cva stroke dr. aidah abu elsoud alkaissi an-najah national university faculty of nursing
TRANSCRIPT



CVAStroke
Dr. Aidah Abu Elsoud Alkaissi
An-Najah National University
Faculty of Nursing



• RECOGNIZING A STROKE
• Sometimes symptoms of a stroke are difficult to identify.
• Unfortunately, the lack of awareness spells disaster.
• The stroke victim may suffer severe brain damage when people nearby fail to recognize the symptoms of a stroke.
• a bystander can recognize a stroke by asking three simple questions:
• S *Ask the individual to SMILE.
• T *Ask the person to TALK . to SPEAK A SIMPLE SENTENCE (Coherently) (i.e. . . It is sunny out today)
• R *Ask him or her to RAISE BOTH ARMS. • {NOTE: Another 'sign' of a stroke is this: Ask the person to 'stick'
out their tongue... if the tongue is 'crooked', if it goes to one side or the other that is also an indication of a stroke}
• If he or she has trouble with ANY ONE of these tasks, call 9-1-1 immediately and describe the symptoms
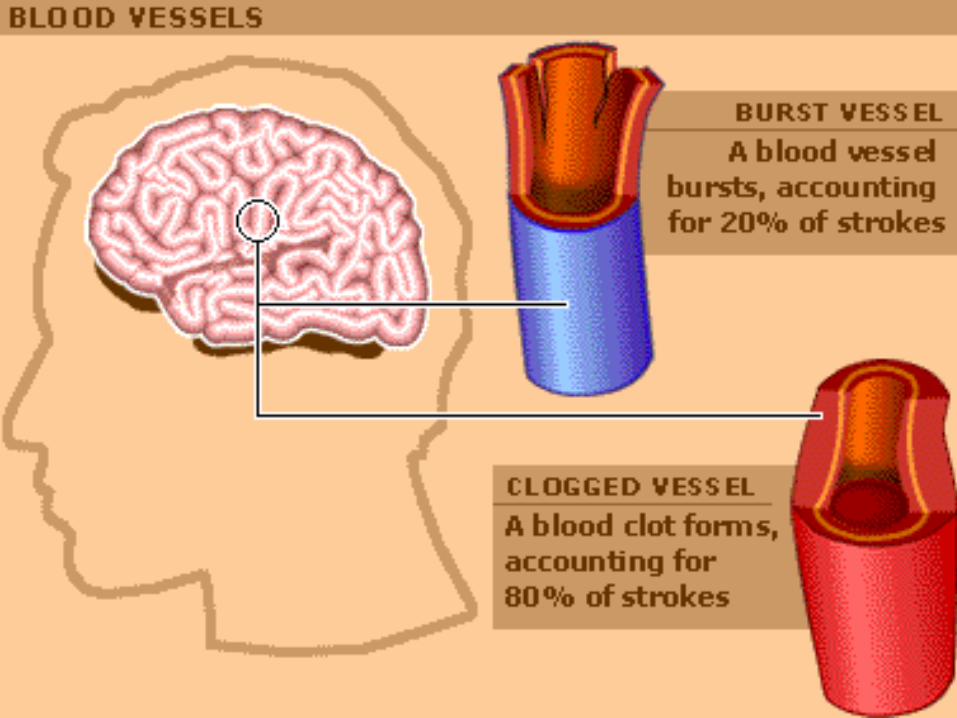

• STROKEThere are two types of stroke - those caused by blood clots in the brain and those that occur when blood vessels burst.
• In both cases, the brain is starved of oxygen, damaging or killing cells.
• Sufferers are often left with difficulty talking, walking and performing other basic tasks.
• The chance of suffering a stroke is cut by eating healthily, quitting smoking and drinking less alcohol.
• People at risk of stroke are often treated with aspirin.
• After a stroke, various drug treatments are available and rehabilitation is commonly used to improve patients' speech and movement.
• Stroke• Over the last several years, advances have
been made in the treatment of stroke.
• Early recognition and prompt entry into the emergency medical system are essential to reduce death and disability from stroke.
• Media campaigns have been launched to increase public awareness about the signs and symptoms of stroke so that care may be sought promptly.

• A stroke is now referred to as a “brain attack” to encourage health care professionals and the public to think about stroke with the same urgency as a “heart attack.
• ” A “brain attack” must be viewed as a medical emergency.
• To reverse cerebral ischemia, patients must be evaluated promptly.
• Ischemic brain injury occurs when arterial occlusion lasts longer than 2 to 3 hours.

• Delay in seeking medical care may eliminate the potential for tissue-saving therapy with thrombolytic agents.
• According to the National Stroke Association, stroke is one of the leading causes of permanent disability in adults.
• Of long-term stroke survivors, 15% require institutional care, 30% are dependent in activities of daily living, and 60% have decreased socialization outside the home.
• The American Heart Association estimates that 15 to 20 billion dollars are spent annually on stroke and stroke-related disorders.

• A stroke may be defined as a neurological deficit that has a sudden onset, lasts more than 24 hours, and results from cerebrovascular disease.
• A stroke occurs when there is a disruption of blood flow to a region of the brain.
• Blood flow is disrupted because of an obstruction of a vessel, on account of a thrombus or embolus, or the rupture of a vessel.
• The clinical features seen depend on the location of the event and region of the brain the vessel perfused.

