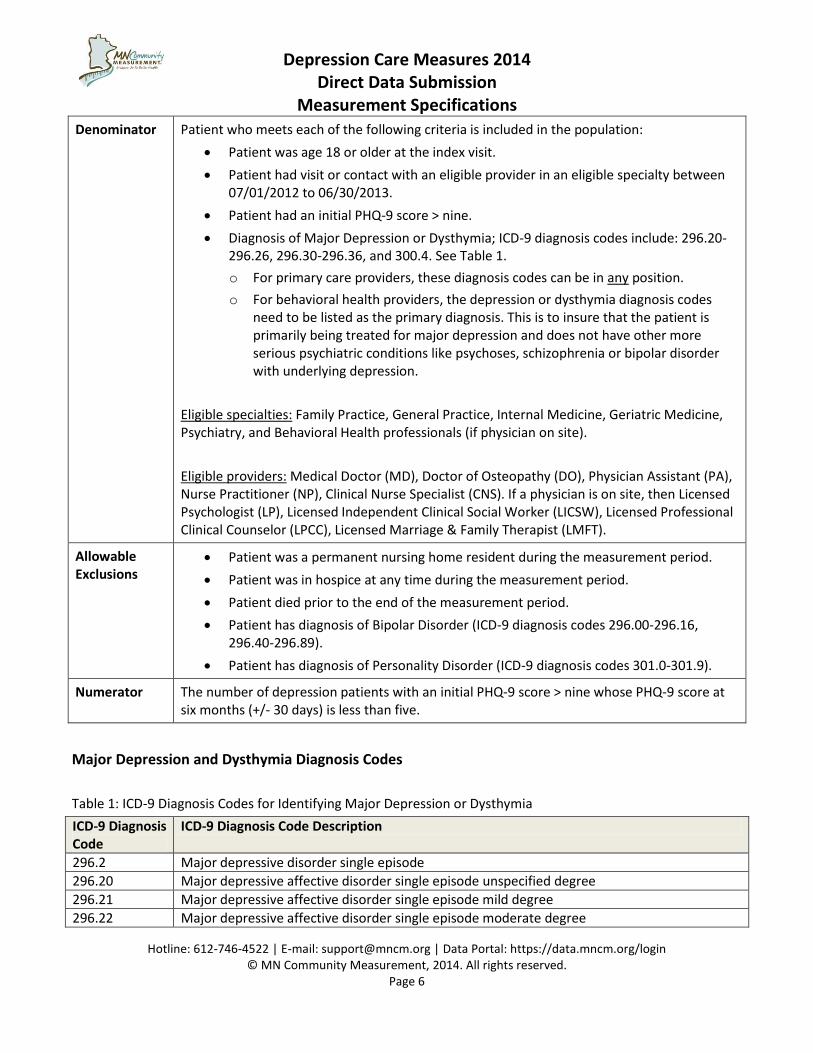
Description A measure of the percentage of adults patients who have reached remission at six months (+/- 30 days) after being identified as having an initial PHQ-9 score > nine. Remission is defined as a PHQ-9 score less than five.
Methodology Population identification is accomplished via a query of a practice management system or Electronic Medical Record (EMR) to identify the population of eligible patients (denominator). Data elements are either extracted from an EMR system or abstracted through medical record review.
Full population data is required.
Rationale The priority aim addressed by this measure is to improve the outcomes of treatment for patients with major depression or dysthymia. The Center for Disease Control and Prevention states that 15.7% of people report being told by a health care professional that they had depression at some point in their lifetime. Persons with a current diagnosis of depression and a lifetime diagnosis of depression or anxiety were significantly more likely than persons without these conditions to have cardiovascular disease, diabetes, asthma and obesity and to be a current smoker, to be physically inactive and to drink heavily. According to National Institute of Mental Health (NIMH), 6.7 percent of the U.S. population ages 18 and older (14.8 million people) in any given year have a diagnosis of a major depressive disorder. Major depression is the leading cause of disability in the U.S. for ages 15 - 44. Additionally, dysthymia accounts for an additional 3.3 million Americans. Suicide rates for Minnesotans are 10.4 per 100,000 or 1.3 suicides per day, with the highest rates among the following groups: males (four times greater than females), ages 30 to 49 years, and non-Hispanic whites.
Depression Care Measures 2014 Direct Data Submission
Measurement Specifications
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 6
Denominator
Patient who meets each of the following criteria is included in the population:
Patient was age 18 or older at the index visit.
Patient had visit or contact with an eligible provider in an eligible specialty between 07/01/2012 to 06/30/2013.
Patient had an initial PHQ-9 score > nine.
Diagnosis of Major Depression or Dysthymia; ICD-9 diagnosis codes include: 296.20-296.26, 296.30-296.36, and 300.4. See Table 1.
o For primary care providers, these diagnosis codes can be in any position.
o For behavioral health providers, the depression or dysthymia diagnosis codes need to be listed as the primary diagnosis. This is to insure that the patient is primarily being treated for major depression and does not have other more serious psychiatric conditions like psychoses, schizophrenia or bipolar disorder with underlying depression.
Eligible specialties: Family Practice, General Practice, Internal Medicine, Geriatric Medicine, Psychiatry, and Behavioral Health professionals (if physician on site).
Eligible providers: Medical Doctor (MD), Doctor of Osteopathy (DO), Physician Assistant (PA), Nurse Practitioner (NP), Clinical Nurse Specialist (CNS). If a physician is on site, then Licensed Psychologist (LP), Licensed Independent Clinical Social Worker (LICSW), Licensed Professional Clinical Counselor (LPCC), Licensed Marriage & Family Therapist (LMFT).
Allowable Exclusions
Patient was a permanent nursing home resident during the measurement period.
Patient was in hospice at any time during the measurement period.
Patient died prior to the end of the measurement period.
Patient has diagnosis of Bipolar Disorder (ICD-9 diagnosis codes 296.00-296.16, 296.40-296.89).
Patient has diagnosis of Personality Disorder (ICD-9 diagnosis codes 301.0-301.9).
Numerator The number of depression patients with an initial PHQ-9 score > nine whose PHQ-9 score at six months (+/- 30 days) is less than five.
Major Depression and Dysthymia Diagnosis Codes
Table 1: ICD-9 Diagnosis Codes for Identifying Major Depression or Dysthymia
ICD-9 Diagnosis Code
ICD-9 Diagnosis Code Description
296.2 Major depressive disorder single episode
296.20 Major depressive affective disorder single episode unspecified degree
296.21 Major depressive affective disorder single episode mild degree
296.22 Major depressive affective disorder single episode moderate degree
Depression Care Measures 2014 Direct Data Submission
Measurement Specifications
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 7
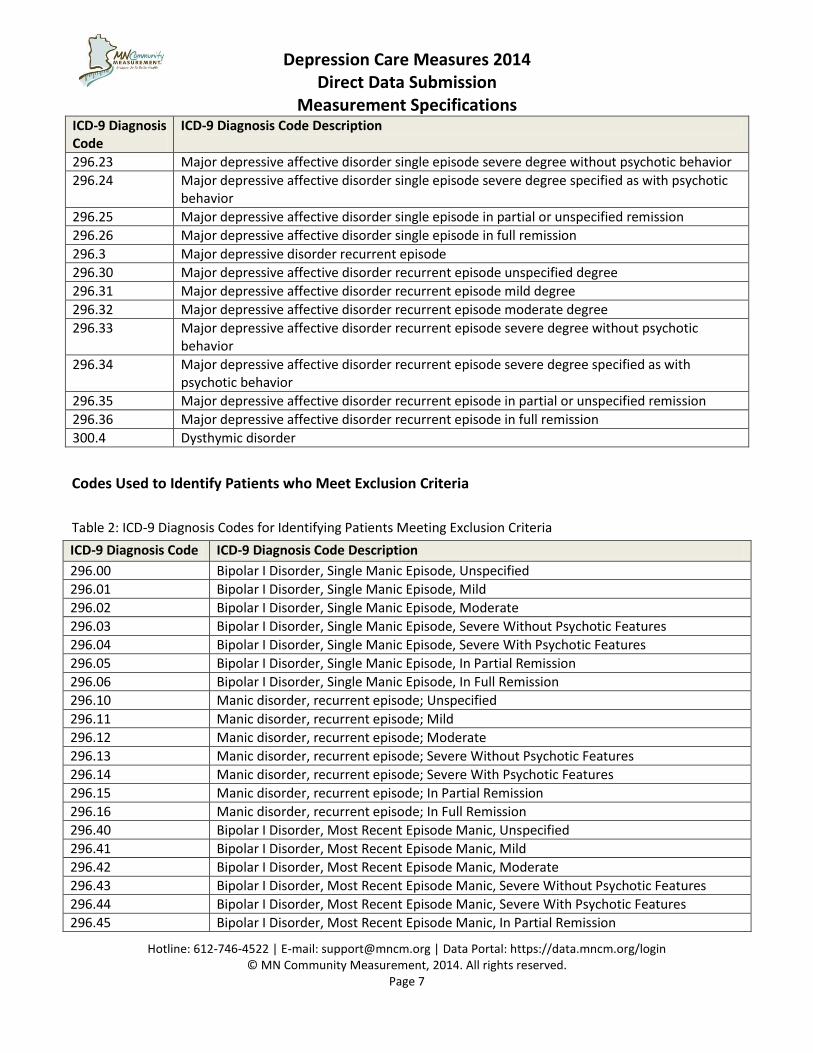
ICD-9 Diagnosis Code
ICD-9 Diagnosis Code Description
296.23 Major depressive affective disorder single episode severe degree without psychotic behavior
296.24 Major depressive affective disorder single episode severe degree specified as with psychotic behavior
296.25 Major depressive affective disorder single episode in partial or unspecified remission
296.26 Major depressive affective disorder single episode in full remission
296.3 Major depressive disorder recurrent episode
296.30 Major depressive affective disorder recurrent episode unspecified degree
296.31 Major depressive affective disorder recurrent episode mild degree
296.32 Major depressive affective disorder recurrent episode moderate degree
296.33 Major depressive affective disorder recurrent episode severe degree without psychotic behavior
296.34 Major depressive affective disorder recurrent episode severe degree specified as with psychotic behavior
296.35 Major depressive affective disorder recurrent episode in partial or unspecified remission
296.36 Major depressive affective disorder recurrent episode in full remission
300.4 Dysthymic disorder
Codes Used to Identify Patients who Meet Exclusion Criteria
Table 2: ICD-9 Diagnosis Codes for Identifying Patients Meeting Exclusion Criteria
ICD-9 Diagnosis Code ICD-9 Diagnosis Code Description
296.00 Bipolar I Disorder, Single Manic Episode, Unspecified
296.01 Bipolar I Disorder, Single Manic Episode, Mild
296.02 Bipolar I Disorder, Single Manic Episode, Moderate
296.03 Bipolar I Disorder, Single Manic Episode, Severe Without Psychotic Features
296.04 Bipolar I Disorder, Single Manic Episode, Severe With Psychotic Features
296.05 Bipolar I Disorder, Single Manic Episode, In Partial Remission
296.06 Bipolar I Disorder, Single Manic Episode, In Full Remission
296.10 Manic disorder, recurrent episode; Unspecified
296.11 Manic disorder, recurrent episode; Mild
296.12 Manic disorder, recurrent episode; Moderate
296.13 Manic disorder, recurrent episode; Severe Without Psychotic Features
296.14 Manic disorder, recurrent episode; Severe With Psychotic Features
296.15 Manic disorder, recurrent episode; In Partial Remission
296.16 Manic disorder, recurrent episode; In Full Remission
296.40 Bipolar I Disorder, Most Recent Episode Manic, Unspecified
296.41 Bipolar I Disorder, Most Recent Episode Manic, Mild
296.42 Bipolar I Disorder, Most Recent Episode Manic, Moderate
296.43 Bipolar I Disorder, Most Recent Episode Manic, Severe Without Psychotic Features
296.44 Bipolar I Disorder, Most Recent Episode Manic, Severe With Psychotic Features
296.45 Bipolar I Disorder, Most Recent Episode Manic, In Partial Remission
Depression Care Measures 2014 Direct Data Submission
Measurement Specifications
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 8
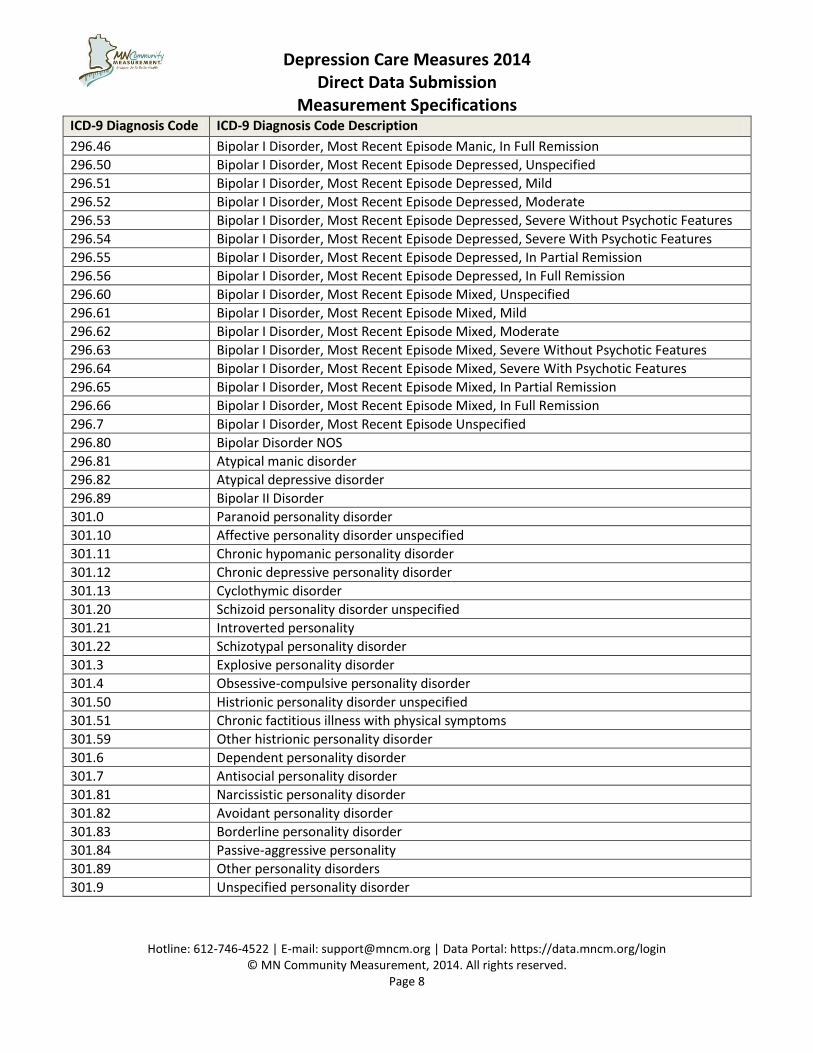
ICD-9 Diagnosis Code ICD-9 Diagnosis Code Description
296.46 Bipolar I Disorder, Most Recent Episode Manic, In Full Remission
296.50 Bipolar I Disorder, Most Recent Episode Depressed, Unspecified
296.51 Bipolar I Disorder, Most Recent Episode Depressed, Mild
296.52 Bipolar I Disorder, Most Recent Episode Depressed, Moderate
296.53 Bipolar I Disorder, Most Recent Episode Depressed, Severe Without Psychotic Features
296.54 Bipolar I Disorder, Most Recent Episode Depressed, Severe With Psychotic Features
296.55 Bipolar I Disorder, Most Recent Episode Depressed, In Partial Remission
296.56 Bipolar I Disorder, Most Recent Episode Depressed, In Full Remission
296.60 Bipolar I Disorder, Most Recent Episode Mixed, Unspecified
296.61 Bipolar I Disorder, Most Recent Episode Mixed, Mild
296.62 Bipolar I Disorder, Most Recent Episode Mixed, Moderate
296.63 Bipolar I Disorder, Most Recent Episode Mixed, Severe Without Psychotic Features
296.64 Bipolar I Disorder, Most Recent Episode Mixed, Severe With Psychotic Features
296.65 Bipolar I Disorder, Most Recent Episode Mixed, In Partial Remission
296.66 Bipolar I Disorder, Most Recent Episode Mixed, In Full Remission
296.7 Bipolar I Disorder, Most Recent Episode Unspecified
296.80 Bipolar Disorder NOS
296.81 Atypical manic disorder
296.82 Atypical depressive disorder
296.89 Bipolar II Disorder
301.0 Paranoid personality disorder
301.10 Affective personality disorder unspecified
301.11 Chronic hypomanic personality disorder
301.12 Chronic depressive personality disorder
301.13 Cyclothymic disorder
301.20 Schizoid personality disorder unspecified
301.21 Introverted personality
301.22 Schizotypal personality disorder
301.3 Explosive personality disorder
301.4 Obsessive-compulsive personality disorder
301.50 Histrionic personality disorder unspecified
301.51 Chronic factitious illness with physical symptoms
301.59 Other histrionic personality disorder
301.6 Dependent personality disorder
301.7 Antisocial personality disorder
301.81 Narcissistic personality disorder
301.82 Avoidant personality disorder
301.83 Borderline personality disorder
301.84 Passive-aggressive personality
301.89 Other personality disorders
301.9 Unspecified personality disorder
Depression Care Measures 2014 Direct Data Submission
Measurement Specifications
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 9
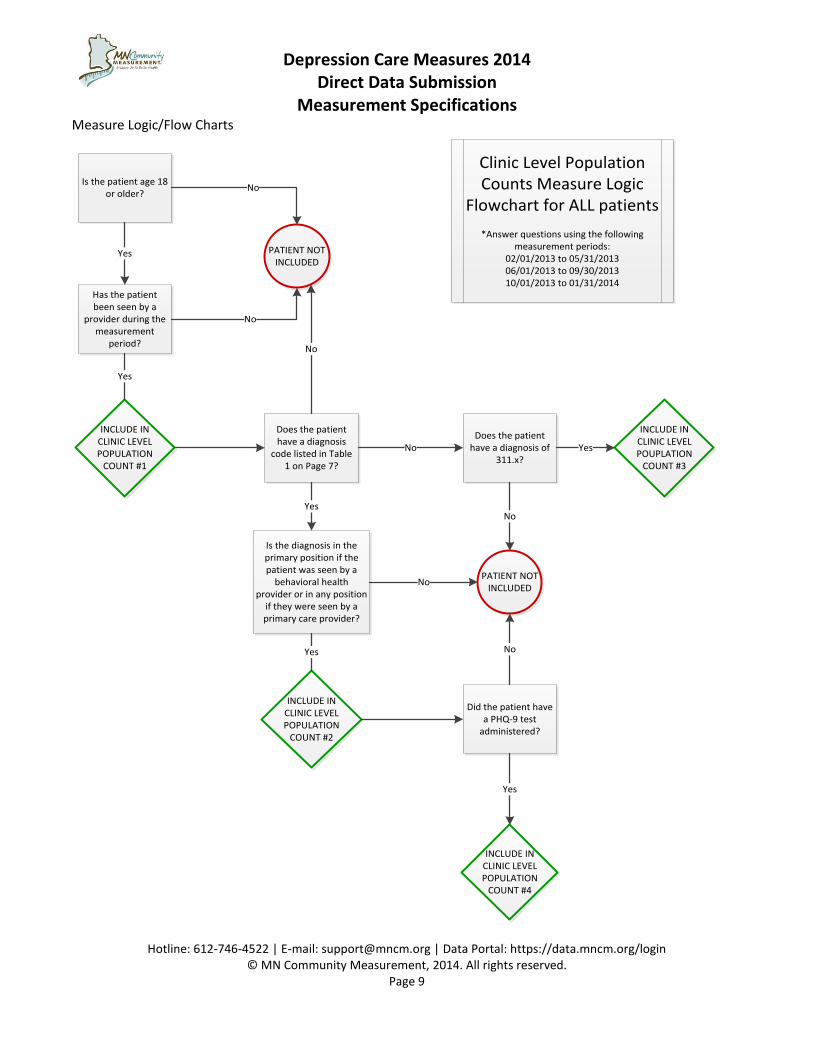
Measure Logic/Flow Charts
Is the patient age 18 or older?
