correlation of prenatal ultrasound diagnosis and pathologic findings in fetuses with trisomy 13
TRANSCRIPT

PRENATAL DIAGNOSISPrenat Diagn 2006; 26: 1262–1266.Published online 13 November 2006 in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pd.1604
Correlation of prenatal ultrasound diagnosis and pathologicfindings in fetuses with trisomy 13
Zsanett Szigeti, Zsolt Csapo, Jozsef G Joo, Barbara Pete, Zoltan Papp and Csaba Papp*First Department of Obstetrics and Gynecology, Semmelweis University Faculty of Medicine, Budapest, Hungary
Objectives This study was conducted to compare the prenatal ultrasound findings and postmortem pathologicfindings of fetuses with trisomy 13.
Methods Of 22 150 fetal chromosome analyses, 28 fetuses with trisomy 13 were diagnosed between 1990and 2004. Findings of second-trimester sonography and subsequent fetal autopsy were compared by organsystem, and their correlation was assigned to one of three categories based on the degree of agreement.
Results Of the total of 79 abnormalities that were found on autopsy, prenatal sonography showed 48(60.8%). The agreement was more than 75% of all abnormalities of these systems: central nervous system(CNS) (76.5%), facial abnormalities (76.5%), urinary system (81.8%) and fetal hydrops (100%), whereasthe sensitivity of sonography was lower in these organ systems: heart (53.3%), extremities (12.5%) andabdominal abnormalities (33.3%). In 39.2% of the cases, autopsy findings were not detected by sonography.These additional findings at autopsy involved mainly three organ systems: heart, face and extremities. Someultrasound findings (n = 17) were not verified at autopsy; most of them were quantitative markers (mildventriculomegaly, mild pyelectasis).
Conclusion Our results indicate that thorough sonographic examination of the fetal face (including ears)and extremities (including hands and feet) with an extensive use of fetal echocardiography may increase thesensitivity of prenatal sonography in detecting trisomy 13. Copyright 2006 John Wiley & Sons, Ltd.
KEY WORDS: fetal autopsy; prenatal sonography; trisomy 13
INTRODUCTION
Trisomy 13 is the third most common of the autosomaltrisomies that give rise to live-born neonates. The birth-prevalence of this trisomy is estimated at between 1in 5000 and 1 in 20 000 births, resulting in newbornswho die shortly after birth (Patau et al., 1960). Becausethe prognosis of the syndrome is very poor, earlyprenatal diagnosis is important. Since maternal serumscreening for trisomy 13 seems to be less promising thanscreening for trisomy 21, prenatal diagnosis of trisomy13 is usually accomplished by ultrasound. However, theaccuracy of ultrasonography in the prenatal diagnosis oftrisomy 13 has not been adequately studied.
In pregnancies ending up with termination, prenatalultrasound diagnosis may be confirmed or revised bypostmortem examination of aborted fetuses (Yeo et al.,2002). Thus, perinatal autopsy gives additional infor-mation to evaluate the accuracy of prenatal ultrasoundexamination (Johns et al., 2004). If the termination ofthe pregnancy occurs because of fetal aneuploidy, post-mortem autopsy may verify the findings of prenatalultrasound examination or reveal additional major orminor structural anomalies that are characteristic for theparticular aneuploidy (Isaksen et al., 2000a). That is,perinatal autopsy plays an important role in the quality
*Correspondence to: Csaba Papp, First Department of Obstetricsand Gynecology, Semmelweis University, Faculty of Medicine,H-1088 Budapest, Baross u. 27, Hungary.E-mail: [email protected]
control of the sonographic examination. It can also helpto describe major or minor anomalies of fetal aneu-ploidies that have a potential for screening at the mid-trimester scan (Keeling et al., 1997).
In a recent study, we reported our data about the mostfrequent sonographic abnormalities among fetuses withtrisomy 13 (Papp et al., 2006). The present study wasdesigned to evaluate the concordance of prenatal ultra-sound findings with the results of subsequent autopsyexamination in fetuses with trisomy 13.
