comorbidities and complications of tbi - healthsouth .../media/hospital-sites...•can lead to...
TRANSCRIPT
Comorbidities and
Complications of TBI
Rocco A Chiappini, MD
TBI: A Disease Process, Not
an Event
• WHO definition of a chronic disease
– Permanent
– Caused by non-reversible pathological
alterations
– Requires special training of patient
– May require a long period of observation,
supervision or care
Masel and DeWitt,
J Neurotrauma 2010 • TBI increases long term mortality and
decreases life expectancy. It is associated with increased incidence of seizures, sleep disorders, neurodegenerative disease, neuroendocrine dysregulation and psychiatric diseases as well as non-neurologic disorders such as sexual dysfunction, bladder and bowel…
Masel and Dewitt
J Neurotrauma 2010
• … incontinence and systemic metabolic
dysregulation that may arise and/or
persist for months or years after injury.
TBI Complications and
Comorbidities
• Seizures
• Sleep disturbance
• Fatigue
• Infections
• Craniectomy
• Hydrocephalus
• Shunt issues
TBI Complications and
Comorbidities
• Subdural/Epidural Hematoma
• Neuro-endocrine dysfunction
• Spasticity
• Post-traumatic headache
Seizures
• TBI is the leading cause of epilepsy in
young adults
• Early seizures- within the first week
• Late seizures- after the first week
• Incidence of late seizures
– Nonpenetrating severe TBI 17%
– Penetrating TBI 35-65%
Seizures- risk factors
• Depressed skull
fracture
• Bone/metal
fragments
• Focal contusions
• Intracranial
hemorrhage

Gunshot wound
Types of Seizures
• Partial 25%
• Generalized 25%
• Partial with secondary generalization
50%
Frontal Lobe Epilepsy
• Complex, semipurposeful motor
automatisms
Temporal Lobe Epilepsy
• May have emotional symptoms like
panic followed by post-ictal confusion or
amnesia
Seizures
Current Recommendations
• Prophylaxis for the first week
• Discontinue prophylaxis and monitor
• Treat late seizures with carbamazepine,
valproate, lamotrigine or levetiracetam
• Avoid phenytoin
Sleep Disorders
• Guilleminault studied 184 TBI survivors
– Restless sleep 49%
– Regular loud snoring 36%
– Leg and body jerking during sleep 18%
Sleep Disorders
• Ouellet studied 452 TBI survivors (avg
time since injury 8 years)
– 50% had symptoms of insomnia
– 30% met criteria for insomnia (general
public 10%)
Sleep disorders
• TBI population
– Decreased REM
– Decreased total sleep time
– More frequent awakenings
– Decreased deep sleep stages
Sleep Disorders
Causes
• Damage to brain centers involved in
sleep (hypothalamus, midbrain,
ascending reticular activating system)
• Disruption of circadian pacemaker in the
hypothalamus with decrease in level of
melatonin production
Sleep Disorders
Causes
• Pain
• Depression
• Anxiety
• Medications
• Environment
Sleep Disorders
Treatment • Treat depression, anxiety, pain
• Treat sleep apnea if present
• Improve sleep hygiene
• Melatonin
• Hypnotics, TCAs, antiepileptics may be helpful although no studies have shown best pharmacotherapy for insomnia in TBI
Fatigue
• The awareness of a decreased capacity
for physical and/or mental activity due to
an imbalance in the availability,
utilization and/or restoration of
resources needed to perform activity.
Fatigue
• Physiologic- arises from depletion of
energy, hormones, neurotransmitters, or
neural connections
• Psychologic- weariness related to
reduced motivation, prolonged mental
activity or boredom
Fatigue
• Kreutzer found 46% of 722 outpatients
with TBI self reported fatigue
Fatigue
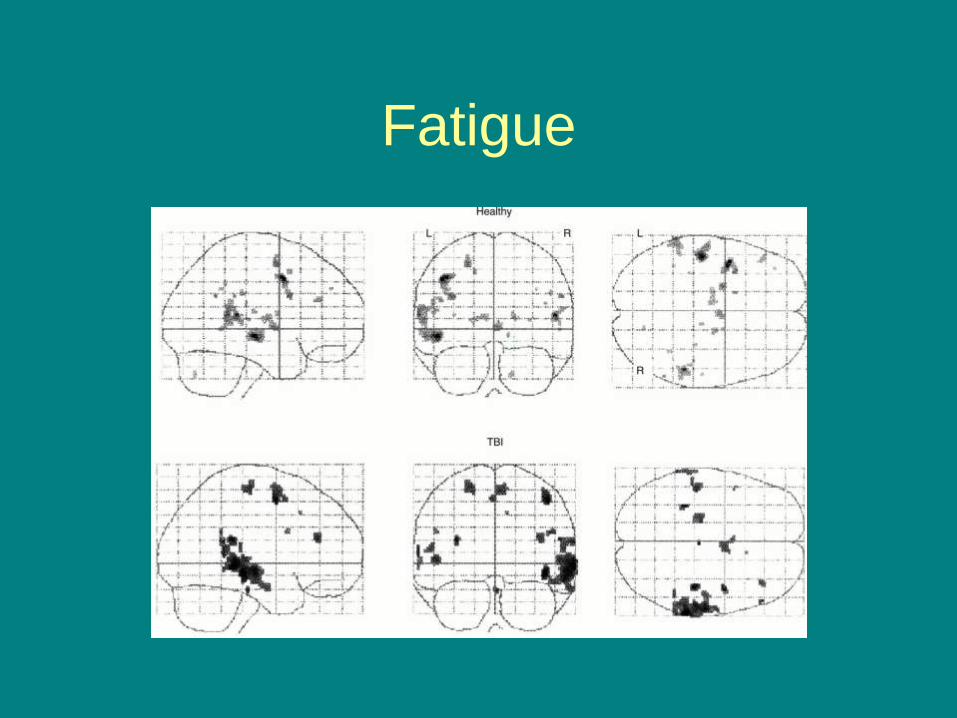
• May result from diffuse neuronal injury,
particularly from damage to brain
centers that control arousal, attention
and response speed including the
ARAS, limbic system, anterior cingulate,
basal ganglia
• Alteration in chemistry. Histamine and
growth factor.
