common viral infecions measles mumps rubella chicken pox erythema infectiousum (fifth disease)...
TRANSCRIPT
Common Viral Infecions
MeaslesMumps Rubella Chicken poxErythema infectiousum (Fifth Disease)Roseola infantum(Sixth Disease)
Rashes caused by childhood infections.
Macular/papular /maculopapular:Macules-red/pink discrete flat areas,blanch on pressure ex
rubella,measles..ectPapules –solid raised hemispherical lesions,usually
tiny ,also blanch on perssure.ex scarlet fever,kawasaki disease.
Purpuric/petechial: Non-blanching red/purple spots.ex meningococcal.
Vesicular:Raised hemispherical lesions,<0.5 cm diameter,contain
clear fluid.ex chicken poxPustular/bullous:Raised hemispherical lesions,>0.5cm diameter,contain
clear or purulent fluid.ex ImptigoDesquamation:Dry and flaky loss of surface epidermis, often
peripheries. ex Kawasaki disease.
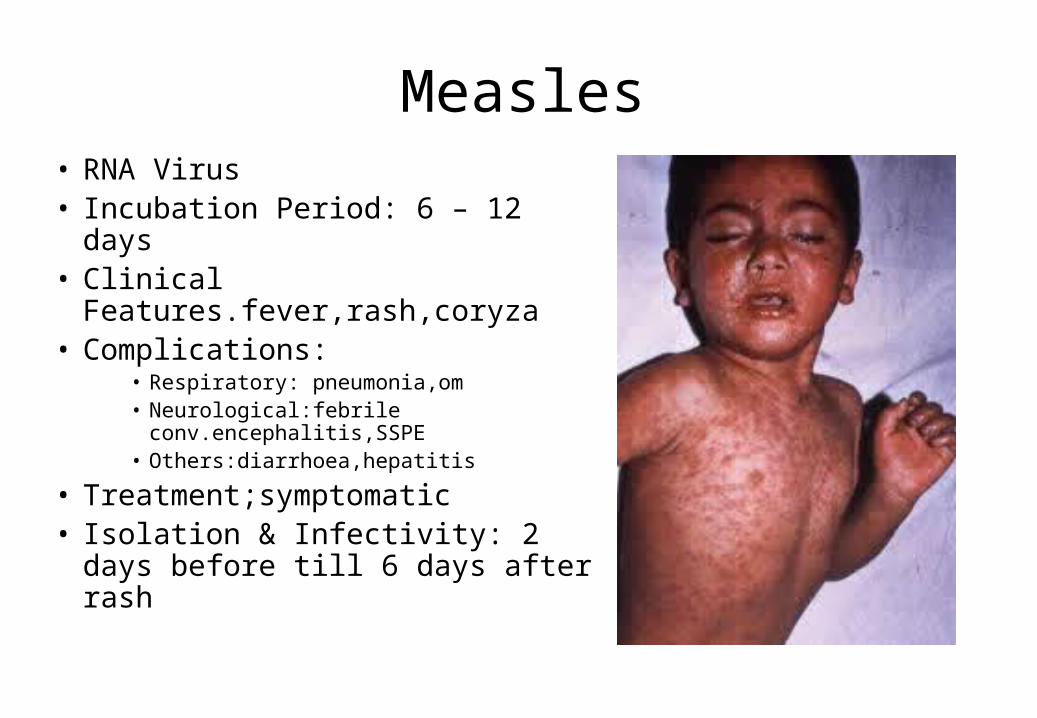
Measles• RNA Virus• Incubation Period: 6 – 12 days• Clinical
Features.fever,rash,coryza• Complications:
• Respiratory: pneumonia,om• Neurological:febrile
conv.encephalitis,SSPE• Others:diarrhoea,hepatitis
• Treatment;symptomatic• Isolation & Infectivity: 2 days
before till 6 days after rash

CLINICAL MANIFESTATIONS
• 1.Incubation period is approximately 6~18days,10days is the most common.
(3-4weeks)• 2 .predromal phase 3~4 days. 1. Fever. 2. Catarrhal inflammation of URT. 3. Koplik’s spots: white spots in the inner cheeks that
appears after 24-48 hours of the infection. It’s the first to appear.
4. Transient prodromal rashes ( rash does not appear from the 1st day )
• 3. Eruption stage 1. Time: the 3~5 days after fever ; but the 4th day is most
common; 2 . Shape: maculopapular 3. Sequence: behind the ear→along the
hairline→face→neck→chest→back→abdomen→limbs→hand and feet(palm , sole)
( rash starts in the face then the trunk then on the periphery ) 4 . The temperature rise continuously and accompanied with
the toxic symptoms .• 4 . Convalescent stage brown staining. fine desquamation. course:10-14 days
COMPLICATIONS : the disease itself is not severe but its complications are serious. • 1 .Bronchopneumonia.• 2 .Myocarditis.• 3 .Laryngitis.• 4 .Neurologic complications: Encephalitis and SSPE . subacute sclerosing panencephalitis Persistent infection of the brain. Rare,psychologic.neuro deterioration. Personality changes,seziure,coma. It happens 7-10
years after the infection.
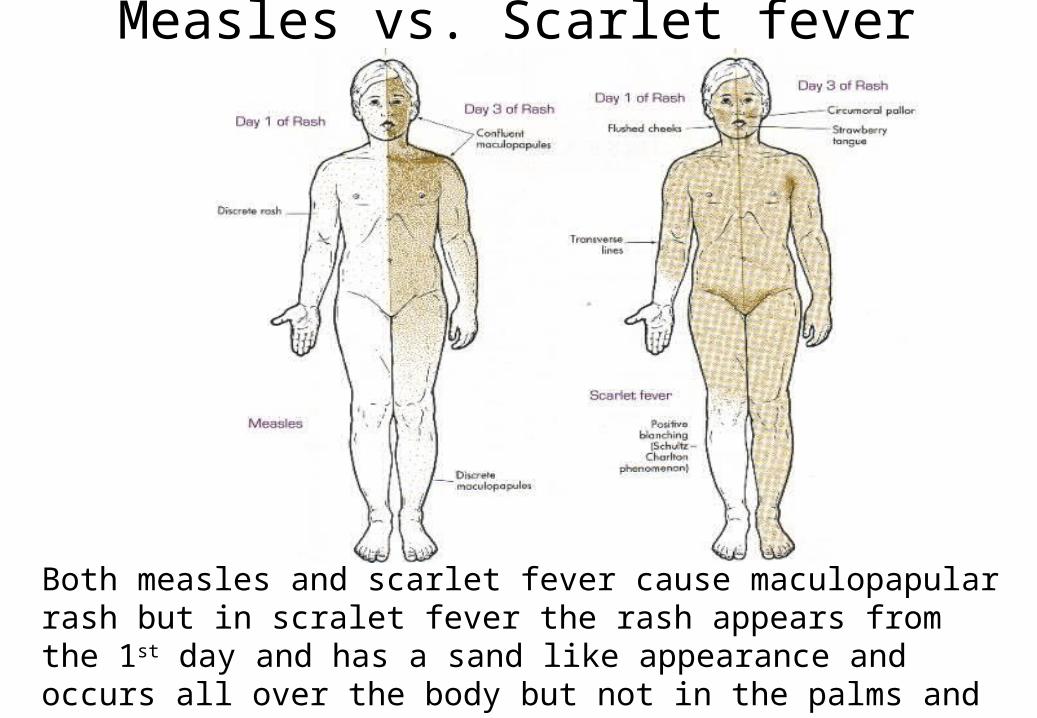
Measles vs. Scarlet fever
Both measles and scarlet fever cause maculopapular rash but in scralet fever the rash appears from the 1st day and has a sand like appearance and occurs all over the body but not in the palms and soles. Scarlet comes with a strawberry tongue white cirumoral lesions and is caused by strep infection.
DIAGNOSIS.
• 1 .Epidemiologic data.• 2 .Clinical manifestations. • 3. Laboratory findings:
. 1 .Multinucleated giant cells are detected in nasopharyax mucosa secretions.
