cms value-based purchasing initiatives - satro connors satro 11.pdf · 2016-12-21 · barbara j....
TRANSCRIPT
Barbara J. Connors, DO, MPH
Chief Medical Officer, Region III
The Centers for Medicare and Medicaid Services
Region III
CMS
Value-Based Purchasing
Initiatives

CMS’ Quality Improvement
Roadmap
Vision: The right care for every
person every time
Make care:
Safe
Effective
Efficient
Patient-centered
Timely
Equitable
CMS’ Quality Improvement
Roadmap
Strategies Work through partnerships
Measure quality and report comparative results
Encourage adoption of effective health
information technology
Promote innovation and the evidence base for
effective use of technology
Value-Based Purchasing: Improve quality
and avoid unnecessary costs
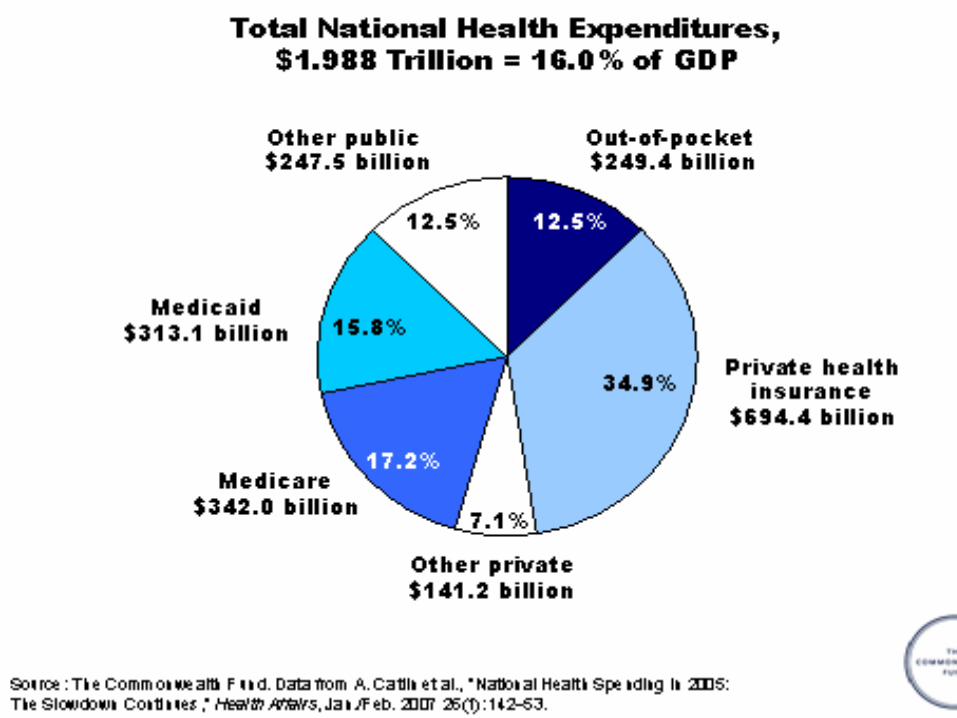
Why VBP?
Medicare Solvency and Beneficiary Impact Expenditures up from $219 billion in 2000 to a
projected $486 billion in 2009
Part A Trust Fund Excess of expenditures over tax income in 2007
Projected to be depleted by 2019
Part B Trust Fund Expenditures increasing 11% per year over the last 6
years
Medicare premiums, deductibles, and cost-sharing are projected to consume 28% of the average beneficiaries’ Social Security check in 2010
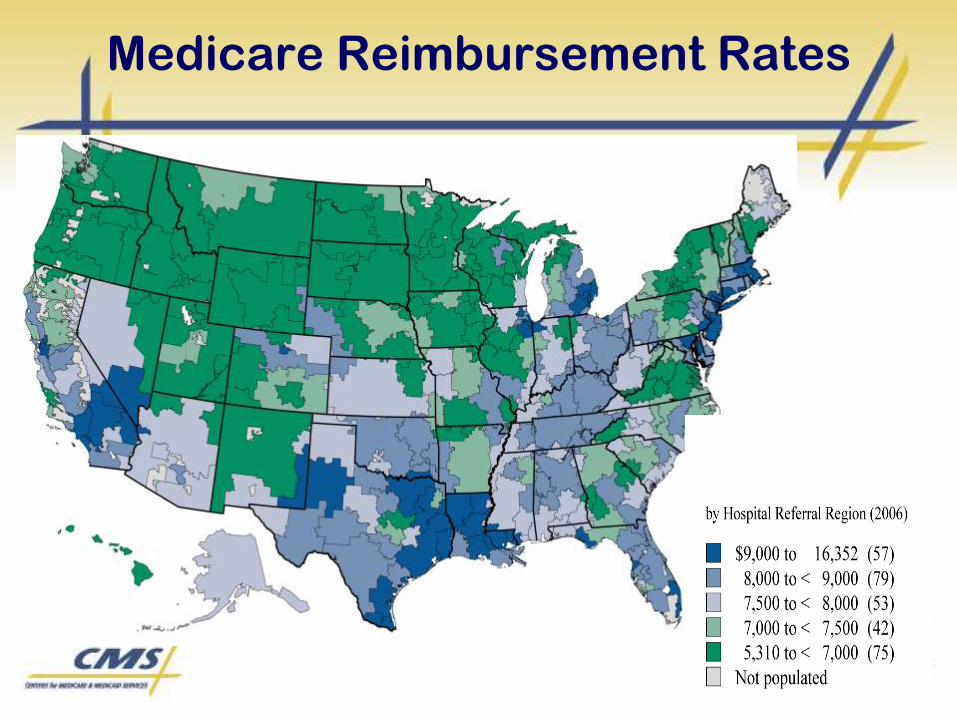
Medicare Reimbursement Rates
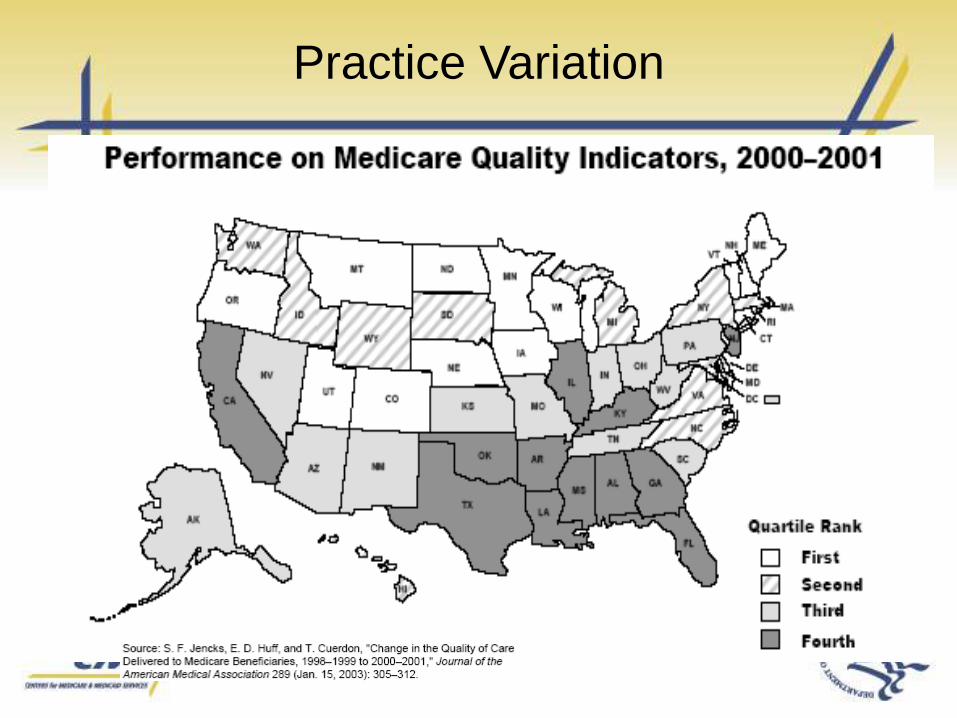
Practice Variation
What Does VBP Mean to CMS?
