damned if you don’t - up.ac.za 2019 presentations/damned... · outline • the importance of...
TRANSCRIPT

Damnedifyoudon’t-improvingoutcomeintheveryprematureinfant
JessievanDykDivisionHead,NeonatologyStJoseph’sHealthCentre
UniversityofToronto
Conflictofinterest
Nothingtodeclare…

Outline
• Theimportanceofhavingaplan• Thegoldenhour• Smallbabyprotocol• Preventingmorbidity• Family-integratedcare
PrematureBirth• ‘Burdenofprematurity’• Majorityofpretermsfreeofmajormorbidity
• Majormorbidityaccountsfor6-25%– Cerebralpalsy– Visionimpairment– Hearingimpairment– Cognitiveimpairment
• 50-70%mayhaveminormorbidities
Starthere…
Haveaplan…
• Borrowcarefully• Takeintoaccountlocalresources&expertise
• Ensurepre-implementationtraining&audits
• Guidelinesensureeveryonereceivesatleastminimumbeststandardofcare…butleaveroomforpatientvariation
• Canidentifysystemerrorsordeficiencies,especiallywhenbuiltintoEMR’s

Antenatalcounseling
• RevisedCanadianPaediatricSocietystatementadvisesprognosis-basedapproachthattakesintoaccount
ü BestestimateofGAü Estimatedfetalweightü Receiptofantenatalsteroidsü Singletonversusmultiplepregnancyü FetalstatusandpresenceofanomaliesonUSü Placeofbirth


Justtokeepthingsinteresting…
23wksGAn(%)
24wksGAn(%)
25wksGAn(%)
26wksGAn(%)
Fullweek 92(94.8) 272(80.5) 277(64.1) 222(48.8)
0-3 40(95.2) 172(85.6) 174(69.6) 157(55.9)
4-6 52(94.5) 100(73) 103(56.6) 65(37.4)
95%CI (-8.8,10.2) (3.1,22.1) (3.3,22.7) (8.8,28.2)
p-value 1 0.0064 0.0073 0.004
Whataboutatthewatershedweeks?234-6vs.240-3weeks(p-value=0.14)244-6vs.250-3weeksGA(p-value=0.6)Thusnodifferenceincompositeoutcome(neonatalmorbidityandmortality)
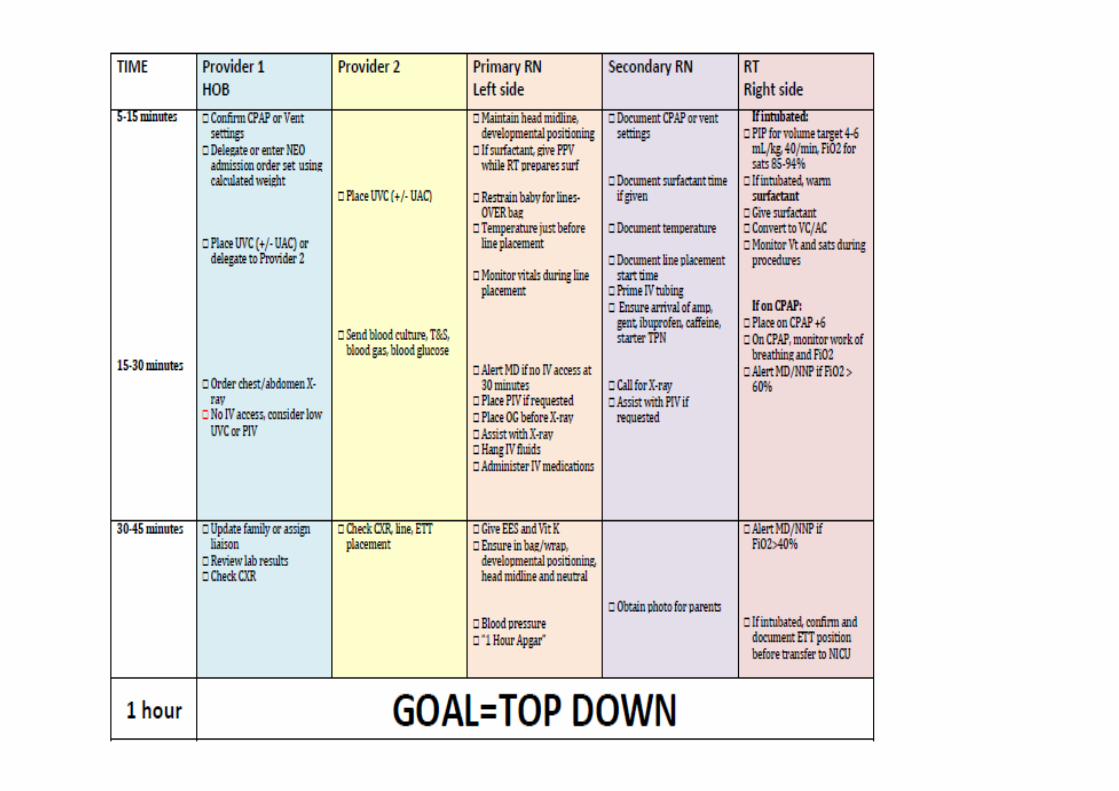
Thegoldenhour
Successfulstabilisationbeginswithobstetricalmanagement
• Deliverinahigh-riskperinatalcentre• Antenatalsteroids• AntenatalMgSo4• Preventchorioamnionitis• Timely,gentle,atraumaticdelivery-AssessmentandmanagementbyexperiencedMFMspecialist-Considerdeliveringencaul-Caesariansection(classical)ifmalpositioning/fetaldistress• Delayedumbilicalcordclampingifpossible

Careofmotheratriskforextremelypretermdelivery
AssessingGA• USmostaccurate(afterIVF)• 1sttrimestercrown-rumplength
accuratewithin3-8days• Degreeofimprecisionincreases
withGA(±10daysat16-22wks,±14daysat24wks)
Modeofdelivery• Notenoughevidencetosupport
routineC-section(potentialharmtomothervsbenefitforinfant,weighharmsvsbenefitforeachcase)
Antenatalsteroids• Debates:infants<24wksGAnot
initiallyincludedinNIHconsensusstatement,fearsofharmafter>1course(maxefficacywithin7days)
• Latestguideline:givetoallmothersinTPTLat≥22wksGAwhereearlyintensivecareisanticipated,probablynoharminrepeatedcourses(reducedRDSandothermorbidities,noevidenceofharminlaterchildhood)
Placeofcare• Improvedmortalityandmorbidity
withdeliveryattertiarycentresàtransferin-uterowheneverpossible

• 194interventioncasesvs194retrospectivelymatchedcontrols
• Comprehensiveprotocolchange-dedicateddeliveryarea,improvedplanningandcommunicationaswellaschangesinpractice–cordbloodsampling,temperaturecontroletc
• Improvedadmissiontemperature(p<0.001),BPD(p=0.028)andlate-onsetsepsis(p=0.035)
• Trendtowardslowerratesofearlybloodtransfusionandventilationduration
‘Gentleresuscitation’…
• ‘Mybiasisthatthedeliveryroombeepershouldinitiateafocusontransition-adaptationand,withpatienceandafterabitoftime,resuscitationifnecessary.’
• ‘Thereisperhapsnothingmoredangerousforthepretermlung
thanananxiousphysicianwithanendotrachealtubeandabag.’
AlanJobe,JournalofPediatrics,2005