– 2 .Measles virus can be isolated in tissues culture.. 3 . Antibody titer. specific antibody IgM.– 4 . Other Ag and multinucleated giant cells
EPIDEMIOLOGY
• 1.Source of infection The patients are the only source of infection. • 2 .Routes of transmission air-borne ( highly infectious ) by sneezing and cough. • 3. Susceptibility of population 1 . All age person is susceptible; 90% of contact people acquire
the disease. 2 .The permanent immunity acquire after disease.• 4.Epidemic features season:winter and spring age:6 months to 5 years old ( seen in young age group )
DIFFERENTIAL DIAGNOSIS
• 1 .Rubella (German measles)• 2. scarlet fever.• 3 .Roseola infantum (infant subitum,exanthem
subitum)• 4. Drug rashes. In drug rash there will be no:
fever, conjuctivitis, congestion or cough.
Mumps
• RNA Virus• Incubation Period: 14 – 21
days• Clinical Features: fever,
swelling• Complications:
• Glandular• Non glandular
• Isolation & Infectivity: 9 days after onset of parotid swelling
Clinical manifestation of mumps are:
• Parotid inflammation (or parotitis) in 60–70% of infections and 95% of patients with symptoms Parotitis causes swelling and local pain, particularly when chewing. It can occur on one side (unilateral) but is more common on both sides (bilateral) in about 90% of cases.
• Fever• Headache• Pancreatitis: inflammation of the affected pancreas.• Orchitis: painful inflammation of the testicles might affect
the future fertility (most important complication).
Diagnosis:
• Person infected with mumps is contagious from approximately 6 days before the onset of symptoms until about 9 days after symptoms start.
• Usually the disease is diagnosed on clinical grounds and no confirmatory laboratory testing is needed, you might ask for amylase.
Rubella
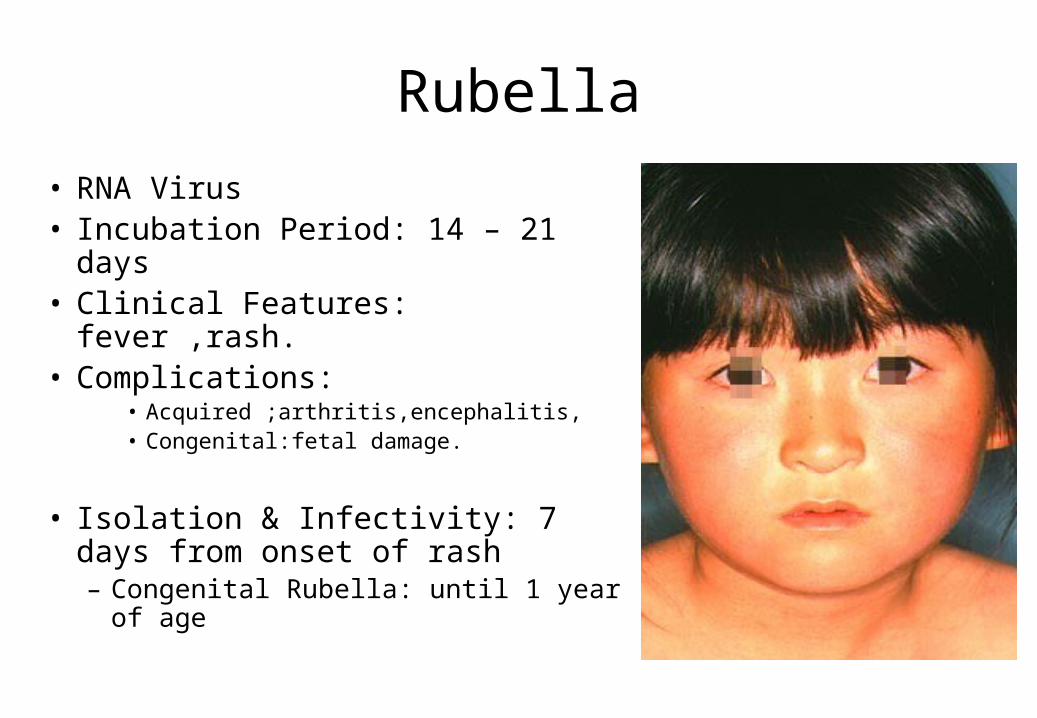
• RNA Virus• Incubation Period: 14 – 21 days• Clinical Features: fever ,rash.• Complications:
• Acquired ;arthritis,encephalitis,• Congenital:fetal damage.
• Isolation & Infectivity: 7 days from onset of rash– Congenital Rubella: until 1 year of
age
Rubella• Symptoms include: low grade fever, swollen glands (sub
occipital & posterior cervical lymphadenopathy), joint pains, headache and conjunctivitis.
• The swollen glands or lymph nodes can persist for up to a week and the fever rarely rises above 38 °C (100.4 °F) therefore no toxic appearance unlike measles.
• The rash (blueberry muffin rash) of German measles is typically pink or light red. The rash causes itching and often lasts for about three days. It starts severe and starts improving on the 3rd day on the face (unlike measles), but is still present on extremities. It’s seen in the face and trunk but more prominent in the peripheries.
• 1st patient to get infected has the best presentation, whereas the last has the worst presentation.
Congenital rubella syndrome
• Rubella can cause CRS in the newly born, whch is the most serious. The syndrome (CRS) follows intrauterine infection by the Rubella virus and comprises cardiac (PDA), cerebral (microcephaly), ophthalmic (cataract) and auditory defects.
• It may also cause prematurity, low birth weight, and neonatal thrombocytopenia, anaemia and hepatitis.
• The risk of major defects or organogenesis is highest for infection in the first trimester.
Chicken Pox (Varicella)
• DNA Virus(VZV).• Incubation Period: 10 – 21 days very contagious especially in the first 48 hours from the
rash. Almost 99%. • Clinical Features: Generalized macules, Papules- vesicles- pusules-crust and then it scales.
The rash has no specific sequence all present at the same time and do not differ from day to day as in rubella. The zoster rash has a dermatomal distribution.