Transforming Medicare from a passive payer to an
active purchaser of higher quality, more efficient health
care
Tools and initiatives for promoting better quality, while
avoiding unnecessary costs
Tools: measurement, payment incentives, public reporting,
conditions of participation, coverage policy, QIO program
Initiatives: pay for reporting, pay for performance,
gainsharing, competitive bidding, bundled payment, coverage
decisions, direct provider support
Value-Based Purchasing-
What it is really about:
It is about defining/rewarding
providers for the value of their
contribution to quality and
efficient care that leads to better
health outcomes.
VBP: Payment Methodologies
• Pay for Reporting
• Pay for Participation
• Pay for Care Coordination
• Pay for Process
• Pay for Outcomes
VBP Programs
Physician Quality Reporting Initiative
Physician Resource Use Reporting
Hospital Quality Initiative: Inpatient & Outpatient Pay for Reporting
Hospital VBP Plan & Report to Congress
Hospital-Acquired Conditions & Present on Admission Indicator Reporting
VBP
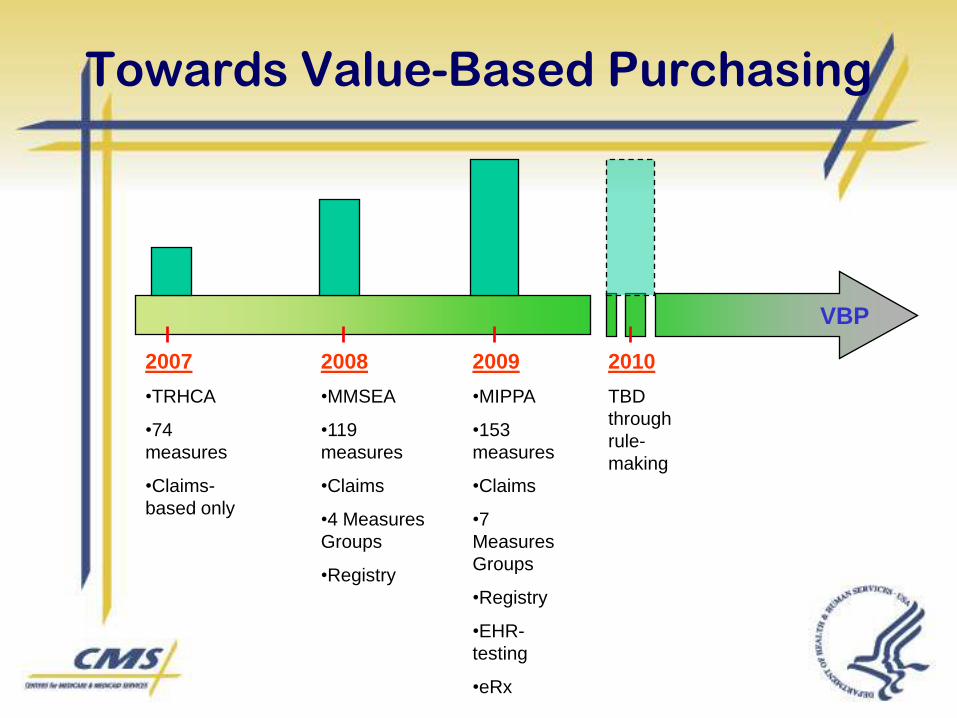
Towards Value-Based Purchasing
2007
•TRHCA
•74
measures
•Claims-
based only
2008
•MMSEA
•119
measures
•Claims
•4 Measures
Groups
•Registry
2009
•MIPPA
•153
measures
•Claims
•7
Measures
Groups
•Registry
•EHR-
testing
•eRx
2010
TBD
through
rule-
making
Statutory Authority
• Medicare Improvements for Patients and
Providers Act of 2008 (MIPPA)
– Section 131(d)
• Plan for Transition to Value-Based
Purchasing Program for Physicians and
Other Practitioners
• Report to Congress due May 1, 2010
Issues Paper Assumptions &
Design Principles
PVBP Planning will:– Focus on performance-based payment
– Accommodate different practice arrangements
– Recognize the contributions of members of the health professional team
– Address multiple levels of accountability
– Be at least budget neutral—across at least Medicare Parts A and B—and will seek to identify program savings
– Initially focus on traditional fee-for-service Medicare
– Have short-term and longer-term timeframes, with attention to transitions
– Avoid creating additional health care disparities and work to reduce existing disparities
– Include an ongoing evaluation process
Stakeholder Input:
Overarching Issues
• Affirmed goal and objectives
• Advocated for new payment approaches that
cut across settings and align Part A and B
payment incentives
• Agreed with the need to accommodate
different practice arrangements
• Praised attention to disparities
• Urged attention to operational transitions

Next Steps in Plan Development
• Receive direction from new leadership
• Design options– Physician Fee Schedule (PFS) overlay
• Performance-based PFS payments
• Medical Home
– Levels of accountability beyond individuals• Groups
• Accountable Care Entities
– Shared savings models
– Bundled payment arrangements
• Simulations pending availability of resources
• Opportunities for stakeholder input– PFS 2010 rulemaking
– Potential additional Listening Sessions
Medicare Improvements for Patients
and Providers Act of 2008 (MIPPA)
- Makes PQRI permanent; however
only 2009 and 2010 incentives are
funded
- Increased 2009 PQRI incentive to 2%
PQRI
• PQRI reporting focuses attention on quality of care– Foundation is evidence-based measures developed by
professionals.
– Reporting data for quality measurement is rewarded with financial incentive.
– Measurement enables improvements in care.
– Reporting is the first step toward pay-for-performance.
• Measures address various aspects of quality care– Prevention
– Chronic Care Management
– Acute Episode of Care Management
– Procedural Related Care
– Resource Utilization
– Care Coordination
2009 PQRI:
Eligible Professionals
• Physicians
– MD/DO
– Podiatrist
– Optometrist
– Oral Surgeon
– Dentist
– Chiropractor
• Therapists
– Physical Therapist
– Occupational Therapist
– Qualified Speech-Language Pathologist
• Practitioners
– Physician Assistant
– Nurse Practitioner
– Clinical Nurse
– Specialist
– Certified Registered Nurse
– Anesthetist
– Certified Nurse Midwife
– Clinical Social Worker
– Clinical Psychologist
– Registered Dietician
– Nutrition Professional
– Audiologist
PQRI Introduction:
Key Information
• No need to register: just begin
reporting.
• Must be an enrolled Medicare
provider (but need not have signed a
Medicare participation agreement).
• Need to use individual National
Provider Identifier (NPI).