• Idealstartingoxygenlevelforpreterminfantsremainsunknown
• Mostinfants<32weekswillrequireatleastsomeoxygen
Pediatrics,2019
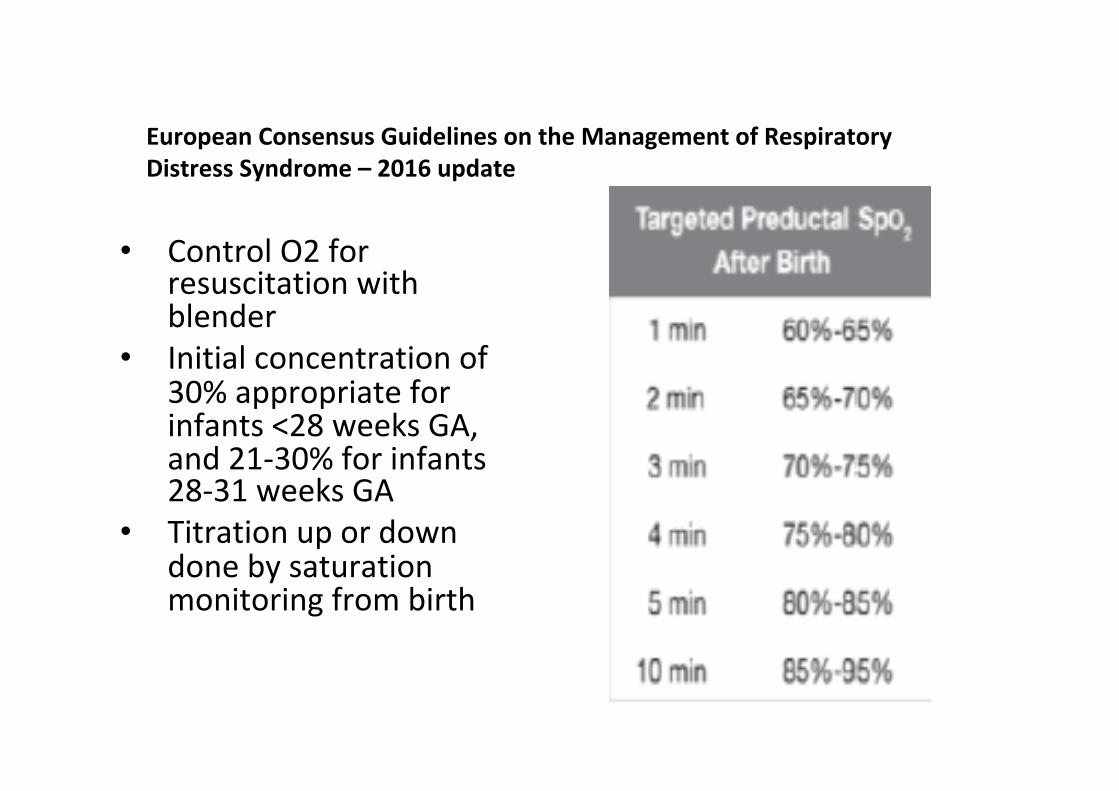
EuropeanConsensusGuidelinesontheManagementofRespiratoryDistressSyndrome–2016update
• ControlO2forresuscitationwithblender
• Initialconcentrationof30%appropriateforinfants<28weeksGA,and21-30%forinfants28-31weeksGA
• Titrationupordowndonebysaturationmonitoringfrombirth
2015ILCORguidelines:delayedcordclamping
• Outcomes:mortality,severeIVH,anyIVH,haemodynamicstability,hyperbilirubinemia,neurodevelopment
• Sixteenarticlesincluded-12RCTs(691cases)+4non-RCTs(811cases)• NodifferenceinmortalityorsevereIVH• Dataawaitedforneurodevelopment• ReducedanyIVHandimprovedhaemodynamicstabilityILCORrecommendation:suggestDCCfor30secforpreterminfantsnotrequiringimmediateresuscitationafterbirth


‘Smallbabyprotocol’
• Pediatrics,2015• 2yearsafterimplementingspecifictreatmentprotocols• Reducedchroniclungdisease(47.5%to34.5%,p=0.097),
hospital-acquiredinfection(39.3%to19.4%,p<0.001)• Lessinfantsdischargedwithgrowthrestriction(62.3%to
37.3%,p=0.001)• Lowerresourceutilisation(decreasedlabtestsand
radiographs)