MATERIAL AND METHODS
The genetic counseling database of the First Departmentof Obstetrics and Gynecology, Semmelweis UniversityFaculty of Medicine, was reviewed during this study.The study was approved by the Ethics Committee ofour institution. Cytogenetic records of fetuses were col-lected between 1990 and 2004, and karyotypically doc-umented trisomy 13 fetuses were analyzed. Singletonfetuses, which underwent prenatal sonography duringthe second trimester in our institution, made up thestudy population. Mothers were referred to our geneticcounselling department for different reasons: advancedmaternal age, family history of genetic problems in pre-vious pregnancies, ‘suspect’ ultrasound findings foundin other institutions and abnormal triple test results. Inthis respect, our study population represents a high-riskgroup of patients.
Copyright 2006 John Wiley & Sons, Ltd. Received: 18 August 2006Accepted: 5 October 2006
Published online: 13 November 2006

FETUSES WITH TRISOMY 13 1263
All sonographic examinations were performed bythree sonographers and were further evaluated by twoobstetricians with great experience in maternal-fetalmedicine. Two types of ultrasound equipment were usedfor the examinations: an ATL Ultramark 9 HDI 3000(Phillips Medical Systems, Bothell, WA) and a GEVoluson 730 (GE Medical Systems, Milwaukee, WI).The course of the examinations followed the guidelinesof the Hungarian Society of Ultrasound in Obstetricsand Gynecology, and routinely targeted basically allstructures of the fetus: the head (brain, face), theneck, thoracic cavity (four-chamber-view of the heart,cardiac outflow tracts), abdominal cavity, extremities,the spine, long bones and genitalia. Abnormalities ofeach organ were recorded. If a patient underwent morethan one sonographic examination, the results of thefirst examination alone were included in the analysis.The sonographic examinations were carried out beforeobtaining knowledge of the cytogenetic results of thefetuses to rule out any bias.
Cytogenetic evaluation of the fetuses was performedeither by amniocentesis, or chorionic villus sampling(CVS), followed by amniotic cell culture (in case ofamnio) or direct analysis method (in case of CVS) usingstandard techniques.
Each sonographic finding was classified as majorstructural anomaly or minor (‘soft’) sonographic marker.Major structural anomalies were defined as centralnervous system (CNS) anomalies, cardiac anomalies,abdominal anomalies, renal anomalies, limb anomalies,facial anomalies, hydrops and cystic hygroma. Amongminor anomalies, we paid special attention to the fol-lowing: nuchal fold thickness >6 mm, short femuror humerus (<10th percentile), pyelectasis (>4 mm),echogenic bowel, echogenic intracardiac focus, choroidplexus cyst. (Since echogenic bowel and EIF weredescribed as soft markers in the mid-1990s, we did notlook for them consistently in the first part of our study.)We also detected intrauterine growth restriction (if esti-mated fetal weight <10th percentile), amniotic fluidabnormalities (oligo- or polyhydramnios) and umbilicalcord abnormalities.
Therapeutic termination of pregnancy was performedfollowing proper genetic counselling. The couples optedfor termination in all cases.
All autopsies were performed by two pathologists whowere specialized in perinatal pathology. Standard proto-col for the autopsies was followed for each examination(Keeling, 1993). The results of the sonographic exam-inations were available to the pathologists prior to thepathologic examinations. Until autopsy was performed,the corpses were stored at low temperature (4 ◦C). Thetime that elapsed between abortion and autopsy was1–3 days. All cases underwent histologic examinationof the organs and the placenta.
The ultrasound and pathology reports were analyzedby organ systems, and the findings were compared. Thecorrelation was assigned to one of three categories: classA, full agreement between the findings on sonographyand autopsy; class B, autopsy findings not detected byultrasound (false-negative sonographic findings); class
C, ultrasound findings not confirmed at autopsy (false-positive sonographic findings).