Fatigue
Fatigue
Treatments • Exercise
• Sleep assessment
• Hormonal screening
• Light therapy
• Assessment of meds. D/C meds that increase
fatigue
• Try antidepressants with activating effect
• Modafinil
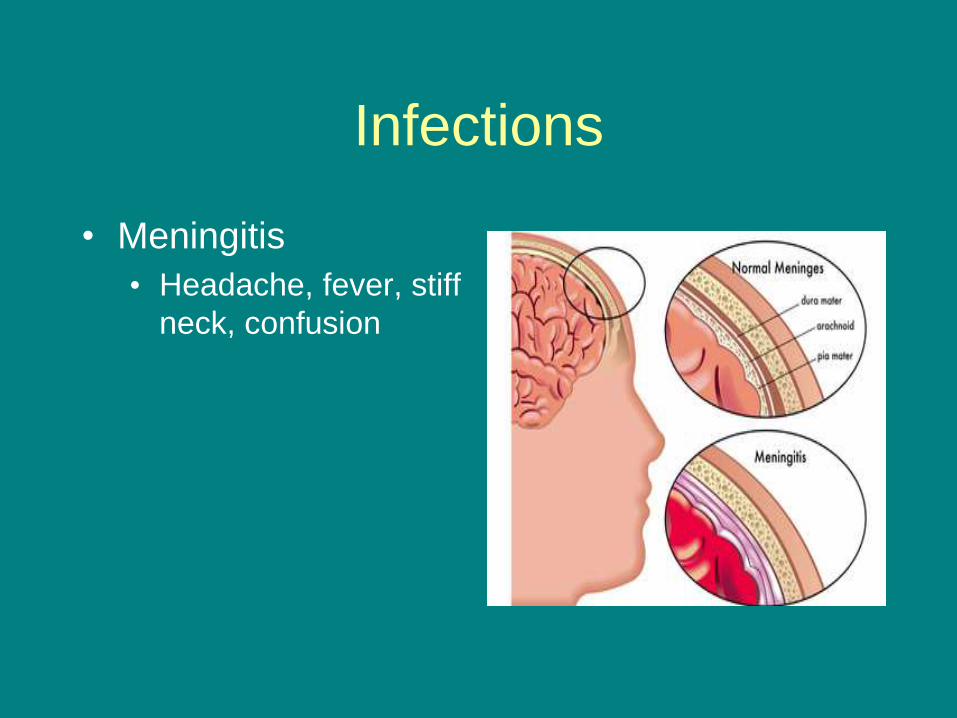
Infections
• Meningitis
• Headache, fever, stiff
neck, confusion
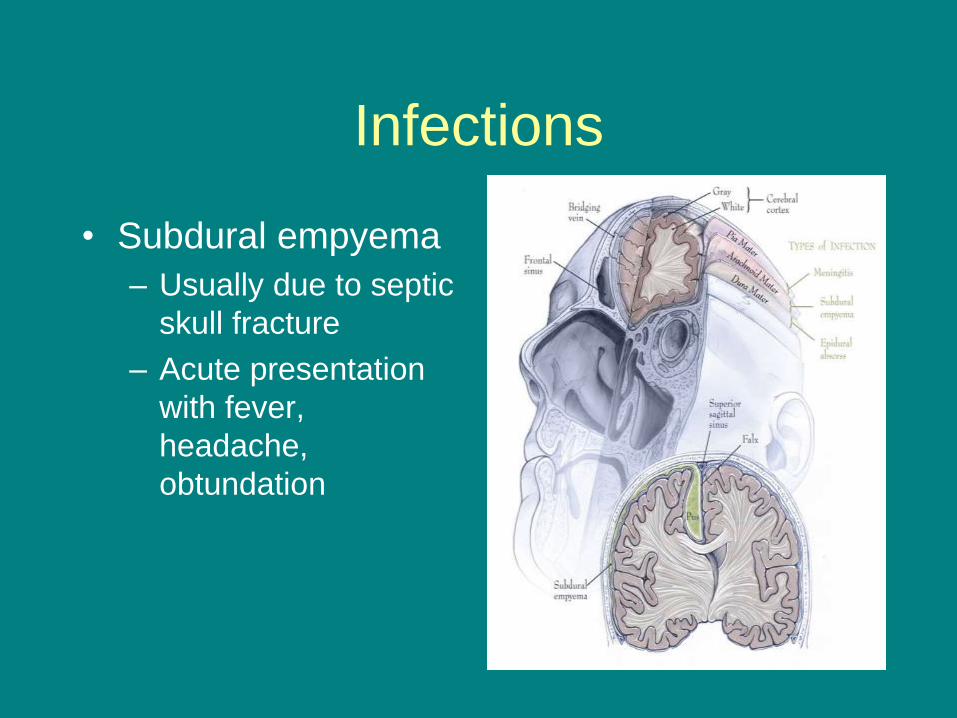
Infections
• Subdural empyema
– Usually due to septic
skull fracture
– Acute presentation
with fever,
headache,
obtundation
Infections
• Brain abscess
– 3 times more likely with gunshot wound
