complementary medicine (cam)
TRANSCRIPT
COMPLEMENTARY MEDICINE
(CAM)
ITS CURRENT POSITION AND ITS POTENTIAL FOR
EUROPEAN HEALTHCARE
March 2008
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 2 –
ThisisajointpublicationbytheEuropeanCommitteeforHomeopathy(ECH),theEuropeanCouncilofDoctorsforPluralityinMedicine(ECPM),theInternationalCouncilofMedicalAcupunctureandRelatedTechniques(ICMART)andtheInternationalFederationofAnthroposophicMedicalAssociations(IVAA),representing132medicalCAMassociationsacrossEurope(seeAnnex2).European Committee for Homeopathy (ECH), Chaussée de Bruxelles 132, box 1, 1190Brussels,Belgium.www.homeopathyeurope.orgemail:[email protected] Council of Doctors for Plurality in Medicine (ECPM), 1 Rue Goethe, 67000Strasbourg,France.www.ecpm.orgemail:info@ecpm.orgInternationalCouncilofMedicalAcupunctureandRelatedTechniques(ICMART),GeneralSecretary, Rue de l'Amazone 62, 1060 Brussels, Belgium www.icmart.org email:[email protected] Federation of Anthroposophic Medical Associations (IVAA), MedizinischeSektion am Goetheanum, Rüttiweg, 4143 Dornach, Switzerland. www.ivaa.info email:[email protected]
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 3 –
DefinitionsofComplementarymedicine(CAM)TheCochraneComplementaryMedicineFielddefinesComplementaryMedicineasfollows: Complementarymedicineincludesallsuchpracticesandideaswhichareoutsidethedomainofconventionalmedicineinseveralcountriesanddefinedbyitsusersaspreventingortreatingillness,orpromotinghealthandwellbeing.Thesepracticescomplementmainstreammedicineby 1)contributingtoacommonwhole,2)satisfyingademandnotmetbyconventionalpractices,and3)diversifyingtheconceptualframeworkofmedicine.The National Center for Complementary and AlternativeMedicine (NCCAM) in the USAdefines Complementary and Alternative Medicine (CAM) as follows: CAM is a group ofdiversemedical and health care systems, practices, and products that are not presentlyconsidered tobepartof conventionalmedicine.Alternativemedicineoften refers to theuse of therapies as substitutes for biomedical treatment, and complementary medicinereferstotheuseofsuchtherapiesinconjunctionwithbiomedicine.IntegrativemedicinereferstoasystemofmedicinethatintegratesbiomedicinewithCAM.TheNCCAM’scategorizationofCAM:•WholeMedicalSystems:medicalsystemsoftheoryandpracticee.g.ayurveda,anthroposophicmedicine,homeopathy,naturopathicmedicine,traditionalChinesemedicine•Mind‐BodyMedicine:mindscapacityaffectsbodilyfunctionse.g.meditation,imaging•BiologicallyBasedPractices:useofnaturalsubstancese.g.herbs,vitamins•ManipulativeandBody‐BasedPractices:chiropractic,osteopathy,massage•EnergyMedicine:‐BiofieldTherapies:affectenergyfieldsofthehumanbody‐Bioelectromagneticbasedtherapies:useofelectromagneticfields
TheupsurgeofCAMAlthoughWestern/conventionalmedicinehasbroughtmuchgood,Europe is confrontedwitheverincreasinghealthcareexpenditure,anincreasingprevalenceofchronicdiseasesandfailureofeffectivelymanagingthem,ahugeburdenofmorbidityandmortalityduetothetoxicityofprescriptiondrugs1,andagrowingresistancetoantibiotics2,reflectedinthegrowingproblemofhospitalsuperbugs.Patientsarebecominggrowinglyworriedabouttheadverseeffectsandtoxicityofmanyconventionaldrugs–infactamajorcauseofdeathand hospitalization – and the inability of conventional medicine to provide adequateclinicaleffectivenessforchronicdiseases.Increasingnumbersofpatients,therefore,lookfor less‐toxic alternatives, especially in the case of chronic illness. Current citizens’attitudes towards health include a preference for natural treatments and products overchemicaldrugs,aholisticviewofhealth,abeliefinindividualresponsibilityforachievinghealth, less unquestioning acceptance of medical authority and anti‐technologysentiments.CAM is becoming increasingly popular in Europe with up to 65% of the populationreporting that they have used this form of medicine3. Approximately 30‐50% of theEuropeanpopulationuseCAMasself‐supportand10‐20%oftheEuropeanpopulationhas

– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 4 –
seen a CAM physician/practitionerwithin the previous year. Manymainstream generalpractitionerssharetheirpatients’concernsaboutconventionalmedicine.Overthelast15years they have moved from a position of silent interest to one of open enquiry andgrowing use. Large numbers of mainstream doctors are either referring to CAMpractitionersorpractising someof themoreprominentandwell‐known formsofCAM4.Moreover, many doctors believe that these therapies are useful or efficacious. A majorresponse to these changes is the growing number of practitioners of the various CAMmodalitieswho have organized themselves in professional groupings underpinnedwithappropriateeducationandtraining.IntheEuropeanUnionthereareapproximately150,000medicaldoctorswhohavetakentraining courses in a particular CAM therapy such as acupuncture, homeopathy,anthroposophic medicine or natural medicine, with figures for each therapy that arecomparabletothoseofmainstreammedicalspecialties.MostdoctorspractisingCAMworkin the ambulatory sector asGPsormedical specialists (any sort of specialty), in severalEuropean countries some of them work in mainstream hospitals including universityteachinghospitals.InspiteoftheimpressivegrowthofCAM,overallthecurrentlegalsituationofCAMacrossEurope is patchy5. The European Parliament, the Council of Europe and theWHO haveeachadoptedresolutionsthatcallontheMemberStatestostartanationalpolicyonCAM.However, a recentWHOglobal survey6 shows that only a few countrieshave anationalpolicy, lawsorregulationsonCAM,somecountriesonlyregulatespecificCAMtherapies,andothercountrieshavenonationalpolicy,lawsorregulationsonCAMatallorevenhavenoplanstoestablishthese.
Citizens’decisionsabouttheirhealthandtheirmotivestochooseCAMToday'sEuropeancitizenshavestartedtofeelthemselvesresponsiblefortheirownlivesandtheirownhealth.Thisrightofself‐determinationmay, in fact,beconsideredabasicright of European citizens. They want to make their own informed choice of therapywhether itbelongs toconventionalmedicineorCAM.MostusersofCAMdonotwant togive up conventional medicine, but rather want to choose the medical approach thatseemstoproducethebestresult incertainsituationsorthatfits intotheir lifestyle.Theability tomake their own choices and the capacity to use the resources available is keywithin the concept of salutogenesis7, a concept that has become established in publichealthandhealthpromotion,andthatfocusesonresources,maintainsandimprovesthemovementtowardshealth.Severalauthorshaveinvestigatedthecitizens’motivestochooseCAMtreatmentoptions8andconcludedthatthefollowingfactorsplayarole:1. Themost important reason is the patient’s dissatisfactionwith biomedical treatmentbecause ithasbeen ineffective– thevastmajorityofpatients consultCAMpractitionersonly after exhausting biomedical treatments, orwith conditionswhere biomedicine hasachievedonlylimitedsuccessorhadbeenunabletoofferanyrelief.2.Patientsarebecomingmoreandmoreworriedaboutissuessuchastheadverseeffectsand toxicity of many conventional drugs – in fact a major cause of death andhospitalization – and the growing resistance to antibiotics. They look for less‐toxicalternativesandvisitaGPorclinicprovidingCAMtherapies.
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 5 –
3. Patients want to be given time and to be listened to, and seek alternative therapiesbecause they see them as less authoritarian with more personal autonomy, input andcontrol over thedecision‐making regarding their care.They are also looking for amoreintimate relationship with their health care providers. They want health professionalswho will respect them as partners in their care and who see and understand them aswholepeoplewithcomplexlives,notjust‘lesions’andlabvalues.Biomedicaltreatmentisseenasimpersonalandtootechnologicallyoriented.4.CAMtherapiesareattractivebecausetheyareseenasmorecompatiblewithpatients’values, ethics,world‐view, spiritual/religiousphilosophyor beliefs regarding thenatureand meaning of health and illness. These developments have been facilitated by therevolution in information technology, which is enabling easy access to sources of CAMinformationontheinternet.
Citizens’needforproperinformationAccording to theWHOGuidelines on Developing Consumer Information on Proper Use ofTraditional,ComplementaryandAlternativeMedicine(2004)“itisextremelyimportanttocreatetheconditionsforthecorrectandappropriateuseofCAMwhich,ifusedcorrectly,cancontribute to theprotectionand theenhancementofcitizens’healthandwellbeing.One such condition is the need to make sure that consumers are better informed andaware of CAM strategies and treatments so as to enable them to make appropriatedecisions on how to improve their health. […] The long‐term goal is to maximize thebenefitsandminimizetherisksofCAMusebyempoweringconsumerstobecomeactiveparticipantsinhealthcareandtomakeinformedchoices”9.These guidelines ‘provide governments and other stakeholderswith an overview of thegeneral principles and activities necessary for the development of reliable consumerinformation’.Thedocumentisalsomeanttobe‘ausefulreferencetoconsumersinguidingthemontheinformationtheyneedtohaveinordertochooseaTM/CAMtherapythatissafeandeffective’.The long‐termgoalof theWHO is toempowerconsumers tobecomeactiveparticipantsinhealthcareandtomakeinformedchoices.TheWHO suggests that general consumer information regarding CAMmay include thefollowingkeyissues:• The importance of the need to take charge of one’s own health by being an informedconsumer.• The need for all providers, both conventional health care providers and CAMpractitioners,tobeawareofthemajorCAMandconventionaltherapiesinuseinordertopromote the best treatment strategy to meet the patient’s specific needs and preventpotentiallydangerousinteractions.•The importanceofensuringthat theprovider iscompetentandprovidesCAMservicesandproductsofquality.•Whererelevant,theneedforconsumerstofindoutaboutstandardchargesandpossiblehealthinsurancecoverageforCAMtherapies.