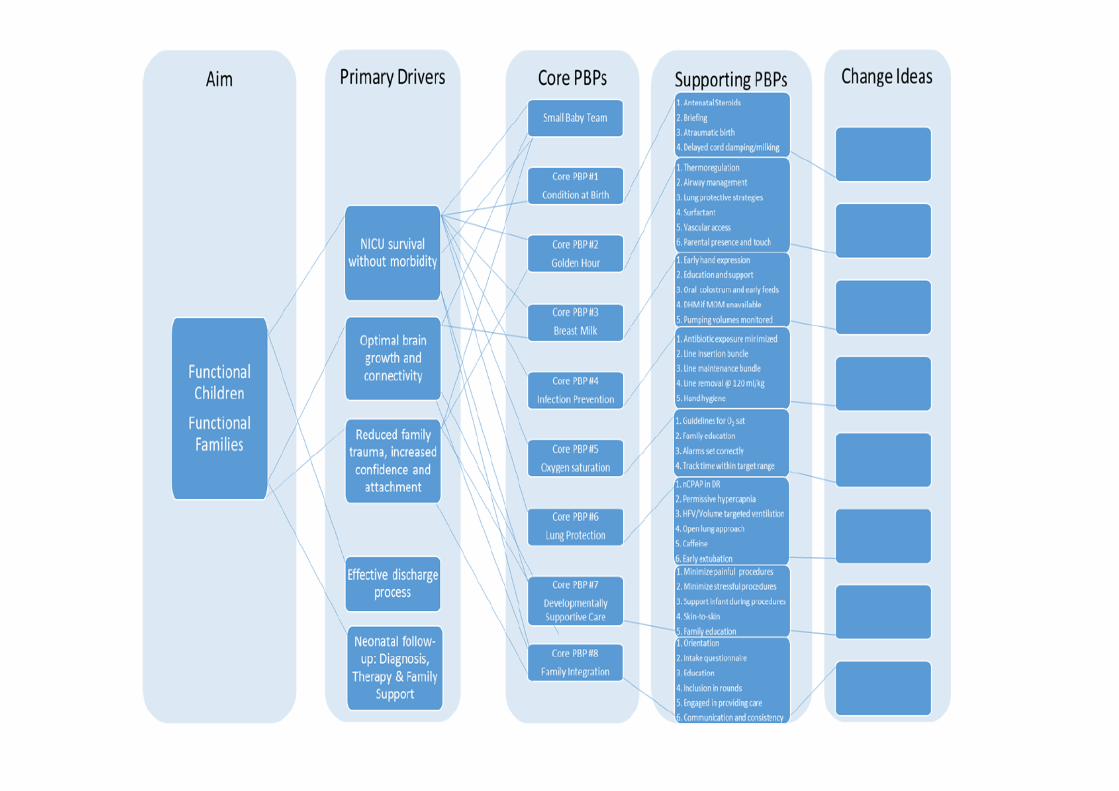
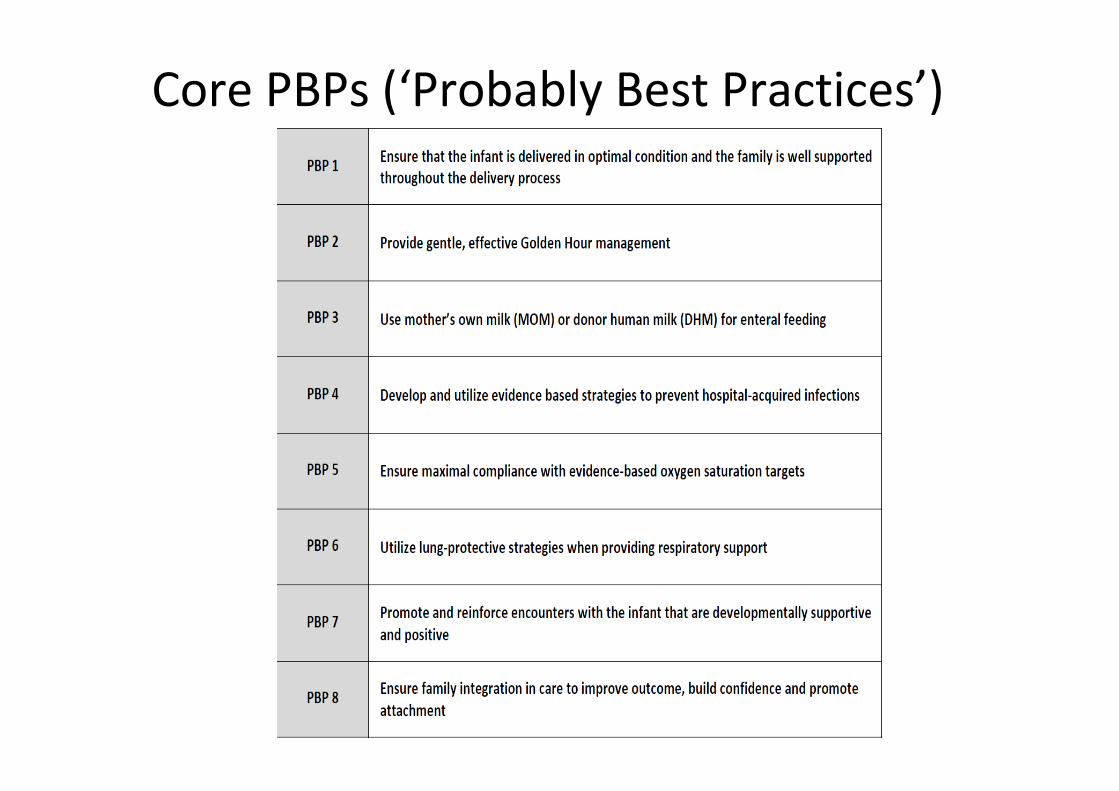
CorePBPs(‘ProbablyBestPractices’)