PQRI Reporting
• CPT Category II codes used to report the
measure
• CPT II codes used in PQRI are referred to
as Quality Data Codes (QDCs)
• CPT II codes are non-billable
• Measures without assigned CPT II codes
may require the use of G Codes
Understanding the
Measure Construct
NUMERATOR
CPT II Code or Temporary G-code
(describes clinical action required for performance)
DENOMINATOR
ICD-9-CM & CPT Cat I Codes
(Describes eligible cases for which a clinical actionwas performed: the eligible patient population as
defined by denominator specification)
Reporting Quality Data
• Identify ICD-9 Code and CPT I code
• Chose CPT II code
• Exclusion modifiers
- 1P, 2P, 3P or 8P
• Modifiers indicate exclusions:– 1P- Exclusion due to Medical Reasons
– 2P- Exclusion due to Patient Reason
– 3P- Exclusion due to System Reason
– 8P- Action not performed, reason not otherwise specified
G Codes used for some measures
No modifiers apply with G codes
Different G Code for each clinical scenario
Reporting
• Paper based CMS 1500 claims
• Electronic 837-P claims
• Reported on the same claim as CPT I
• No registration is required to participate
• Voluntary program
Understanding the Measures:
Performance Time Frame
• Some measures have a Performance Timeframe related to the clinical action that may be distinct from the reporting frequency.
– Perform within 12 months
– Most Recent • Clinical test result needs to be obtained,
reviewed, reported one time. It need not have been performed during the reporting period.
Understanding the Measures:
Reporting Frequency
• Each measure has a Reporting Frequency
requirement for each eligible patient seen
during the reporting period
– Report one-time only
– Report once for each procedure performed
– Report for each acute episode
May have age relatedness
2009 PQRI Quality Measures
• 153 PQRI quality measures for 2009
– Includes 101 measures from the 2008 PQRI and 52
new measures
– E-prescribing measure (Measure #125) removed, as
required by MIPPA as a separate incentive program
– 18 measures reportable only through registries
– Measure specifications are available in the
Measures/Codes section of the website at
http://www.cms.hhs.gov/pqri.
2009 PQRI Reporting Periods
• 1 reporting period for claims-based
reporting of individual measures:
January 1, 2009 – December 31, 2009
• 2 reporting periods for reporting
measures groups and registry-based
reporting:
– January 1, 2009 – December 31, 2009
– July 1, 2009 – December 31, 2009
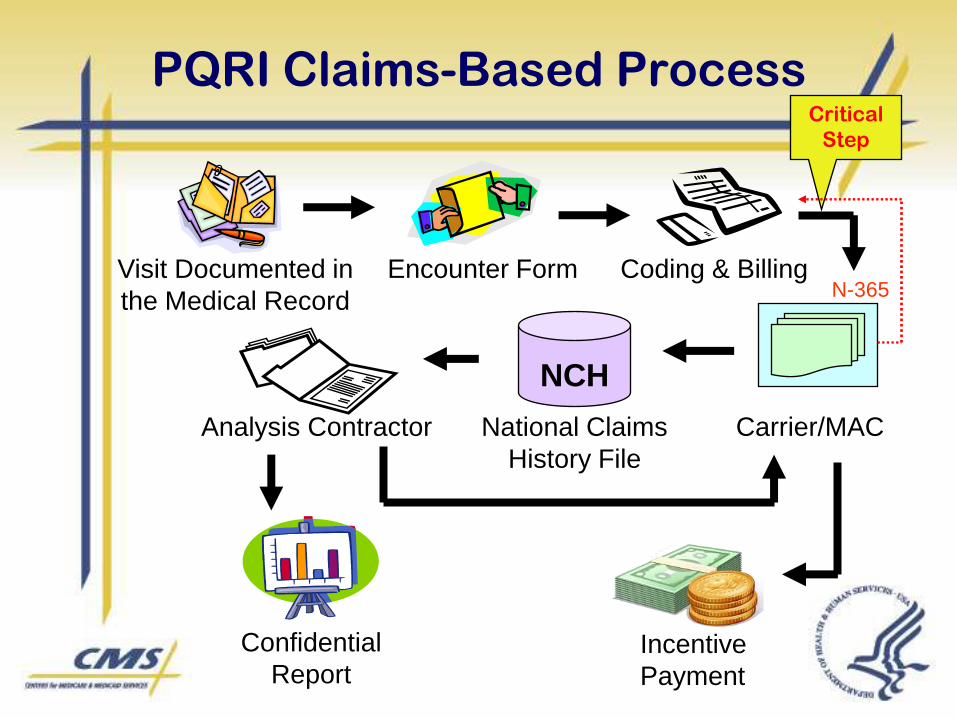
PQRI Claims-Based Process
Visit Documented in
the Medical Record
Encounter Form Coding & Billing
Carrier/MAC
NCH
Analysis Contractor National Claims
History File
Incentive
Payment
Confidential
Report
Critical
Step
N-365
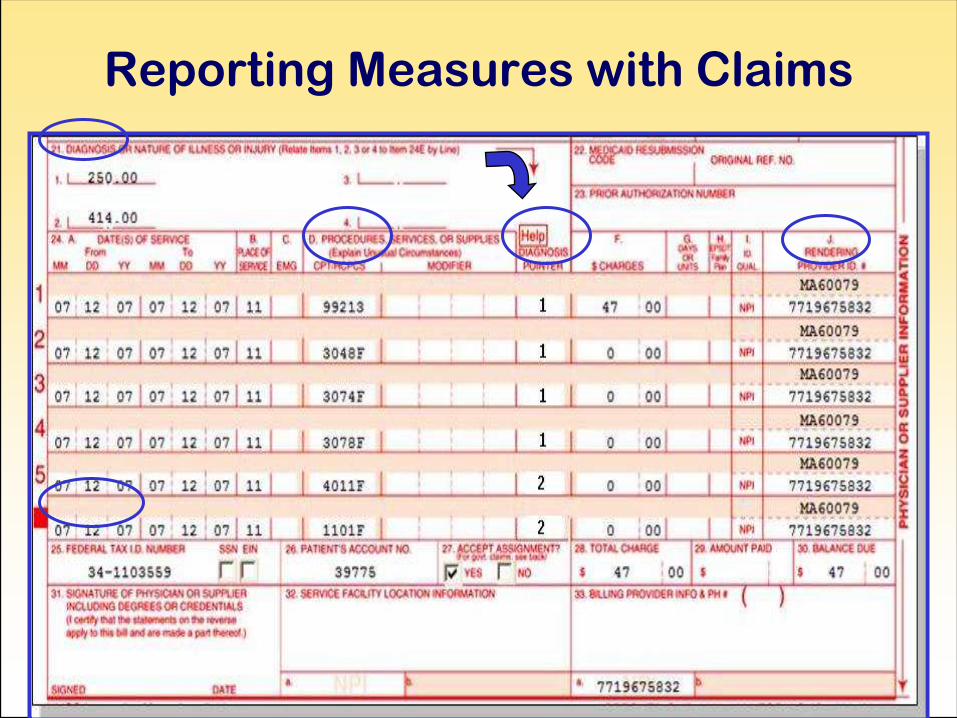
Reporting Measures with Claims
Tips: Reporting Via Registry
• At least 3 individual measures must be reported;
OR
• At least 1 measures group, which, as long as Medicare Part B FFS patients are included, may also include Medicare Advantage and non-Medicare patients when reporting using the consecutive patient sample method
• 18 PQRI measures are reportable through registry only
Measure #124: (HIT): Adoption/Use of
Electronic Health Records (EHR)
2009 PQRI REPORTING OPTIONS:
CLAIMS-BASED, REGISTRY
DESCRIPTION:
• Documents whether provider has adopted
and is using health information technology.
