current management pleural effusion, empyema, complicated ... · current management pleural...
TRANSCRIPT
Current ManagementPleural Effusion, Empyema,
Complicated Pneumonia
Update in Pediatrics
Vincent Adolph, MD
Pediatric Surgery
July 20, 2019
• No Financial Conflicts of Interest
• Thrombolytic use is off-label
• Describe the difference between pleural effusion and empyema
• Explain the role of imaging in patients with complicated pneumonia
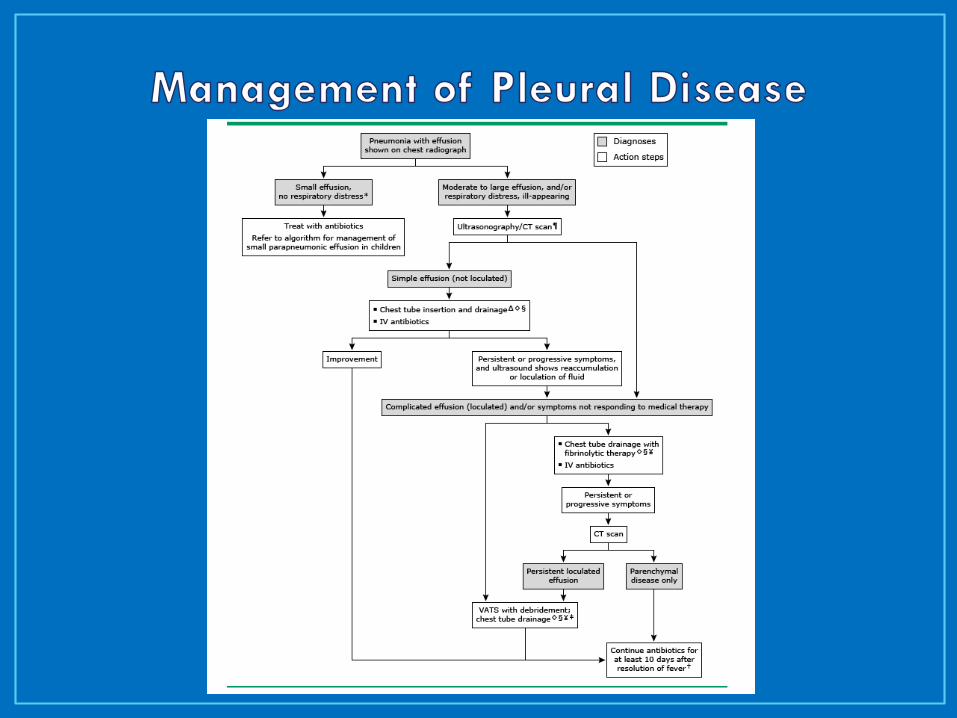
• Explain the options for management of pleural effusion and empyema
• Know how to evaluate for parenchymal complications of pneumonia
• Evaluation / Decision making
• Antibiotic Selection
• Definitions
• Imaging
• Treatment