Has the patient been seen by a
provider during the measurement
period?
INCLUDE IN CLINIC LEVEL POPULATION
COUNT #1
Does the patient have a diagnosis
code listed in Table 1 on Page 7?
INCLUDE IN CLINIC LEVEL POPULATION
COUNT #2
Is the diagnosis in the primary position if the patient was seen by a
behavioral health provider or in any position
if they were seen by a primary care provider?
Did the patient have a PHQ-9 test
administered?
INCLUDE IN CLINIC LEVEL POPULATION
COUNT #4
Does the patient have a diagnosis of
311.x?
INCLUDE IN CLINIC LEVEL POUPLATION
COUNT #3
PATIENT NOT INCLUDED
Clinic Level Population Counts Measure Logic
Flowchart for ALL patients
*Answer questions using the following measurement periods:
02/01/2013 to 05/31/201306/01/2013 to 09/30/201310/01/2013 to 01/31/2014
PATIENT NOT INCLUDED
No
No
No
Yes
No Yes
No
No
Yes
NoYes
Yes
Yes
Depression Care Measures 2014 Direct Data Submission
Measurement Specifications
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 10
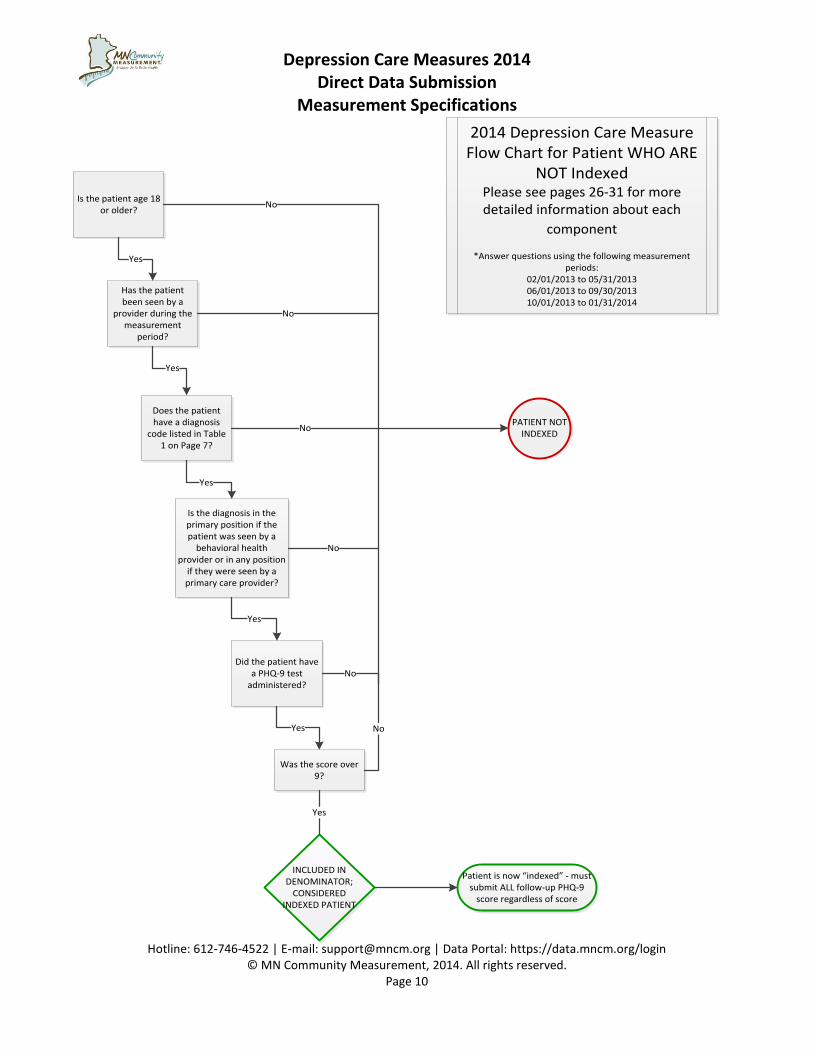
Is the patient age 18 or older?
Has the patient been seen by a
provider during the measurement
period?
Does the patient have a diagnosis
code listed in Table 1 on Page 7?
Is the diagnosis in the primary position if the patient was seen by a
behavioral health provider or in any position
if they were seen by a primary care provider?
Did the patient have a PHQ-9 test
administered?
2014 Depression Care Measure Flow Chart for Patient WHO ARE
NOT IndexedPlease see pages 26-31 for more detailed information about each
component
*Answer questions using the following measurement periods:
02/01/2013 to 05/31/201306/01/2013 to 09/30/201310/01/2013 to 01/31/2014
PATIENT NOT INDEXED
Yes
Yes
Was the score over 9?
Yes
Yes
Yes
INCLUDED IN DENOMINATOR;
CONSIDERED INDEXED PATIENT
Patient is now “indexed” - must submit ALL follow-up PHQ-9
score regardless of score
Yes
No
No
No
No
No
No
Depression Care Measures 2014 Direct Data Submission
Measurement Specifications
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 11
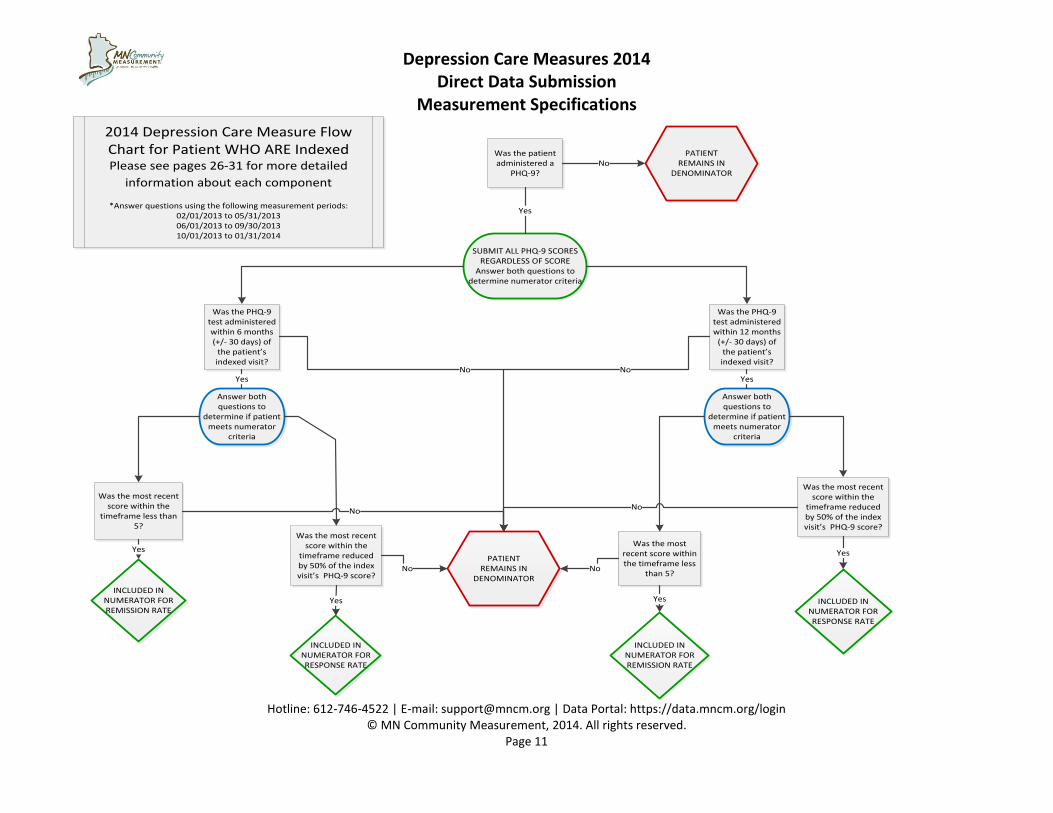
Was the patient administered a
PHQ-9?
SUBMIT ALL PHQ-9 SCORES REGARDLESS OF SCORE
Answer both questions to determine numerator criteria
Was the PHQ-9 test administered within 6 months (+/- 30 days) of
the patient’s indexed visit?
Was the most recent score within the
timeframe less than 5?
Was the most recent score within the
timeframe reduced by 50% of the index visit’s PHQ-9 score?
Was the PHQ-9 test administered within 12 months
(+/- 30 days) of the patient’s indexed visit?
Was the most recent score within the
timeframe reduced by 50% of the index visit’s PHQ-9 score?
Was the most recent score within the timeframe less
than 5?
INCLUDED IN NUMERATOR FOR REMISSION RATE
INCLUDED IN NUMERATOR FOR RESPONSE RATE
INCLUDED IN NUMERATOR FOR RESPONSE RATE
INCLUDED IN NUMERATOR FOR REMISSION RATE
Answer both questions to
determine if patient meets numerator
criteria
Yes
Yes
Yes
Answer both questions to
determine if patient meets numerator
criteria
Yes
Yes
Yes
PATIENT REMAINS IN
DENOMINATORNo No
No No
No No
PATIENT REMAINS IN
DENOMINATORNo
Yes
2014 Depression Care Measure Flow Chart for Patient WHO ARE IndexedPlease see pages 26-31 for more detailed
information about each component
*Answer questions using the following measurement periods:02/01/2013 to 05/31/201306/01/2013 to 09/30/201310/01/2013 to 01/31/2014
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 12
Depression Care Measures 2014
Direct Data Submission (02/01/2013 to 01/31/2014 Dates of Service)
Data Collection and Submission Instructions
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 13
Data Collection and Submission Preparations and Considerations Before collecting and submitting data to MNCM, please review the following items.
Data submission preparations Your medical group and clinics MUST BE REGISTERED in the MNCM Data Portal. Please see Appendix A
for more information about registration.
Save the MNCM websites in your “Favorites” internet folder for future reference.
o MNCM Data Portal: https://data.mncm.org/login
o MNCM website: www.mncm.org
o MN HealthScores: www.mnhealthscores.org
Create a folder in your network drive dedicated to all data submission documents.
o Save all spreadsheets, forms and data submission materials in the dedicated folder.
Name versions of documents clearly, so you are using the most recent files.
Log in to the MNCM Data Portal at https://data.mncm.org/login. In the Resources tab of the data portal, you are able to access the following items:
o Direct Data Submission Resources. Download the following
Depression Care Measures 2014 Direct Data Submission Guide
Depression Care Measures 2014 Denominator Certification Form
Depression Care Measures 2014 Data Collection Form
Depression Care Measures 2014 Spreadsheet Template
Patient attribution A patient is attributed to the clinic site and provider of the indexed visit meaning the visit where the patient had a diagnosis code for major depression or dysthymia AND a PHQ-9 score greater than nine. The portal then matches all subsequent contact dates and PHQ-9 scores to this patient within the medical group regardless of the clinic location of the contact.
Note for Primary Care Clinics: If a medical group assigns a primary care provider for each patient, it is acceptable to use that provider ID in this field. If a group does not assign a primary care provider, then use the provider ID of the provider who cared for the patient at the visit.
A patient is attributed to one clinic and one provider within your medical group that are considered responsible for managing the patient’s care. This method was developed in order to capture and attribute all eligible patients. Please use the following attribution methods in order:
1. After identifying the eligible patients for this measure based on the denominator criteria, first, attribute the patient to the clinic and provider within your medical group that are assigned to the patient OR are responsible for the patient’s care. If the patient does not have an assigned clinic or provider within your medical group, then
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 14
2. Attribute the patient to the clinic and provider within your medical group that saw the patient most often in the measurement period. If more than one provider saw the patient equally, then
3. Attribute the patient to the clinic and provider within your medical group that saw the patient most recently in the measurement period.
Denominator Certification You only need to submit one denominator form if both #1 and #2 listed below are true. If they are not met, you will need to submit multiple denominator certification forms.
1. The correct date of birth and date of visit ranges for each measurement period are included in the form.
2. You will pull data for each measurement period the same way.
About Total Population Submission This measure requires total population submission. When a medical group or clinic submits “total population”, they are submitting data for all of the eligible visits that occurred during the measurement period. The criterion in the “Denominator” section of the Measure Specifications on page 6 define the eligible population and provides details on who should be identified/included in the patient data file.
You must submit data for all patients who meet inclusion criteria during the current measurement period and data for all patients who have been indexed in previous measurement periods.
Patient ID The patient ID number must be maintained for patients across all measurement periods. This means that data for a patient must always be submitted using the same patient ID. If you have questions about this, please contact MNCM by email at [email protected].
PHQ-9 Scores You must submit data for ALL follow-up PHQ-9 scores once a patient is indexed regardless of the score of the PHQ-9 test. You should expect to have some scores 9 and below in your patient data file.
Patient Data File Creation Data will be collected and put into an Excel template titled “Depression Care Data Collection Spreadsheet” which can be found on the MNCM Data Portal. Once all data is collected and input into the Excel template, the file will need to be saved as a CSV file in order to upload the file to the MNCM Data Portal. Please note:
1. The Excel template provided has the correct formatting. Do NOT use “General” formatting in Excel. The Excel template provided on the MNCM Data Portal will provide the correct formatting.
2. After creating the CSV file, do NOT open the CSV file in Excel. Opening the CSV file in Excel destroys the formatting and alters the data. To view the data again, open the original Excel file. If you need to make changes to your file, make the changes in your original excel file, not in the .csv file, and save the
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 15
changes to a new .csv file. If the CSV file is mistakenly opened in Excel, simply re-save a new CSV file from the original Excel file. Rename the old CSV file or delete it entirely. If at any point in the process it is discovered that corrections to the data are needed, make the necessary changes in the Excel file and save as a new CSV file using a different name.
What is a CSV file? Why is a CSV file needed for data submission? CSV stands for “comma separated values.” A CSV file is a common and simple format that is used to import /transport data between systems or software applications that are not directly related (e.g., from a spreadsheet to a database). Please see page 33 for more information on how to create a CSV file from an Excel file.
Patient Data File Submission Data submission consists of submitting clinic level population counts AND a patient data file for each measurement period.
Review Section B on pages 21-22 for more information about the clinic level population counts.
Review Section C on pages 23-31 for more detailed information about the patient data file. The patient data file must be submitted using the measurement period dates of service below. The patient data files must also be submitted to the MNCM Data Portal in chronological order as outlined below:
File Measurement Period Dates of Service Submission Order
File #1 02/01/2013 to 05/31/2013 First
File #2 06/01/2013 to 09/30/2013 Second
File #3 10/01/2013 to 01/31/2014 Third
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 16
Section A: Identifying the Patient Population (Denominator) Denominator Definition: The denominator is the bottom number in a fraction.
This step of the process includes identifying the total number of patients who are eligible for the measure using a standard set of criteria. Please review the “Denominator” section noted in the Measure Specifications in this guide for the detailed criteria used to identify eligible patients for the denominator. You will need to identify the patient population which you will include on the patient data file AND you will need to identify the clinic level populations which you will submit counts to MNCM during data submission.
Step 1: Denominator Certification This must be done prior to identifying your population and collecting data.
To help medical groups achieve accuracy and/or inadvertently pulling the wrong patient population for the measure, MNCM will complete an upfront review of each medical group’s source code or methodology that is used to produce the patient population (denominator) to help identify potential errors. The denominator certification process is intended to help identify potential issues prior to data submission. However, the responsibility to submit an accurate denominator rests with the medical group. Contact [email protected] with any specific questions.
PLEASE NOTE: Denominator certification may also include a comprehensive review by MNCM of the process steps used to identify the denominator, including the final list of patients. Save all original queries, documents, spreadsheets and process steps that are used to identify the patient population. MNCM may ask to review this information.
Denominator Template Form This template is provided to ensure all medical groups are using the same set of criteria to identify patients for the denominator. Medical groups are asked to complete this form and submit it to the MNCM Data Portal. The denominator form asks for source code or “screen shots,” which are helpful in MNCM’s review of the denominator.
1. Login to the MNCM Data Portal ( https://data.mncm.org/login).
2. Go to the RESOURCES tab and select Depression Resources from the drop-down menu. Download the Depression Care Measures 2014 Denominator Template Form.
3. Complete the form and save the form on your network directory.
4. Login to the MNCM Data Portal and click on Denominator Certification under the Depression Measure 02/01/2013 to 05/31/2013 section. Follow the instructions to upload the form to the data portal.