• ETIOLOGY• Approximately three-fourths of strokes
are due to vascular obstruction (thrombi or emboli), resulting in ischemia and infarction.
• About one-fourth of strokes are hemorrhagic, resulting from hypertensive vascular disease (which causes an intracerebral hemorrhage), a ruptured aneurysm, or an arteriovenous malformation
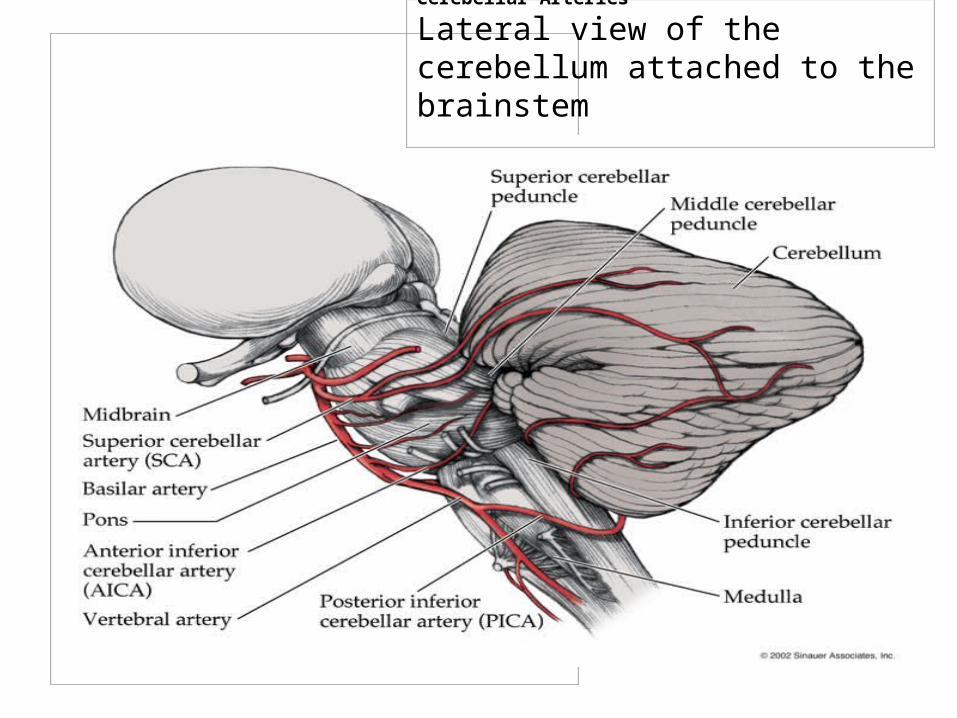
Cerebellar Arteries
Lateral view of the cerebellum attached to the brainstem



• EPIDEMIOLOGY• Approximately 750,000 strokes occur every
year in the United States.
• The incidence in men is greater than in women. It is estimated that there are 3 million stroke survivors and that stroke is a leading cause of disability and a leading diagnosis for long-term care.
• Risk factors for stroke include smoking, hypertension, obesity, cardiac disease, hypercholesterolemia, diabetes, and use of birth control pills.

• Prevention efforts focus on lifestyle changes that can modify risk factors.
• In addition, the appropriate use of warfarin or aspirin in patients at risk for cardiac sources of emboli (e.g., atrial fibrillation) constitutes primary prevention.

• PATHOPHYSIOLOGY• When blood flow to any part of the brain is
impeded as a result of a thrombus or embolus, oxygen deprivation of the cerebral tissue begins.
• Deprivation for 1 minute can lead to reversible symptoms, such as loss of consciousness.
• Oxygen deprivation for longer periods can produce microscopic necrosis of the neurons.
• The necrotic area is then said to be infarcted.
• The initial oxygen deprivation may be caused by general ischemia (from cardiac arrest or hypotension) or hypoxia from an anemic process or high altitude (elevation especially above sea level or above the earth's surface)
• If the neurons are ischemic only and have not
yet necrosed, there is a chance to save them.
• This situation is analogous (similar or equivalent in some respects ) to the focal injury caused by a myocardial infarction.

• An occluded coronary artery can produce an area of infarcted (dead) tissue.
• Surrounding the infarcted zone is an area of ischemic tissue, which has been marginally deprived of oxygen.

• This ischemic tissue, as in the brain, may either be salvaged (rescue) with appropriate treatment or killed by secondary events.
• Cerebral ischemia is a complex process that depends on the severity and duration of the decline in cerebral blood flow.
• The ischemic cascade begins within seconds to minutes after perfusion failure, creating a zone of irreversible infarction and surrounding area of potentially salvageable “ischemic penumbra.” (partial shadow: a partial outer shadow that is lighter than the darker inner shadow umbra, e.g. the area between complete darkness and complete light in an eclipse)
• The goal of acute stroke management is to salvage the ischemic penumbra, or the territory at risk.
• Without prompt intervention, the entire ischemic penumbra can eventually become an infarcted region.

• A stroke caused by an embolus may be a result of blood clots, fragments of atheromatous plaques, lipids, or air.
• Emboli to the brain most often have a cardiac source, secondary to myocardial infarction or atrial fibrillation.
• If hemorrhage is the etiology of a stroke, hypertension often is a precipitating factor.
• Vascular abnormalities, such as arteriovenous malformations and cerebral aneurysms, are more prone to rupture and cause hemorrhage in the presence of hypertension.

