comparing support to breast cancer patients from online communities and face-to-face support groups
TRANSCRIPT

Patient Education and Counseling 85 (2011) e95–e100
Short communication
Comparing support to breast cancer patients from online communities andface-to-face support groups
Yoko Setoyama a,*, Yoshihiko Yamazaki b, Kazuhiro Nakayama a
a Department of Nursing Informatics, St. Luke’s College of Nursing, Tokyo, Japanb Department of Health Sociology, Graduate School of Health Sciences and Nursing, The University of Tokyo, Japan
A R T I C L E I N F O
Article history:
Received 18 April 2010
Received in revised form 15 November 2010
Accepted 21 November 2010
Keywords:
Japan
Breast cancer
Online community
Support resource
Face-to-face support group
A B S T R A C T
Objective: To compare support for three groups by considering usage patterns with regard to two peer
support resources, online communities, and face-to-face support groups, among patients with breast
cancer in Japan.
Methods: We conducted a cross-sectional survey of 1039 breast cancer patients.
Results: Factor analysis indicated that all groups show the five aspects of support: ‘‘Emotional support/
Helper therapy,’’ ‘‘Emotional expression,’’ ‘‘Conflict,’’ ‘‘Advice,’’ and ‘‘Insight/Universality.’’ Within the
group using two support resources, the support scores of ‘‘Emotional expression’’ and ‘‘Advice’’ were
higher for the online community, and those of ‘‘Emotional support/Helper therapy,’’ and ‘‘Insight/
Universality’’ were higher for the face-to-face support group. Among the three groups, the members who
received the most peer support were those who used both an online community and a face-to-face
support group.
Conclusion: Patients who received the most social support from peers were in the group using both
online communities and face-to-face support groups.
Practice implications: Healthcare providers should provide information about peer support through not
only traditional face-to-face support groups but also online communities.
� 2010 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Patient Education and Counseling
jo ur n al h o mep ag e: w ww .e lsev ier . co m / loc ate /p ated u co u
1. Introduction
Participants in face-to-face support groups received emotional,informational, and practical support [1,2]. Such participation wasfound to positively affect social aspects and the overall quality oflife [QOL] [3,4], aiding patients in coping with their stressfulsituation [5].
Recently, Sharf asserted that breast cancer patients exchangedsocial support online [6,7] and that those were useful in variouspsycho-social aspects [8,9]. Winzelberg et al. found onlinecommunities comparable in effectiveness to face-to-face supportgroups [8].
However, little is known about how the functions of support ofeach resource differ and what usage of both resources is desirable.Additionally, despite the Internet penetration rate in Japan [10],research on Japanese online communities and non-Englishlanguage studies is limited [11]. Therefore, through a cross-
* Corresponding author at: St. Luke’s College of Nursing, 10-1, Akashi-cho, Chuo-
ku, Tokyo 104-0044, Japan. Tel.: +81 3 3543 6391; fax: +81 3 5494 8633.
E-mail address: [email protected] (Y. Setoyama).
0738-3991/$ – see front matter � 2010 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.pec.2010.11.008
sectional design survey, we sought to compare three groups byconsidering the usage patterns of peer support resources andinvestigate the desirable usage of the resources.
2. Methods
2.1. Survey procedure
We conducted a simultaneous online and postal surveybetween August and September 2007, using questionnairesdeveloped from pre-interviews with some patients and nurses.We conducted a pretest with 81 patients.
2.2. Online survey
We searched for online communities using the Google JAPANand Yahoo! JAPAN search engines, employing the keywords‘‘breast cancer’’ and ‘‘discussion board [keijiban in Japanese]’’ or‘‘mailing list.’’ Twelve different communities were found. Weeliminated online communities managed by healthcare providersand included patients with cancers other than those of the breastas participants. The final number of online communities among the

Y. Setoyama et al. / Patient Education and Counseling 85 (2011) e95–e10096
12 was 4. From about 1000 enrollments on the 4 onlinecommunities, 465 patients accessed the survey and 220 completedthe questionnaire (response rate: 47.3%).
