copyright © 2010 pearson education, inc. blood tests
TRANSCRIPT

Copyright © 2010 Pearson Education, Inc.
Blood Tests

Copyright © 2010 Pearson Education, Inc.
Diagnostic Blood Tests
• Hematocrit
• Blood glucose tests
• Microscopic examination reveals variations in size and shape of RBCs, indications of anemias
• Differential WBC count
• Prothrombin time and platelet counts assess hemostasis
• SMAC, a blood chemistry profile
• Complete blood count (CBC)

Copyright © 2010 Pearson Education, Inc.
Regulation of Blood Pressure and Heart Rate
Autoregulation (meaning that the tissue or organ regulates blood pressure and flow locally)

Copyright © 2010 Pearson Education, Inc.
Autoregulation
• Automatic adjustment of blood flow to each tissue in proportion to its requirements at any given point in time
• Is controlled intrinsically by modifying the diameter of local arterioles feeding the capillaries
• Is independent of MAP, which is controlled as needed to maintain constant pressure
• Two types of autoregulation
1.Metabolic
2.Myogenic

Copyright © 2010 Pearson Education, Inc. Figure 19.15
Metaboliccontrols
pH Sympathetic
Receptors
ReceptorsEpinephrine,norepinephrine
Angiotensin II
Antidiuretichormone (ADH)
Atrialnatriureticpeptide (ANP)
Dilates
Constricts
Prostaglandins
Adenosine
Nitric oxide
Endothelins
Stretch
O2
CO2
K+
Amounts of:
Amounts of:
Nerves
Hormones
Myogeniccontrols
Intrinsic mechanisms(autoregulation)
• Distribute blood flow to individual organs and tissues as needed
Extrinsic mechanisms
• Maintain mean arterial pressure (MAP)• Redistribute blood during exercise and thermoregulation

Copyright © 2010 Pearson Education, Inc.
Long-Term Autoregulation
• Angiogenesis
• Occurs when short-term autoregulation cannot meet tissue nutrient requirements
• The number of vessels to a region increases and existing vessels enlarge
• Common in the heart when a coronary vessel is occluded, or throughout the body in people in high-altitude areas

Copyright © 2010 Pearson Education, Inc.

Copyright © 2010 Pearson Education, Inc.
Reminder: repeated from previous set of slide, purpose of blood is -
• Diffusion of
• O2 and nutrients from the blood to tissues
• CO2 and metabolic wastes from tissues to the blood
• Lipid-soluble molecules diffuse directly through endothelial membranes
• Water-soluble solutes pass through clefts and fenestrations
• Larger molecules, such as proteins, are actively transported in pinocytotic vesicles or caveolae

Copyright © 2010 Pearson Education, Inc.
Fluid Movements: Bulk Flow
• Extremely important in determining relative fluid volumes in the blood and interstitial space
• Direction and amount of fluid flow depends on two opposing forces: hydrostatic and colloid osmotic pressures

Copyright © 2010 Pearson Education, Inc.
Hydrostatic Pressures
• Capillary hydrostatic pressure (HPc) (capillary blood pressure)
• Tends to force fluids through the capillary walls
• Is greater at the arterial end (35 mm Hg) of a bed than at the venule end (17 mm Hg)
• Interstitial fluid hydrostatic pressure (HPif)
• Usually assumed to be zero because of lymphatic vessels

Copyright © 2010 Pearson Education, Inc.
Colloid Osmotic Pressures
• Capillary colloid osmotic pressure (oncotic pressure) (OPc)
• Created by nondiffusible plasma proteins, which draw water toward themselves
• ~26 mm Hg
• Interstitial fluid osmotic pressure (OPif)
• Low (~1 mm Hg) due to low protein content