• The most frequent neurovascular syndrome seen in thrombotic and embolic strokes is due to involvement of the middle cerebral artery.
• This artery mainly supplies the lateral aspects of the cerebral hemisphere.
• Infarction to that area of the brain can cause contralateral (oppositely positioned in body: describes a body part that is on the opposite side of the body, or that acts in conjunction with such a part) motor and sensory deficits.
• If the infarcted hemisphere is dominant, speech problems result, and dysphasia may be present.

• It is difficult to predict the amount of brain ischemia and infarction resulting from a thrombotic or embolic stroke.
• There is a possibility that the stroke will extend after the initial insult.
• There can be massive cerebral edema and an increase in ICP to the point of herniation and death after a huge thrombotic stroke.
• The area of the brain involved and the extent of the insult influence the prognosis.
• Because thrombotic strokes often are caused by atherosclerosis, there is risk of a future stroke in a patient who already has had one.

• With embolic strokes, patients also may have subsequent episodes of stroke if the underlying cause is not treated.
• If the extent of brain tissue destroyed from hemorrhagic stroke is not excessive and is in a nonvital area, the patient may recover with minimal deficits.
• If the hemorrhage is large or in a vital area of the brain, the patient may not recover; however, if the intracerebral hemorrhage is less massive, survival is possible.

• CLINICAL MANIFESTATIONS• A stroke is usually characterized by the sudden
onset of focal neurological impairment.
• The patient may experiencesigns such as weakness, numbness, visual changes, dysarthria, dysphagia, or aphasia.
• The manifestations of a stroke depend on the anatomical location of the lesion.
• Table 35-8 presents the correlation of blood supply to symptomatology in a brain attack.

• Globus pallidus - Wikipedia, the free encyclopediaThe globus pallidus ( Latin for "pale globe") is a sub- cortical structure of the brain . It is a major element of the basal ganglia system. In this system, it is a major element ... globus pallidusA structure in the brain involved in the regulation of voluntary movements at a subconscious level. The globus pallidus is one of three nuclei that make up the basal ganglia, the ...

• Lateral geniculate nucleus - Wikipedia, the free encyclopedia The lateral geniculate nucleus ( LGN ) of the thalamus is a part of the brain , which is the primary processor of visual information, received from the retina , in the central ...

• at the Centre for Cancer Education, University of ... hemihypesthesia: Definition and Much More from Answers.comhemihypesthesia n. Diminished sensibility on one side of the body.
• homonymous hemianopia- vision impairment: the loss of the outer half of the field of vision of one eye and the inner half of the field of the other eye

• mononuclear- with single nucleus: describes a cell that has a single nucleus- with one ring of atoms: describes an organic compound with a molecular structure containing only one ring of atoms

• The caudate nucleus is a nucleus located within the basal ganglia of the brains of many animal species. The caudate, originally thought to primarily be involved with control of voluntary movement, is now known to be an important part of the brain's learning and memory system.

• Abulic symptoms: Multi-infarct dementia
• Apraxia• Definition• Apraxia is a neurological disorder In general, the
diagnostic term "apraxia" can be used to classify the inability of a person to perform voluntary and skillful movements of one or more body part

• Spatial Neglect - Spatial neglect is a behavioral syndrome occurring after brain injury. Spatial neglect involves the inability to report, respond, or orient to stimuli, generall...

• Homonymous hemianopsia is a medical term for a type of partial blindness
• ipsilateral- of same side of body: being on or affecting the same side of the body

• HemianopsiaHEMIANOPSIA. DESCRIPTION: Literally, "half vision;" a condition resulting from malfunction or damage to one side of the optic tract
• quadrant anopia , refers to an anopia affecting a quarter of the field of vision. It can be associated with a lesion of an optic radiation . If ...

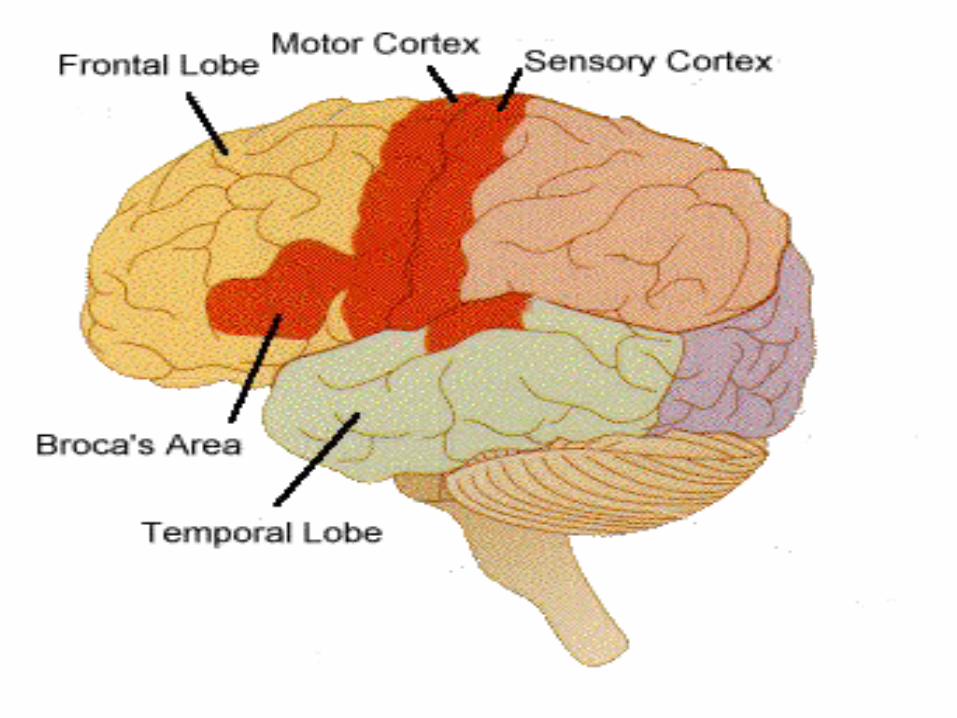
• Wernicke’s Aphasia description, neurologist for whom disease is namedWernicke, Carl: Wernicke’s AphasiaDamage to Broca's area in the frontal lobe causes difficulty in speaking and writing a problem known as Broca's aphasia Injury to Wernicke's area.Aphasia : types of aphasia : Wernicke’s aphasia: Wernicke, CarlWernicke, Carl (1848–1905), German neurologist and psychiatrist. He is known for his study of aphasia (defects of expression or comprehension...

