correlation between serum electrolytes and fasting glucose and hb1ac in saudi diabetic patients
TRANSCRIPT

Correlation between Serum Electrolytes and FastingGlucose and Hb1Ac in Saudi Diabetic Patients
Khalid Al-Rubeaan & Khalid Siddiqui & Khaled Abu Risheh & Roderick Hamsirani &Abdulmajeed Alzekri & Abdulrahman Alaseem & Saleh M. Saleh & Ziad Al-Yami &Ali Al-Ghamdi & Khalid Alayed
Received: 4 January 2011 /Accepted: 5 July 2011 /Published online: 5 August 2011# Springer Science+Business Media, LLC 2011
Abstract In subjects with impaired insulin action, alterations of the serum sodium andpotassium concentrations have been reported. The resulting cationic imbalance, along withthe osmotic effect of the elevated sugar levels, could influence the course of diabetesmellitus management. Therefore, this study was conducted to compare the fasting bloodglucose and HbA1c levels with those of the serum electrolytes. Blood samples werecollected for assessment of HbA1c, fasting blood glucose (FBS), and electrolytes usingdifferent automated methods. A significant association between the serum sodium and FBSlevels among types 1 and 2 insulin-treated patients, and type 2 oral agent patients wasobserved. A total of 138 diabetic subjects were randomly selected from any gender agedbetween 25 and 65 years at the University Diabetes Center, King Saud University, RiyadhKSA. The subjects were classified into types 1 or 2 DM using ADA criteria. Blood sampleswere collected for assessment of HbA1c, FBS, and electrolytes using different automatedmethods. It showed a significant association between serum sodium, FBS among type 1,type 2 insulin treated, and type 2 oral agent groups. However, the association of sodiumand HbA1c was insignificant when analyzed individually. A statistically significantassociation (P<0.001) was observed between the levels of serum sodium and the fastingblood glucose levels. This study demonstrated significant reduction in serum sodiumlevel among types 1 or 2 diabetic patients especially among insulin-treated patients. Nosignificant association was demonstrated by serum potassium with FBS and degree ofdiabetes control.
Biol Trace Elem Res (2011) 144:463–468DOI 10.1007/s12011-011-9144-4
K. Al-Rubeaan (*) : K. Siddiqui :K. Abu Risheh : R. Hamsirani : A. Alzekri :A. Alaseem :S. M. Saleh : Z. Al-Yami : A. Al-Ghamdi : K. AlayedUniversity Diabetes Center, King Abdul Aziz University Hospital, King Saud University,P.O. Box 18397, Riyadh 11415, Saudi Arabiae-mail: [email protected]
K. Al-Rubeaan : K. Siddiqui : R. HamsiraniStrategic Center for Diabetes Research, Riyadh, Saudi Arabia

Keywords Hyponatremia . Hypokalemia . Electrolyte disturbances . Type1 diabetes . Type 2diabetes . HbA1c
Introduction
Diabetes mellitus (DM) refers to a group of metabolic disorders that share the characteristicof hyperglycemia. Complex interactions of genetics and environmental factors play roles inthe etiopathology of this entity. Deregulations resulting from these interactions causesecondary pathophysiologic changes in multiple organ systems [1]. Hyperglycemia sets theinternal environment for osmotic diuresis while causing a dilutional effect on electrolyteconcentrations [2]. The osmotic effect of glucose results in decreased circulating bloodvolume and fluid shift from the intracellular spaces causing cellular dehydration. Insulin hasbeen shown to decrease extracellular potassium concentration as well likely throughactivation of Na-K-ATPase [3]. The synergistic action of cationic imbalance and osmoticeffect of glucose could very well impact the course of diabetes mellitus [4]. However,deficiency of insulin or resistance to insulin action may contribute to the development ofelectrolyte abnormalities. Considering all these factors, the altered distribution of sodiumand potassium between the intracellular and extracellular compartments may affect thecourse of diabetes mellitus as well as its management [5].
Studies on electrolyte imbalances in association with diabetes have reported an inverserelationship between sodium and potassium levels in diabetic coma [6]. This associationmay be based on the movement of electrolytes between intra and extracellular spacedependent on impaired insulin action [7]. A significant direct association was reportedbetween hyperkalemia and hyperglycemia in Saudi diabetic subjects. It was observed thatelderly uncontrolled diabetics are at a higher risk of hyperkalemia. Until now, no studieshave been performed to correlate serum electrolyte concentrations with fasting bloodglucose and HbA1c levels. This study aims to identify the relationship of serum electrolytessodium and potassium with fasting blood glucose and HbA1c levels in types 1 and 2diabetic subjects treated with insulin, oral hypoglycemic agents.