5. MNCM will review the method and respond within 2-3 business days. MNCM will either (1) contact the medical group if more clarification is needed, in which case the medical group will need to make the necessary revisions and re-upload the form, or (2) approve and certify the method in the MNCM Data Portal; an automatic e-mail will notify the medical group that the method is certified.
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 17
Details for the Denominator Methodology The following elements are included on the Depression Care Measures 2014 Denominator Template Form. Medical groups will need to indicate on the form how they will identify each element for MNCM:
Date of birth range.
ICD-9-CM codes.
Visit date range.
o If submitting one form for all three measurement periods, you must include all three date of service date ranges.
Board certified specialties of providers included in the search.
Whether exclusions will be taken and how exclusions will be handled.
o EMR groups can list which accepted exclusions will be filtered through the query process.
o Medical groups that will manually abstract data can describe that exclusions will be identified and documented during record review.
Step 2: Identifying patient population After your denominator form has been approved by MNCM, you will be able to query your system to determine the patient population for this measure.
If a medical group opened or acquired a new clinic in the last year, the new clinic must register and submit data with the medical group. Please contact [email protected] to discuss submitting this data.
For medical groups that implemented a new practice management system or EMR in the last two years, the patient population list will need to be generated using both systems. Two queries or patient lists will be necessary. The lists should then be combined and a common identifier(s) selected to de-duplicate the list. Contact [email protected] with any questions.
1. Eligible Providers and Encounter Types Patients who have visits with provider who practice in the following specialties are included in the depression measurement. Eligible providers include primary care and behavioral health providers. Behavioral health providers are eligible for the measure if there is a physician who is on-site (i.e., a physician who also practices at the clinic anytime during the measurement period). The following is a list of eligible specialties and providers:
Primary Care Behavioral Health Family Practice Psychiatrist Internal Medicine Physician Assistant Geriatric Medicine Nurse Practitioner Obstetrics/Gynecology * Clinical Nurse Specialist Physician Assistant Psychologist (LP) Nurse Practitioner Clinical Social Worker (LICSW) Counselor (LPCC)
Marriage and Family Therapist (LMFT) *OBGYN providers who function in a primary care role are encouraged to submit data for their patients, but it is voluntary.
Keep a “Crosswalk”: It is very important to keep a “crosswalk” between the unique identifier and the patient’s name and DOB, so that records can be located by clinic staff at the time of validation by MNCM.
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 18
2. Eligible Patients If a patient IS NOT AN INDEXED patient: In order to be eligible for this measure, patients must initially meet the following criteria:
1. Depression Diagnosis.
Patients must have one of the following diagnoses (the diagnosis must be in the primary position for behavioral health providers and can be in any position for primary care providers):
296.2.x Major depressive disorder, single episode.
296.3x Major depressive disorder, recurrent episode.
300.4 Dysthymic disorder.
2. PHQ-9 Score above 9.
Patients must have been administered a PHQ-9 test at a face-to-face visit with an eligible provider AND must have scored above a 9.
Once the two above criterions are met, the patient is considered an “indexed” patient. The “indexed” visit is the visit in which the patient had an eligible diagnosis AND scored above nine on the PHQ-9 test at a face-to-face visit with an eligible provider.
If a patient IS AN INDEXED patient: Once the patient has been indexed, all follow-up PHQ-9 scores must be included in the patient data file. Include these scores regardless of diagnosis, who or where the PHQ-9 test was administered. Acceptable encounter/visit types for follow-up PHQ-9 scores for an indexed patient include:
Office visit.
Telephone encounter.
E-Visit.
Any other contact with the patient in which a PHQ-9 is administered.
System Query: Helpful data elements that can be included in the system query Please refer to the data elements and field specifications to determine how to format the data elements that must be submitted to MNCM:
Patient ID number
Patient date of birth
Clinic or facility
Provider name and NPI
Provider type/specialty code
Insurance payer
Insurance member ID
Gender
Zip code
Race/ethnicity, country of origin and preferred language
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 19
Evaluation and Management (E & M) Current Procedural Terminology (CPT) Codes (optional) The following list of codes may be helpful in determining what types of visits to include for identifying the patient population (denominator). E & M codes do not need to be used when querying a practice management system to determine visit counts; however, they have been included here to help further define what is meant by a “face-to-face” visit with a provider. Please refer to a CPT coding manual for more details.
Description CPT Codes
Psychotherapy pt / family or diagnostic evaluation E & M Codes Preventive Codes Office Consultation Preventive Medicine Counseling, Individual Preventive Medicine Counseling, Group Other Preventive Medicine Services Other Outpatient Encounters Unlisted E & M Codes
90791- 90792; 90832-90838; 90832-90838 99201-99205; 99211-99215 99385-99387; 99395 -99397 99241-99245 99401-99404 99411- 99412 99420; 99429 98960-98962; 99078; 99217- 99220; 99341-99345; 99347-99350; 99499
Allowable Exclusions:
Patient death.
Hospice.
Permanent Resident of Nursing Home.
Bipolar Disorder (see Table 2 on pages 7-8).
Personality Disorder (see Table 2 on pages 7-8).
For Patient Death, Hospice and Permanent Resident of Nursing Home Exclusions
Do NOT exclude patients “up front” in the query process for identifying your population. Include the eligible patients as part of the submission file and enter a valid exclusion code and date. Please document how you are identifying exclusions in your denominator certification document. If an exclusion event occurs after a patient has already been submitted, a subsequent record could contain data for the “Exclusion Reason” and “Exclusion Date” fields. Having an exclusion reason and date would prevent the patient being counted in the outcome calculations. If you do not know the exact date of the event, it is acceptable to enter a date that represents the month in which it occurs like 06/01/2014 to represent June 2014.
For Bipolar Disorder and Personality Disorder Exclusions
It is acceptable to exclude patients with a bipolar or personality disorder (listed in Table 2 on pages 7-8) in any position for both behavioral health and primary care providers upfront. Medical groups can now structure their queries to exclude any patient with a secondary or primary diagnosis of bipolar or personality disorder.
For patients that have already been submitted to the data portal and now have bipolar or personality disorder as a diagnosis (primary or not), please submit a record for each patient that includes the appropriate exclusion
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 20
code in the patient data file. It is acceptable to create a fake encounter with the date of 02/01/2013. This will exclude the patient from the measure. Moving forward, any new patient who has bipolar or personality disorder can be excluded upfront through queries and does not need to be submitted in the patient data file with a visit and exclusion code and date.
PLEASE NOTE: These exclusions may be taken by the medical group if the information is available, however, it is optional. If the information is unknown to the clinic, the patient is to be included.
Patient Registries
A patient registry is an important tool to help clinics track patient progress and to use for quality improvement purposes. However, MNCM cautions the use of a patient registry for identifying patients in the population or for the collection of clinical data. Many registries give a “snapshot” of patients at a given time and would therefore not include all patients according to established patient criteria or may not reflect the most recent clinical data (e.g., most recent screening exam). Registries that are programmed to update the patient population and clinical results on a continual basis (24/7) or built using measure specifications can possibly be used, however, please discuss this with MNCM. You can use the data submission template as a registry, but make sure you only send us what we need and in the original CSV format when downloaded from the portal. If changes are made to the spreadsheet, it will not upload correctly into the MNCM portal. During the validation audit, the MNCM auditor will review the patient record for validation and not the patient registry. If a clinic uses data from a patient registry, the auditor may find a more recent date/value in the medical record and this would be counted as a validation error.
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 21
Section B: Clinic Level Population Counts Clinic level population counts are used to calculate general clinic level depression care rates for your clinic (See Appendix F for more information). In addition to creating a file of all your patients with depression and their PHQ-9 scores that meet the inclusion criteria for the measure (see next section), you will be asked to provide specific summary counts in the data portal. These counts that are calculated will not necessarily match the number of patients in the patient data file. The population counts are important and contribute to the measurement calculations. If your clinic does not use the phq-9 test, you still need to submit clinic level population counts.
Purpose To provide information about the population of patients cared for at each clinic site and to understand the processes related to diagnosis, monitoring and treatment of depression.
The incidence of major depression/dysthymia in the clinic’s adult population.
The use or overuse of the non-specific ICD-9 code for depression (311).
The utilization of the PHQ-9 tool for patients with diagnosed depression/dysthymia. All counts pertain to the current measurement period only. Please review the measurement period for which you are submitting data, the name of the period will be next to your medical group name. All are counts of unique patients, not the number of visits. For example, this means that a patient could be counted once in the first measurement period and once in the third measurement period.
Clinic Level Population Count 1: Total Adult Patients The total number of unique adult patients (ages 18+) seen in your clinic for any reason with a contact with an eligible provider during the measurement period.
Clinic Level Population Count 2: Total Adult Patients with Depression Diagnosis (296.2x, 296.3x or 300.4) These ICD-9 codes define major depression and dysthymia and would be a subset of your total adult patients. It does not matter if this is a new diagnosis or if the patient is returning for a follow-up visit. If they have these codes during the measurement period, include them in the count. If the patient has an exclusion ICD-9 diagnosis codes, do NOT include them in this count.
The total number of adult patients with a contact with an eligible provider who have at least one contact in the measurement period with the following ICD-9 codes:
296.2x Major depressive disorder, single episode.
296.3x Major depressive disorder, recurrent episode.
300.4 Dysthymic disorder. If the provider is primary care, the ICD-9 codes can be in any position. If the provider is behavioral health, the ICD-9 codes need to be in the primary position only. This excludes patients with other psychiatric diagnoses with a secondary component of depression.
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 22
If a clinic DID NOT have any patients with a diagnosis of major depression or dysthymia: A “0” should be entered for this count. You must also check “No Depression Patients Seen this Period.”
Clinic Level Population Count 3: Total Adult Patients with Depression NOS (311) code This would be another subset of your adult population. The total number of adult patients with a contact with an eligible provider with a 311 code (Depression NOS not elsewhere classified). Because one of the goals of measuring this population is accurate diagnosis (and subsequently coding), please only include in this count patients who have a 311 code and not the major depression/dysthymia codes of (296.2, 296.3 or 300.4). One way you could structure your query would be to search for ICD-9 code = 311 and is not equal to 296.2, 296.3 or 300.4. If the patient has an exclusion ICD-9 diagnosis codes, do NOT include them in this count.
Clinic Level Population Count 4: Total Adult Patients with a Completed PHQ-9 AND diagnosis of Major Depression or Dysthymia (296.2x, 296.3x or 300.4) This is a subset of the patients ages 18+ with the major depression/dysthymia diagnosis codes of (296.2, 296.3 or 300.4) Count the number of these patients during the measurement period who also have a PHQ-9 test done during the measurement period. If a patient has an exclusion ICD-9 diagnosis code, do NOT include them in this count.
PLEASE NOTE: It is acceptable to “count” a patient has having a PHQ-9 administered if the patient only partially completed the PHQ-9 tool, but do NOT send partial scores as part of the patient data file.
IF YOUR CLINIC DOES NOT USE THE PHQ-9 TEST: You will enter a “0” for this count. Do NOT check “No Depression Patients Seen this Period” unless your clinic truly had no patients with a depression diagnosis seen during this measurement period.
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 23
Section C: Data Collection After the patient population (denominator) is identified, data will need to be collected for the elements found in the Data Elements and Field Specifications table on pages 26-31. Records are submitted at a patient visit or contact level; not at the level of an individual patient such as data submitted for the Optimal Diabetes Care or Optimal Vascular Care measures data submissions. This means there may be several records for one patient, one record for each PHQ-9 score administered. Please refer to the data elements and field specifications section for more detailed information about each data element.
Medical groups can collect clinical data from medical records by either: 1) extracting the data from an electronic medical record through a data query; or 2) abstracting the data from the medical record (paper record or EMR). Data collection occurs after:
1. The clinic’s billing and medical record updates are complete for the measurement period;
2. The denominator method is certified by MNCM; and
3. The patient population is pulled.
Excel Template The Excel template was created to ensure all necessary data elements are collected for DDS. This file contains all of the necessary fields and the correct column formatting according to the measure specifications. Please download the Depression Care Measures 2014 Excel template from the MNCM Data Portal by going to the RESOURCES tab and selecting Depression Resources from the drop-down menu.
Key Points for File Creation File submission reflects visit or contact level information; one row for each visit or contact. The PHQ-9
can be administered by means other than an office visit, like a telephone call, and that is why we refer to the date field as a contact date.
Once a patient has been indexed,all follow-up PHQ-9 scores are to be submitted, regardless of who administers the tool or diagnosis codes associated with susequent visits.
All PHQ-9 scores are expected to be submitted. If a patent was administered the PHQ-9 tool three times during one measurement period, there should be three records for this patient in the patient data file.
It is important to only submit records with dates of service during the measurement period. Dates of service outside of the measurement period will cause an ERROR upon submission.
Locating Data Elements in the Patient Record The primary source of data is the clinic’s documentation in the medical record (e.g., flow sheets, progress notes, lab reports, etc.). Data collectors may also choose to review the outside correspondence in the clinic’s medical record that documents more recent data within the measurement period, but this is optional. If data is used from outside correspondence, please document this for the validation audit. Below are tips for locating data in the patient record. Please follow the measure specifications for data collection.
Data Collection Tips:
When manually collecting data using an EMR, highlight the row, column or cell that contains the data needed. This reduces the chance of looking at the wrong row, column or cell.
Watch for TYPOS when entering data (number transpositions, etc.).
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 24
As long as you are including all your patients with major depression (ICD-9 codes 296.2, 296.3 or 300.4), there are several different ways that the data collection process can be achieved:
Extract information from your EMR by query.
Combination of extracting info from EMR and manual chart abstraction. Establishing an integrated PHQ-9 tool solely within your EMR would mean that scores can be extracted by query.
Registry populated with patients with depression and their visits.
Download as much information as can be attained from a billing system into Excel and then abstract remaining data elements.
Tracking Where Data is Located in the Patient Record It is important to keep track of where data is located in the patient record. For example, if data is used from an outside specialist or provider note (that is within the primary clinic’s record), document the source on the data collection form or Excel spreadsheet.
If you are collecting data directly in the Excel spreadsheet, create a “Notes” column and enter the data source details in this column. After you have completed data collection, SAVE A COPY of the Excel file and remove the “Notes” column in the file that will be used for submitting to MNCM.
Data Quality Checks MNCM recommends completing several internal quality checks of the data before submitting data. Performing quality checks ensures that the data is accurate and able to be validated by a MNCM auditor. If corrections are needed, make these in the Excel file. There are several ways to conduct quality checks:
Option 1: Complete data quality checks of specific data elements in the Excel file using Excel’s AutoFilter. Please use the following directions to set the filter and review specific data elements.
1. Click inside any data cell and activate the AutoFilter by doing the following:
a. In Excel 2003, click the Data menu, point to Filter, and then click AutoFilter.
b. In Excel 2007 and Excel 2010, click the Data tab and in the Sort & Filter area click Filter.
2. The AutoFilter arrows now appear to the right of each column heading.
3. Click on the drop-down boxes of any column and scan for key entry errors, “out-of-range” or missing data and determine if the data needs to be corrected (e.g., If a date for a PH9-9 contact field was outside the measurement period, the field would not be accepted).
4. To display all data again, click on the same drop-down box and select All.
5. Remove the Filter option by doing the following:
a. In Excel 2003, click Data, Filter, and AutoFilter again.
b. In Excel 2007 and Excel 2010, click the Filter option again in the Sort & Filter area.
Example Quality Check: Verify that if there are PHQ-9 scores 9 and below. Filter for all rows in Column V (PHQ-9 Score). When reviewing the list of scores submitted, confirm there are scores 9 and below. Make changes in the original Excel file if appropriate.
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 25
Option 2: Complete an internal audit of clinical data by reviewing a random sample of records (either 8-10 records) or a full sample (30 records) to see if the data matches what was collected from the patient record. If errors are found, make the corrections in the Excel file, however also consider if the errors were isolated cases or indicative of a larger data collection problem. (e.g., there are no patients with PHQ-9 scores, and you are certain that PHQ-9 tests were administered.)
Option 3: Complete the general quality checks outlined below:
1. Complete quality checks listed in the “Notes” section of each data element in the Data Elements and Field Specifications table on pages 26-31.
2. Verify excluded records are removed and recorded on Exclusions Template. Please see Table 2 on pages 7-8 for all applicable codes used to identify patients who meet exclusion criteria.
3. Hyphens or zeroes (0’s): If the data field is supposed to be blank, do NOT enter hyphens or zero (leave blank).
4. Blank rows in spreadsheet: Check that the Excel file does not have blank rows at the bottom of the spreadsheet as blank rows can slow the data submission process. To check for blank rows: Press Ctrl/End at the same time to go to the bottom-most cell in the spreadsheet. If there are several blank rows, remove them by highlighting the blank rows, right-clicking in the left margin, and selecting Delete (this deletes the rows and not only the text within the cells).
Option 4: Review and answer the following questions. If you answered “No” to any of the questions below, please return to the patient data file and correct the issues.
Did you use the same patient ID for patients that were already submitted to the data portal?
Is the file sorted by patient ID and then contact date (oldest to newest)?
Did you include ALL follow-up PHQ-9 scores for patients that were indexed in this period or prior periods regardless of low PHQ-9 scores, non-face-to-face visits or visit diagnosis codes? Did you include scores from scanned PHQ-9s, flowsheets, or visit notes?
Does your excel file match the depression data collection spreadsheet template (the formatting and column headers)?
It is important to complete quality checks of the file before submitting data to MNCM. Completing these checks can help avoid delays in the file submission and ensure that you have the most accurate data. Make any changes/additions in the Excel file before submitting data to MNCM.
