cochrane database of systematic reviews (reviews) || herbal medicine for low back pain
TRANSCRIPT
Herbal medicine for low back pain (Review)
Gagnier JJ, van Tulder MW, Berman BM, Bombardier C
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2011, Issue 2
http://www.thecochranelibrary.com
Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
10DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iHerbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Herbal medicine for low back pain
Joel J Gagnier1, Maurits W van Tulder2, Brian M Berman3, Claire Bombardier4
1Department of Epidemiology, School of Public Health, University of Michigan, Ann Arbor, MI, USA. 2Department of Health
Sciences, Faculty of Earth and Life Sciences, VU University, Amsterdam, Netherlands. 3Center for Integrative Medicine, University of
Maryland School of Medicine, Baltimore, Maryland, USA. 4Institute for Work & Health, Toronto, Canada
Contact address: Joel J Gagnier, Department of Epidemiology, School of Public Health, University of Michigan, 1415 Washington
Heights, Rm M5158, Ann Arbor, MI, 48109-2029, USA. [email protected].
Editorial group: Cochrane Back Group.
Publication status and date: Edited (no change to conclusions), published in Issue 2, 2011.
Review content assessed as up-to-date: 14 December 2005.
Citation: Gagnier JJ, van Tulder MW, Berman BM, Bombardier C. Herbal medicine for low back pain. Cochrane Database of SystematicReviews 2006, Issue 2. Art. No.: CD004504. DOI: 10.1002/14651858.CD004504.pub3.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Low-back pain is a common condition and a substantial economic burden in industrialized societies. A large proportion of patients
with chronic low-back pain use complementary and alternative medicine (CAM), visit CAM practitioners, or both. Several herbal
medicines have been purported for use in low-back pain.
Objectives
To determine the effectiveness of herbal medicine for non-specific low-back pain.
Search methods
We searched the following electronic databases: Cochrane Complementary Medicine Field Trials Register (Issue 3, 2005), MEDLINE
(1966 to July 2005), EMBASE (1980 to July 2005); checked reference lists in review articles, guidelines and retrieved trials; and
personally contacted individuals with expertise in this very specialized area.
Selection criteria
We included randomized controlled trials, examining adults (over 18 years of age) suffering from acute, sub-acute or chronic non-
specific low-back pain. The interventions were herbal medicines, defined as plants that are used for medicinal purposes in any form.
Primary outcome measures were pain and function.
Data collection and analysis
Two authors (JJG & MVT) conducted the database searches. One author contacted content experts and acquired relevant citations. Full
references and abstracts of the identified studies were downloaded. A hard copy was retrieved for final inclusion decisions. Methodological
quality and clinical relevance were assessed separately by two individuals. Disagreements were resolved by consensus.
Main results
Ten trials were included in this review. Two high quality trials examining the effects of Harpagophytum Procumbens (Devil’s Claw) found
strong evidence that daily doses standardized to 50 mg or 100 mg harpagoside were better than placebo for short-term improvements
in pain and rescue medication. Another high quality trial demonstrated relative equivalence to 12.5 mg per day of rofecoxib (Vioxx).
Two trials examining the effects of Salix Alba (White Willow Bark) found moderate evidence that daily doses standardized to 120 mg or
1Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

240 mg salicin were better than placebo for short-term improvements in pain and rescue medication. An additional trial demonstrated
relative equivalence to 12.5 mg per day of rofecoxib. Three low quality trials on Capsicum Frutescens (Cayenne), examining various
topical preparations, found moderate evidence that Capsicum Frutescens produced more favourable results than placebo and one trial
found equivalence to a homeopathic ointment.
Authors’ conclusions
Harpagophytum Procumbens, Salix Alba and Capsicum Frutescens seem to reduce pain more than placebo. Additional trials testing
these herbal medicines against standard treatments are needed. The quality of reporting in these trials was generally poor. Trialists
should refer to the CONSORT statement extension for reporting trials of herbal medicine interventions.
P L A I N L A N G U A G E S U M M A R Y
Herbal medicine for low-back pain
Significance of the review
Back pain is common, affecting as much as 35% of the population in a given month. Non-specific low-back pain is defined as pain
between the lowest rib and the bottom of the buttocks that is not caused by serious, underlying problems such as rheumatoid arthritis,
infection, fracture, cancer, or sciatica due to a herniated disc or other pressure on nerves. Oral and topical herbal medicines are being
used to treat many conditions; several are used for back pain and have been tested in clinical trials.
Description of the trials
Three oral herbal medications were tested in ten randomized controlled trials that included 1567 adults with non-specific acute or
chronic low-back pain. Two oral herbal medications, Harpagophytum Procumbens (Devil’s Claw) and Salix Alba (White Willow Bark),
were compared with placebo (fake pills) and with rofecoxib (Vioxx). Topical Capsicum frutescens (Cayenne) was compared with placebo
and a homeopathic gel.
Findings
Devil’s Claw, in a standardized daily dose of 50 mg or 100 mg harpagoside, seemed to reduce pain more than placebo; a standardized
daily dose of 60 mg reduced pain about the same as a daily dose of 12.5 mg of Vioxx. While Willow Bark, in a standardized daily dose
of 120 mg and 240 mg of salicin reduced pain more than placebo; a standardized daily dose of 240 mg reduced pain about the same as
a daily dose of 12.5 mg of Vioxx. Cayenne was tested in plaster form and reduced pain more than placebo and about the same as the
homeopathic gel Spiroflor SLR. Adverse effects were reported, but appeared to be primarily confined to mild, transient gastrointestinal
complaints.
Limitations
Most of the trials were of moderate or high quality, but they only tested the effects of short term use (up to six weeks). The authors
of half of the studies were judged to have a potential conflict of interest and two others did not discuss conflict of interest. Vioxx has
been withdrawn from the market because of adverse effects, so all three substances should be compared with readily available pain
medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen, to test for relative effectiveness and safety.
Conclusion
Although there are good results with three herbal medicines in short-term trials, with strong evidence for a particular form of one of
the herbal medicines, there is no evidence yet that any of these substances are safe and useful for long term use.
2Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
B A C K G R O U N D
Low-back pain and related disability are major public health prob-
lems across industrialized nations. As a result, the past 15 years
have seen an intensive research effort to identify effective treatment
and management strategies for low-back pain (Mounce 2002).
The one-month prevalence of low-back pain is reported to be be-
tween 35% and 37%, with a lifetime prevalence between 70%
and 85%, peaking between 45 and 59 years of age (Papageorgiou
1995; Andersson 1999). In the United States, back pain is the
most common cause of disability in those under 45 years of age
(Borkan 1995) and back sprains and strains represent about one
quarter of work-related injuries resulting in lost work-days (Dept
Labor 1995). Low-back pain is the second most frequent cause
of work absence in industrialized nations (Praemer 1992) and is a
frequent reason for visits to a physician (Coste 1994; Andersson
1999). It has been estimated that in the United States, back pain
has associated direct costs of US $20 billion and indirect costs of
between US $75 and 100 billion (Borkan 1995). In the United
Kingdom, costs associated with low-back pain are estimated to
be over £500 million (Little 1996). This amounts to substantial
societal loss of productivity and an economic burden for health-
care systems in many industrialized countries (Mounce 2002).
The traditional treatment of low-back pain includes medication,
tissue stimulation (e.g. TENS, ultrasound), rest and orthotics (e.g.
braces; Cherkin 1993). Although systematic reviews suggest that
few of these have enough evidence to suggest benefit, it does appear
that acute low-back pain can usually be effectively managed by en-
couraging activity, reassurance and short-term symptom control
(analgesics or non-steroidal anti-inflammatory drugs (NSAIDs);
van Tulder 2002a). Treatments that demonstrate some effective-
ness for the management of chronic low-back pain include ex-
ercise therapy, behavioural treatment and multidisciplinary treat-
ment programs (van Tulder 2002b). To alter beliefs about back
pain that are correlated with impairment or disability is one of the
major challenges in low-back pain management (Borkan 1995).
Research in complementary and alternative medicine (CAM) has
blossomed in the past 10 years. Rigorous literature is growing
steadily and is subsequently clarifying the validity of these tech-
niques. Specifically, the number of randomised trials of comple-
mentary treatments has doubled approximately every five years
(Vickers 2000) and currently, the Cochrane Complementary
Medicine Field Trials Registry contains over 6500 randomized
and controlled clinical trials. In addition, CAM teaching insti-
tutions are now beginning to teach principles of evidence-based
medicine and clinical epidemiology (Mills 2002; Sierpina 2002).
These initiatives are well placed, given the large number of visits
to CAM practitioners (Millar 2001). A recent population survey
in Canada found that 2.2 million women and 1.6 million men
visited a CAM practitioner during 1998-1999 (Millar 2001). Of
these, more than 26% of individuals who reported chronic pain
visited an alternative practitioner during the previous year, com-
pared with only 15% of those who did not report chronic pain.
Those who reported back pain had a higher percentage of visits
to alternative practitioners than any other pain condition. More
specifically, 37% of the individuals who reported back pain visited
an alternative practitioner, compared with only 17% of the entire
population (Millar 2001). Similar percentages have been found in
surveys conducted in the United States (Astin 2000; Druss 1999;
Eisenberg 1998).
Several herbal medicines have been reported to be treatments
for various types of pain. These include: Camphora Molmol,
Capsicum Frutescens, Salix Alba, Maleluca Alternifolia, Angelica
Sinensis, Aloe Vera, Thymus Officinalis, Menthe Peperita, Arnica
Montana, Curcuma Longa, Tancaetum Parthenium, Harpago-
phytum Procumbens, and Zingiber Officinicalis (Blumenthal
1998). Many of these herbs have been the subject of extensive
biochemical research, resulting in the delineation of their pharma-
cological and physiological effects (Mills 2000). For example, the
mechanism of Capsicum Frutescens is partially related to its abil-
ity to deplete substance P (Keitel 2001). Salix Alba is a platelet in-
hibitor and analgesic, and Harpagophytum Procumbens has anal-
gesic and anti-inflammatory properties (Chrubasik 1996). In ad-
dition, some of these herbal species have been clinically tested for
the relief of symptoms of low-back pain (Mills 2000; Stam 2001;
Laudahn 2001a; Krivoy 2000).
Given the large public health and economic burden low-back pain
causes and the large number of such sufferers who regularly visit
CAM practitioners, a systematic review of these practices was war-
ranted.
O B J E C T I V E S
To determine the effectiveness of herbal medicine compared to
placebo, no intervention, or other interventions in the treatment
of non-specific low-back pain.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Only randomized controlled trials (RCTs) were included.
Types of participants
Trials included adults (older than 18 years of age), suffering from
acute (lasting up to six weeks), sub-acute (lasting six to 12 weeks)
or chronic (lasting longer than 12 weeks) non-specific low-back
pain.
3Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Low-back pain was defined as pain localized to the area between
the costal margin or the 12th rib to the inferior gluteal fold.
Non-specific low-back pain indicated that no specific cause was
detectable, such as infection, neoplasm, metastasis, osteoporosis,
rheumatoid arthritis, fracture, inflammatory process or radicular
syndrome (Waddell 1996).
Types of interventions
For the purpose of the present review, an herbal medicine was de-
fined as all or part of a plant that was used for medicinal purposes,
administered orally (ingestion) or applied topically. This definition
did not include plant substances that were smoked (e.g. Cannabis
Sativa), individual chemicals that were derived from plants or syn-
thetic chemicals that were based on constituents of plants. How-
ever, Cannabis Sativa, or other plants that can be smoked, will be
considered herbal medicines for this review if they were ingested.