2.3. Postal survey
We searched for face-to-face support groups, using the samesearch engines and the keywords ‘‘breast cancer [nyuu gan inJapanese]’’ and ‘‘face-to-face support group [kanjakai in Japanese].’’We contacted 41 administrators from out of 98 groups, and thefinal number of groups surveyed was 29. From among 1887enrollments in the support groups, 1019 members completed thequestionnaire (response rate: 53.8%).
To ensure a homogeneous sample, we excluded 200 partici-pants whose cancer had recurred (n = 168), had not had anysurgery (n = 21), and had an extremely low daily activity level(‘‘almost staying in bed’’) (n = 11), leaving 1039 valid responses.Although the ages of the online and postal survey participantsdiffered significantly, controlling for the age variable resulted in nosignificant differences between the two groups.
2.4. Instruments
The survey inquired about patients’ socio-demographic vari-ables (see Table 1). Respondents were asked to report on fivedisease-related characteristics: (1) time since diagnosis of breastcancer; (2) stage of cancer at the time of diagnosis; (3) physicalsymptoms due to breast cancer or its treatment, using multiplechoice; (4) personal daily activity level, indicating physicalcondition, asked using a 5-point Likert scale, responses to whichcould be revised into three categories on analysis; and (5)treatments received.
We asked about respondents’ current participation in eitheronline communities or face-to-face support groups. The timerespondents began using these resources was noted.
We also identified participants’ initial expectations of the peersupport resources from social support research [12]. Patients ratedtheir levels of anxiety and depression on the Hospital Anxiety andDepression Scale [HADS] [13]. We used the Japanese version [14] ofthis scale, by which a higher score indicates greater anxiety anddepression. Cronbach’s a coefficient was 0.91.
Thirty-four original items were developed based on the self-help group theory proposed by Mishima [2] and other researches[15,16]. The response items were on a 5-point Likert scale from 5
‘‘strongly agree’’ to 1 ‘‘strongly disagree.’’ Respondents using bothonline communities and face-to-face support groups had to eachanswer the questions. These items were checked by nurses expertsas to face validity.
2.5. Statistical analysis
First, we categorized participants into the following threegroups: ‘‘participants using only online communities (n = 127),’’‘‘participants using both online communities and face-to-facesupport groups (n = 374),’’ and ‘‘participants using only face-to-face support groups (n = 538).’’
To state factor constructions for each group, we conductedfactor analysis with promax rotation four times separately inrelation to peer support function from the following: (1) onlinecommunities for the participants using only online communities;(2) online communities for the participants using both supportresource; (3) face-to-face support groups for the participants usingboth support resources; and (4) face-to-face support groups for theparticipants using only face-to-face support groups.
We calculated the total scores by simply adding up the scores ofall the items for each support function, calling this the ‘‘support
score.’’ These support scores were converted out of 100 points.We conducted a t-test to compare the scores within the groupusing both support resources. Additionally, to compare the peersupport received by each group, we conducted an ANCOVAsabout support scores, controlling for age, marital status,education, working conditions, and time since diagnosis. Forthe middle group, in which people used both an onlinecommunity and a face-to-face support group, we used theaverage of each support score from the online community andthat from the face-to-face support group.
3. Results
3.1. Participant characteristics
Table 1 shows the characteristics of respondents. Amongparticipants using only online communities, 210 (42.0%) beganusing them ‘‘just after their diagnosis.’’ However, among partici-pants using only face-to-face support groups, 457 (50.2%) beganusing them later ‘‘after finishing the first treatment,’’ and 344(37.8%) began using them ‘‘after beginning the first treatment.’’More than 80% in each of the three groups expected ‘‘informationalsupport’’ from each resource during their first use.
3.2. Support functions
We performed principal axis factor extractions with promaxrotation. Excluding items with more than one factor loading above0.4, the 5-factor solution for each separate analysis was simplystructured and most interpretable in the context of previoustheories; therefore, we adopted 5 factors as the function of eachsupport resource. The five peer support factors are presented inTable 2. We extracted the same 5 factors from 4-times factoranalysis. They were ‘‘Emotional support/Helper therapy,’’ ‘‘Emo-tional expression,’’ ‘‘Conflict,’’ ‘‘Advice,’’ and ‘‘Insight/Universality.’’Each factor had a Cronbach’s a above 0.8.