• Complications:• 2nd bacterial infection: staph.strep causing cellulitis • Neurological: cerebellitis, encephalitis (a week after the infection)• Reye syndrome• Disseminated: immunocompromised
• Treatment: (Acyclovir- to decrease symptoms; in measles and rubella there is no need for treatment). – ZIG (zoster immunoglobulin) given for 2 day to immuno-compromised patients who
are exposed.• Isolation & Infectivity: 2 days before rash till all skin lesions have crusted (6th day of rash)
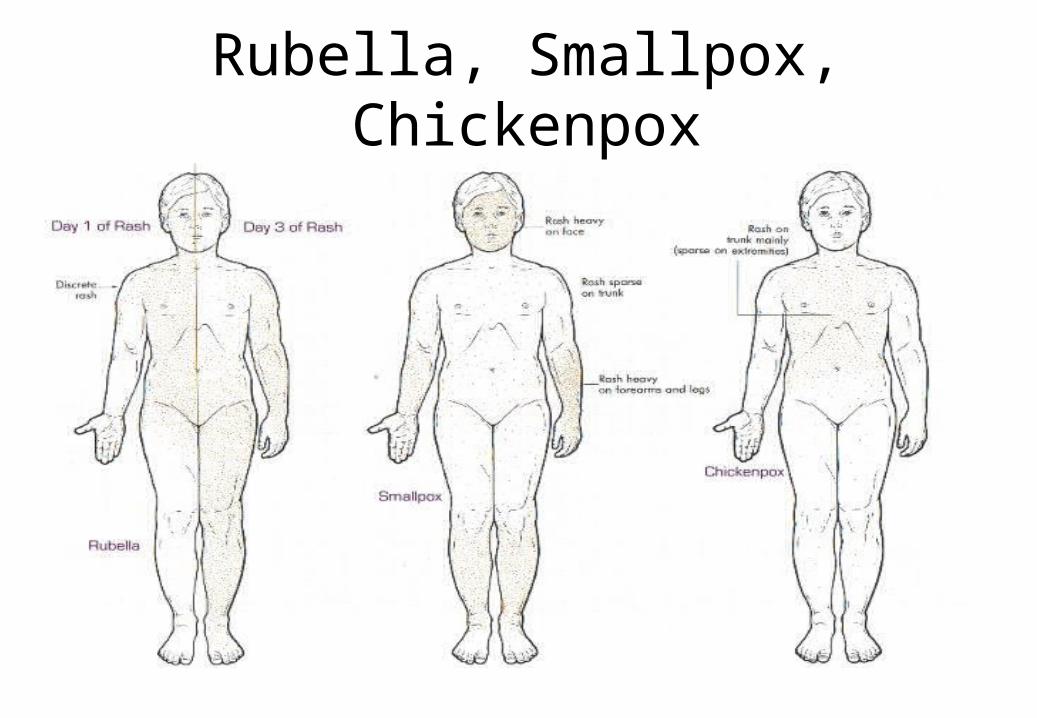
Rubella, Smallpox, Chickenpox
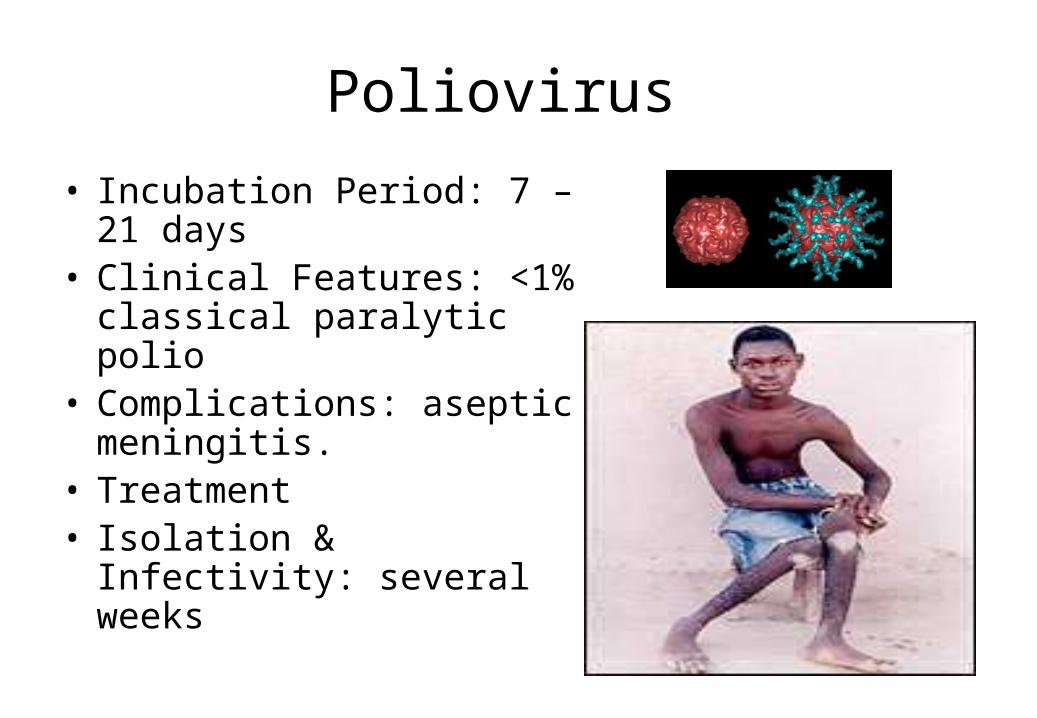
Poliovirus
• Incubation Period: 7 – 21 days
• Clinical Features: <1% classical paralytic polio
• Complications: aseptic meningitis.
• Treatment• Isolation & Infectivity:
several weeks
What is Poliomyelitis?
• polio= gray matter• Myelitis= inflammation of the spinal cord• This disease result in the destruction of motor
neurons caused by the poliovirus.• Polio is causes by a virus that attacks the nerve
cells of the brain & spinal cord although not all infections result in severe injuries and paralysis.
How is polio transmitted?
• Poliovirus is transmitted through both oral and fecal routes with implantation and replication occurring in either the oropharyngeal and/or in the intestine of mucosa ( highly contagious )
• Polio cases are most infective for 7-10 days before and after clinical symptoms begin.
What are the symptoms?
• Many include fever, pharyngitis, headache, anorexia, nausea, and vomiting. Illness may progress to aseptic meningitis and menigoencephalitis in 1% to 4% of patients. These patients develop a higher fever, myalgia and severe headache with stiffness of the neck and back.
Can it cause paralytic disease?
• Paralytic disease occurs 0.1% to 1% of those who become infected with the polio virus.
• Paralysis of the respiratory muscles or from cardiac arrest if the neurons in the medulla oblongata are destroyed.
• Patients have some or full recovery from paralysis usually apparent with proximally 6 months
• Physical therapy is recommended for full recovery.
Vaccine
• Polio vaccine first appeared to be licensed in the United States in 1955.
• Advantages:– Ease to administration– Good local mucosal immunity
• Disadvantage:– Strict cold shipping (it gets destroyed by heat) & storage
requirements– Multiple doses required to achieve high humeral
conservation rates against all virus types
Vaccine (continuation)
• Babies are given 4 doses throughout their infancy.• Adolescents and adults should get vaccinated as
well. Adolescents younger than 18 should receive the routine four doses.
• You should get it if you travel outside places where polio is still an epidemic.
Treatment
• Supportive treatment: bed rest with close monitoring of respiratory and cardiovascular functioning is essential during the acute stage of poliomyelitis along with fever control and pain relievers for muscle spasms.
• No antiviral medications.• If respiratory failure: must be hospitalized for
mechanical ventilation, respiratory therapy may be needed depending of the severity of patients.
Croup
• Parainfluenza any strain• Incubation Period: 2 – 6
days• Clinical Features• Complications• Treatment• Isolation & Infectivity:
contact precaution in hospital, infective up to 3 weeks
Croup (or laryngotracheobronchitis)
• Is a respiratory condition that is usually triggered by an acute viral infection of the upper airway.
• The infection leads to swelling inside the throat, which interferes with normal breathing and produces the classical symptoms of a "barking" cough, stridor, and hoarseness
croup
• Croup is characterized by a "barking" cough, stridor, hoarseness, and difficult breathing which usually worsens at night.
• The "barking" cough is often described as resembling the call of a seal or sea lion.
• The stridor is worsened by agitation or crying, and if it can be heard at rest, it may indicate critical narrowing of the airways. As croup worsens, stridor may decrease considerably
Diagnosis
• The first step is to exclude other obstructive conditions of the upper airway, especially epiglottitis (it’s a more serious infection than croup, once suspected you can’t examine the patient, you do x-ray (thumb sign) and intubate), an airway foreign body, subglottic stenosis, angioedema, retropharyngeal abscess, and bacterial tracheitis.
Diagnosis
• A frontal X-ray of the neck is not routinely performed, but if it is done, it may show a characteristic narrowing of the trachea, called the steeple sign, because of the subglottic stenosis, which is similar to a steeple in shape
Croup treatment:
• Corticosteroids (inhaled or nebulized), such as dexamethasone and budesonide, have been shown to improve outcomes in children with all severities of croup, single dose is usually all that is required.