Various forms of oral herbal medicine include: standardized ex-
tracts (encapsulated or tablet form), tinctures (alcohol, glycerine,
etc), dried herb (encapsulated or tablet form), raw whole herb infu-
sion (e.g. tea) and decoction (e.g. boiled down tea). Topical herbal
applications include: ointments, essential oils, creams (petroleum
or glycerine based), powders, plasters, and poultices. Opioids will
be excluded from this review, given they bridge the definitions of
herbal medicine and analgesic.
Types of outcome measures
1. Pain intensity [e.g., visual analogue scale (VAS), numerical rat-
ing scale (NRS)] and proportion of pain free patients.
2. Back pain specific functional status measured by validated in-
struments [e.g. Roland Disability Questionnaire (RDQ), Owestry
Disability index (ODI)]
3. Overall improvement (% reporting subjective improvement,
NRS)
4. Return to Work or Work Status (% of population, number of
days of absenteeism).
Search methods for identification of studies
We searched the following electronic databases:
1. Cochrane Complementary Medicine Field Trials Registry (Issue
3, 2005)
2. MEDLINE (1966 to July 2005)
3. EMBASE (1980 to July 2005)
4. Clinical Evidence (January 2005)
We used the search strategy recommended by the Cochrane Back
Review Group for both MEDLINE and EMBASE (van Tulder
2003; van Tulder 1997). Terms included: low back pain, backache,
lumbago. The specific search terms for randomized controlled tri-
als (Robinson 2002) and herbal medicine for both MEDLINE and
EMBASE are listed in Appendix 1 and Appendix 2. The search
terms were modified as necessary for the Cochrane Complemen-
tary Medicine Field Trials Registry.
We also reviewed reference lists in review articles, guidelines and
in the retrieved trials and contacted individuals with expertise in
herbal medicine and low-back pain (JJG) to identify additional
trials. Non-English articles were translated and discussed by JJG
and MvT following the same procedures described below.
Data collection and analysis
One author (JJG) conducted the electronic searches. Two authors
(JJG & MvT) independently selected studies based on title, ab-
stract, and keywords. Studies that met the inclusion criteria were
included in the review. If it was not clear from the title and abstract
if a study fulfilled the inclusion criteria, a full copy was retrieved
for final selection. A consensus method was used to resolve dis-
agreements.
Methodological quality assessment
Methodological quality was independently assessed by two authors
(JJG & MvT). Given one of the authors’ (JJG) familiarity with
the literature, studies were not blinded for authors, institution or
journal. The eleven items reflecting internal validity, together with
operational definitions, recommended by the Back Group in their
updated method guidelines for systematic reviews were used to
assess methodological quality (van Tulder 2003; Table 1). Each
criterion was scored as “yes”(Y), “no”(N) or “don’t know”(DK).
’Yes’ indicated that the criterion was met. ’No’ reflected the lack
of fulfilment of that criterion. ’Don’t know’ reflect the fact that
there was insufficient information to determine if this criterion
was fulfilled or not. A trial was considered high quality if more
than 50% (6/11) of internal validity items were met.
Data extraction
Two authors (JJG & MvT) independently extracted the data from
each trial, using a standardized form. The following data were ex-
tracted from each study: recruitment, characteristics of the study
population (age, gender), setting (e.g. year, country of origin),
duration of low-back pain (acute, subacute, or chronic), previous
treatment for low-back pain, number of patients initially recruited,
number of patients randomized, number of drop-outs or with-
drawals, duration of intervention, type of herbal medicine used
(plant name and form of delivery and dosage), standardization in-
formation (e.g. percentage of active constituent per delivery unit),
characteristics of the control intervention (type and duration),
types of outcome measures, summary statistics, timing of outcome
assessments, compliance, adverse effects due to intervention, and
author’s conclusions as to the effectiveness of the intervention.
4Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Clinical relevance
The clinical relevance of each study was independently assessed by
two authors, using these five questions:
1. Are the patients described in detail so that you can decide
whether they are comparable to those that you see in your prac-
tice?
2. Are the interventions and treatment settings described well
enough so that you can provide the same for your patients?
3. Were all clinically relevant outcomes measured and reported?
4. Is the size of the effect clinically important?
5. Are the likely treatment benefits worth the potential harms?
Data analysis
Due to insufficient data and clinically heterogeneity, a qualitative
analysis was conducted, using a rating system consisting of five
levels of evidence (van Tulder 2003):
1. Strong evidence - consistent findings among multiple high
quality RCTs
2. Moderate evidence - consistent findings among multiple low
quality RCTs and/or one high quality RCT
3. Limited evidence - one low quality RCT
4. Conflicting evidence - inconsistent findings among multiple
RCTs
5. No evidence from trials - no RCTs
Sensitivity analyses were carried out to explore the results when
definitions of high quality trials were 40% and 60% fulfilment of
internal validity criteria. We also conducted an additional sensi-
tivity analysis, assuming the validity criteria that were scored as
“DK” were, in fact, positive.
Subgroup analyses were conducted separately for acute low-back
pain (lasting less than six weeks), subacute low-back pain (lasting
from six to 12 weeks) and chronic low-back pain (lasting longer
than 12 weeks).
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
A total of 295 references were identified from Cochrane Comple-
mentary Medicine Field Trials Registry, MEDLINE, EMBASE,
Clinical Evidence searches and by contacting content experts. Af-
ter reviewing titles and abstracts, 266 citations were excluded for
not meeting the predetermined inclusion criteria. Twenty-nine
papers were retrieved in full, 19 of which were excluded due to
improper study design (not RCT). A total of 10 citations met in-
clusion criteria and were included in this review (Chrubasik 1996;
Chrubasik 1999; Chrubasik 2000; Chrubasik 2001; Chrubasik
2003; Frerick 2003; Ginsberg 1987; Krivoy 2001; Keitel 2001;
Stam 2001).
Three studies used an oral form of the herbal species Harpago-
phytum Procumbens (Devil’s Claw; Chrubasik 1996; Chrubasik
1999; Chrubasik 2003), three used oral Salix Alba (White Wil-
low Bark; Chrubasik 2000; Chrubasik 2001; Krivoy 2001) and
four used topical Capsicum Frutescens (Cayenne; Frerick 2003;
Ginsberg 1987; Keitel 2001; Stam 2001).
Four studies compared various oral herbal medicines with placebo
(Chrubasik 1996; Chrubasik 1999; Chrubasik 2000; Krivoy
2001). Two studies compared oral herbal medicines to standard
pain medications (Chrubasik 2001; Chrubasik 2003). Three stud-
ies compared topical herbal medicines to placebo (Frerick 2003;
Ginsberg 1987; Keitel 2001). One study compared a topical herbal
medicine to a topical homeopathic medicine (Stam 2001).
The three studies using Harpagophytum Procumbens included
patients with acute exacerbations of chronic non-specific low-back
pain (Chrubasik 1996; Chrubasik 1999; Chrubasik 2003). Sim-
ilarly, the three trials examining the effects of Salix Alba prepara-
tions included homogeneous populations with acute episodes of
chronic non-specific low-back pain (Chrubasik 2001; Chrubasik
2000; Krivoy 2001). One of the trials using a topical Capsicum
Frutescens ointment included patients with acute mechanical low-
back pain (Ginsberg 1987). Two additional trials using a Cap-
sicum pain plaster included participants with chronic non-specific
low-back pain (Frerick 2003; Keitel 2001). One trial using a top-
ical Capsicum ointment included a sample of patients with either
newly occurring acute low-back pain or acute episodes of chronic
low-back pain (Stam 2001).
Three of these studies (Chrubasik 1996; Chrubasik 1999; Frerick
2003) used a relatively unknown low-back pain scale, the Arhus
Index, which was designed to monitor outcomes of clinical trials of
low-back pain. The Arhus Index is a back-pain specific index that
includes physical impairment, pain, and disability scores, which
are summed into a total score (Manniche 1994). The pain scale
is rated by the patient and includes back pain and leg pain, with
a score that ranges from 0 to 60. The disability scale consists of
a questionnaire that asks about 15 daily tasks, with a score that
ranges from 0 to 30. The physical impairment score is obtained
by scoring on a deep knee bend, a modified Schober’s test, a low-
back strength test and a measure of analgesic use, with a total
combined score ranging from 0 to 40. The higher the scores,
the more physical impairment, pain and disability. This test takes
approximately 15 minutes to complete. It has been shown to be a
valid and reliable measure of low-back pain (Manniche 1994).
In the trials using Harpagophytum Procumbens, Chrubasik 1996
used a standardized dosage of 50 mg harpagoside per day or 2400
mg of the crude extract; Chrubasik 1999 used daily dosages of the
proprietary extract WS 1531 at 600 and 1200 mg of the crude
herb, which was the equivalent of 50 and 100 mg harpagoside;
and Chrubasik 2003 used a proprietary extract of Doloteffin, con-
taining a daily dose of 60 mg harpagoside, or 12.5 mg rofecoxib
5Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Vioxx).
In the trials using White Willow Bark extract, Chrubasik 2000
utilized an extract containing 0.153 mg salicin per mg and made
comparisons between daily dose of 120 mg salicin, 240 mg of
salicin and a matched placebo; Chrubasik 2001 used Salix Alba
containing a daily dose of 240 mg salicin and compared it to
12.5 mg rofecoxib; and Krivoy 2001 used a daily dose of Salix
Alba containing 240 mg salicin compared to placebo and 100 mg
acetylsalicyliate.
The four trials using topical Capsicum Frutescens preparations
used a topical plaster application containing 11 mg of capsaici-
noids per plaster (Keitel 2001); a plaster containing an ethonolic
extract of Cayenne Pepper standardized to 22 ug/cm2 of capsai-
cinoids (Frerick 2003); a gel called Cremor Capsici Compositus
FNA, which contains 100 mg of Capsicum Oleoresin (BPC), 10
g of glycol salicylate, 1 g of methylnictinate, and a combined 1 g
of histamine hydrochloride, sorbitol, methylprahydroxybenzoate,
triethanolamine, lanette wax, stearic acid, and purified water (Stam
2001); or another gel, Rado-Sailil, containing 17.64 mg acetylsal-
icylate, 26.47 mg methylsalicylate, 8.82 mg glycosalicylate, 8.82
mg salicylic acid, 4.41 mg camphor, 55.14 mg menthol and 15.44
mg Capsicum Oleoresin per gram (Ginsberg 1987).
Nine of the ten studies reported adverse events associated with
the study medication. One trial did not report any information
regarding adverse events. All details of each trial are reported in
the table of included studies.
Conflict of interest was assessed by looking at funding sources
(public vs. private) and whether an author was employed by a
private pharmaceutical, nutraceutical, or herbal medicine man-
ufacturer. Two trials reported no conflict of interest (Ginsberg
1987; Chrubasik 1999). A conflict of interest was deemed possible
in six trials (Chrubasik 1996; Chrubasik 2000; Chrubasik 2003;
Frerick 2003; Keitel 2001; Stam 2001). In three trials, an author
was employed by a pharmaceutical company (Keitel 2001; Frerick
2003; Stam 2001), one trial was funded by a professional academy
(Chrubasik 2000), one trial was funded by a pharmaceutical com-
pany (Chrubasik 2003), and for one trial, the experimental herbal
medicine was supplied by a company (Chrubasik 1996). In the
final two trials (Chrubasik 2001; Krivoy 2001), we felt a conflict
of interest was unlikely.