3.3. The amount of peer support received by each group
Fig. 1 shows the result of the ANCOVAs, which yielded the fivesupport scores for each group. The four positive support scores(Emotional support/Helper Therapy, Emotional expression, Advice,Insight/Universality) were significantly high in the middle group,in which members used both support resources.
Though it did not showed on the figure, within the middlegroup, using both support resources at the same time, wecompared the support scores between online community andface-to-face support scores. The ‘‘Emotional expression (supportscore of online community = 67.3, support score of face-to-facesupport group = 51.3, p < .001)’’ and ‘‘Advice (62.8, 56.3, p = .038)’’scores were higher for online communities, Support scores for‘‘Emotional support/Helper therapy (60.5, 73.5, p < .001)’’ and‘‘Insight/Universality (70.1, 80.3, p < .001)’’ were, conversely,higher for face-to-face support groups.
4. Discussion and conclusion
4.1. Discussion
The differences in the mean ages of the three groups wereassumed to arise from familiarity with the Internet and supportedprevious research findings [17]. In terms of online communities,this age distribution was wider than Roger’s research sample [18],perhaps because of recent Internet penetration among the olderpopulation [19]. The ages of our sample reflected the ages ofJapanese breast cancer patients [20].

Table 1Sociodemographic characteristics of participants by type of support group N = 1039.
Participants using
only online
communities
(n = 127a)
Participants using both
online communities
and face-to-face
support
groups (n = 374a)
Participants using
only face-to-face
support groups
(n = 538a)
p-Value
n % n % n %
Demographic characteristics
Age
�29 3 (2.5) 4 (1.1) 0 (0) .000b
30–39 23 (19.0) 36 (9.7) 6 (1.1)
40–49 74 (61.2) 129 (34.7) 72 (13.4)
50–59 18 (14.9) 143 (38.4) 186 (34.6)
60–69 3 (2.5) 45 (12.1) 187 (34.8)
70–79 0 (0) 14 (3.8) 79 (14.7)
80+ 0 (0) 1 (0.3) 7 (1.3)
Mean � SD 43.6 �7.4
51.2 �9.4
60.0 �9.4
Marital status
Unmarried 24 (19.8) (42) (11.3) 42 (7.9) .000b
Married 84 (69.4) (297) (80.1) 379 (71.2)
Separated/widowed 13 (10.7) (32) (8.6) 111 (20.9)
Education
Middle school 0 (0.0) 9 (2.4) 47 (8.9) .000b
High school 27 (22.5) 136 (36.8) 235 (44.4)