• Determining treatment failure
• Pulmonary Necrosis / Abscess / Pneumatocele
• Recurrent Pneumonia / Congenital Lung Lesions
• Duration of Antibiotic Therapy
• Assess Symptoms
• Resp sx, O2, fever, oral intake
• Parenchymal Process vs Pleural Disease
• Effusion vs Empyema
• Parenchymal Complications
Abscess, Necrosis, Pneumatocele
• Hypoxemia (SaO2 < 92%)
• Tachypnea (infants RR > 70 , older >50)
• Retractions, nasal flaring, grunting, etc
• Inadequate oral intake
• Other chronic conditions
• Toxic appearance
• Suspicion of Staph or group A Strep
• Failure of outpatient therapy
• Complications (effusion, empyema, abscess)
• Impending respiratory failure
• Inability to maintain sats > 92%
• Apnea or irregular respirations
• Hypotension / Refractory tachycardia
• Multi-lobar infiltrates
• Mental status changes
• Pleural disease (effusion / empyema)
• SS ds, immuno-compromise
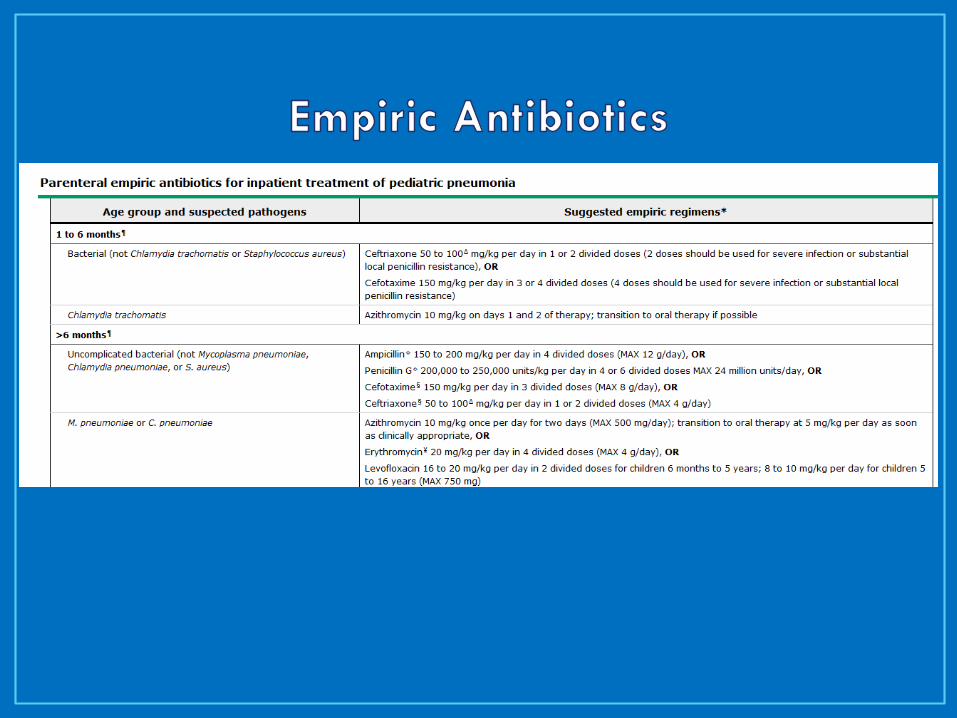
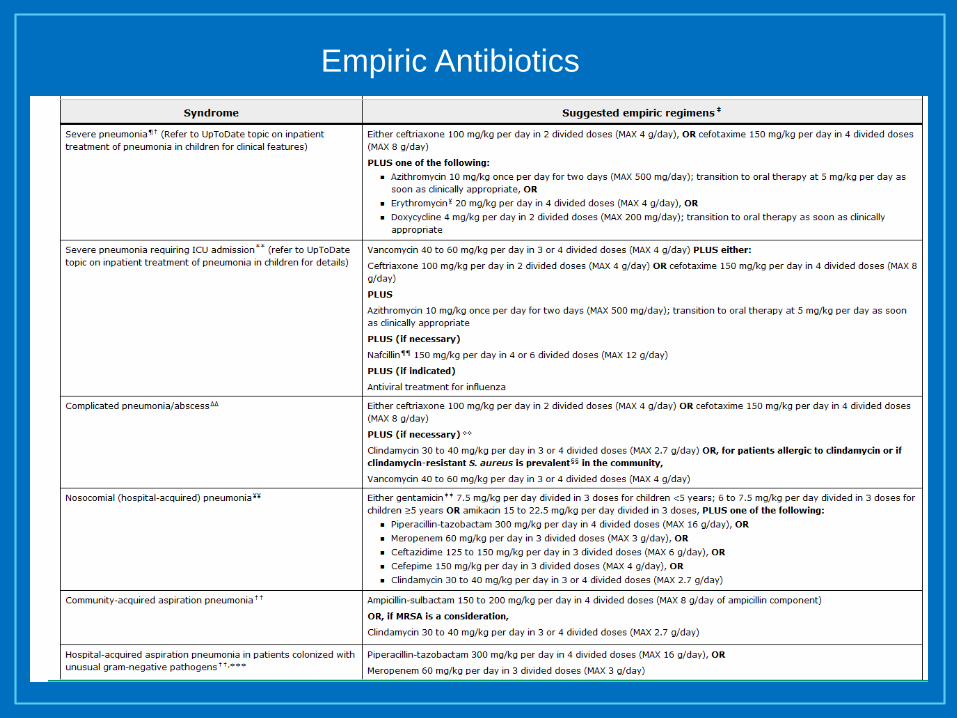
Empiric Antibiotics
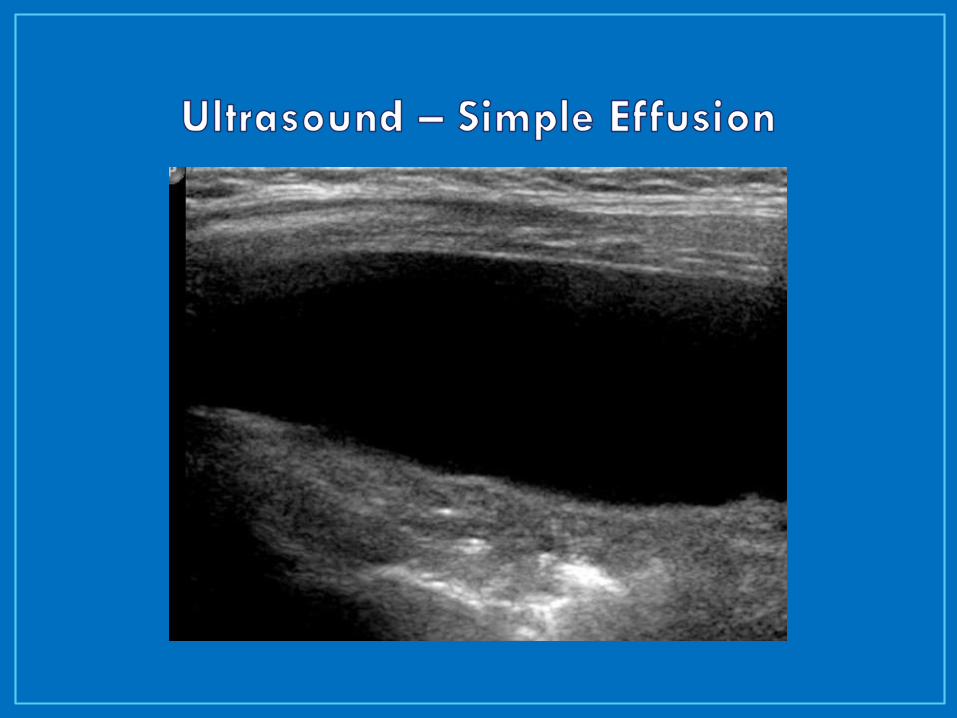
• Effusion
• Transudate
• Simple, free-flowing fluid
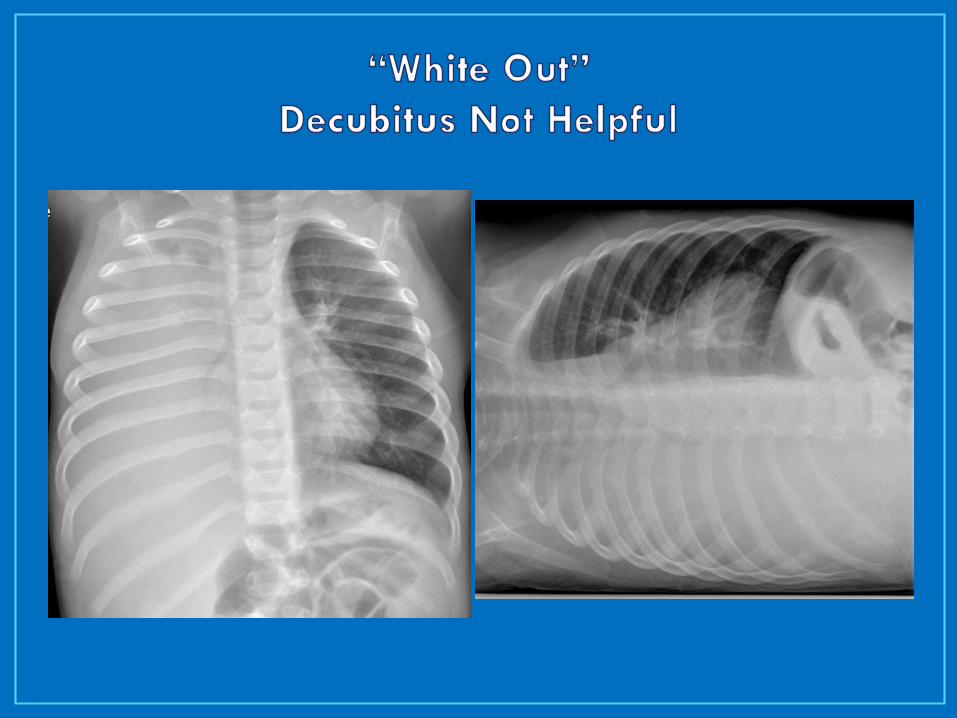
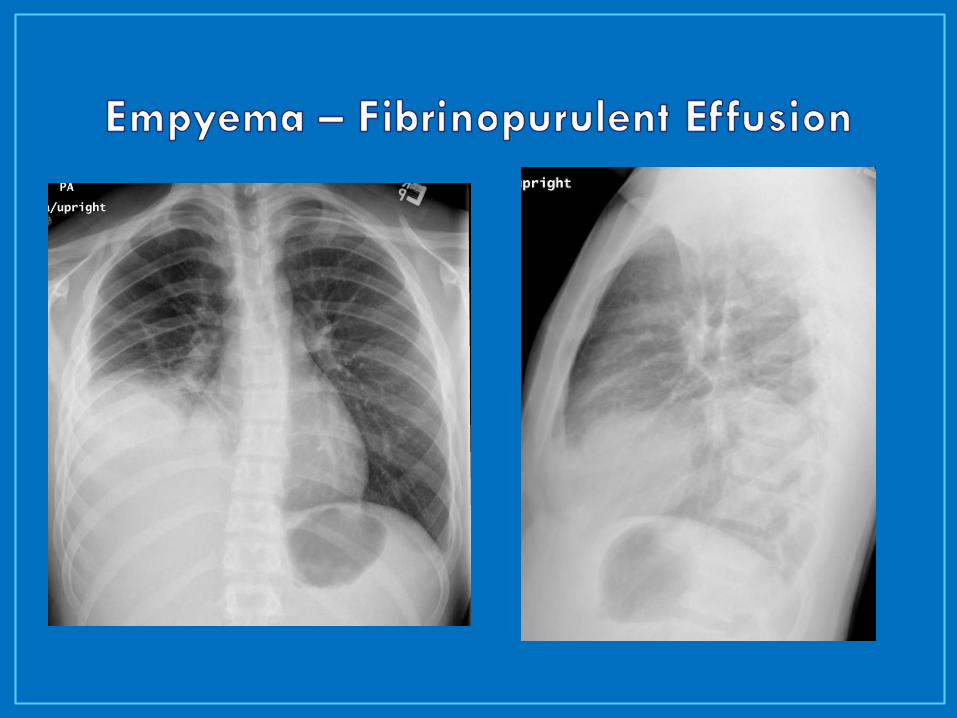
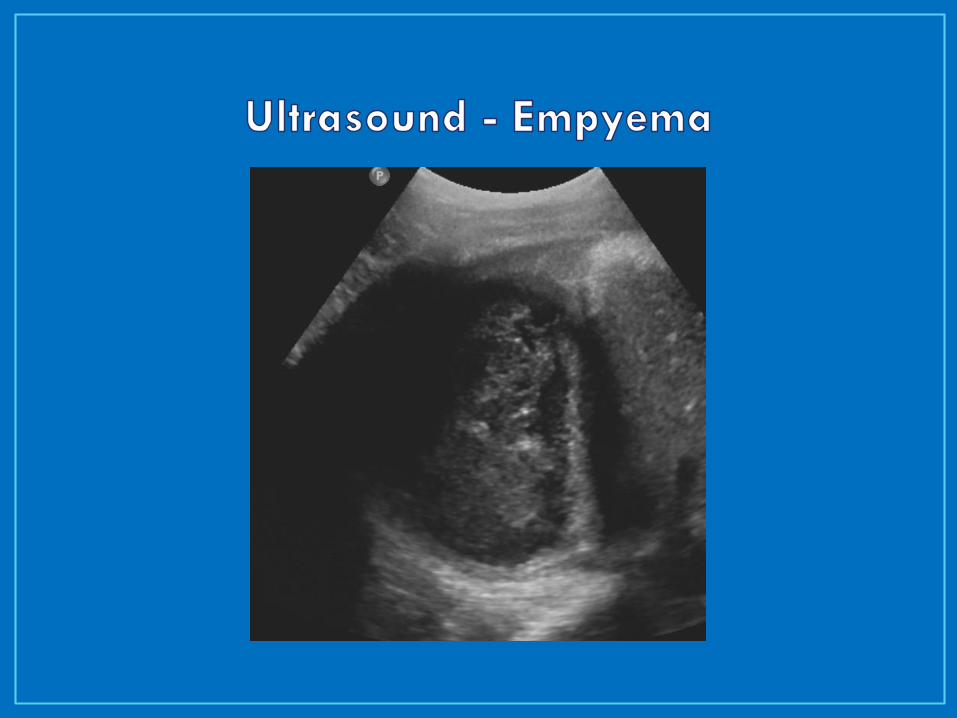
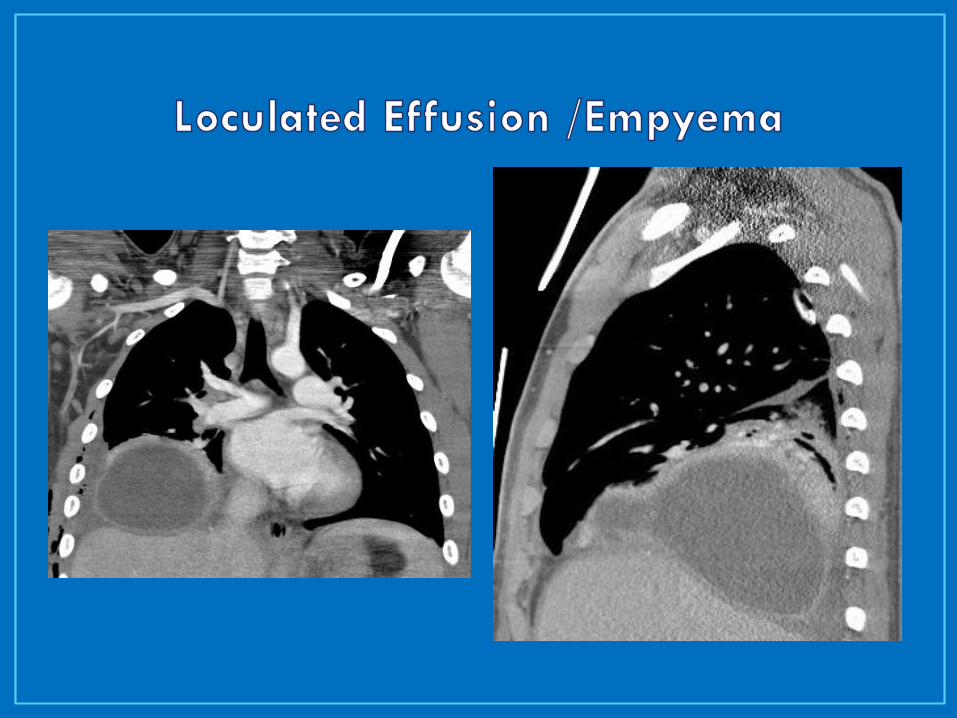
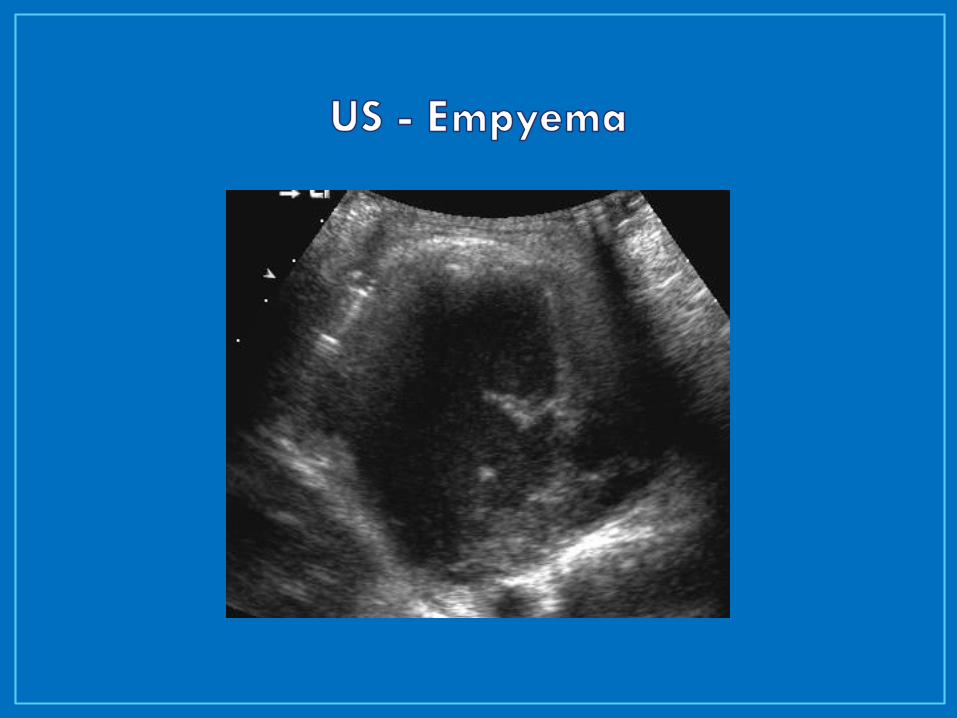
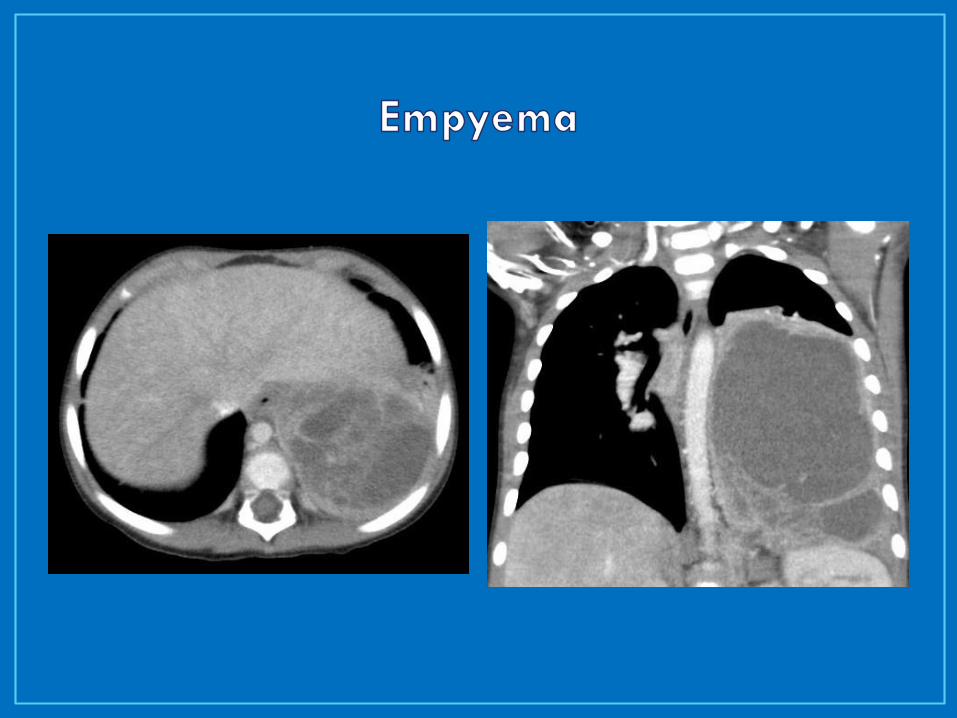
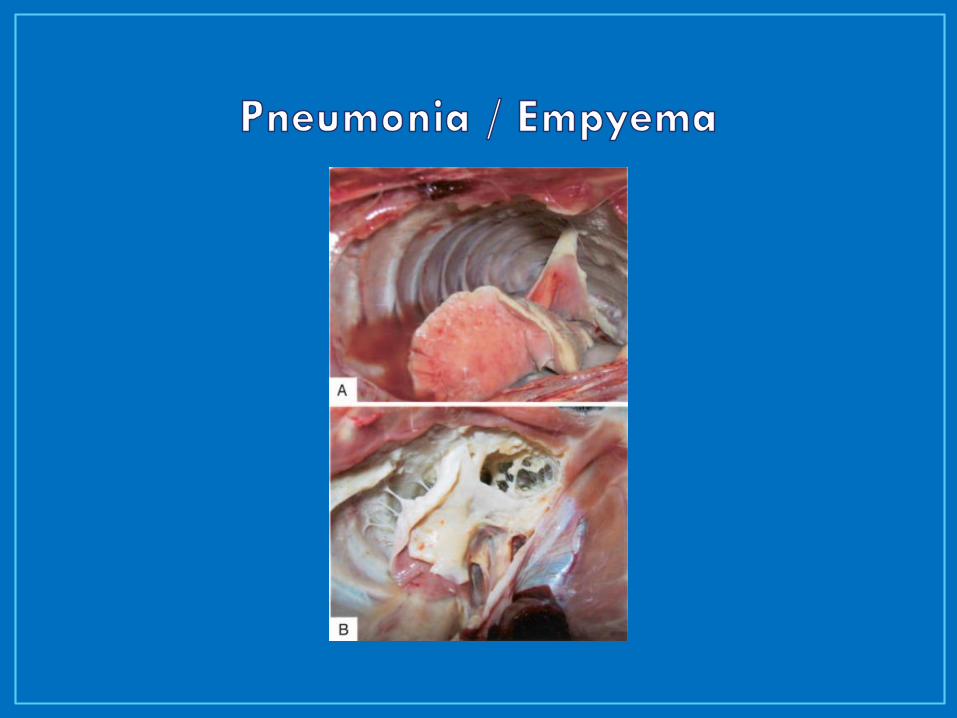
• Empyema
• Grossly purulent, WBC > 10,000 (<?)