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 26
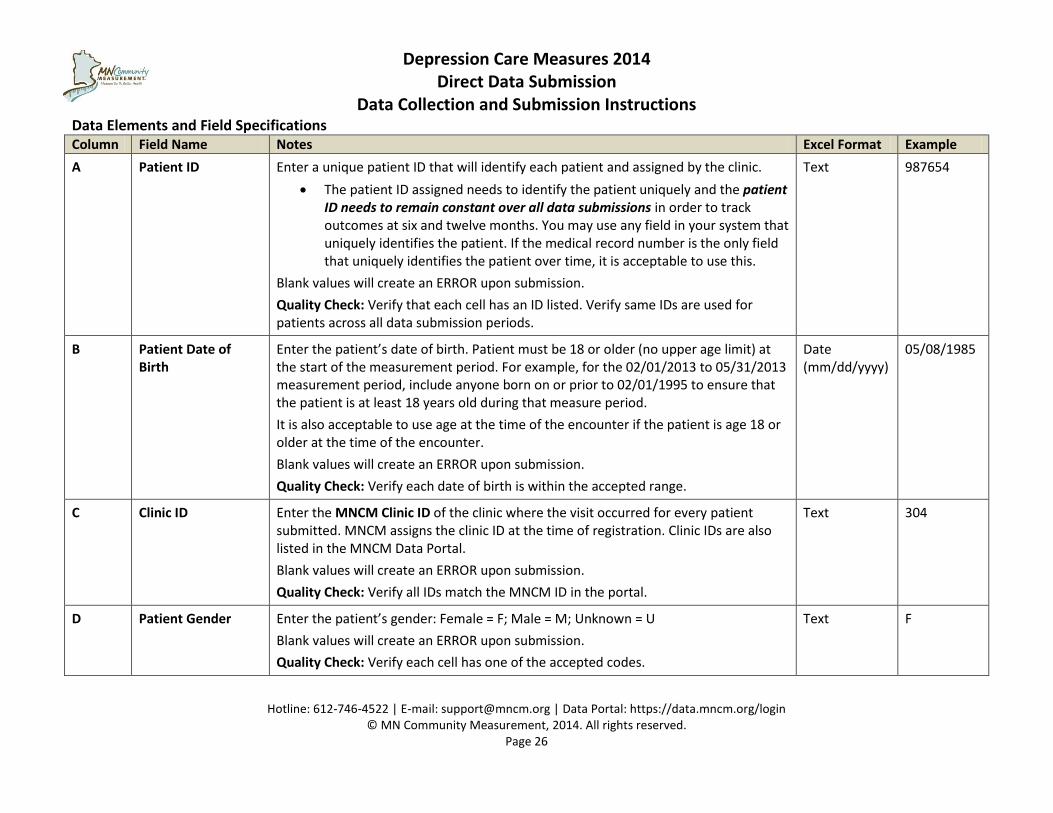
Data Elements and Field Specifications Column Field Name Notes Excel Format Example
A Patient ID
Enter a unique patient ID that will identify each patient and assigned by the clinic.
The patient ID assigned needs to identify the patient uniquely and the patient ID needs to remain constant over all data submissions in order to track outcomes at six and twelve months. You may use any field in your system that uniquely identifies the patient. If the medical record number is the only field that uniquely identifies the patient over time, it is acceptable to use this.
Blank values will create an ERROR upon submission.
Quality Check: Verify that each cell has an ID listed. Verify same IDs are used for patients across all data submission periods.
Text 987654
B Patient Date of Birth
Enter the patient’s date of birth. Patient must be 18 or older (no upper age limit) at the start of the measurement period. For example, for the 02/01/2013 to 05/31/2013 measurement period, include anyone born on or prior to 02/01/1995 to ensure that the patient is at least 18 years old during that measure period.
It is also acceptable to use age at the time of the encounter if the patient is age 18 or older at the time of the encounter.
Blank values will create an ERROR upon submission.
Quality Check: Verify each date of birth is within the accepted range.
Date (mm/dd/yyyy)
05/08/1985
C Clinic ID Enter the MNCM Clinic ID of the clinic where the visit occurred for every patient submitted. MNCM assigns the clinic ID at the time of registration. Clinic IDs are also listed in the MNCM Data Portal.
Blank values will create an ERROR upon submission.
Quality Check: Verify all IDs match the MNCM ID in the portal.
Text 304
D Patient Gender Enter the patient’s gender: Female = F; Male = M; Unknown = U
Blank values will create an ERROR upon submission.
Quality Check: Verify each cell has one of the accepted codes.
Text F
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 27
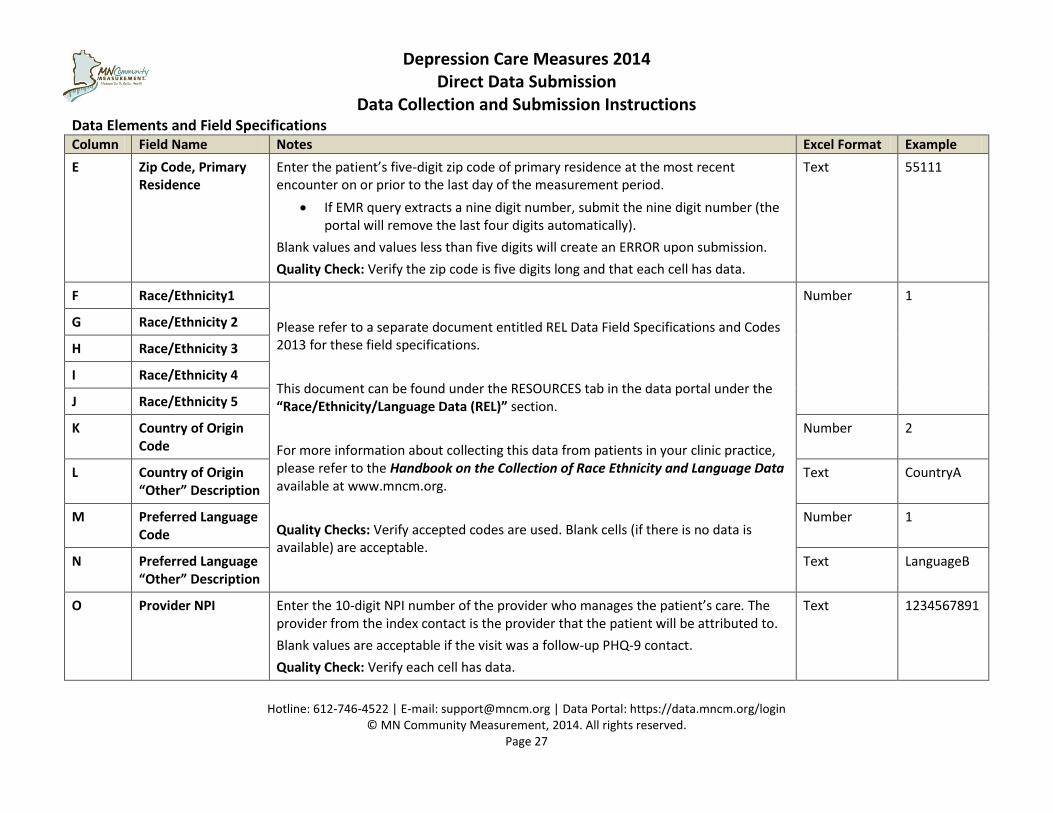
Data Elements and Field Specifications Column Field Name Notes Excel Format Example
E Zip Code, Primary Residence
Enter the patient’s five-digit zip code of primary residence at the most recent encounter on or prior to the last day of the measurement period.
If EMR query extracts a nine digit number, submit the nine digit number (the portal will remove the last four digits automatically).
Blank values and values less than five digits will create an ERROR upon submission.
Quality Check: Verify the zip code is five digits long and that each cell has data.
Text 55111
F Race/Ethnicity1
Please refer to a separate document entitled REL Data Field Specifications and Codes 2013 for these field specifications.
This document can be found under the RESOURCES tab in the data portal under the “Race/Ethnicity/Language Data (REL)” section.
For more information about collecting this data from patients in your clinic practice, please refer to the Handbook on the Collection of Race Ethnicity and Language Data available at www.mncm.org.
Quality Checks: Verify accepted codes are used. Blank cells (if there is no data is available) are acceptable.
Number
1
G Race/Ethnicity 2
H Race/Ethnicity 3
I Race/Ethnicity 4
J Race/Ethnicity 5
K Country of Origin Code
Number 2
L Country of Origin “Other” Description
Text CountryA
M Preferred Language Code
Number 1
N Preferred Language “Other” Description
Text LanguageB
O Provider NPI Enter the 10-digit NPI number of the provider who manages the patient’s care. The provider from the index contact is the provider that the patient will be attributed to.
Blank values are acceptable if the visit was a follow-up PHQ-9 contact.
Quality Check: Verify each cell has data.
Text 1234567891
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 28
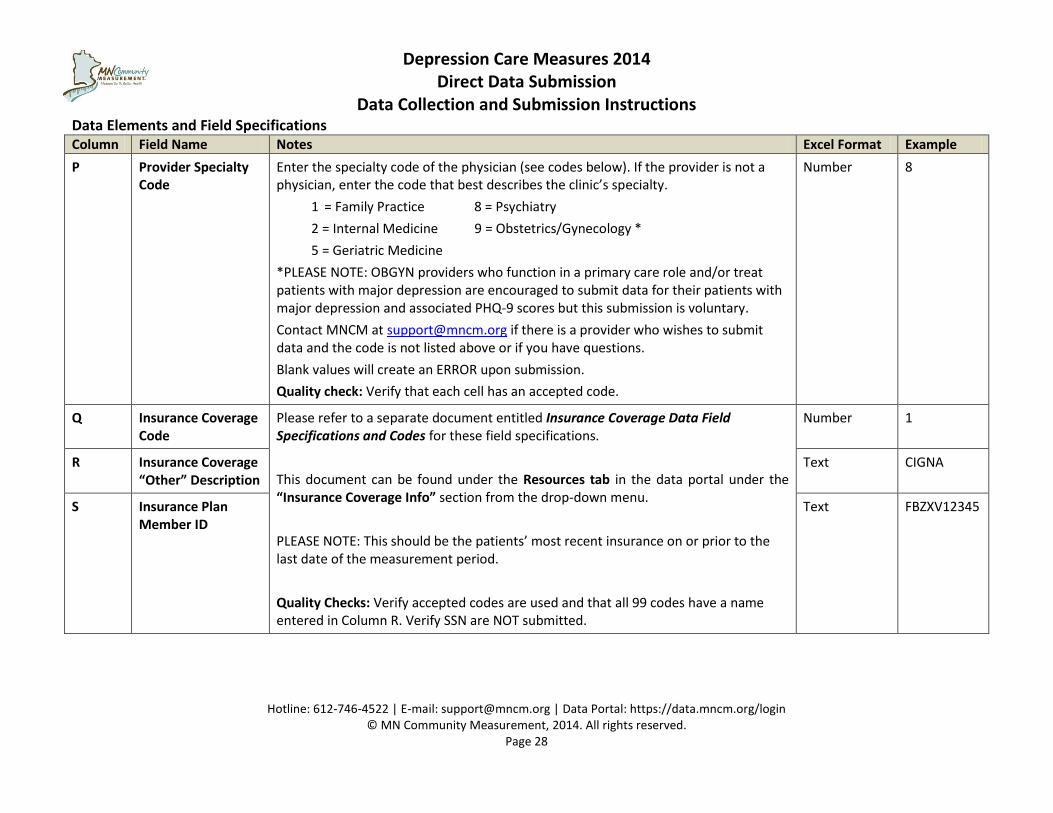
Data Elements and Field Specifications Column Field Name Notes Excel Format Example
P Provider Specialty Code
Enter the specialty code of the physician (see codes below). If the provider is not a physician, enter the code that best describes the clinic’s specialty.
1 = Family Practice 8 = Psychiatry
2 = Internal Medicine 9 = Obstetrics/Gynecology *
5 = Geriatric Medicine
*PLEASE NOTE: OBGYN providers who function in a primary care role and/or treat patients with major depression are encouraged to submit data for their patients with major depression and associated PHQ-9 scores but this submission is voluntary.
Contact MNCM at [email protected] if there is a provider who wishes to submit data and the code is not listed above or if you have questions.
Blank values will create an ERROR upon submission.
Quality check: Verify that each cell has an accepted code.
Number 8
Q Insurance Coverage Code
Please refer to a separate document entitled Insurance Coverage Data Field Specifications and Codes for these field specifications.
This document can be found under the Resources tab in the data portal under the “Insurance Coverage Info” section from the drop-down menu.
PLEASE NOTE: This should be the patients’ most recent insurance on or prior to the last date of the measurement period.
Quality Checks: Verify accepted codes are used and that all 99 codes have a name entered in Column R. Verify SSN are NOT submitted.
Number 1
R Insurance Coverage “Other” Description
Text CIGNA
S Insurance Plan Member ID
Text FBZXV12345
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 29
Data Elements and Field Specifications Column Field Name Notes Excel Format Example
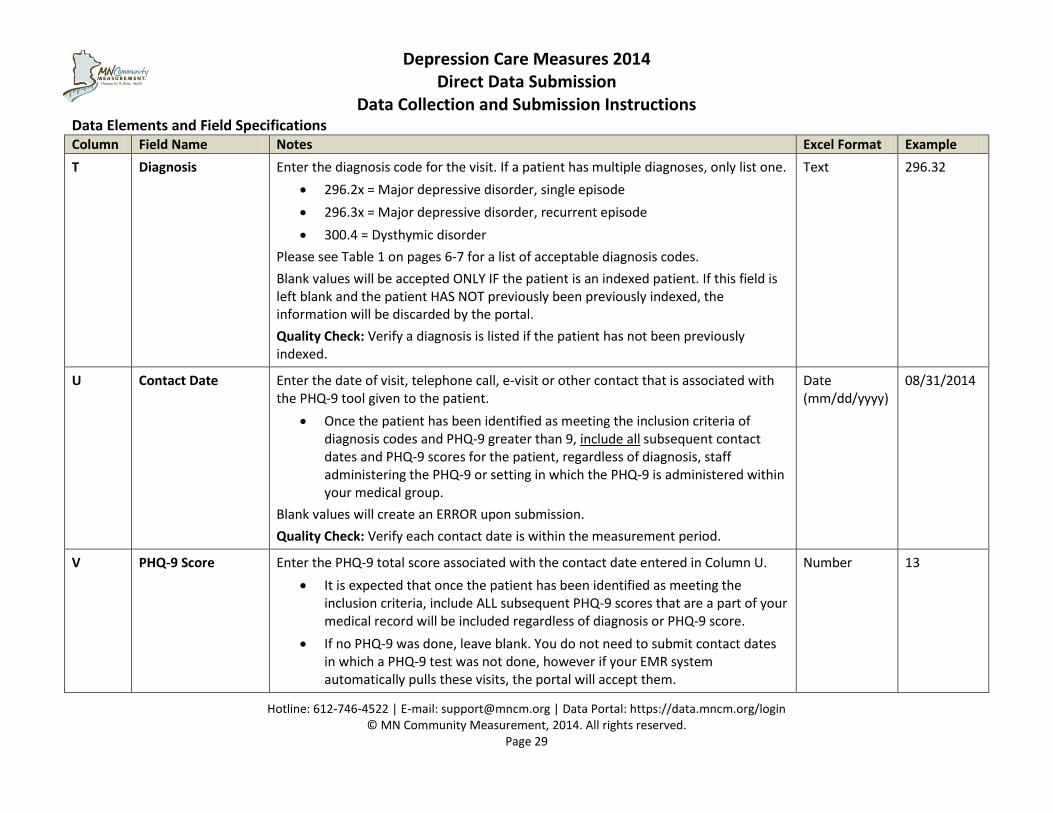
T Diagnosis
Enter the diagnosis code for the visit. If a patient has multiple diagnoses, only list one.
296.2x = Major depressive disorder, single episode
296.3x = Major depressive disorder, recurrent episode
300.4 = Dysthymic disorder
Please see Table 1 on pages 6-7 for a list of acceptable diagnosis codes.
Blank values will be accepted ONLY IF the patient is an indexed patient. If this field is left blank and the patient HAS NOT previously been previously indexed, the information will be discarded by the portal.
Quality Check: Verify a diagnosis is listed if the patient has not been previously indexed.
Text 296.32
U Contact Date
Enter the date of visit, telephone call, e-visit or other contact that is associated with the PHQ-9 tool given to the patient.
Once the patient has been identified as meeting the inclusion criteria of diagnosis codes and PHQ-9 greater than 9, include all subsequent contact dates and PHQ-9 scores for the patient, regardless of diagnosis, staff administering the PHQ-9 or setting in which the PHQ-9 is administered within your medical group.
Blank values will create an ERROR upon submission.
Quality Check: Verify each contact date is within the measurement period.
Date (mm/dd/yyyy)
08/31/2014
V
PHQ-9 Score
Enter the PHQ-9 total score associated with the contact date entered in Column U.
It is expected that once the patient has been identified as meeting the inclusion criteria, include ALL subsequent PHQ-9 scores that are a part of your medical record will be included regardless of diagnosis or PHQ-9 score.
If no PHQ-9 was done, leave blank. You do not need to submit contact dates in which a PHQ-9 test was not done, however if your EMR system automatically pulls these visits, the portal will accept them.