Vocational school/2 year-college 47 (38.2) 142 (38.4) 146 (27.6)
University/graduate school or higher 46 (38.3) 83 (22.4) 101 (19.1)
Working conditions
Full-time job 34 (28.1) 82 (22.0) 59 (11.1) .000b
Housewife 33 (27.3) 133 (35.8) 227 (42.7)
Part-time job 31 (25.6) 86 (23.1) 94 (17.7)
Unemployed 23 (19.0) 71 (19.1) 152 (28.6)
Disease related characteristics
Time since the diagnosis
Less than 1 year 63 (50.0) 49 (13.1) 48 (8.9) .000d
1–2 years 45 (35.7) 112 (29.9) 103 (19.1)
3–5 years 14 (11.1) 107 (28.6) 149 (27.7)
6–9 years 2 (1.6) 83 (22.2) 136 (25.3)
More than 10 years 2 (1.6) 23 (6.1) 102 (19.0)
Cancer stage at diagnosis
Stage I 58 (46.4) 138 (37.6) 181 (34.5) .000b
Stage II 54 (43.2) 154 (42.0) 154 (29.3)
Stage III 9 (7.2) 41 (11.2) 78 (14.9)
Not known 4 (3.2) 34 (9.3) 112 (21.3)
Symptomse
Patients with symptom/s 109 (85.8) 292 (78.1) 350 (65.1) .000b
Patients with no symptom/s 18 (14.2) 82 (21.9) 188 (34.9)
Total number of symptoms; mean � SD 1.8 � 1.6 1.9 � 1.4 1.8 � 1.3 .721c
Physical condition
Living completely as usual 63 (49.6) 234 (62.6) 358 (66.5) .025d
Living not completely as usual 64 (50.4) 140 (37.4) 180 (33.5)
Treatment <multiple choices>
Breast mastectomy 40 (31.5) 191 (51.1) 334 (62.1) .000b
Conservative breast surgery 90 (70.9) 190 (50.8) 215 (40.0) .000b
Chemotherapy 58 (45.7) 193 (51.6) 198 (36.8) .000b
Radiation therapy 63 (49.6) 189 (50.5) 205 (38.1) .000b
Hormone therapy 48 (37.8) 240 (64.2) 315 (58.6) .000b
Alternative medicine 5 (3.9) 63 (16.8) 56 (10.4) .000b
Other 2 (1.6) 26 (7.0) 25 (4.6) .004b
HADS
Summate scores; mean � SD 12.7 � 7.3 12.0 � 8.7 10.3 � 8.4 .036c
Anxiety 6.6 � 4.4 5.6 � 4.8 4.6 � 4.4 .001c
Depression 6.1 � 3.5 6.4 � 4.7 5.7 � 4.5 .674c
a Excluded missing data.b x2 test.c Oneway.d Kruskal–Wallis test.e Respondents listed all the current symptoms they had due to breast cancer (e.g., ‘‘pain,’’ ‘‘feeling of weariness,’’ ‘‘paralysis of arm,’’ and ‘‘nausea’’). They were classified into
‘‘patients with symptoms’’ if they reported more than one symptom.
Y. Setoyama et al. / Patient Education and Counseling 85 (2011) e95–e100 e97
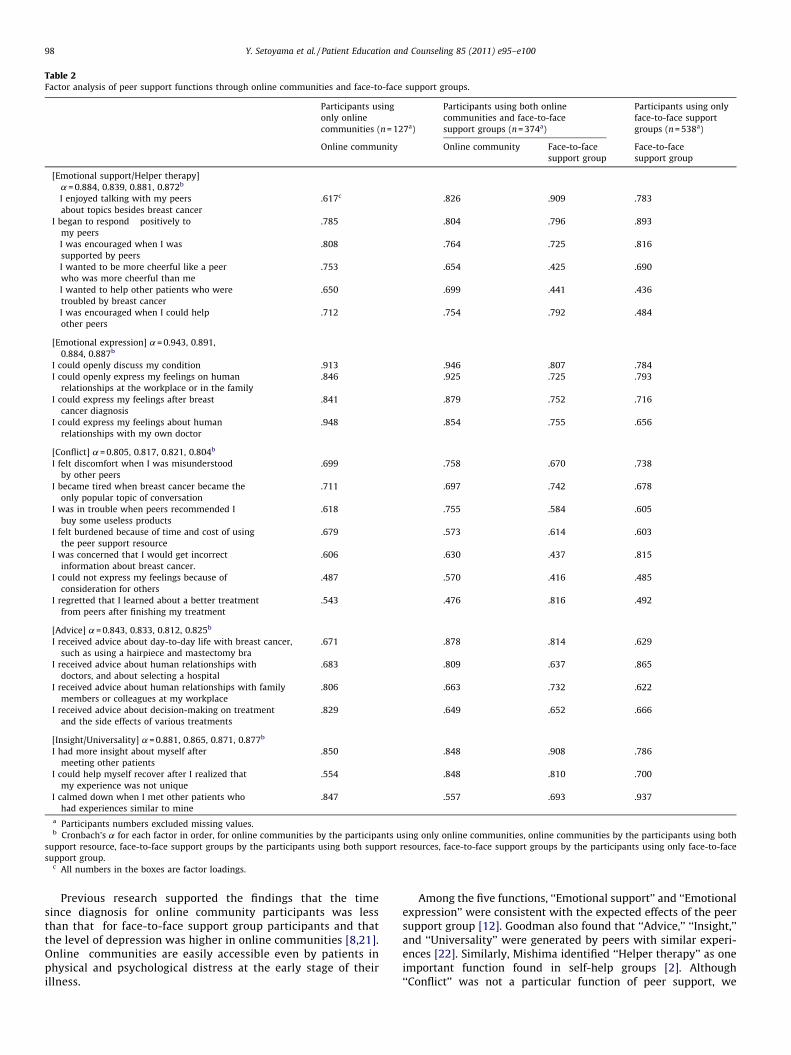
Table 2Factor analysis of peer support functions through online communities and face-to-face support groups.