RESULTS
During the time period of 1990–2004, we performed 22150 fetal karyotypings and found 514 (2.32%) chromo-some abnormalities. Among them, 28 trisomy 13 fetuseswere identified prenatally. All of the fetal aneuploidieswere diagnosed by amniocentesis (78.6%, n = 22) orCVS (2l.4%, n = 6) after sonographic examinations.
The mean maternal age of the patients was 32.4 years(range: 17–44 years) at the time of the sonographicexamination. The median gestational age at the timeof the sonogram was 19.5 weeks (13–25 weeks). Allfetuses were sonographycally examined before kary-otyping.
The couples opted for therapeutic termination ofpregnancy in all cases after genetic counseling. Themean gestational age at the time of the abortion was22 weeks (range 13–25 weeks). Terminations were donewith the method of dilatation and evacuation (D + E)in three cases, in which proper pathology evaluationof fetuses could not be performed (because of thefragmented specimens). We excluded these three casesfrom the study population.
Of the remaining 25 fetuses, all had 1 or more abnor-mal structural findings at postabortion pathologic exami-nation. There were five fetuses among them where majorstructural anomalies remained undetected by sonog-raphy (three cases of ventricular septal defects andtwo cases of polydactyly). Of the 79 separate majorstructural abnormalities detected on autopsy, sonogra-phy showed 48 (60.8%). We evaluated the sensitiv-ity of sonography in the identification of major orminor abnormalities found at autopsy by organ system.Among major defects (Table 1), the agreement was morethan 75% of all abnormalities of these systems: CNS(76.5%, 13/17), facial abnormalities (76.5%, 13/16), uri-nary system (81.8%, 9/11) and fetal hydrops (100%,2/2). Whereas, the sensitivity of sonography was lowerin these organ systems: cardiac system (53.3%, 8/15),extremities (12.5%, 2/16) and abdominal organs (33.3%,1/3). Additional findings at autopsy (‘false-negativeultrasound signs’) were not detected by sonography in39.2% and involved mainly three organ systems: heart(n = 6), face (including ear; n = 5), extremities (includ-ing hands and feet; n = 14). Of the 6 heart defects,3 small ventricular septal defects, 2 small atrial septaldefects and 1 hypoplastic left ventricle were missed bysonography; all 5 of the face defects were low-set ears;of the 14 abnormalities of the hands missed by sonogra-phy, 10 cases of polydactyly and 4 cases of overlappingfingers were diagnosed at the pathologic examination.Of the additional findings on autopsy, 5 were major dis-agreements: 2 cases of small omphalocele, 2 cases ofmild renal cystic anomaly and 1 isolated spina bifida.
Some ultrasound findings (n = 17) were not con-firmed at autopsy in our series (‘false-positive ultra-sound signs’). Most of them were ‘quantitative’ markers:
Copyright 2006 John Wiley & Sons, Ltd. Prenat Diagn 2006; 26: 1262–1266.DOI: 10.1002/pd