Risk of bias in included studies
Initially, several ratings for the fulfilment of methodological quality
criteria for individual studies varied between authors. Specifically,
there were 28 disagreements on 110 individual ratings, for a raw
agreement of 74.5%. A total 19 of the disagreements resulted from
disparate interpretations of the methodological quality items and
the additional nine disagreements resulted from reading errors
in the trials. These disagreements were easily resolved through
discussion between the raters without the need for a third party.
The agreement between the two authors (JJG, MVT) regarding
total methodological quality scores for individual trials was fair, as
indicated by a Cohen’s kappa statistic of 0.42. Contact with one
primary author clarified one ’don’t know’, changing the item to a
’yes’ in one trial (Chrubasik 2003).
The mean score for methodological quality of all included studies
was 6.6, with a median score of seven and a range of five to nine.
Using a cut-off point of six fulfilled criteria out of 11, eight of the
10 trials (80%) were of high quality (Chrubasik 1996; Chrubasik
1999; Chrubasik 2003; Chrubasik 2000; Chrubasik 2001; Frerick
2003; Keitel 2001; Stam 2001).
The main methodological shortcomings of the Harpagophytum
trials included a lack of reporting of allocation concealment, com-
pliance rates, controls for co-interventions and acceptability of
withdrawal or drop-out rates during the follow-up period. Of the
Salix trials, one was an open-label trial and the additional two did
not report allocation concealment, compliance rates, controls for
co-interventions or the acceptability of withdrawal or drop-out
rates during the follow-up period. The Capsicum trial by Stam
2001 was assessed to be of high methodological quality. The addi-
tional Capsicum trials failed to report the type of randomization,
allocation concealment, similarity of baselines, outcome assessor,
investigator and participant blinding, comparability of co-inter-
ventions, and acceptability of compliance. Details regarding the
fulfilment of specific criteria for each individual trial are given in
Figure 1.
6Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
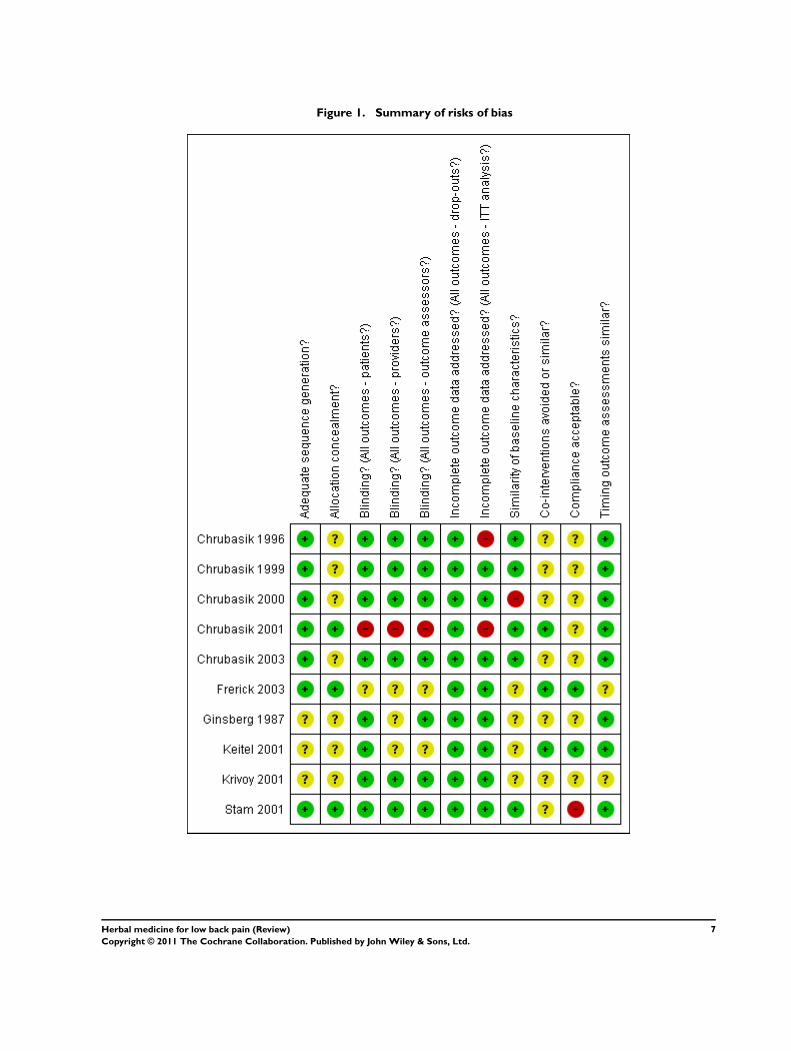
Figure 1. Summary of risks of bias
7Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Clinical relevance
There were 15 disagreements on 50 individual ratings of clini-
cal relevance, but these were easily resolved during the consen-
sus meeting. Three trials met all five clinical relevance criteria
(Chrubasik 1996; Chrubasik 2000; Ginsberg 1987). Of the tri-
als testing Harpagophytum Procumbens, two trials did not meet
items four and five (Chrubasik 1999; Chrubasik 2003). Of the
Salix Alba trials, one did not meet item one (Krivoy 2001), one
did not meet items four and five (Chrubasik 2001) and it was
not possible to tell if one trial fulfilled items four and five or not
(Krivoy 2001). Of the Capsicum Frutescens trials, two did not
meet item one (Ginsberg 1987; Keitel 2001), two did not meet
items four and five (Stam 2001; Frerick 2003), and for one trial,
it was not possible to tell if items four and five were met or not
(Keitel 2001).
Effects of interventions
1a) Harpagophytum Procumbens (Devil’s Claw)
verses placebo
Three trials were identified, all of which included participants
suffering from acute exacerbations of chronic low-back pain lasting
longer than six months.
Chronic LBP
50 mg Harpagoside dose
A total of 325 patients were included in two four-week trials,
which tested extracts of Harpagophytum Procumbens standard-
ized to 50 mg harpagoside (H) per day verses placebo (Chrubasik
1999; Chrubasik 1996). Both trials found a significant increase in
the number of pain-free patients in the 50 mg H group (9% to
17%) over placebo (2% to 5%). One trial found that for patients
taking 50 mg H, the percentage with no pain or mild low-back
pain increased over the four week period (from 2% in week 1, to
24% in week 4), whereas the percentage with unbearable or severe
pain decreased over the four weeks (from 59% in week 1, to 35%
in week 4, Chrubasik 1999). Though tramadol consumption de-
creased more in both trials in the group that received 50 mg H than
in the group that received placebo, this did not reach statistical sig-
nificance in one trial (Chrubasik 1999) and the other trial did not
perform a statistical test on this measure (Chrubasik 1996). Both
trials used the Arhus Index. The overall Arhus score improved by
21% in both the 50 mg H group and the placebo group, with
no significant difference between groups. The pain subscale was
significantly improved in favour of the 50 mg H group in both tri-
als (median change for those with current low-back pain of 43%,
Chrubasik 1999; median change of 34%, Chrubasik 1996), which
was a greater improvement than that of the group that received an
additional 100 mg H in one trial (median change for those with
current low-back pain of 37%, Chrubasik 1999).
Therefore, there is strong evidence that a daily dose of 50 mg
harpagoside in an aqueous extract of Harpagophytum Procumbens
reduces pain more than placebo in the short-term, in patients with
acute episodes of chronic non-specific low-back pain. Long-term
treatment data are not yet available.
100 mg Harpagoside dose
A total of 197 patients were included in one four-week trial,
which tested Harpagophytum Procumbens standardized to 100
mg harpagoside (H) per day verses placebo (Chrubasik 1999). The
number of patients who were pain free for at least five days in the
fourth week of treatment was significantly higher (n = 10) than
in either the placebo (n = 3) or lower dose (50 mg H) groups (n
= 6). Half of the pain free patients in the 100 mg H group had a
neurological deficit at the start of the trial. The changes from base-
line in the overall Arhus Index, the pain index, invalid index and
physical impairment index were not different between the three
groups. The percentage of patients with no or mild low-back pain
increased over the four-week period, whereas the percentage with
unbearable or severe pain decreased.
Therefore, there is moderate evidence that a daily dose of 100 mg
harpagoside in an aqueous extract of Harpagophytum Procumbens
leads to a greater number of patients who are pain free for at least
five days, in the fourth week of treatment of acute episodes of
chronic non-specific low-back pain. Superiority of the higher dose
has not been shown.
1b) Salix alba versus placebo
Two trials were identified, both of which included participants
suffering from acute exacerbations of chronic low-back pain lasting
longer than six months.
CHRONIC LBP
120 mg Salicin dose
A total of 210 patients were included in a four-week trial, which
tested two doses of Salix Alba, standardized to either 120 mg or
240 mg salicin (S) per day, against placebo (n = 70 for each group;
Chrubasik 2000). The number of patients who were pain free for
8Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

at least five days in the fourth week of treatment increased from
baseline in the placebo (n = 4), 120 mg salicin group (n = 15) and
the 240 mg salicin group (n = 27), with the trend for dose being
significant. The number of patients requiring relief medication
(tramadol) during each week decreased to 33 during week four for
the placebo group, 10 for the 120 mg salicin group and three for
the 240 mg salicin group, with the trend for dose being significant.
The total Arhus Index, pain index, invalid index, and physical
impairment index did not change from baseline for the placebo
group but improved in the groups receiving either 120 mg or 240
mg salicin. The trend for dose was significant, with the group
receiving 240 mg salicin showing more improvement in the total
Arhus Index score and the pain index than the group receiving
120 mg salicin group.
Therefore, there is moderate evidence that a daily dose of 120
mg salicin from an extract of Salix Alba results in more pain-free
patients in the short-term for individuals with acute episodes of
chronic non-specific low-back pain.
240 mg Salicin dose
A total of 261 patients were included in two trials (Chrubasik
2000; Krivoy 2001). Results for the Chrubasik 2000 trial are re-
ported above. In summary, for the group that received 240 mg
salicin per day, there were more patients who were pain free for five
days during the fourth week of treatment, fewer patients required
relief medication. There was a trend of greater improvements with
higher dose for all outcomes and significant differences between
the groups receiving 120 mg and 240 mg salicin for the total Arhus
Index score and the pain index. The additional trial by Krivoy
2001, which was designed to test platelet aggregation of salix alba
extract, did not measure clinically relevant outcomes. Although
the authors stated that fewer patients in the group receiving 240
mg salicin required rescue medication (i.e. tramadol) than in the
placebo group, they did not provide any data.
Therefore, there is moderate evidence that a daily dose of 240 mg
salicin from an extract of Salix Alba reduces pain more than either
placebo or a daily dose of 120 mg of salicin in the short term for
individuals with acute episodes of chronic non-specific low-back
pain.
1c) Capsicum Frutescens versus placebo
Two trials were identified, one with acute low-back pain (Ginsberg
1987), though the actual duration of low-back pain was not de-
scribed, and one with chronic low-back pain that had lasted longer
than three months (Keitel 2001).
Acute LBP
In the trial by Ginsberg 1987, 40 subjects with acute mechanical
low-back pain were given either a cream called Rado-Salil, contain-
ing salicylate and capsicum (n = 20) or a placebo cream containing
bergamont and lavender (n = 20) for a period of 14 days. At day
three, there was an improvement in pain score in the Rado-Salil
group of almost 2 cm on the VAS, which was significantly better
than the placebo group. By day 14, the improvement increased
to 3.79 cm, which was also significantly greater than the placebo
group. In addition, both patients and physicians rated the effect
of Rado-Salil more favourably than the placebo group rated the
effect of their cream.