• pH < 7.0, LDH > 1,000, Glucose < 40
• Positive gram stain
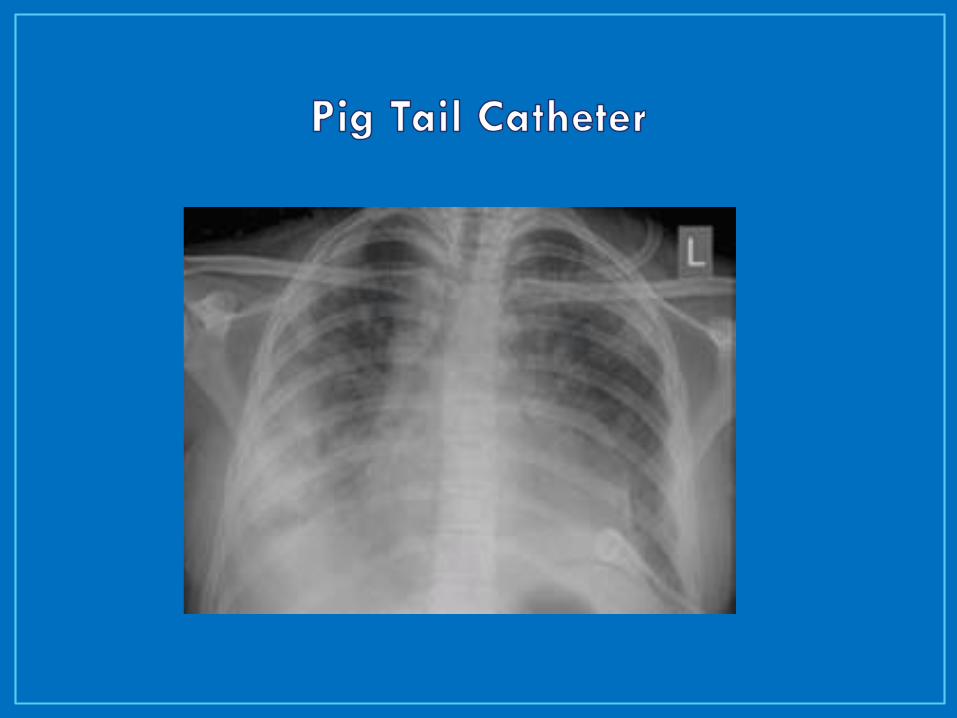
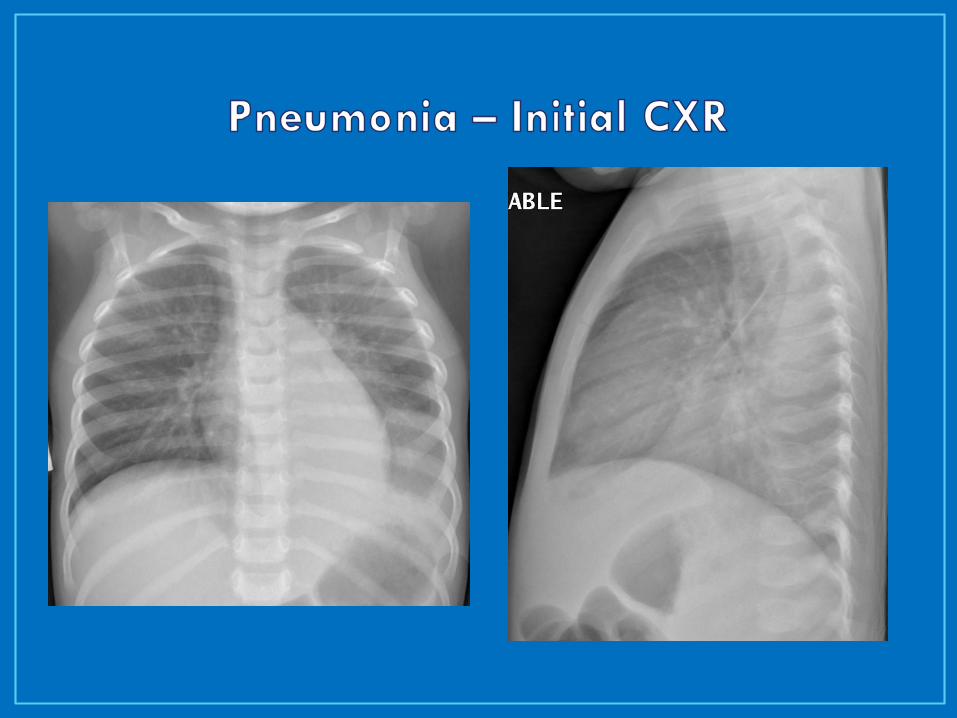
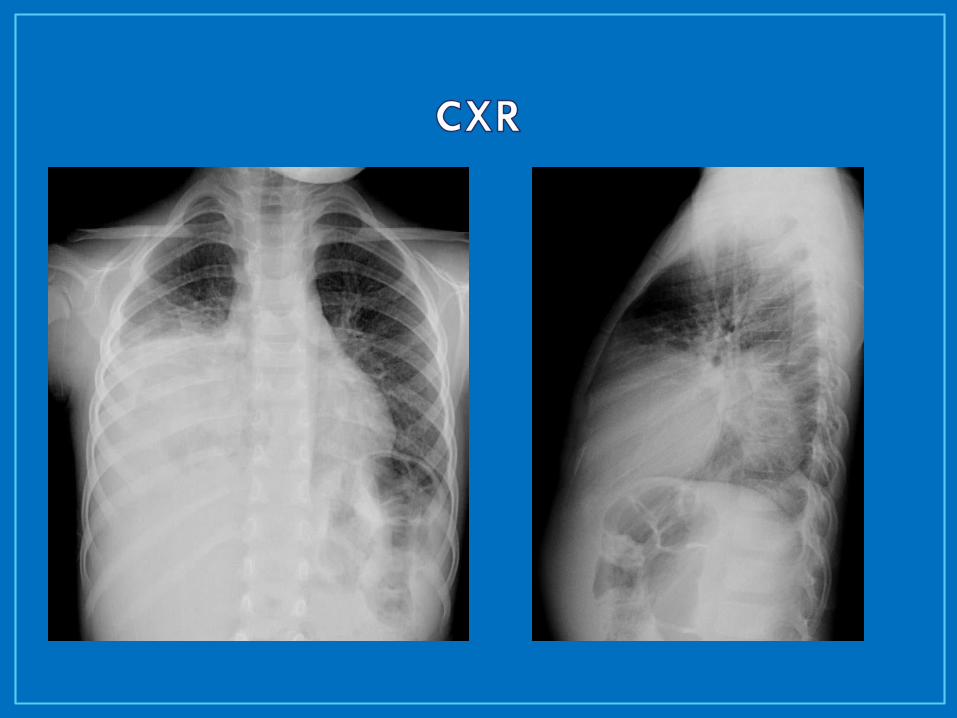
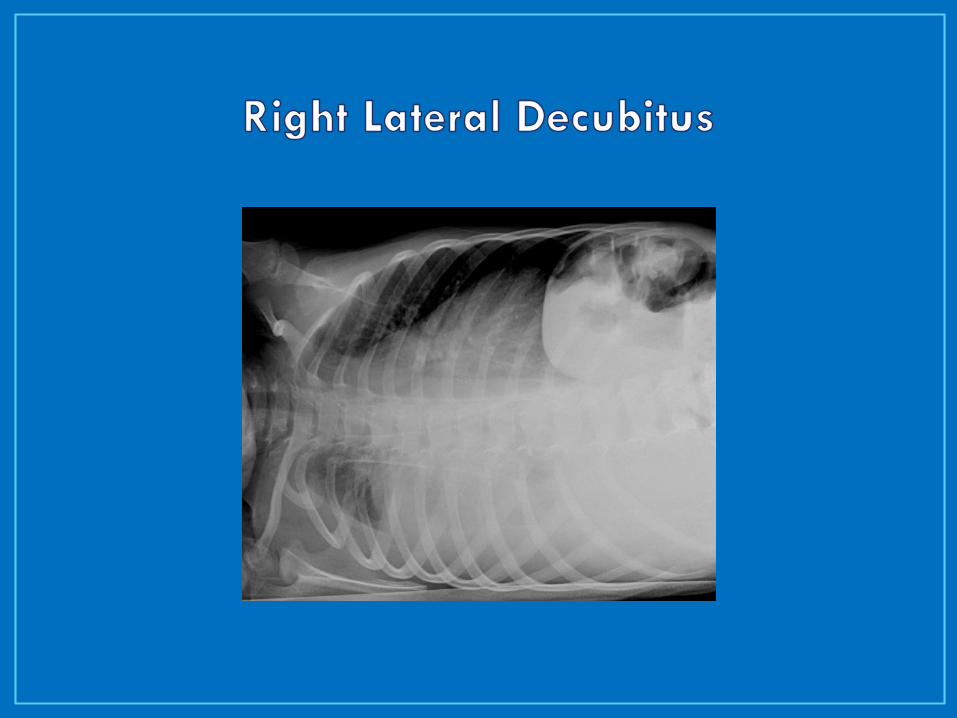
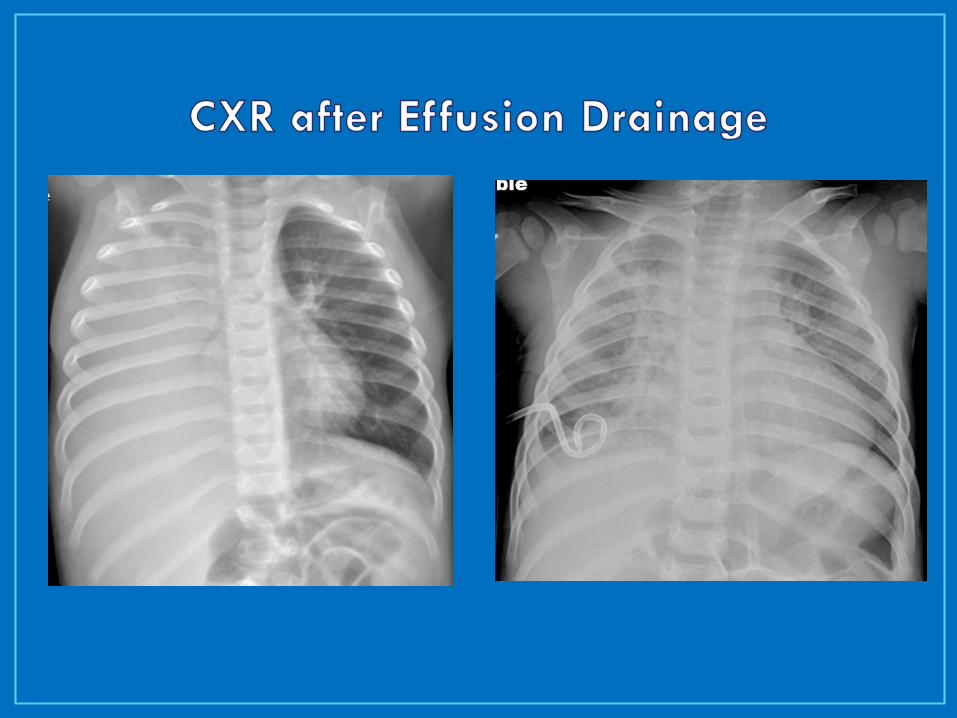
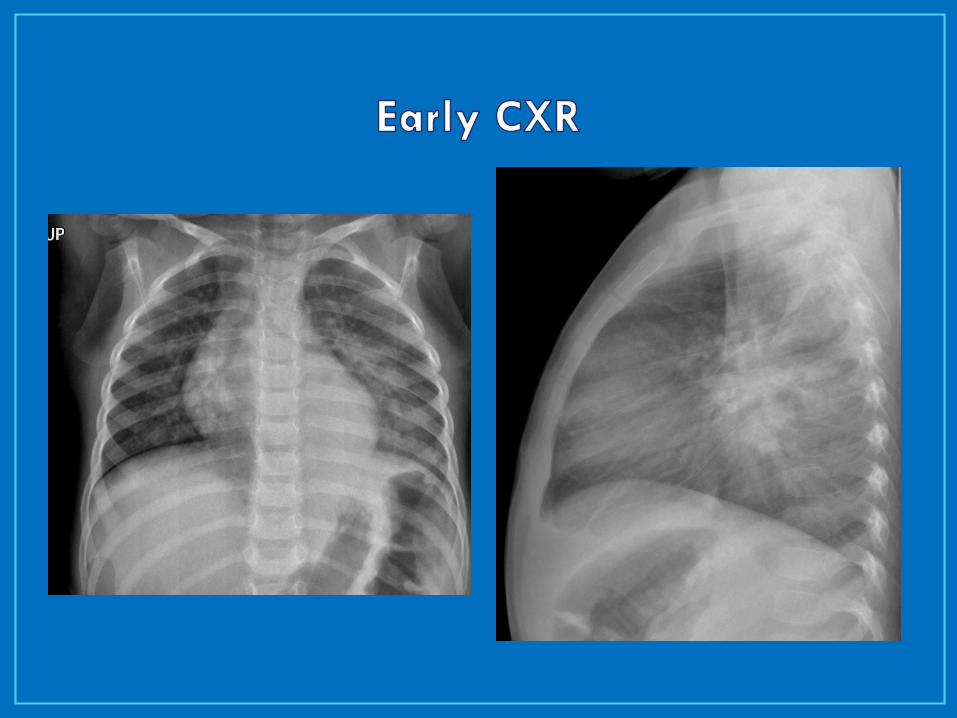
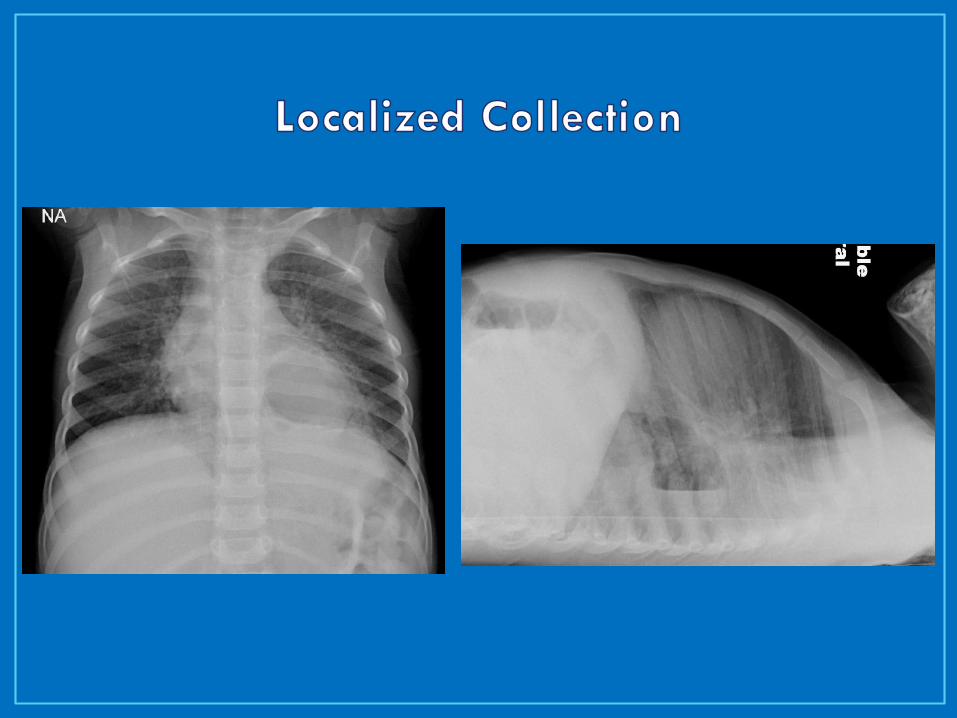
CXR
AP +/- decubitus (affected side down)
Ultrasound
Assess for pleural fluid volume / character