– Usually 2-3 weeks post injury
– Headache, vomiting, change in mental
status 50%, seizure 33%
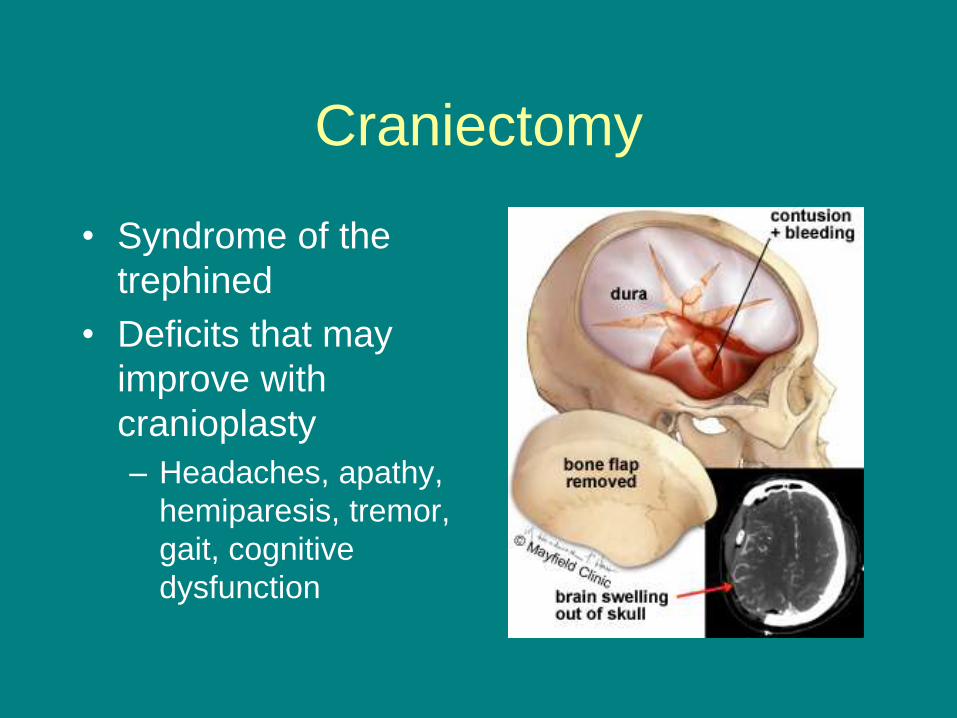
Craniectomy
• Syndrome of the
trephined
• Deficits that may
improve with
cranioplasty
– Headaches, apathy,
hemiparesis, tremor,
gait, cognitive
dysfunction
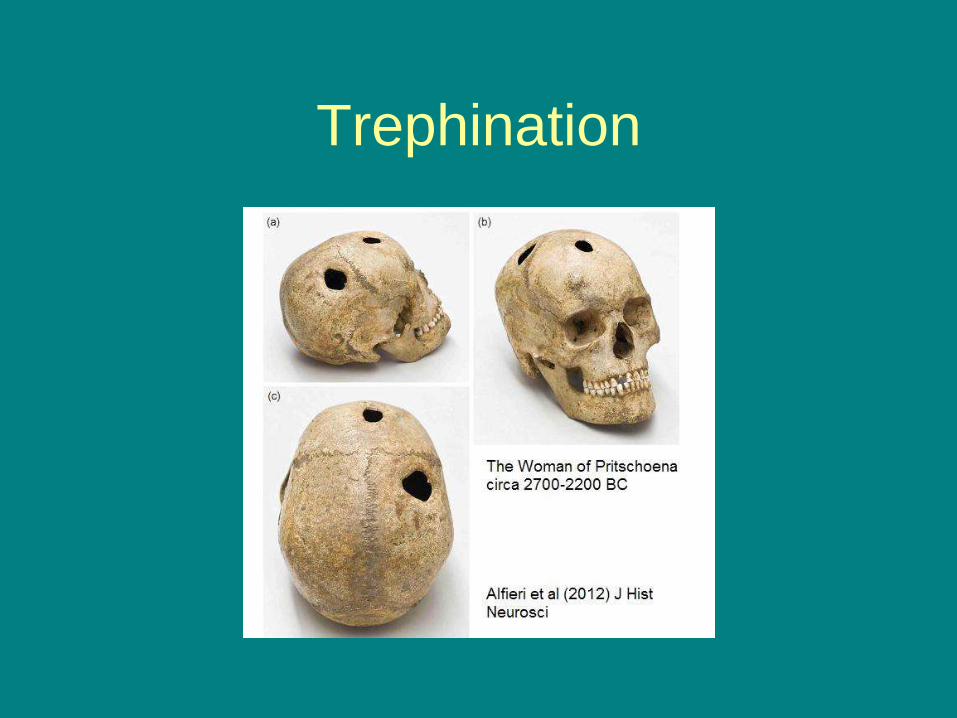
Trephination
Hydrocephalus
• Occurs in about 40% of patients with
severe TBI
• Usually begins to appear within the first
2 weeks post injury
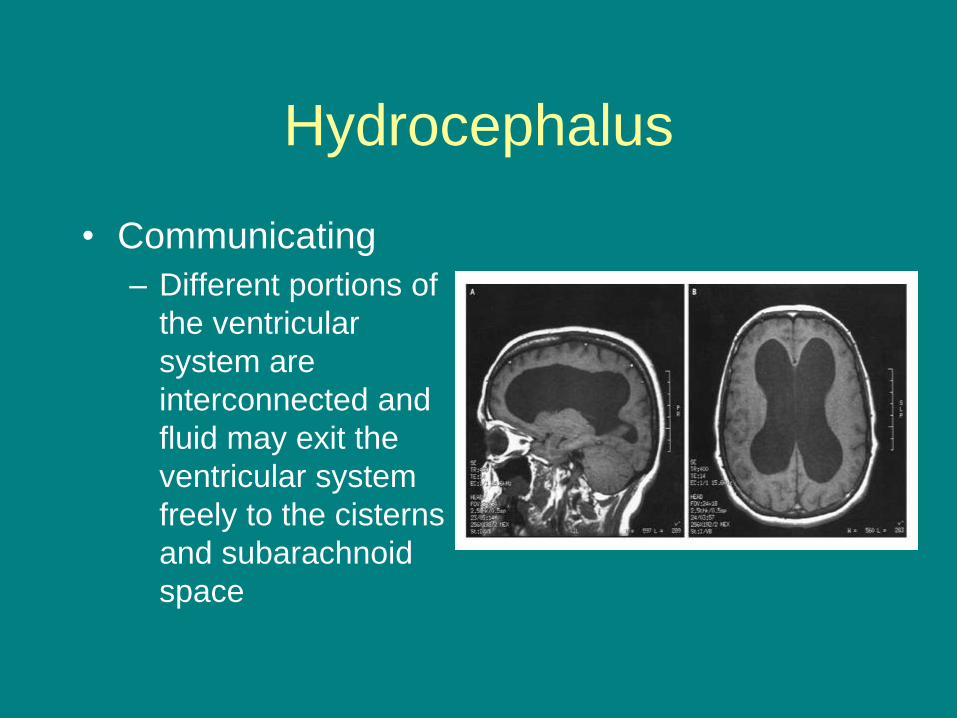
Hydrocephalus
• Communicating