PotentiallyBetterPractice1PBP1:Ensurethattheinfantisdeliveredinoptimalconditionandthefamilyiswellsupportedthroughoutthedeliveryprocess
SupportingPBPs:1. Administerafullcourseofantenatalcorticosteroidsto
mother2. Conductapre-deliverybriefingthatincludesObstetrics,
NICUteamandthefamily3. Minimizebirthtrauma4. Practicedelayedcordclamping
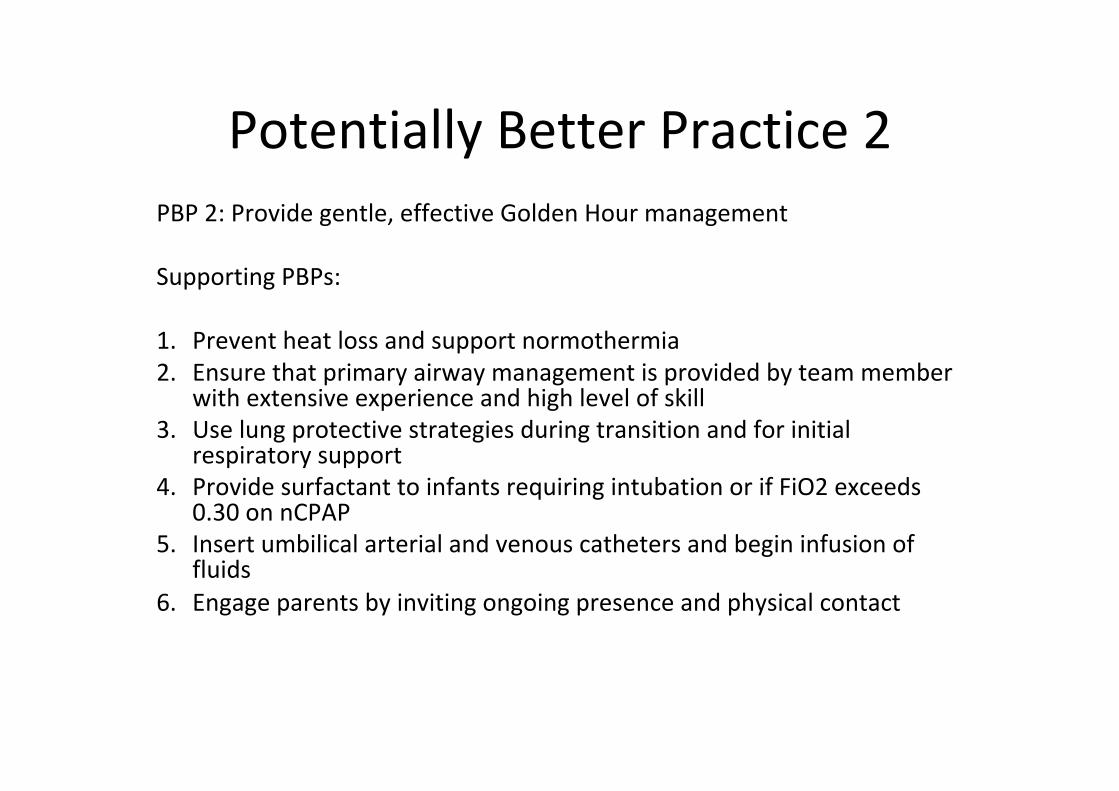
PotentiallyBetterPractice2PBP2:Providegentle,effectiveGoldenHourmanagementSupportingPBPs:1. Preventheatlossandsupportnormothermia2. Ensurethatprimaryairwaymanagementisprovidedbyteammember
withextensiveexperienceandhighlevelofskill3. Uselungprotectivestrategiesduringtransitionandforinitial
respiratorysupport4. ProvidesurfactanttoinfantsrequiringintubationorifFiO2exceeds
0.30onnCPAP5. Insertumbilicalarterialandvenouscathetersandbegininfusionof
fluids6. Engageparentsbyinvitingongoingpresenceandphysicalcontact
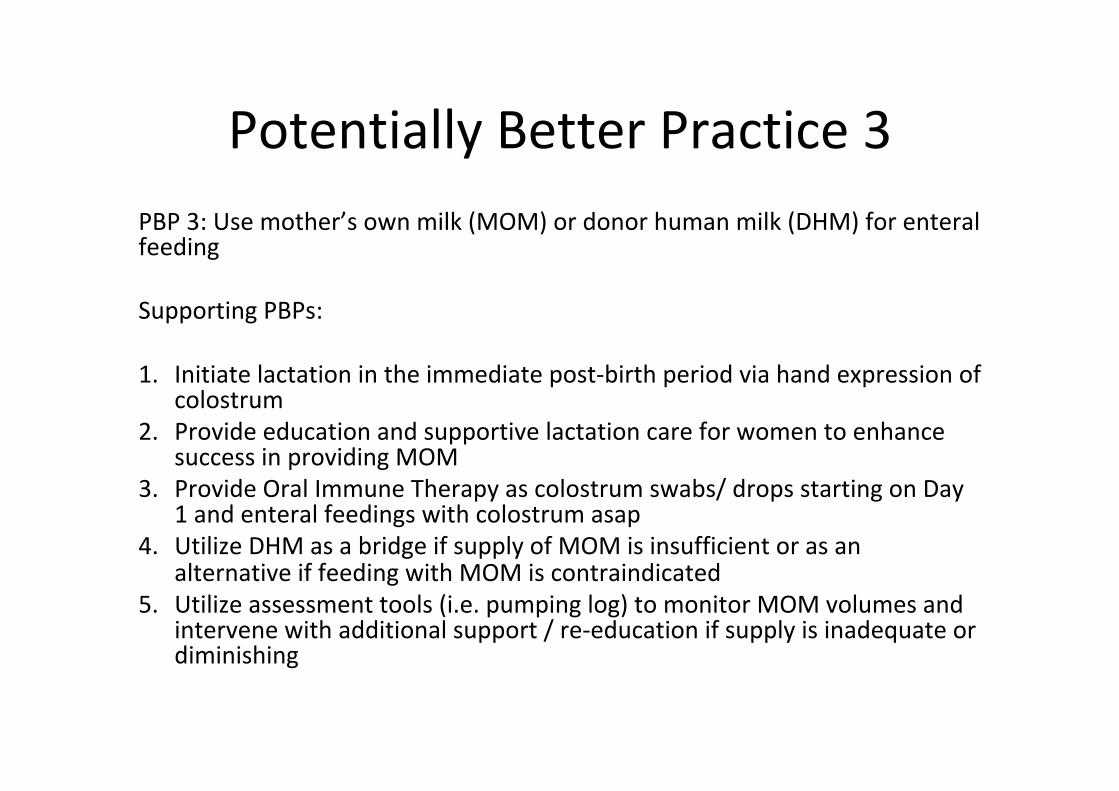
PotentiallyBetterPractice3PBP3:Usemother’sownmilk(MOM)ordonorhumanmilk(DHM)forenteralfeeding
SupportingPBPs:1. Initiatelactationintheimmediatepost-birthperiodviahandexpressionof
colostrum2. Provideeducationandsupportivelactationcareforwomentoenhance
successinprovidingMOM3. ProvideOralImmuneTherapyascolostrumswabs/dropsstartingonDay
1andenteralfeedingswithcolostrumasap4. UtilizeDHMasabridgeifsupplyofMOMisinsufficientorasan
alternativeiffeedingwithMOMiscontraindicated5. Utilizeassessmenttools(i.e.pumpinglog)tomonitorMOMvolumesand
intervenewithadditionalsupport/re-educationifsupplyisinadequateordiminishing
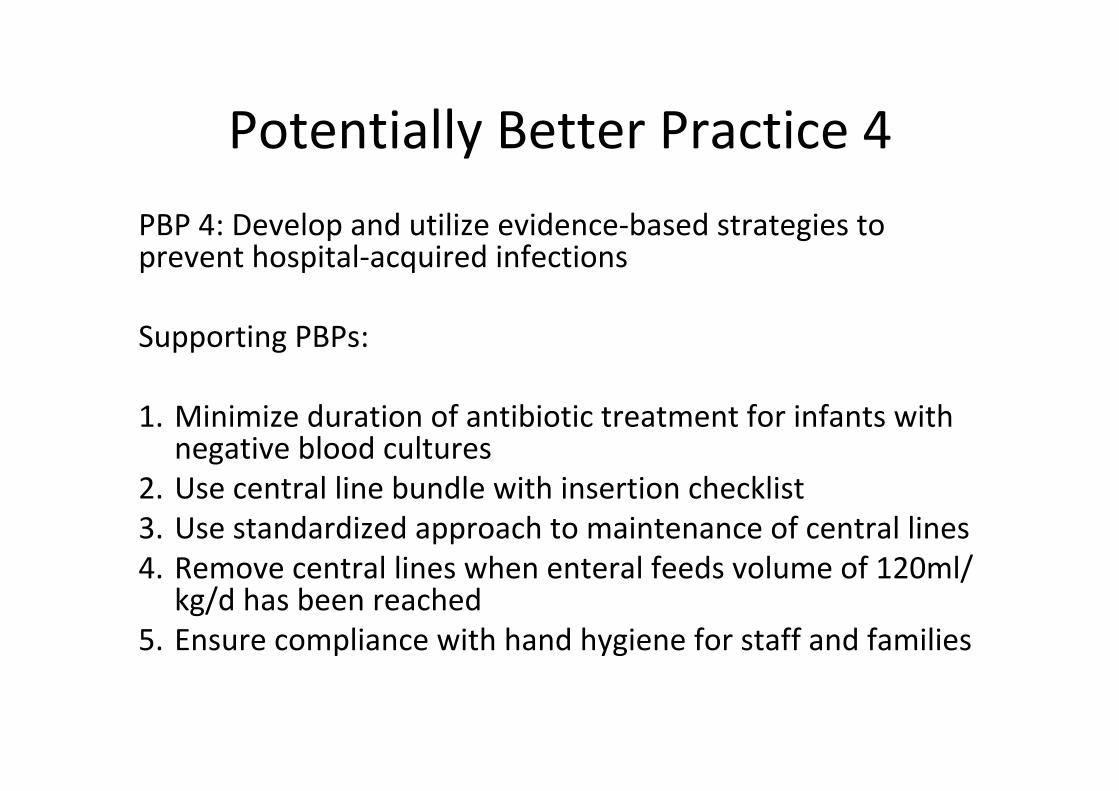
PotentiallyBetterPractice4PBP4:Developandutilizeevidence-basedstrategiestopreventhospital-acquiredinfections
SupportingPBPs:
1. Minimizedurationofantibiotictreatmentforinfantswithnegativebloodcultures
2. Usecentrallinebundlewithinsertionchecklist3. Usestandardizedapproachtomaintenanceofcentrallines4. Removecentrallineswhenenteralfeedsvolumeof120ml/
kg/dhasbeenreached5. Ensurecompliancewithhandhygieneforstaffandfamilies
PotentiallyBetterPractice5PBP5:Ensuremaximalcompliancewithevidence-basedoxygensaturationtargets
SupportingPBPs:
1. Determineanddisseminateguidelinesforsaturationtargets,alarmlimitsandrequiredresponses
2. Educatefamiliesaboutoxygentherapy,monitorsandalarms.Engagetheminfacilitatingappropriateresponsestoalarms
3. Ensurethatallmonitorshavealarmsettingsincompliancewithguidelines4. Developgoalsforthepercentageoftimeindividualpatientsareachieving
O2saturationtargets.Regularlyassesscompliancewhileprovidingfeedbacktostaffusingmethodssuchasreviewofmonitor-generatedhistogramsanddiscussstrategiestoimprovepracticeandoutcomes