1264 Z. SZIGETI ET AL.
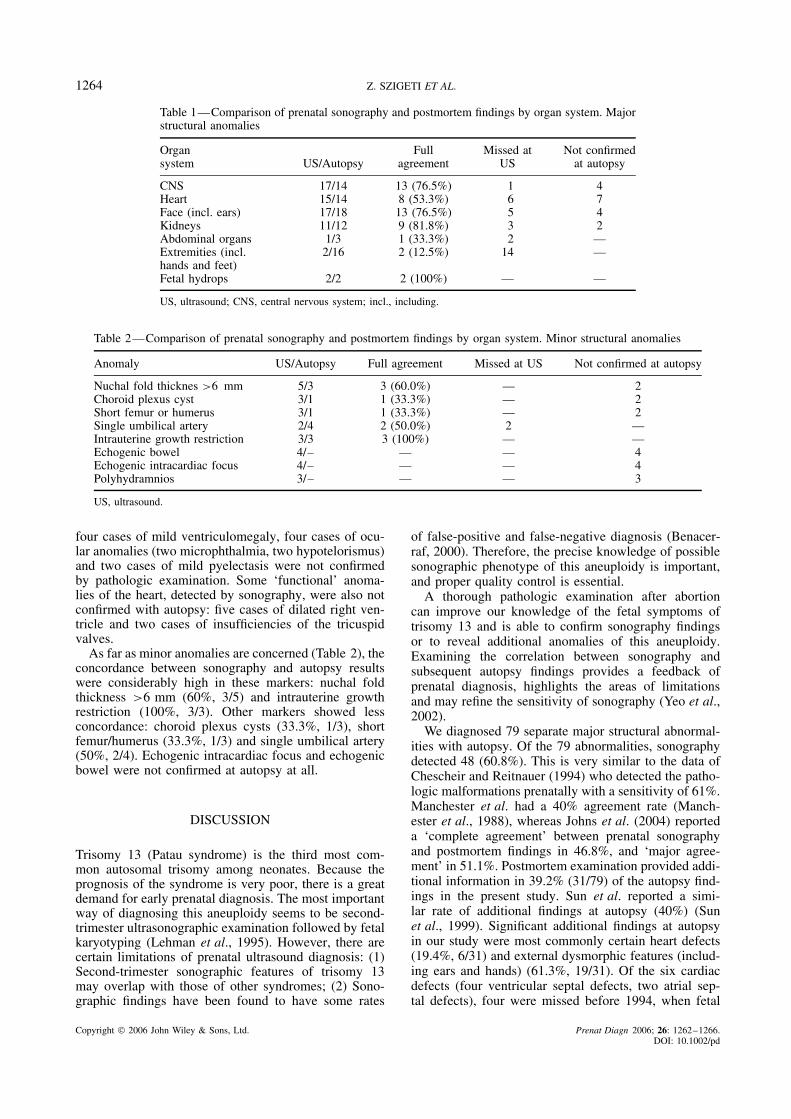
Table 1—Comparison of prenatal sonography and postmortem findings by organ system. Majorstructural anomalies
Organsystem US/Autopsy
Fullagreement
Missed atUS
Not confirmedat autopsy
CNS 17/14 13 (76.5%) 1 4Heart 15/14 8 (53.3%) 6 7Face (incl. ears) 17/18 13 (76.5%) 5 4Kidneys 11/12 9 (81.8%) 3 2Abdominal organs 1/3 1 (33.3%) 2 —Extremities (incl.hands and feet)
2/16 2 (12.5%) 14 —
Fetal hydrops 2/2 2 (100%) — —
US, ultrasound; CNS, central nervous system; incl., including.
Table 2—Comparison of prenatal sonography and postmortem findings by organ system. Minor structural anomalies
Anomaly US/Autopsy Full agreement Missed at US Not confirmed at autopsy
Nuchal fold thicknes >6 mm 5/3 3 (60.0%) — 2Choroid plexus cyst 3/1 1 (33.3%) — 2Short femur or humerus 3/1 1 (33.3%) — 2Single umbilical artery 2/4 2 (50.0%) 2 —Intrauterine growth restriction 3/3 3 (100%) — —Echogenic bowel 4/– — — 4Echogenic intracardiac focus 4/– — — 4Polyhydramnios 3/– — — 3
US, ultrasound.
four cases of mild ventriculomegaly, four cases of ocu-lar anomalies (two microphthalmia, two hypotelorismus)and two cases of mild pyelectasis were not confirmedby pathologic examination. Some ‘functional’ anoma-lies of the heart, detected by sonography, were also notconfirmed with autopsy: five cases of dilated right ven-tricle and two cases of insufficiencies of the tricuspidvalves.
As far as minor anomalies are concerned (Table 2), theconcordance between sonography and autopsy resultswere considerably high in these markers: nuchal foldthickness >6 mm (60%, 3/5) and intrauterine growthrestriction (100%, 3/3). Other markers showed lessconcordance: choroid plexus cysts (33.3%, 1/3), shortfemur/humerus (33.3%, 1/3) and single umbilical artery(50%, 2/4). Echogenic intracardiac focus and echogenicbowel were not confirmed at autopsy at all.