– Different portions of
the ventricular
system are
interconnected and
fluid may exit the
ventricular system
freely to the cisterns
and subarachnoid
space
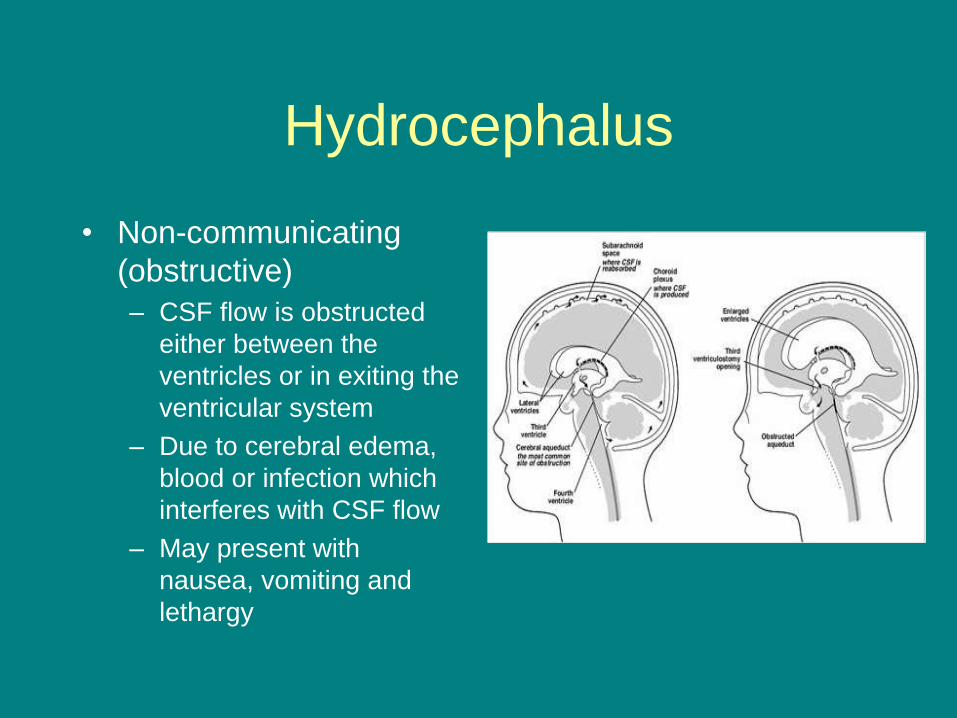
Hydrocephalus
• Non-communicating
(obstructive)
– CSF flow is obstructed
either between the
ventricles or in exiting the
ventricular system
– Due to cerebral edema,
blood or infection which
interferes with CSF flow
– May present with
nausea, vomiting and
lethargy
Shunting
• Study of 356 adults with VP shunts over
18 years. Incidence of revision 30%.