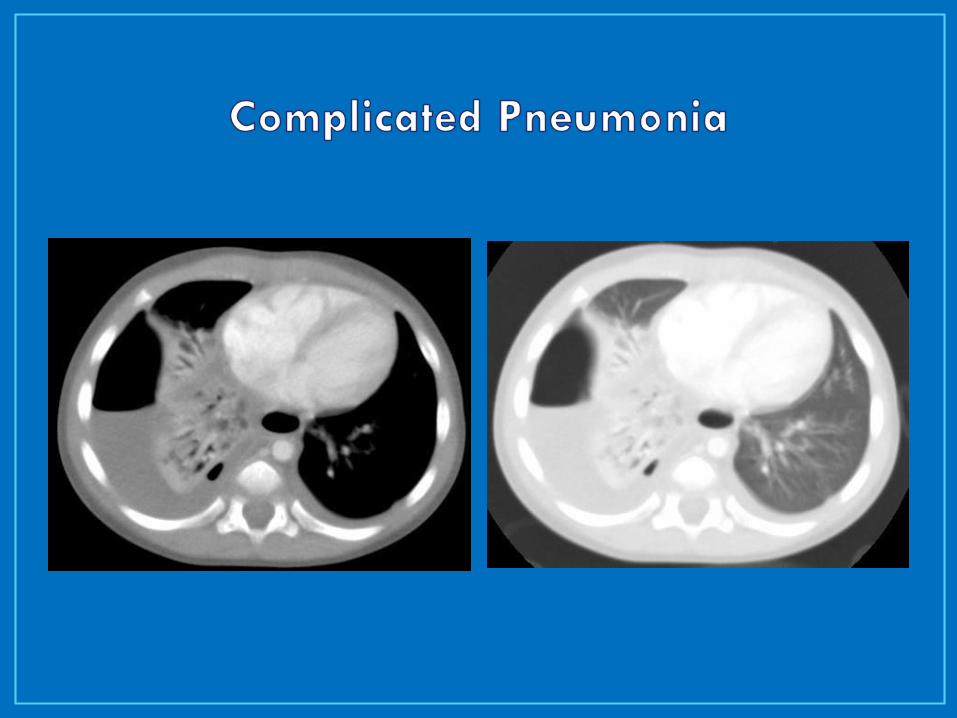
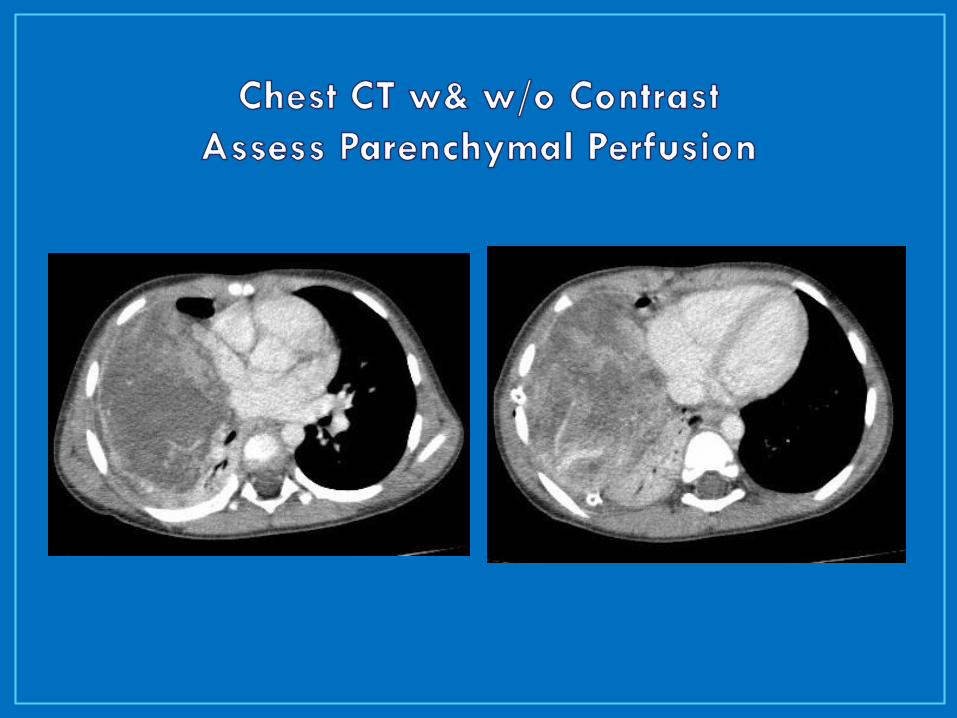
CT
Assess for parenchymal complications
IV contrast to assess for necrosis
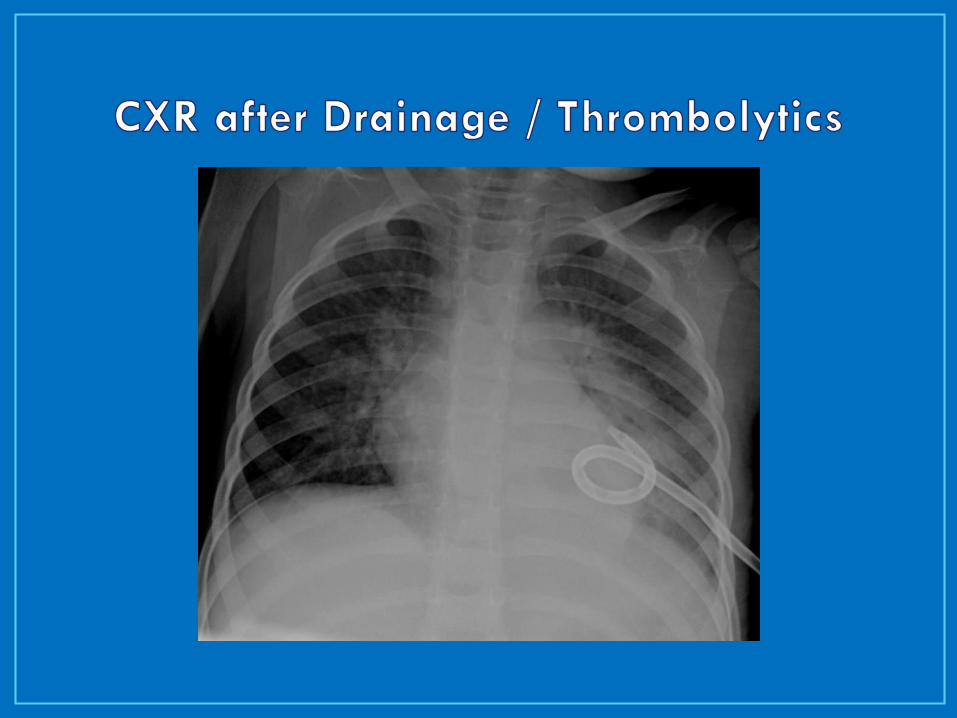
• tPA (Urokinase, Streptokinase)
• tPA: 4 mg in 40 ml NS
• Dwell time of 1 hour
• 3 doses over 48 hrs
• tPA: 0.1 mg/kg (up to 3 mg in 30 ml NS
• Every 8 hours for nine doses (3 days)
• Contraindications:
• Active air leak (broncho-pleural fistula)
• Recently healed leak ?