Participants using
only online
communities (n = 127a)
Participants using both online
communities and face-to-face
support groups (n = 374a)
Participants using only
face-to-face support
groups (n = 538a)
Online community Online community Face-to-face
support group
Face-to-face
support group
[Emotional support/Helper therapy]
a = 0.884, 0.839, 0.881, 0.872b
I enjoyed talking with my peers
about topics besides breast cancer
.617c .826 .909 .783
I began to respond positively to
my peers
.785 .804 .796 .893
I was encouraged when I was
supported by peers
.808 .764 .725 .816
I wanted to be more cheerful like a peer
who was more cheerful than me
.753 .654 .425 .690
I wanted to help other patients who were
troubled by breast cancer
.650 .699 .441 .436
I was encouraged when I could help
other peers
.712 .754 .792 .484
[Emotional expression] a = 0.943, 0.891,
0.884, 0.887b
I could openly discuss my condition .913 .946 .807 .784
I could openly express my feelings on human
relationships at the workplace or in the family
.846 .925 .725 .793
I could express my feelings after breast
cancer diagnosis
.841 .879 .752 .716
I could express my feelings about human
relationships with my own doctor
.948 .854 .755 .656
[Conflict] a = 0.805, 0.817, 0.821, 0.804b
I felt discomfort when I was misunderstood
by other peers
.699 .758 .670 .738
I became tired when breast cancer became the
only popular topic of conversation
.711 .697 .742 .678
I was in trouble when peers recommended I
buy some useless products
.618 .755 .584 .605
I felt burdened because of time and cost of using
the peer support resource
.679 .573 .614 .603
I was concerned that I would get incorrect
information about breast cancer.
.606 .630 .437 .815
I could not express my feelings because of
consideration for others
.487 .570 .416 .485
I regretted that I learned about a better treatment
from peers after finishing my treatment
.543 .476 .816 .492
[Advice] a = 0.843, 0.833, 0.812, 0.825b
I received advice about day-to-day life with breast cancer,
such as using a hairpiece and mastectomy bra
.671 .878 .814 .629
I received advice about human relationships with
doctors, and about selecting a hospital
.683 .809 .637 .865
I received advice about human relationships with family
members or colleagues at my workplace
.806 .663 .732 .622
I received advice about decision-making on treatment
and the side effects of various treatments
.829 .649 .652 .666
[Insight/Universality] a = 0.881, 0.865, 0.871, 0.877b
I had more insight about myself after
meeting other patients
.850 .848 .908 .786
I could help myself recover after I realized that
my experience was not unique
.554 .848 .810 .700
I calmed down when I met other patients who
had experiences similar to mine
.847 .557 .693 .937
a Participants numbers excluded missing values.b Cronbach’s a for each factor in order, for online communities by the participants using only online communities, online communities by the participants using both
support resource, face-to-face support groups by the participants using both support resources, face-to-face support groups by the participants using only face-to-face
support group.c All numbers in the boxes are factor loadings.
Y. Setoyama et al. / Patient Education and Counseling 85 (2011) e95–e10098
Previous research supported the findings that the timesince diagnosis for online community participants was lessthan that for face-to-face support group participants and thatthe level of depression was higher in online communities [8,21].Online communities are easily accessible even by patients inphysical and psychological distress at the early stage of theirillness.