HolisticapproachandthecontributionofCAMMost CAM therapies are based on a holistic approach to the individual patient and areprimarily aimed at restoring and promoting health rather than defeating disease, an
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 6 –
approachwhichisincreasinglygainingamorecentralpositioninpublichealth.Sincetheholisticmodel viewsmost illness anddiseaseas thedirect consequenceof imbalance intheindividual’senvironment,habitsand/orwayofliving,whichispotentiallycorrectable,an important part of the practitioner’s job is detective work: working in closecollaborationwiththepatientintrackingdownthepathogenicimbalance,andthenwiththeaidofnaturaltreatmentsandmedicinesandthepatient’sowncommitmenttochange,facilitatingthehealingpowerofnature,vismedicatrixnaturae, torestorethebalancewecallhealth.Holismdoesnotrejectthebiomedicalconceptofdisease,nordoesitattempttoreplaceitwith its own. Rather, it seeks to include all that expand this concept to include a widespectrumofpredisposingfactorsthattheaveragemedicaldoctortypically(althoughnotnecessarily)hasneitherthetime,theinterest,northetrainingtoexplore.Since each person is unique, the treatment programme, to be most effective, must beindividualized.CAMpractitionersmayprescribeapackageof care,whichwould includemodification of lifestyle, dietary change, reduction or elimination of substance‐abusebehaviours, acquisition of stress‐reduction techniques and exercise aswell asmaking aspecificCAMmedicinalprescription (herbal,homeopathicoranthroposophicmedicines)or giving abodily treatment (acupuncture, osteopathy, chiropractic, shiatsu, reflexology,massageorbodyexercisesetc.).Healthpsychologyapproachesaredesignedtomodulatethestressresponseandimprovehealthbehavioursbyteachingindividualsmoreadaptivemethodsofinterpretinglifechallengesandmoreeffectivecopingresponses. Holisticapproach,salutogenesis,andthecontributionofCAMThe holistic model describes interactions between mental, psychosocial and biologicalfactors in thecauseandprogressionof illnessanddisease.Howan individual interpretsand responds to the outer and inner environment determines responses to stress,influences health behaviour, contributes to the neuro‐endocrine and immune response,andmayultimatelyaffecthealthoutcomes.Theactualmanifestationofdisease isalwaysmulti‐causal and depends on the conjunction of precipitating mental, psychosocial andpathogenic factors, along with the individual’s constitutional susceptibilities in generaland in particular organ systems. Environmental hazards, infectious agents andpsychologicalstressorsaredestabilizingfactors,whereuponinternalsystemagentsactorare ready to act to maintain constancy or homeostasis. Disease is a failure of adaptiveresponse, resulting in disruption of the overall equilibrium of the system. Within theholisticmodelhealthisnotmerelytheabsenceofdisease,buttheabilityofanorganismtorespond adaptively to a wide range of environmental hazards, infectious agents andpsychologicalstressors.Withintheconceptofsalutogenesis10healthisseenasamovementinacontinuumonanaxis between total ill health (dis‐ease) and total health (ease), in which it is moreimportant to focus on peoples’ resources and capacity to create health than the classicfocusonrisks,illhealth,anddisease.Thisapproachisincreasinglygainingamorecentralposition in public health and health promotion research and practice. The ability tocomprehendthewholesituationandthecapacitytousetheresourcesavailable iscalled‘sense of coherence’. This capacity is a combination of peoples’ ability to assess andunderstand thesituation theywere in, to findameaning tomove inahealthpromotingdirection, also having the capacity to do so—that is, comprehensibility,meaningfulness,

– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 7 –
andmanageability.Thebeautyoftheconceptualworldofthesalutogenesisisitsdynamicandflexibleapproachandthepersistentfocusonabilityandcapacitytomanage.Thereisevidence (Surtees et al.11) demonstrating that a strong sense of coherence is associatedwith a 30% reduction in mortality from all causes, cardiovascular disease and cancer,independentofage,sex,andprevalentchronicdisease.InthefinalreportoftheEuropeanMastersforHealthPromotion(EUMAHP)thissenseofcoherenceisalsousedasalearningprinciple.Most CAM therapies are based on a holistic approach of the individual patient and areprimarilyaimedatpromotinghealthratherthandefeatingdisease,inotherwordsgivingimportancetosalutogenesisinadditiontopathogenesis.CAMpractitionersmayprescribeapackageofcare,whichwouldincludemodificationoflifestyle,dietarychange,reductionoreliminationof substance‐abusebehaviours, acquisitionof stress‐reduction techniquesandexerciseaswellasaspecificCAMtreatmentand/orprescription.Healthpsychologyapproachesaredesignedtomodulatethestressresponseandimprovehealthbehavioursby teaching individualsmore adaptivemethods of interpreting life challenges andmoreeffective coping responses. The holistic CAM practitioner typically sees each patient asunique and tailors their advice to fit thepatient's life, rather than expectinghim/her toadapt to a standard set of recommendations. CAM therapies involve the patient as anactivepartnerinhis/hercare,withanemphasisonpatienteducationconcerninghowtheycanbestimprovetheirhealth.
AimisoptimumhealthAccording to the holistic CAM model, health is not merely the absence of disease orinfirmity, but the ability of an individual to respond adaptively to a wide range ofenvironmentalchallenges,e.g.physical,chemical, infectious,psychological,etc.Diseaseisthedefaultnegativevalueresultingfromafailuretomaintainoptimumhealth,afailureofadaptive response, resulting in disruption of the overall equilibrium of the system.Consequently, the way to treat disease is not so much to attack the symptoms or theimmediateunderlyingpathologyasitistorestorethepatienttoastateofoverallhealth.It istheaimofCAMtobringaboutaconditionofindividualoptimumhealth,notjusttheabsenceofsymptomsofdisease.It isthisfocusuponhealthratherthandiseasewhichislargely responsible for the nature of holistic medicine and its effectiveness for diseaseprevention,earlydiagnosis,andthetreatmentofsub‐clinicalandchronicdisease.Thepre‐disease state, the area between complete symptom‐freewellbeing and actual disease isviewedasalackofhealthneedingattention.It shouldbeemphasised that theholisticpractitioner isnotdrawingattentionmerely tothe obvious predisposing factors, such as smoking in the case of lung cancer or fat andcholesterol in the case of heart disease. Dozens of other factors may predispose onetowardscancerandsimultaneouslydetractfromoptimumhealth.Manymayseemtohavenothingtodowithcancerperse,butinsteadweakentheimmunesystem’sabilitytoresistcancer,aswellasotherdiseases.Theholist ismoreconcernedwith themultiple factorsthat contribute to overall health, but taken individually are often neither necessary norsufficient for the occurrence of specific diseases. According to Rosenman12, it appearsprudenttopay increasedattentiontothe individualwhopossessesarisk factor,andnottheriskfactorperse.

– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 8 –
TherapeuticpartnershipandpatientempowermentMost CAM practitioners employ a holistic approach to treatment which focuses on theemotionalandspiritualwell‐beingof theirpatients, aswell as theirphysicalhealth.Theholistic model of health and disease shifts a greater responsibility not only for healthmaintenance,butalso for treatmentofdisease, fromtheprovider to thepatient.HolisticCAM practitioners encourage people to use and to recognise their own self‐healingabilitiesandtodevelopmoreactiveapproachestolifeandhealth.Theyinvolvethepatientas an active partner in his/her care,with an emphasis on patient education concerninghow they can best improve their health. They contribute to the patient’s autonomy byrestoringtheirownnaturalsystemsfor fightingdiseaseandmaintaininghealthwiththeaid of naturalmedicines,modification of lifestyle, dietary change andhealth psychologyapproaches.TheholisticCAMpractitionerstypicallyseeeachpatientasuniqueandtailortheiradvicetofitthepatient's life,ratherthanexpectinghim/hertoadapttoastandardset of recommendations. They rely on input from their patients to keep them informedaboutchangesinlifestyles,moodsandattitudes.Patients’primarymotivationtoseeaCAMpractitioneristheircontinuingsearchforrelieffrom chronic problems. Studies have demonstrated13 that the patients of CAMpractitioners have more independent and self‐reliant views and typically believe eachpatient should have the main responsibility for their own health and decisions aboutwhichkindoftreatmenttopursue,whereasmostpatientswhodonotuseCAMtherapiesbelieve that their doctors should play the key role (the traditional paternalistic doctor‐patient‐relationship). CAM patients argue that each kind of practitioner has distinctiveskills andexpertiseand that theywant to selectdifferenthealingoptions,dependingontheir particular situation. Their relationships with their practitioners are largelypragmatic; if thepractitioners couldhelp them, theywouldcontinue to see them; ifnot,theywouldmoveontotryanotherpractitioneroranotherkindoftherapy.CAMpatientsreportthattheytypicallyworkaspartnerswiththeirpractitionersinthehealingprocessby accepting responsibility for their own care. They are more likely than the averagepatient topayattention to theirdiet,posture, sleeppatternsandexerciseregimens.Theconcept of self‐care requires a daily conscious focus on one’s physical, mental, andemotionalstateandtheabilitytotakecorrectiveactionwheneverimbalanceissensed.
Thefollowingtableshowsthedifferencesbetweentheholisticandbiomedicalmodel:Model Holisticmedicine Biomedicine Body/mindasanadaptable,
flexibleandcreativesysteminterlinkedwithothersystems
Mind/bodyseparation;bodyasanobject,acomplex,butpredictablemachine
Emphasis Health DiseasePriority Prevention Repair,neutralisation,
normalisationDiagnosticfocus Whatmadethisperson
susceptibletodisease?Causesonphysical,emotional,social,mental,spirituallevel
Whatiswronginthispersonandhastobefixed?Localisedtissuedisruption&specificpathogen
Treatmentapproach
Mobilisingandstimulatinganindividual’sregenerativecapacities(vismedicatrix
Eradicating,neutralisingormanagingaphysicalproblem,interveningindiseasepathway,

– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 9 –
naturae),restoringbalancetothewholepsychosomaticsystem
symptomatic,mechanistic
Individualization/standardization
Individualizationofcare Standardizationofcare
Long‐term/short‐term
Along‐termfocusoncreatingandmaintaininghealthandwell‐being
Offensiveinterventionwithemphasisonshort‐termresults
Militarymetaphorfortherapy
Stimulatethehomeforces Searchanddestroytheinvader
Patient/physicianrelationship
Authorityandresponsibilityinherentineachindividual,co‐operativepartnership,empowering
Authorityandresponsibilityinherentinpractitionerandnotpatient,paternalistic,disempowering
CAMasasafecomplementoralternativetoconventionalmedicineWhile biomedicine has had extraordinary successes with many acute illnesses such aspneumonia and heart conditions, it has not been able to offermuch assistance to theirpatientswhosufferwithchronicproblems.Biomedicinecontinues torelyon itsexistingarmamentarium of solutions such as drugs and surgery for conditions which requiredifferentand lessdrasticapproaches.CAMtherapies,however,havemuch tooffer; theycanoftenbeusedasafirstoptionincertainproblems,keepingmorecostly,moreinvasiveandpotentiallytoxictreatmentasasecondoption,whichisinaccordancewiththebasicmedicalprinciple,originallyascribedtoHippocrates, ‘Primumnonnocere’meaning‘First,do no harm’. The risks generally related to CAM therapies are rather low whenappropriately prescribed and used. These therapies may therefore help to prevent theoften long‐term dependency on conventional medication and to reduce the enormousburden of mortality and morbidity caused by the adverse effects of conventionalprescriptiondrugsandtheever‐increasingresistancetoantibiotics.Individual risk levelsmayhowevervary fromoneCAMtherapy toanother.Only in rarecircumstances acupuncture can produce the complications associated with any type ofneedleuse,whichcanbeavoidedbybasicstandardsofgoodpractice14.Homeopathicandanthroposophic medicinal products have shown to be very safe15. Herbal medicines,althoughmanyofthemhavegoodsafetyprofiles,mayprobablypresentagreaterriskofadverse effects and interaction than other CAM therapies16. The evidence regarding thenature and incidence of adverse effects of herbalmedicines is highly incomplete17.Onlyrelatively few clinical cases of interactions between herbal medicines and prescriptiondrugshavebeendocumentedinthemedicalliterature18,butitmustbeborneinmindthatherbal medicines can be taken over an extended period of time, which provides theopportunity for enzyme induction and othermechanisms of interaction to take effect19.Nevertheless, adverse effects from herbalmedicinal products aremore infrequent thantheequivalentconventionaltreatment;herbalmedicinalproductscanbeacceptablysafeifusedproperlyandundertheguidanceofaprofessional.Risks also include adverse events following sub‐standard practices or the misuse ofTM/CAM by unqualified practitioners. These indirect risks may occur, when CAMpractitionersarenotfullytrained;whenpractitionersdonotfollowtheprofessionalcode
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 10 –
of ethics; when practitioners disregard possible interactions with conventionalprescriptiondrugsandcontra‐indications;whenpractitionersdonotmakeacomparativeassessment as to the therapeutic possibilities of CAM versus any necessity of otherinterventions, includingbiomedicine,orwhen the treatment isnot adjustedormodifiedaccording to the condition or constitution of the patient. The European medical CAMassociations ECH, ECPM, ICMART and IVAA have therefore established guidelines fortraining,certificationandpractice.