• clumsiness- moving awkwardly: poorly coordinated physically- said or done awkwardly
• Horner syndrome is rare condition caused by injury to the sympathetic nerves of the face. It involves a collection of symptoms, including:
• Sinking of the eyeball into the face • Small (constricted) pupil • Drooping eyelid (ptosis)• Lack of face sweating

• pseudobulbar paralysis spastic weakness of the muscles innervated by the cranial nerves, i.e., the facial muscles, pharynx, and tongue, due to bilateral lesions

• If symptoms resolve in less than 24 hours, the event is classified as a transient ischemic attack (TIA).
• Most TIAs last for only minutes to less than an hour, which further clouds recognition and prompt treatment.
• the differential diagnosis of stroke includes ruling out intracerebral hemorrhage, SAH, subdural or epidural hematoma, neoplasm, seizure, or migraine headache.
• DIAGNOSIS• Rapid diagnosis of a stroke is
essential so that appropriate patients can receive thrombolytic therapy, the goal of which is to save damaged brain tissue and minimize permanent deficits.
• The patient should be taken to an emergency department where a neurologist can perform an initial screening and obtain appropriate neuroimaging studies.
• The time of symptom onset to administration of thrombolytic therapy (or “time to needle”) should be within a 3-hour window.
• Emergency departments need to have services streamlined so that testing may be performed and treatment initiated promptly.

• streamlined- make something more efficient: to make something such as a business, organization, or manufacturing process more efficient, especially by simplifying or modernizing it

• The patient’s history helps determine what has happened to the individual.
• It is important to obtain a description of the neurological event; how long it lasted; and whether the symptoms are resolving, completely gone, or the same as at the time of onset.
• Identifying the type of symptoms can help determine and locate a possible vascular etiology.
• Determination of risk factors for stroke, such as hypertension, chronic atrial fibrillation, elevated serum cholesterol, smoking, oral contraceptive use, or a familial history of stroke, also aids in diagnosis.
• In the emergency department, some of the tests that are frequently used to evaluate the patient with acute ischemic stroke are a CT scan of the brain without contrast, blood studies, neurological examination, and a screen performed using the National Institutes of Health Stroke Scale (NIHSS).
• This tool allows a score to be given for the severity of the stroke. Table 35-9 summarizes the NIHSS.

• gaze intr.v. , gazed , gazing , gazes . To look steadily, intently, and with fixed
• ataxia- lack of muscle control: the inability to coordinate the movements of muscles
• There is no definitive laboratory study that will determine if a patient has experienced a stroke.
• Rather, the studies are viewed in conjunction with the history, neurological examination, and results of neuroimaging studies.
• Laboratory studies, including complete blood cell count, electrolytes, glucose, and coagulation parameters, are obtained.
• An emergent CT scan should be performed to rule out intracerebral hemorrhage.
• Ideally, the CT scan is obtained within 60 minutes of arrival in the emergency department so that treatment decisions can be made.
• A CT scan can be useful in differentiating between cerebrovascular and nonvascular lesions.
• For example, a subdural hemorrhage, brain abscess, tumor, SAH, or intracerebral hemorrhage is visible on the CT scan. However, an area of infarction may not show on the CT scan for 48 hours.
• Newer neuroimaging techniques also provide valuable information.
• T1- and T2-weighted, fluid-attenuated inversion recovery (FLAIR), diffusion-weighted, and perfusionweighted
• Diffusion-weighted MRI (DWI) is highly sensitive to early cerebral ischemia, but its dependence on lesion location, acuity, and etiology remains unknown. Furthermore,
although a marked perfusion-weighted MRI (PWI)-DWI mismatch may exist in a subset of acute strokes.

• MRI techniques have become widely available and are better at detecting infarction than a CT scan.
• The earliest changes normally appear within the first 24 hours. Using FLAIR, images can be manipulated so that only abnormal areas are hyperintense.