To qualify, the provider must have adopted
and be using a certified/qualified EHR
Measure #102: Prostate Cancer: Avoidance
of Overuse of Bone Scan for Staging Low-
Risk Prostate Cancer Patients
2009 PQRI REPORTING OPTIONS: CLAIMS-BASED, REGISTRY
DESCRIPTION
• Percentage of patients, regardless of age, with a diagnosis of prostate cancer at low risk of recurrence receiving interstitial prostate brachytherapy, OR external beam radiotherapy to the prostate, OR radical prostatectomy, OR cryotherapy who did not have a bone scan performed at any time since diagnosis of prostate cancer
Measure #104: Prostate Cancer:
Adjuvant Hormonal Therapy for High-
Risk Prostate Cancer
• 2009 PQRI REPORTING OPTIONS: CLAIMS-BASED, REGISTRY
• DESCRIPTION:
• Percentage of patients, regardless of age, with a diagnosis of prostate cancer at high risk of recurrence receiving external beam radiotherapy to the prostate who were prescribed adjuvant hormonal therapy (GnRH agonist or antagonist)
Measure #105: Prostate Cancer:
Three-Dimensional (3D) Radiotherapy
2009 PQRI REPORTING OPTIONS:CLAIMS-BASED, REGISTRY
DESCRIPTION:
• Percentage of patients, regardless of age, with a diagnosis of clinically localized prostate cancer receiving external beam radiotherapy as a primary therapy to the prostate with or without nodal irradiation (no metastases; no salvage therapy)
Measure #143: Oncology: Medical and
Radiation – Pain Intensity Quantified
2009 PQRI REPORTING OPTIONS: CLAIMS-BASED, REGISTRY
• This is a two-part measure which is paired with Measure #144: Oncology: Medical and Radiation: Plan of Care for Pain. If pain is present (CPT II code 1125F is submitted), #144 should also be reported.
DESCRIPTION:
• Percentage of patient visits, regardless of patient age, with a diagnosis of cancer currently receiving chemotherapy or radiation therapy in which pain intensity is quantified
Measure #144: Oncology: Medical and
Radiation – Plan of Care for Pain
2009 PQRI REPORTING OPTIONS: CLAIMS-BASED, REGISTRY
• This is a two-part measure which is paired with Measure #143: Oncology: Medical and Radiation: Pain Intensity Quantified. This measure should be reported if CPT II code 1125F “Pain severity quantified; pain present” is submitted for Measure #143.
• DESCRIPTION:
• Percentage of patient visits, regardless of patient age, with a diagnosis of cancer currently receiving chemotherapy or radiation therapy who report having pain with a documented plan of care to address pain
Measure #156: Oncology: Radiation
Dose Limits to Normal Tissues
2009 PQRI REPORTING OPTIONS: CLAIMS-
BASED, REGISTRY
DESCRIPTION:
• Percentage of patients, regardless of age, with a
diagnosis of pancreatic or lung cancer receiving
3D conformal radiation therapy with
documentation in medical record that radiation
dose limits to normal tissues were established
prior to the initiation of a course of 3D conformal
radiation for a minimum of two tissues
2009 PQRI Measures Resources
http://www.cms.hhs.gov/PQRI/15_MeasuresCodes.asp#TopOfPage
• List of 153 2009 PQRI Measures – measure developer, reporting method
• Reporting Individual Measures via Claims
– 2009 PQRI Measures Specifications Manual for Claims and Registry and Release Notes
– 2009 PQRI Implementation Guide
• Reporting Measures Groups via Claims
– 2009 PQRI Measures Groups Specifications Manual and Release Notes
– Getting Started with 2009 PQRI Reporting of Measures Groups
– Measures Group Sample Claim
http://www.cms.hhs.gov/PQRI/30_EducationalResources.asp#TopOfPage
• MLN Matters Articles
• Fact Sheets
• Tip Sheets
• 2009 PQRI Patient-Level Measures List

Registries
• CMS received over 55 self-nomination requests for registries to become ―qualified‖ to submit quality data for possible incentive payment on behalf of their clients.
• 32 registries have been selected for ―production‖ (eligible to earn a payment incentive for their providers)
• The final list of ―qualified‖ registries is posted on the PQRI website at: http://www.cms.hhs.gov/PQRI/20_Reporting.asp#TopOfPage and go to the first download (―2008 List of Qualified Registries‖)
• CMS received over 55 self-nomination requests for registries to become ―qualified‖ to submit quality data for possible incentive payment on behalf of their clients.
• 32 registries have been selected for ―production‖ (eligible to earn a payment incentive for their providers)
• The final list of ―qualified‖ registries is posted on the PQRI website at: http://www.cms.hhs.gov/PQRI/20_Reporting.asp#TopOfPage and go to the first download (―2008 List of Qualified Registries‖)
PQRI Reporting:
Ensuring Success
• Ensure rendering professionals’ Individual
National Provider Identifier (NPI) on all claims
• Start reporting early to increase the probability of
achieving the 80 percent rate of reporting during
the reporting period.
• Report on as many measures as possible to
increase the likelihood of achieving successful
reporting.
• Ensure that quality data codes are reported on the
same claim as the diagnosis or CPT-I codes.
Current Procedural Terminology © 2006 American Medical Association. All Rights Reserved.
42
Benefits of PQRI Participation
• Receive confidential feedback reports to support quality improvement
• Earn a bonus incentive payment
• Make an investment in the future of the practice
– Prepare for higher bonus incentives over time
– Prepare for pay-for-performance
– Prepare for public reporting of performance results
2007 PQRI Reporting
Participation Statistics
• 109, 349 NPI/TINs – Attempted to Submit
• 101,138 NPI/TINs – Submitted a Quality Data
Code Successfully
– A feedback report is available
• 70,207 NPI/TINS – Satisfactorily Reported 1 or
more measures
– A feedback report is available
• 56,722 NPI/TINs – Earned Incentive
– A feedback report & incentive payment are available
Some Common Errors in
Claims-based Reporting
• Eligible claim submitted without QDC(s)
– Providers are not identifying all eligible claims per the measure denominator: some measures include additional sites of care other than an office visit; Medicare Secondary Payer claim without QDC
• Eligible claim submitted as a QDC-only claim (no denominator information on the claim)
– Billing software may be splitting the claim
• Ineligible claim with QDC for measure
Watch the denominator:
– Dx is incorrect or insufficient on claim for measure reported
– Surgical procedure is incorrect on claim for measure reported
– Age/gender on claim is incorrect for measure reported
2007 PQRI Experience Report
QDC Submission Attempts
• 12.15% Missing NPI
• 18.89% Incorrect HCPCS code*
• 13.93% Incorrect DX code*
• 7.24% Both incorrect HCPCS code and incorrect DX code*
• 4.97% All line items were QDCs only
*Denominator mismatch
Some Common Errors in
Claims-based Reporting
• Eligible claim with insufficient QDCs
• Eligible claim denied by carrier,
subsequently submitted but without
QDC
• Eligible claim paid partially by primary
payer submitted without
QDC as Medicare Secondary Payer
• Eligible claim without individual NPI
Top Ten Most Frequently
Reported Measures by Clinical Topic
1. Pneumonia
2. Chest Pain
3. Perioperative Care
4. Diabetes
5. ECG for Syncope
6. Coronary Artery Disease
7. Myocardial Infarction
8. Heart Failure
9. Macular Degeneration
10. Glaucoma

E-Prescribing
• The Medicare Improvements for Patients
and Providers Act of 2008 (MIPPA)
authorized an additional 2% incentive
payment to EPs who are voluntary
successful e-prescribers for program years
2009 through 2013.
What is E-Prescribing?
• The transmission, using electronic media,
of prescription or prescription-related
information between a prescriber,
dispenser, pharmacy benefit manager, or
health plan either directly or through an
intermediary, including an e-prescribing
network. E-prescribing includes, but is not
limited to, two-way transmissions between
the point of care and the dispenser.