• Moderate to severe croup may be improved temporarily with nebulized epinephrine
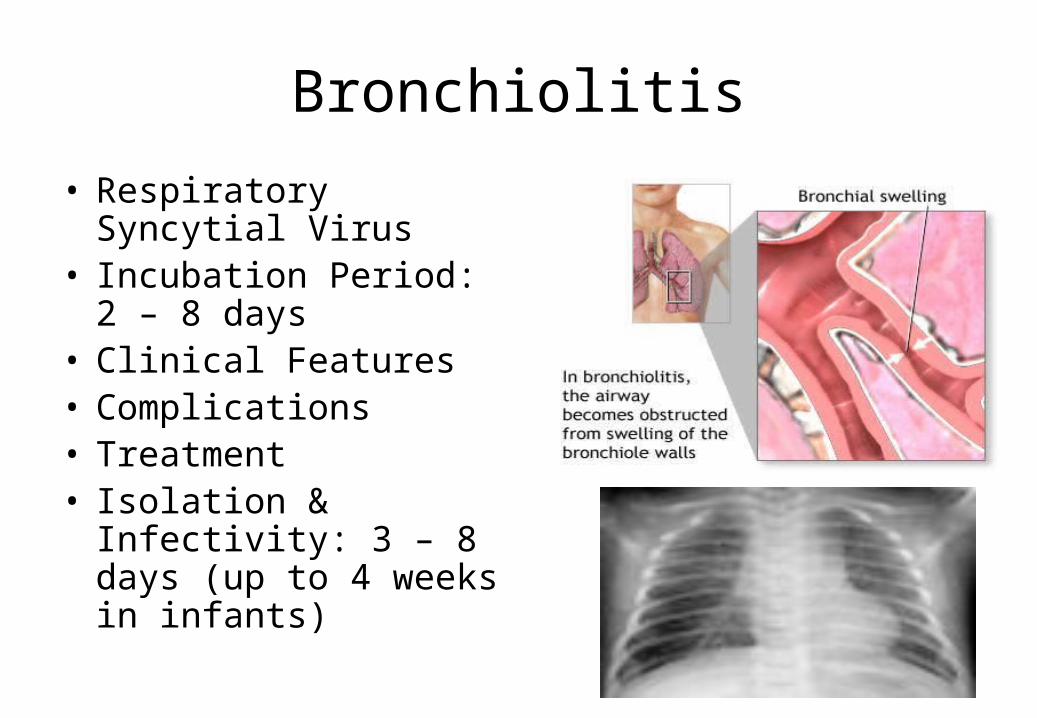
Bronchiolitis
• Respiratory Syncytial Virus
• Incubation Period: 2 – 8 days
• Clinical Features• Complications• Treatment• Isolation & Infectivity:
3 – 8 days (up to 4 weeks in infants)
Bronchiolitis
• most often affects infants and young children because their small airways can become blocked more easily than those of older kids or adults ( in older group children and adults it causes URTI)
• typically occurs during the first 2 years of life, with peak occurrence at about 3 to 6 months of age
• is more common in males, children who have not been breastfed, and those who live in crowded conditions.
• Its more common in premature babies.
Signs & Symptoms
• Sudden breathing difficulty, usually preceded by fever and a mild common cold and cough, and characterized by the following: – Wheezing. – Rapid, shallow breathing (60 to 80 times a minute). – Retractions (seesaw movements) of the chest and abdomen,
and nasal flaring. – Fever (occasionally). – Blue discoloration of skin or nails (severe cases).
Treatment General Measures • Keep the humidity in the child's room as high as possible,
preferably with an ultrasonic cool-mist humidifier. Clean humidifier daily. If you don't have a humidifier, run cold or hot water in the shower with windows and doors closed to produce a high-humidity room. Hold the child in this room for 20 minutes several times a day, especially at bedtime. If the child awakens at night with wheezing or shortness of breath, repeat the process.
• Sometimes they give ventolin but its not very effective.
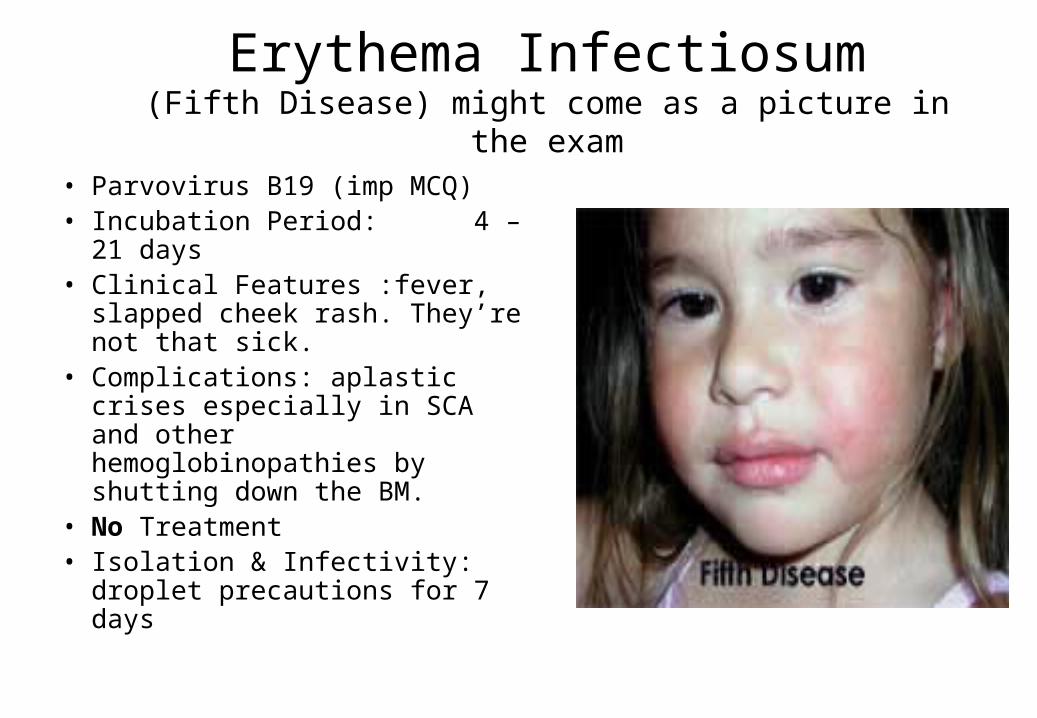
Erythema Infectiosum(Fifth Disease) might come as a picture in the exam
• Parvovirus B19 (imp MCQ)• Incubation Period: 4 – 21
days• Clinical Features :fever,
slapped cheek rash. They’re not that sick.
• Complications: aplastic crises especially in SCA and other hemoglobinopathies by shutting down the BM.
• No Treatment• Isolation & Infectivity: droplet
precautions for 7 days
Fifth disease symptoms• Bright red cheeks are a defining symptom of the
infection in children (hence the name "slapped cheek disease"). Occasionally the rash will extend over the bridge of the nose or around the mouth.
• In addition to red cheeks, children often develop a red, lacy rash on the rest of the body, with the upper arms and legs being the most common locations.
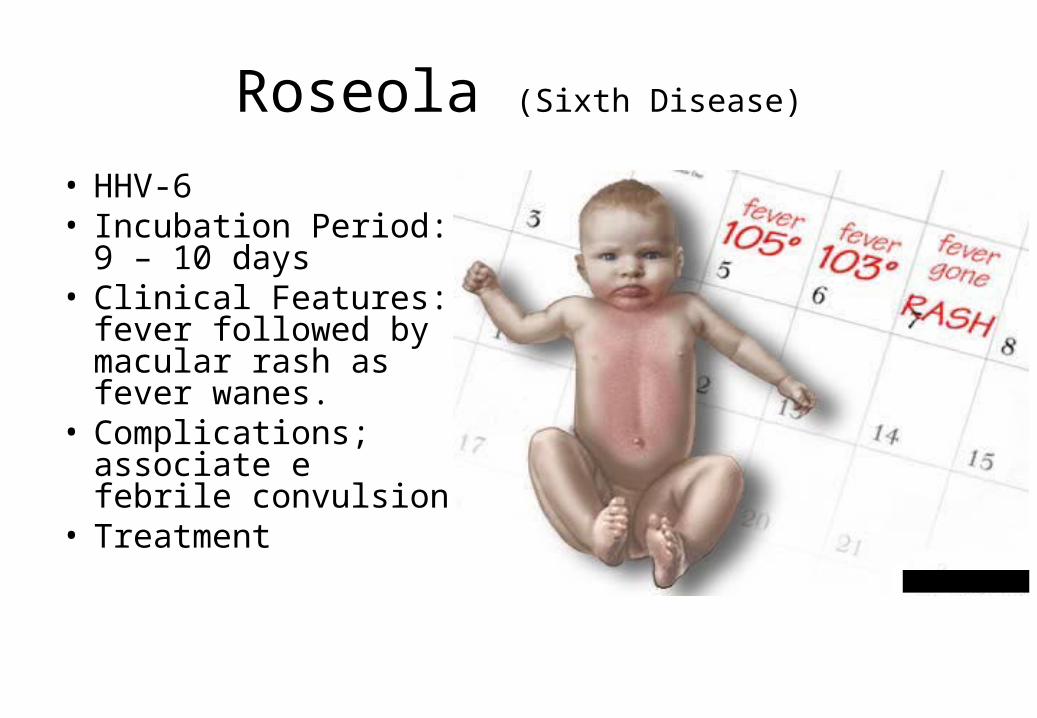
Roseola (Sixth Disease)
• HHV-6• Incubation Period:
9 – 10 days• Clinical Features:
fever followed by macular rash as fever wanes.