• The interrelationship of changes in T1, T2 and diffusion weighted images of tissue water were studied in mouse models of permanent and transient focal cerebral ischemia.
• A sham surgery or either permanent or transient (30 min) middle cerebral artery occlusion (MCAO) were induced in 14 mice. Magnetic resonance (MR) images of the brain were acquired including: T2 maps, T1 maps and diffusion weighted spin-echo images to produce apparent diffusion coefficient of water apparent diffusion coefficient (ADC) maps. I
• Another study that may be performed, based on availability of the technology, is diffusion-weighted imaging (DWI) and perfusion-weighted imaging (PWI).
• This technique helps identify the infarct core and penumbra, which is important because the presence of viable tissue directs interventions such as reperfusion.

• The ischemic penumbra surrounds the infarcted tissue
• It is the marginally perfused area of the brain that has been damaged by the insult but is potentially salvageable.
• DWI detects acute infarction as early as a few hours after the onset of symptoms.
• It can reveal changes in infarcted tissue hours before a CT scan or MRI can detect any abnormality.
• It also discriminates acute from chronic ischemic changes. PWI looks at the region of cerebral blood flow.

• The difference between the diffusion defect and the perfusion defect represents the ischemic penumbra, or the “territory at risk.”
• DWI-PWI identifies patients who are ideal candidates for thrombolytic therapy.

• Cerebral angiography has been the gold standard for evaluating cerebral vasculature.
• There is an estimated 1.5% to 2% associated risk of morbidity or mortality with this procedure.
• It can, however, demonstrate an arterial occlusion or embolus.
• Because of the time that it takes to perform cerebral angiography, the window of opportunity to treat a patient with thrombolytics may be missed.
• The vasculature can be evaluated noninvasively by the use of TCD (Transcranial Doppler Monitoring , ultrasonography, MRA

• Cerebral angiography is a form of angiography which provides images of blood vessels in and around the brain, thereby allowing detection of abnormalities such as arteriovenous malformations and aneurysms.
• Typically a catheter is inserted into a large artery (such as the femoral artery) and threaded through the circulatory system to the carotid artery, where a contrast agent is injected. A series of radiographs is taken as the contrast agent spreads through the brain's arterial system, then a second series as it reaches the venous system.
• For some applications[citation needed] this method may yield better images than less invasive methods such as computed tomography angiography and magnetic resonance angiography. In addition, cerebral angiography allows certain treatments to be performed immediately, based on the its findings. If, for example, the images reveal an aneurysm, metal coils may be introduced through the catheter already in place and maneuvered to the site of aneurysm; over time these coils encourage formation of connective tissue at the site, strengthening the vessel walls.

• Transcranial Doppler Monitoring and the Causes of Stroke from
Carotid Endarterectomy• Merrill P. Spencer, M.D.
Sound Vascular Monitoring and The Institute of Applied Physiology and Medicine
Seattle, Washington, USA• Abstract
• Background and Purpose: The value of carotid endarterectomy (CEA) depends on the safety of the operation. Transcranial Doppler (TCD) was used to evaluate the possibilities of hypoperfusion, hyperperfusion, and embolization as causes of stroke and evaluated the significance of Doppler microembolic signals (DMES).
• Also, an electrocardiogram (ECG) should be obtained to assess for evidence of arrhythmia or cardiac ischemia.
• The ECG helps determine if an arrhythmia is present, which may have caused the stroke.
• Atrial fibrillation is an arrhythmia in which clots form in the heart and may travel to the brain (hence a cardioembolic etiology).
• Other changes that might be found on an ECG are an inverted T wave, ST depression, and QT elevation and prolongation.

• Additional tests that can be done are transesophageal echocardiography (TEE) and Holter monitoring.

• Definition of Transesophageal echocardiography• Transesophageal echocardiography: A diagnostic test,
using a special probe placed within the esophagus, that employs ultrasound waves to make images of the heart chambers, valves and surrounding structures.
• Transesophageal echocardiography (TEE) has unusually accurate imaging capabilities that permit the identification of previously unidentified anatomic features and surgical results that may necessitate a change in surgical plan or surgical revision before the patient leaves the operating suite.
• TEE is used to assess the anatomy and blood flow in congenital heart disease. TEE is used during surgery to evaluate the effects on the heart, for example, of the repair of a congenital heart defect. TEE can detect blood clots in the atrium and is therefore useful in guiding cardioversion (to normalize the heart rhythm) in patients with atrial fibrillation who are prone to form such clots.



• In medicine, a Holter monitor (also called an ambulatory electrocardiography device), named after its inventor, Dr. Norman J. Holter, is a portable device for continuously monitoring the electrical activity of the heart for 24 hours or more. Its extended recording period is sometime useful for observing occasional cardiac arrhythmias that would be difficult to identify in a shorter period of time. For patients having more transient symptoms, a cardiac event monitor which can be worn for a month or more can be used.





• In summary, prompt performance and interpretation of a CT scan is crucial to acute stroke management.
• Head CT and TCD provide vital information and allow the physician to make the decision to use thrombolytic therapy.
• An alternate approach is urgent MRI with PWI and DWI.

• CLINICAL MANAGEMENT• The management of an ischemic
stroke comprises four primary goals: restoration of cerebral blood flow (reperfusion),
• prevention of recurrent thrombosis, neuroprotection, and supportive care.
• The timing of each element of clinical management needs to be implemented in a decisive manner.