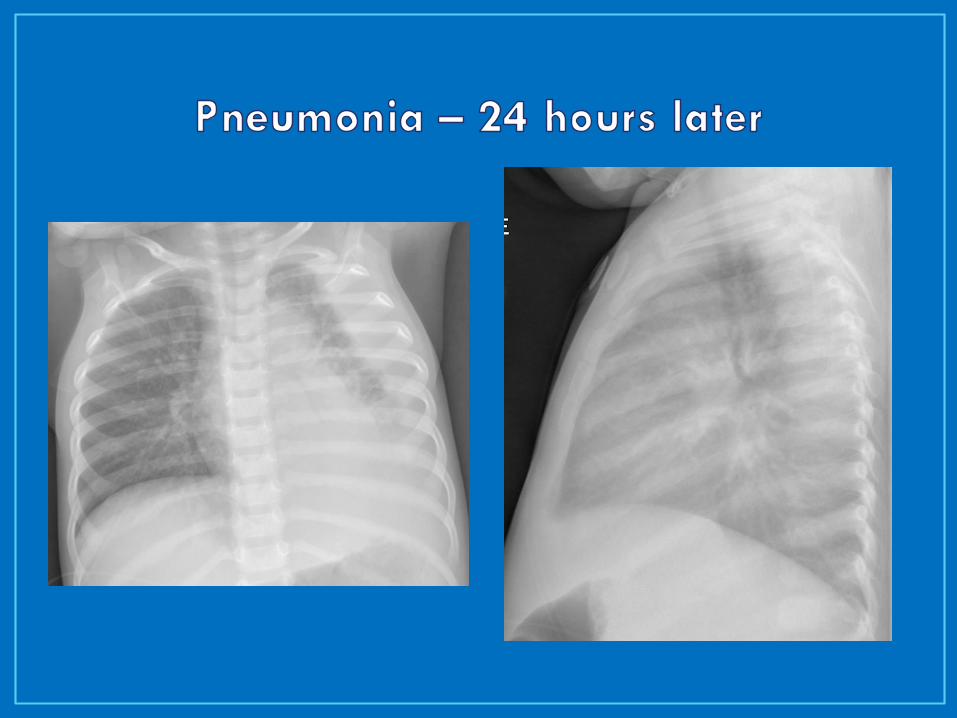
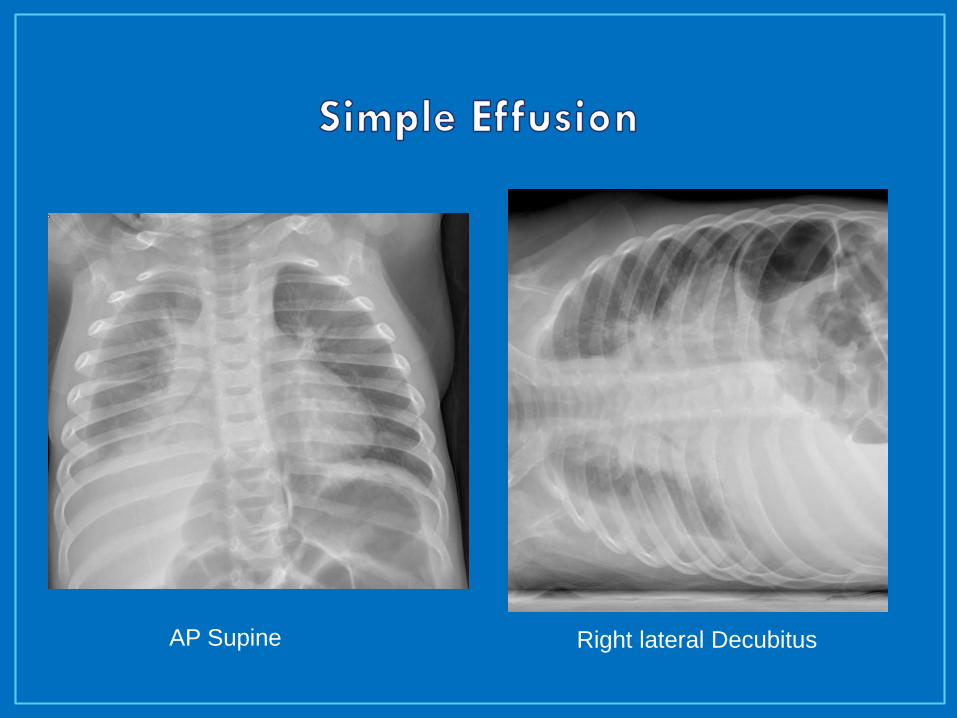
AP Supine Right lateral Decubitus
48-72 hours for CT / thrombolysis
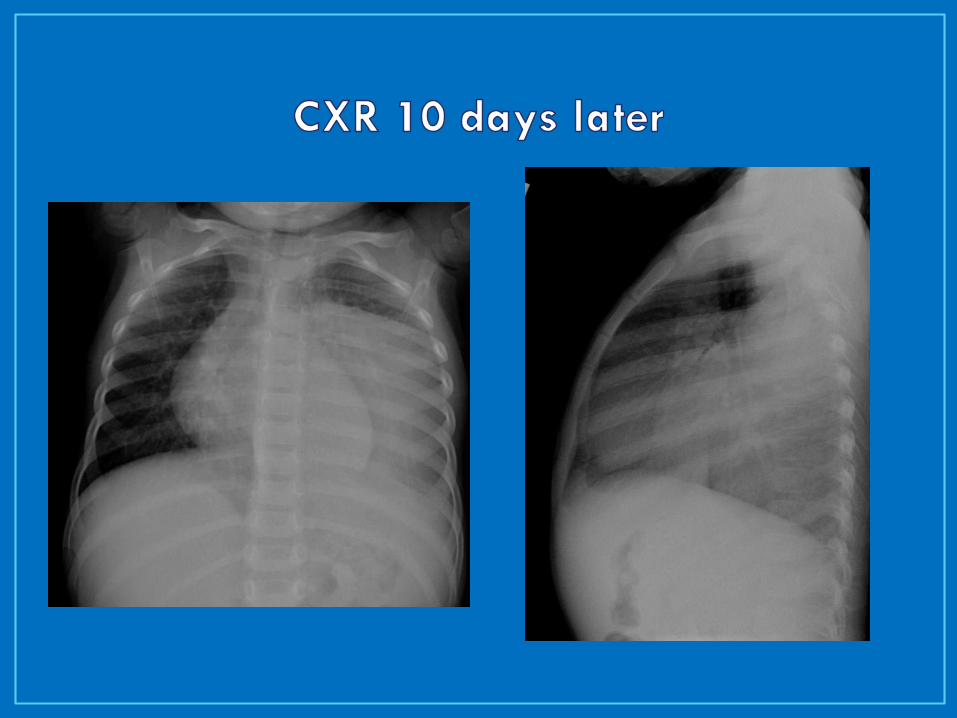
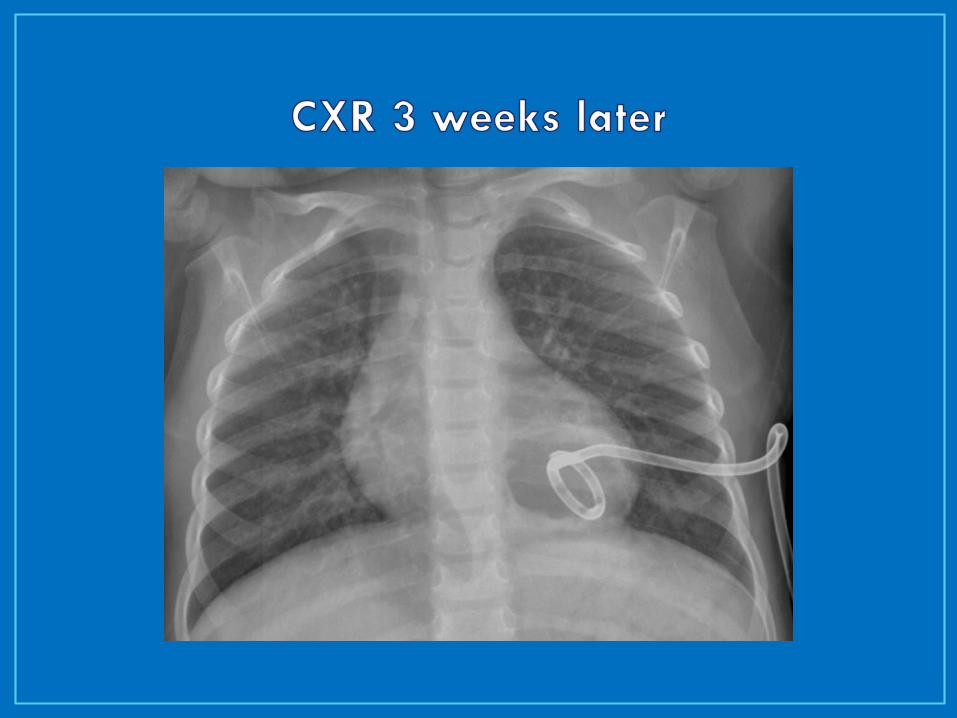
Failure to improve
Fever, Resp status, oral intake, O2 need
Re-image
Assess pleural space
Assess lung parenchyma
• Indications:
• Failure to improve with CT / thrombolytics
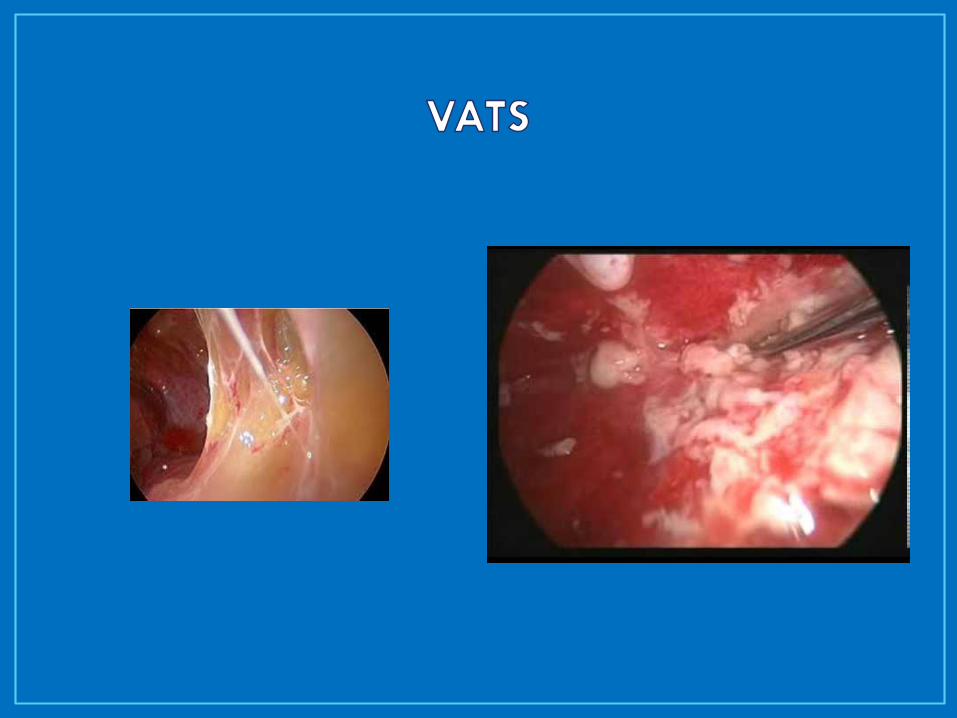
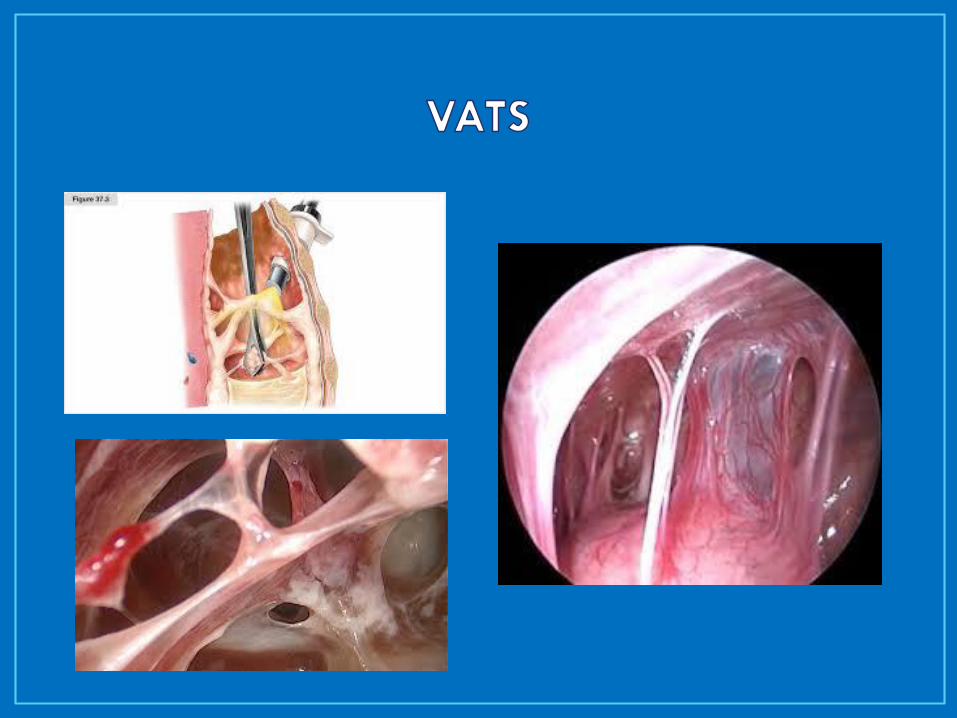
• VATS (Video-Assisted Thorascopic Surgery)
• Thorascopic debridement
• Thoracotomy