Among the five functions, ‘‘Emotional support’’ and ‘‘Emotionalexpression’’ were consistent with the expected effects of the peersupport group [12]. Goodman also found that ‘‘Advice,’’ ‘‘Insight,’’and ‘‘Universality’’ were generated by peers with similar experi-ences [22]. Similarly, Mishima identified ‘‘Helper therapy’’ as oneimportant function found in self-help groups [2]. Although‘‘Conflict’’ was not a particular function of peer support, we

60.2
52.2
24.4
55.9 62.4
67.0 59.3
28.6
59.6
75.2
61.5
54.6
28.6
53.7
70.2
0.0
20.0
40.0
60.0
80.0
100.0
Emo�onal support/Helper therapy
Emo�onal Expression Conflict Adv ice Insight/ Universality
Par�cipants using only online communi�e s(n = 127)Par�cipants using both online communi�es and face-to-face support gr oups(n = 374)Par�cipants using only face-to-face supp ort group s(n = 538)
P<.001
P<.001 P=.021
P=.00 1
P<.00 1 P=.003
P=.00 4
P=.039
P=.02 3
P=.03 7
P=.047
Fig. 1. Support scores which each group gain from peer. (ANCOVAs controlling for age, marital status, education, working conditions, and time since diagnosis ‘‘Support
scores’’, calculated total scores by simply adding up the scores of all the items for each support function. Then those scores were converted out of 100 points.)
Y. Setoyama et al. / Patient Education and Counseling 85 (2011) e95–e100 e99
included it as a negative social support event, following Goodman[22]. Our study reaffirmed that breast cancer patients can receivethe same functions of peer support from both online communitiesand face-to-face support groups [18].
In terms of support scores, the group using both supportresources received the most peer support and even controlled forsignificantly different variables among the three groups.
With regard to the group using both support resources, the‘‘Emotional expression’’ score was higher for online communities;Coulson attributed this to online anonymity, which makes it easierto express feelings [23]. People with definite questions (abouttreatment or its side effects, for instance) may first seek answersonline; thus, it is natural that the ‘‘Advice’’ score is higher for onlinecommunities. Support scores for ‘‘Emotional support/Helpertherapy’’ and ‘‘Insight/Universality’’ were, conversely, higher forface-to-face support groups. It would appear that the participantscould establish a closer relationship with other members in face-to-face support groups. Our study implies that online communitiesand face-to-face support groups have different characteristicsdespite the five similar peer support functions.
As for the amount of peer support received by each group, thegroup using both support resources simultaneously received themost support. It is possible that the two resources are comple-mentary to each other. It is therefore recommended that bothresources be used simultaneously by people seeking peer supportin the course of their recuperation. Although evidence on theeffectiveness of traditional face-to-face support groups in Japanhas accumulated, people can gain greater peer support benefit bysimultaneously using another support resource.
Sampling bias must be considered. It is possible that patientsevaluated the resources more positively. Because of the cross-sectional design, we cannot reveal the causal association betweenresource use and health outcomes. Despite these limitations, thisstudy was valuable in showing that using more than one resourcesimultaneously could be effective in seeking peer support. Thisstudy is also highly valuable because it uses data of Japanese breastcancer patients.
4.2. Conclusion
The group that received the most social support from peers wasthat which simultaneously used support from both online
communities and face-to-face support groups. Healthcare provi-ders should provide information on both peer support resources,because people who already participate in face-to-face supportgroups can receive further peer support benefits through anothersupport resource.
Acknowledgements
We wish to thank the patients who cooperated in our surveyand the members of the Department of Health Sociology, TheUniversity of Tokyo. This research was supported by 2007 BasicResearch Grant (A) from the Ministry of Education, Sports, Culture,Science and Technology.
References
[1] Gray R, Fitch M, Davis C, Phillips C. A qualitative study of breast cancer self-help groups. Psychooncology 1997;6:279–89.
[2] Mishima I. Self-help-group no kinou to yakuwari [The functions and role ofself-help groups] In: Kubo H, Ishikawa T, editors. Self-help-group no riron totenkai. [The theory and practice of self-help groups]3rd ed., Tokyo: Chuou-houki; 2001.
[3] Michalec B. Exploring the multidimensional benefits of breast cancer supportgroups. J Psychosoc Oncol 2005;23:159–79.
[4] Song Y, Lindquist R, Windenburg D, Cairns B, Thakur A. Review of outcomes ofcardiac support groups after cardiac events, Western journal of nursingresearch; in press.