• Optimally, patients are initially evaluated at a center that has a stroke program.
• Decisions in the emergency department determine the patient’s treatment plan.
• Emergency departments may have emergi-paths, critical pathways, or protocols that have been developed by a multidisciplinary team to guide care.

• The focus of initial treatment should be to save as much of the ischemic area as possible.
• Three ingredients necessary to this area are oxygen, glucose, and adequate blood flow.
• The oxygen level can be monitored through arterial blood gases (ABGs), and oxygen can be given to the patient if indicated.
• Hypoglycemia can be evaluated with serial checks of blood glucose. Reperfusion may be accomplished by the use of IV tissue plasminogen activator (t-PA).

• Cerebral perfusion pressure is a reflection of the systemic blood pressure, ICP, functioning autoregulation in the brain, and heart rate and rhythm.
• The parameters most easily controlled externally are the blood pressure and cardiac rate and rhythm.
• Arrhythmias usually can be corrected.
• If the patient is a candidate for thrombolytic therapy, treatment with t-PA begins in the emergency department, and he or she is then moved to the ICU for further monitoring.
• If the individual is not a candidate for thrombolytic therapy, the complexity of the patient’s problems determines his or her placement in the ICU, medical unit, or stroke specialty unit.
• Pharmacological Management• Thrombolytic agents are exogenous drugs
that dissolve clots.
• The U.S. Food and Drug Administration currently approves t-PA for stroke.
• Dissolving the clot permits reperfusion of the brain tissue.
• IV thrombolytic therapy should be initiated within 3 hours or less of the onset of neurological symptoms.
• The clock begins for the patient from the time he or she was last seen well.
• For example, a patient retires to bed at 11:00 P.M. and awakens at 5:00 A.M. to go to the bathroom.
• As he attempts to rise from the bed, he feels weak and has difficulty standing up.
• As he calls out for his wife’s help, his speech is garbled.

• The last time he was awake and functioning normally was 11:00 P.M. Even if his symptoms started only a few minutes ago, the time he was last seen well was 6 hours ago.
• Therefore, he is already outside of the treatment window for IV t-PA.
• Candidate selection for t-PA must be done carefully.
• The neurological examination, NIHSS score, and results of neuroimaging studies assist the physician with the decision to offer thrombolytic therapy.
• Box 35-2 outlines eligibility criteria for this treatment.
• The standards for the administration of IV t-PA to treat stroke are a result of the National Institute of Neurologic Disorders and Stroke (NINDS) t-PA Stroke Study
• . A dose of IV t-PA, 0.9 mg/kg (maximum dose, 90 mg), is administered as 10% of the total dose as a bolus over 1 to 2 minutes, with the remainder infused over 60 minutes.
• The t-PA activates plasminogen, a naturally occurring enzyme present in the intravascular endothelium that protects against excessive clotting.
• Activating plasminogen initiates the process of dissolving the clot through fibrinolysis.
• No other antithrombotic therapy should be given for the next 24 hours.
• A major risk of this therapy is intracerebral hemorrhage.
• However, it is encouraging that this agent may prove effective in reversing neurological deficit and improving quality of life after a stroke.

• The direct administration of a thrombolytic into a vessel is an alternative to IV t-PA.
• Such administration is effective in acute ischemic stroke and can be given up to 6 hours after the onset of symptoms.
• A limiting factor is that the patient must be admitted to a specialty center in which localized intra-arterial infusion of thrombolytic agents is possible

• Through this approach, an occluded cerebral artery can be reopened.
• For intra-arterial therapy, a femoral arterial sheath is usually inserted, through which a microcatheter can be threaded, under fluoroscopy.
• The catheter tip is positioned into the clot and advanced as the clot dissolves.

• The femoral sheath usually remains in place for 24 hours in case of recurrent vessel occlusion.
• The advantage of this approach is that the medication can be delivered directly to its target.
• Aside from thrombolytic therapy, secondary treatment options for stroke include anticoagulation with antithrombotic and antiplatelet agents.
• If a patient experiences atrial fibrillation, anticoagulation with warfarin (Coumadin) may be warranted.
• The patient needs instruction about bleeding precautions, however.
• Education also includes the purpose of the medication, information about moderate consumption of leafy green vegetables containing vitamin K, and the importance of having blood drawn regularly to monitor prothrombin time (PT) and the international normalized ratio (INR).
• In addition, for safety, patients should be instructed to obtain Medic Alert cards and bracelets so they can be identified as taking an anticoagulant in the event of a medical emergency.

• Antiplatelet drugs include dipyridamole-ER, ticlopidine, clopidogrel, and aspirin.
• These agents deter platelets from adhering to the wall of an injured blood vessel or other platelets and are given to prevent a future thrombotic or embolic event.
• The modified-release formula of dipyridamole increases the effect of specific factors that act as antiaggregates to reduce platelet aggregation.

• Ticlopidine inhibits platelet function by suppressing adenosine diphosphate–induced platelet aggregation and aggregation due to other factors.
• The recommended dose for ticlopidine is 250 mg twice a day.
• Neutropenia and thrombocytopenia are known side effects.