• Decortication – removal of thick fibrous pleural rind
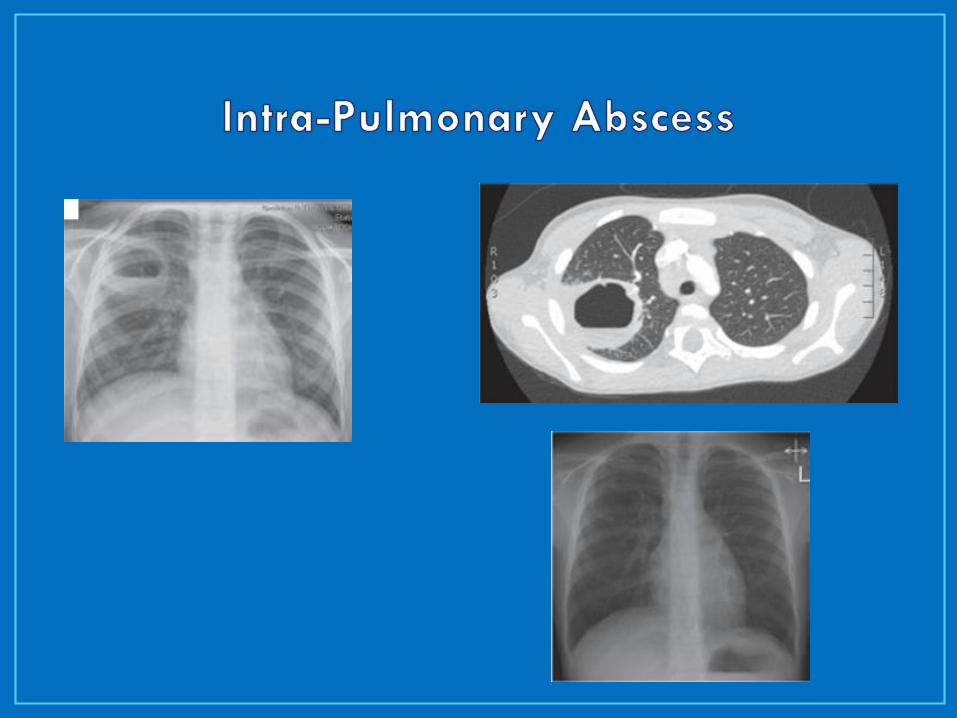
• Abscess
• Usually respond to longer course of antibiotics
• Selective aspiration / drainage
• Pneumothorax, pyo-pneumothorax
• Broncho-pleural fistula
• Pulmonary Necrosis
• Prolonged antibiotic course
• Very high risk with drainage, debridement, bx
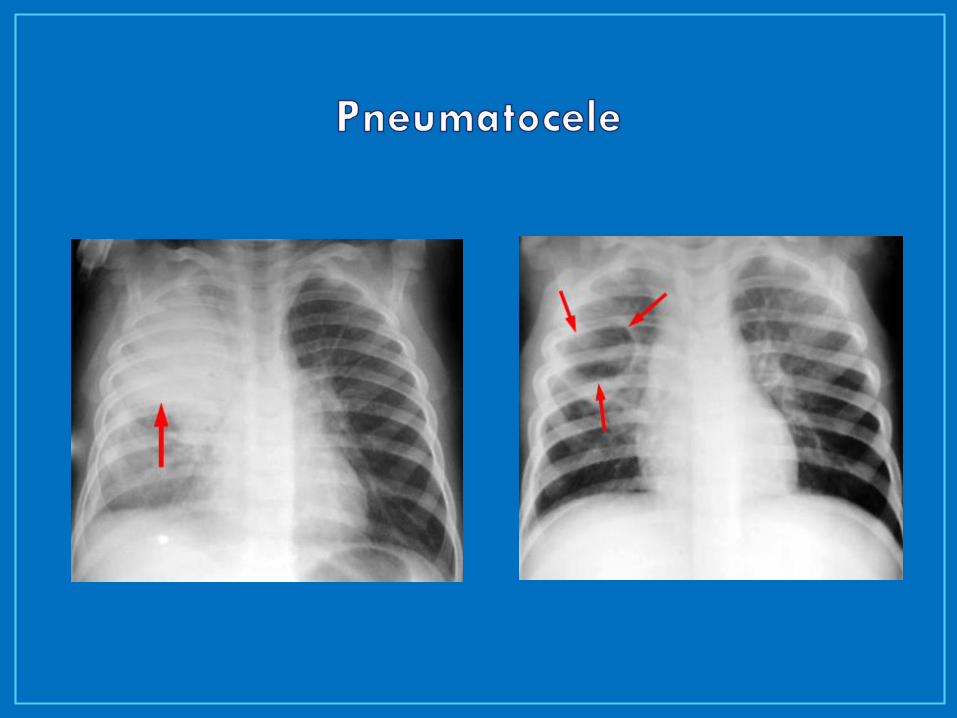
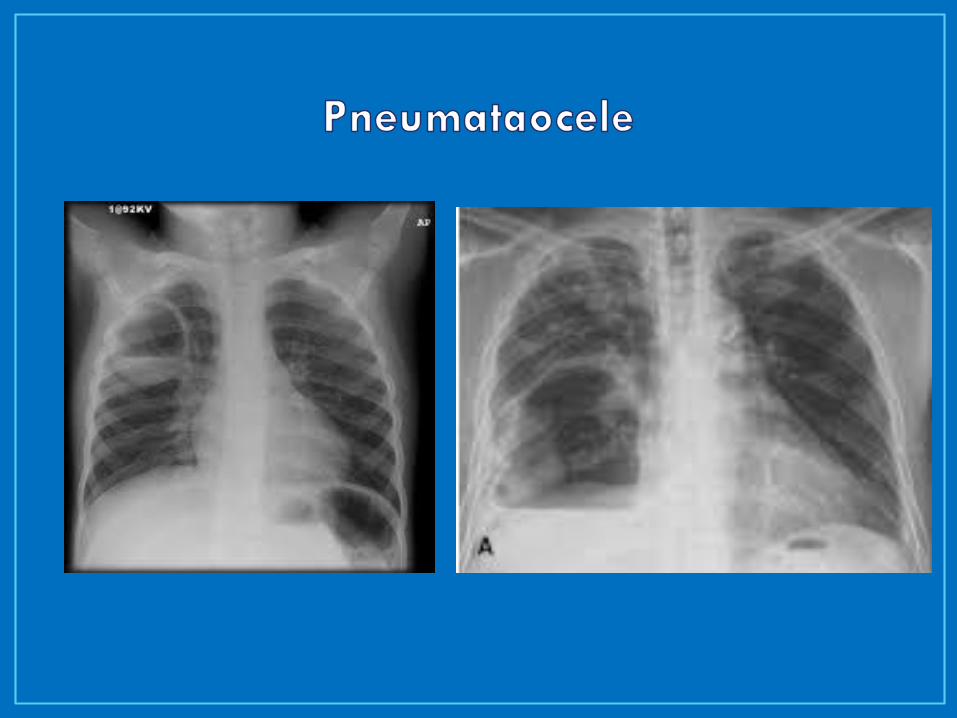
• Pneumatocele
• Recurrent Pneumonia in same lobe
• Pneumatocele
• Congenital Pulmonary Malformations
• CCAM
• (Congenital Cystic Adenomatoid Malformation)
• Sequestration
• Intrapulmonary