DISCUSSION
Trisomy 13 (Patau syndrome) is the third most com-mon autosomal trisomy among neonates. Because theprognosis of the syndrome is very poor, there is a greatdemand for early prenatal diagnosis. The most importantway of diagnosing this aneuploidy seems to be second-trimester ultrasonographic examination followed by fetalkaryotyping (Lehman et al., 1995). However, there arecertain limitations of prenatal ultrasound diagnosis: (1)Second-trimester sonographic features of trisomy 13may overlap with those of other syndromes; (2) Sono-graphic findings have been found to have some rates
of false-positive and false-negative diagnosis (Benacer-raf, 2000). Therefore, the precise knowledge of possiblesonographic phenotype of this aneuploidy is important,and proper quality control is essential.
A thorough pathologic examination after abortioncan improve our knowledge of the fetal symptoms oftrisomy 13 and is able to confirm sonography findingsor to reveal additional anomalies of this aneuploidy.Examining the correlation between sonography andsubsequent autopsy findings provides a feedback ofprenatal diagnosis, highlights the areas of limitationsand may refine the sensitivity of sonography (Yeo et al.,2002).
We diagnosed 79 separate major structural abnormal-ities with autopsy. Of the 79 abnormalities, sonographydetected 48 (60.8%). This is very similar to the data ofChescheir and Reitnauer (1994) who detected the patho-logic malformations prenatally with a sensitivity of 61%.Manchester et al. had a 40% agreement rate (Manch-ester et al., 1988), whereas Johns et al. (2004) reporteda ‘complete agreement’ between prenatal sonographyand postmortem findings in 46.8%, and ‘major agree-ment’ in 51.1%. Postmortem examination provided addi-tional information in 39.2% (31/79) of the autopsy find-ings in the present study. Sun et al. reported a simi-lar rate of additional findings at autopsy (40%) (Sunet al., 1999). Significant additional findings at autopsyin our study were most commonly certain heart defects(19.4%, 6/31) and external dysmorphic features (includ-ing ears and hands) (61.3%, 19/31). Of the six cardiacdefects (four ventricular septal defects, two atrial sep-tal defects), four were missed before 1994, when fetal
Copyright 2006 John Wiley & Sons, Ltd. Prenat Diagn 2006; 26: 1262–1266.DOI: 10.1002/pd

FETUSES WITH TRISOMY 13 1265
echocardiography was not yet part of our prenatal diag-nostic services. The high number of missed externaldysmorphoric features deserves attention. The detectionrate of sonography could be improved with the use ofthree-dimensional ultrasound, because it provides betterinformation regarding the severity and extent of theseabnormalities (Chang et al., 2002). However, it shouldbe acknowledged that the gestational age at sonographyplays a major role in its accuracy. Some fetal abnor-malities can be easily overlooked in the early secondtrimester (e.g. face anomalies, cardiac defects or anoma-lies of the hands).
In our series, there was full agreement between find-ings from sonography and perinatal autopsy in 76.5%of all CNS abnormalities. This concurs with the dataof Caroll et al. (2000) who found a 77% concordancebetween sonography and autopsy findings regardingbrain defects. We had four cases in which sonogra-phy detected mild ventriculomegaly (the posterior hornmeasured 10–15 mm) that was not verified by autopsy.None of them was an isolated finding. It is generallyaccepted that pathologic evaluation of the brain is some-times hampered by autolytic processes. (Caroll et al.,2000). Not considering these cases of ventriculomegalyas true false-positives, the concordance between sonog-raphy and autopsy findings increase to 92.9% withregard to CNS anomalies. This is similar to the dataof Isaksen et al. who reported a 94% concordance rate(Isaksen et al., 1998).