• Clopidogrel also inhibits the activity of adenosine diphosphate, but is not associated with an increased risk of neutropenia.
• Aspirin limits platelet adhesion and aggregation.
• The suggested dose of aspirin is 81 to 325 mg per day.
• The administration of these agents plays a role in stroke prevention by decreasing the risk of future strokes.
• Control of Hypertension• and Increased Intracranial Pressure• The control of hypertension, ICP, and CPP may
take the efforts of both the nurse and the physician.
• The nurs must assess for these problems, recognize them and their significance, and ensure that medical interventions are initiated.

• Patients with moderate hypertension usually are not treated acutely.
• If their blood pressure decreases after the brain becomes accustomed to the hypertension needed for adequate perfusion, the brain’s perfusion pressure will fall along with the blood pressure.
• If the diastolic blood pressure is above approximately 105 mm Hg, it may need to be lowered gradually.
• This may be accomplished effectively with labetalol (antihypertensive drug (trade names Trandate and Normodyne) that blocks alpha and beta-adrenergic receptors of the sympathetic nervous system).

• If ICP is elevated in a patient who has had a stroke, it usually occurs after the first day.
• Although this is a natural response of the brain to some cerebrovascular lesions, it is destructive to the brain.
• The destructive response, such as edema or arterial vasospasm, can sometimes be treated or prevented
• The usual methods of controlling increased ICP can be instituted: hyperventilation; fluid restriction; head elevation; avoidance of neck flexion or severe head rotation that would impede venous outflow from the head; and the use of osmotic diuretics (mannitol) to decrease cerebral edema
• Surgical Management• In patients with carotid stenosis, carotid
endarterectomy may be performed to prevent a stroke.
• Carotid endarterectomy is a surgical procedure in which atherosclerotic plaque that has accumulated inside the carotid artery is surgically removed.
• Once the plaque is removed, blood flow is restored.

• This surgery has fallen in and out of favor during the last decade.
• The North American Symptomatic Carotid Endarterectomy Trial (NASCET) and the European Carotid Surgery Trial (ECST) were designed to examine the benefit of surgery for patients with symptomatic carotid stenosis.
• These studies determined that carotid endarterectomy is justifiable in patients with high-grade stenosis (≥70%) if the operation is performed by a skilled surgeon.
• The benefit of surgery increases for male patients with a prior history of stroke.
• Patients with less than 50% stenosis do not benefit from surgery.

• Nursing Management• Assessment. A thorough neurological assessment
is essential to identify deficits the patient is experiencing. As previously discussed, the NIHSS is a valuable tool that can be used in the emergency department to rate severity of the stroke and determine if the individual is a candidate for
• t-PA (see Table 35-9). The brevity and reliability of the tool make it ideal for use in the emergency department.
• The NIHSS is also helpful for making subsequent assessments and should be performed in conjunction with the neurological examination.
• As a member of a large multidisciplinary team, the nurse must be prepared to assume a critical role to assist with the administration of thrombolytic therapy, optimize acute patient care, and move the patient to rehabilitation quickly to maximize the patient’s outcome.

• The patient needs to be carefully monitored for infection, changes in temperature, and changes in glucose level, all of which have potentially deleterious effects in patients who have had a stroke.
• The nurse is in the unique position to identify problems and collaborate with the physician to initiate appropriate referrals to rehabilitation medicine specialists, social workers, speech–language pathologists, or dietitians.
• Because of the nature of the patient’s problems, the multidisciplinary approach provides comprehensive care by addressing all needs.

• Plan. The nurse plays a significant role in preventing complications associated with immobility, hemiparesis, or any neurological deficit produced by a stroke.
• Preventive measures are particularly important in the areas of urinary tract infections, aspiration, pressure ulcers, contractures, and thrombophlebitis.
• Effective interventions for the treatment of acute stroke help lower the death rate and reduce the morbidity of patients who have had a stroke.
• The Collaborative Care Guide (Box 35-3) delineates the specific outcomes and interventions for the patient who has had a stroke.

• Emotional and Behavioral Modification. Patients who have experienced a stroke may display emotional problems, and their behavior may be different from baseline.
• Emotions may be labile; for example, the patient may cry one moment and laugh the next, without explanation or control
• Tolerance to stress may also be reduced..

• A minor stressor in the prestroke state may be perceived as a major problem after the stroke.
• Families may not understand the behavior.
• Patients may show frustration or agitation with the nursing staff or their family members.

• It is the nurse’s role to help the family understand these behavioral changes.
• Also, the nurse can help modify the patient’s behavior by controlling stimuli in the environment, providing rest periods throughout the day to prevent the patient from becoming overtired, giving positive feedback, and providing repetition when the patient is trying to relearn a skill.
• Communication. Patients can demonstrate much frustration with their deficits.
• Probably no deficit produces more frustration for the patient and those trying to communicate with him or her than the one involving the production and understanding of language.

• Dysphasia can involve motor abilities, sensory function, or both.
• If the area of brain injury is in or near the left Broca’s area, the memory of motor patterns of speech is affected.
• This results in an expressive dysphasia, in which the patient understands language but is unable to use it appropriately.

• Receptive dysphasia usually is a result of injury to the left Wernicke’s area, which is the control center for recognition of spoken language.
• The patient therefore is unable to understand the significance of the spoken word.
• The presence of both expressive and receptive dysphasia is referred to as global dysphasia.
• Box 35-4 summarizes differences between expressive and receptive problems.