CAMasaneffectivecomplementoralternativetoconventionalmedicineCAM therapies are not only safe, they are also effective: over the last few decades anincreasingamountofresearchhasbeenpublishedontheeffectivenessofCAMtherapies,notablyhomeopathy,acupuncture,herbalmedicineandanthroposophicmedicine,inpeer‐reviewed scientific journals. Research ranges from basic science studies related toidentifying potential mechanisms of action, to randomized controlled clinical trials inhumansandanimals, to cost‐effectiveness studiesandhealthservices research.There isan increasing body of clinical evidence for the effectiveness of some of thewell‐knownCAM therapies. Several long‐term outcome studies have showed that e.g. homeopathy,acupuncture and anthroposophic medicine can be at least as effective as conventionalcare,withfewersideeffectsandhigherpatientsatisfaction20.Otherresearchstudieshaveshown overall that three quarters of the chronically ill patients achieved what theydescribedas ‘moderatelybetter’or ‘muchbetter’.Anumberofrandomisedclinical trialshaveshownhomeopathyandacupuncturesuperior toplacebo;othershaveshownthemtohaveatleastequaleffectivenesstoconventionaltreatments.There exist a number of treatments for specific ailments where the implementation ofCAM therapies may offer significant cost savings to public health bodies, and to theeconomymorewidely,andothersinwhichadditionalbenefitstopatientsmaybeobtainedcosteffectively21.Until2004morethan50economicevaluationshavebeenpublishedandabouthalfofthemhavefoundlowercostforCAMthanforregularcare.Incontrastwithconventionalprescriptiondrugs,homeopathicandanthroposophicmedicinesaregeneric,non‐patentedandnon‐patentablemedicinalsubstances,producedatlowcosts.Moreover,they do not imply any costs associatedwith iatrogenic illness. Several research studieshave demonstrated that patients who were treated with homeopathy, acupuncture oranthroposophicmedicineused fewermedications,hadbetterhealth, fewerdaysoffsick,andfewervisitstomedicalspecialiststhanpatientsofconventionalphysicians.During the last three years the cost‐effectiveness of acupuncture according tointernational benchmarks was determined for headache, low back pain and neck pain,which account for large amounts of absenteeism amongst Europe’s workforce. Forhomeopathy, two economic evaluations have recorded the outcomes and costs oftreatmentbyGermanandFrenchGeneralPractitioners(GPs)whointegratehomeopathyintheirpractice,andcomparedthemwithGPswhodonot.Theresultsofbothstudiesarecongruent: GPs who integrate homeopathy in their practice achieve better results forsimilar costs. Cost‐effectiveness of anthroposophic medicine was demonstrated in theSwissPEKstudy(ProgramEvaluationKomplementärmedizin). IntheUKmainlystudiesfor spinal‐manipulation and acupuncturewereperformed and the incremental costs foroneadditionalyearofperfectqualityoflife(1QALY)duetotheCAMtreatmenthavebeenfoundtobeabout€15,000.
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 11 –
NeedforCAMresearchResearch in CAMhas been seriously hampered by a lack of research infrastructure andfunding,lackofresearchexpertiseamongCAMpractitioners,lackofappropriateresearchmodelsandstrategiesaswellasthescepticismoftheconventionalscientificcommunity.Whilst CAM may improve health, reduce disease, and reduce health costs, the CAMindustryalonecannotbeexpectedtosupporttheresearchtoanswerthesequestions.Thisispartlybecauseof the lackof financial incentives for industry, andpartlybecause, likemainstreammedicalresearch,thereisasocialresponsibilityforgovernmenttofundsuchresearch.ThereisahugedisparitybetweenpublicfundingforconventionaldrugresearchandthatforCAMresearch.Fundingbytheindustryislimitedbythefactthathomeopathicandherbalmedicinesaregenericandcannotbepatented;thustherearenolargeprofitstobemadefrominvestmentsinresearchasformanynewbiomedicaldrugs.Notably in the USA, the national authorities have taken the growing demand for CAMseriously. In1998 theCongress established theNationalCenter forComplementary andAlternative Medicine (NCCAM) at the National Institutes of Health that is charged to‘conductbasic and applied research (intramural and extramural), research training, anddisseminate health information and other programmes with respect to identifying,investigating, and validating CAM treatments, diagnostic and prevention modalities,disciplinesandsystems’.Itsannualbudgetis$120million(approx.€80million).TodatetheNCCAMhas funded10university‐based centres for research onCAM. ‘Seed’ fundinganddedicatedfundingprovidedsomeimpetustoestablishandcontinueaneffectiveCAMresearch program. Over the last decade, some Western‐European countries (Denmark,Germany,Norway, theNetherlands and theUK)have granted somemoney for researchprojectsinCAM.
SupranationalCAMpolicyrecommendationsBoththeEuropeanParliamentandtheCouncilofEuropeadvocatetheofficialrecognitionofCAM.TheParliament,initsresolutionofMay1997,calledontheEuropeanCommissiona. to launchaprocessofrecognizingnon‐conventionalmedicineand, to thisend, to takethenecessarystepstoencouragetheestablishmentofappropriatecommittees;b.tocarryoutathoroughstudyintothesafety,effectiveness,areaofapplicationandthecomplementaryoralternativenatureofallnon‐conventionalmedicinesandtodrawupacomparativestudyofthevariousnationallegalmodelstowhichnon‐conventionalmedicalpractitionersaresubject;c.tomake,informulatingEuropeanlegislationonnon‐conventionalformsofmedicine,aclear distinction between non‐conventional medicines which are 'complementary' innature and those which are 'alternative' medicines in the sense that they replaceconventionalmedicine;andcallsontheCouncilofMinistersaftercompletionofthepreliminaryworkreferredtoabove(atb.) toencourage thedevelopmentof researchprogrammes in the fieldofnon‐conventionalmedicinescoveringtheindividualandholisticapproach,thepreventiveroleand the specific characteristics of the non‐conventional medical disciplines; Parliamentundertakestodolikewise.Inasimilarvein,theCouncilofEuropein1999statedthat“[T]hedemandsofpublichealthand therightof individuals tohealthprotectionmustcome first.The limitationsofnon‐conventionalmedicinesmust not be ignorednor underestimated.[…]Establishing a legal
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 12 –
frameworkfornon‐conventionalmedicineisadifficultundertakingbutitispreferabletobeing too liberal. [… ][T]he best guarantee for patients lies in a properly trainedprofession,whichisawareofitslimitations,hasasystemofethicsandself‐regulationandisalsosubjecttooutsidecontrol.[….][I]nthefuturealternativeorcomplementaryformsofmedicinecouldbepractisedbydoctorsofconventionalmedicineaswellasbyanywell‐trained practitioner of non‐conventional medicine (a patient could consult one or theother, eitherupon referralbyhisorher familydoctororofhisorher freewill), shouldethical principles prevail. Appropriate courses should be offered in universities to trainallopathic doctors in alternative and complementary forms of treatment. The Assemblytherefore calls on member states to promote official recognition of these forms ofmedicineinmedicalfacultiesandtoencouragehospitalstousethem.”In 2003 WHO General Assembly adopted a resolution on Traditional Medicine andComplementary and Alternative Medicine, which urged Member States, among otheritems,–toadapt,adoptandimplement,whereappropriate,WHO’straditionalmedicinestrategyasabasisfornationaltraditionalmedicineprogrammesorworkplans;– where appropriate, to formulate and implement national policies and regulations ontraditionalandcomplementaryandalternativemedicine insupportof theproperuseoftraditionalmedicine,and its integration intonationalhealth‐caresystems,dependingonthecircumstancesintheircountries;–toprovideadequatesupportforresearchontraditionalremedies;– to promote and support, if necessary and in accordancewith national circumstances,provisionoftrainingand,ifnecessary,retrainingoftraditionalmedicinepractitioners,andof a system for the qualification, accreditation or licensing of traditional medicinepractitioners;– to provide reliable information on traditional medicine and complementary andalternativemedicinetoconsumersandprovidersinordertopromotetheirsounduse.TheWHO report ‘TraditionalMedicine Strategy 2002‐2005’ 22, describes its first globalstrategyontraditionalandalternativemedicine,which ‘providesa framework forpolicyto assist countries to regulate traditional or complementary/alternative medicine(TM/CAM)tomakeitsusesafer,moreaccessibletotheirpopulationsandsustainable’.FormoredetailsseeAnnex1.
IntegratedMedicineIntegrated Medicine (in the USA: Integrative Medicine) is a recent movement thatcombines thebestof twoworlds, i.e. it integrates conventionalmedicinewithCAM. It isthe practice of medicine that reaffirms the importance of the relationship between thepractitionerandpatient,focusesonthewholeperson,isinformedbyevidence,andmakesuseofallappropriatetherapeuticapproaches(i.e.conventionalmedicineaswellasCAM),healthcareprofessionalsanddisciplinestoachievehealthandhealing.IntheUSAtheConsortiumofAcademicHealthCentersforIntegrativeMedicine(CAHCIM)includes39highlyesteemedacademicmedicalcentres(=20%ofallUSacademicmedicalcentres). Among them areHarvardMedical School, YaleUniversity, StanfordUniversity,MayoClinic,JohnsHopkinsUniversity,etc.
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 13 –
It aims to "help transformmedicine and healthcare through rigorous scientific studies,new models of clinical care, and innovative educational programs that integratebiomedicine,thecomplexityofhumanbeings,theintrinsicnatureofhealingandtherichdiversityoftherapeuticsystems".TheConsortiumhasissuedthefollowingstatement:“Integrativemedicineisnotaradicalmovementbutitcanproducemajorchange.Itspointistopositionmedicinetocontinuetobuilduponitsfundamentalplatformofsciencebuttorepositionitselftocreateahealthsystemwhichmorebroadlyfocusesonthewellbeingofourpatientsaswellasitspractitioners.Todoso,medicaleducationandpracticemust:• Refocus on the patient as a whole and the primacy of meaningful physician‐patientrelationships.Moreandmoreofthebenefitsofourhealthsystemwillrequirechangesinpatient behaviour, i.e., modifying lifestyle as well as taking therapeutics correctly. Suchchanges will require far more meaningful physician‐patient relationships and medicalschoolcurriculamustincorporatestrategiestoreflecttheseneeds.• Involve the patient as an active partner in his/her care,with an emphasis on patienteducationconcerninghowtheycanbestimprovetheirhealth.• Be open to understanding the benefits and limitations of conventional allopathicmedicine and the realization that science alone will not effectively deal with all thecomplex needs of our patients. Many patients, particularly, those with chronic or lifethreateningconditionswantaccesstoCAMapproaches.Ourhealthsystemmustrationallyaddresstheseneeds.• Teach practitioners the fundamentals of CAM strategies including their underlyingprinciplesaswellasevidence,orlackthereof,ofefficacy.•AdvocateforsoundclinicalresearchtotesttheefficacyofCAMstrategies.•Usethebestinscientificallybasedmedicaltherapieswheneverappropriatebutprovidecompassion, attention to our patient’s spiritual and emotional needs as well asappropriatecomplementaryandalternativeapproacheswhentheyimproveconventionalmedicine. Fundamentally, Integrative Medicine is meant to provide the best possiblemedicine/healthcare,forbothdoctorandpatient,andthesuccessofthemovementwillbesignalledbydroppingtheadjective. ItisourbeliefandrecommendationthatIntegrativeMedicine be a cornerstone of the urgently needed reconfiguration of our increasinglydysfunctionalsystemofhealthcare. TheIntegrativeMedicineoftodaywillsimplybethemedicineofthenewcentury.”Asattitudeschangeandscientificevidencecontinuestogrow,itisenvisagedthattheterm"complementary"willsoonbeoutdatedandreplacedwith"integrated",whichsuggeststhehealthybalancethatcanbeachievedbetweenmodernWesternmedicineandcomplementarytherapies.