• Shunt failure
• Shunt infection
• Overdrainage
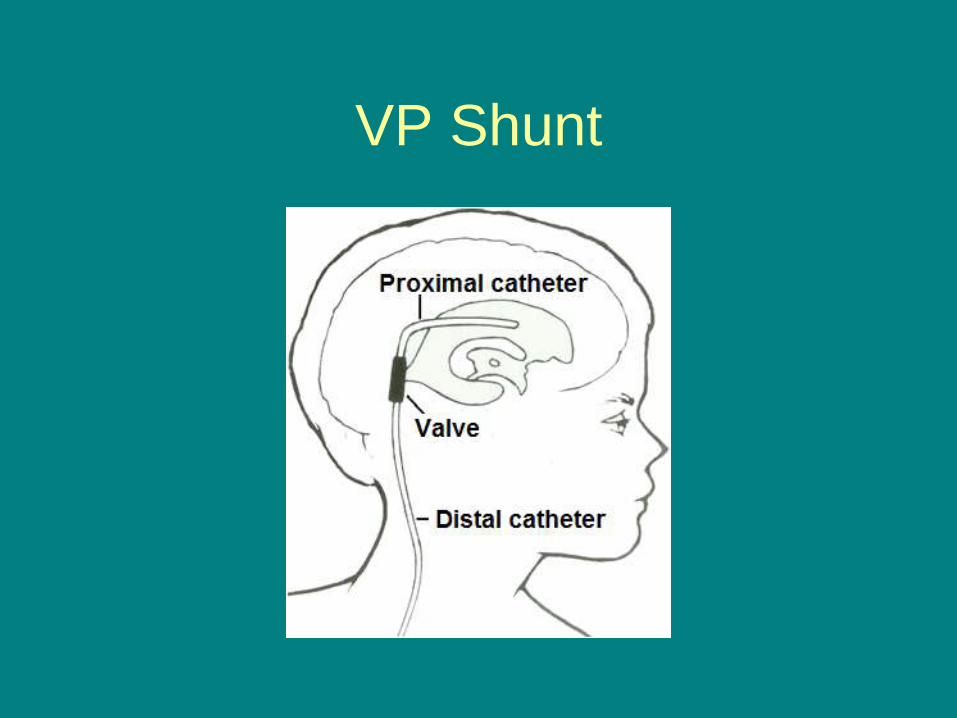
VP Shunt
Shunt failure
• Proximal occlusion of the ventricular catheter is the most common source of blockage (30%)
• Disconnection of shunt components account for 15%
• Distal shunt obstruction due to encystment and loculation of peritoneal contents around distal tip
Shunt infection
• 70% present within the first 2 months
after shunt placement
• Low grade fever, malaise, irritability,
nausea, erythema over shunt site
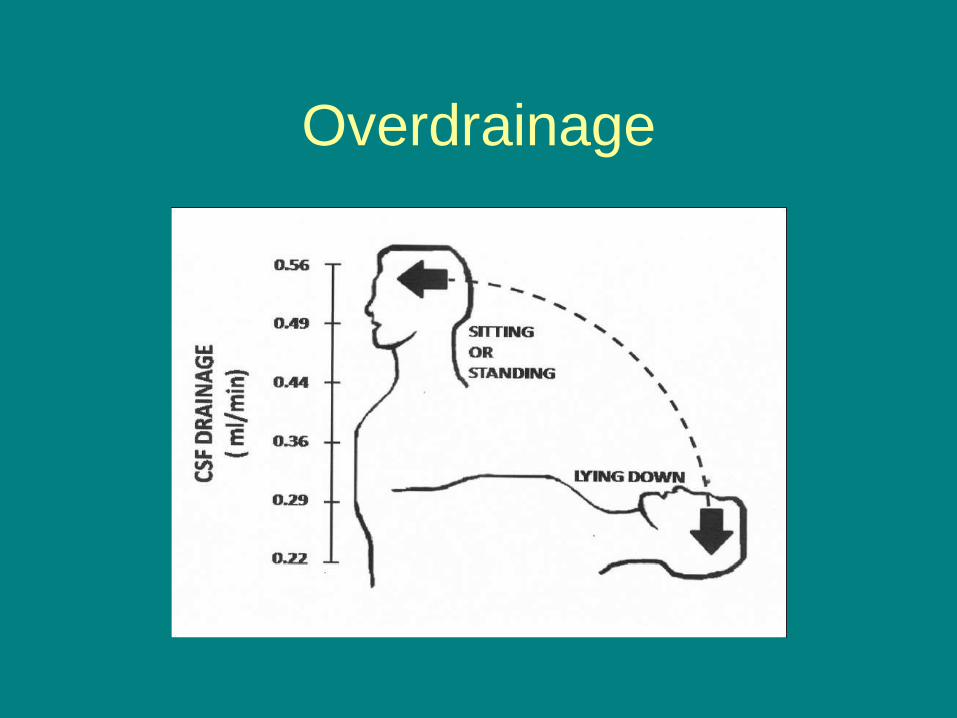
Overdrainage
• Not seen as much with modern shunt
components (programmable valves)
• Orthostatic headache, dizziness,
nausea, lethargy, diplopia
• Can lead to chronic subdural hematoma
Overdrainage
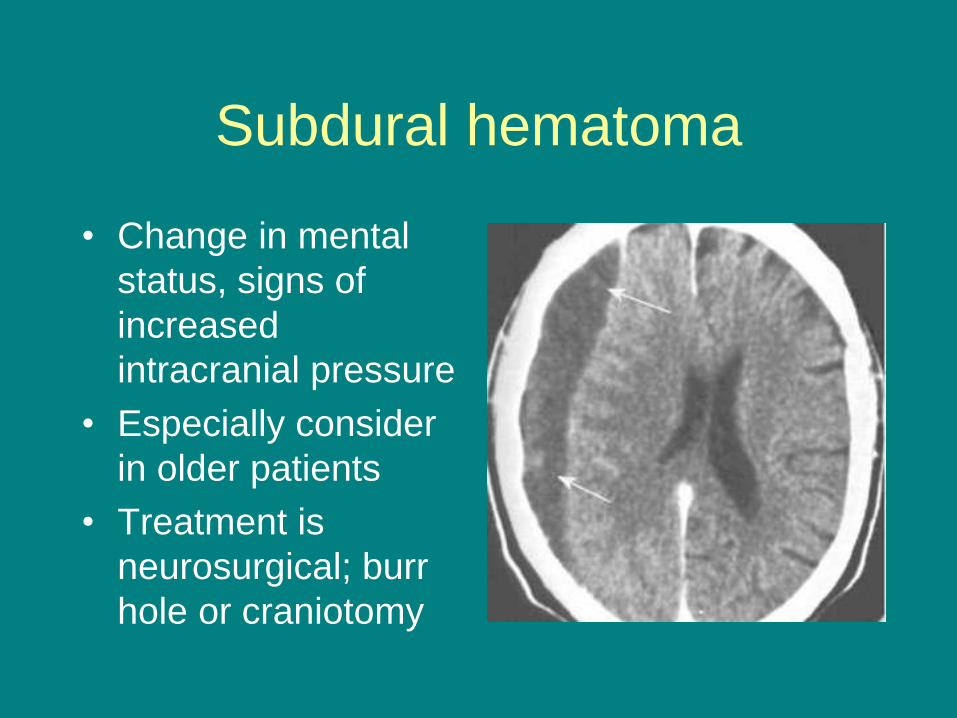
Subdural hematoma
• Change in mental
status, signs of
increased
intracranial pressure
• Especially consider
in older patients
• Treatment is
neurosurgical; burr
hole or craniotomy
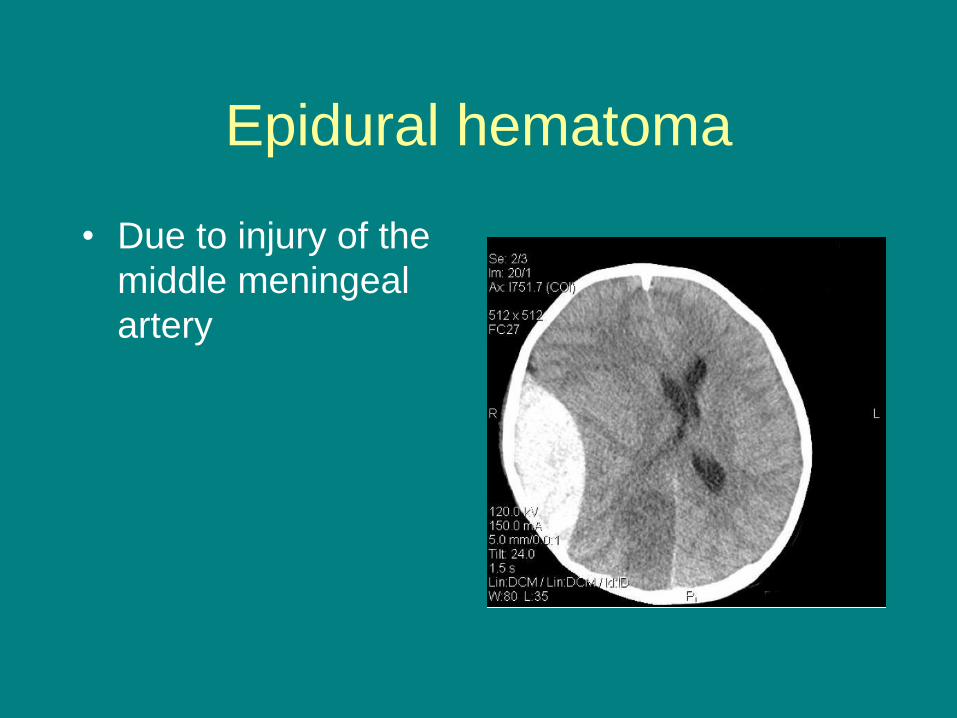
Epidural hematoma
• Due to injury of the
middle meningeal
artery
Spasticity