• Complications; associate e febrile convulsion
• Treatment
Roseola • Typically the disease affects a child between six months and
two years of age, and begins with a sudden high fever (39–40 °C; 102.2-104 °F) that persists up to 5 days.
• This can cause, in rare cases, febrile convulsions (also known as febrile seizures or "fever fits") due to the sudden rise in body temperature, but in many cases the child appears normal. To prevent this, we need to give regular antipyretics.
• After a few days, the fever subsides, and just as the child appears to be recovering, a red rash appears. This usually begins on the trunk, spreading to the legs and neck. The rash is not itchy and may last 1 to 2 days
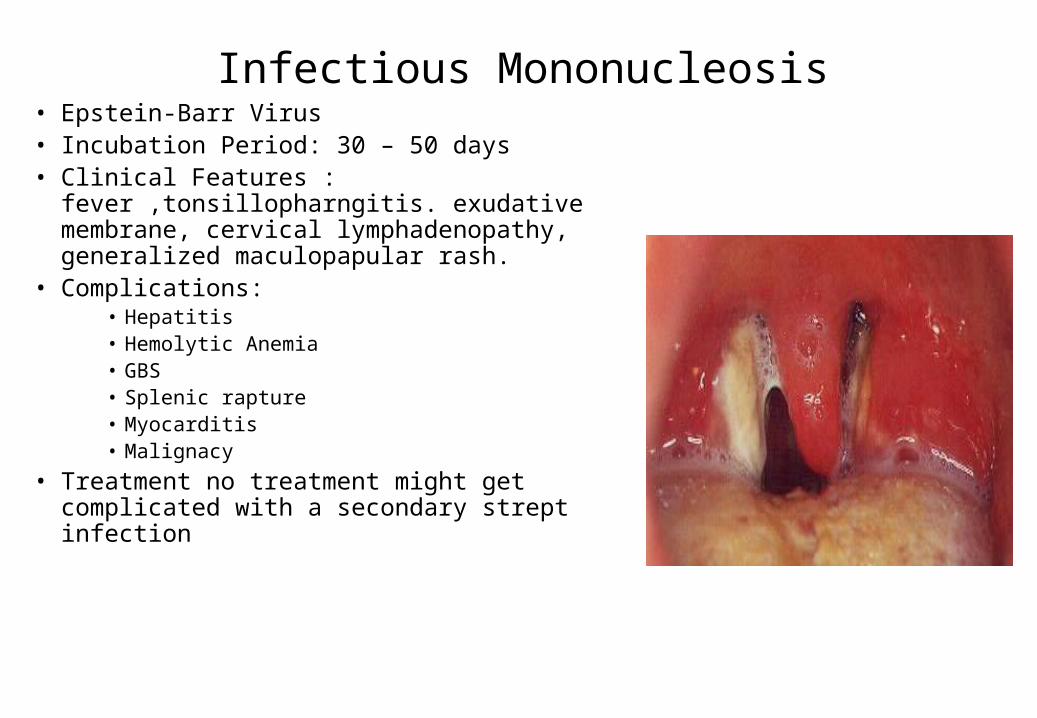
Infectious Mononucleosis• Epstein-Barr Virus• Incubation Period: 30 – 50 days• Clinical Features :
fever ,tonsillopharngitis. exudative membrane, cervical lymphadenopathy, generalized maculopapular rash.
• Complications:• Hepatitis • Hemolytic Anemia• GBS • Splenic rapture• Myocarditis• Malignacy
• Treatment no treatment might get complicated with a secondary strept infection
COMMON BACTERIAL INFECTIONS
• Staphylococcal and Group A streptoccocal infections.
• By direct effect –abscess, celluitis, imptigo, orbital celluitis.
• Toxin mediated: toxic shock syndrome• Toxic epidermial necrolysis.
Continue….
• Group A streptococcus:• Direct effect: tonsillitis, osteomyelitis, otitis media,
cellulitis• Toxin mediated: toxic shock like syndrome, scarlet
fever • Post infectious: rheumatic fever,
glomerulonephritis.
Haemophilus influenzae type b (Hib)
• Clinical Features• Complications• Treatment• Isolation &
Infectivity: droplet precautions for 24 hours after starting antimicrobial therapy
• Vaccine
Cerebrospinal fluid culture positive for Hib
(Gram stain)
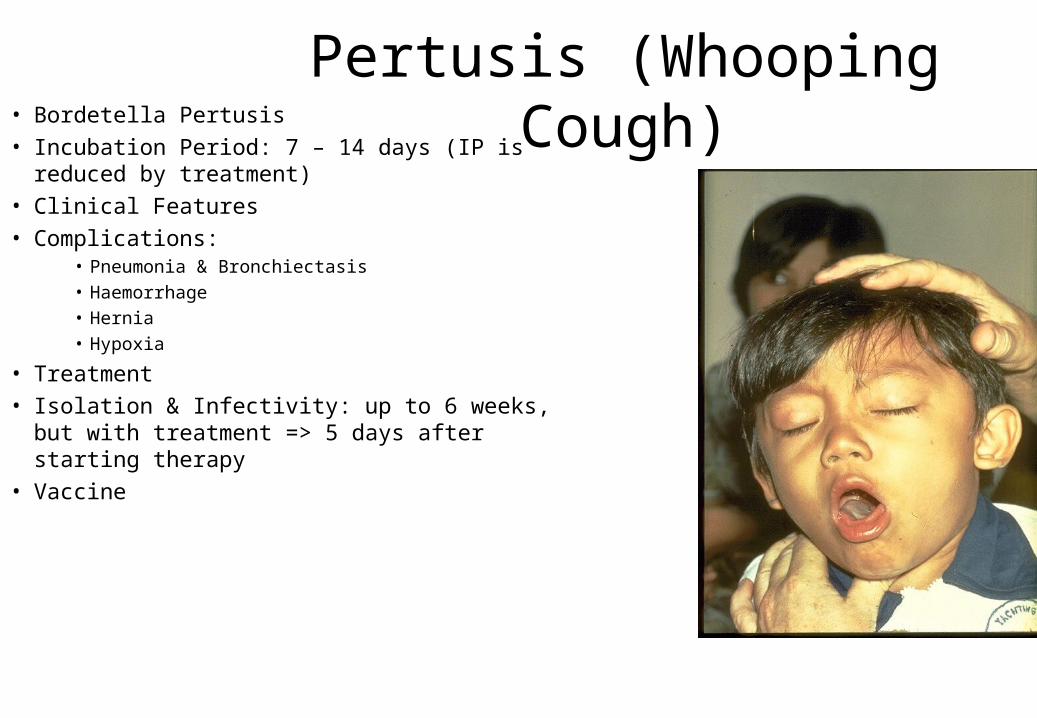
Pertusis (Whooping Cough)• Bordetella Pertusis• Incubation Period: 7 – 14 days (IP is reduced
by treatment)• Clinical Features• Complications:
