claudio moretti, md – university of turin, turin, italy – [email protected]
TRANSCRIPT
Claudio Moretti, MD – University of Turin, Turin, Italy – [email protected]

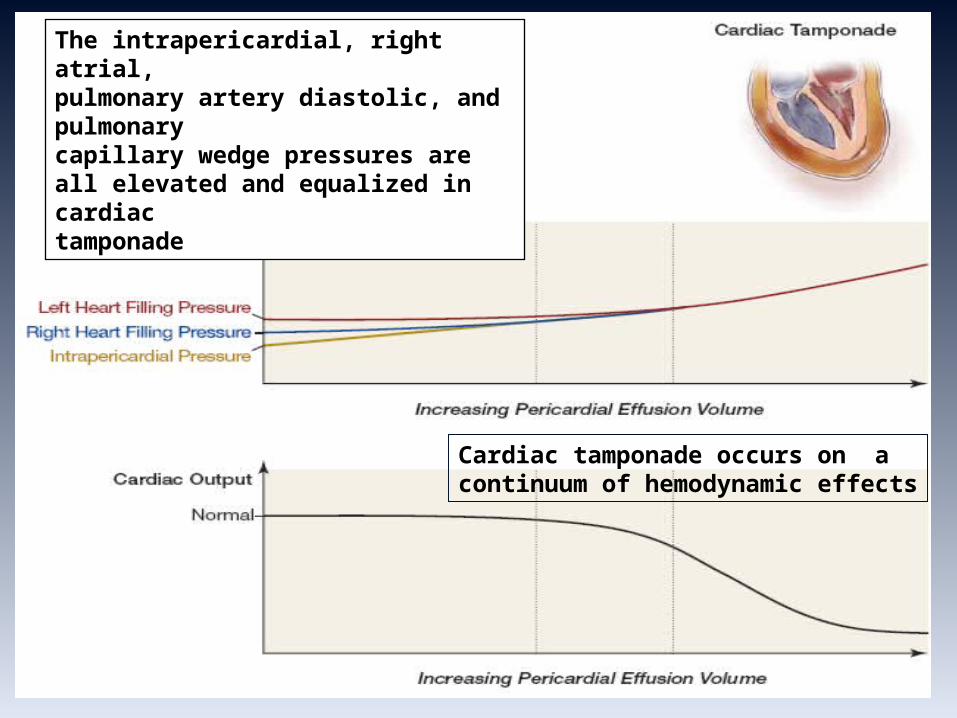
The intrapericardial, right atrial,pulmonary artery diastolic, and pulmonarycapillary wedge pressures areall elevated and equalized in cardiactamponade
Cardiac tamponade occurs on a continuum of hemodynamic effects
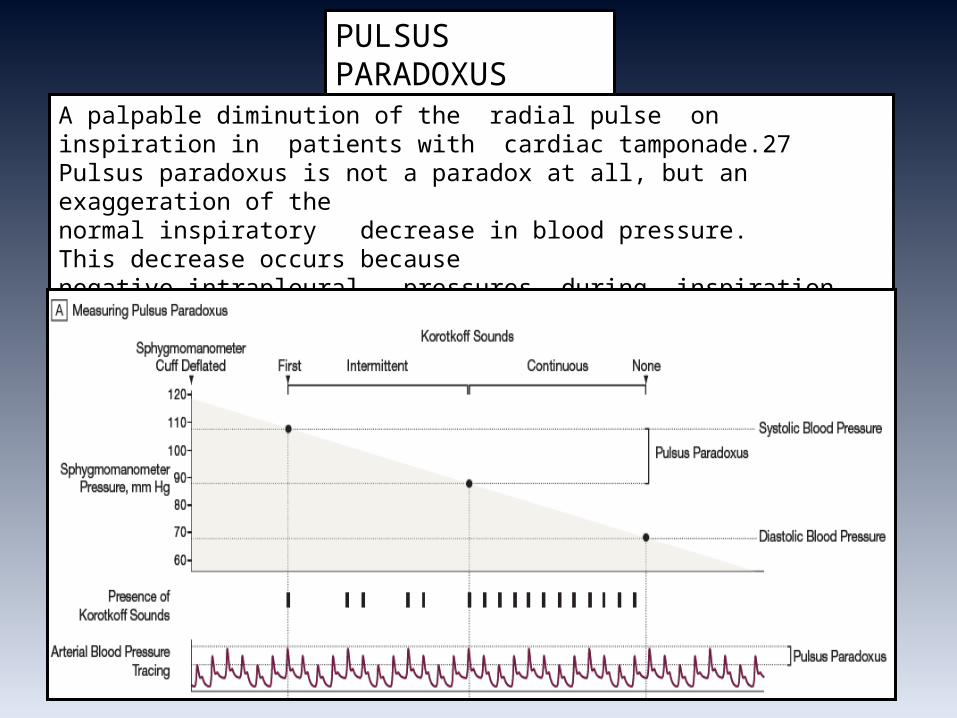
PULSUS PARADOXUS