Therefore, there is limited evidence that Rado-Salil cream reduces
pain more than placebo in the short-term (14 days) for individuals
with newly occurring episodes of acute non-specific low-back pain.
Chronic LBP
Keitel 2001 included 154 patients with acute episodes of chronic
non-specific low-back pain who were randomly allocated to a
placebo plaster group (n = 77) and a Capsicum plaster group (n =
77) for a period of three weeks. A reduction in pain by at least 30%
was achieved in 60.9% of the Capsicum group and 42.1% of the
placebo group. A reduction in pain by at least 50% was achieved
in 35.1% of the Capsicum group and 17.1% of the placebo group.
The total Arhus score improved significantly more in the group
using Capsicum (38.5%) than in the group using placebo (28%).
Physician global ratings of efficacy were considered “excellent” or
“good” in 75.7% of those using Capsicum and 47.4% of those
using the placebo. After treatment, 13.5% of the those using Cap-
sicum and 6.6% of those using the placebo were completely symp-
tom-free. Compliance was 90.6% in the group using Capsicum
and 88.1% in the group using placebo.
In the study by Frerick 2003, 320 participants suffering from
chronic non-specific low-back pain were randomly allocated to a
placebo plaster group (n = 180) and a Capsicum plaster group (n =
180) for a period of 21 days. The total Arhus Index score decreased
significantly more in the group using Capsicum (33%) than in
the group using placebo (22%). The Arhus compound pain score
decreased significantly more in the group using Capsicum (42%)
than in those using placebo (31%). A reduction in pain by at least
30% was achieved in 67% of those using Capsicum and 49% in
those using placebo, and a reduction in pain by at least 50% was
seen in 45% and 24%, respectively. The Arhus subscale for physical
impairment also decreased significantly more in the Capsicum
group (21%) than in the placebo group (10%). Similar results
were found for the disability subscale (35% vs. 22%, respectively).
The capsicum treatment was rated as either ’excellent’ or ’good’
by investigators in 74% of cases compared to 36% for the placebo
group. Compliance was reported as being ’very good’ or ’good’ in
both groups (91% and 93%, respectively).
Therefore, there is moderate evidence that a plaster of Capsicum
Frutescens reduces pain and improves function more than placebo
in the short-term for individuals with acute episodes of chronic
non-specific low-back pain.
9Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2a) Harpagophytum Procumbens verses rofecoxib
Chronic LBP
A total of 88 patients with acute episodes of chronic non-spe-
cific low-back pain were included in a six-week trial, which tested
Harpagophytum Procumbens standardized to 60 mg harpagoside
per day verses 12.5 mg rofecoxib per day (Chrubasik 2003). There
were no statistically significant differences in the number of pa-
tients who were pain free for at least five days in the sixth week of
treatment in the 60 mg Harpagophytum Procumbens group (10/
44) than in the rofecoxib group (5/44). The number of patients
with improvements in pain scores was not different between the
two groups. This study may lack power due to its small sample
size. The number of patients using rescue medication (tramadol)
decreased from baseline in both groups, but did not differ be-
tween groups at week six. At the end of six weeks, there were no
differences between groups for current low-back pain, scores on
the Arhus pain index, invalid index, functional index, or the total
score for the Arhus Index. The health assessment questionnaire
(HAQ) improved in both groups during the six-week period, with
no differences between groups.
Therefore, there is moderate evidence that there are no statisti-
cally significant or clinically relevant differences in effectiveness
between a daily dose of 60 mg harpagoside in an aqueous extract of
Harpagophytum Procumbens and daily dose of 12.5 mg rofecoxib
the short-term for individuals with acute episodes of chronic non-
specific low-back pain.
2b) Salix alba versus rofecoxib
Chronic LBP
A total of 228 subjects with acute episodes of chronic non-spe-
cific low-back pain were included in a four-week trial (Chrubasik
2001), which tested Salix Alba standardized to provide a daily dose
of 240 mg salicin against 12.5 mg per day of rofecoxib. Both the
rofecoxib and the 240 mg salicin groups improved by 44% on
the pain scale, the Arhus invalid index, pain index, and physical
impairment index. The percentage of patients requiring NSAIDs,
tramadol, or both was 10% for the Salix Alba group and 13% for
the rofecoxib group. Approximately 90% of physicians and pa-
tients rated either treatment as effective and close to 100% rated
either treatment as acceptable.
Therefore, there is moderate evidence that there are no differences
in effectiveness between a daily dose of 240 mg salicin of an extract
of Salix Alba and a daily dose of 12.5 mg rofecoxib in the short
term, for individuals with acute episodes of chronic non-specific
low-back pain in the short-term.
3) Capsicum Frutescens verses homeopathic
treatment
Acute and chronic LBP
The trial by Stam 2001 included 161 subjects who were a mixed
group of patients with new acute low-back pain and acute episodes
of chronic low-back pain. Participants were randomly allocated to
either a Spiroflor SLR homeopathic gel (SLR) group (n = 83) or
a Cremor Capsici Compositus FNA, the Capsici Oleoresin gel,
(CCC) group (n = 78) for a period of seven days. Each of the gels
was applied at 3 g/day. Both groups showed a significant reduction
in pain on the VAS scale, with a decrease of 38.2 mm in the
SLR group and 36.6 mm in the CCC group. In the SLR group,
50% of subjects reported that treatment was 80% effective and
18% reported total (100%) effectiveness. In the CCC group, this
was 55% and 15%, respectively. There were also no differences in
the proportion of subjects using paracetamol, the proportion of
subjects still unable to work at the end of the study, and overall
efficacy.
Therefore, there is moderate evidence that there are no statistically
significant or clinically relevant differences in effectiveness between
Spiroflor SLR homeopathic gel and Cremor Capsici Compositus
FNA gel.
Sensitivity Analysis
The definition of high quality given above is somewhat arbitrary.
Therefore, the cutoff of 50% for the internal validity item score
was modified to 40% and 60% to determine if conclusions of this
review changed.
With a 40% cutoff (up to 5/11), all 10 trials included in this
review were high quality. With a 50% cutoff (up to 6/11), all trials
examining the effects of Harpagophytum extracts were of high
quality (Chrubasik 1996; Chrubasik 1999; Chrubasik 2003), two
trials examining Salix alba extracts were of high quality (Chrubasik
2000; Chrubasik 2001) while one was low quality (Krivoy 2001),
three Capsicum Frutescens trials were high quality (Frerick 2003;
Keitel 2001; Stam 2001) while one was low quality (Ginsberg
1987). With a 60% cutoff for high quality (up to 7/11), two of
the Harpagophytum trials were high quality (Chrubasik 1999;
Chrubasik 2003) while one was low quality (Chrubasik 1996),
none of the Salix Alba trials were high quality (Chrubasik 2000;
Chrubasik 2001; Krivoy 2001), and one of the Capsicum trials was
high quality (Stam 2001) while the three others were low quality
(Ginsberg 1987; Keitel 2001, Frerick 2003).
D I S C U S S I O N
10Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Methodological Quality
A total of 10 RCTs were included in this review. Three exam-
ined Harpagophytum Procumbens (Devil’s Claw), three Salix Alba
(White Willow Bark), and four Capsicum Frutescens (Cayenne).
The sensitivity analysis for methodological quality revealed that
the Harpagophytum trials were generally of high quality, the Salix
Alba trials were generally of moderate quality, and the Capsicum
trials were generally of low quality.
Although the reporting quality in these trials was poor, it is known
that methodological quality is not directly related to reporting
quality (Huwiler-Muntener 2002). Therefore, the methodological
quality of trials that were poorly reported remains unclear. The
present authors did not contact all trial authors to clarify method-
ological aspects of trials that were inadequately reported in the
published manuscripts.
Efficacy
The results of these 10 trials suggest that specific herbal medicines
may be effective for short-term (4 to 6 weeks) improvement in
pain and functional status for individuals with acute episodes of
chronic non-specific low-back pain. Seven of the trials included
in the review were placebo-controlled while three trials were com-
parative. There is insufficient evidence to make definitive con-
clusions regarding those trials comparing herbal medicine inter-
ventions with standard drugs. Two of the comparative trials used
Vioxx as a comparator and the other used a homeopathic topical
preparation. Given the recent findings of severe adverse effects of
Vioxx and its subsequent removal from the retail market, addi-
tional trials testing these herbal medicines against standard drugs
(acetaminophen, NSAIDs) are needed.
Although eight of these studies were considered to have homoge-
nous LBP populations, statistical pooling was not possible due
to lack of reporting of sufficient raw data. Therefore, we could
not provide quantitative evidence of efficacy of herbal medicine in
general, or of any of the three individual herbal medicines used in
these trials. Instead, we used levels of evidence to synthesize. Long
term efficacy (e.g. return to work, recurrence) was not assessed in
any of these trials and therefore remains to be determined.
Given the overwhelming evidence that conflicts of interest may
bias trial results, we assessed the potential for conflict of interest
in these trials. We determined that a conflict of interest was a
possibility in six trials included in this review. At this point, it is
not possible to determine the specific influence of these potential
conflicts on results of this review.
This review highlights research that, when combined, indicates
that there are at least two herbal medicines that have good evidence
for the short-term treatment of acute episodes of non-specific low-
back pain. These interventions are reported to have very few side
effects, but more research is required to more extensively explore
the safety of these herbals. The adverse effects appear to be primar-
ily confined to mild, transient gastrointestinal complaints. Large
observational studies are needed to explore the relative safety of
these herbals to standard medications such as acetaminophen and
NSAIDs.
This review has several strengths, including the comprehensive
search strategy, the inclusion of only the highest quality trial design
and use of suggested methods for systematic reviews of interven-
tions for low-back pain (van Tulder 2003). One obvious drawback
of this review is that many of the trials included were authored by
the same trialists (Chrubasik and colleagues). It is possible that the
results may be systematically biased in some way. It is imperative
that trials of these herbal medicines be repeated by other research
groups and in different settings.
The qualitative analysis used here may be regarded as a strength
and drawback. That is, though it would have been incorrect to
statistically combine data from heterogeneous trials, the qualita-
tive method used does not provide information on the size of the
treatment effect. Without this quantitative data it is hard to de-
termine whether these herbal interventions cause clinically signifi-
cant effects on patients suffering from non-specific low-back pain.
Quantitative analyses were precluded by incomplete reporting in
these trials. Recent evidence suggests that reporting of clinical tri-
als, irrespective of the intervention, is poor (e.g. Moher 2001).
Specifically, randomised controlled trials of herbal interventions
have been found to report less than half of the required informa-
tion as outlined by the CONSORT statement (Gagnier 2006a).
An extension of the CONSORT statement for the reporting of
RCTs of herbal medicine interventions has been developed and
should be referred to when reporting such trials (Gagnier 2006b).
These guidelines will aid trialists in planning, implementing, and
reporting controlled clinical trials.
Another drawback of this review results from the known hetero-
geneity of herbal medicine products. That is, herbal medicines
often vary the in the type of preparation (liquid, VS dried, VS
topical) and thus in the amount of chemical constituents per dose.
These variations influence the pharmacokinetics and therefore the
relative efficacy of these products.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
An aqueous extract of Harpagophytum Procumbens at a stan-
dardized daily dosage of 50 mg harpagoside, an extract of Salix
Alba at a standardized dosage of 240 mg salicin/day, and a plaster
of Capsicum Frutescens seem to reduce pain more than placebo.