• Pneumonia & Bronchiectasis• Haemorrhage• Hernia• Hypoxia
• Treatment• Isolation & Infectivity: up to 6 weeks, but with
treatment => 5 days after starting therapy• Vaccine
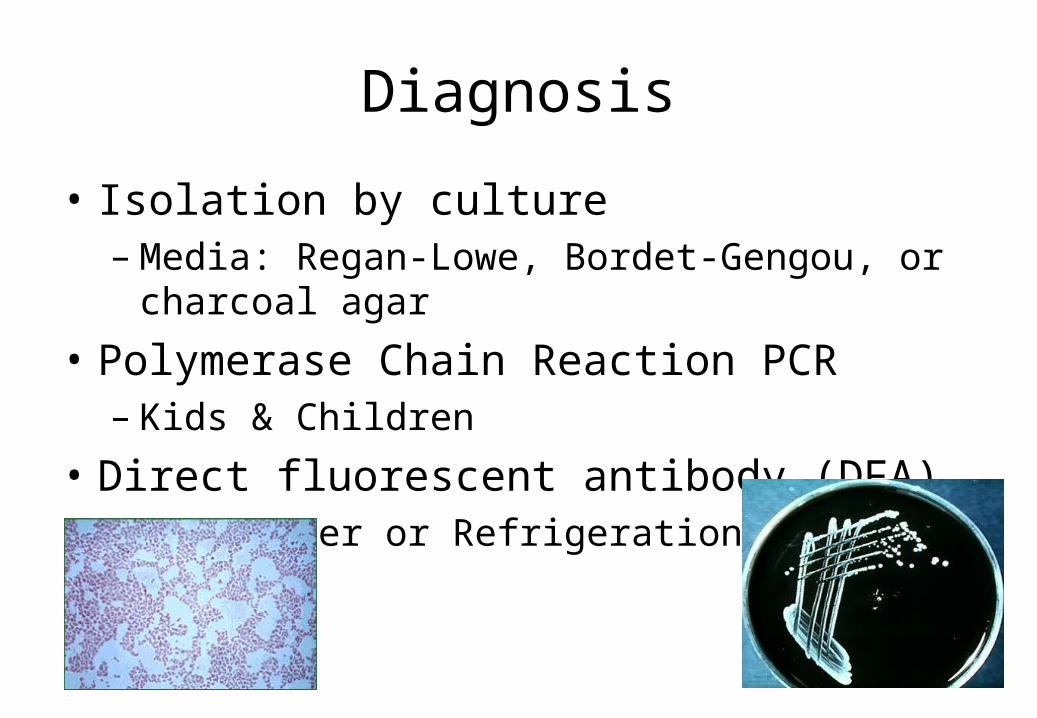
Diagnosis
• Isolation by culture– Media: Regan-Lowe, Bordet-Gengou, or charcoal agar
• Polymerase Chain Reaction PCR – Kids & Children
• Direct fluorescent antibody (DFA)– NO Freezer or Refrigeration of samples
Route of Transmission
• Spread through direct contact of respiratory secretions.
• Most contagious during first few stages of infection
• Resides in upper airway pathways, mostly the trachea and bronchi.
• Very contagious
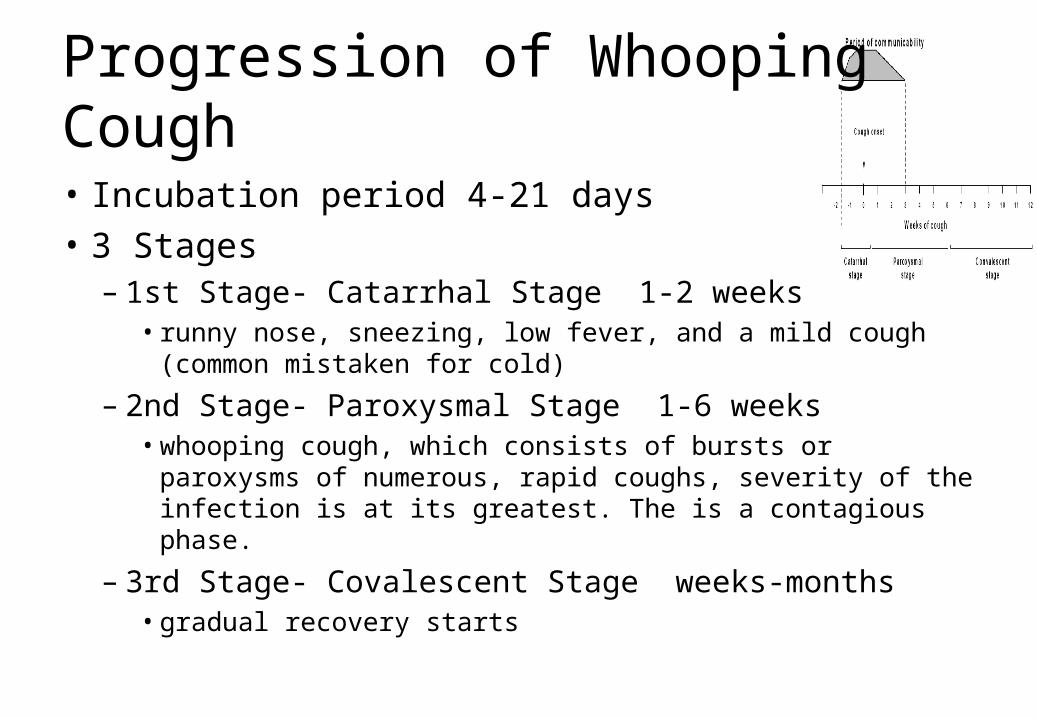
Progression of Whooping Cough
• Incubation period 4-21 days• 3 Stages– 1st Stage- Catarrhal Stage 1-2 weeks
• runny nose, sneezing, low fever, and a mild cough (common mistaken for cold)
– 2nd Stage- Paroxysmal Stage 1-6 weeks• whooping cough, which consists of bursts or paroxysms of
numerous, rapid coughs, severity of the infection is at its greatest. The is a contagious phase.
– 3rd Stage- Covalescent Stage weeks-months• gradual recovery starts
Complications
ChildrenHypoxia
Apnea
Pneumonia
Seizures
AdultsPneumonia
Rib Fracture
Weight Loss
Hernias
Urinary Incontinence

Treatment
• Antibiotic Therapy- Macrolides– Erythromycin– Azithromycin – Clarithromycin
Prevention
CDC recoomends children be given the Diphtheria, Tetanus, and Pertussis (DTaP) vaccine as early as 6 weeks but no later than 6 y/o.
Good hygiene
Cover mouth/nose when coughing and sneezing.
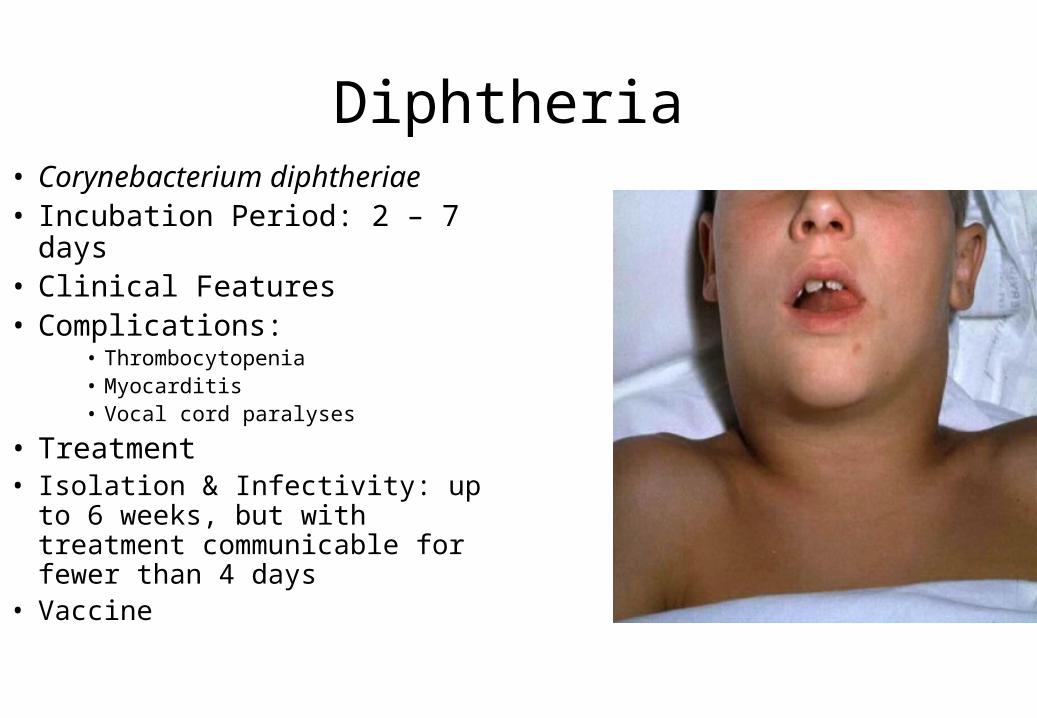
Diphtheria• Corynebacterium diphtheriae • Incubation Period: 2 – 7 days• Clinical Features• Complications:
• Thrombocytopenia• Myocarditis• Vocal cord paralyses
• Treatment• Isolation & Infectivity: up to 6
weeks, but with treatment communicable for fewer than 4 days
• Vaccine
Diphtheria
• Is an upper respiratory tract illness caused by Corynebacterium diphtheriae, a facultative anaerobic, Gram-positive bacterium.