Copyright © 2010 Pearson Education, Inc.
Net Filtration Pressure (NFP)
• NFP—comprises all the forces acting on a capillary bed
• NFP = (HPc—HPif)—(OPc—OPif)
• At the arterial end of a bed, hydrostatic forces dominate
• At the venous end, osmotic forces dominate
• Excess fluid is returned to the blood via the lymphatic system
Copyright © 2010 Pearson Education, Inc. Figure 19.17
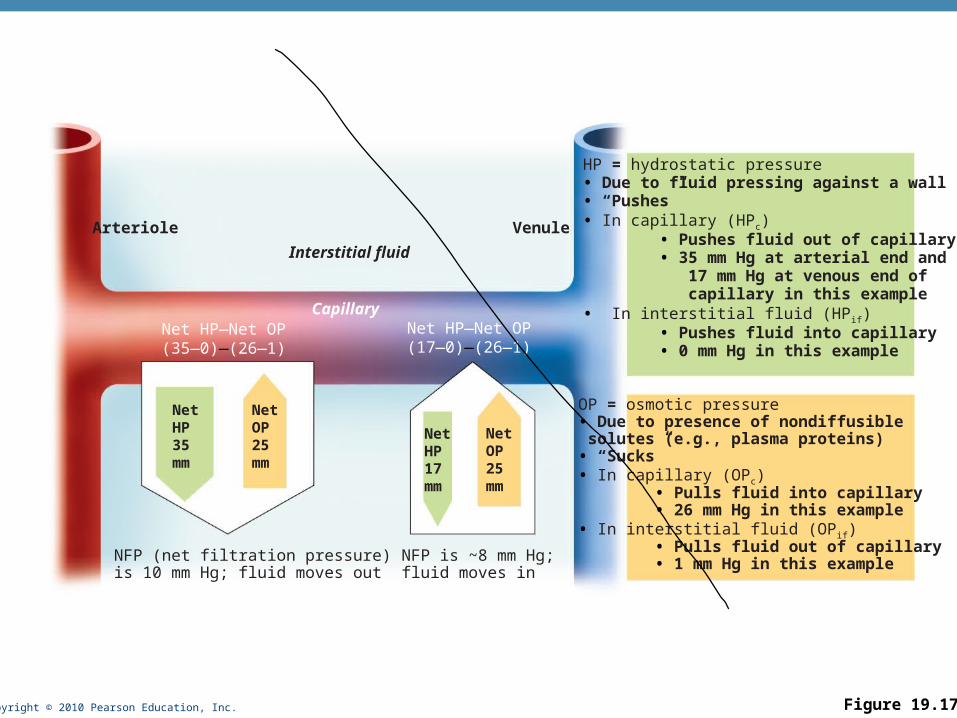
HP = hydrostatic pressure• Due to fluid pressing against a wall• “Pushes”• In capillary (HPc) • Pushes fluid out of capillary • 35 mm Hg at arterial end and 17 mm Hg at venous end of capillary in this example• In interstitial fluid (HPif) • Pushes fluid into capillary • 0 mm Hg in this example
OP = osmotic pressure• Due to presence of nondiffusible solutes (e.g., plasma proteins)• “Sucks”• In capillary (OPc) • Pulls fluid into capillary • 26 mm Hg in this example• In interstitial fluid (OPif) • Pulls fluid out of capillary • 1 mm Hg in this example
Arteriole
Capillary
Interstitial fluid
Net HP—Net OP(35—0)—(26—1)
Net HP—Net OP(17—0)—(26—1)
Venule
NFP (net filtration pressure)is 10 mm Hg; fluid moves out
NFP is ~8 mm Hg;fluid moves in
NetHP35mm
NetOP25mm
NetHP17mm
NetOP25mm
Copyright © 2010 Pearson Education, Inc.
Circulatory Shock
• Any condition in which
• Blood vessels are inadequately filled
• Blood cannot circulate normally
• Results in inadequate blood flow to meet tissue needs

Copyright © 2010 Pearson Education, Inc.
Circulatory Shock
• Hypovolemic shock: results from large-scale blood loss
• Vascular shock: results from extreme vasodilation and decreased peripheral resistance
• Cardiogenic shock results when an inefficient heart cannot sustain adequate circulation

Copyright © 2010 Pearson Education, Inc. Figure 19.18
Signs and symptoms
Acute bleeding (or other events that causeblood volume loss) leads to:
1. Inadequate tissue perfusion resulting in O2 and nutrients to cells2. Anaerobic metabolism by cells, so lactic acid accumulates3. Movement of interstitial fluid into blood, so tissues dehydrate
Initial stimulus
Result
Physiological response
Chemoreceptors activated(by in blood pH)
Baroreceptor firing reduced(by blood volume and pressure)
Hypothalamus activated(by pH and blood pressure)
Major effect Minor effect
Brain
Activation ofrespiratory centers
Cardioacceleratory andvasomotor centers activated
Sympathetic nervoussystem activated
ADHreleased
Neuronsdepressed
by pH
Intense vasoconstriction(only heart and brain spared)
Heart rate Centralnervous system
depressed
Adrenalcortex
Kidney
Renin released
Renal blood flow
Aldosteronereleased
Kidneys retainsalt and water
Angiotensin IIproduced in blood
Waterretention
Urine outputRate anddepth of
breathing
Tachycardia,weak, thready
pulse
Skin becomescold, clammy,and cyanotic
Thirst Restlessness(early sign)
Coma(late sign)
CO2 blownoff; bloodpH rises
Blood pressure maintained;if fluid volume continues to
decrease, BP ultimatelydrops. BP is a late sign.