Why e-Prescribing?
- Provides warnings and alert systems
- Provides access to pts medication history and allergies
- Reduces time on pharmacy phone calls and faxing
- Automation of renewals and authorizations
- Improves formulary adherence
- lower administrative costs
- Reduces oral miscommunications and confusion at hand offs
- Solves problem of hard to read prescriptions
Why e-Prescribing?
• 98,000 die from medical errors annually
– more than breast cancer, AIDS, or motor vehicle
accidents
• 1.5 million preventable adverse drug events
annually
– Hospitals, long-term care, outpatient encounters
– 530,000 among Medicare beneficiaries
– $877 million per year for Medicare beneficiaries
Source Institute of Medicine 1999, 2000, 2003, 2006
Getting Started in E-Prescribing
• Plan and implement a process within your practice to ensure successful claims-based reporting of the E-prescribing measure.
• Appoint a member of your team as the main contact person for trouble-shooting or fielding questions.
• Ensure that your system meets qualified e-prescribing system requirements, i.e., must employ standards adopted by the Secretary for Part D by virtue of the 2003 Medicare Modernization Act (MMA) and is capable of ALL of the following functionalities:
Getting Started
– Generating a complete active medication listincorporating electronic data received from pharmacies and pharmacy benefit managers (PBMs) if available
– Selecting medications, printing prescriptions, electronicallytransmitting prescriptions, and conducting all alerts*
– Providing information related to lower cost, therapeutically appropriate alternatives (if any).
• The availability of an e-prescribing system to receive tiered formulary information, if available, would meet this requirement for 2009.
– Providing information on formulary or tiered formulary medications, patient eligibility, and authorization requirements received electronically from the patient’s drug plan (if available)
*An alert on an e-prescribing system is an automated prompt that indicates a potential inappropriate medication dose, route of administration, interactions, allergy concerns and warnings/cautions.
2009 Adoption and Use of
Medication E-Prescribing Measure
• E-prescribing quality measure may only be reported via a claims-based method.
• Eligible professionals (EPs) who successfully report (e-prescribers) may receive an incentive payment equal to 2% of total allowed charges for covered professional services furnished to patients enrolled in Medicare Part B* during the reporting period (January 1 through December 31, 2009).
• To qualify as a successful e-prescriber, a minimum of 10% of their Medicare Part B allowed charges must be generated from the specified denominator codes in the measure and the e-prescriber must report on at least 50% of all Medicare Part B patient encounters.
*Medicare Advantage or Private FFS patients are not included in the incentive
E-Prescribing Measure –
Denominator
Patient encounter for covered services during the reporting period (CPT or HCPCS):
• 90801, 90802, 90804, 90805, 90806, 90807, 90808, 90809
• 92002, 92004, 92012, 92014
• 96150, 96151, 96152
• 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, 99215, 99241, 99242, 99243, 99244, 99245
• G0101, G0108, G0109
E-Prescribing Measure –
Numerator
• Prescriptions Generated via Qualified E-Prescribing System
– G8443: All prescriptions created during the encounter were generated using a qualified e-prescribing system OR
• Qualified E-Prescribing System Available, but noPrescription(s) were Generated During the Encounter– G8445: No prescriptions were generated during the encounter.
Provider does have access to a qualified e-prescribing systemOR
• E-Prescribing System Available, but not Used for One or More Prescriptions Due to Patient/System Reasons
– G8446: Provider does have access to a qualified e-prescribing system. Some or all prescriptions generated during the encounter were printed or phoned in as required by state or federal law or regulations, patient request, or pharmacy system being unable to receive electronic transmission; OR because they were for narcotics or other controlled substances
Understanding G8446
• Only allowable exceptions are delineated in
code descriptor:
– Controlled substance
– State, federal law
– Patient asks for hard copy
– Pharmacy cannot receive eRx
• Even if the clinician is not sure if the Medicare
service(s) billed for eligible denominator codes will
exceed 10% of Medicare allowed revenues, each
clinician should report the e-prescribing codes.
What is Not E-Prescribing
• Calling in a prescription
• Patient seen in ED is sent home with a written prescription
• Physician-generated faxed prescription to receiving pharmacy fax
• Sending a prescription via PDA (exception: depends on software used – must meet e-prescribing system qualifications)
• Knowingly sending a computer-generated fax initiated at the doctor’s office to a pharmacy (exception: if sent via qualified e-prescribing system and pharmacy system generates message as a fax, it is e-prescribing)
• Office visits during a global surgical period that result in a prescription
• Medicare Advantage patients (exception: some private fee-for-service plans can e-prescribe, but this does not count toward incentive payment calculation)
How eRx works
• An eligible professional decides to order a
prescription for a patient.
• The prescription is entered into an eRx
program and is transmitted to the desired
pharmacy.
• Communication also occurs between the
pharmacy benefit manager and the
physician.
eRx Communication
Professional
PharmacyPBM
SureScripts-RxHub
• This is the network where the prescription communication or messaging travels (between the 3 entities involved in eRx’ing i.e. the professional, pharmacy and PBM)
• Approximately 90% of U.S. prescriptions use the SureScripts-RxHub network
• eRx vendors using the SureScripts-RxHub network must be certified by SureScripts-RxHub
Selection of a System
• After you have checked on the part D
standards, a professional should ask the
eRx vendor if their system meets the
functionality requirements listed in our
measure?
• Ask to see each function demonstrated.
CCHIT
• CCHIT currently certifies EHRs which contain eRx
modules
– These systems meet the functionality requirements of the
measure if they have 2008 certification
• Some of the CCHIT certified programs may the
eRx component available for purchase separately
• Some products are designated ―partners‖ of
CCHIT certified EHRs
• CCHIT expects to review stand-alone systems for
certification in 2009
Part D Standards
• As part of SureScripts-RxHub’s vetting process, all vendors who are listed on the SureScripts website: http://www.surescripts.com/get-connected.aspx?ptype=physician meet the 2009 Part D standards for the functions they provide.
• If an eRx system is not on the SureScripts network, a potential customer should look at the Part D standards on the CMS website and check with the product’s vendor.