• Components of UMNS
– Spasticity
– Mass synergy patterns
– Weakness
– Loss of finger dexterity

Spasticity
• Rule out exacerbating factors
• Non-pharmacological treatments
• Oral medications
• Intrathecal baclofen
• Focal treatments
• Surgery
Neuroendocrine Dysfunction
• More common than once thought
• Autopsy study of 100 patients with TBI
found 62% had injury to pituitary
• Studies of hormone levels in patients
with severe TBI found 36-69% had
abnormal levels of at least 1 hormone
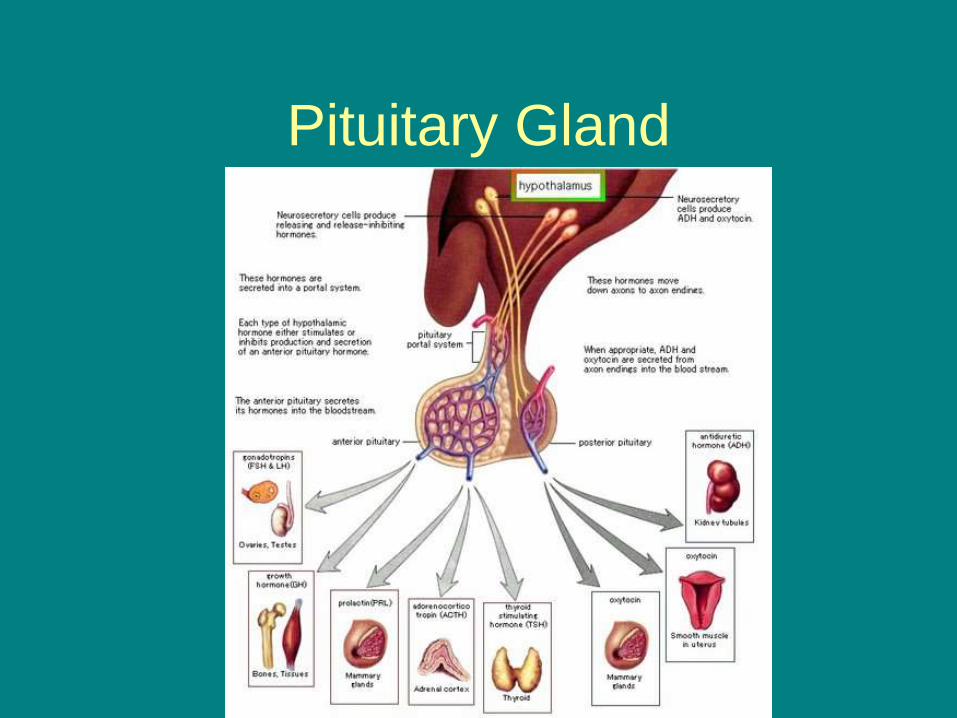
Pituitary Gland
Neuroendocrine Dysfunction
• All of the following have been reported abnormal in TBI survivors – Antidiuretic hormone
– Cortisol
– Growth hormone
– Thyroxine
– FSH/LH
– Prolactin
– Glucagon
– Somatostatin
Normal Pressure
Hydrocephalus • Classic triad- incontinence, gait disorder and
dementia
• Classic gait is short, wide based, magnetic steps
• Some believe this is the most common cause of post trauma HA – IGF1
– Urine assessment if polyuria
• Patients with moderate to severe TBI should undergo hormone evaluation at 3 months and 12 months post ICU discharge – Somatostatin