PotentiallyBetterPractice6PBP6:Utilizelung-protectivestrategieswhenprovidingrespiratorysupport
SupportingPBPs:
1. InitiaterespiratorysupportwithnCPAPinDRwheneverpossible2. Allowmodestpermissivehypercapniaduringnon-invasiveor
invasivesupport3. UseHFOVorvolume-targetedmethodsifinvasiveventilationis
required4. Avoidatelectraumabyutilizinganopenlungapproach5. Treatwithcaffeinesoonafterbirth6. Extubateassoonaspossible

PotentiallyBetterPractice7PBP7:Promoteandreinforceencounterswiththeinfantthataredevelopmentallysupportiveandpositive
SupportivePBPs:
1. Reducepainfultissue-damagingprocedurestoaminimumforsafecare2. Minimizestressfulprocedures(definedasanyhandlingthatisnotforthe
purposeofnurturing)3. Whenpainfulorstressfulproceduresarenecessary,utilizestrategiesthat
supporttheinfantincludingcontainment,two-personhandlingandpositiveinputs
4. Makeskin-to-skinwiththeparentthepreferredlocusofcarefortheinfant
5. Educateparentsindevelopmentallysupportivemethods

PotentiallyBetterPractice8PBP8:Ensurefamilyintegrationincaretoimproveoutcome,buildconfidenceandpromoteattachment
SupportingPBPs:1. WELCOME:Ensureeveryfamilyreceivestimelyandcompleteorientationtothe
unitandhospital2. LEARN:Ensurethateachfamilyhasbeeninterviewedwithintakequestionnaire3. TEACH:Createeducationalandsupportiveprogrammingforfamilies4. ENGAGE:Includefamilyonroundsasactiveparticipantsandenableaccesstothe
medicalteam,particularlybeforekeytransitionalmomentsforthebabyand/orfamily.Whenfamiliesarepresent,ensuretheyaresupportedandencouragedtoprovidecareandarethesecondsetofhandssupportingthebabyduringprocedures
5. PREPARE:Provideon-goingindividualizedcommunicationabouttheinfant’sNICUstayandplanofcareemphasizingconsistencyofinformation(independentofdeliverymechanism)andincludinganticipatoryguidance
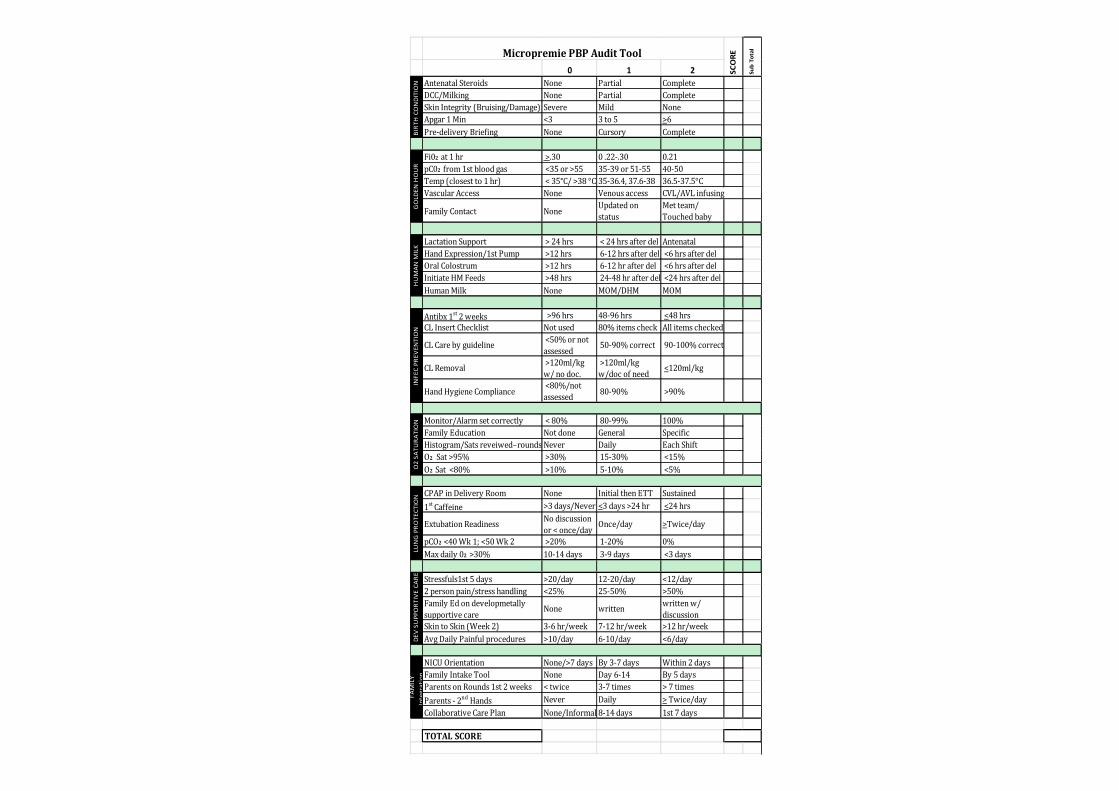
0 1 2AntenatalSteroids None Partial CompleteDCC/Milking None Partial CompleteSkinIntegrity(Bruising/Damage) Severe Mild NoneApgar1Min <3 3to5 >6Pre-deliveryBriefing None Cursory Complete
Fi02 at1hr >.30 0.22-.30 0.21pC02 from1stbloodgas <35or>55 35-39or51-55 40-50Temp(closestto1hr) <35°C/>38°C 35-36.4,37.6-38 36.5-37.5°CVascularAccess None Venousaccess CVL/AVLinfusing
FamilyContact None Updatedonstatus
Metteam/Touchedbaby
LactationSupport >24hrs <24hrsafterdel AntenatalHandExpression/1stPump >12hrs 6-12hrsafterdel <6hrsafterdelOralColostrum >12hrs 6-12hrafterdel <6hrsafterdelInitiateHMFeeds >48hrs 24-48hrafterdel <24hrsafterdelHumanMilk None MOM/DHM MOM
Antibx1st2weeks >96hrs 48-96hrs <48hrsCLInsertChecklist Notused 80%itemscheck Allitemschecked
CLCarebyguideline <50%ornotassessed 50-90%correct 90-100%correct
CLRemoval >120ml/kgw/nodoc.
>120ml/kgw/docofneed <120ml/kg
HandHygieneCompliance <80%/notassessed 80-90% >90%
Monitor/Alarmsetcorrectly <80% 80-99% 100%FamilyEducation Notdone General SpecificHistogram/Satsreveiwed–rounds Never Daily EachShiftO2 Sat>95% >30% 15-30% <15%O2 Sat<80% >10% 5-10% <5%
CPAPinDeliveryRoom None InitialthenETT Sustained1stCaffeine >3days/Never <3days>24hr <24hrs
ExtubationReadiness Nodiscussionor<once/day Once/day >Twice/day
pCO2 <40Wk1;<50Wk2 >20% 1-20% 0%Maxdaily02>30% 10-14days 3-9days <3days
Stressfuls1st5days >20/day 12-20/day <12/day2personpain/stresshandling <25% 25-50% >50%FamilyEdondevelopmetallysupportivecare
None written writtenw/discussion
SkintoSkin(Week2) 3-6hr/week 7-12hr/week >12hr/weekAvgDailyPainfulprocedures >10/day 6-10/day <6/day
NICUOrientation None/>7days By3-7days Within2daysFamilyIntakeTool None Day6-14 By5daysParentsonRounds1st2weeks <twice 3-7times >7timesParents-2ndHands Never Daily >Twice/dayCollaborativeCarePlan None/Informal 8-14days 1st7days
TOTALSCORE
DEV
SUPPORT
IVECA
REFA
MILY
Integration
LUNGPRO
TECTION
INFECPR
EVEN
TION
O2SA
TURA
TION
SCORE
SubTotal
BIRT
HCONDITION
GOLDEN
HOUR
HUMAN
MILK
MicropremiePBPAuditTool
Preventingmorbidity
ImpactofBronchopulmonaryDysplasia,BrainInjury,andSevereRetinopathyontheOutcomeof
ExtremelyLow-Birth-WeightInfantsat18MonthsResultsfromtheTrialofIndomethacinProphylaxisinPretermsSchmidtetal,JAMA2003• 910infants,birthweight500-999g• 32NICU’sUS,Canada,Australia,NewZealandandHongKong• Survivedto36weeksPMA
• ROP,BPDandbraininjuryeachsimilarly&independentlycorrelatedtopoor18mooutcome
• NoROP,BPDorbraininjury–rateofpoorlongtermoutcome18%
• With1,2or3ofmorbidities–correspondingrates42%,62%and88%