Copyright © 2010 Pearson Education, Inc.
Maintaining Blood Pressure
• The main factors influencing blood pressure:
• Cardiac output (CO)
• Peripheral resistance (PR)
• Blood volume

Copyright © 2010 Pearson Education, Inc.
Maintaining Blood Pressure
• F = P/PR and CO = P/PR
• Blood pressure = CO x PR (and CO depends on blood volume)
• Blood pressure varies directly with CO, PR, and blood volume
• Changes in one variable are quickly compensated for by changes in the other variables

Copyright © 2010 Pearson Education, Inc.
Cardiac Output (CO)
• Determined by venous return and neural and hormonal controls
• Resting heart rate is maintained by the cardioinhibitory center via the parasympathetic vagus nerves
• Stroke volume is controlled by venous return (EDV)

Copyright © 2010 Pearson Education, Inc.
Cardiac Output (CO)
• During stress, the cardioacceleratory center increases heart rate and stroke volume via sympathetic stimulation
• ESV decreases and MAP increases

Copyright © 2010 Pearson Education, Inc. Figure 19.8
Venous return
Exercise
Contractility of cardiac muscle
Sympathetic activity Parasympathetic activity
Epinephrine in blood
EDV ESV
Stroke volume (SV) Heart rate (HR)
Cardiac output (CO = SV x HR
Activity of respiratory pump(ventral body cavity pressure)
Activity of muscular pump(skeletal muscles)
Sympathetic venoconstriction
BP activates cardiac centers in medulla
Initial stimulus
Result
Physiological response

Copyright © 2010 Pearson Education, Inc.
Control of Blood Pressure
• Short-term neural and hormonal controls
• Counteract fluctuations in blood pressure by altering peripheral resistance
• Long-term renal regulation
• Counteracts fluctuations in blood pressure by altering blood volume

Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Neural Controls
• Neural controls of peripheral resistance
• Maintain MAP by altering blood vessel diameter
• Alter blood distribution in response to specific demands
Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Neural Controls
• Neural controls operate via reflex arcs that involve
• Baroreceptors
• Vasomotor centers and vasomotor fibers
• Vascular smooth muscle

Copyright © 2010 Pearson Education, Inc.
The Vasomotor Center
• A cluster of sympathetic neurons in the medulla that oversee changes in blood vessel diameter
• Part of the cardiovascular center, along with the cardiac centers
• Maintains vasomotor tone (moderate constriction of arterioles)
• Receives inputs from baroreceptors, chemoreceptors, and higher brain centers

Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Baroreceptor-Initiated Reflexes
• Baroreceptors are located in
• Carotid sinuses
• Aortic arch
• Walls of large arteries of the neck and thorax
Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Baroreceptor-Initiated Reflexes
• Increased blood pressure stimulates baroreceptors to increase input to the vasomotor center
• Inhibits the vasomotor center, causing arteriole dilation and venodilation
• Stimulates the cardioinhibitory center

Copyright © 2010 Pearson Education, Inc. Figure 19.9
Baroreceptors in carotid sinusesand aortic archare stimulated.
Baroreceptorsin carotid sinusesand aortic archare inhibited.
Impulses from baroreceptorsstimulate cardioinhibitory center(and inhibit cardioacceleratorycenter) and inhibit vasomotorcenter.
Impulses from baroreceptors stimulatecardioacceleratory center (and inhibit cardioinhibitorycenter) and stimulate vasomotor center.
CO and Rreturn bloodpressure tohomeostatic range.
CO and Rreturn blood pressureto homeostatic range.
Rate ofvasomotor impulsesallows vasodilation,causing R
Vasomotorfibers stimulatevasoconstriction,causing R
Sympatheticimpulses to heartcause HR, contractility, and CO.
Sympatheticimpulses to heartcause HR, contractility, and CO.
Stimulus: Blood pressure(arterial bloodpressure falls belownormal range).
Stimulus: Blood pressure(arterial bloodpressure rises abovenormal range).
3
2
1
5
4a
4b
Homeostasis: Blood pressure in normal range
4b
3
2
1
5
4a