Towardssafe,patient‐orientedhealthcareservicesinEuropeIf the EUwants to deliver high quality care on all levels, not merely technological andpharmaceutical,aneffective,safe,patient‐orientedsystemofhealthcareisneeded.Merelyadding additional therapies to a system of carewithout implementing a holistic, caringapproach to the careofpatientswilldo little to improvehealth care.All themajorCAMtherapiesapproachillnessfirstbytryingtosupportandinducetheself‐healingprocessoftheindividual.Ifrecoverycanoccurfromthisalone,thelikelihoodofadverseeffectsandtheneedforhigh‐impact,high‐costinterventionisreduced.It isthisorientationtowards

– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 14 –
self‐healingandhealthpromotion–improvinghealthratherthandefeatingdisease–thatmakesCAMapproachesespeciallyappropriate.CAM,whichisdemandedbymanymillionsofEuropeancitizens,hasthepotentialtohumanisemodernmedicineandwidenitsvisionbeyonddiseasetohealthandwellbeinginitswidestsense.All themajor CAM systems are aimed at bringing about a condition of individualoptimum health, not just the absence of symptomsof disease.Wheneverpossible,CAM is collaborative and focusedon strengthening andempoweringpatients, andoncontributingtotheirautonomy.ThisapproachisfullyinlinewiththeaimoftheHealthandConsumerProtectionProgramme20082013thatfocusesonpromotinghealthandpoliciesthatleadtoahealthierwayoflife.
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 15 –
References1.‐WorldHealthOrganization(2002)SafetyofMedicines.Aguidetodetectingandreportingadversedrugreactions:Whyhealthprofessionalsneedtotakeaction.WHO,Geneva,Switzerland2.‐WorldHealthOrganization(2000)Antibioticresistance:synthesisofrecommendationsbyexpertpolicygroups.AllianceforthePrudentUseofAntibioticsWHO/CDS/CSR/DRS/2001/103.–WorldHealthOrganization(2001)LegalStatusofTraditionalMedicineandComplementary/AlternativeMedicine:AWorldwideReview,Geneva,Switzerland‐WorldHealthOrganization(2002)TraditionalMedicineStrategy20022005,Geneva,Swtzerland‐ErnstE(2000).Prevalenceofuseofcomplementary/alternativemedicine:asystematicreview.BulletinoftheWorldHealthOrganization,78:252‐257.‐SteinsbekkA,AdamsJ,SibbrittD,JacobsenG,JohnsenR(2007)Theprofilesofadultswhoconsultalternativehealthpractitionersand/orgeneralpractitioners.ScandinavianJournalofPrimaryHealthCare,25:86‐92‐HarrisP,ReesR(2000).Theprevalenceofcomplementaryandalternativemedicineuseamongthegeneralpopulation:asystematicreviewoftheliterature.ComplementaryTherapiesinMedicine,8:88‐96.‐Menniti‐IppolitoF,GargiuloL,BolognaE,ForcellaE,RaschettiR(2002)UseofunconventionalmedicineinItaly:anation‐widesurvey.EuropeanJournalofClinicalPharmacology,58:61‐64.‐FeatherstoneC,GoddenD,GaultC,EmslieM,Took‐ZozayaM(2003)PrevalencestudyofconcurrentuseofcomplementaryandalternativemedicineinpatientsattendingprimarycareservicesinScotland.AmericanJournalofPublicHealth,93:1080‐1082.‐WolfU,Maxion‐BergemannS,BornhöftG,MatthiessenPF,WolfM(2006).UseofcomplementarymedicineinSwitzerland.ForschendeKomplementärmedizin,13Suppl2:4‐6.‐HanssenB,GrimsgaardS,LaunsøL,FønnebøV,FalkenbergT,RasmussenNK(2005)UseofcomplementaryandalternativemedicineintheScandinaviancountries.ScandinavianJournalofPrimaryHealthCare,23:57‐62.‐HärtelU,VolgerE(2004)InanspruchnameundAkseptanzklassischerNaturheilverfahrenundalternativerHeilmethodeninDeutschland‐ErgebnisseeinerrepräsentativenBevölkerungsstudie[UseandacceptanceofclassicalnaturalandalternativemedicineinGermany‐findingsofarepresentativepopulation‐basedsurvey]ForschendeKomplementärmedizinundKlassischeNaturheilkunde,11:327‐334.‐ThomasKJ,ColemanP(2004)UseofcomplementaryoralternativemedicineinageneralpopulationinGreatBritain.ResultsfromtheNationalOmnibusSurvey.JournalofPublicHealth,26:152‐157.‐ThomasKJ,NichollJP,ColemanP(2001).UseandexpenditureoncomplementarymedicineinEngland:apopulationbasedsurvey.ComplementaryTherapiesinMedicine,9:2‐11.‐NilssonM,TrehnG,AsplundK(2001)UseofcomplementaryandalternativemedicineremediesinSweden.Apopulation‐basedlongitudinalstudywithinthenorthernSwedenMONICAProject.JournalofInternalMedicine,250:225–2334.‐AstinJA(1998b)AreviewoftheincorporationofComplementaryandAlternativeMedicinebymainstreamphysicians.ArchivesofInternalMedicine.158:2303‐2310‐WhiteAR,ReschK‐L,ErnstE(1997)Complementarymedicine:useandattitudesamongGPs.Familypractice,14:302‐306.‐LewithGT,HylandM,GraySF(2001).AttitudestoanduseofcomplementarymedicineamongphysiciansintheUnitedKingdom.ComplementaryTherapiesinMedicine,9:167‐172.‐vanHaselenRA,ReiberU,NickelI,JakobA,FisherPA(2004).ProvidingComplementaryandAlternativeMedicineinprimarycare:theprimarycareworkers'perspective.ComplementaryTherapiesinMedicine,12:6‐16‐SchmidtK,JacobsPA,BartonA(2002)Cross‐culturaldifferencesinGPs'attitudestowardscomplementaryandalternativemedicine:asurveycomparingregionsoftheUKandGermany.ComplementaryTherapiesinMedicine,10:141‐147.5.‐ErsdalG,RamstadS,HowareEuropeanpatientssafeguardedwhenusingcomplementaryandalternativemedicine(CAM)?Jurisdiction,supervisionandreimbursementstatusintheEEAarea(EUandEFTA)andSwitzerland,CAMCancerProject,28October2005;availableat:
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 16 –
http://www.camcancer.org/mod_product/uploads/camcancer_legal_report_%28FINAL%29.pdf6.WHOGlobalAtlasofTraditional,ComplementaryandAlternativeMedicine(textvolumeandmapvolume).Kobe,Japan,WorldHealthOrganization,CentreforHealthDevelopment,2005.7.‐LindströmBetal(2005)Salutogenesis.JournalofEpidemiologyandCommunityHealth,59:440‐4428.‐AstinJA(1998)Whypatientsusealternativemedicine:resultsofanationalstudy.JournaloftheAmericanMedicalAssociation,279:1548‐1553‐JobstKA(1998)Towardintegratedhealthcare:practicalandphilosophicalissuesattheheartoftheintegrationofbiomedical,complementary,andalternativemedicines,JournalofAlternativeandComplementaryMedicine,4,122‐126‐KaptchukTJ,EisenbergDM(1998)Thepersuasiveappealofalternativemedicine,AnnalsofInternalMedicine,129,1061‐1065‐MitzdorfU,BeckK,Horton‐HausnechtJ,WeidenhammerW,KindermannA,TakacsM,AstorG,MelchartD(1999)Whydopatientsseektreatmentinhospitalsofcomplementarymedicine?JournalofAlternativeandComplementaryMedicine,5,463‐473‐ZollmanC.VickersA(1999)ABCofcomplementarymedicine:ComplementarymedicineandthepatientBritishMedicalJournal,319,1486–1489.9. ‐ World Health Organization WHO (2004) Guidelines on developing consumer information onproperuseoftraditional,complementaryandalternativemedicine.WHO,Geneva,Switzerland10.‐LindströmBetal(2005)Salutogenesis.JournalofEpidemiologyandCommunityHealth;59;440‐44211.‐SurteesP,WainwrightN,LubenR,KhawKT,DayN(2003).SenseofcoherenceandmortalityinmenandwomenintheEPIC‐NorfolkUnitedKingdomprospectivecohortstudy.AmericanJournalofEpidemiology,158:1202‐1209.12.‐RosenmanRH.(1997)Doenvironmentaleffectsonhumanemotionscausecardiovasculardisorders?ActaPhysiologicaScandinavicaSuppl.640:133‐136.13.‐KelnerM(2000).Thetherapeuticrelationshipunderfire.In:ComplementaryandAlternativeMedicine:ChallengeandChangeeditedbyMerrijoyKelner,BeverlyWellman.HarwoodAcademicPublishers.‐FlöistrupH,SwartzJ,BergströmA,AlmJS,ScheyniusA,vanHageM,WaserM,Braun‐FahrländerC,Schram‐BijkerkD,HuberM,ZutavernA,vonMutiusE,UblaggerE,RiedlerJ,MichaelsKB,PershagenG,TheParsifalStudyGroup(2006).AllergicdiseaseandsensitizationinSteinerschoolchildren.Journalofallergyandclinicalimmunology,117:59‐66.14.NationalInstitutesofHealth(NIH)Acupuncture.NIHConsensusStatementOnline1997Nov3‐5;15(5):1‐34(availableathttp://odp.od.nih.gov/consensus/cons/107/107_statement.htm).15.‐DantasFRampesH(2000)Dohomeopathicmedicinesprovokeadverseeffects?Asystematicreview.BritishHomeopathicJournal.89,Suppl1:35‐38‐BaarsEWetal(2005)Safetyofhomeopathicinjectablesforsubcutaneousadministration:adocumentationoftheexperienceofprescribingpractitioners.JournalofAlternativeandComplementaryMedicine;11:609‐616.‐HamreHJ,WittCM,GlockmannA,TrögerW,WillichSN,KieneH(2006)Useandsafetyofanthroposophicmedicationsinchronicdisease:a2‐yearprospectiveanalysis.DrugSafety,29:1173‐1189.16.VickersA,ZollmanC(1999)ABCofcomplementarymedicine:HerbalmedicineBritishMedicalJournal,319:1050–1053.17.ErnstE (2004)Challenges forphytopharmacovigilance.PostgraduateMedical Journal80;249‐
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 17 –
25018. Fugh‐Berman A, Ernst E (2001) Herb‐drug interactions: review and assessment of reportreliability.BritishJournalofClinicalPharmacology52:587–595.19. Williamson EM (2003) Drug interactions between herbal and prescription medicines. DrugSafety,26:1075‐109220.Effectivenessstudies:General,aboutqualityofCAMstudies:‐LawsonML,PhamB,KlassenTP,MoherD(2005)Systematicreviewsinvolvingcomplementaryandalternativemedicineinterventionshadhigherqualityofreportingthanconventionalmedicinereviews.Journalofclinicalepidemiology,58:777‐784.‐KlassenTP,PhamB,LawsonML,MoherD(2005)Forrandomizedcontrolledtrials,thequalityofreportsofcomplementaryandalternativemedicinewasasgoodasreportsofconventionalmedicine.Journalofclinicalepidemiology,58:763‐768.Evaluationofacupuncture,anthroposophicmedicine,homeopathy,neuraltherapy,herbalmedicineandTraditionalChineseMedicine:‐MelchartD,MitscherlichF,AmietM,EichenbergerR,KochR(2005)ProgrammEvaluationKomplemantärmedizin(PEK)Schlussbericht(24/04/2005).Acupuncture:Non‐exhaustivelistofobservationalstudies:‐LindeK,WeidenhammerW,StrengA,HoppeA,MelchartD.(2006)Acupunctureforosteoarthriticpain:anobservationalstudyinroutinecare.Rheumatology(Oxford),45:222‐227‐MelchartD,WeidenhammerW,StrengA,HoppeA,PfaffenrathV,LindeK.(2006)Acupunctureforchronicheadaches‐‐anepidemiologicalstudy.Headache,46:632‐641‐LindeK,StrengA,HoppeA,WeidenhammerW,WagenpfeilS,MelchartD.(2007)Randomizedtrialvs.observationalstudyofacupunctureformigrainefoundthatpatientcharacteristicsdifferedbutoutcomesweresimilar.JournalofClinicalEpidemiology,60:280‐287‐WeidenhammerW,StrengA,LindeK,HoppeA,MelchartD(2007)Acupunctureforchronicpainwithintheresearchprogramof10GermanHealthInsuranceFunds‐‐basicresultsfromanobservationalstudy.ComplementaryTherapiesinMedicine,15:238‐246‐WeidenhammerW,LindeK,StrengA,HoppeA,MelchartD(2007)Acupunctureforchroniclowbackpaininroutinecare:amulticenterobservationalstudy.ClinicalJournalofPain,23:128‐135.Non‐exhaustivelistofsystematicreviews:‐BowerWF,DiaoM,TangJL,YeungCK(2005).Acupuncturefornocturnalenuresisinchildren:asystematicreviewandexplorationofrationale.Neurourologyandurodynamics,24:267–272.‐BermanB,EzzoJ,HadhazyV,etal.(1999)Isacupunctureeffectiveinthetreatmentoffibromyalgia?JournalofFamilyPractice,48:213‐218.‐CasimiroL,BrosseauL,MilneSetal.AcupunctureandelectroacupunctureforthetreatmentofRA(2003).CochraneDatabaseSystematicReviews,3:CD003788.‐ErnstE,PittlerMH(1998).Theeffectivenessofacupunctureintreatingacutedentalpain:asystematicreview.BritishDentalJournal,184:443–447.‐ErnstE,WhiteAR(1999).Acupunctureasatreatmentfortemporomandibularjointdysfunction:asystematicreviewofrandomizedtrials.ArchivesofOtolaryngologyHead&NeckSurgery,125:269–272.‐ErnstE,WhiteAR(1998).Acupunctureforbackpain:ameta‐analysisofrandomizedcontrolledtrials.ArchivesofInternalMedicine,158:2235–41.‐EzzoJ,BermanB,HadhazyVAetal(2000).Isacupunctureeffectiveforthetreatmentofchronicpain?Asystematicreview.Pain,86:217–225.‐EzzoJ,HadhazyV,BirchS,etal.(2001)Acupunctureforosteoarthritisoftheknee:asystematicreview.ArthritisandRheumatism,44:819‐825.‐FurlanAD,vanTulderM,CherkinD,TsukayamaH,LaoL,KoesB,BermanB.(2005)Acupunctureanddry‐needlingforlowbackpain:anupdatedsystematicreviewwithintheframeworkofthecochranecollaboration.Spine,30:944‐463‐GreenS,BuchbinderR,HetrickS(2005).Acupunctureforshoulderpain.CochraneDatabaseSystematicReviews,2:CD005319.