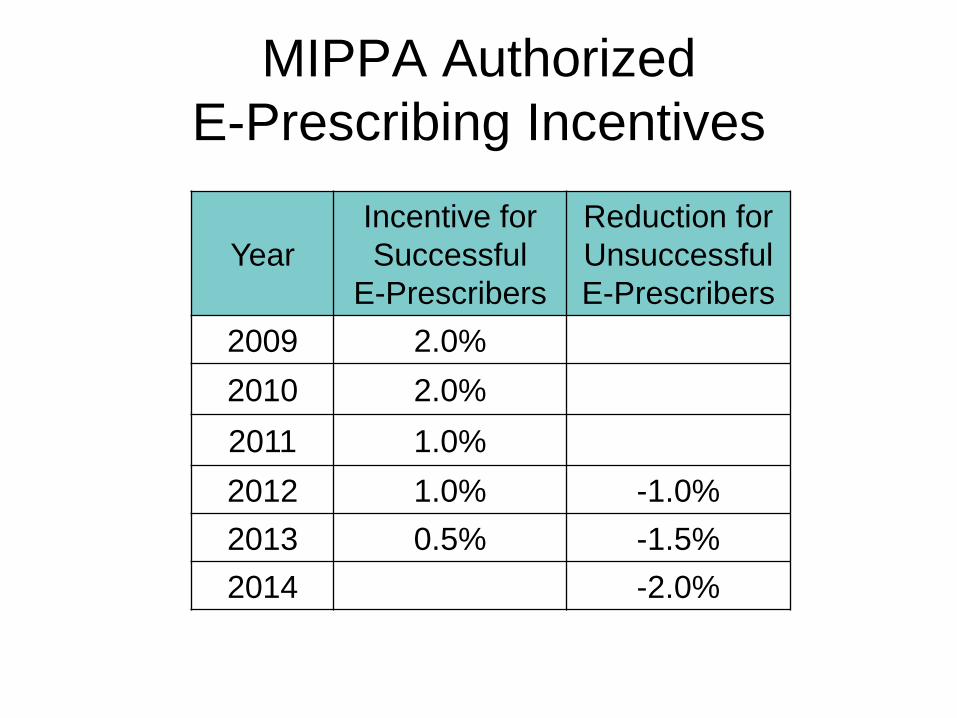
MIPPA Authorized
E-Prescribing Incentives
Year
Incentive for
Successful
E-Prescribers
Reduction for
Unsuccessful
E-Prescribers
2009 2.0%
2010 2.0%
2011 1.0%
2012 1.0% -1.0%
2013 0.5% -1.5%
2014 -2.0%
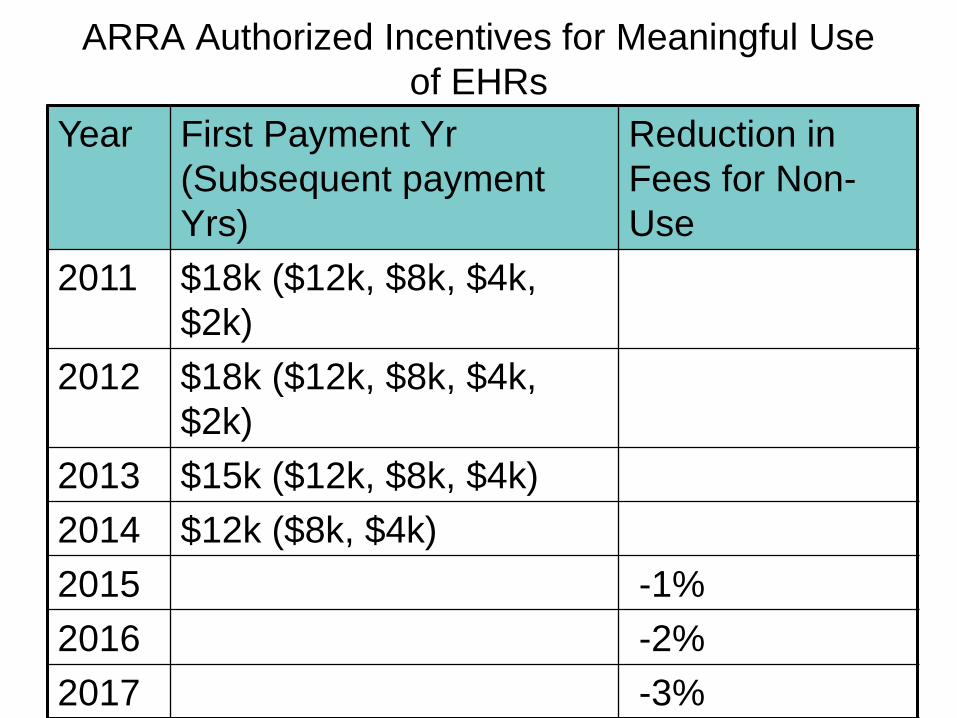
ARRA Authorized Incentives for Meaningful Use
of EHRs
Year First Payment Yr
(Subsequent payment
Yrs)
Reduction in
Fees for Non-
Use
2011 $18k ($12k, $8k, $4k,
$2k)
2012 $18k ($12k, $8k, $4k,
$2k)
2013 $15k ($12k, $8k, $4k)
2014 $12k ($8k, $4k)
2015 -1%
2016 -2%
2017 -3%
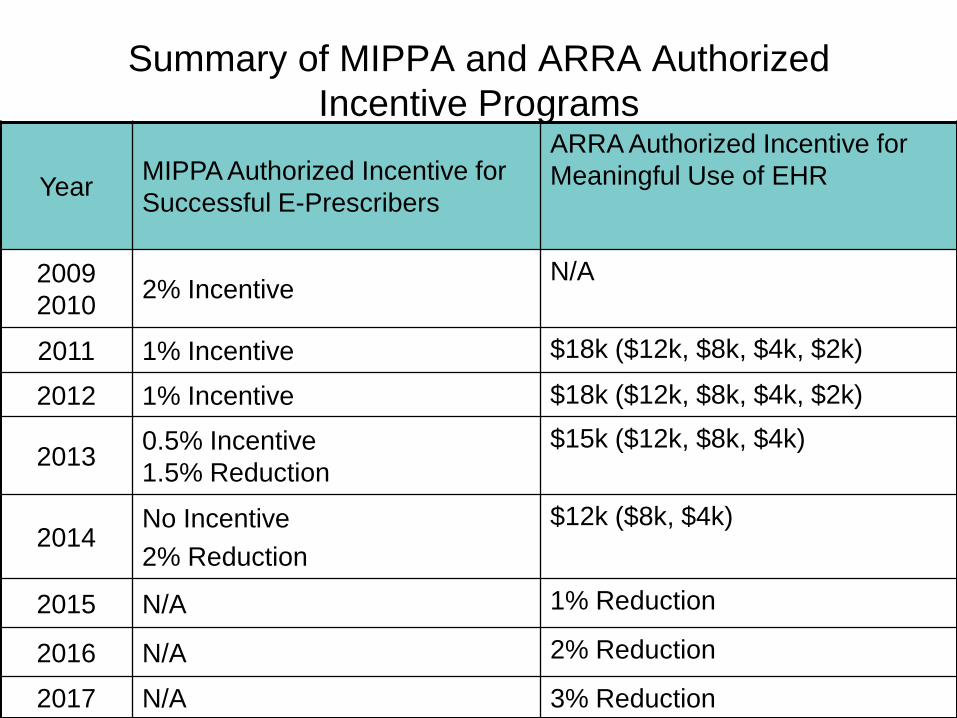
Summary of MIPPA and ARRA Authorized
Incentive Programs
YearMIPPA Authorized Incentive for
Successful E-Prescribers
ARRA Authorized Incentive for
Meaningful Use of EHR
2009
20102% Incentive
N/A
2011 1% Incentive $18k ($12k, $8k, $4k, $2k)
2012 1% Incentive $18k ($12k, $8k, $4k, $2k)
20130.5% Incentive
1.5% Reduction
$15k ($12k, $8k, $4k)
2014No Incentive
2% Reduction
$12k ($8k, $4k)
2015 N/A 1% Reduction
2016 N/A 2% Reduction
2017 N/A 3% Reduction
Demonstration Projects
• CMS currently pays for quality through a series of Demonstration Projects
• Several Demonstrations are mandated through Congressional Legislation
• Must be budget neutral
VBP Demonstrations and
Pilots
• Physician Group Practice Demonstration
• Medicare Care Management Performance
Demonstration
• Medicare Medical Home Demonstration
• Medicare Healthcare Quality
• Gainsharing Demonstrations
• Accountable Care Episode (ACE)
Demonstration

Demonstration Purpose
• Test the development and implementation
of Medicare policy changes prior to
legislation enacting such changes on a
national basis
– Whether it works…
– What refinements…
• Generally look at payment, new benefit,
new organization of care delivery
Acute Care Episode (ACE)
Demonstration
Problems with Current System
• Increased number of services not
necessarily correlated with better care
• Conflicting provider incentives
– Hospitals paid per discharge
– Physicians paid per service
Global Payment
• Fee-for-service
• Part A and Part B
• Services related to acute care
episode only
• Cardiovascular and/or orthopedic
procedures
Sites Selected
• Hillcrest Medical Center – Tulsa
• Baptist Health System – San Antonio
• Oklahoma Heart Hospital – Oklahoma City
• Lovelace Health System – Albuquerque
• Exempla Saint Joseph Hospital – Denver
• Two are cardiovascular only
• One is orthopedic only
• Two are both cardiovascular and orthopedic
Determination of Payment Rates
• Based on competitive bids from sites
• Compared to regular average Medicare payments to the hospitals and physicians
• Evaluated based upon the size of the discount
• Subject to annual IPPS updates
Benefits for Providers
• Potentially increased patient volume
– Value-Based Care Center
• Increased coordination leading to
increased efficiency
• Flexibility of managing global payments
• Option to engage in gainsharing
Gainsharing Demonstrations
• Authority
– Deficit Reduction Act (DRA) Section 5007
– Medicare Modernization Act (MMA) Section 646
– In the absence of statutory authority, gainsharing is restricted by law
• Purpose
– To allow hospitals to provide gainsharing payments designed to improve quality and efficiency of care to physicians
• Timing
– 3-year projects
• Target
– Hospitals and physicians
• Compensation
– Hospitals may share savings with physicians

Hospital and Physician
Alignment of Incentives
• Medicare pays hospitals prospectively for bundles
of services using DRGs
• Physicians generally paid per service
• How to align incentives to improve quality and
efficiency?