Neuroendocrine Dysfunction
• Recommendations of Global Experts
Consensus Panel 2005
• Patients with moderate to severe TBI
should undergo hormonal evaluation at
3 months and 12 months post ICU
discharge
Neuroendocrine Dysfunction
• Hormone evaluation should include – 9 AM cortisol level
– fT3, fT4
– TSH
– FSH
– LH
– Testosterone in males
– E2 in females
– Prolactin
– IGF1
SIADH
• Inappropriate ADH release will produce
hyponatremia by interfering with urinary
dilution and decreasing excretion of
ingested water
• Na < 135
• Nausea, fatigue, muscle cramps,
change in mental status, seizure, coma
Post Traumatic Headache
• Most common complaint after mTBI
• Consider causes such as hematomas, hydrocephalus, VP shunt malfunction
• Types – Musculoskeletal
– Cervicogenic
– Neuralgic
– Post traumatic migraine
– Post traumatic sinus headache
Musculoskeletal Headache
• Referred pain from muscles such as
trapezius and SCM
• Pattern often refers pain to retro or peri
orbital area
• Treatment with trigger point
management, acupuncture, postural
correction, meds
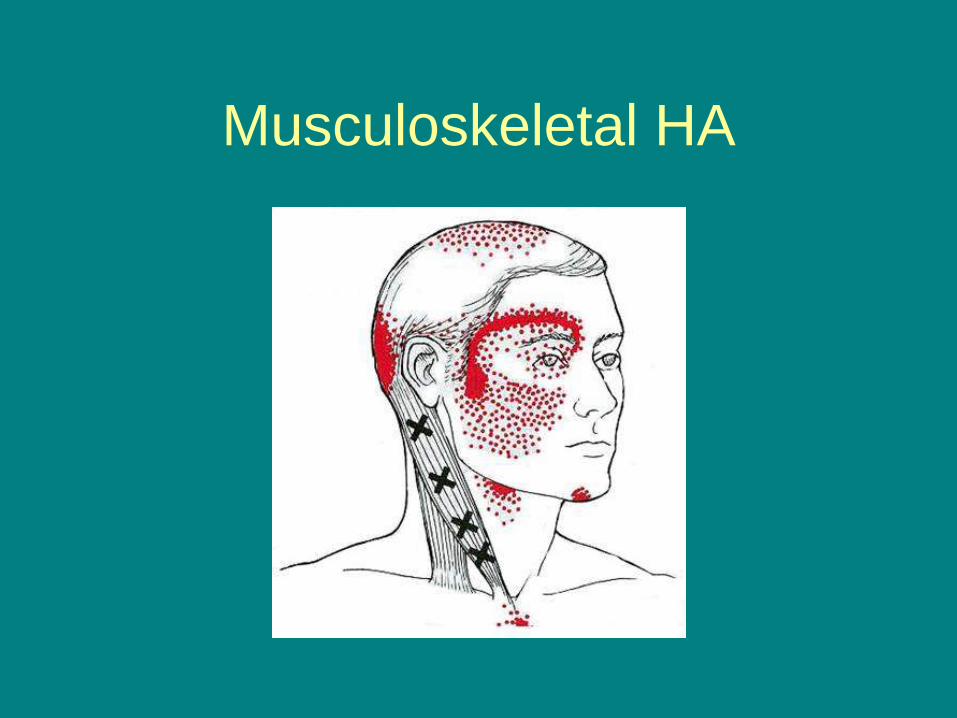
Musculoskeletal HA
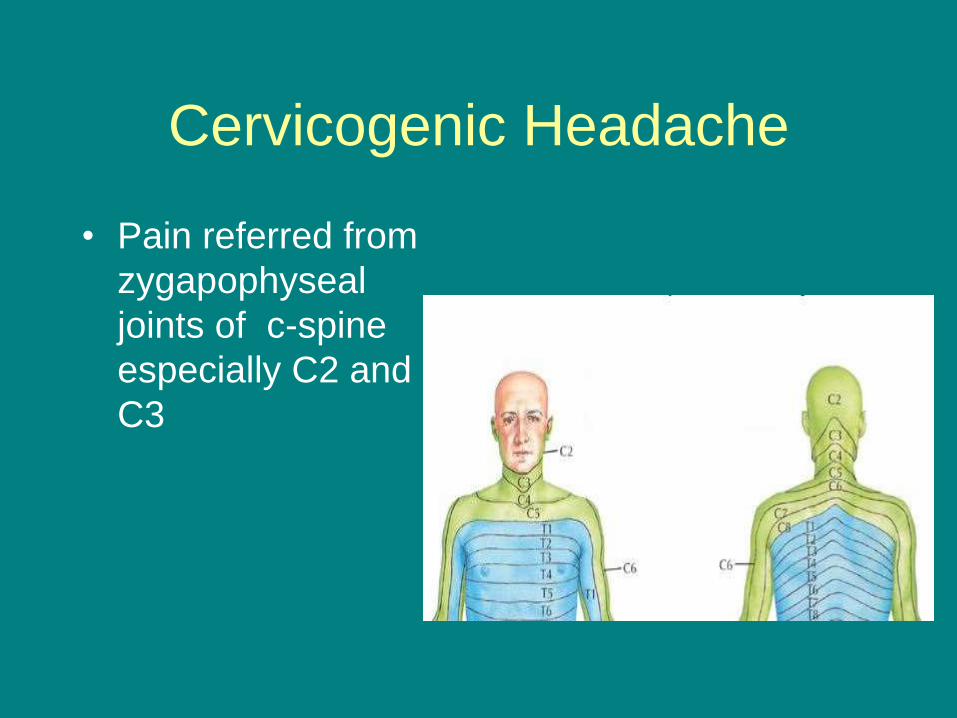
Cervicogenic Headache
• Pain referred from
zygapophyseal
joints of c-spine
especially C2 and
C3
Neuralgic Headache
• Most common is greater occipital nerve
• Splenius muscle spasm or overactivity exacerbates
• Ipsilateral frontotemporal scalp
• Treatment with trigger point management, gabapentin, TCAs, NSAIDs, blocks, surgical decompression
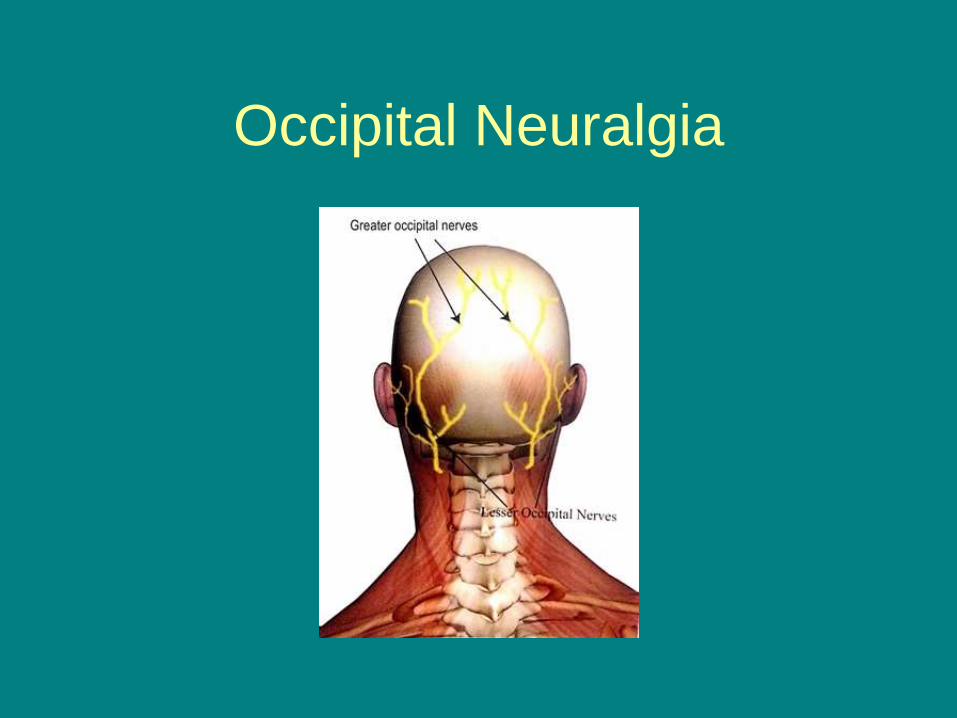
Occipital Neuralgia
Post Traumatic Migraine
• Described as throbbing, unilateral, worse with
cough or bending over. May have visual
issues, nausea, vomiting
• Treatment like migraine in general population.
Prophylactic meds (NSAIDs, beta blockers,
calcium channel blockers, TCAs, depakote)
and abortive meds (triptans, ergot,
dihydroergotamine). Possible role for botox
Post Traumatic Sinus HA
• Patient with history of facial bone
fractures
• HA pattern may be based on drainage
angles
– Frontal and ethmoid worse with supine
– Maxillary and sphenoid better supine
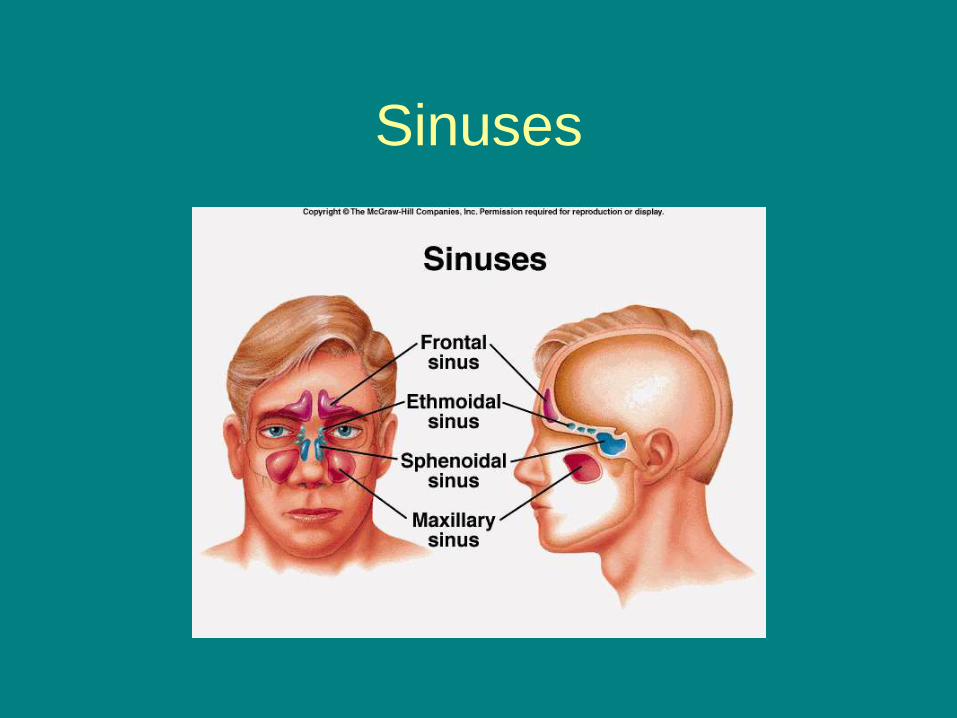
Sinuses