Number
13
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 30
Data Elements and Field Specifications Column Field Name Notes Excel Format Example
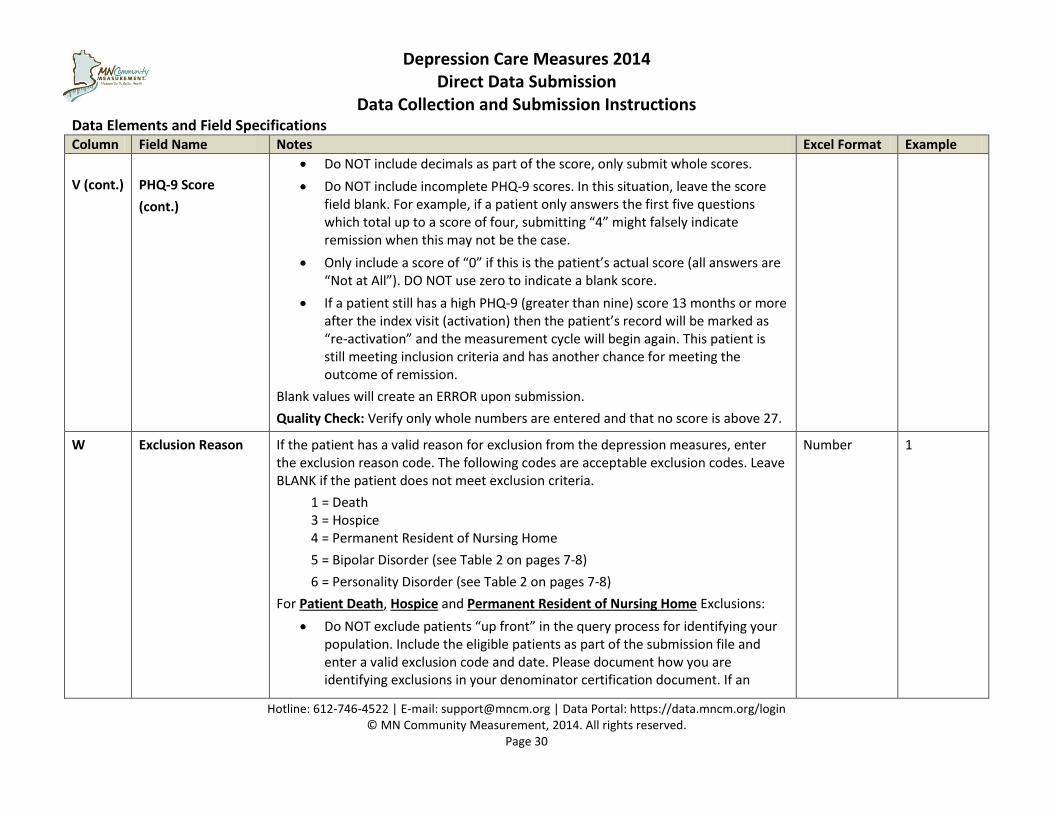
V (cont.)
PHQ-9 Score
(cont.)
Do NOT include decimals as part of the score, only submit whole scores.
Do NOT include incomplete PHQ-9 scores. In this situation, leave the score field blank. For example, if a patient only answers the first five questions which total up to a score of four, submitting “4” might falsely indicate remission when this may not be the case.
Only include a score of “0” if this is the patient’s actual score (all answers are “Not at All”). DO NOT use zero to indicate a blank score.
If a patient still has a high PHQ-9 (greater than nine) score 13 months or more after the index visit (activation) then the patient’s record will be marked as “re-activation” and the measurement cycle will begin again. This patient is still meeting inclusion criteria and has another chance for meeting the outcome of remission.
Blank values will create an ERROR upon submission.
Quality Check: Verify only whole numbers are entered and that no score is above 27.
W
Exclusion Reason
If the patient has a valid reason for exclusion from the depression measures, enter the exclusion reason code. The following codes are acceptable exclusion codes. Leave BLANK if the patient does not meet exclusion criteria.
1 = Death 3 = Hospice 4 = Permanent Resident of Nursing Home
5 = Bipolar Disorder (see Table 2 on pages 7-8)
6 = Personality Disorder (see Table 2 on pages 7-8)
For Patient Death, Hospice and Permanent Resident of Nursing Home Exclusions:
Do NOT exclude patients “up front” in the query process for identifying your population. Include the eligible patients as part of the submission file and enter a valid exclusion code and date. Please document how you are identifying exclusions in your denominator certification document. If an
Number 1
Depression Care Measures 2014 Direct Data Submission
Data Collection and Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 31
Data Elements and Field Specifications Column Field Name Notes Excel Format Example
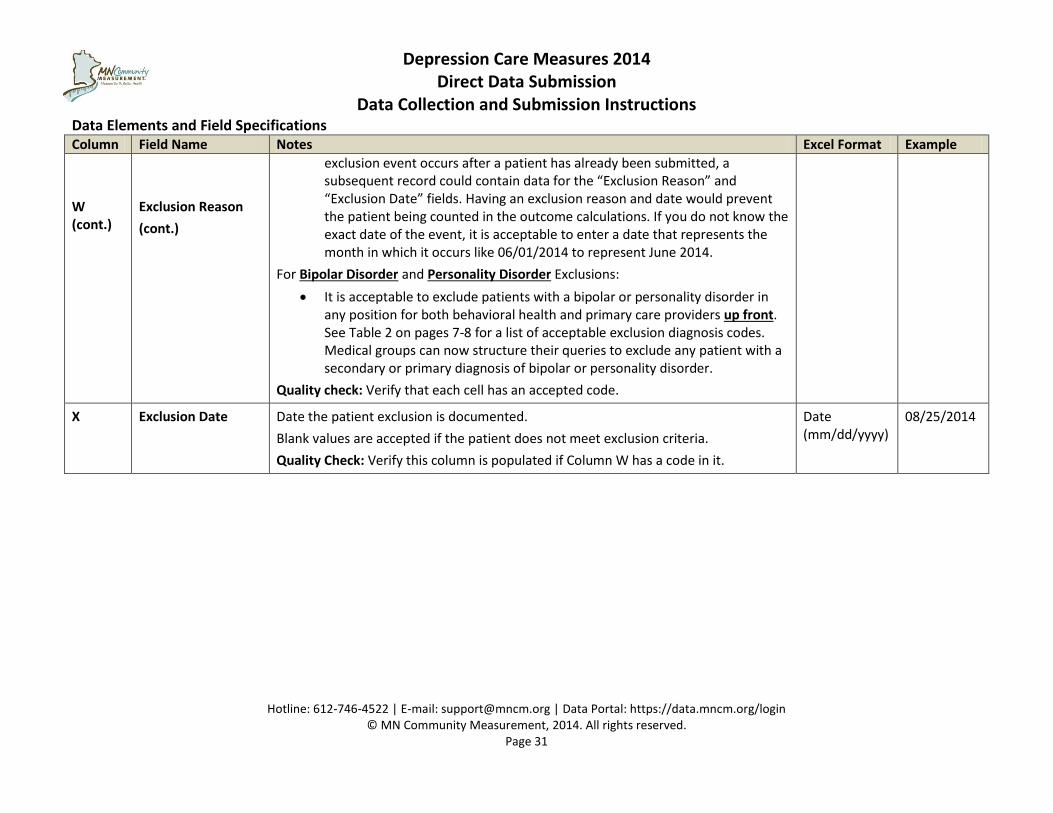
W (cont.)
Exclusion Reason
(cont.)
exclusion event occurs after a patient has already been submitted, a subsequent record could contain data for the “Exclusion Reason” and “Exclusion Date” fields. Having an exclusion reason and date would prevent the patient being counted in the outcome calculations. If you do not know the exact date of the event, it is acceptable to enter a date that represents the month in which it occurs like 06/01/2014 to represent June 2014.
For Bipolar Disorder and Personality Disorder Exclusions:
It is acceptable to exclude patients with a bipolar or personality disorder in any position for both behavioral health and primary care providers up front. See Table 2 on pages 7-8 for a list of acceptable exclusion diagnosis codes. Medical groups can now structure their queries to exclude any patient with a secondary or primary diagnosis of bipolar or personality disorder.
Quality check: Verify that each cell has an accepted code.
X Exclusion Date
Date the patient exclusion is documented.
Blank values are accepted if the patient does not meet exclusion criteria.
Quality Check: Verify this column is populated if Column W has a code in it.
Date (mm/dd/yyyy)
08/25/2014
Depression Care Measures 2014 Direct Data Submission
Direct Data Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 32
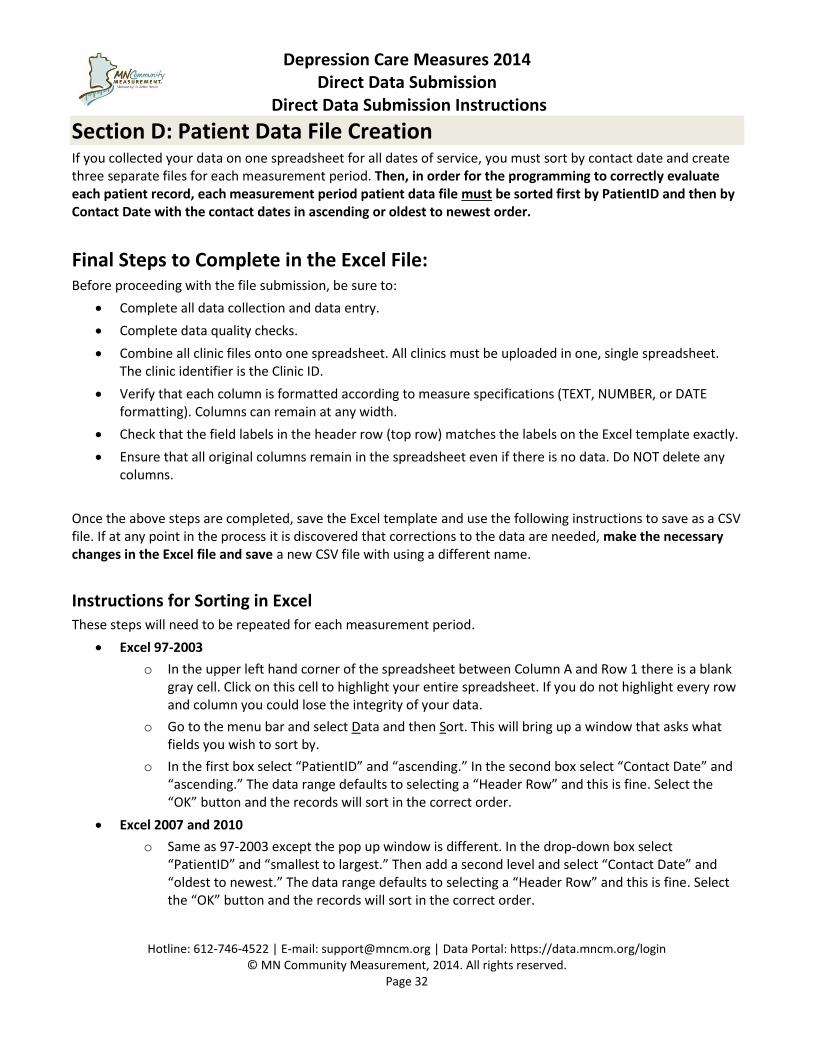
Section D: Patient Data File Creation If you collected your data on one spreadsheet for all dates of service, you must sort by contact date and create three separate files for each measurement period. Then, in order for the programming to correctly evaluate each patient record, each measurement period patient data file must be sorted first by PatientID and then by Contact Date with the contact dates in ascending or oldest to newest order.
Final Steps to Complete in the Excel File: Before proceeding with the file submission, be sure to:
Complete all data collection and data entry.
Complete data quality checks.
Combine all clinic files onto one spreadsheet. All clinics must be uploaded in one, single spreadsheet. The clinic identifier is the Clinic ID.
Verify that each column is formatted according to measure specifications (TEXT, NUMBER, or DATE formatting). Columns can remain at any width.
Check that the field labels in the header row (top row) matches the labels on the Excel template exactly.
Ensure that all original columns remain in the spreadsheet even if there is no data. Do NOT delete any columns.
Once the above steps are completed, save the Excel template and use the following instructions to save as a CSV file. If at any point in the process it is discovered that corrections to the data are needed, make the necessary changes in the Excel file and save a new CSV file with using a different name.
Instructions for Sorting in Excel These steps will need to be repeated for each measurement period.
Excel 97-2003
o In the upper left hand corner of the spreadsheet between Column A and Row 1 there is a blank gray cell. Click on this cell to highlight your entire spreadsheet. If you do not highlight every row and column you could lose the integrity of your data.
o Go to the menu bar and select Data and then Sort. This will bring up a window that asks what fields you wish to sort by.
o In the first box select “PatientID” and “ascending.” In the second box select “Contact Date” and “ascending.” The data range defaults to selecting a “Header Row” and this is fine. Select the “OK” button and the records will sort in the correct order.
Excel 2007 and 2010
o Same as 97-2003 except the pop up window is different. In the drop-down box select “PatientID” and “smallest to largest.” Then add a second level and select “Contact Date” and “oldest to newest.” The data range defaults to selecting a “Header Row” and this is fine. Select the “OK” button and the records will sort in the correct order.
Depression Care Measures 2014 Direct Data Submission
Direct Data Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 33
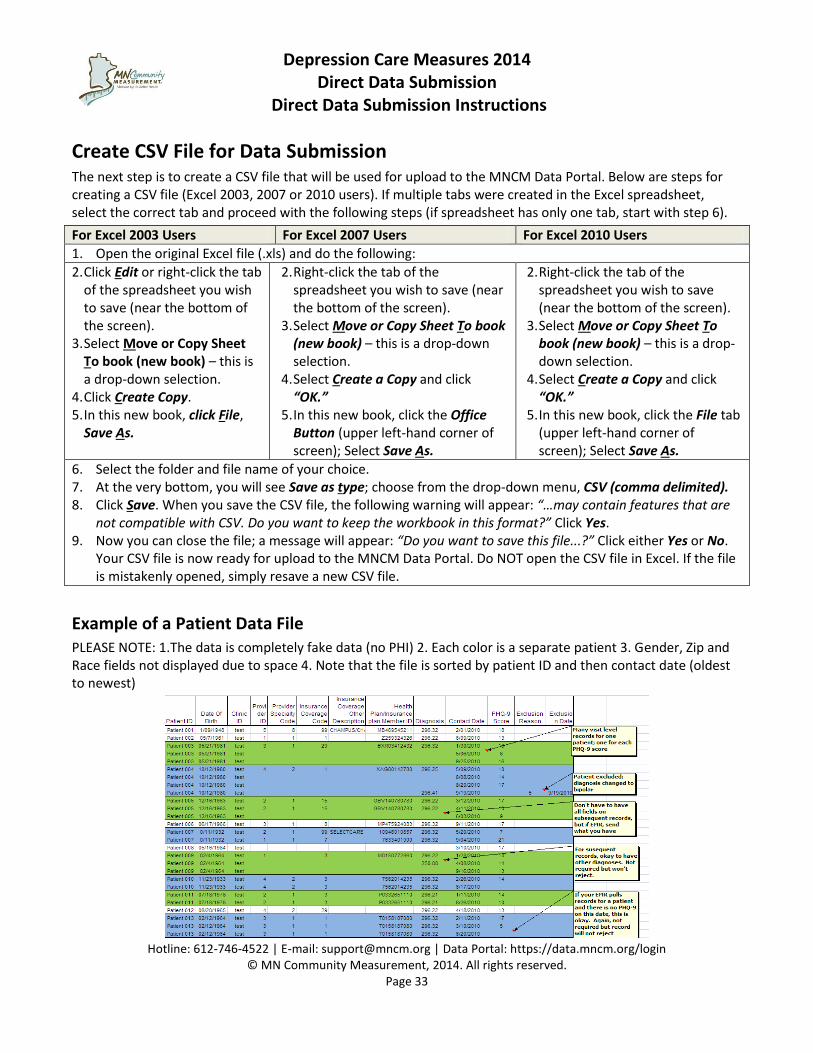
Create CSV File for Data Submission The next step is to create a CSV file that will be used for upload to the MNCM Data Portal. Below are steps for creating a CSV file (Excel 2003, 2007 or 2010 users). If multiple tabs were created in the Excel spreadsheet, select the correct tab and proceed with the following steps (if spreadsheet has only one tab, start with step 6).
For Excel 2003 Users For Excel 2007 Users For Excel 2010 Users
1. Open the original Excel file (.xls) and do the following:
2. Click Edit or right-click the tab of the spreadsheet you wish to save (near the bottom of the screen).
3. Select Move or Copy Sheet To book (new book) – this is a drop-down selection.
4. Click Create Copy. 5. In this new book, click File,
Save As.
2. Right-click the tab of the spreadsheet you wish to save (near the bottom of the screen).
3. Select Move or Copy Sheet To book (new book) – this is a drop-down selection.
4. Select Create a Copy and click “OK.”
5. In this new book, click the Office Button (upper left-hand corner of screen); Select Save As.
2. Right-click the tab of the spreadsheet you wish to save (near the bottom of the screen).
3. Select Move or Copy Sheet To book (new book) – this is a drop-down selection.
4. Select Create a Copy and click “OK.”
5. In this new book, click the File tab (upper left-hand corner of screen); Select Save As.
6. Select the folder and file name of your choice. 7. At the very bottom, you will see Save as type; choose from the drop-down menu, CSV (comma delimited). 8. Click Save. When you save the CSV file, the following warning will appear: “…may contain features that are
not compatible with CSV. Do you want to keep the workbook in this format?” Click Yes. 9. Now you can close the file; a message will appear: “Do you want to save this file...?” Click either Yes or No.
Your CSV file is now ready for upload to the MNCM Data Portal. Do NOT open the CSV file in Excel. If the file is mistakenly opened, simply resave a new CSV file.
Example of a Patient Data File PLEASE NOTE: 1.The data is completely fake data (no PHI) 2. Each color is a separate patient 3. Gender, Zip and Race fields not displayed due to space 4. Note that the file is sorted by patient ID and then contact date (oldest to newest)
Depression Care Measures 2014 Direct Data Submission
Direct Data Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 34
Section E: Patient Data File Submission Go to the HOME tab on the data portal and scroll down to the correct Depression measure period. You will need to repeat the following steps for each of the three measurement periods.
REMINDER: You must submit the depression patient data files #1, #2 and #3 in chronological order.
Step 1: Enter Denominator Medical groups can either manually enter denominator counts and information into the data portal or they can choose to enter the information into an Excel sheet and upload the Excel file to the portal. Please use either the manual instructions (Instructions A) or the upload instructions (Instructions B) below.
Instruction A: To manually enter denominator counts and information, use the following instructions.
Enter the following information for each clinic row. Once the information is entered, click on Save and Continue.
REL Data Collection: Please indicate if you collect race, Hispanic ethnicity, preferred language and country of birth using best practice methods. Best practice methods include:
o Hispanic Ethnicity and Race: Allowing patient to self-report race AND not using a multi-racial category AND system allows the collection and reporting of more than one race.
o Preferred Language and Country of Birth: Allowing patient to self-report these demographic data.
Clinic Level Population Counts: Enter counts for each clinic level population count listed below.
o Clinic Level Population Count 1: Total Adult Patients.
o Clinic Level Population Count 2: Total Adult Patients with Depression Diagnosis (296.2x, 296.3x or 300.4).
o Clinic Level Population Count 3: Total Adult Patients with Depression NOS (311) code.
o Clinic Level Population Count 4: Total Adult Patients Depression Diagnosis (296.2x, 296.3x or 300.4) and Completed PHQ-9.