• It is important for the nursing staff to inform families that having dysphasia does not mean that a person is intellectually impaired.
• Communication at some level should be attempted, whether it is by writing, using picture boards, or gestures.
• PATIENT EDUCATION• AND DISCHARGE PLANNING• Education must provide information to
patients about modifying risk factors and teach individuals to recognize the signs and symptoms of a stroke.
• Information can be presented regarding medication and other lifestyle modifications to manage blood pressure.
• Patients can be referred to smoking cessation programs.
• Education can also be provided about weight management and exercise programs.
• Compliance with medication regimens should also be stressed.

• Hospitals need to organize community outreach programs regarding stroke prevention, the recognition of signs and symptoms of a stroke, its emergent nature, and the need to contact 911 at the onset of symptoms.
• There must be public awareness about the signs and symptoms, such as sudden onset of numbness or weakness of the face, arm, or leg; confusion; trouble speaking or understanding; vision problems; dizziness; loss of balance; or severe headache.

• The urgency of immediate attention must be stressed.
• Emergency medical personnel need to be able to identify the symptoms of a stroke and mobilize the patient to the nearest hospital with a full complement of stroke services from diagnosis to discharge.

• In addition, a stroke is often a life-changing experience for the patient and family.
• Depending on the outcome, family members may require education about how to provide care for the patient at home.
• Instruction about mobility, nutrition, safety, sleep, and eliminative care must occur, along with referrals for home care, if appropriate.
• With support, the patient will be able to achieve maximum quality of life and reintegrate into the community.
• Hemianopsia, sometimes called Hemianopia, is blindness in one half of the visual field.

• Stroke. 2001;32:2042.)© 2001 American Heart Association, Inc. Original Contributions
• Parenchymal Hyperdensity on Computed Tomography After Intra-Arterial Reperfusion Therapy for Acute Middle Cerebral Artery Occlusion
• Incidence and Clinical Significance • Shinichi Nakano, MD; Tsutomu
• All patients underwent intra-arterial reperfusion therapy, either thrombolytic therapy or percutaneous transluminal angioplasty (PTA), or both. Before the initiation of reperfusion therapy, a microcatheter was introduced beyond the thrombus and local
angiography was performed to assess the size of thrombus or the precise site of occlusion. Therefore, contrast medium may be injected to the ischemic core even without recanalization. As for treatments, we had no prospective protocol. As for CT examinations, however, there was a prospective protocol. Informed
consent for CT examinations and treatments was obtained from the patients or their family members.
All patients underwent intra-arterial reperfusion therapy, either thrombolytic therapy or percutaneous transluminal angioplasty
(PTA), or both. Before the initiation of reperfusion therapy, a microcatheter was introduced beyond the thrombus and local
angiography was performed to assess the size of thrombus or
the precise site of occlusion. Therefore, contrast medium may
be injected to the ischemic core even without recanalization.
As for treatments, we had no prospective protocol. As for CT
examinations, however, there was a prospective protocol. Informed consent for CT examinations and treatments was obtained from the patients or their family members.

• Direct PTA was performed with a Stealth angioplasty balloon catheter with a maximum diameter of 2.0 to 2.5 mm. The balloon catheter was advanced into the occlusion site and inflated to 2 atm initially and subsequently up to 3 atm. Several inflations of 30 seconds each were performed until recanalization of the MCA trunk was established. After each inflation, repeated angiography was obtained to assess the degree of recanalization and the presence or absence of distal embolic occlusions.
• Before 1996, all patients were treated with intra-arterial thrombolytic therapy. Our recent therapeutic protocol since 1996 has been reported previously.7,8 In brief, when early CT signs were present and/or lenticulostriate arteries were involved in ischemia, we preferred direct PTA to thrombolytic therapy as the first choice of the treatment. For patients with MCA trunk occlusion with neither lenticulostriate artery involvement nor early CT signs, intra-arterial thrombolytic therapy was selected. For patients with M2 occlusion, intravenous infusion of native tissue
plasminogen activator (tPA [tisokinase]) was selected in case without early CT signs and intra-arterial thrombolysis was performed only when early CT signs were present.
• Direct PTA was performed with a Stealth angioplasty balloon catheter with a maximum diameter of 2.0 to 2.5 mm. The balloon
catheter was advanced into the occlusion site and inflated to 2 atm initially and subsequently up to 3 atm. Several inflations of 30 seconds each were performed until recanalization of the MCA trunk was established. After each inflation, repeated angiography was obtained to assess the degree of recanalization and the
presence or absence of distal embolic occlusions.

• Doses of urokinase ranged from 60 000 to 600 000 U, with 10 mL saline/60 000 U, in boluses. Doses of native tPA ranged from 3.6 to 14.4 mg, with 10 mL saline/1.8 mg tPA, in boluses. Just before the initiation of reperfusion therapy, 5000 U heparin was administered intravenously. An additional 1000 U intravenous heparin was administered at 1-hour intervals during the procedure of the reperfusion therapy. For incomplete recanalization or residual severe stenosis without intraparenchymal hyperdense areas on posttherapeutic CT only, an intravenous continuous infusion of 10 000 to 15 000 U heparin/d was administered for 7 days. When complete recanalization was achieved or intraparenchymal hyperdense areas were seen, we performed strict blood pressure to <160/90 mm Hg with neither anticoagulation nor antiplatelet treatment after reperfusion therapy. The degree of recanalization was classified into 3 grades: complete, partial, and no recanalization.