Methodology
This cross-sectional descriptive randomized clinical study has selected 138 diabetic patientsfrom outpatient department at University Diabetes Center, King Abdul Aziz UniversityHospital at King Saud University during the period of January 2008 to January 2009. Patientswere selected randomly from any gender aged between 25 and 65 (mean 46.14±15.4)yearsboth types 1 or 2 diabetic patients. The patients were classified into types 1 and 2 diabetesmellitus using the 1997 American Diabetes Association criteria which were adopted by theWorld Health Organization [2]. Patients with kidney or coronary artery diseases were excludedand any patients using diuretics and antihypertensive medications were also excluded fromthe study. There were 31 type 1 diabetic patients and 107 type 2 with a mean duration of 12.1±6.7 years, out of which 74 were using oral hypoglycemic agents and 33 were using insulin.
On at least four different occasions HbA1c, fasting blood sugar, sodium, and potassiumwere assessed and the measurements were taken after every 3 months followed by thecalculation of mean value for each parameter. Blood samples were collected after 10 h offasting by sampling the cubital vein. For fasting blood glucose, serum was separated from5 ml blood samples in plain tubes and was sent to the laboratory using Glucose Oxidase
464 Al Rubeaan et al.
Test (Hitachi 912, USA). Potassium and sodium level was estimated using ISE IndirectMethod (Hitachi 912, USA). Five milliliter fresh blood samples in ethylenediaminetetra-acetic acid tubes were sent to the laboratory for HbA1c assessment using Ion ExchangeHPLC Variant II principle (Cobas Integra system 400, Roche Diagnostics, USA). HbA1cwas expressed in percentage while fasting blood sugar, sodium, and potassium wereexpressed in mill mole per liter (mM/L).
Statistical Analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS 12.0, Chicago,IL, USA). Descriptive statistics were applied for demographic data (i.e., frequency,percentage, mean, and standard deviation). Testing hypothesis was performed usingregression analysis. P values less than 0.005 were considered as of statistical significance.Correlation coefficient was used to measure the degree to which two variables are linearlyrelated and coefficient of determination (R2) was used to measure the relative variation thatdescribes the variation in one value occurring in proportion to variations of another value.
Results
In this study, a total of 138 subjects were recruited with a mean age of 46.1±15.5 years anddiabetes duration mean of 12.1±6.7 years duration. Gender distribution revealed 62(44.9%) males and 76 (55.1%) females, 31 (22.5%) subjects were type 1 and 107 (77.5%)were type 2 diabetic patients. The use of oral hypoglycemic agent was found in 74 subjects(53.6%) and insulin therapy was in 64 (46.4%) was shown in Tables 1 and 2. The meanvalue for fasting plasma glucose was 10.8±2.9 mM/L, sodium was 138.1±1.8 mM/L, andpotassium 4.1±0.3 mM/L for the whole studied group.
In Table 3, the fasting serum glucose and HbA1c levels in the different groups (types 1and 2 diabetics) are given in relation to their treatment methods (i.e., insulin vs. oralhypoglycemic agent). Both the mean fasting blood glucose and HbA1c values areexpressed along with the R2 and the correlation coefficients. The P values were calculatedfor each parameter in each type and treatment group. The association between sodium asthe outcome variable and the FBS as independent variable calculated by R2 revealedsignificant association in type 1 diabetic subject (P<0.00), and type 2 insulin treated (P<
Values (%)
Sex
Male 62 (44.9)
Female 76 (55.1)
DM
Type 1 31 (22.5)
Type 2 107 (77.5)
Treatment
Oral 74 (53.6)
Insulin 64 (46.4)
Table 1 Comparative averagevalues related with 138 Saudidiabetic patients with respect tosex type of diabetes andtreatment given
Correlation Study between Serum Electrolyte 465

0.008), and type 2 oral agent group (P<0.00). P value was also strongly significant in the totalgroup (P<0.00) when looking at serum sodium with both fasting blood sugar and HbA1c.