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 18 –
‐HeL,ZhouD,WuB,LiN,ZhouMK(2004).AcupunctureforBell’spalsy.CochraneDatabaseSystematicReviews,1:CD002914.‐JedelE(2005).Acupunctureinxerostomia–asystematicreview.JournalofOralRehabilitation,32:392–396.‐JewellD,YoungG(2003).Interventionsfornauseaandvomitinginearlypregnancy.CochraneDatabaseSystematicReviews,4:CD000145.‐LeeA,DoneML(2004).StimulationofthewristacupuncturepointP6forpreventingpostoperativenauseaandvomiting.CochraneDatabaseSystematicReviews,3:CD003281.‐LeeH,ErnstE(2005).Acupunctureanalgesiaduringsurgery:asystematicreview.Pain,114:511–517.‐LeeH,ErnstE(2004).AcupunctureforGIendoscopy:asystematicreview.GastrointestinalEndoscopy,60:784–789.‐LeeH,ErnstE(2004).Acupunctureforlaborpainmanagement:asystematicreview.Americanjournalofobstetricsandgynecology,191:1573–1579.‐LeeH,SchmidtK,ErnstE(2005).Acupunctureforthereliefofcancer‐relatedpain–asystematicreview.EuropeanJournalofPain,9:437–444.‐LindeK,JobstK,PantonJ.(2001)Acupunctureforchronicasthma.(CochraneReview).In:TheCochraneLibrary.Issue2,Oxford:UpdateSoftware.‐ManheimerE,WhiteA,BermanB,ForysK,ErnstE(2005).Meta‐analysis:acupunctureforlowbackpain.AnnalsofInternalMedicine,142:651–663.‐McCarneyRW,BrinkhausB,LassersonTJ,LindeK(2004).Acupunctureforchronicasthma.CochraneDatabaseSystematicReviews,1:CD000008.‐MelchartD,LindeK,FischerPetal(2001).Acupunctureforidiopathicheadache.CochraneDatabaseSystematicReviews,1:CD001218.‐MukainoY,ParkJ,WhiteA,ErnstE(2005).Theeffectivenessofacupuncturefordepression–asystematicreviewofrandomisedcontrolledtrials.AcupunctureinMedicine,23:70–76.‐PanCX,MorrisonRS,NessJ,Fugh‐BermanA,LeipzigRM(2000).Complementaryandalternativemedicineinthemanagementofpain,dyspnea,andnauseaandvomitingneartheendoflife.Asystematicreview.JournalofPainandSymptomManagement,20:374–387.‐ParkJ,WhiteAR,ErnstE(2000).Efficacyofacupunctureasatreatmentfortinnitus:asystematicreview.ArchivesofOtolaryngologyHead&NeckSurgery,126:489–492.‐PittlerMH,ErnstE(2005).Complementarytherapiesforperipheralarterialdisease:systematicreview.Atherosclerosis,181:1–7.‐PittlerMH,ErnstE(2005).Complementarytherapiesforreducingbodyweight:asystematicreview.InternationalJournalofObesityandRelatedMetabolicDisorders,29:1030–1038.‐ProctorML,SmithCA,FarquharCM,StonesRW(2002).Transcutaneouselectricalnervestimulationandacupunctureforprimarydysmenorrhoea.CochraneDatabaseSystematicReviews,1:CD002123.‐SmithCA,CrowtherCA(2004).Acupunctureforinductionoflabour.CochraneDatabaseSystematicReviews,1:CD002962.‐SmithCA,HayPP(2005).Acupuncturefordepression.CochraneDatabaseSystematicReviews,2:CD004046.‐SmithLA,OldmanAD,McQuayHJ,MooreRA(2000).Teasingapartqualityandvalidityinsystematicreviews:anexamplefromacupuncturetrialsinchronicneckandbackpain.Pain,86:119–132.‐SokSR,ErlenJA,KimKB(2003).Effectsofacupuncturetherapyoninsomnia.JournalofAdvancedNursing,44:375–384.‐Stener‐VictorinE(2005).Thepain‐relievingeffectofelectro‐acupunctureandconventionalmedicalanalgesicmethodsduringoocyteretrieval:asystematicreviewofrandomizedcontrolledtrials.HumanReproduction,20:339–349.‐SzeFK,WongE,OrKK,LauJ,WooJ(2002).Doesacupunctureimprovemotorrecoveryafterstroke?Ameta‐analysisofrandomizedcontrolledtrials.Stroke,33:2604–2619.‐TrinhKV,PhillipsSD,HoEetal(2004).Acupunctureforthealleviationoflateralepicondylepain:asystematicreview.Rheumatology(Oxford),43:1085–1090.‐vanTulderM,CherkinD,BermanB,etal.(2001)Acupunctureforlowbackpain(CochraneReview).In:TheCochraneLibrary.Issue2,Oxford:UpdateSoftware.‐VickersAJ.(1996)Canacupuncturehavespecificeffectsonhealth?AsystematicreviewofacupunctureantiemesisRCTs.JournaloftheRoyalSocietyofMedicine,89:303‐311.
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 19 –
‐WhiteAR,ErnstE(1999).Asystematicreviewofrandomizedcontrolledtrialsofacupunctureforneckpain.Rheumatology(Oxford),38:143–147.‐WhiteAR,RampesH,ErnstE(2002).Acupunctureforsmokingcessation.CochraneDatabaseSystematicReviews,2:CD000009.‐ZhangSH,LiuM,AsplundK,LiL(2005).Acupunctureforacutestroke.CochraneDatabaseSystematicReviews,2:CD003317.Anthroposophicmedicine:Non‐exhaustivelistofobservationalstudies:‐HamreH,WittC,GlockmannA,ZieglerR,WillichS,KieneH(2007)Anthroposophicmedicaltherapyinchronicdisease:afour‐yearprospectivecohortstudy.BMCComplementAlternativeMedicine,7:10‐Grossarth‐MaticekR,ZieglerR(2007).Prospectivecontrolledcohortstudiesonlong‐termtherapyofovariancancerpatientswithmistletoe(ViscumalbumL.)extractsiscador.Arzneimittelforschung,57:665‐678‐Grossarth‐MaticekR,ZieglerR.(2006)Prospectivecontrolledcohortstudiesonlong‐termtherapyofbreastcancerpatientswithamistletoepreparation(Iscador).ForschendeKomplementärmedizin,13:285‐292‐CarlssonM,ArmanM,BackmanM,FlattersU,HatschekT,HamrinE(2006)AFive‐yearFollow‐upofQualityofLifeinWomenwithBreastCancerinAnthroposophicandConventionalCare.‐HeusserP,BraunSB,ZieglerR,BertschyM,HelwigS,vanWegbergB,CernyT(2006)Palliativein‐patientcancertreatmentinananthroposophichospital:I.Treatmentpatternsandcompliancewithanthroposophicmedicine.ForschendeKomplementärmedizin,13:94‐100.‐HeusserP,BraunSB,BertschyM,BurkhardR,ZieglerR,HelwigS,vanWegbergB,CernyT(2006).Palliativein‐patientcancertreatmentinananthroposophichospital:II.Qualityoflifeduringandafterstationarytreatment,andsubjectivetreatmentbenefits.ForschendeKomplementärmedizin,13:156‐166.Non‐exhaustivelistofsystematicreviews:‐KienleGS,KieneH(2007).Complementarycancertherapy:asystematicreviewofprospectiveclinicaltrialsonanthroposophicmistletoeextracts.Europeanjournalofmedicalresearch,12:103‐119EvidenceBasedComplementaryandAlternativeMedicine,3:523‐531‐KienleGS,HamreHJ,KieneH.(2004)Anthroposophicalmedicine:asystematicreviewofrandomisedclinicaltrials.WienerklinischeWochenschrift,116:407‐408‐KienleGS,KieneH,AlbonicoHU(2006)[Anthroposophicmedicine:healthtechnologyassessmentreport,shortversion.]ForschendeKomplementärmedizin;13Suppl2:7‐18‐KienleG,KieneH,AlbonicoHU(2006)AnthroposophicMedicineEffectiveness,Utility,CostsSafety.SchattauerVerlagHomeopathy:Non‐exhaustivelistofobservationalstudies:‐SpenceD,ThompsonEA,BarronSJ(2005)HomeopathicTreatmentforChronicDisease:A6‐Year,University‐HospitalOutpatientObservationalStudy.JournalofAlternativeandComplementaryMedicine11(5):793‐798.‐WittCM,LüdtkeR,BaurR,WillichSN(2005)HomeopathicMedicalPractice:Long‐termresultsofaCohortStudywith3981Patients.BMCPublicHealth.5(1):115.GüthlinC,LangeO,WalachH(2004).Measuringtheeffectsofacupunctureandhomoeopathyingeneralpractice:Anuncontrolledprospectivedocumentationapproach.BMCPublicHealth,4:6‐SharplesF,vanHaselenR,FisherP(2003).NHSpatiënts’perspectiveoncomplementarymedicine.ComplementaryTherapiesinMedicine,11:243–248Non‐exhaustivelistofsystematicreviews:‐KleijnenJ,KnipschildP,terRietG(1991).Clinicaltrialsofhomeopathy,BritishMedicalJournal,302:316‐323‐CucheratM,HaughMC,GoochM,BoisselJP(2000).Evidenceofclinicalefficacyofhomeopathy–Ameta‐analysisofclinicaltrials.EuropeanJournalofClinicalPharmacology,56:27–33‐LindeK,ClausiusN,RamirezG,MelchartD,EitelF,HedgesLV,JonasWB(1997)Aretheclinicaleffectsofhomeopathyplaceboeffects?Ameta‐analysisofplacebo‐controlledtrials.Lancet,350:834‐843