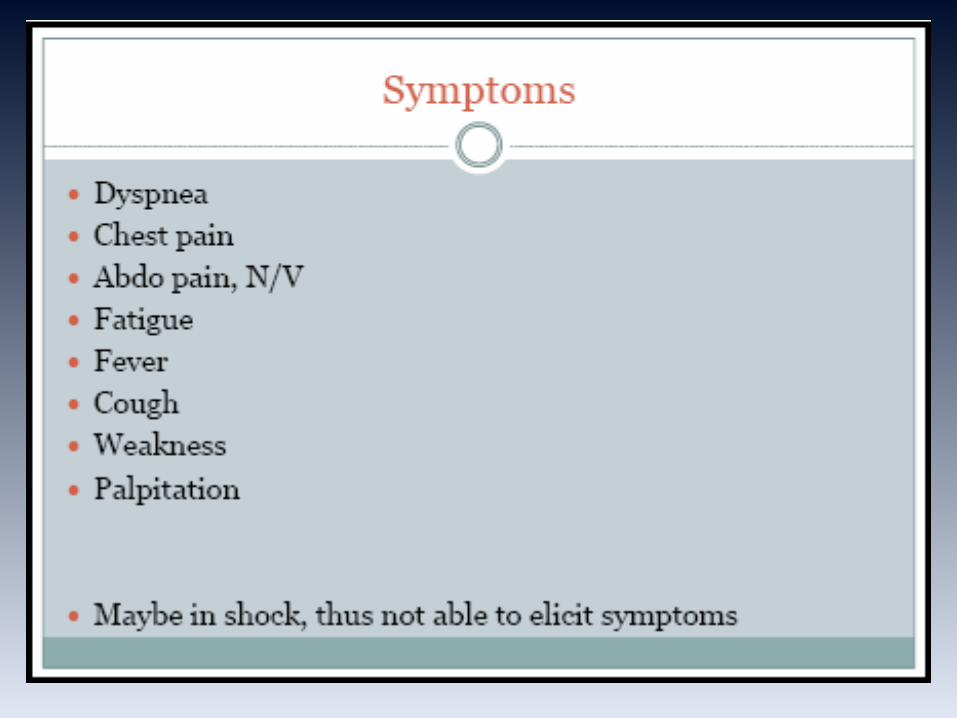
A palpable diminution of the radial pulse on inspiration in patients with cardiac tamponade.27 Pulsus paradoxus is not a paradox at all, but an exaggeration of thenormal inspiratory decrease in blood pressure. This decrease occurs becausenegative intrapleural pressures during inspiration cause increased venous return and filling of the right heart, which result in bowing of the septum to the left, decreasing filling of the left heart.