These herbal medicines could be considered as treatment options
for acute episodes of chronic low-back pain.
Implications for research
Additional high quality trials must be done to determine if
11Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Harpagophytum Procumbens standardized to 100 mg harpagoside
and Salix Alba standardized to 120 mg salicin are effective in the
treatment of low-back pain. Also, more trials are needed to more
accurately determine the efficacy of topical Capsicum Frutescens
in any kind of low-back pain. Additional trials testing these herbal
medicines against standard treatments (acetaminophen, NSAIDs)
will clarify their equivalence in terms of efficacy and effectiveness.
The quality of reporting in these trials was generally poor and thus
trialists should refer to the CONSORT statement in designing
and reporting clinical trials of herbal medicines.
A C K N O W L E D G E M E N T S
The primary author (JJG) is supported with a post-graduate fel-
lowship by the Canadian Institutes of Health Research and the
Natural Health Products Directorate, both public funding bodies
within Health Canada. Brian Berman’s work on this review was
partially funded by Grant Number R24 AT001293 from the Na-
tional Center for Complementary and Alternative Medicine (NC-
CAM). The contents of this article are solely the responsibility of
the authors and do not necessarily represent the official views of
the NCCAM, or the National Institutes of Health
R E F E R E N C E S
References to studies included in this review
Chrubasik 1996 {published data only}∗ Chrubasik S, Zimpfer CH, Schutt U, Ziegler R.
Effectiveness of harpagophytum procumbens in the
treatment of acute low back pain. Phytomedicine 1996;3:
1–10.
Chrubasik 1999 {published data only}
Chrubasik S, Junck H, Breitschwerdt H, Conradt C, Zappe
H. Effectiveness of Harpagophytum extract WS 1531 in the
treatment of exacerbation of low back pain: a randomized,
placebo-controlled, double-blind study. European Journal of
Anaesthesiology 1999;16:118–29.
Chrubasik 2000 {published data only}
Chrubasik S, Eisenberg E, Balan E, Weinberger T, Luzzati
R, Conradt C. Treatment of low back pain exacerbations
with willow bark extract: A randomized Double-Blind
Study. American Journal of Medicine 2000;109:9–14.
Chrubasik 2001 {published data only}
Chrubasik S, Kunzel O, model A, Conradt C, Black A.
Treatment of low back pain with a herbal or synthetic anti-
rheumatic: a randomized controlled study. Willow bark
extract for low back pain. Rheumatology 2001;40:1388–93.
Chrubasik 2003 {published data only}
Chrubasik S, model A, Black A, Pollak S. A randomized
double-blind pilot study comparing Doloteffin and Vioxx
in the treatment of low back pain. Rheumatology 2003;42:
141–8.
Frerick 2003 {published data only}
Frerick H, Keitel W, Kuhn U, Schmidt S, Bredehorst A,
Kuhlmann M. Topical treatment of chronic low back pain
with a capsicum plaster. Pain 2003;106:59–64.
Ginsberg 1987 {published data only}
Ginsberg F, Famaey JP. A double-blind study of topical
massage with Rado-Salil Ointment in mechanical low back
pain. The Journal of International Medical Research 1987;
15:148–53.
Keitel 2001 {published data only}
Keitel W, Frerick H, Kun U, Schmidt U, Kuhlmann M,
Bredehoorst A. Capsicum pain plaster in chronic non-
specific low back pain. Arzneimtel Forschung 2001;51(11):
896–903.
Krivoy 2001 {published data only}
Krivoy N, Pavlotzky E, Chrubasik S, Eisenberg E, Brook
G. Effects of salicis cortex extract on human platelet
aggregation. Planta Medica 2000;67:209–12.
Stam 2001 {published data only}
Stam C, Bonnet MS, van Haselen RA. The efficacy and
safety of a homeopathic gel in the treatment of acute
low back pain: a multi-centre, randomized, double-blind
comparative clinical trial. British Homeopathic Journal 2001;
90:21–8.
References to studies excluded from this review
Blank 1970 {published data only}
Blank K. Observation on the hitherto little known use of
opino-gel. Z Allgemeinmed 1970;46(17):893–4.
Chrubasik 2001a {published data only}
Chrubasik S, Kunzel O, Black A, Conradt C, Kerschbaumer
F. Potential economic impact of using a proprietary willow
bark extract in outpatient treatment of low back pain: an
open non-randomized study. Phytomedicine 2001;8(4):
241–51.
Chrubasik 2002 {published data only}
Chrubasik S, Pollak S. Pain management with herbal
antirheumatic drugs. Wien Med Wochenschr 2002;152(7-8):
198–203.
Chrubasik 2002a {published data only}
Chrubasik S, Pollak S, Conradt C. Clinical trial of willow
bark extract. We have by no means compared apples and
pears. MMW Fortschr Med 2002;28(9):10.
Chrubasik 2002b {published data only}
Chrubasik S, Pollak S. Herbal antirheumatics in treatment
of pain. Wiener Medizinische Wochenschrift 2002;152(7-8):
198–203.
Gensthaler 2000 {published data only}
Gensthaler BM. Willow bark extract relieves low back pain.
Pharmazeutische Zeitung 2000;145(48):41–2.
12Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Gobel 2001 {published data only}
Gobel H, Heinze A, Ingwersen M, Niederberger U. Effects
of Harpagophytum procumbens LI 174 (devil’s claw)
on sensory, motor und vascular muscle reagibility in the
treatment of unspecific back pain. Schmerz 2001;15(1):
10–8.
Harden 2000 {published data only}
Harden RN, Argoff C. A review of three commonly
prescribed skeletal muscle relaxants. Journal of Back &
Musculoskeletal Rehabilitation 2000;15(2/3):63–6.
Hemmila 1997 {published data only}
Hemmila HM, Keinanen-Kiukaanniemi SM, Levoska S,
Puska P. Does folk medicine work? A randomized clinical
trial on patients with prolonged back pain. Arch Phys Med
Rehabil. 1997;78(6):571–7.
Hogeboom 2001 {published data only}
Hogeboom CJ, Sherman KJ, Cherkin DC. Variation in
diagnosis and treatment of chronic low back pain by
traditional Chinese medicine acupuncturists. Complement
Ther Med 2001;9(3):154–66.
Jiang 1986 {published data only}
Jiang WZ, Zhou W, Zhao YG, Li YM, Zheng GC, Meng
WC, et al.Treatment of discogenic back and leg pain
based on differentiation of symptom-complex according to
traditional Chinese medicine. J Tradit Chin Med 1986;6(4):
267–72.
Kunzel 2002 {published data only}
Kunzel O, Conradt C, Black A, Pollak S. Comparison of
outcome measures during treatment with the proprietary
Harpagophytum extract Doloteffin(R) in patients with pain
in the lower back, knee or hip. Phytomedicine 2002;9(3):
181–94.
Laudahn 2001a {published data only}
Laudahn D, Walper A. Efficacy and tolerance of
Harpagophytum extract LI 174 in patients with chronic
non-radicular back pain. Phytotherapy Research 2001;15(7):
621–4.
Marz 2002 {published data only}
Marz RW, Kemper F. Willow bark extract--effects and
effectiveness. Status of current knowledge regarding
pharmacology, toxicology and clinical aspects. Wien Med
Wochenschr 2002;152(15-16):354–9.
Sherman 2001a {published data only}
Sherman KJ, Hogeboom CJ, Cherkin DC. How traditional
Chinese medicine acupuncturists would diagnose and
treat chronic low back pain: results of a survey of licensed
acupuncturists in Washington State. Complement Ther Med
2001;9(3):146–53.
Sherman 2001b {published data only}
Sherman KJ, Cherkin DC, Hogeboom CJ. The diagnosis
and treatment of patients with chronic low-back pain by
Traditional Chinese Medical acupuncturists. Journal of
Alternative & Complementary Medicine 2001;7(6):641–50.
Takabayashi 1990 {published data only}
Takabayashi T, Sasaki H, Shintaku Y, Sasamoto K, Ozawa
N, Hamazaki Y, et al.Effects of a medicinal herbal liqueur,
“yomeishu”, on post-operative gynecological patients. Am J
Chin Med 1990;18(1-2):51–8.
Wimmer 1997 {published data only}
Wimmer C, Ogon M, Sterzinger W, Landauer F, Stockl B.
Conservative treatment of tuberculous spondylitis: a long-
term follow-up study. J Spinal Disord 1997;10(5):417–9.
Xu 1993 {published data only}
Xu JH, Cui L, Jia BH. Effect of tonifying kidney on
compliability of the aged. Zhongguo Zhong Xi Yi Jie He Za
Zhi 1993;13(4):208–11.
Additional references
Andersson 1999
Andersson, GBJ. Epidemiological features of chronic low
back pain. Lancet 1999;354:581–5.
Astin 2000
Astin, JA, Pelletier, KR, Hansen, E. Complementary and
alternative medicine use among elderly persons: one-year
analysis of a Blue-Shield Medicare Supplement. J Gerentol:
A Biol Sci Med Sci 2000;55A(1):M4–M9.
Blumenthal 1998
Blumenthal M (Ed.). The Complete German Commission E
Monographs: Therapeutic Guide to Herbal Medicines. Austin:
American Botanical Council, 1998.
Borkan 1995
Borkan J, Reis S. Talking about pain: A patient-centered
study of low back pain in primary care. Soc Sci Med 1995;
40(7):977–88.
Cherkin 1993
Cherkin DC, Deyo RA. Non-surgical hospitalization for
low back pain. Is it necessary?. Spine 1993;18:1728–35.
Coste 1994
Coste J, Delecoeuillerie G, Cohen de Lara, Le Parc JM,
Paolaggi JB. Clinical course and prognostic factors in acute
low back pain: an inception cohort study in primary care
practice. Br Med J 1994;308:577–80.
Dept Labor 1995
United States Department of Labor, Bureau of Labor
Statistics. Survey of Occupational Injuries and Illnesses
1993. U.S. Dept. of Labor, Bureau of Labor Statistics
website. Washington: U.S. Department of Labor Bureau of
Labor Statistics, 1995.
Druss 1999
Druss BG, Rosenheck RA. Association between use of
unconventional therapies and conventional medical services.
JAMA 1999;282(7):651–6.
Eisenberg 1998
Eisenberg DM, Davis RB, Ettner SL. Trends in alternative
medicine use in the United States, 1990-1997: Results of a
follow-up national survey. JAMA 1998;280(18):1569–75.
Gagnier 2006a
Gagnier JJ, DeMelo J, Boon H, Rochon P, Bombardier C.
Quality of reporting of randomized controlled trials of
herbal interventions. American Journal of Medicine 2006 (In
press);119(9):800.e1–11.
13Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Gagnier 2006b
Gagnier JJ, Boon H, Rochon P, Moher D, Barnes J,
Bombardier C for the CONSORT Group. Reporting
randomized, controlled trials of herbal interventions: an
elaborated CONSORT statement. Annals of Internal
Medicine 2006 (In Press);144(5):364–7.
Huwiler-Muntener 2002
Huwiler-Muntener K, Juni P, Junker C, Egger M, Jadad A.
Quality of reporting of randomized trials as a measure of
methodologic quality. JAMA 2002;287(21):2801–4.
Krivoy 2000
Krivoy N, Pavlotzky E, Chrubasik S. Effects of salicis cortex
extract on human platelet aggregation. Planta Medica 2000;
67:209–12.