• Additionalroleofinfectionornecrotizingenterocolitis,butsmalleroddsratiothanBPD,ROPorbraininjury
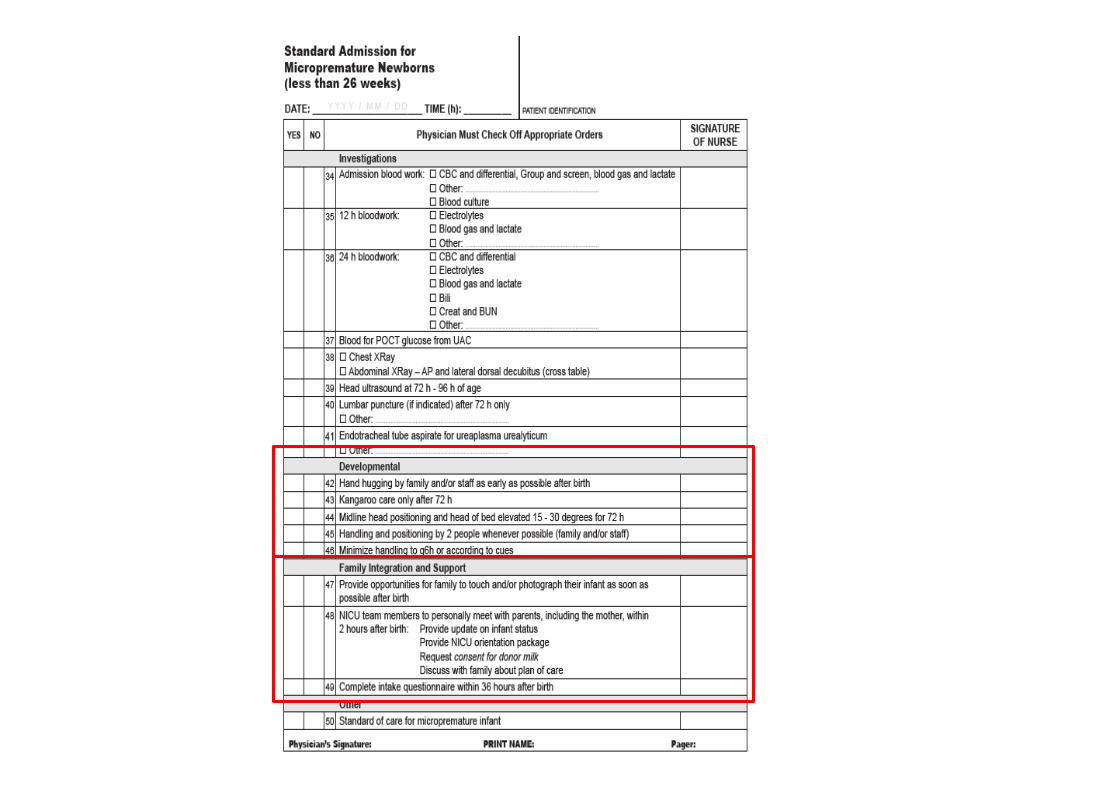
Neuroprotectionbundle
• Handhuggingbyfamilyand/orstaffasearlyaspossibleafterbirth
• Kangaroocareonlyafter72hrs• Midlineheadpositioningandheadelevation15-30
degreesfor72hrs• Handlingandpositioningby2peoplewhenever
possible(familyand/orstaff)• Minimizehandlingtoq6horaccordingtocues
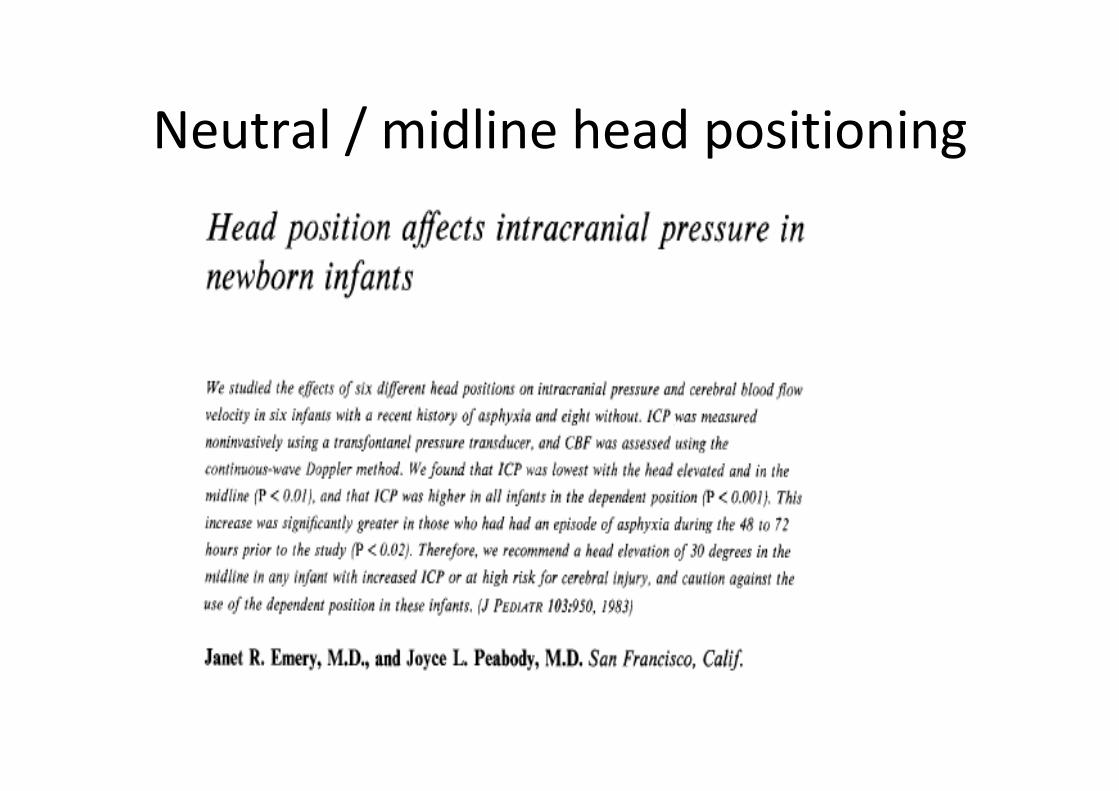
Neutral/midlineheadpositioning