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 20 –
‐ShangA,Huwiler‐MuntenerK,NarteyL,JuniP,DorigS,SterneJA,PewsnerD,EggerM(2005).Aretheclinicaleffectsofhomoeopathyplaceboeffects?Comparativestudyofplacebo‐controlledtrialsofhomoeopathyandallopathy.Lancet,366:726–732‐JacobsJ,JonasWB,Jimenez‐PerezM,CrothersD(2003).Homeopathyforchildhooddiarrhea:combinedresultsandmetaanalysisfromthreerandomized,controlledclinicaltrials.PediatricInfectiousDiseaseJournal,22:229–234‐VickersA,SmithC(2006).HomoeopathicOscillococcinumforpreventingandtreatinginfluenzaandinfluenza‐likesyndromes(CochraneReview).In:TheCochraneLibrary.Chichester,UK:JohnWiley&Sons,Ltd.CD001957‐BarnesJ,ReschK‐L,ErnstE(1997).Homeopathyforpostoperativeileus?Ameta‐analysis.JournalofClinicalGastroenterology,25:628–633‐WiesenauerM,LüdtkeR(1996).Ameta‐analysisofthehomeopathictreatmentofpollinosiswithGalphimiaglauca.ForschendeKomplementärmedizinundKlassischeNaturheilkunde,3:230–236‐TaylorMA,ReillyD,Llewellyn‐JonesRH,McSharryC,AitchisonTC(2000).Randomisedcontrolledtrialsofhomoeopathyversusplaceboinperennialallergicrhinitiswithoverviewoffourtrialseries.BritishMedicalJournal,321:471–476‐BellaviteP,OrtolaniR,PontarolloF,PiasereV,BenatoG,ConfortiA(2006).Immunologyandhomeopathy.4.Clinicalstudies–Part2.Evidence‐basedComplementaryandAlternativeMedicine:eCAM,3:397–409‐SchneiderB,KleinP,WeiserM(2005).Treatmentofvertigowithahomeopathiccomplexremedycomparedwithusualtreatments:ameta‐analysisofclinicaltrials.Arzneimittelforschung,55:23–29‐ErnstE,BarnesJ(1998).Arehomoeopathicremedieseffectivefordelayed‐onsetmusclesoreness?–Asystematicreviewofplacebo‐controlledtrials.Perfusion(Nürnberg),11:4–8‐UllmanD(2003).Controlledclinicaltrialsevaluatingthehomeopathictreatmentofpeoplewithhumanimmunodeficiencyvirusoracquiredimmunedeficiencysyndrome.JournalofAlternativeandComplementaryMedicine,9:133–141‐McCarneyRW,LindeK,LassersonTJ(2004).Homeopathyforchronicasthma(CochraneReview).In:TheCochraneLibrary.Chichester,UK:JohnWiley&Sons,Ltd.CD000353‐McCarneyR,WarnerJ,FisherP,vanHaselenR(2004).Homeopathyfordementia(CochraneReview).In:TheCochraneLibrary.Chichester,UK:JohnWiley&Sons,Ltd.CD003803‐OwenJM,GreenBN(2004).Homeopathictreatmentofheadaches:Asystematicreviewoftheliterature.JournalofChiropracticMedicine,3:45–52‐SmithCA(2003).Homoeopathyforinductionoflabour(CochraneReview).In:TheCochraneLibrary.Chichester,UK:JohnWiley&Sons,Ltd.CD003399‐PilkingtonK,KirkwoodG,RampesH,FisherP,RichardsonJ(2005).Homeopathyfordepression:asystematicreviewoftheresearchevidence.Homeopathy,94:153–163‐PilkingtonK,KirkwoodG,RampesH,FisherP,RichardsonJ(2006).Homeopathyforanxietyandanxietydisorders:Asystematicreviewoftheresearch.Homeopathy,95:151–162‐LongL,ErnstE(2001).Homeopathicremediesforthetreatmentofosteoarthritis–Asystematicreview.BritishHomeopathicJournal,90:37–43‐ErnstE(1999).Homeopathicprophylaxisofheadachesandmigraine?Asystematicreview.JournalofPainandSymptomManagement,18:353–35721.Cost‐effectivenessstudies:CAMingeneral:‐SmallwoodC(2005).TheroleofComplementaryandAlternativeMedicineintheNHS–anInvestigationintothePotentialContributionofMainstreamComplementaryTherapiestoHealthcareintheUK.‐CanterPH,CoonJT,ErnstE(2006).Cost‐effectivenessofcomplementarytherapiesintheUnitedKingdom‐asystematicreview.EvidenceBasedComplementaryandAlternativeMedicine,3:425‐432.‐HermanPM,CraigBM,CaspiO(2005).Iscomplementaryandalternativemedicine(CAM)cost‐effective?Asystematicreview.BMCComplementaryandAlternativeMedicine,5:11.‐Maxion‐BergemannS,WolfM,BornhöftG,MatthiessenPF,WolfU(2006).Complementaryandalternativemedicinecosts‐asystematicliteraturereview.ForschendeKomplementärmedizin,13Suppl2:42‐45.‐CanterPH,ThompsonCoonJ,ErnstE(2005).CosteffectivenessofcomplementarytreatmentsintheUnitedKingdom:asystematicreview.BritishMedicalJournal,331:880–881.Acupuncture:
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 21 –
‐RatcliffeJ,ThomasKJ,MacPhersonH,BrazierJ(2006).Arandomisedcontrolledtrialofacupuncturecareforpersistentlowbackpain:costeffectivenessanalysis.BritishMedicalJournal,333:626.‐ReinholdT,WittCM,JenaS,BrinkhausB,WillichSN(2007).Qualityoflifeandcost‐effectivenessofacupuncturetreatmentinpatientswithosteoarthritispain.TheEuropeanJournalofHealthEconomics,1618‐7598‐ThomasKJ,MacPhersonH,RatcliffeJ,ThorpeL,BrazierJ,CampbellM,FitterM,RomanM,WaltersS,NichollJP(2005)Longertermclinicalandeconomicbenefitsofofferingacupuncturecaretopatientswithchroniclowbackpain.HealthTechnologyAssessment,9(32):iii‐iv,ix‐x,1‐109.‐VickersAJ,ReesRW,ZollmanCE,McCarneyR,SmithCM,EllisN,FisherP,VanHaselenR,WonderlingD,GrieveR(2004)Acupunctureofchronicheadachedisordersinprimarycare:randomisedcontrolledtrialandeconomicanalysis.HealthTechnologyAssessment,8(48):iii,1‐35.‐WittCM,JenaS,SelimD,BrinkhausB,ReinholdT,WruckK,LieckerB,LindeK,WegscheiderK,WillichSN(2006).Pragmaticrandomizedtrialevaluatingtheclinicalandeconomiceffectivenessofacupunctureforchroniclowbackpain.AmericanJournalofEpidemiology,164:487‐496.‐WillichSN,ReinholdT,SelimD,JenaS,BrinkhausB,WittCM(2006)Cost‐effectivenessofacupuncturetreatmentinpatientswithchronicneckpain.Pain,125:107‐113.‐WittCM,ReinholdT,BrinkhausB,RollS,JenaS,WillichSN(2008).Acupunctureinpatientswithdysmenorrhea:arandomizedstudyonclinicaleffectivenessandcost‐effectivenessinusualcare.AmericanJournalofObstetricsandGynecology,198:166.e1‐8.