Little 1996
Little P, Smith L, Cantrell T, Chapman J, Langridge J,
Pickering R. General practitioners’ management of acute
back pain: a survey of reported practice compared with
clinical guidelines. BMJ 1996;312:485–8.
Manniche 1994
Manniche C, Asmussen K, Lauritsen B, Vinterberg H,
Kreiner S, Jordan A. Low back rating scale: validation of a
tool for assessment of low back pain. Pain 1994;57:317–26.
Millar 2001
Millar WJ. Patterns of use: Alternative health-care
practitioners. Health Reports 2001;13(1):9–22.
Mills 2000
Mills S, Bone K. Principles and Practice of Phytotherapy:
Modern Herbal Medicine. Edinburgh: Churchill Livingston,
1999.
Mills 2002
Mills EJ, Hollyer T, Guyatt G, Ross CP, Saranchuk R,
Wilson K. Teaching evidence-based complementary and
alternative medicine: 1. A learning structure for clinical
decision changes. J Altern Complement Med 2002;8(2):
207–14.
Moher 2001
Moher D, Jones A, Lepage L for the CONSORT Group.
Use of the CONSORT statement and quality of reports
of randomized trials: A comparative before and after
evaluation. JAMA 2001;285(15):1992–5.
Mounce 2002
Mounce K. Back Pain (editorial). Rheumatology 2002;41:
1–5.
Papageorgiou 1995
Papageorgiou AC, Croft PR, Ferry S, Jayson MIV, Silman
AJ. Estimating the prevalence of low back pain in the
general population. Evidence from the South Manchester
Back Pain Survey. Spine 1995;20:1889–94.
Praemer 1992
Praemer A, Furner S, Rice DP. Musculoskeltal conditions in
the United States. 1992.
Robinson 2002
Robinson KA, Dickerson K. Development of a highly
sensitive strategy for the retrieval of reports of controlled
trials using PubMed. Intern J Clin Epi 2002;31:150–3.
Sierpina 2002
Sierpina V. Progress notes: A review of educational
developments in CAM. Alternative Therapies in Health and
Medicine 2002;8(6):104–6.
van Tulder 1997
van Tulder MW, Assendelft WJJ, Koes BW. Method
guidelines for systematic reviews in the Cochrane
Collaboration Back Review Group for Spinal Disorders.
Spine 1997;22(20):2323–30.
van Tulder 2002a
van Tulder M, Koes B. Low back pain and sciatica: acute.
Clinical Evidence 2002;8:1156–70.
van Tulder 2002b
van Tulder M, Koes B. Low back pain and sciatica: chronic.
Clinical Evidence 2002;8:1171–87.
van Tulder 2003
VanTulder M, Furlan A, Bombardier C, Bouter L and the
Editorial Board of the Cochrane Collaboration Back Review
Group. Updated guidelines for systematic reviews in the
Cocrhane Collaboration Back Review Group. Spine 2003;
12:1290–9.
Vickers 2000
Vickers A. Recent advances: Complementary Medicine.
BMJ 2000;321:683–6.
Waddell 1996
Waddell, G. Low back pain: a twentieth century health-care
enigma. Spine 1996;21:2820–5.∗ Indicates the major publication for the study
14Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
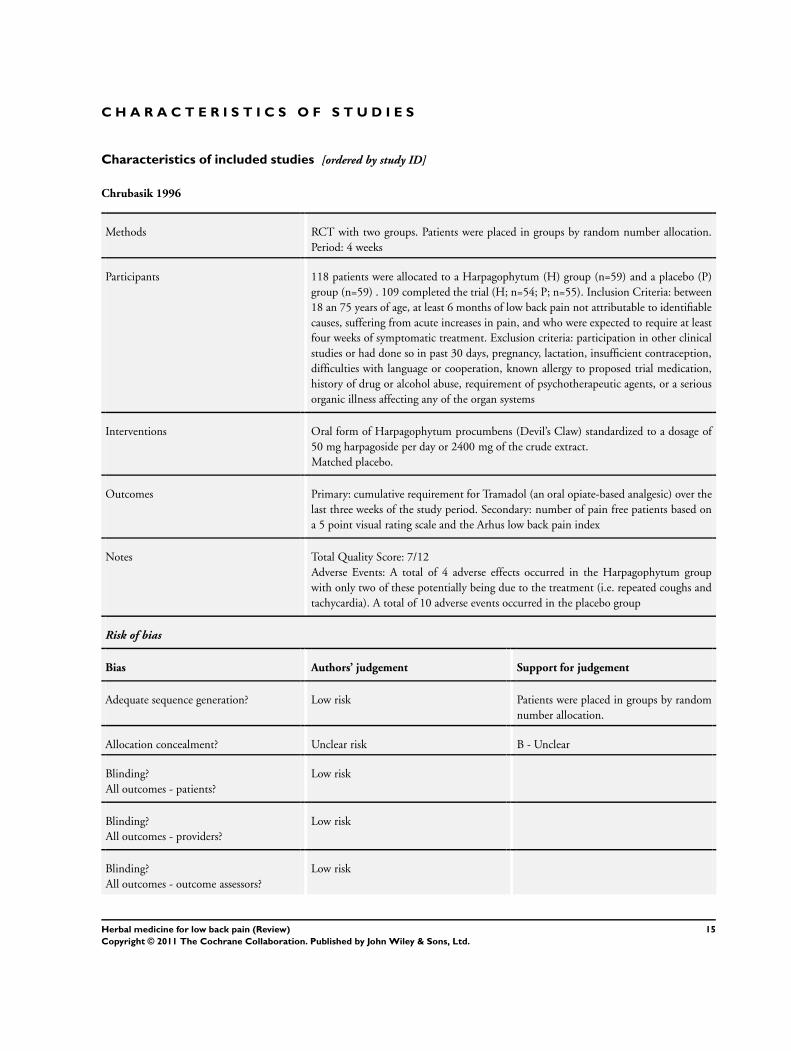
Chrubasik 1996
Methods RCT with two groups. Patients were placed in groups by random number allocation.
Period: 4 weeks
Participants 118 patients were allocated to a Harpagophytum (H) group (n=59) and a placebo (P)
group (n=59) . 109 completed the trial (H; n=54; P; n=55). Inclusion Criteria: between
18 an 75 years of age, at least 6 months of low back pain not attributable to identifiable
causes, suffering from acute increases in pain, and who were expected to require at least
four weeks of symptomatic treatment. Exclusion criteria: participation in other clinical
studies or had done so in past 30 days, pregnancy, lactation, insufficient contraception,
difficulties with language or cooperation, known allergy to proposed trial medication,
history of drug or alcohol abuse, requirement of psychotherapeutic agents, or a serious
organic illness affecting any of the organ systems
Interventions Oral form of Harpagophytum procumbens (Devil’s Claw) standardized to a dosage of
50 mg harpagoside per day or 2400 mg of the crude extract.
Matched placebo.
Outcomes Primary: cumulative requirement for Tramadol (an oral opiate-based analgesic) over the
last three weeks of the study period. Secondary: number of pain free patients based on
a 5 point visual rating scale and the Arhus low back pain index
Notes Total Quality Score: 7/12
Adverse Events: A total of 4 adverse effects occurred in the Harpagophytum group
with only two of these potentially being due to the treatment (i.e. repeated coughs and
tachycardia). A total of 10 adverse events occurred in the placebo group
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Patients were placed in groups by random
number allocation.
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - providers?
Low risk
Blinding?
All outcomes - outcome assessors?
Low risk
15Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chrubasik 1996 (Continued)
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
High risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk Unclear from text
Compliance acceptable? Unclear risk Unclear from text
Timing outcome assessments similar? Low risk
Chrubasik 1999
Methods RCT with 3 groups. Period: 4 weeks
Participants 197 patients allocated to Harpagophytum at 600 mg (n=65), or 1200 mg (n=66) or
matched placebo (n=66). Inclusion criteria: 18-75 years of age, 6 months of non-specific
low back pain, a current exacerbation of their complaint that was effecting both rest
and movement, which was giving rise to pain greater than 5 on a 1-10 VAS and was
expected to require at least 4 weeks of symptomatic treatment. Exclusion criteria: current
or recent participation in any other clinical study, serious organic illness effecting any
organ system, a history of drug or alcohol abuse or requirement for psychotherapeutic
agents, pregnancy (actual or possible), or lactation, known allergy to any the proposed
trial medications, difficulties with language or anticipated co-operation
Interventions Harpagophytum Extract WS 1531 600 mg (50 mg harpagoside), 1200 mg (100 mg
harpagoside)
Outcomes Primary outcome: proportion of pain free patients without tramadol for at least 5 days
during the last week of treatment. Secondary outcomes: Arhus index, percentage requir-
ing tramadol, verbal pain ratings
Notes Total Quality Score: 8/12
Adverse effects included: 9 with gastrointestinal upset (4 in each active group and 1 in
the placebo group)
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk
Allocation concealment? Unclear risk B - Unclear
16Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chrubasik 1999 (Continued)
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - providers?
Low risk
Blinding?
All outcomes - outcome assessors?
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
Low risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk Unclear from text
Compliance acceptable? Unclear risk Unclear from text
Timing outcome assessments similar? Low risk
Chrubasik 2000
Methods RCT with three groups. No report of randomization method. Period: 4 weeks
Participants Patients were recruited from the Haifa area in Israel between May and November. 210
patients were randomized into three groups (n=70 in each group). 191 completed the
trial (P; n= 59; 120; n=67; 240; n=65).
Inclusion criteria: Between 18 and 75 years of age, at least 6 months of intermittent
low back pain that was not attributable to identifiable causes, a current exacerbation
of their complaint at rest and with movement that caused pain of at least 5 out of 10
on a VAS and that was expected to require at least 4 weeks of treatment. Exclusion
Criteria: participation in other clinical studies or had done so in past 30 days, pregnancy,
lactation, insufficient contraception, difficulties with language or cooperation, known
allergy to proposed trial medication, history of drug or alcohol abuse, requirement of
psychotherapeutic agents
Interventions Extract of dry Willow Bark (Salix Alba): 120 mg salicin, 240 mg salicin. Matched placebo
Outcomes Primary outcome: the proportion of patients who responded to treatment by being pain
free without tramadol for at least 5 days during the last week of treatment. Secondary
outcome: The Arhus Low Back Pain Index scores
Notes Total quality score: 7/12
Adverse events: one adverse reaction (exanthem, swollen eyes, pruritis) could be at-
tributed to the 120 mg willow bark extract group. A total of two patients in the 240
17Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chrubasik 2000 (Continued)
mg group reported short lasting adverse events (dizziness attributed to tramadol, dizzi-
ness and fatigue). These patients dropped-out for seemingly unrelated reasons. A total 6
adverse events were reported in the placebo group including 3 attributable to tramadol
(dizziness/headache, dizziness/ vomiting/diarrhea, dry mouth) and the 3 others reported
mild abdominal pain 2 of whom dropped out on the first day of the trial
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - providers?
Low risk
Blinding?
All outcomes - outcome assessors?
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
Low risk
Similarity of baseline characteristics? High risk
Co-interventions avoided or similar? Unclear risk Unclear from text
Compliance acceptable? Unclear risk Unclear from text
Timing outcome assessments similar? Low risk
Chrubasik 2001
Methods Open RCT with two groups comparing an herbal medicine (Salix alba) to a synthetic
anti-rheumatic (rofecoxib).
Period: 4 weeks.
Participants 228 individuals divided equally in to two groups (n=114 per group).