No Depression Patients with Diagnosis of 296.2x, 296.3x or 300.4 Seen this Period: Check this box if a clinic is not reporting for this cycle of data collection.
o Provide a reason the clinic is not reporting. For example: The clinic has no patients meeting eligibility criteria.
Instruction B:
To enter the denominator counts and information into an Excel sheet that will then be uploaded to the portal, use the following instructions.
1. Click on “Download the Denominator Worksheet.” The clinic names will be displayed in Column A and the clinic IDs will be displayed in Column B.
2. Complete the worksheet by entering the following information for each clinic:
Depression Care Measures 2014 Direct Data Submission
Direct Data Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 35
REL Data Collection (Columns C – F): Please indicate if you collect race, Hispanic ethnicity, preferred language and country of birth using best practice methods. Best practice methods include:
Race and Hispanic Ethnicity: Allowing patient to self-report race AND not using a multi-racial category AND system allows the collection and reporting of more than one race.
Preferred Language and Country of Birth: Allowing patient to self-report these demographic data.
For each clinic ID indicate if best practices are used by using the following codes and instructions:
1 = Yes, we follow the best practice
0 = No, we do not follow the best practice
o Column C: Enter the appropriate code (1 or 0) to indicate if patients are allowed to self-report race and Hispanic Ethnicity
o Column D: Enter the appropriate code (1 or 0) to indicate if clinic is NOT using a multi-racial category AND system allows the collection and reporting of more than one race
o Column E: Enter the appropriate code (1 or 0) to indicate if patients are allowed to self-report preferred language
o Column F: Enter the appropriate code (1 or 0) to indicate if patients are allowed to self-report race and Hispanic Ethnicity
Clinic Level Population Counts: Enter counts for each clinic level population count listed below.
o Clinic Level Population Count 1: Total Adult Patients (Column G).
o Clinic Level Population Count 2: Total Adult Patients with Depression Diagnosis (296.2x, 296.3x or 300.4) (Column H).
o Clinic Level Population Count 3: Total Adult Patients with Depression NOS (311) code (Column I).
o Clinic Level Population Count 4: Total Adult Patients Depression Diagnosis (296.2x, 296.3x or 300.4) and Completed PHQ-9 (Column J).
Not Reporting (Column K): Please indicate if a clinic is not reporting for this cycle of data collection by entering the following code. Leave as “0” if a clinic is reporting data.
1 = Clinic is NOT reporting
o Please be advised that MNCM’s policy is that ALL clinic sites within a medical group submit their data through the DDS process. Likewise, this is a condition of participation for Minnesota Bridges to Excellence (BTE) and other pay-for-performance programs.
Reason not reporting (Column L): Provide a reason the clinic is not reporting. For example: The clinic has no patients meeting eligibility criteria.
3. Save the Excel file as a CSV file (please see page 33 for more information about how to save a CSV file). Click Browse to search and find the CSV file and click Submit File.
Depression Care Measures 2014 Direct Data Submission
Direct Data Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 36
Step 2 Review and Save Verify the numbers entered by reviewing all of the clinic site’s information for accuracy (no typos or duplicate patients). Click Save and Continue, or click Back to Step 1 to re-enter the counts.
Step 3: Upload Data Click Browse to search for the CSV file and click Upload CSV and Continue. The portal will now scan the CSV file to identify possible errors. The portal will then provide an “Upload Status” that will indicate if there are errors or warnings in the patient data file. You may have to click on Refresh. To view errors and warnings, please click View Errors & Warnings. If there are errors, the patient data file will need to be corrected and resubmitted to portal. Please refer to the Data Elements and Field Specifications (pages 26-31) to review the required data for each column.
1. Errors: Corrections must be made to the original Excel patient data file and a new patient data file uploaded (e.g.: A date of birth is out-of-range). If corrections to the patient data file are necessary, proceed to instructions below.
2. Warnings: Review possible errors and decide whether corrections are needed (e.g.: Health Plan Member ID is blank). If corrections to the patient data file are necessary, proceed to instructions below. If corrections are not necessary, click Continue to Step 4.
If corrections to the patient data file are necessary:
To start from Step 3: If corrections are only needed to the patient data file, make corrections in the original Excel file and save the corrected file with a new name. Then save as a new CSV file to upload. Do NOT make corrections in CSV file as this will destroy the format and alter the data. Go back to the portal submission page and click Re-Upload Data (csv) File. Begin again with Step 3 Upload Data.
To start from Step 1: Click Clear & Start Over to start the process completely over from Step 1 Enter Denominator. Please note: All denominator count entries and a new file upload will be necessary if Clear & Start Over is clicked.
Once the Data (CSV) File has been uploaded to the portal, click Continue to Step 4.
Step 4: Review & Submit Review and check each box of the Pre-Submission Quality Checklist and contact MNCM if you have any questions regarding the Pre-Submission Quality Checklist. Please review the quality checks for each item listed in the Data Elements and Field Specifications table on pages 26-31.
If you need to resubmit the patient data file, please click Re-Upload Data (CSV) File. If you need to resubmit the denominator counts, click Clear & Start Over at the bottom of the page.
If you have checked all the boxes, please click Continue.
The page will be refreshed. You will be asked to review the current measurement period’s preliminary rates for each clinic compared to the prior period’s data submission and consider any changes between the current period and the prior period. Provide an explanation in the text box for any changes or indicate that the data comparison is what you expected.
If you need to resubmit the patient data file, please click either Re-Upload Data (CSV) File or Clear & Start Over at the bottom of the page.
Depression Care Measures 2014 Direct Data Submission
Direct Data Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 37
If you need to review information in more detailed prior to submitting the file to MNCM, enter “Will Review” into the text box and then click Save as Draft. To access your information, you can click on Data Submission under the appropriate measurement period section on the HOME tab.
Once you have entered an explanation, click Save Notes.
You can download the data by clicking Download Data near the top of the data comparison section to see the visit types by viewing the additional columns on the right hand side of the document. This may be helpful in considering if you need to resubmit the patient data file.
When the data file is ready to submit to MNCM: Click Submit Data to MNCM and proceed to Step 5 Done.
Step 5: Done The patient data file has been successfully submitted. MNCM will send an e-mail that the data has been received.
Depression Care Measures 2014 Direct Data Submission
Direct Data Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 38
Section F: MNCM Validation The validation audit is conducted to verify that the submitted data matches the source data in the medical record. After the patient data file is successfully uploaded to the MNCM Data Portal, MNCM will contact the medical group about the validation process.
The validation audit may be conducted remotely via HIPAA secure WebEx technology for groups with an Electronic Medical Record (EMR). On-site audits will occur for medical groups with paper chart systems.
A. A medical record audit will occur with a groups’ last measurement period submission in the measurement year – after the February 2014 submission.
B. Medical audits may occur more frequently for groups with a history of unsuccessful direct data submissions.
MNCM Validation Process MNCM utilizes the NCQA (National Committee for Quality Assurance) “8 and 30” process for validation audits. The following method is used for each measure:
MNCM randomly selects 33 records for each clinic site for validation. At most, 30 records for each clinic site will be reviewed. The additional three records requested are oversamples to ensure there will be 30 records available on the day of the review.
MNCM auditor reviews the first eight records of the clinic site’s selected sample to verify that the submitted data matches the source data in the medical record.
If all of the first eight records reviewed are in perfect compliance (100%), the clinic site is determined to be in high compliance, and the MNCM auditor may determine that no further record review for that site is necessary.
If the first clinic site is in high compliance and the data collection process for all clinic sites within the medical group is identical, further review may be abbreviated at the discretion of the MNCM auditor.
If clinic sites are not in high compliance after review of the first eight records, the MNCM auditor will continue to review the remaining 22 records. If after review of all 30 records the clinic site is not in high compliance on all factors (less than 90%), the MNCM auditor will review the results with the clinic representative and communicate the results with MNCM. MNCM will then contact the medical group to develop a mutually-agreed upon re-submission plan. Re-submission plans will only be allowed for errors in the numerator portion.
Clinic sites that are not in high compliance or have not been in high compliance in a previous MNCM audit may be held to a more rigorous denominator certification and validation audit.
Validation Results: Once all clinics within a medical group have passed the MNCM validation process, MNCM will approve the data in the MNCM Data Portal, which generates and automatic e-mail to the medical group’s data contact that the data is verified and approved.
Please maintain the data submission files and other documents for two years.
Depression Care Measures 2014 Direct Data Submission
Direct Data Submission Instructions
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 39
Clinic Preparations for the Validation Audit All medical groups should plan for a validation audit.
MNCM auditor will contact medical group to schedule the audit.
MNCM will provide list of sample records to be audited.
Medical group or clinic site representative must be available to participate in the entire audit process. o For validation audits using an EMR, a medical group or clinic representative will retrieve and
display the selected records and various screens necessary to complete the validation.
During the audit, the patient’s date of birth is used to verify the correct record. All other patient information may be blocked out.
Clinics must have the following available at the time of the validation audit: o ALL requested patient records. o The “crosswalk” between the unique patient identifier and the patient’s name and DOB, so that
the record can be located by clinic staff at the time of validation audit. o Data collection forms and other notes describing location of data elements in patient record. o List of patients that were excluded.
After Validation Audit Following the successful submission and validation of the clinical data, medical groups can expect to see results posted in November on the MN HealthScores website at www.mnhealthscores.org. Results will also be included in the annual Health Care Quality Report later in the year. DDS results can also be found on the RESULTS tab on the MNCM Data Portal.
Depression Specific Results: A new functionality (reporting wizard) has been developed in the Results tab of the data portal. The goal is to provide users with the following capabilities:
Ease in selecting either process measure or outcome measure results.
o Process measures are based on the period the counts are submitted. o Outcome measures like remission are based on the patient’s index contact date.
Provide a patient level file back to the users; each medical group can access their own file of patients, similar to current functionality for diabetes and vascular patients. Visit level depression data that is submitted is not helpful as on output back to medical groups. This enhancement provides the information summarized by patient (initial PHQ-9, six month PHQ-9 score, achievement of remission, etc.). This could also be used to create or update a registry for groups that are not yet on an EHR.
When selecting parameters for the outcome measures, remember to specify only the index contact dates for patients that would have enough data. For example, if the most current submission is dates of service through 05/31/2013 you would need to count back seven months to get patients with enough data to measure the six month remission measure. Therefore the index contact date would need to be in a range where the upper index contact date limit is less than 10/31/2012. The portal cannot pull data it does not have, but you may think you are reporting on something other than what is available.
Pay-For-Performance Programs Medical groups will receive individual communications from health plans and MN Bridges to Excellence regarding their pay-for-performance programs that utilize DDS results.
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 40
Depression Care Measures 2014
Direct Data Submission (02/01/2013 to 01/31/2014 Dates of Service)
Appendices
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 41
Appendix A
Registration on the MNCM Data Portal
Your medical group/clinic should be registered with MN Community Measurement. Registration must be completed prior to data submission.
Registration must be completed once annually. Please refer to separate registration instructions for this process. A downloadable registration instruction guide is available on the MNCM Data Portal. Please contact MNCM if you did not register.
PLEASE NOTE: If your medical group opened or closed clinics after the 2014 Clinic and Provider Registration ended in February 2014, please contact MNCM to discuss updating registration and clinic information.
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 42
Appendix B
Resources to Help You Get Started
To identify your population, collect data, and get started in the data submission process, MN Community Measurement offers a selection of resources and tools.
To access the resources and tools for Depression measure, log in to the data portal at: https://data.mncm.org and click on the RESOURCES tab.
Select Depression RESOURCES from the drop-down menu.
The Depression RESOURCES screen contains Frequently Asked Questions, Depression Patient Assessment Tools and Depression resources.
The documents you will need to download include:
Depression Care Measures Data Collection Guide 2014
Depression Care Measures 2014 Excel Template
Depression Care Measures 2014 Denominator Template
Depression Care Measures 2014 Data Collection Form (most useful for medical groups and clinics using paper records)
Using Multiple Data Collectors | Inter-Rater Reliability (IRR) Ideally, one data collector or data collection process is preferred because it ensures that the data is collected in one consistent way. If, however, more than one person will abstract data, we recommend conducting several sample audits with all abstractors for training purposes to improve IRR.
Internal training could include a review of the guide and data collection form, and instructions for locating information in the clinic’s medical record. Also, refer to data collection errors made in previous submissions, make plans to improve the data collection process, and perform quality checks on the data. This ensures that the measurement specifications are interpreted consistently and that the data is collected in a uniform way.
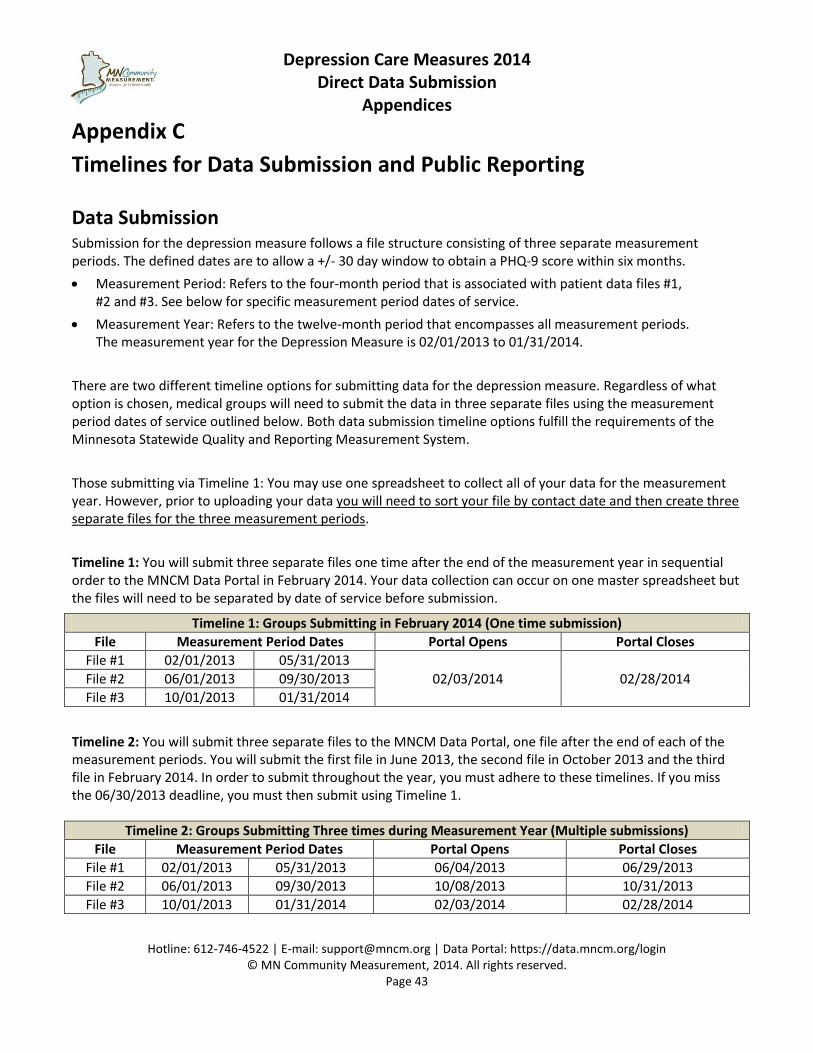
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 43
Appendix C
Timelines for Data Submission and Public Reporting
Data Submission Submission for the depression measure follows a file structure consisting of three separate measurement periods. The defined dates are to allow a +/- 30 day window to obtain a PHQ-9 score within six months.
Measurement Period: Refers to the four-month period that is associated with patient data files #1, #2 and #3. See below for specific measurement period dates of service.
Measurement Year: Refers to the twelve-month period that encompasses all measurement periods. The measurement year for the Depression Measure is 02/01/2013 to 01/31/2014.
There are two different timeline options for submitting data for the depression measure. Regardless of what option is chosen, medical groups will need to submit the data in three separate files using the measurement period dates of service outlined below. Both data submission timeline options fulfill the requirements of the Minnesota Statewide Quality and Reporting Measurement System.
Those submitting via Timeline 1: You may use one spreadsheet to collect all of your data for the measurement year. However, prior to uploading your data you will need to sort your file by contact date and then create three separate files for the three measurement periods.
Timeline 1: You will submit three separate files one time after the end of the measurement year in sequential order to the MNCM Data Portal in February 2014. Your data collection can occur on one master spreadsheet but the files will need to be separated by date of service before submission.
Timeline 2: You will submit three separate files to the MNCM Data Portal, one file after the end of each of the measurement periods. You will submit the first file in June 2013, the second file in October 2013 and the third file in February 2014. In order to submit throughout the year, you must adhere to these timelines. If you miss the 06/30/2013 deadline, you must then submit using Timeline 1.