• Extrapulmonary
• Bronchogenic Cysts
Uncomplicated Pneumonia
One week after fever resolves
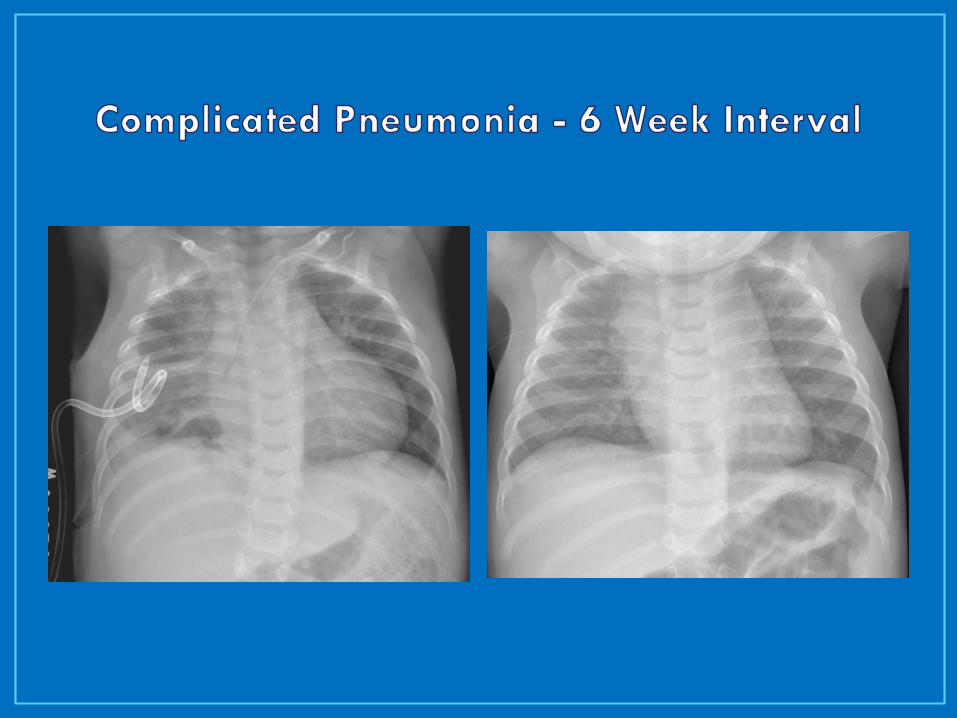
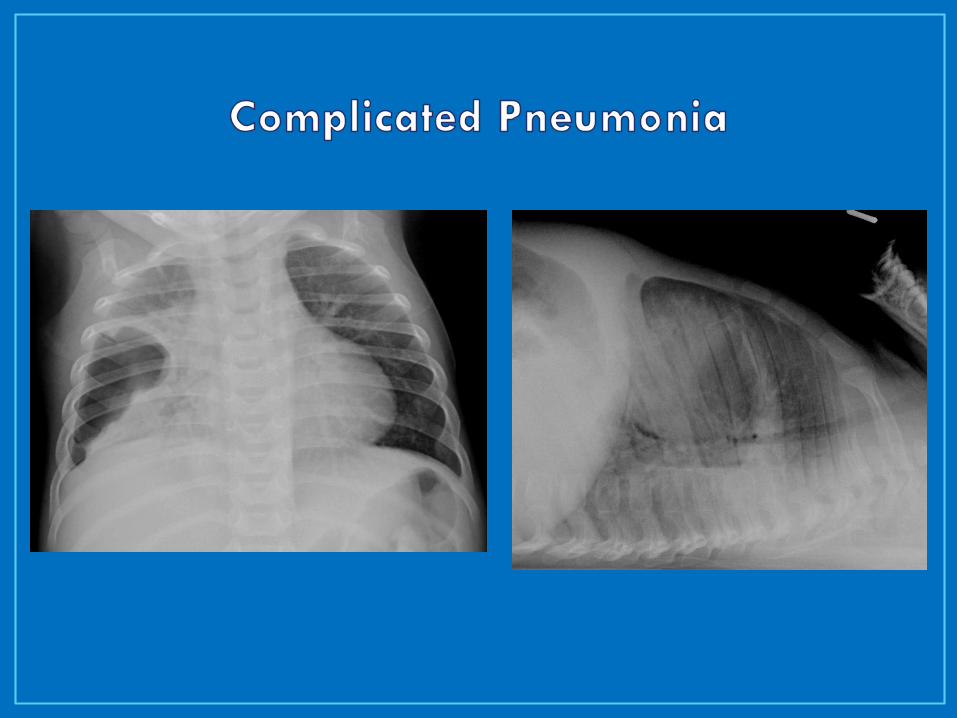
Complicated Pneumonia
Empyema:
7-10 days after CT out, clinically well, afebrile
Abscess/ Necrosis:
10-14 days after resolution – minimum
Some recommend 2-4 weeks
• Describe the difference between pleural effusion and empyema
• Explain the role of imaging in patients with complicated pneumonia
• Explain the options for management of pleural effusion and empyema
• Know how to evaluate for parenchymal complications of pneumonia