Inclusion criteria: age 18 to 80, 6 at least 6 months non-specific low back pain.
Exclusion criteria: recent trauma, a history of cancer or risk factors for spinal infection,
unexplained weight loss or recent fever or chills, pain exacerbated by being supine or
severe nocturnal pain, perineal anaesthesia, recent onset of bladder dysfunction or severe
18Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
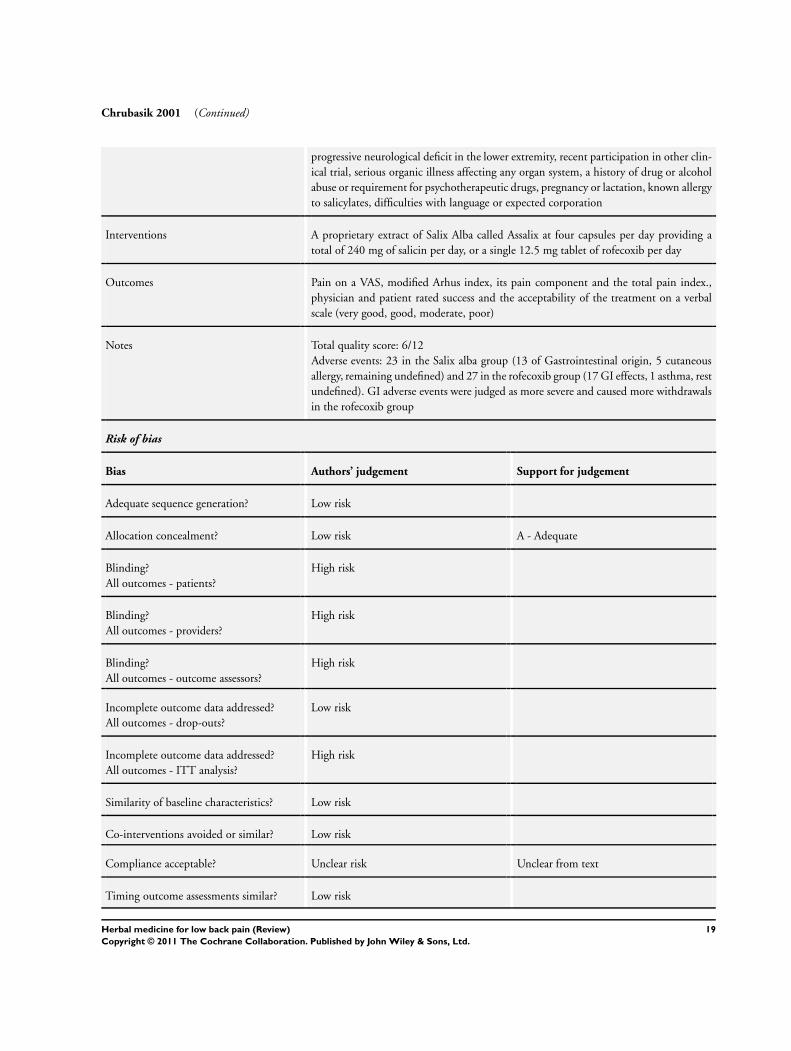
Chrubasik 2001 (Continued)
progressive neurological deficit in the lower extremity, recent participation in other clin-
ical trial, serious organic illness affecting any organ system, a history of drug or alcohol
abuse or requirement for psychotherapeutic drugs, pregnancy or lactation, known allergy
to salicylates, difficulties with language or expected corporation
Interventions A proprietary extract of Salix Alba called Assalix at four capsules per day providing a
total of 240 mg of salicin per day, or a single 12.5 mg tablet of rofecoxib per day
Outcomes Pain on a VAS, modified Arhus index, its pain component and the total pain index.,
physician and patient rated success and the acceptability of the treatment on a verbal
scale (very good, good, moderate, poor)
Notes Total quality score: 6/12
Adverse events: 23 in the Salix alba group (13 of Gastrointestinal origin, 5 cutaneous
allergy, remaining undefined) and 27 in the rofecoxib group (17 GI effects, 1 asthma, rest
undefined). GI adverse events were judged as more severe and caused more withdrawals
in the rofecoxib group
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk
Allocation concealment? Low risk A - Adequate
Blinding?
All outcomes - patients?
High risk
Blinding?
All outcomes - providers?
High risk
Blinding?
All outcomes - outcome assessors?
High risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
High risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Low risk
Compliance acceptable? Unclear risk Unclear from text
Timing outcome assessments similar? Low risk
19Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chrubasik 2003
Methods RCT with two groups. Period: 6 weeks
Participants 88 subjects allocated to Harpagophytum Procubens (n=44) group or rofecoxib (n=44).
Inclusion criteria: age 45 to 75, at least 6 months of non-specific low back pain, current
exacerbation of complaints for 8 weeks that was affecting both rest and movement,
was causing pain of at least 5 out of 10 on a visual analogue scale and was judged to
require symptomatic treatment for 6 weeks. Exclusion criteria: red flags for low back
pain, participation in any other clinical study within the last 30 days, serious organic
illness affecting any organ system, a history of drug or alcohol abuse or requirement of
psychotherapeutic drugs, pregnancy or lactation, known allergies to trial medication,
and anticipated difficulties with language or corporation
Interventions Harpagophytum Procumbens in a proprietary aqueous extract called Doloteffin (stan-
dardized to contain 60 mg harpagoside) or 12.5 mg rofecoxib per day
Outcomes Primary outcome: proportion of patients who recorded “no pain” without using tra-
madol for at least 5 days in the final week or treatment. Secondary and other outcomes:
proportion of patients in whom the averaged daily pain scores in the 6th week had
decreased by 20 to 50% of the average in the first week; the percentage change from
baseline of a modified Arhus low back pain index; the percentage change from baseline
on the Health Assessment Questionnaire; tramadol requirement
Notes Total Quality Score: 8/12
Adverse effects: 14 participants in each group. GI: 8 in the Devil’s claw group, 9 in
the Vioxx group which tended to be more severe. Two serious adverse events occurred
in the Devil’s claw group but were judged as being unrelated to the study medication.
Circulatory and laboratory variables were not affected by either treatment
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - providers?
Low risk
Blinding?
All outcomes - outcome assessors?
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
20Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chrubasik 2003 (Continued)
Incomplete outcome data addressed?
All outcomes - ITT analysis?
Low risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk Unclear from text
Compliance acceptable? Unclear risk Unclear from text
Timing outcome assessments similar? Low risk
Frerick 2003
Methods RCT with two groups. Period: 3 weeks
Participants 320 subjects with chronic non-specific low back pain divided equally between capsicum
plaster group and placebo group
Interventions Topical plaster containing an ethonolic extract of Cayenne Pepper standardized to 22
ug/cm2 of capsaicinoinds or placebo plaster
Outcomes Outcomes: Arhus Low Back Pain Rating Scale, global assessment of efficacy by patient
and investigator, global assessment of safety by patient and investigator
Notes Total Quality Score: 6/12
Adverse effects: 14 participants in each group. GI: 8 in the Devil’s claw group, 9 in
the Vioxx group which tended to be more severe. Two serious adverse events occurred
in the Devil’s claw group but were judged as being unrelated to the study medication.
Circulatory and laboratory variables were not affected by either treatment
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk
Allocation concealment? Low risk A - Adequate
Blinding?
All outcomes - patients?
Unclear risk Unclear from text
Blinding?
All outcomes - providers?
Unclear risk Unclear from text
Blinding?
All outcomes - outcome assessors?
Unclear risk Unclear from text
21Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Frerick 2003 (Continued)
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
Low risk
Similarity of baseline characteristics? Unclear risk Unclear from text
Co-interventions avoided or similar? Low risk
Compliance acceptable? Low risk
Timing outcome assessments similar? Unclear risk Unclear from text
Ginsberg 1987
Methods RCT with 40 patients assigned to 1 of 2 groups for period of 14 days
Participants 40 patients with acute mechanical low back pain were assigned to either the Rado-Salil
(a capsicum containing cream) group (n=20) or a placebo group (n=20). Each patient
was also given 45 paracetamol 250 mg tablets. No other analgesic, anti-inflammatory
drug or physical treatment was allowed during the 12 week period.
Method of patient selection: clinical examination, standard radiological examination of
the lumber spine, routine laboratory tests
Interventions Rado-Salil ointment (containing 17.64 mg ethysalicylate, 26.47 mg methylsalicylate, 8.
82 mg glycosalicylate, 8.82 mg salicylic acid, 4.41 mg camphor, 55.14 mg menthol and
15.44 mg capsicum oleoresin per 1 g) in the form of a 40 g stick applied as needed or
a placebo (containing only the excipient with three times the amount of lavendula and
bergamot essences) matched for appearance
Outcomes Outcomes: pain evaluation on a 10 cm linear scale, duration of confinement to bed,
muscular reflex contracture evaluation by the physician on a scale of 0 to 4, and spine
mobility by determination of Schober’s index, the finger to floor distance, the degree of
lumbar extension, global appreciation of treatment by patient and physician
Notes Total Quality Score: 5/12
Adverse events: Pruritis, 1 in placebo, 1 in Rado-Salil group. Local erythema and burning,
3 in the Rado-Salil group
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Unclear from text
Allocation concealment? Unclear risk B - Unclear
22Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Ginsberg 1987 (Continued)
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - providers?
Unclear risk Unclear from text
Blinding?
All outcomes - outcome assessors?
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
Low risk
Similarity of baseline characteristics? Unclear risk Unclear from text
Co-interventions avoided or similar? Unclear risk Unclear from text
Compliance acceptable? Unclear risk Unclear from text
Timing outcome assessments similar? Low risk
Keitel 2001
Methods RCT with two groups. No report of randomization method. Period: 1 plaster per day at
maximum pain site for 4 to 12 hours for 3 weeks
Participants 154 patients were randomly allocated to a placebo plaster group (n=77) and a capsicum
plaster group (n=77) A total of 132 patients completed the study with data being available
for the intention to treat (ITT) analysis on 150 patients (P=0.002). A total 22 exclusions
occurred due to premature discontinuation of the treatment (n=19) failure to meet the
inclusion criteria (n=2) or unauthorized concurrent treatment (n=1). Inclusion criteria:
subjective back pain rating of 5 or more on an 11 grade visual analogue scale as well as
a duration of back pain for a minimum of 3 months at enrolment. Exclusion criteria:
alcohol abuse, drug dependence, forms of specific back pain, concomitant systemic
inflammatory rheumatic condition, no concurrent therapy for back pain
Interventions Topical plaster type application of Capsicum Frutescens (Cayenne) containing 12 mg of
capsaicinoids per plaster. Matched placebo plaster
Outcomes Primary outcome measure: Arhus Low Back Rating Scale. Secondary outcome measures:
global assessment of efficacy and tolerance by physician and patient
Notes Total quality score: 6/12
Adverse events: A total of 24 adverse events were reported (C=15; P=9). Most of these
were warmth and itching locally. The C group had 5 cases of severe adverse events
23Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Keitel 2001 (Continued)
(inflammatory contact eczema, urticaria, minute haemorrhagic spots, and vesiculation
or dermatitis) and the P group had two such cases (vesiculation or allergic dermatosis).
A total of 16 patients withdrew because of adverse events (C=10; P=6). Also, 95.9% of
the C group and 48.7% of the P group experienced sensations of warmth locally. Pruritis
was mentioned in 45.9% of the C group and 31.6% of the P group
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk No report of randomization method
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - providers?