Timeline 1: Groups Submitting in February 2014 (One time submission)
File Measurement Period Dates Portal Opens Portal Closes
File #1 02/01/2013 05/31/2013
02/03/2014 02/28/2014 File #2 06/01/2013 09/30/2013
File #3 10/01/2013 01/31/2014
Timeline 2: Groups Submitting Three times during Measurement Year (Multiple submissions)
File Measurement Period Dates Portal Opens Portal Closes
File #1 02/01/2013 05/31/2013 06/04/2013 06/29/2013
File #2 06/01/2013 09/30/2013 10/08/2013 10/31/2013
File #3 10/01/2013 01/31/2014 02/03/2014 02/28/2014
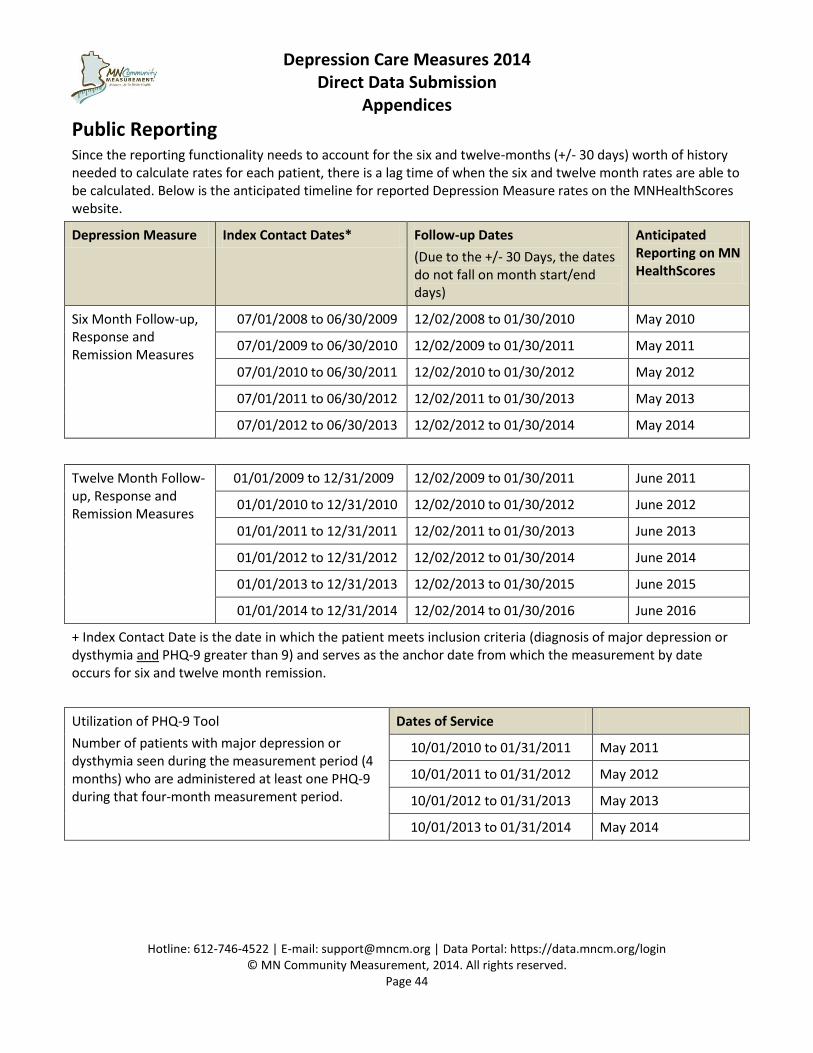
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 44
Public Reporting Since the reporting functionality needs to account for the six and twelve-months (+/- 30 days) worth of history needed to calculate rates for each patient, there is a lag time of when the six and twelve month rates are able to be calculated. Below is the anticipated timeline for reported Depression Measure rates on the MNHealthScores website.
Depression Measure Index Contact Dates* Follow-up Dates
(Due to the +/- 30 Days, the dates do not fall on month start/end days)
Anticipated Reporting on MN HealthScores
Six Month Follow-up, Response and Remission Measures
07/01/2008 to 06/30/2009 12/02/2008 to 01/30/2010 May 2010
07/01/2009 to 06/30/2010 12/02/2009 to 01/30/2011 May 2011
07/01/2010 to 06/30/2011 12/02/2010 to 01/30/2012 May 2012
07/01/2011 to 06/30/2012 12/02/2011 to 01/30/2013 May 2013
07/01/2012 to 06/30/2013 12/02/2012 to 01/30/2014 May 2014
Twelve Month Follow-up, Response and Remission Measures
01/01/2009 to 12/31/2009 12/02/2009 to 01/30/2011 June 2011
01/01/2010 to 12/31/2010 12/02/2010 to 01/30/2012 June 2012
01/01/2011 to 12/31/2011 12/02/2011 to 01/30/2013 June 2013
01/01/2012 to 12/31/2012 12/02/2012 to 01/30/2014 June 2014
01/01/2013 to 12/31/2013 12/02/2013 to 01/30/2015 June 2015
01/01/2014 to 12/31/2014 12/02/2014 to 01/30/2016 June 2016
+ Index Contact Date is the date in which the patient meets inclusion criteria (diagnosis of major depression or dysthymia and PHQ-9 greater than 9) and serves as the anchor date from which the measurement by date occurs for six and twelve month remission.
Utilization of PHQ-9 Tool
Number of patients with major depression or dysthymia seen during the measurement period (4 months) who are administered at least one PHQ-9 during that four-month measurement period.
Dates of Service
10/01/2010 to 01/31/2011 May 2011
10/01/2011 to 01/31/2012 May 2012
10/01/2012 to 01/31/2013 May 2013
10/01/2013 to 01/31/2014 May 2014
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 45
Appendix D
Notes about the PHQ-9 Test
PLEASE NOTE: If you have not already implemented the PHQ-9 assessment tool in your clinic, you need to start in order to participate in these measures, which are based on serial PHQ-9 assessments, and resulting scores. If you need to obtain a copy of the PHQ-9 tool, please access www.phqscreeners.com or you can download a copy from the data portal in the Resources section. Please include the following copy right information on all PHQ-9 assessment tools utilized by clinicians.
Developed by Drs. Robert L. Spitzer, Janet B.W. Williams, Kurt Kroenke and colleagues, with an educational grant from Pfizer Inc. No permission required to reproduce, translate, display or distribute.
Portal Functionality In order for the programming to correctly evaluate each patient record, the file must be sorted first by
PatientID and then by Contact Date with the contact dates in ascending or oldest to newest order. (e.g., A visit in March should be listed before a visit in May). This allows the portal program to evaluate each patient and incoming visit record correctly. Records that are out of sort order will not have the index and follow-up visits assigned appropriately and will not pass validation audit.
The portal is structured to look at each incoming patient record according to Medical Group ID and Patient ID to determine index visits and follow-up contacts.
For patients who HAVE NOT BEEN indexed: If a patient visit record is submitted to the portal with the correct diagnosis codes but a low PHQ-9 score, this record will be rejected and the portal will keep searching until a visit with diagnosis codes and PHQ-9 greater than nine occurs. Likewise, if a visit record is submitted with a high PHQ-9 score but no associated diagnosis codes, the record will be rejected.
For patients who HAVE BEEN indexed: All subsequent visits are allowed to match up to that patient. This is to allow for the various settings in which a PHQ-9 can be administered (phone, e-visit or other type of visit) for which there may not be a diagnosis code or insurance information.
If the patient does not yet have an index visit and other diagnosis codes are submitted, the records containing the other diagnosis will cause an error on file submission and will need to be removed.
The index visit record will contain the information that is stored for each patient. This record contains the clinic ID, the provider ID, gender, zip code, diagnosis code and insurance coverage information. The clinic site and the provider ID that are a part of the indexed visit is where the patient will be attributed to. The insurance coverage will be updated if it changes, but the rest of this record will remain the same.
A patient’s measurement period will end 13 months from the activation date; this allows for the +30 days to obtain subsequent PHQ-9 scores. If, after this point a patient does meet the inclusion criteria again by having a PHQ-9 score above nine; a new index/re-activation record will be created and measurement will “start over” for his patient. In these situations, the patient is still meeting criteria for inclusion.
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 46
Appendix E
Explaining the Depression Measures to Providers and Clinical Staff
These measures apply to patients who are diagnosed with major depression or dysthymia; either newly diagnosed or have existing depression.
If you are coding a patient’s visit as 296.2x, 296.3x or 300.4, the codes for major depression or dysthymia, then you should also be using the PHQ-9 tool.
Need to have both of the following: A confirmed diagnosis of major depression or dysthymia and a PHQ-9 score greater than nine in order to be eligible for the measure denominator. Patients are not eligible to be included in the measure denominator based on PHQ-9 score alone.
For behavioral health providers, the diagnoses need to be in the primary position. For primary care providers, the diagnoses are either primary or secondary (any position).
It is an expectation that patients with major depression or dysthymia are assessed on an ongoing basis using the PHQ-9 tool and that the PHQ-9 is used with every patient visit; however MNCM cannot dictate how frequently you administer the PHQ-9 to your patients. It is our experience that groups that are only trying to obtain a six month score miss the benefits re-assessment of patient status and need for intervention sooner that the point of measurement.
Once the patient is identified as having depression and an elevated PHQ-9 score (inclusion criteria), then any time a PHQ-9 is administered, the score needs to be included in the submission, regardless of the reason for the visit/contact.
Each patient’s starting point is different (index visit). For the six month remission measure, a window of time is allowed to connect with the patient, either 30 days prior to the six month date or 30 days after the six month date. It takes seven months of data collection to report the outcome of the six month measure. The data portal calculates the reporting period for each patient by date. Only scores within this 60 day window “count” towards measuring remission. The most recent PHQ-9 score within this window is the score that will be used.
Remission is defined as a PHQ-9 score of less than five. This corresponds with the validated PHQ-9 tool interpretation of scores:
o 0 to 4 No depressive symptoms o 5 to 9 Mild depression o 10 to 14 Moderate depression o 15 to 19 Moderately severe depression o 20 to 27 Severe depression
Patients who are not assessed within the 60 day window are considered to “not be in remission” and are counted in the denominator of the remission measure.
Rate is calculated as follows: # adult pts with a PHQ-9 score < 5 at 6 months (+/- 30 days)
# adult pts with depression with index contact PHQ-9 > 9
The patient data file is structured at the visit/contact level. For example, a patient seen and assessed in February, June and August would have three records in the file, one for each PHQ-9 score obtained.
There are several measures that are captured through a single file submission process.
X 100
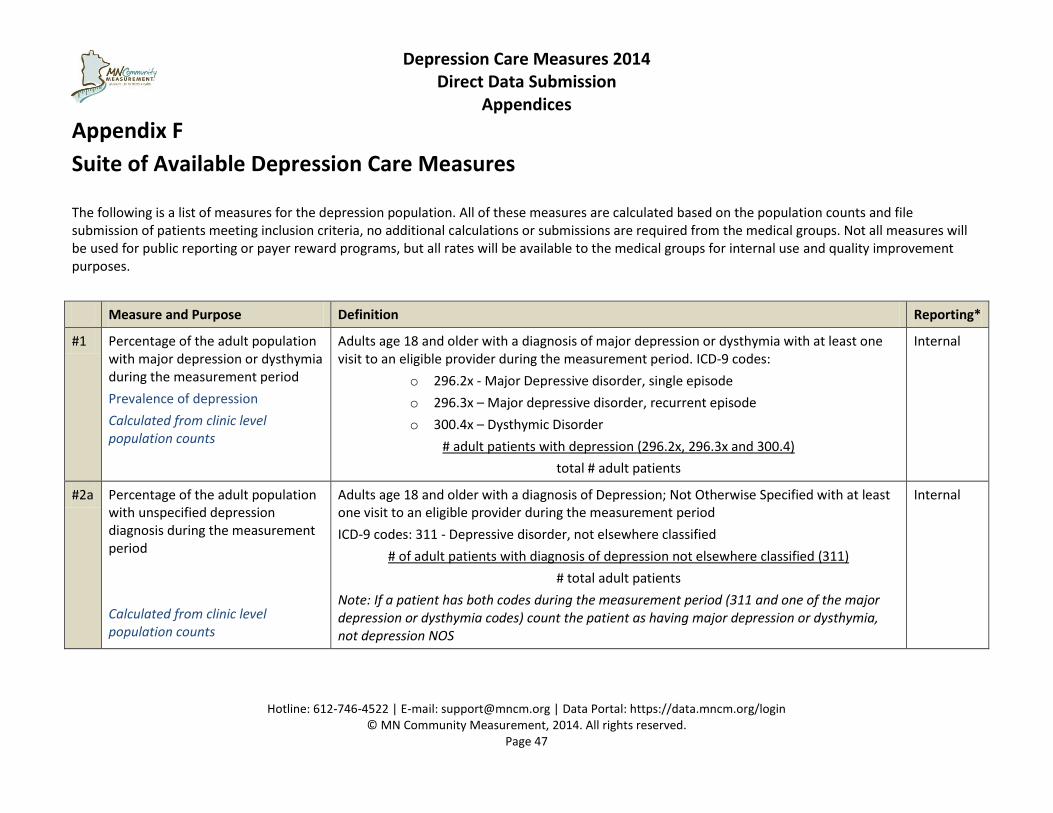
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 47
Appendix F
Suite of Available Depression Care Measures
The following is a list of measures for the depression population. All of these measures are calculated based on the population counts and file submission of patients meeting inclusion criteria, no additional calculations or submissions are required from the medical groups. Not all measures will be used for public reporting or payer reward programs, but all rates will be available to the medical groups for internal use and quality improvement purposes.
Measure and Purpose Definition Reporting*
#1 Percentage of the adult population with major depression or dysthymia during the measurement period
Prevalence of depression
Calculated from clinic level population counts
Adults age 18 and older with a diagnosis of major depression or dysthymia with at least one visit to an eligible provider during the measurement period. ICD-9 codes:
o 296.2x - Major Depressive disorder, single episode
o 296.3x – Major depressive disorder, recurrent episode
o 300.4x – Dysthymic Disorder
# adult patients with depression (296.2x, 296.3x and 300.4)
total # adult patients
Internal
#2a Percentage of the adult population with unspecified depression diagnosis during the measurement period
Calculated from clinic level population counts
Adults age 18 and older with a diagnosis of Depression; Not Otherwise Specified with at least one visit to an eligible provider during the measurement period
ICD-9 codes: 311 - Depressive disorder, not elsewhere classified
# of adult patients with diagnosis of depression not elsewhere classified (311)
# total adult patients
Note: If a patient has both codes during the measurement period (311 and one of the major depression or dysthymia codes) count the patient as having major depression or dysthymia, not depression NOS
Internal
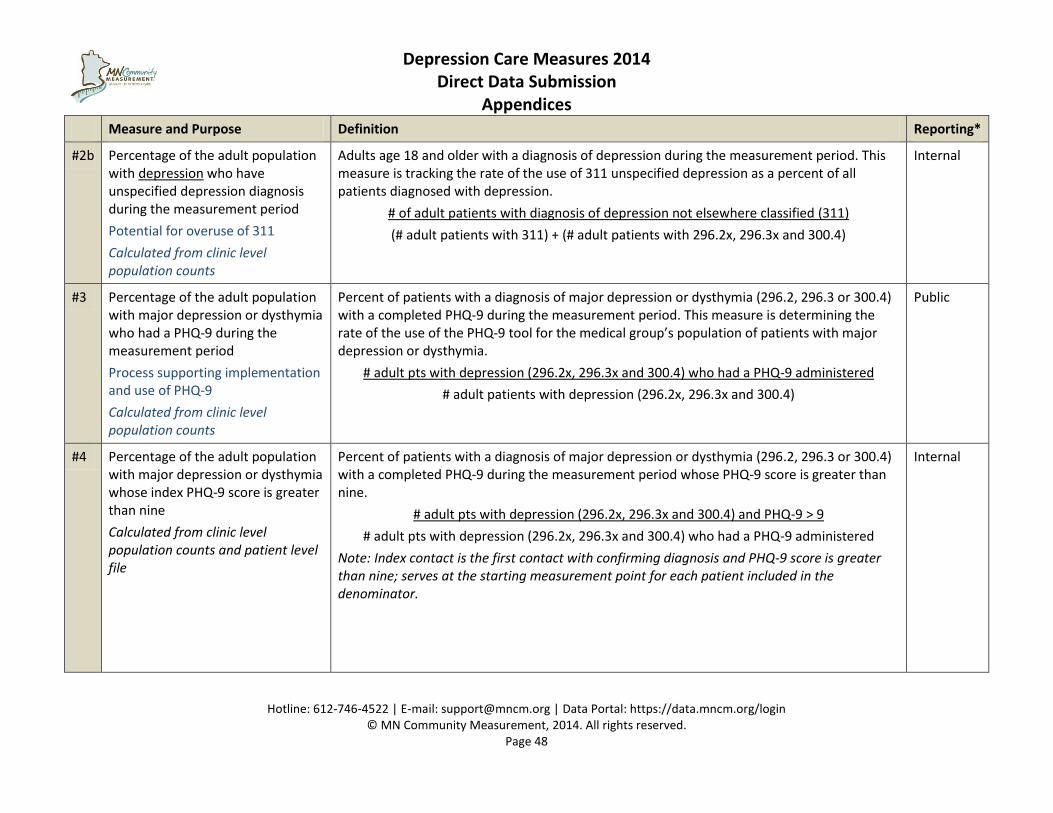
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 48
Measure and Purpose Definition Reporting*
#2b Percentage of the adult population with depression who have unspecified depression diagnosis during the measurement period
Potential for overuse of 311
Calculated from clinic level population counts
Adults age 18 and older with a diagnosis of depression during the measurement period. This measure is tracking the rate of the use of 311 unspecified depression as a percent of all patients diagnosed with depression.
# of adult patients with diagnosis of depression not elsewhere classified (311)
(# adult patients with 311) + (# adult patients with 296.2x, 296.3x and 300.4)
Internal
#3 Percentage of the adult population with major depression or dysthymia who had a PHQ-9 during the measurement period
Process supporting implementation and use of PHQ-9
Calculated from clinic level population counts
Percent of patients with a diagnosis of major depression or dysthymia (296.2, 296.3 or 300.4) with a completed PHQ-9 during the measurement period. This measure is determining the rate of the use of the PHQ-9 tool for the medical group’s population of patients with major depression or dysthymia.
# adult pts with depression (296.2x, 296.3x and 300.4) who had a PHQ-9 administered
# adult patients with depression (296.2x, 296.3x and 300.4)
Public
#4 Percentage of the adult population with major depression or dysthymia whose index PHQ-9 score is greater than nine
Calculated from clinic level population counts and patient level file
Percent of patients with a diagnosis of major depression or dysthymia (296.2, 296.3 or 300.4) with a completed PHQ-9 during the measurement period whose PHQ-9 score is greater than nine.
# adult pts with depression (296.2x, 296.3x and 300.4) and PHQ-9 > 9
# adult pts with depression (296.2x, 296.3x and 300.4) who had a PHQ-9 administered
Note: Index contact is the first contact with confirming diagnosis and PHQ-9 score is greater than nine; serves at the starting measurement point for each patient included in the denominator.