20.4%20.9%
14.0%
6.5%
13.6%
10.7%
0%
5%
10%
15%
20%
25%
AllMicroprems InbornMicroprems
SevereIVHRate
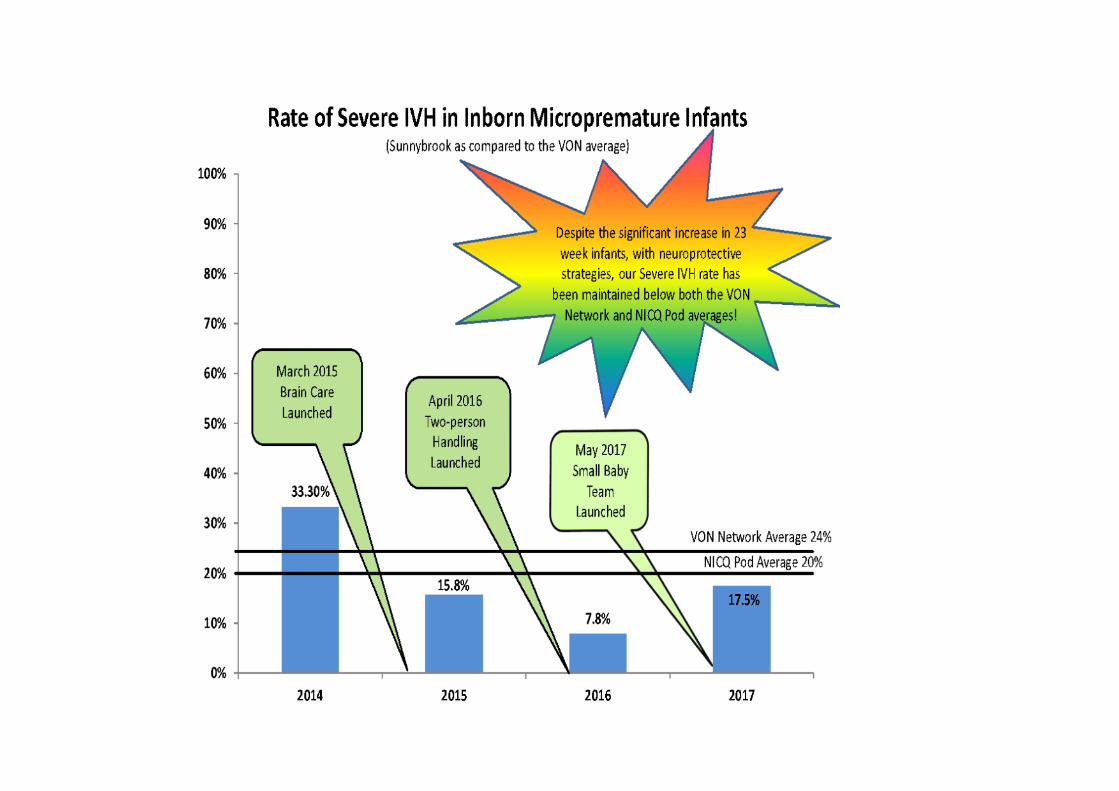
SevereIVHRateinMicropremature Infants
BeforeBrainCareLaunch
AfterLaunch:First10months
Afterlaunch:40months
Includingfamiliesinpatientcare
EffectivenessofFamilyIntegratedCareinneonatalintensivecareunitsoninfantandparentoutcomes:amulticentre,multinational,cluster-randomisedcontrolledtrialKarelO'Brien,KateRobson,MarianneBracht,MelindaCruz,KeiLui,RubenAlvaro,OrlandodaSilva,LuisMonterrosa,MichaelNarvey,EugeneNg,AmuchouSoraisham,XiangYYe,LuciaMirea,WilliamTarnow-Mordi,ShooKLeeTheLancetchild&adolescenthealth2018,2(4):245-254
• 26tertiaryNICUsfromCanada,Australia,andNewZealand• FICareorstandardNICUcare• Eligibleinfantswerebornat33weeks'gestationorearlier,and
hadnoorlow-levelrespiratorysupport• ParentsintheFICaregrouphadtocommittobepresentforat
least6haday,attendeducationalsessions,andactivelycarefortheirinfant
• Theprimaryoutcome:infantweightgainatday21afterenrolment
• Secondaryoutcomes:weightgainvelocity,highfrequencybreastfeeding(≥6timesaday)athospitaldischarge,parentalstressandanxietyatenrolmentandday21,NICUmortalityandmajorneonatalmorbidities,safety,andresourceuse(includingdurationofoxygentherapyandhospitalstay)
Findings• RandomlyassignedtoprovideFICare(n=14)orstandardcare
(n=12)• 895infantseligibleinFICaregroupvs891instandardcaregroup• Day21weightgaingreaterinFICaregroupthaninthestandard
caregroup(meanchangeinZscores-0·071[SD0·42]vs-0·155[0·42];p<0·0002)
• AveragedailyweightgainsignificantlyhigherininfantsreceivingFICare(meandailyweightgain26·7g[SD9·4]vs24·8g[9·5];p<0·0001)
• Thehigh-frequencyexclusivebreastmilkfeedingrateatdischargewashigherforinfantsintheFICaregroup(279[70%]of396vs394[63%]of624;p=0·016)
• ParentsintheFICaregrouphadlowermeanstressscores(2·3[SD0·8]vs2·5[0·8];p<0·00043),andlowermeananxietyscores(70·8[20·1]vs74·2[19·9];p=0·0045)
• Nosignificantdifferencesbetweengroupsinratesofthesecondaryoutcomesofmortality,majormorbidity,durationofoxygentherapy,anddurationofhospitalstay

‘SSCisaneffectiveandevidence-basedcarestrategythatreducestheinfant’straumaticNICUexperiencesbyimprovingparentalproximity,
attachment,andlactation;decreasingstressandpain;improvingphysiologicstability;supportingsleep;andenhancingneurologicoutcomes.’
Includefamiliesindevelopmentalcare

LessonsfromNIDCAPNIDCAPapproachbasedon3assumptions:• Detailedobservationofbehaviorprovidesbasisforrecommendationsinhowtominimizestressandoptimizedevelopment
• Caregiversbenefitfromsupportiveeducation,aswellasguidanceandmodelinginimplementingrecommendations
• Resultantchangesleadtoimprovedmedicalandneurobehavioralfunctioning
AlsH.NewbornIndividualizedDevelopmentandAssessmentProgram(NIDCAP):Newfrontierforneonatalandperinatalmedicine.JNeoPerinatalMed2009;2:135-149.