• Encourage physician-hospital collaboration by
permitting hospitals to share internal savings
Gainsharing Payments
• Incentive system must be uniform across
physicians, can be reviewed and audited.
• Payments must be linked to quality and
efficiency
• Gainsharing must be a transparent
• Must represent share of internal hospital
savings and be tied to quality improvement
• Limited to 25% of physician fees for care of
patients affected by quality improvement
activity
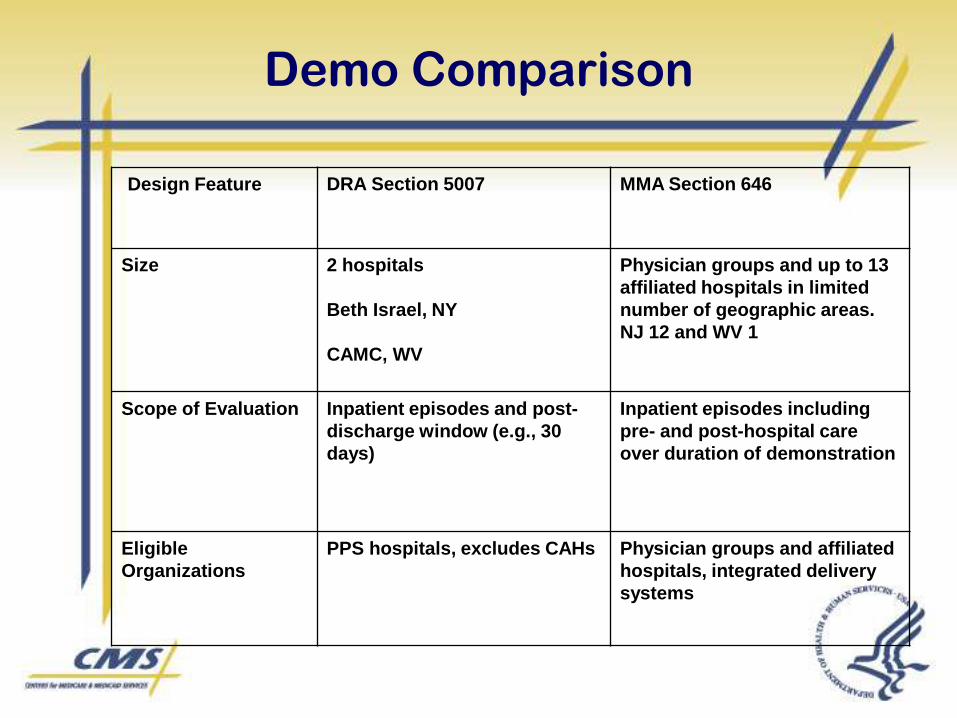
Demo Comparison
Design Feature DRA Section 5007 MMA Section 646
Size 2 hospitals
Beth Israel, NY
CAMC, WV
Physician groups and up to 13
affiliated hospitals in limited
number of geographic areas.
NJ 12 and WV 1
Scope of Evaluation Inpatient episodes and post-
discharge window (e.g., 30
days)
Inpatient episodes including
pre- and post-hospital care
over duration of demonstration
Eligible
Organizations
PPS hospitals, excludes CAHs Physician groups and affiliated
hospitals, integrated delivery
systems
Efficiency in the Quality Context
Efficiency Is One of the Institute of
Medicine's Key Dimensions of Quality
1. Safety
2. Effectiveness
3. Patient-Centeredness
4. Timeliness
5. Efficiency: absence of waste, overuse,
misuse, and errors
6. Equity
• Institute of Medicine: Crossing the Quality Chasm:
A New Health System for the 21st Century, March, 2001.
Physician Resource Use Reports
Pilot
Statutory Authority
Medicare Improvement for Patients and Providers Act of 2008, Section 131(c)
The Secretary shall establish a Physician Feedback Program under which the Secretary shall use claims data (and may use other data) to provide confidential reports to physicians (and, as determined appropriate by the Secretary, to groups of physicians) that measure the resources involved in furnishing care. The Secretary may include information on the quality of care furnished by the physician (or group of physicians) in such reports.