Copyright © 2010 Pearson Education, Inc. Figure 19.9 step 5
Baroreceptorsin carotid sinusesand aortic archare inhibited.
Impulses from baroreceptorsstimulate cardioacceleratory center(and inhibit cardioinhibitory center)and stimulate vasomotor center.
CO and Rreturn bloodpressure tohomeostaticrange.
Vasomotorfibers stimulatevasoconstriction,causing R
Sympatheticimpulses to heartcause HR, contractility, and CO.
Stimulus: Blood pressure(arterial bloodpressure fallsbelow normalrange).
2
3
1
4b
4a
5
Homeostasis: Blood pressure in normal range

Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Baroreceptor-Initiated Reflexes
• Baroreceptors taking part in the carotid sinus reflex protect the blood supply to the brain
• Baroreceptors taking part in the aortic reflex help maintain adequate blood pressure in the systemic circuit

Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Chemoreceptor-Initiated Reflexes
• Chemoreceptors are located in the
• Carotid sinus
• Aortic arch
• Large arteries of the neck

Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Chemoreceptor-Initiated Reflexes
• Chemoreceptors respond to rise in CO2, drop in pH or O2
• Increase blood pressure via the vasomotor center and the cardioacceleratory center
• Are more important in the regulation of respiratory rate (Chapter 22)

Copyright © 2010 Pearson Education, Inc.
Influence of Higher Brain Centers
• Reflexes that regulate BP are integrated in the medulla
• Higher brain centers (cortex and hypothalamus) can modify BP via relays to medullary centers

Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Hormonal Controls
• Adrenal medulla hormones norepinephrine (NE) and epinephrine cause generalized vasoconstriction and increase cardiac output
• Angiotensin II, generated by kidney release of renin, causes vasoconstriction

Copyright © 2010 Pearson Education, Inc.
Short-Term Mechanisms: Hormonal Controls
• Atrial natriuretic peptide causes blood volume and blood pressure to decline, causes generalized vasodilation
• Antidiuretic hormone (ADH)(vasopressin) causes intense vasoconstriction in cases of extremely low BP

Copyright © 2010 Pearson Education, Inc.
Long-Term Mechanisms: Renal Regulation
• Baroreceptors quickly adapt to chronic high or low BP
• Long-term mechanisms step in to control BP by altering blood volume
• Kidneys act directly and indirectly to regulate arterial blood pressure
1. Direct renal mechanism
2. Indirect renal (renin-angiotensin) mechanism

Copyright © 2010 Pearson Education, Inc.
Direct Renal Mechanism
• Alters blood volume independently of hormones
• Increased BP or blood volume causes the kidneys to eliminate more urine, thus reducing BP
• Decreased BP or blood volume causes the kidneys to conserve water, and BP rises

Copyright © 2010 Pearson Education, Inc.
Indirect Mechanism
• The renin-angiotensin mechanism
• Arterial blood pressure release of renin
• Renin production of angiotensin II
• Angiotensin II is a potent vasoconstrictor
• Angiotensin II aldosterone secretion
• Aldosterone renal reabsorption of Na+ and urine formation
• Angiotensin II stimulates ADH release

Copyright © 2010 Pearson Education, Inc. Figure 19.10
Arterial pressure
Baroreceptors
Indirect renalmechanism (hormonal)
Direct renalmechanism
Sympathetic stimulationpromotes renin release
Kidney
Renin release
catalyzes cascade,resulting in formation of
ADH releaseby posterior
pituitary
Aldosteronesecretion by
adrenal cortex
Waterreabsorptionby kidneys
Blood volume
Filtration
Arterial pressure
Angiotensin II
Vasoconstriction( diameter of blood vessels)
Sodiumreabsorptionby kidneys
Initial stimulus
Physiological response
Result

Copyright © 2010 Pearson Education, Inc. Figure 19.11
Activity ofmuscularpump andrespiratory
pump
Releaseof ANP
Fluid loss fromhemorrhage,
excessivesweating
Crisis stressors:exercise, trauma,
bodytemperature
Bloodbornechemicals:
epinephrine,NE, ADH,
angiotensin II; ANP release
Body size
Conservationof Na+ and
water by kidney
Blood volumeBlood pressure
Blood pH, O2, CO2
Dehydration,high hematocrit
Bloodvolume
Baroreceptors Chemoreceptors
Venousreturn
Activation of vasomotor and cardiacacceleration centers in brain stem
Heartrate
Strokevolume
Diameter ofblood vessels
Cardiac output
Initial stimulus
Result
Physiological response
Mean systemic arterial blood pressure
Bloodviscosity
Peripheral resistance
Blood vessellength