• It is characterized by sore throat, low fever, and an adherent membrane (a pseudomembrane) on the tonsils, pharynx, and/or nasal cavity.
Case classification
• Probable: a clinically compatible case that is not laboratory-confirmed and is not epidemiologically linked to a laboratory-confirmed case
• Confirmed: a clinically compatible case that is either laboratory-confirmed or epidemiologically linked to a laboratory-confirmed case
• Empirical treatment should generally be started in a patient in whom suspicion of diphtheria is high.
Treatment
• Antibiotics are used in patients or carriers to eradicate C. diphtheriae and prevent its transmission to others. The CDC recommends either:– Metronidazole– Erythromycin (orally or by injection) for 14 days (40 mg/kg/day
with a maximum of 2 g/d), or– Procaine penicillin G given intramuscularly for 14 days (300,000
U/d for patients weighing <10 kg and 600,000 U/d for those weighing >10 kg).
– Patients with allergies to penicillin G or erythromycin can use rifampin or clindamycin.
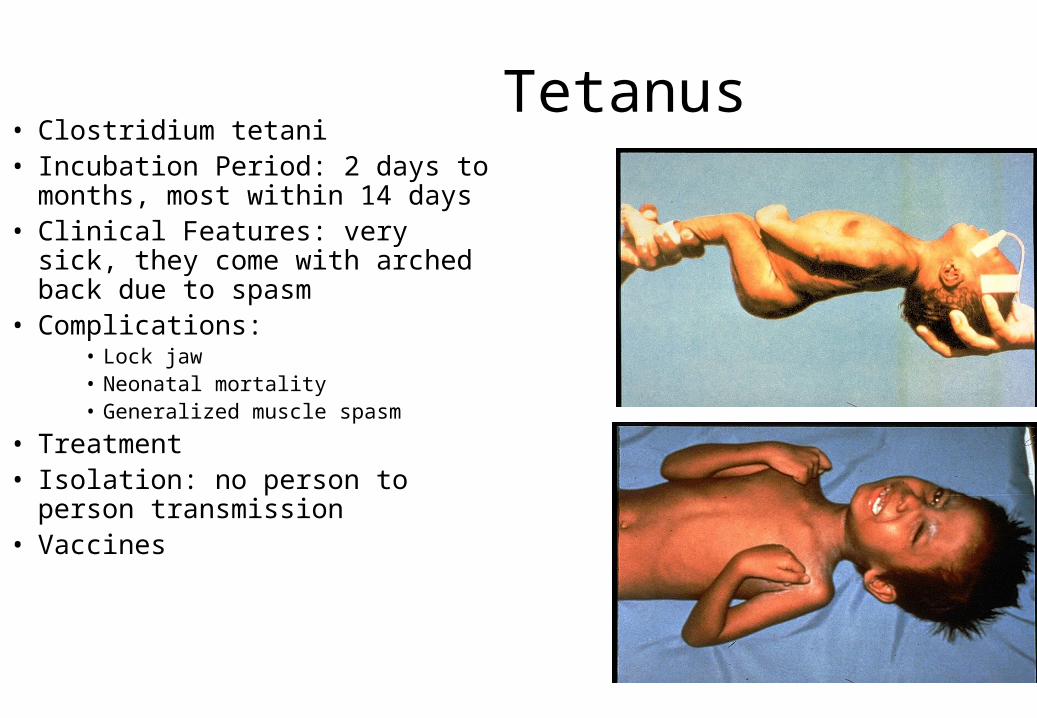
Tetanus• Clostridium tetani• Incubation Period: 2 days to
months, most within 14 days• Clinical Features: very sick,
they come with arched back due to spasm
• Complications:• Lock jaw• Neonatal mortality• Generalized muscle spasm
• Treatment• Isolation: no person to person
transmission• Vaccines
Tetanus• Medical condition characterized by a prolonged contraction of skeletal
muscle fibers.- The primary symptoms are caused by tetanospasmin, a neurotoxin
produced by the Gram-positive, rod-shaped, obligate anaerobic bacterium Clostridium tetani.
- Infection generally occurs through wound contamination and often involves a cut or deep puncture wound. As the infection progresses, muscle spasms develop in the jaw (thus the name "lockjaw") and elsewhere in the body.
- Neonates may develop it by using infected instruments to cut the umbilical cord after delivery.
• The wound must be cleaned. Dead and infected tissue should be removed by surgical debridement. Administration of the antibiotic metronidazole decreases the number of bacteria but has no effect on the bacterial toxin.
• Penicillin was once used to treat tetanus, but is no longer the treatment of choice, owing to a theoretical risk of increased spasms.
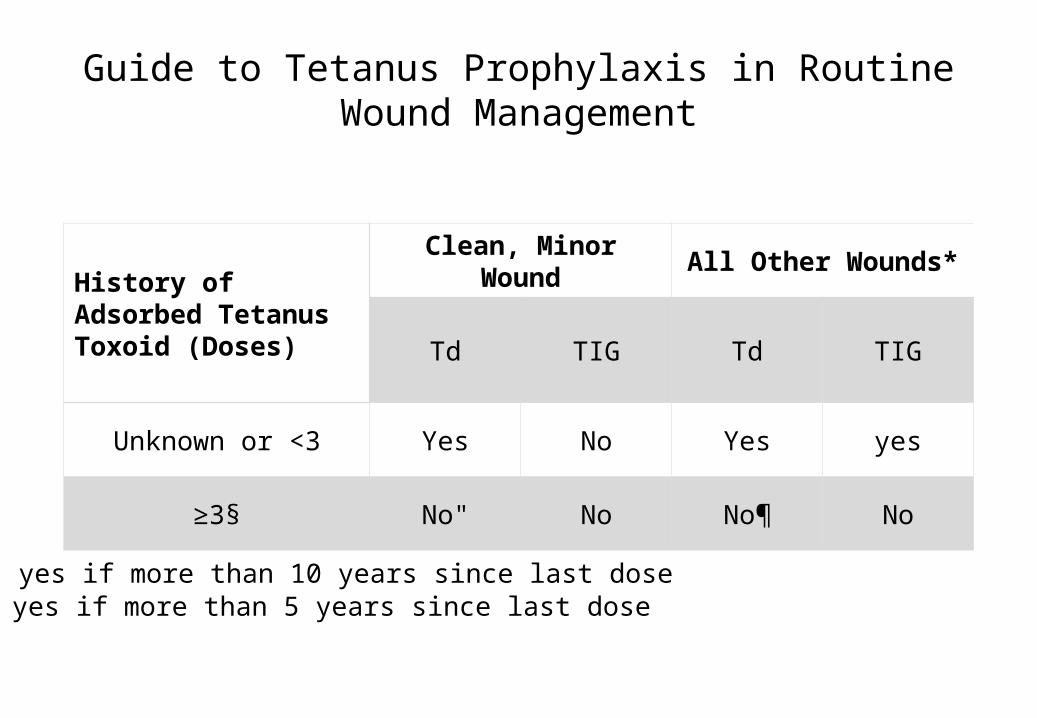
Guide to Tetanus Prophylaxis in Routine Wound Management
History of Adsorbed Tetanus Toxoid (Doses)
Clean, Minor Wound All Other Wounds*
Td TIG Td TIG
Unknown or <3 Yes No Yes yes
≥3§ No" No No¶ No
" yes if more than 10 years since last dose¶ yes if more than 5 years since last dose
• Tetanus can be prevented by vaccination with tetanus toxoid.