[5] Pinheiro CP, da Silva RM, Mamede MV, Fernandes AF. Participating in a supportgroup: experience lived by women with breast cancer. Rev Lat Am Enferma-gem 2008;16:733–8.
[6] Fox S. Online Health Research; 2006. Available from: http://www.pewinternet.org/Reports/2006/Online-Health-Search-2006.aspx [cited 2008/6/30].
[7] Sharf BF. Communicating breast cancer on-line: support and empowerment onthe Internet. Women Health 1997;26:65–84.
[8] Winzelberg AJ, Classen C, Alpers GW, Roberts H, Koopman C, Adams RE, et al.Evaluation of an Internet support group for women with primary breastcancer. Cancer 2003;97:1164–73.
[9] Lieberman MA, Goldstein BA. Self-help on-line: an outcome evaluation ofbreast cancer bulletin boards. J Health Psychol 2005;10:855–62.
[10] Union IT. ITU global view: a comprehensive view of current telecommunica-tions infrastructure, projects, and statistics; 2008. Available from: http://www.itu.int/net/home/index.aspx [cited 2008/10/10].
[11] Hoybye MT, Johansen C, Tjornhoj-Thomsen T. Online interaction. Effects ofstorytelling in an Internet breast cancer support group. Psychooncology2005;14:211–20.
[12] Cohen S, Underwood LG, Gottlieb BH, editors. Social support measurement andintervention. New York: Oxford University Press; 2000.
[13] Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the HospitalAnxiety and Depression Scale. An updated literature review. J Psychosom Res2002;52:69–77.

Y. Setoyama et al. / Patient Education and Counseling 85 (2011) e95–e100100
[14] Kugaya A, Akechi T, Okumura H, Uchitomi H. Screening for psychologicaldistress in Japanese cancer patients. Jpn J Clin Oncol 1998;28:333–8.
[15] Takahashi I, Ogasawara T, Kume Y. Gan taikensya no QOL ni taisuru jijyo groupno joutyo teki support no kouka [The effect of self-help group emotionalsupport on cancer survivors’ QOL] Nihon gan kango gakkaishi J Jpn Soc CancerNurs2004;18:14–24.
[16] Hirose H, Hisada M, Aoki Y, Ittetsu T, Shiraiwa H. Jutsu go nyu gan kanja notame no tanki support group no kinou ni kansuru shitsu teki kennkyu [Aqualitative study on the functions of time-limited support groups for post-surgical breast cancer patients: analyses of the group process] Gan kango[Cancer Nursing]2001;6:428–37.
[17] Fukui S, Kugaya A, Kamiya M, Koike M, Okamura H, Nakanishi T, et al. Participa-tion in psychosocial group intervention among Japanese women with primarybreast cancer and its associated factors. Psychooncology 2001;10:419–27.
[18] Rodgers S, Chen Q. Internet community group participation: psychosocialbenefits for women with breast cancer. J Comput Mediat Commun 2005;10:5.
[19] Soumusyou [Ministry of Internal Affairs and Communications]. Tsuushin riyoudoukou tyousa [Communication Use Trend Surrvey]; 2006. Available from:http://www.soumu.go.jp/johotsusintokei/statistics/statistics05a.html [cited2008/11/7].
[20] Matsuda T, Marugame T, Kamo K, Katanoda K, Ajiki W, Sobue T. Japan CancerSurveillance Research Group Cancer incidence and incidence rates in Japan in2003: based on data from 13 population-based cancer registries in theMonitoring of Cancer Incidence in Japan (MCIJ) project. Jpn J Clin Oncol2009;39:850–8.
[21] Klemm P, Hardie T. Depression in Internet and face-to-face cancer supportgroups: a pilot study. Oncol Nurs Forum 2002;29:e45–51.
[22] Goodman CC. Perceived social support for caregiving: measuring the benefit ofself-help/support group participation. J Gerontol Soc Work 1991;J16:163–75.
[23] Coulson NS, Buchanan H, Aubeeluck A. Social support in cyberspace: a contentanalysis of communication within a Huntington’s disease online supportgroup. Patient Educ Couns 2007;68:173–8.