Whataboutfeeding?
Whydofeedingproblemsoccur?
• Earlysensoryinformationmayhaveaneffectonthearchitectureofthebrain(Sweeney,2010,Shaker,2013)– Structurally(braininjury,reducedcorticalandcerebellarvolumes)– Functionally-“wiring”
• Combinationofphysiologicinstabilitycoupledwith(toxic)stress,imposedonasensorysystemthatisundergoingrapiddevelopment:– Maycausealteredsensorymotorpathwaysinthebrain– Maybeariskfactorforneurobehavioralanddevelopmentaldysfunctionlater
inlife– MayaffecttheabilityanddesiretoeatbothintheNICUandafterdischarge
(Ross,2009)

Evenafterdischarge
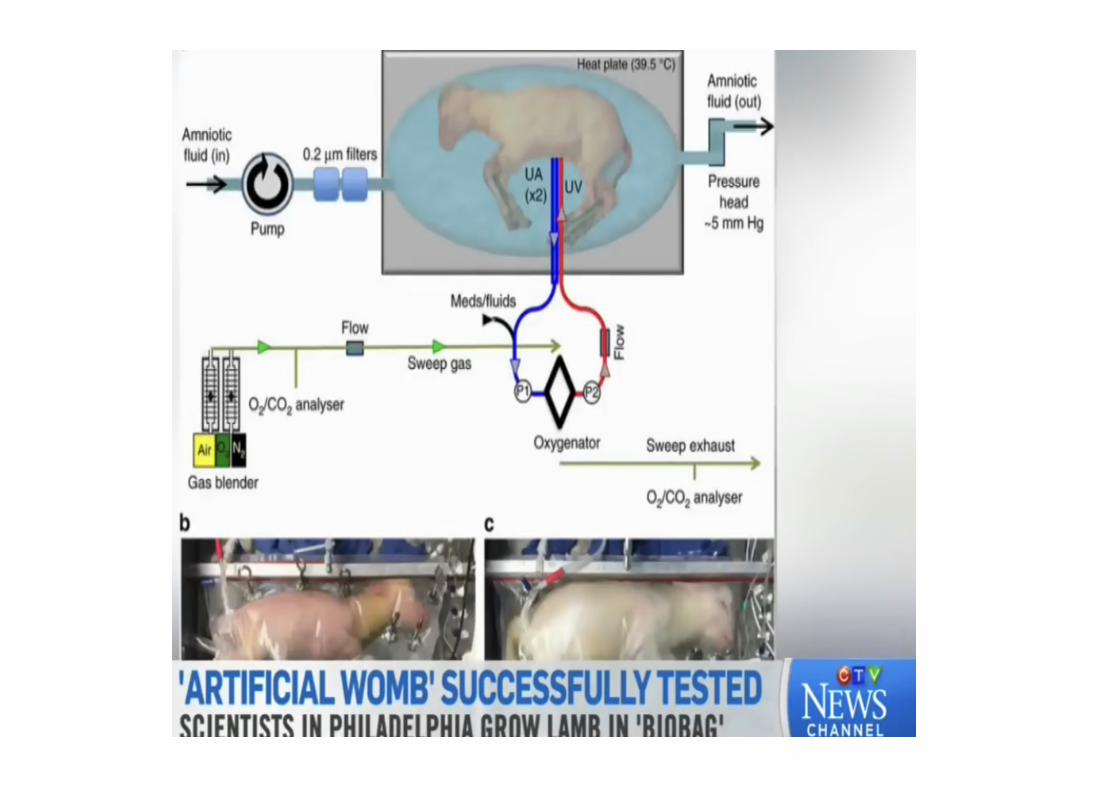
Whatisnext?
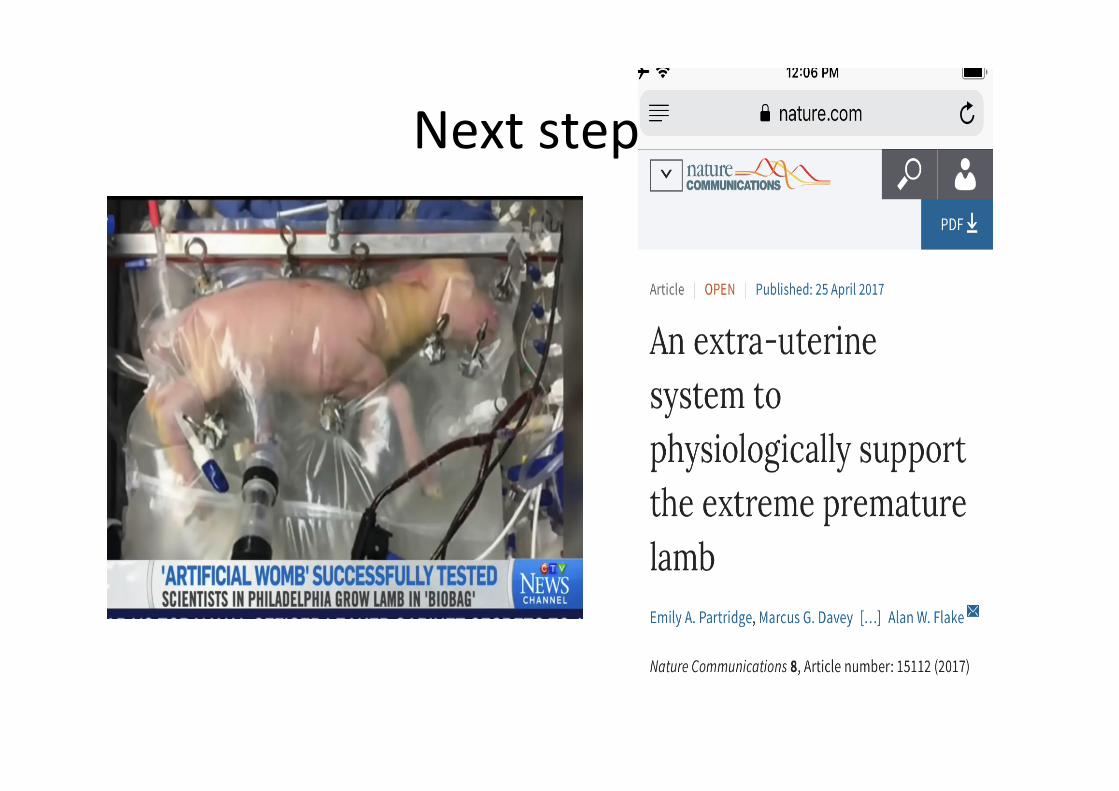
Nextstep…?

Resources• Tysonneonatalmortality/
morbiditycalculator(infants<26weeks)https://www1.nichd.nih.gov/epbo-calculator/Pages/epbo_case.aspx
• VermontOxfordNetworkwebpagehttps://public.vtoxford.org/
• Cochranelibraryhttps://www.cochranelibrary.com/