• The CDC recommends that adults receive a booster vaccine every ten years, and standard care practice in many places is to give the booster to any patient with a puncture wound who is uncertain of when he or she was last vaccinated, or if he or she has had fewer than three lifetime doses of the vaccine
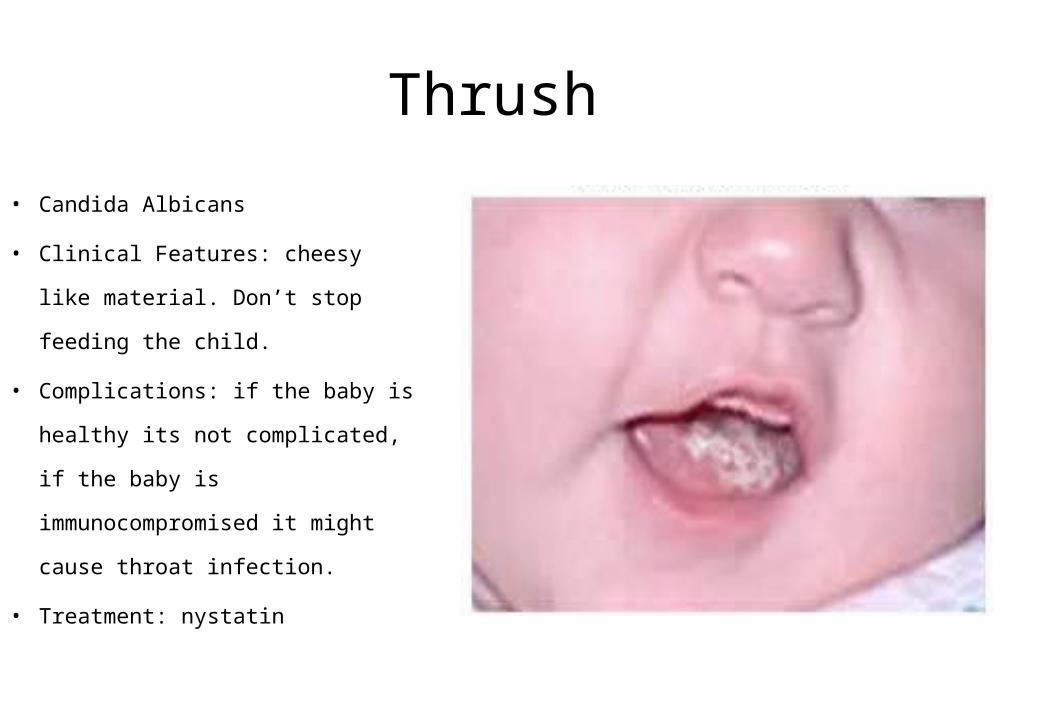
Thrush
• Candida Albicans
• Clinical Features: cheesy like
material. Don’t stop feeding the
child.
• Complications: if the baby is
healthy its not complicated, if the
baby is immunocompromised it
might cause throat infection.
• Treatment: nystatin
Kawasaki disease
• Affect infant and young children• Clinical criteria– Fever >5days and 4 of the following • Conjunctival injection• Red mucous membrane • Cervical lymphadenopathy• Rash• Oedema of palms & soles with peeling
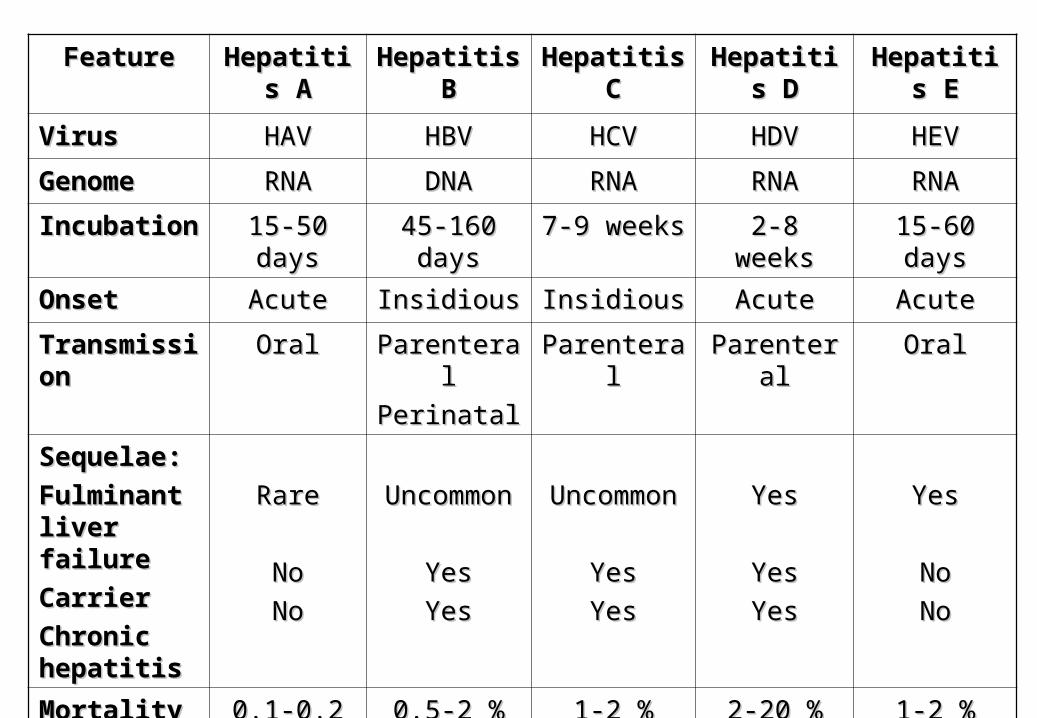
FeatureFeature HepatitiHepatitis As A
Hepatitis Hepatitis BB
Hepatitis Hepatitis CC
Hepatitis Hepatitis DD
Hepatitis Hepatitis EE
VirusVirus HAVHAV HBVHBV HCVHCV HDVHDV HEVHEV
GenomeGenome RNARNA DNADNA RNARNA RNARNA RNARNA
IncubationIncubation 15-50 15-50 daysdays
45-160 45-160 daysdays
7-9 weeks7-9 weeks 2-8 weeks2-8 weeks 15-60 15-60 daysdays
OnsetOnset AcuteAcute InsidiousInsidious InsidiousInsidious AcuteAcute AcuteAcute
TransmissTransmissionion
OralOral ParenteralParenteral
PerinatalPerinatalParenteralParenteral ParenteraParentera
llOralOral
Sequelae:Sequelae:
Fulminant Fulminant liver liver failurefailure
CarrierCarrier
Chronic Chronic hepatitishepatitis
RareRare
NoNo
NoNo
UncommoUncommonn
YesYes
YesYes
UncommoUncommonn
YesYes
YesYes
YesYes
YesYes
YesYes
YesYes
NoNo
NoNo
MortalityMortality 0.1-0.2 %0.1-0.2 % 0.5-2 %0.5-2 % 1-2 %1-2 % 2-20 %2-20 % 1-2 %1-2 %
Further Reading
• READ BOOK by Report of the committee on Infectious Diseases.