‐WonderlingD,VickersAJ,GrieveR,McCarneyR(2004).Costeffectivenessanalysisofarandomisedtrialofacupunctureforchronicheadacheinprimarycare.BritishMedicalJournal,328:747‐749.Anthroposophicmedicine:‐HamreHJ,WittCM,GlockmannA,ZieglerR,WillichSN,KieneH(2007)Anthroposophicmedicaltherapyinchronicdisease:afour‐yearprospectivecohortstudy.BMCComplementaryandAlternativeMedicine,7:10.‐HamreHJ,WittCM,GlockmannA,ZieglerR,WillichSN,KieneH(2006).Healthcostsinanthroposophictherapyusers:atwo‐yearprospectivecohortstudy.BMCHealthServicesResearch,6:65.‐HamreHJ,Becker‐WittC,GlockmannA,ZieglerR,WillichSN,KieneH(2004)Anthroposophictherapiesinchronicdisease:theAnthroposophicMedicineOutcomesStudy(AMOS).EuropeanJournalofMedicalResearch9:351‐360.‐RitchieJ(2001)AmodelofIntegratedPrimaryCare:AnthroposophicMedicine.DepartmentofGeneralPracticeandPrimaryCare,StBatholomew'sandtheRoyalLondonSchollofMedicineandDentistry,QueenMary,UniversityofLondon‐KienleG,KieneH,AlbonicoHU(2006)AnthroposophicMedicineEffectiveness,Utility,CostsSafety.SchattauerVerlagHomeopathy:‐WittC,KeilT,SelimD,RollS,VanceW,WegscheiderK,WillichSN(2005).Outcomeandcostsofhomeopathicandconventionaltreatmentstrategies:acomparativecohortstudyinpatientswithchronicdisorders.ComplementaryTherapiesinMedicine,13:79–86‐TrichardM,ChaufferinGNicoloyannisN(2005).Pharmacoeconomiccomparisonbetweenhomeopathicandantibiotictreatmentstrategiesinrecurrentacuterhinopharyngitisinchildren.Homeopathy,94:3–9‐BornhöftG,WolfU,vonAmmonK,RighettiM,Maxion‐BergemannS,BaumgartnerS,ThurneysenAE,MatthiessenPF(2006).Effectiveness,safetyandcost‐effectivenessofhomeopathyingeneralpractice‐summarizedhealthtechnologyassessment.ForschendeKomplementärmedizin,13Suppl2:19‐29.‐CaisseNationaledel’AssuranceMaladiedesTravailleursSalariés(CNAMTS),CarnetsStatistiques,Lesecteurlibéraldesprofessionsdesanté(07/1998).‐VainchtockAetal(2002)Descriptiveandcomparativestudyofpatient‐managementbyhomeopathicGPsversusallopathicGPs.ValueinHealth5:468.22.WorldHealthOrganizationWHO(2002)TraditionalMedicinesStrategy:20022005.WHO,Geneva,Switzerland(documentreferenceWHO/EDM/TRM/2002.1)
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 22 –
ANNEXI
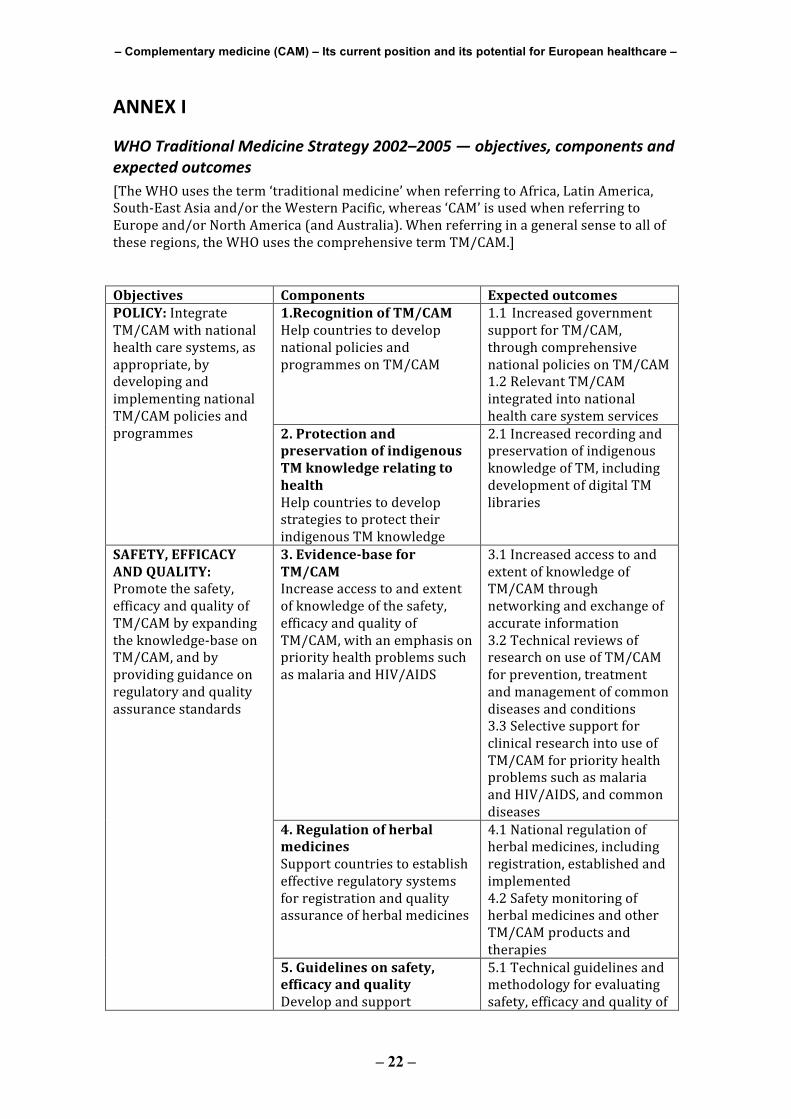
WHOTraditionalMedicineStrategy2002–2005—objectives,componentsandexpectedoutcomes[TheWHOusestheterm‘traditionalmedicine’whenreferringtoAfrica,LatinAmerica,South‐EastAsiaand/ortheWesternPacific,whereas‘CAM’isusedwhenreferringtoEuropeand/orNorthAmerica(andAustralia).Whenreferringinageneralsensetoalloftheseregions,theWHOusesthecomprehensivetermTM/CAM.] Objectives Components Expectedoutcomes
1.RecognitionofTM/CAMHelpcountriestodevelopnationalpoliciesandprogrammesonTM/CAM
1.1 IncreasedgovernmentsupportforTM/CAM,throughcomprehensivenationalpoliciesonTM/CAM1.2RelevantTM/CAMintegratedintonationalhealthcaresystemservices
POLICY:IntegrateTM/CAMwithnationalhealthcaresystems,asappropriate,bydevelopingandimplementingnationalTM/CAMpoliciesandprogrammes 2.Protectionand
preservationofindigenousTMknowledgerelatingtohealthHelpcountriestodevelopstrategiestoprotecttheirindigenousTMknowledge
2.1IncreasedrecordingandpreservationofindigenousknowledgeofTM,includingdevelopmentofdigitalTMlibraries
3.EvidencebaseforTM/CAMIncreaseaccesstoandextentofknowledgeofthesafety,efficacyandqualityofTM/CAM,withanemphasisonpriorityhealthproblemssuchasmalariaandHIV/AIDS
3.1IncreasedaccesstoandextentofknowledgeofTM/CAMthroughnetworkingandexchangeofaccurateinformation3.2TechnicalreviewsofresearchonuseofTM/CAMforprevention,treatmentandmanagementofcommondiseasesandconditions3.3SelectivesupportforclinicalresearchintouseofTM/CAMforpriorityhealthproblemssuchasmalariaandHIV/AIDS,andcommondiseases
4.RegulationofherbalmedicinesSupportcountriestoestablisheffectiveregulatorysystemsforregistrationandqualityassuranceofherbalmedicines
4.1Nationalregulationofherbalmedicines,includingregistration,establishedandimplemented4.2SafetymonitoringofherbalmedicinesandotherTM/CAMproductsandtherapies
SAFETY,EFFICACYANDQUALITY:Promotethesafety,efficacyandqualityofTM/CAMbyexpandingtheknowledge‐baseonTM/CAM,andbyprovidingguidanceonregulatoryandqualityassurancestandards
5.Guidelinesonsafety,efficacyandqualityDevelopandsupport
5.1Technicalguidelinesandmethodologyforevaluatingsafety,efficacyandqualityof
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 23 –
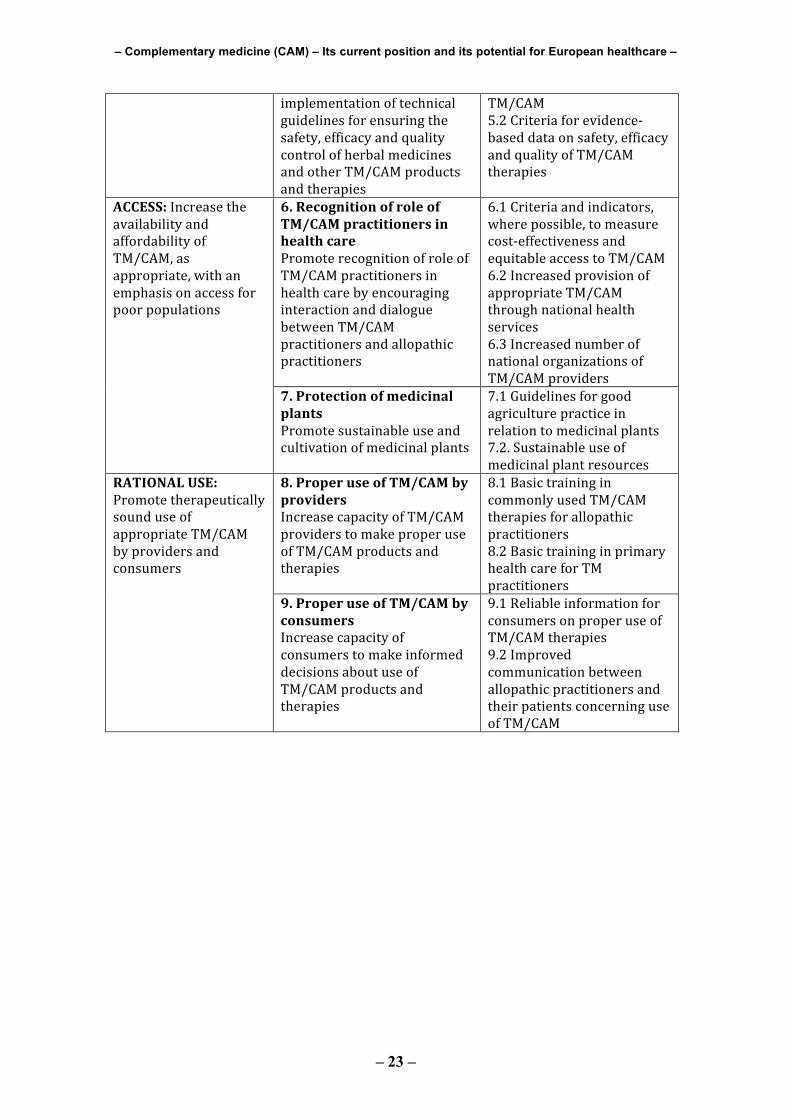
implementationoftechnicalguidelinesforensuringthesafety,efficacyandqualitycontrolofherbalmedicinesandotherTM/CAMproductsandtherapies
TM/CAM5.2Criteriaforevidence‐baseddataonsafety,efficacyandqualityofTM/CAMtherapies
6.RecognitionofroleofTM/CAMpractitionersinhealthcarePromoterecognitionofroleofTM/CAMpractitionersinhealthcarebyencouraginginteractionanddialoguebetweenTM/CAMpractitionersandallopathicpractitioners
6.1Criteriaandindicators,wherepossible,tomeasurecost‐effectivenessandequitableaccesstoTM/CAM6.2IncreasedprovisionofappropriateTM/CAMthroughnationalhealthservices6.3IncreasednumberofnationalorganizationsofTM/CAMproviders
ACCESS:IncreasetheavailabilityandaffordabilityofTM/CAM,asappropriate,withanemphasisonaccessforpoorpopulations
7.ProtectionofmedicinalplantsPromotesustainableuseandcultivationofmedicinalplants
7.1Guidelinesforgoodagriculturepracticeinrelationtomedicinalplants7.2.Sustainableuseofmedicinalplantresources
8.ProperuseofTM/CAMbyprovidersIncreasecapacityofTM/CAMproviderstomakeproperuseofTM/CAMproductsandtherapies
8.1BasictrainingincommonlyusedTM/CAMtherapiesforallopathicpractitioners8.2BasictraininginprimaryhealthcareforTMpractitioners
RATIONALUSE:PromotetherapeuticallysounduseofappropriateTM/CAMbyprovidersandconsumers
9.ProperuseofTM/CAMbyconsumersIncreasecapacityofconsumerstomakeinformeddecisionsaboutuseofTM/CAMproductsandtherapies
9.1ReliableinformationforconsumersonproperuseofTM/CAMtherapies9.2ImprovedcommunicationbetweenallopathicpractitionersandtheirpatientsconcerninguseofTM/CAM
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 24 –
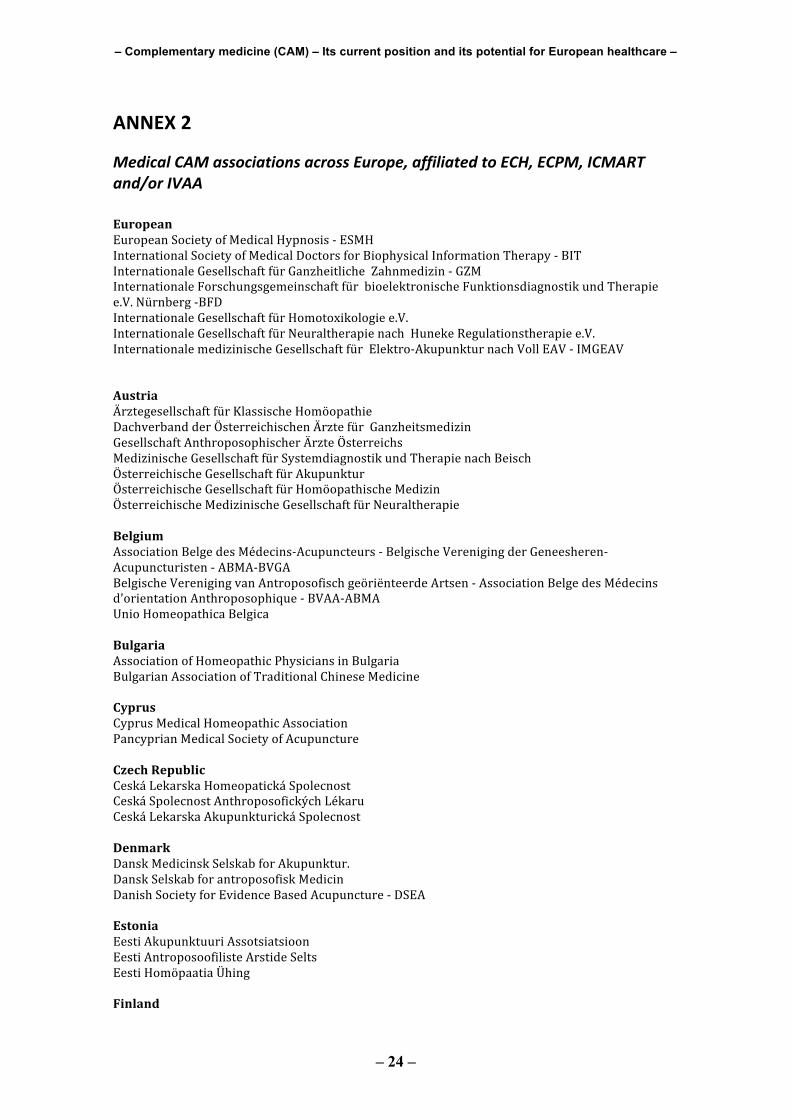
ANNEX2
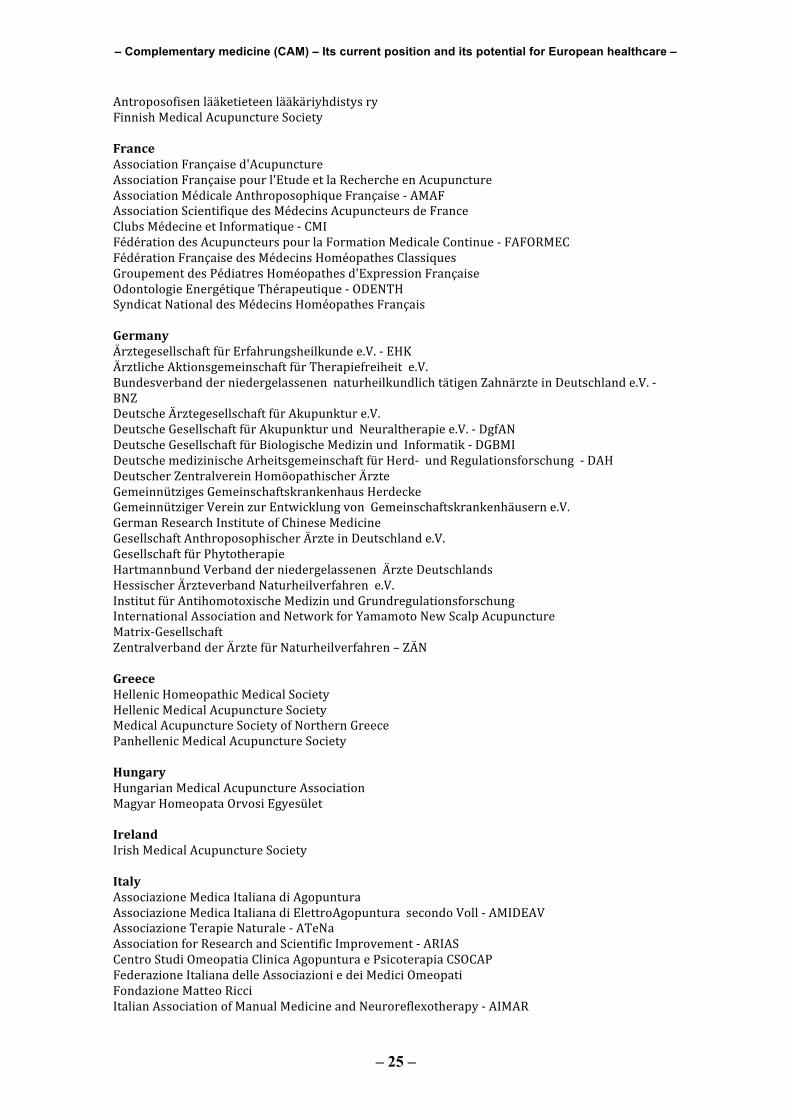