We identified 80% of renal abnormalities found atautopsy on sonography. This is higher than what Sunet al. (1999) reported previously (64%), whereas oth-ers had higher correlations between sonographic andautopsy findings (87%) (Isaksen et al., 2000b). Of thethree additional findings found at autopsy, there weretwo cases of horseshoe kidneys. This anomaly is some-times difficult to detect with two-dimensional ultra-sonography (Daneman and Alton, 1991).
We found complete agreement in 53.3% of all cardiacanomalies. This is higher than what Sun et al. found(27%) (12), but lower that what Isaksen et al. reported(82%) (Isaksen et al., 1999). One possible explanationof our relatively low concordance is that we did nothave fetal echocardiography in our institution during thefirst years of the study period (before 1994). There werethree cases of small ventricular septal defects and twocases of small atrial septal defects among the additionalfindings revealed by autopsy examination. We wouldnot call these discrepancies ‘sonographic error’, sincethese defects are difficult to diagnose by sonography(Copel et al., 1987) and they do not have strong clinicalrelevance, since most of the small ventricular septaldefects spontaneously close after birth (Whiteman andReece, 1994; Kidd et al., 1993). However, these cardiacanomalies may indicate associated disorders such aschromosomal defects (Isaksen et al., 1999).
Full agreement was revealed between sonography andautopsy findings in 76.5% of the facial abnormalities.All midline defects were detected by sonography in ourseries, whereas five ear anomalies were missed. The highfrequency of facial anomalies at autopsy underlines the
importance of this marker in sonographic screening oftrisomy 13.
As far as soft markers are concerned, the rate offull agreement between ultrasonographic and autopsyfindings was more than 50% in the cases of thick-ened nuchal fold (60%, 3/5) and intrauterine growthrestriction (100%, 3/3). Although major structural mark-ers have obvious significance in diagnosing trisomy 13,the importance of soft markers is not negligible in thisrespect.
We found that fetal pathologic examination followingtermination of pregnancy has limited value regardingtwo soft markers: echogenic bowel cases and caseswith echogenic intracardial foci were not confirmed atautopsy.
There is an interesting aspect of comparing sono-graphic and pathologic findings: sonographic signs thatwere not confirmed at autopsy (‘false-positive sono-graphic findings’). Of the 17 such signs, the majority wasbased on the measurements of different organs (‘quan-titative signs’): mild ventriulomegaly (4 cases), mildpyelectasis (2 cases), micropthalmus (2 cases), hypoth-elorismus (2 cases). Regarding the heart, false-positivesonographic findings were represented more as ‘func-tional anomalies’ instead of real malformations: dilatedventricles (5 cases) and insufficiency of the tricuspidvalves (2 cases).
Examining the correlation between sonography andpathologic findings may reveal the possible limitationsof the diagnostic accuracy of prenatal ultrasound exami-nation and indicates possible directions of further devel-opment in sonographic screening for trisomy 13. Ourdata show that thorough sonographic examination ofthe fetal face (including ears) and extremities (includinghands and feet) with an extensive use of fetal echocar-diography may increase the sensitivity of prenatal sonog-raphy in detecting trisomy 13.
REFERENCES
Benacerraf BR. 2000. Should sonographic screening for fetal downsyndrome be applied to low risk women? Ultrasound ObstetGynecol 15: 451–455.
Caroll SGM, Porter H, Abdel-Fattah S, Kyle PM, Soothill PW. 2000.Correlation of prenatal ultrasound diagnosis and pathologic findingsin fetal brain abnormalities. Ultrasound Obstet Gynecol 16: 49–153.
Chang LW, Chang FM, Chang CH, Yu CH, Cheng YC, Chen HY.2002. Prenatal diagnosis of fetal multicystic dysplastic kidney withtwo-dimensional and three-dimensional ultrasound. Ultrasound MedBiol 28: 853–858.
Chescheir NC, Reitnauer PJ. 1994. A comparative study of prenataldiagnosis and perinatal autopsy. J Ultrasound Med 13: 451–456.