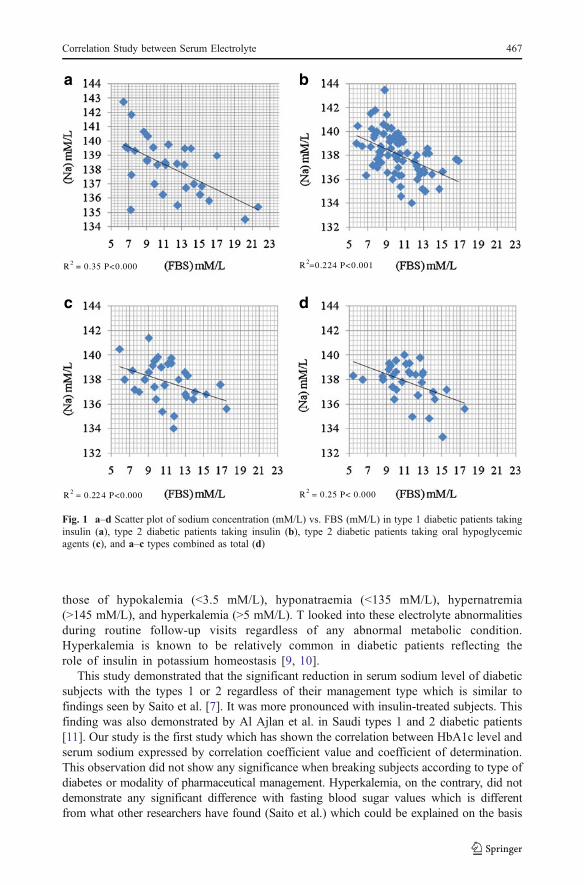
This was not the case when looking at potassium where it was insignificant for type 1,type 2 insulin therapy groups, and type 2 oral therapy groups with a P value of 0.15, 0.06,and 0.67 respectively. Also, the total group did not show significant association betweenpotassium and fasting blood sugar (P=0.32) and HbA1c (P=0.28). Association betweensodium and HbA1c was insignificant in the three groups individually with P values of 0.08,0.07, and 0.12, respectively, but it was significant when taken as a whole with a P value of0.01. Potassium association with HbA1c values was insignificant in all the three groupswith a P value 0.92, 0.73, 0.50, respectively, and the total group did not show a significantrelation as well (P=0.28). Figure 1a–d is expressing the same findings by using fastingblood glucose mean regression values and expressing R2 which shows the significantreduction in plasma sodium level with increase fasting blood glucose values in type 1, type2 oral therapy, type 2 insulin therapy, and total subjects.
Discussion
To our knowledge, no studies have been performed to investigate the relation between twoelectrolytes (sodium and potassium) with FBS and HbA1c in different diabetic groups. Ithas been already known that electrolyte imbalances are the consequences of hyperglycemia,hyperosmolality, and acidosis [8]. The biochemical parameters noted in this study were
Table 3 Statistical correlation and significance levels on Na and K with FBS and HbA1c levels for threedifferent groups of diabetic subjects (type 1 diabetic subjects taking insulin, type 2 diabetic subjects takinginsulin, type 2 diabetic subjects taking oral hypoglycemic agents and all 138 subjects combined as total)
Parameters Type 1 Type 2 Total
Insulin Insulin Oral
CC R2 P CC R2 P CC R2 P CC R2 P
FBS Na 0.592 0.35 0.00* 0.473 0.224 0.01* 0.473 0.224 0.00* 0.497 0.25 0.00*
K 0.267 0.07 0.15 0.326 0.106 0.06 0.020 0.000 0.67 0.085 0.007 0.32
HbA1c Na 0.319 0.10 0.08 0.320 0.103 0.07 0.123 0.033 0.12 0.224 0.05 0.008*
K 0.020 0.00 0.92 0.012 0.004 0.73 0.167 0.006 0.50 0.093 0.009 0.28
cc Correlation coefficient, R2 coefficient of regression
*P values <0.05 considered significant
Values
Age (year) 46.1±15.5
Duration (years) 12.1±6.7
HbA1c (%) 9.5±1.5
FBS (mM/L) 10.8±2.9
Na+ (mM/L) 138.1±1.8
K+ (mM/L) 4.1±0.3
Table 2 Average values age,duration of disease, levels ofHbA1c, FBS, and Na andK concentrations obtained from138 Saudi diabetic subjects
466 Al Rubeaan et al.
those of hypokalemia (<3.5 mM/L), hyponatraemia (<135 mM/L), hypernatremia(>145 mM/L), and hyperkalemia (>5 mM/L). T looked into these electrolyte abnormalitiesduring routine follow-up visits regardless of any abnormal metabolic condition.Hyperkalemia is known to be relatively common in diabetic patients reflecting therole of insulin in potassium homeostasis [9, 10].