Physician Resource Use Measurement
Goals
Construct resource use measures that are meaningful, actionable, and fair
Provide confidential reports of resource use to individual/groups of physicians
Compare actual use to expected resource use
Link resource use to measures of quality and patient experiences of care
Statutory Authority
MIPPA Section 131(c)
MIPPA Options:
Resource use can be measured on an episode or
per capita basis, or both
Resource use can be measured with claims or
through other data sources
Focus can be on selected physicians by: specialty,
conditions treated, geography, high cost outliers,
minimum # of cases
CMS can make adjustments to resource use
measures to render them comparable across
physicians
Resource use measures can apply to individual
physicians or physician groups
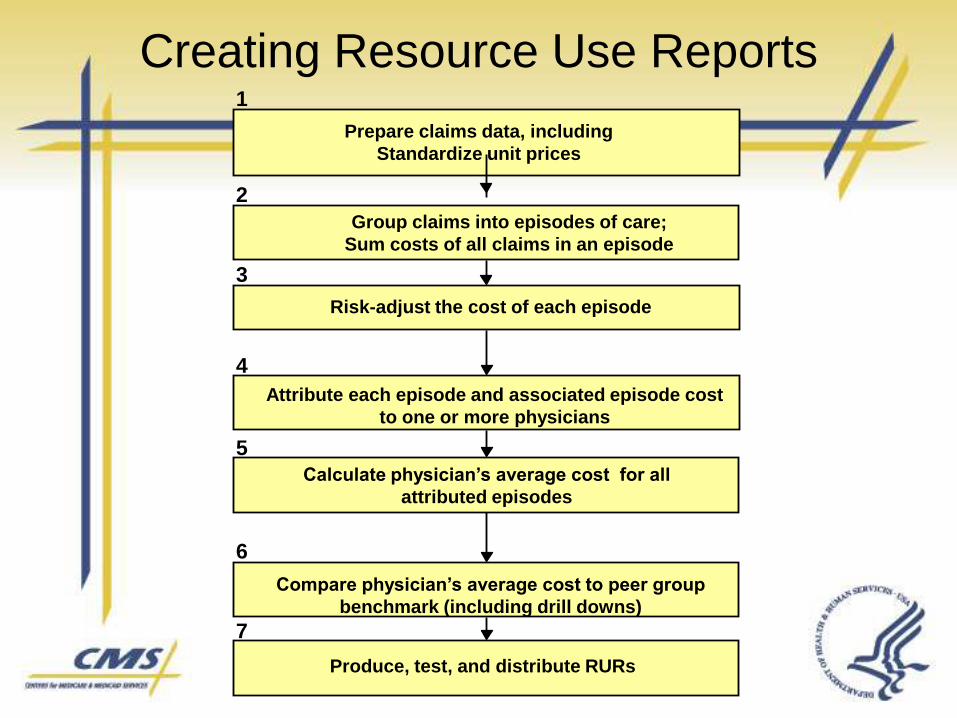
Prepare claims data, including
Standardize unit prices
Group claims into episodes of care;
Sum costs of all claims in an episode
Risk-adjust the cost of each episode
Attribute each episode and associated episode cost
to one or more physicians
Calculate physician’s average cost for all
attributed episodes
Compare physician’s average cost to peer group
benchmark (including drill downs)
Produce, test, and distribute RURs
1
2
3
4
5
6
7
Creating Resource Use Reports
Value-Based Purchasing and
Hospital-Acquired Conditions
• The Hospital-Acquired Conditions provision
is a step toward Medicare VBP for hospitals
• Strong public support for CMS to pay less for
conditions that are acquired during a hospital
stay
• Considerable national press coverage of
HAC has prompted dialogue of how to
further eliminate healthcare-associated
infections and conditions
Statutory Authority:
DRA Section 5001(c)
Beginning October 1, 2007, hospitals were required to submit data on their claims for payment indicating whether diagnoses were present on admission (POA)
Beginning October 1, 2008, CMS cannot assign a case to a higher DRG based on the occurrence of one of the selected conditions, if that condition was acquired during the hospitalization
This provision does not apply to Critical Access Hospitals, Rehabilitation Hospitals, Psychiatric Hospitals, or any other facility not paid under the Medicare Hospital IPPS
Statutory Selection Criteria
CMS must select conditions that
are
1. High cost, high volume, or both
2. Assigned to a higher paying
DRG when present as a
secondary diagnosis
3. Reasonably preventable
through the application of
evidence-based guidelines
Present on Admission
Present on admission (POA) is defined as present at the time the order for inpatient admission occurs– Conditions that develop during an outpatient encounter,
including emergency department, observation, or outpatient surgery, are considered POA
POA indicator is assigned to – Principal diagnosis
– Secondary diagnoses
– External cause of injury codes (Medicare requires reporting only if E-code is reported as an additional diagnosis)

POA Indicator Reporting Options
Code Reason for Code
Y Diagnosis was present at time of inpatient admission.
N Diagnosis was not present at time of inpatient admission.
U Documentation insufficient to determine if condition was
present at the time of inpatient admission.
W Clinically undetermined. Provider unable to clinically
determine whether the condition was present at the time
of inpatient admission.
1 Unreported/Not used. Exempt from POA reporting. This code
is equivalent code of a blank on the UB-04; however, it was
determined that blanks are undesirable when submitting this
data via the 4010A.
― A joint effort between the healthcare
provider and the coder is essential to
achieve complete and accurate
documentation, code assignment, and
reporting of diagnoses and procedures.‖
Selected HACs for
Implementation
1. Foreign object retained after surgery
2. Air embolism
3. Blood incompatibility
4. Pressure ulcers– Stages III & IV
5. Falls– Fracture
– Dislocation
– Intracranial injury
– Crushing injury
– Burn
– Electric shock
Selected HACs for
Implementation
6. Manifestations of poor glycemic control
– Hypoglycemic coma
– Diabetic ketoacidosis
– Nonketotic hyperosmolar coma
– Secondary diabetes with ketoacidosis
– Secondary diabetes with hyperosmolarity
7. Catheter-associated urinary tract infection
8. Vascular catheter-associated infection
9. Deep vein thrombosis (DVT)/pulmonary embolism
(PE)
– Total knee replacement
– Hip replacement
Selected HACs for
Implementation
10. Surgical site infection
– Mediastinitis after coronary artery bypass graft (CABG)
– Certain orthopedic procedures
• Spine
• Neck
• Shoulder
• Elbow
– Bariatric surgery for obesity
• Laprascopic gastric bypass
• Gastroenterostomy
• Laparoscopic gastric restrictive surgery
Candidate HACs
• Fiscal Year 2009 Inpatient Prospective
Payment System (IPPS) final rule
http://edocket.access.gpo.gov/2008/pdf/E8-
17914.pdf (page 39)
Candidate HACs
1. Surgical site infection following device
procedures
2. Failure to rescue
3. Death or disability associated with drugs,
devices, or biologics
4. Dehydration
5. Malnutrition
Candidate HACs
6. Water-borne pathogens
7. Surgical site infections following
procedures – orthopedic and other
8. Ventilator-associated pneumonia
9. Clostridium difficile-associated disease
Proposed 2010 IPPS Rule
http://federalregister.gov/OFRUpload/OFR
Data/2009-10458_PI.pdf
Guidelines for Preventing HACs
• Where are guidelines developed– Professional organizations, Task Forces,
Government agencies, academic institutions
• What are they– Recommendations for interventions based
scientific evidence or expert opinion
• Who develops and uses them– Scientists, clinicians
– Policy makers, consumers
Future Considerations
• Risk adjustment– Individual and population level
• Rates of HACs for VBP– Appropriate for some HACs
• Uses of POA information– Public reporting
• Adoption of ICD-10– Example: 125 codes capturing size, depth, and location of
pressure ulcer
• Expansion of the IPPS HAC payment provision to other settings– Discussion in the IRF, OPPS/ASC, SNF, LTCH
regulations
Never Events
• Wrong surgery performed on a patient
• Surgery performed on wrong body part
• Surgery performed on the wrong patient
http://www.cms.hhs.gov/mcd/viewdecisionmemo.asp?id=223
Resources Available
Physician Quality Reporting Initiative:https://www.cms.hhs.gov/pqri
CMS Quality Initiatives – General Information:http://www.cms.hhs.gov/QualityInitiativesGenInfo/
12/9/08 Issues Paper: Development of a Plan to Transition to a Medicare Value-Based Purchasing Program for Physician and Other Professional Services
http://www.cms.hhs.gov/center/physician.asp
Hospital Quality Reporting:www.hospitalcompare.hhs.gov
Demonstrations:http://www.cms.hhs.gov/DemoProjectsEvalRpts/
Resources
• E-Prescribing Incentive Program Website:
http://www.cms.hhs.gov/PQRI/03_EPrescribingIncentiveProgram.asp#TopOfPage
• Medicare’s Practical Guide to the E-Prescribing Incentive Program:
http://www.cms.hhs.gov/partnerships/downloads/11399.pdf
• E-Prescribing General Information:
http://www.cms.hhs.gov/eprescribing/
• SureScripts’ E-Rx Hub includes list of vendors who meet E-Prescribing qualifications:
http://www.surescripts.com/get-connected.aspx?ptype=physician
• Clinician’s Guide to Electronic Prescribing– http://ehealthinitiative.org/eRx/clinicians.mspx
• National E-prescribing Conference CME– http://www.massmed.org >e-prescribing CME information