Copel JA, Pilu G, Green J, Hobbins JC, Kleinmann CS. 1987. Fetalechocardiographic screening for congenital heart disease: theimportance of the four-chamber view. Am J Obstet Gynecol 157:648–655.
Daneman A, Alton DJ. 1991. Radiographic manifestations of renalanomalies. Radiol Clin North Am 29: 351–363.
Isaksen CV, Eik-Nes SH, Blaas HG, Torp SH. 1998. Comparison ofprenatal ultrasound and postmortem findings in fetuses and infantswith central nervous system anomalies. Ultrasound Obstet Gynecol11: 246–253.
Isaksen CV, Eik-Nes SH, Blaas HG, Tegnander E, Torp SH. 1999.Comparison of prenatal ultrasound and postmortem findings in
Copyright 2006 John Wiley & Sons, Ltd. Prenat Diagn 2006; 26: 1262–1266.DOI: 10.1002/pd
1266 Z. SZIGETI ET AL.
fetuses and infants with congenital heart defects. Ultrasound ObstetGynecol 13: 117–126.
Isaksen CV, Eik-Nes SH, Blaas HG, Torp SH. 2000b. Fetuses andinfants with congenital urinary system anomalies: correlationbetween prenatal ultrasound and postmortem findings. UltrasoundObstet Gynecol 15: 177–185.
Isaksen CV, Eik-Nes SH, Blaas HG, Torp SH, Van Der Hagen CB,Ormerod E. 2000a. A correlative study of prenatal ultrasound andpost-mortem findings in fetuses and infants with an abnormalkaryotype. Ultrasound Obstet Gynecol 16: 37–45.
Johns N, Al-Salti W, Cox P, Kilby MD. 2004. A comparative studyof prenatal ultrasound findings and post-mortem examination in atertiary referral centre. Prenat Diagn 24: 339–346.
Keeling JW. 1993. The perinatal autopsy. In Fetal and NeonatalPathology, Keeling JW (ed.). Springer-Verlag: London; 465–469.
Keeling JW, Hansen BF, Kjaer I. 1997. Pattern of malformations inthe axial skeleton in human trisomy 21 fetuses. Am J Med Genet68: 466–471.
Kidd L, Driscoll DJ, Gersony WM, et al. 1993. Second naturalhistory study of congenital heart defects. Circulation 87(Suppl. 1):38–51.
Lehman CD, Nyberg DA, Winter TC III, Kapur RP, Resta RG,Luthy DA. 1995. Trisomy 13 syndrome: prenatal US findings ina review of 33 cases. Radiology 194: 217–222.
Manchester DK, Pretorius DH, Avery C. 1988. Accuracy of ultra-sound diagnoses in pregnancies complicated by suspected fetalanomalies. Prenat Diagn 8: 109–117.
Papp Cs, Beke A, Ban Z, Szigeti Zs, Toth-Pal E, Papp Z. 2006.Prenatal diagnosis of trisomy 13: analysis of 28 cases. J UltrasoundMed 25: 429–435.
Patau K, Smith DW, Therman E, Inborn SL, Wagner HP. 1960.Multiple congenital anomaly caused by an extra chromosome.Lancet 1: 790–793.
Sun CJ, Grumbach K, DeCosta DT, Meyers CM, Dungan JS. 1999.Correlation of prenatal ultrasound diagnosis and pathologic findingsin fetal anomalies. Pediatr Dev Pathol 2: 131–142.
Whiteman VE, Reece EA. 1994. Prenatal diagnosis of majorcongenital malformations. Curr Opin Obstet Gynecol 6: 459–467.
Yeo L, Guzman ER, Shen-Schwartz S, Walters C, Vintzileos AM.2002. Value of a complete sonographic survey in detecting fetalabnormalities. Correlation with perinatal autopsy. J Ultrasound Med21: 501–510.
Copyright 2006 John Wiley & Sons, Ltd. Prenat Diagn 2006; 26: 1262–1266.DOI: 10.1002/pd