This study demonstrated that the significant reduction in serum sodium level of diabeticsubjects with the types 1 or 2 regardless of their management type which is similar tofindings seen by Saito et al. [7]. It was more pronounced with insulin-treated subjects. Thisfinding was also demonstrated by Al Ajlan et al. in Saudi types 1 and 2 diabetic patients[11]. Our study is the first study which has shown the correlation between HbA1c level andserum sodium expressed by correlation coefficient value and coefficient of determination.This observation did not show any significance when breaking subjects according to type ofdiabetes or modality of pharmaceutical management. Hyperkalemia, on the contrary, did notdemonstrate any significant difference with fasting blood sugar values which is differentfrom what other researchers have found (Saito et al.) which could be explained on the basis
R2 = 0.35 P<0.000
R2 = 0.22 4 P<0.000 R2 = 0.25 P< 0.000
R2=0.224 P<0.001
a b
c d
Fig. 1 a–d Scatter plot of sodium concentration (mM/L) vs. FBS (mM/L) in type 1 diabetic patients takinginsulin (a), type 2 diabetic patients taking insulin (b), type 2 diabetic patients taking oral hypoglycemicagents (c), and a–c types combined as total (d)
Correlation Study between Serum Electrolyte 467

of the subject’s number and degree of control since our subjects mean HbA1c is 9.5±1.5 vs. 9.4±0.2 for the other study [7]. Age could be a factor for this difference sinceour subjects mean age was 46.1±15.5 while it was 53.5±17.5 from the other study.Age has been found to be a confounding factor for hyperkalemia as demonstrated[12]. Hypokalemia or hyperkalemia was not found to be associated with degree ofdiabetes control as represented from our data regardless of diabetes type or managementmodality [13].
Conclusion
This study demonstrated significant reduction in serum sodium level among types 1 or 2diabetic patients especially among insulin-treated patients. Serum potassium demonstratedno significant association with FBS and degree of diabetes control.
References
1. King H, Rewers M (1993) Global estimates for prevalence of diabetes mellitus and impaired glucosetolerance in adults. WHO Ad Hoc Diabetes Reporting Group. Diabetes Care 16:157–177
2. Alberti KG, Zimmet PZ (1998) Definition diagnosis and classification of diabetes mellitus and itscomplications. Part 1: diagnosis and classification of diabetes mellitus, provisional report of a WHOConsultation. Diabet Med 15:539–553
3. Wannamethee G, Whincup PH, Shaper AG et al (1994) Serum sodium concentration and risk of stroke inmiddle-aged males. J Hypertens 12(8):971–979
4. Rao GM (1992) Serum electrolytes and osmolality in diabetes mellitus. Indian J Med Sci 46(10):301–303
5. Toledo JD, Modesto V, Peinador M et al (2009) Sodium concentration in rehydration fluids for childrenwith ketoacidotic diabetes: effect on serum sodium concentration. J Pediatric 154(6):895–900
6. Rohrscheib M, Tzamaloukas AH, Ing TS et al (2005) Serum potassium concentration in hyperglycemiaof chronic dialysis. Adv Perit Dial 21:102–105
7. Saito T, Ishikawa S, Higashiyama M et al (1999) Inverse distribution of serum sodium and potassium inuncontrolled in patients with diabetes mellitus. Endocr J 46(1):75–80
8. Yawar A, Jabbar A, Haque NU et al (2008) Hyponatraemia: etiology, management and outcome. J CollPhysicians Surg Pak 18(8):467–471
9. Shahid SM, Mahboob T (2008) Electrolytes and NA (+)-K (+)-ATPase: potential risk factors for thedevelopment of diabetic nephropathy. Pak J Pharm Sci 21(2):172–179
10. Shahid SM, Rafique R, Mahboob T (2005) Electrolytes and sodium transport mechanism in diabetesmellitus. Pak J Pharm Sci 18(2):6–10
11. Al Ajlan AR (2007) Incidence of hyperkalemia in patients of type 1 and type 2 diabetes mellitus in SaudiArabia. MEJFM 5(3):27–29
12. Ogbera AO, Awobusuyi J, Unachukwu C et al (2009) Clinical features, predictive factors and outcome ofhyperglycaemic emergencies in a developing country. BMC Endocr Disord 9:9
13. Rodriguez-Sorian J (1995) Potassium homeostasis and its disturbances in children. Pedia Nephrol 9(3):364–374
468 Al Rubeaan et al.