Internal
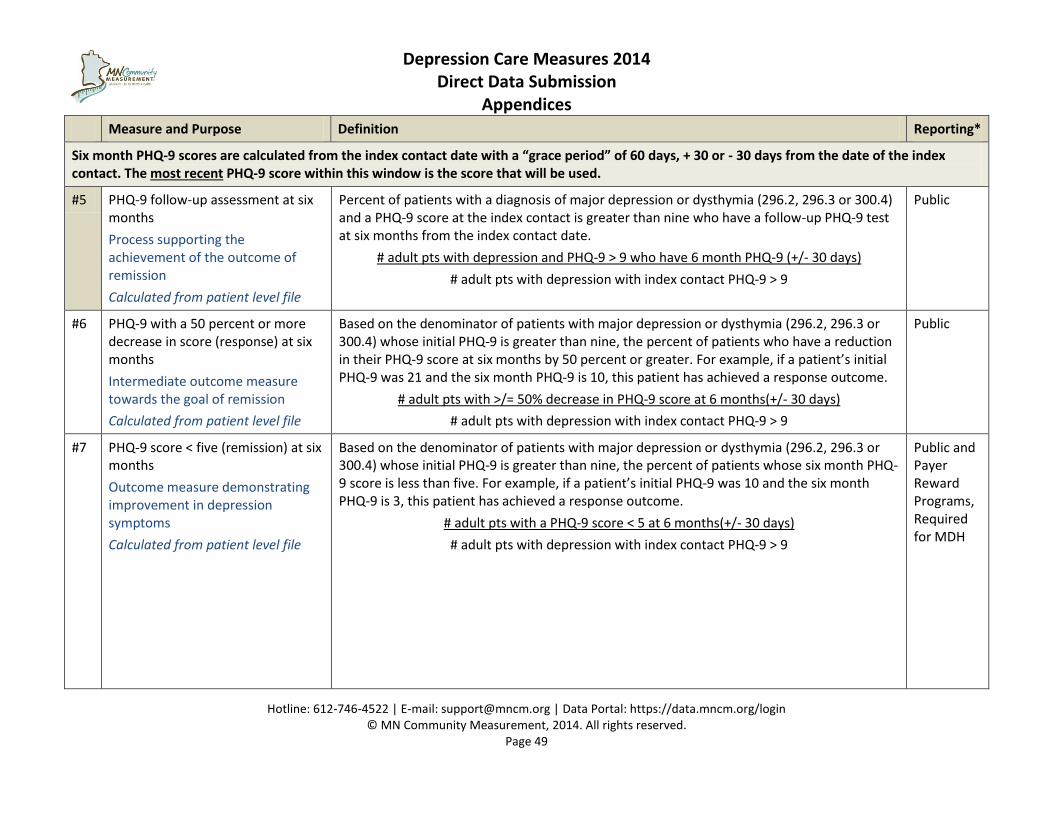
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 49
Measure and Purpose Definition Reporting*
Six month PHQ-9 scores are calculated from the index contact date with a “grace period” of 60 days, + 30 or - 30 days from the date of the index contact. The most recent PHQ-9 score within this window is the score that will be used.
#5 PHQ-9 follow-up assessment at six months
Process supporting the achievement of the outcome of remission
Calculated from patient level file
Percent of patients with a diagnosis of major depression or dysthymia (296.2, 296.3 or 300.4) and a PHQ-9 score at the index contact is greater than nine who have a follow-up PHQ-9 test at six months from the index contact date.
# adult pts with depression and PHQ-9 > 9 who have 6 month PHQ-9 (+/- 30 days)
# adult pts with depression with index contact PHQ-9 > 9
Public
#6 PHQ-9 with a 50 percent or more decrease in score (response) at six months
Intermediate outcome measure towards the goal of remission
Calculated from patient level file
Based on the denominator of patients with major depression or dysthymia (296.2, 296.3 or 300.4) whose initial PHQ-9 is greater than nine, the percent of patients who have a reduction in their PHQ-9 score at six months by 50 percent or greater. For example, if a patient’s initial PHQ-9 was 21 and the six month PHQ-9 is 10, this patient has achieved a response outcome.
# adult pts with >/= 50% decrease in PHQ-9 score at 6 months(+/- 30 days)
# adult pts with depression with index contact PHQ-9 > 9
Public
#7 PHQ-9 score < five (remission) at six months
Outcome measure demonstrating improvement in depression symptoms
Calculated from patient level file
Based on the denominator of patients with major depression or dysthymia (296.2, 296.3 or 300.4) whose initial PHQ-9 is greater than nine, the percent of patients whose six month PHQ-9 score is less than five. For example, if a patient’s initial PHQ-9 was 10 and the six month PHQ-9 is 3, this patient has achieved a response outcome.
# adult pts with a PHQ-9 score < 5 at 6 months(+/- 30 days)
# adult pts with depression with index contact PHQ-9 > 9
Public and Payer Reward Programs, Required for MDH
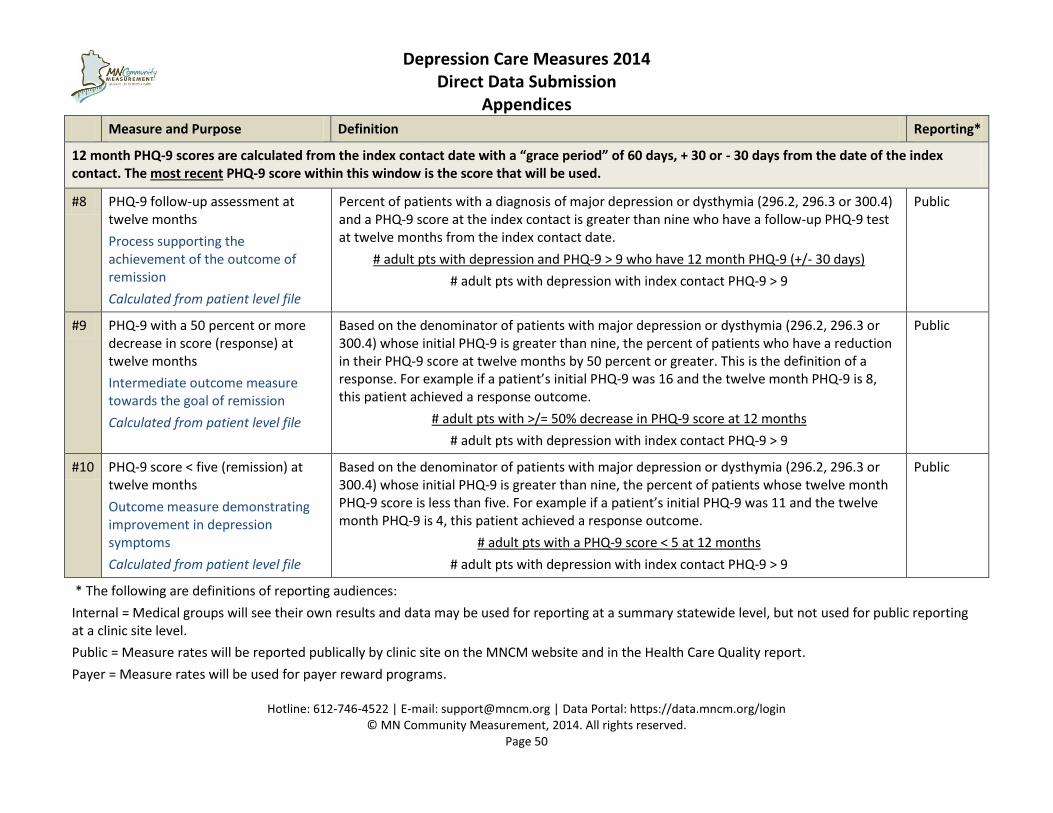
Depression Care Measures 2014 Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 50
Measure and Purpose Definition Reporting*
12 month PHQ-9 scores are calculated from the index contact date with a “grace period” of 60 days, + 30 or - 30 days from the date of the index contact. The most recent PHQ-9 score within this window is the score that will be used.
#8 PHQ-9 follow-up assessment at twelve months
Process supporting the achievement of the outcome of remission
Calculated from patient level file
Percent of patients with a diagnosis of major depression or dysthymia (296.2, 296.3 or 300.4) and a PHQ-9 score at the index contact is greater than nine who have a follow-up PHQ-9 test at twelve months from the index contact date.
# adult pts with depression and PHQ-9 > 9 who have 12 month PHQ-9 (+/- 30 days)
# adult pts with depression with index contact PHQ-9 > 9
Public
#9 PHQ-9 with a 50 percent or more decrease in score (response) at twelve months
Intermediate outcome measure towards the goal of remission
Calculated from patient level file
Based on the denominator of patients with major depression or dysthymia (296.2, 296.3 or 300.4) whose initial PHQ-9 is greater than nine, the percent of patients who have a reduction in their PHQ-9 score at twelve months by 50 percent or greater. This is the definition of a response. For example if a patient’s initial PHQ-9 was 16 and the twelve month PHQ-9 is 8, this patient achieved a response outcome.
# adult pts with >/= 50% decrease in PHQ-9 score at 12 months
# adult pts with depression with index contact PHQ-9 > 9
Public
#10 PHQ-9 score < five (remission) at twelve months
Outcome measure demonstrating improvement in depression symptoms
Calculated from patient level file
Based on the denominator of patients with major depression or dysthymia (296.2, 296.3 or 300.4) whose initial PHQ-9 is greater than nine, the percent of patients whose twelve month PHQ-9 score is less than five. For example if a patient’s initial PHQ-9 was 11 and the twelve month PHQ-9 is 4, this patient achieved a response outcome.
# adult pts with a PHQ-9 score < 5 at 12 months
# adult pts with depression with index contact PHQ-9 > 9
Public
* The following are definitions of reporting audiences:
Internal = Medical groups will see their own results and data may be used for reporting at a summary statewide level, but not used for public reporting at a clinic site level.
Public = Measure rates will be reported publically by clinic site on the MNCM website and in the Health Care Quality report.
Payer = Measure rates will be used for payer reward programs.
Depression Care Measures 2014
Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 51
Appendix G
About MN Community Measurement and Measure Development
Mission and Vision of MN Community Measurement (MNCM) The mission of MN Community Measurement is to accelerate the improvement of health by publicly reporting health care information. MN Community Measurement’s vision is to:
Be the trusted source for performance measurement and public reporting of quality data across the spectrum of health care that;
Drive change towards more safe, effective, patient centered, timely, efficient, and equitable care;
Be a resource used by providers to improve care and patients to make better decisions; and
Catalyze our community to work together on health care measurement to reduce administrative costs and maximize value.
About the Measure Development Measures are selected according to MN Community Measurement’s Strategic Measurement Development Process. An impact and recommendation document presents the topic for discussion at the Measurement and Reporting Committee (MARC). Topics for measure development must meet the following criteria for consideration of development:
Will the measure/s make a difference?
o Degree of impact
o Degree of improvability
o Degree of inclusiveness
o Degree of performance variation
o Outcome measures desired
Will the measure improve care by affecting the patient/physician relationship?
o Pass the feasibility test (resources/barriers/culture)
o Align with national, regional and local priorities
o Relevant to consumers
o Support and enhance the patient/provider relationship
Impact of Major Depression and Dysthymia According to National Institute of Mental Health (NIMH), 6.7 percent of the U.S. population ages 18 and older (14.8 million people) in any given year have a diagnosis of a major depressive disorder. Major depression is the leading cause of disability in the U.S. for ages 15 - 441. Additionally, dysthymia accounts for an additional 3.3
1 National Institute of Mental Health www.nimh.nih.gov “The Numbers Count: Mental Disorders in America” 2008
Depression Care Measures 2014
Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 52
million Americans. The Center for Disease Control and Prevention states that 15.7% of people report being told by a health care professional that they had depression at some point in their lifetime. Persons with a current diagnosis of depression and a lifetime diagnosis of depression or anxiety were significantly more likely than persons without these conditions to have cardiovascular disease, diabetes, asthma and obesity and to be a current smoker, to be physically inactive and to drink heavily.2 Suicide rates for Minnesotans are 10.4 per 100,000 or 1.3 suicides per day, with the highest rates among the following groups: Males (4 times greater than females), ages 30 to 49 years, and non-Hispanic whites.3
Depression Care in Minnesota Efforts to improve care and outcomes for patients with depression have been accelerated in Minnesota by two related initiatives. DIAMOND- “Depression Improvement Across MN, Offering a New Direction” is a new care model with payment restructuring and outcome measurement; primary care clinics are participating in this project. MN Community Measurement (MNCM) is partnering with Bridges to Excellence (BTE), Minnesota Department of Health and other payers to provide depression outcome measurement for all adults with major depression or dysthymia who are treated in a primary care or behavioral health setting. Patient outcomes for both of these initiatives are tracked according to the patient’s PHQ-9 depression scores over time.
What is the difference between DIAMOND and MNCM Depression? Measures for the two initiatives are the same in terms of six and twelve month outcomes for depression; however, the patient populations are slightly different. DIAMOND is measuring those patients who agree to be in the new care model, whereas MNCM measures are applied the whole adult population of patients with major depression or dysthymia. DIAMOND clinics that want to participate in the BTE program need to submit data for all their patients with depression. DIAMOND is also capturing additional measures for the care management process. For more information about the DIAMOND initiative, please access the ICSI website at www.icsi.org.
2 Centers for Disease Control and Prevention 2006 Behavioral Risk Factor Surveillance
3 Suicide Prevention Resource Center www.sprc.org/stateinformation “Minnesota Suicide Prevention Fact Sheet”
DIAMOND
Only reporting for patients with
depression and a PHQ-9 score greater
than nine who opt in to the care model
Partial population reporting
Monthly Data Collection
Additional data elements and measures
MNCM Depression
All patients with major depression
and a PHQ-9 score greater than nine
Full population reporting
Data collection three times/year
(or annual submission of three
separate files)
So, for those clinics participating in DIAMOND Submit all your patients with depression, not just those who enrolled in DIAMOND
Depression Care Measures 2014
Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 53
How is the Depression Submission Different from Other DDS Measures?
Example: Diabetes Measure A snapshot with a retrospective look back
Over the last year what was the value of
the most recent A1c
File = Patient Level Records; one row for
each patient
Annual submission
Depression Measure Prospective, looking forward. Longitudinal
over time
Patients meet inclusion criteria and then
measured for outcome at six months
File = Visit Level Record; a single patient
has many rows one for each contact
with PHQ-9 test administration
Three times a year submission
(Or annual submission of three separate
files)
Depression Care Measures 2014
Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 54
Appendix F
About Direct Data Submission (DDS)
The goal of Direct Data Submission (DDS) is to collect data from medical groups on specific health care conditions and publicly report comparable rates of health care quality at the clinic site level. All medical groups follow the same instructions for population identification and data collection. MNCM certifies methodologies prior to data collection. Then, each medical group submits data to MNCM via a secure, online data portal. As an independent auditor and as a service to each medical group, MNCM validates the data for accuracy, calculates rates from the validated data, and publicly reports the data on the MNCM Web site www.mnhealthscores.org.
Required Reporting DDS fulfills participation requirements for the Minnesota Department of Health’s Minnesota Statewide Quality Reporting and Measurement System as well as other health plan pay-for-performance programs and Minnesota Bridges to Excellence. In addition, DDS results can be used by medical groups for quality improvement purposes.
Health Care Homes If your medical group has providers or clinics that are certified by the Minnesota Department of Health as a health care home then you will need to enter the patient’s primary care provider NPI in the data file. Please note the additional health care home data fields have been removed from the specifications and are NOT part of data submission for health care homes.
DDS Terms and Conditions To participate in the DDS process, medical groups must agree to:
MNCM’s DDS terms and conditions (sign electronically on the MNCM Data Portal).
Complete a Business Associate Agreement with MNCM (signed electronically on the MNCM Data Portal).
Submit a patient-level file to the secure MNCM Data Portal that automatically calculates rates.
Participate in the data validation process as required by MNCM.
Have results publicly reported on www.mnhealthscores.org and other reports.
Submit data for ALL clinic sites.
Submit data in required format (.csv).
Submit data in good faith.
Adhere to and follow all data submission timelines and formatting specifications.
Medical groups also understand that:
MNCM works with corresponding health plans to determine Primary payer type (Commercial/Private, Medicaid, Medicare, uninsured/self/pay) on your behalf to reduce burden
The MN Bridges to Excellence program and most Minnesota health plans only accept results generated from the DDS method for their incentive programs, because the results can be validated
Depression Care Measures 2014
Direct Data Submission
Appendices
Hotline: 612-746-4522 | E-mail: [email protected] | Data Portal: https://data.mncm.org/login © MN Community Measurement, 2014. All rights reserved.
Page 55
Compliance with Federal and State Regulations Our legal counsel has assured us that the DDS method complies with applicable provisions of the Health Insurance Portability and Accountability Act (HIPAA), Health Information Technology for Economic and Clinical Health (HITECH) Act, and Minnesota statute as long as we are acting as a business associate to each participating medical group (e.g., by gathering and submitting data on its behalf) and have a signed Business Associate Agreement (BAA) with the medical group. The BAA can be signed electronically on the MNCM Data Portal, or MNCM is open to signing a medical group’s standard BAA document version if certain key provisions from MNCM’s BAA are added to the group’s standard BAA. The BAA is signed once and remains in effect for all DDS measures.
Health Insurance Portability and Accountability Act (HIPAA) Law:
The activities of data collection, data submission, public reporting and use of results for quality improvement are considered within the scope of “health care operations” associated with the medical group quality improvement efforts.
The federal HIPAA law specifically allows release of individually identifiable health information - without the consent or authorization of the individual - for treatment, payment and health care operations of, or for, the provider.
MNCM’s business associate agreement has been updated to include all provisions required by the HITECH Act and its implementing regulations.
Minnesota Statute:
The primary governing Minnesota statute is MN Stat. Section 144.335.
Subd. 3a. entitled "Patient consent to release of records; liability" states: (a) A provider, or a person who receives health records from a provider, may not release a patient's health records to a person without a signed and dated consent from the patient or the patient's legally authorized representative authorizing the release, unless the release is specifically authorized by law.
However, the statute does not restrict release (without patient authorization) to only those circumstances authorized by state law – the statute also applies to a release authorized by federal law.
Legal counsel assures us that it is reasonable to conclude that the HIPAA privacy regulation does specifically authorize the release of such information. A covered entity is authorized by HIPAA to release patient information for, among other things, health care operations and to its business associate that is providing such health care operations on its behalf. As stated above, the services MNCM is engaged in with providers falls within the scope of health care operations, and MNCM is acting as a business associate to the medical groups when performing the services discussed above.