MedicalCAMassociationsacrossEurope,affiliatedtoECH,ECPM,ICMARTand/orIVAA EuropeanEuropeanSocietyofMedicalHypnosis‐ESMHInternationalSocietyofMedicalDoctorsforBiophysicalInformationTherapy‐BITInternationaleGesellschaftfürGanzheitlicheZahnmedizin‐GZMInternationaleForschungsgemeinschaftfürbioelektronischeFunktionsdiagnostikundTherapiee.V.Nürnberg‐BFDInternationaleGesellschaftfürHomotoxikologiee.V.InternationaleGesellschaftfürNeuraltherapienachHunekeRegulationstherapiee.V.InternationalemedizinischeGesellschaftfürElektro‐AkupunkturnachVollEAV‐IMGEAVAustriaÄrztegesellschaftfürKlassischeHomöopathie DachverbandderÖsterreichischenÄrztefürGanzheitsmedizinGesellschaftAnthroposophischerÄrzteÖsterreichsMedizinischeGesellschaftfürSystemdiagnostikundTherapienachBeischÖsterreichischeGesellschaftfürAkupunktur ÖsterreichischeGesellschaftfürHomöopathischeMedizinÖsterreichischeMedizinischeGesellschaftfürNeuraltherapieBelgiumAssociationBelgedesMédecins‐Acupuncteurs‐BelgischeVerenigingderGeneesheren‐Acupuncturisten‐ABMA‐BVGABelgischeVerenigingvanAntroposofischgeöriënteerdeArtsen‐AssociationBelgedesMédecinsd'orientationAnthroposophique‐BVAA‐ABMAUnioHomeopathicaBelgicaBulgariaAssociationofHomeopathicPhysiciansinBulgariaBulgarianAssociationofTraditionalChineseMedicineCyprusCyprusMedicalHomeopathicAssociationPancyprianMedicalSocietyofAcupunctureCzechRepublicCeskáLekarskaHomeopatickáSpolecnostCeskáSpolecnostAnthroposofickýchLékaruCeskáLekarskaAkupunkturickáSpolecnostDenmarkDanskMedicinskSelskabforAkupunktur.DanskSelskabforantroposofiskMedicinDanishSocietyforEvidenceBasedAcupuncture‐DSEAEstoniaEestiAkupunktuuriAssotsiatsioonEestiAntroposoofilisteArstideSeltsEestiHomöpaatiaÜhingFinland
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 25 –
AntroposofisenlääketieteenlääkäriyhdistysryFinnishMedicalAcupunctureSocietyFranceAssociationFrançaised'AcupunctureAssociationFrançaisepourl'EtudeetlaRechercheenAcupunctureAssociationMédicaleAnthroposophiqueFrançaise‐AMAFAssociationScientifiquedesMédecinsAcupuncteursdeFranceClubsMédecineetInformatique‐CMIFédérationdesAcupuncteurspourlaFormationMedicaleContinue‐FAFORMECFédérationFrançaisedesMédecinsHoméopathesClassiquesGroupementdesPédiatresHoméopathesd'ExpressionFrançaiseOdontologieEnergétiqueThérapeutique‐ODENTHSyndicatNationaldesMédecinsHoméopathesFrançaisGermanyÄrztegesellschaftfürErfahrungsheilkundee.V.‐EHKÄrztlicheAktionsgemeinschaftfürTherapiefreiheite.V.BundesverbandderniedergelassenennaturheilkundlichtätigenZahnärzteinDeutschlande.V.‐BNZDeutscheÄrztegesellschaftfürAkupunkture.V.DeutscheGesellschaftfürAkupunkturundNeuraltherapiee.V.‐DgfANDeutscheGesellschaftfürBiologischeMedizinundInformatik‐DGBMIDeutschemedizinischeArheitsgemeinschaftfürHerd‐undRegulationsforschung‐DAHDeutscherZentralvereinHomöopathischerÄrzteGemeinnützigesGemeinschaftskrankenhausHerdeckeGemeinnützigerVereinzurEntwicklungvonGemeinschaftskrankenhäuserne.V.GermanResearchInstituteofChineseMedicineGesellschaftAnthroposophischerÄrzteinDeutschlande.V.GesellschaftfürPhytotherapieHartmannbundVerbandderniedergelassenenÄrzteDeutschlandsHessischerÄrzteverbandNaturheilverfahrene.V.InstitutfürAntihomotoxischeMedizinundGrundregulationsforschungInternationalAssociationandNetworkforYamamotoNewScalpAcupunctureMatrix‐GesellschaftZentralverbandderÄrztefürNaturheilverfahren–ZÄNGreeceHellenicHomeopathicMedicalSocietyHellenicMedicalAcupunctureSocietyMedicalAcupunctureSocietyofNorthernGreecePanhellenicMedicalAcupunctureSocietyHungaryHungarianMedicalAcupunctureAssociationMagyarHomeopataOrvosiEgyesületIrelandIrishMedicalAcupunctureSocietyItalyAssociazioneMedicaItalianadiAgopunturaAssociazioneMedicaItalianadiElettroAgopunturasecondoVoll‐AMIDEAVAssociazioneTerapieNaturale‐ATeNaAssociationforResearchandScientificImprovement‐ARIASCentroStudiOmeopatiaClinicaAgopunturaePsicoterapiaCSOCAPFederazioneItalianadelleAssociazioniedeiMediciOmeopatiFondazioneMatteoRicciItalianAssociationofManualMedicineandNeuroreflexotherapy‐AIMAR
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 26 –
SocietàItalianadiMedicinaAntroposoficaSocietàItalianadiMedicinaOmeopaticaSocietàItalianadiOmeopatiaeMedicinaIntegrataLatviaLatvianMedicalSociety.AssociationofAcupunctureandRelatedTechniquesLatvijasHomeopatuAsociacijaLatvijasantroposofoārstuasociācijaLithuaniaAcupuncturegroupofKaunasUniversityofMedicineLietuvosHomeopatuAsocijacijaLituanianMedicalDoctorsAssociationofAcupunctureandTraditionalMedicineLuxemburgAssociationluxembourgeoisedesmédecins‐acupuncteursNetherlandsArtsenverenigingvoorhomeopathieVHANNederlandseArtsenAcupunctuurVerenigingNederlandseVerenigingvanAnthroposofischeArtsenNorwayNorskeLegersForeningforAntroposofiskMedisinNorwegianSocietyofMedicalAcupuncture,Physician'sSectionPolandLubelskieStowarzyszenieLekarzyHomeopatowiFarmaceutowMalopolskieStowarzyszenieLekarzyHomeopatowNadbaltyckieStowarzyszenieHomeopatówLekarzyFarmaceutówiWeterynarzyPolskieTowarzystwoAkupunkturyPolskieTowarzystwoHomeopatycznePolskiTowarzystwoMedycynyAntropozoficznejPomorskieStowarzyszenieHomeopatowLekarzyiFarmaceutowStowarzyszenieHomeopatowLekarzyiFarmaceutowRegionuLodzkiegoWielkopolskieStowarzyszenieLekarzyHomeopatowiFarmaceutowPortugalMedicalAcupunctureSocietyofPortugalSociedadeHomeopáticadePortugalSociedadeMédicaHomeopáticadePortugalSociedadeMédicaPortuguesaOzono‐OxigenioTerapia,Lda.SociedadeMédicaPortuguesaRegulaçaoeTerapiaNeuralsegundoHuneke,Lda.SociedadePortuguesadeHomeopatia RomaniaAsociațieiMedicilorpentruoMedicinăCompletatăcuCunoştințeAntroposoficeRomanianAcupunctureSocietyTranssylvanianAssociationofIntegratedQuantumMedicineSocietateaRomanadeHomeopatieSlovakiaSlovakMedicalSocietyofAcupunctureintheSlovakMedicalAssociationSlovenskáhomeopatickáspolocnostSloveniaSlovenianAssociationofAcupunctureandTraditionalChineseMedicineSlovenskohomeopatskodrustvo
– Complementary medicine (CAM) – Its current position and its potential for European healthcare –
– 27 –
SpainAcademiaMédicoHomeopáticadeBarcelonaAcupuncturistSection,OfficialCollegeofPhysicians,BarcelonaAsociaciónCientíficadeMédicosAcupuntoresdeSevilla"Huangdi"AsociaciónMédicaEspañoladeElectroacupunturasegunVoll‐AMEDEVAsociaciónMédicaEspañoladeHomeopatiayBioterapíaFederaciónEspañoladeMédicosHomeópatasGrupoMasterUniversitariodeAcupuncturaNuevaAsociaciónMédicaAntroposóficadeEspaña(NAMA)SociedadEspañoladeOrganoterapíayOrganologíaSwedenLäkarföreningenförAntroposofiskOrienteradMedicin(LAOM)SwedishMedicalAcupunctureSocietySwitzerlandSchweizerischeÄrztegesellschaftfürErfahrungsmedizin‐SAGEMSchweizerischerVereinHomöopathischerÄrzteVereinigunganthroposophischorientierterÄrzteinderSchweizUnitedKingdomAnthroposophicalMedicalAssociationBritishDentalAcupunctureSocietyBritishMedicalAcupunctureSocietyFacultyofHomeopathy