Unclear risk Unclear from text
Blinding?
All outcomes - outcome assessors?
Unclear risk Unclear from text
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
Low risk
Similarity of baseline characteristics? Unclear risk Unclear from text
Co-interventions avoided or similar? Low risk
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Krivoy 2001
Methods 35 subjects randomized to two groups and a further 16 acted as controls. Period: 4 weeks
Participants 51 subjects with 19 in the salix alba group, 16 in a placebo group, and 16 in an acetyl-
salicylate group.
Inclusion criteria:acute exacerbations of chronic low back pain, stable ischemic heart
disease. Exclusion criteria: NSAID use
Interventions 786.48 mg twice per day of an ethanol extract of the bark of Salix Daphnoides (240 mg
salicin content per day), matched placebo, or 100 mg acetylsalicylate
24Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Krivoy 2001 (Continued)
Outcomes Primary outcome: platelet aggregation
Notes Total quality score: 5/12
Adverse events: none reported
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Unclear from text
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - providers?
Low risk
Blinding?
All outcomes - outcome assessors?
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
Low risk
Similarity of baseline characteristics? Unclear risk Unclear from text
Co-interventions avoided or similar? Unclear risk Unclear from text
Compliance acceptable? Unclear risk Unclear from text
Timing outcome assessments similar? Unclear risk Unclear from text
Stam 2001
Methods RCT with two groups (No placebo). Randomisation was performed using RCODE
software (version 3.4) in blocks of four. Period: 7 days
Participants 161 subjects who were randomly allocated to either group. A total of 6 subjects were
lost to follow-up (SLR=2; CCC=4). 21 subjects met all per protocol criteria. Inclusion
criteria: Between the ages of 18 and 65, acute attack of low back pain within previous 72
hours, free from back pain during the previous three months, at least moderately painful
limitation of movement on physical examination. Exclusion criteria: radicular symptoms,
pain above T12, rheumatoid arthritis, ankylosing spondylitis, known hypersensitivity to
25Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
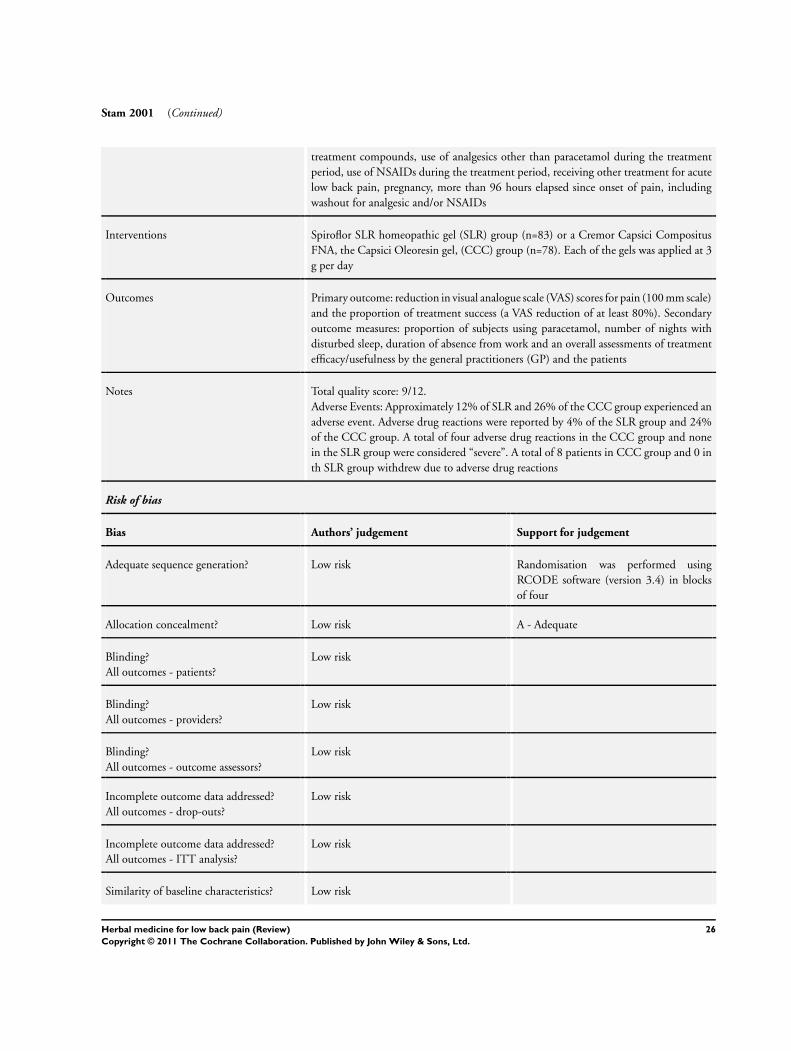
Stam 2001 (Continued)
treatment compounds, use of analgesics other than paracetamol during the treatment
period, use of NSAIDs during the treatment period, receiving other treatment for acute
low back pain, pregnancy, more than 96 hours elapsed since onset of pain, including
washout for analgesic and/or NSAIDs
Interventions Spiroflor SLR homeopathic gel (SLR) group (n=83) or a Cremor Capsici Compositus
FNA, the Capsici Oleoresin gel, (CCC) group (n=78). Each of the gels was applied at 3
g per day
Outcomes Primary outcome: reduction in visual analogue scale (VAS) scores for pain (100 mm scale)
and the proportion of treatment success (a VAS reduction of at least 80%). Secondary
outcome measures: proportion of subjects using paracetamol, number of nights with
disturbed sleep, duration of absence from work and an overall assessments of treatment
efficacy/usefulness by the general practitioners (GP) and the patients
Notes Total quality score: 9/12.
Adverse Events: Approximately 12% of SLR and 26% of the CCC group experienced an
adverse event. Adverse drug reactions were reported by 4% of the SLR group and 24%
of the CCC group. A total of four adverse drug reactions in the CCC group and none
in the SLR group were considered “severe”. A total of 8 patients in CCC group and 0 in
th SLR group withdrew due to adverse drug reactions
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Randomisation was performed using
RCODE software (version 3.4) in blocks
of four
Allocation concealment? Low risk A - Adequate
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - providers?
Low risk
Blinding?
All outcomes - outcome assessors?
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis?
Low risk
Similarity of baseline characteristics? Low risk
26Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Stam 2001 (Continued)
Co-interventions avoided or similar? Unclear risk Unclear from text
Compliance acceptable? High risk
Timing outcome assessments similar? Low risk
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Blank 1970 not an RCT
Chrubasik 2001a not an RCT
Chrubasik 2002 not an RCT
Chrubasik 2002a not an RCT
Chrubasik 2002b not an RCT
Gensthaler 2000 not an RCT
Gobel 2001 not an RCT
Harden 2000 not an RCT
Hemmila 1997 not an herbal medicine
Hogeboom 2001 not an RCT, not an herbal medicine
Jiang 1986 not an herbal medicine
Kunzel 2002 not an RCT
Laudahn 2001a not an RCT
Marz 2002 not an RCT
Sherman 2001a not an RCT, not an herbal medicine
Sherman 2001b not an RCT, not an herbal medicine
Takabayashi 1990 not low back pain
Wimmer 1997 not low back pain, not an herbal medicine
27Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
(Continued)
Xu 1993 not an RCT
28Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
This review has no analyses.
A D D I T I O N A L T A B L E S
Table 1. Criteria for the Risk of Bias Assessment
Criteria for a judgment of yes for the sources of risk of bias
Was the method of randomisation adequate? A random (unpredictable) assignment sequence. Examples of adequate methods are
computer generated random number table and use of sealed opaque envelopes. Methods of allocation using date of birth, date of
admission, hospital numbers, or alternation should not be regarded as appropriate.
Was the treatment allocation concealed? Assignment generated by an independent person not responsible for determining the eligibility
of the patients. This person has no information about the persons included in the trial and has no influence on the assignment
sequence or on the decision about eligibility of the patient.
Was the patient blinded to the intervention? The review author determines if enough information about the blinding is given in order
to score a “yes.”
Was the care provider blinded to the intervention? The review author determines if enough information about the blinding is given
in order to score a “yes.”
Was the outcome assessor blinded to the intervention? The review author determines if enough information about the blinding is
given in order to score a “yes.”
Was the withdrawal/drop-out rate described and acceptable? The number of participants who were included in the study but did
not complete the observation period or were not included in the analysis must be described and reasons given. If the percentage
of withdrawals and drop-outs does not exceed 20% for short-term follow-up or 30% for long-term follow-up and does not lead to
substantial bias a “yes” is scored. (note: these percentages are arbitrary and not supported by the literature)
Did the analysis include an intention-to-treat analysis? All randomized patients are reported/analyzed in the group to which they
were allocated by randomization for the most important moments of effect measurement (minus missing values) irrespective of
noncompliance and co-interventions
Were the groups similar at baseline regarding the most important prognostic indicators? In order to receive a “yes,” groups have to
be similar at baseline regarding demographic factors, duration and severity of complaints, percentage of patients with neurologic
symptoms, and value of main outcome measure(s).
Were co-interventions avoided or similar? Co-interventions should either be avoided in the trial design or be similar between the
index and control groups.
Was the compliance acceptable in all groups? The review author determines if the compliance to the interventions is acceptable, based
on the reported intensity, duration, number and frequency of sessions for both the index intervention and control intervention(s).
Was the timing of the outcome assessment in all groups similar? Timing of outcome assessment should be identical for all intervention
groups and for all important outcome assessments
29Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
W H A T ’ S N E W
Last assessed as up-to-date: 14 December 2005.
Date Event Description
19 January 2011 Amended Contact details updated.
H I S T O R Y
Protocol first published: Issue 4, 2003
Review first published: Issue 2, 2006
Date Event Description
23 November 2009 Amended Contact details updated.
11 June 2008 Amended Converted to new review format.
15 December 2005 New citation required and conclusions have changed Substantive amendment
C O N T R I B U T I O N S O F A U T H O R S
JJG: Wrote the body of the review, searched the literature, contacted experts for trials and clarification of methods, screened trials for
inclusion, assessed methodological quality. Prepared submission for Cochrane Back Review Group.
MVT: Searched the literature, screened trials for inclusion, assessed methodological quality, edited and contributed to the body of the
review.
CB: Edited final versions of protocol and review
BB: Screened trials for inclusion, edited final version of protocol and review.
D E C L A R A T I O N S O F I N T E R E S T
One of the authors (Claire Bombardier) is Co-ordinating Editor of the Cochrane Back Review Group. Editors are required to conduct
at least one Cochrane review. Dr. Bombardier is not the first authors of the review. An editor who is an author is excluded from editorial
decisions on the review in which they are contributors. Therefore, this involvement does not seem to be a source of conflict of interest
in the Cochrane Collaboration.
30Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
S O U R C E S O F S U P P O R T
Internal sources
• No sources of support supplied
External sources
• Natural Health Products Directorate/Canadian Institutes of Health Research, Canada.
• National Center for Complementary and Alternative Medicine, USA.
I N D E X T E R M S
Medical Subject Headings (MeSH)
∗Phytotherapy; Benzyl Alcohols [therapeutic use]; Capsicum; Cyclooxygenase 2 Inhibitors [therapeutic use]; Glucosides; Harpago-
phytum; Herbal Medicine; Lactones [therapeutic use]; Low Back Pain [∗drug therapy]; Randomized Controlled Trials as Topic; Salix;
Sulfones [therapeutic use]
MeSH check words
Adult; Humans
31Herbal medicine for low back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.