“Best” and worst case scenario…
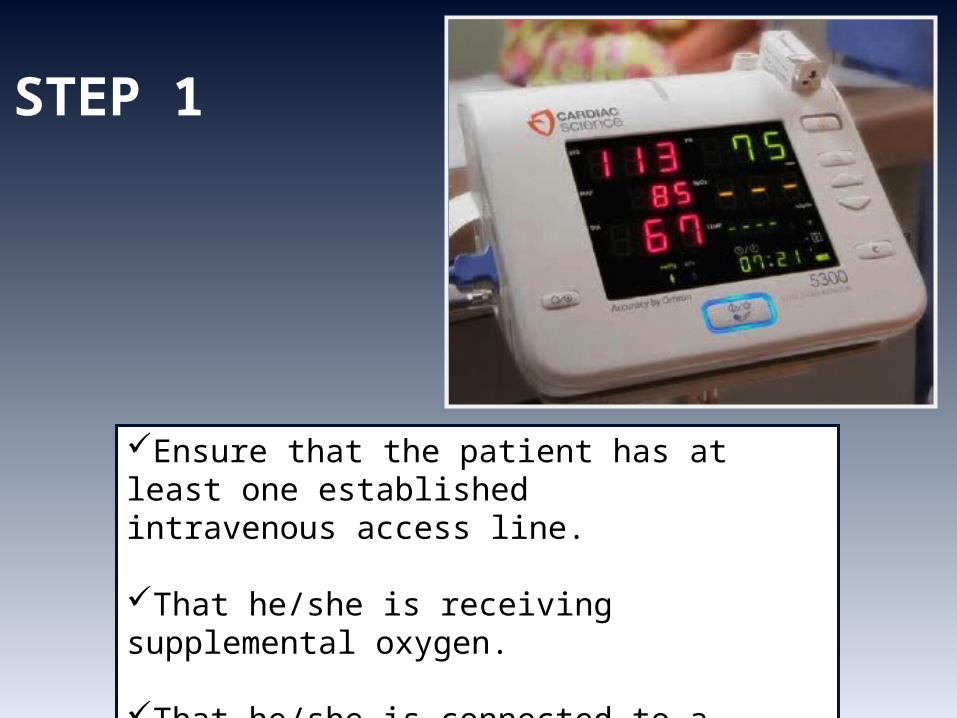
Ensure that the patient has at least one established intravenous access line.
That he/she is receiving supplemental oxygen.
That he/she is connected to a cardiac monitor and continuous pulse oximetry.
STEP 1
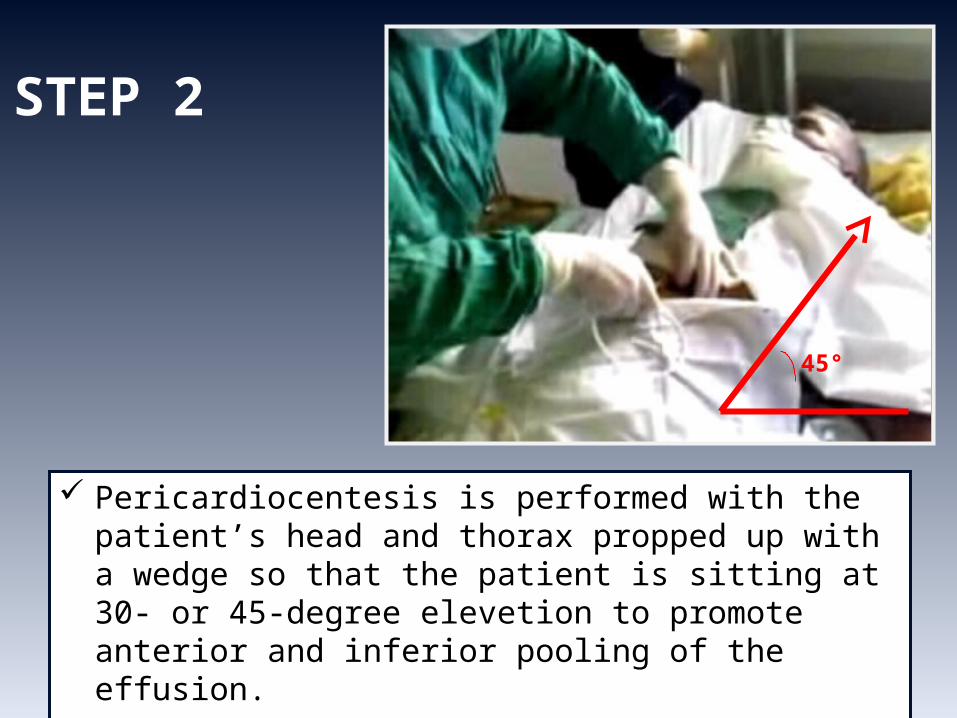
STEP 2
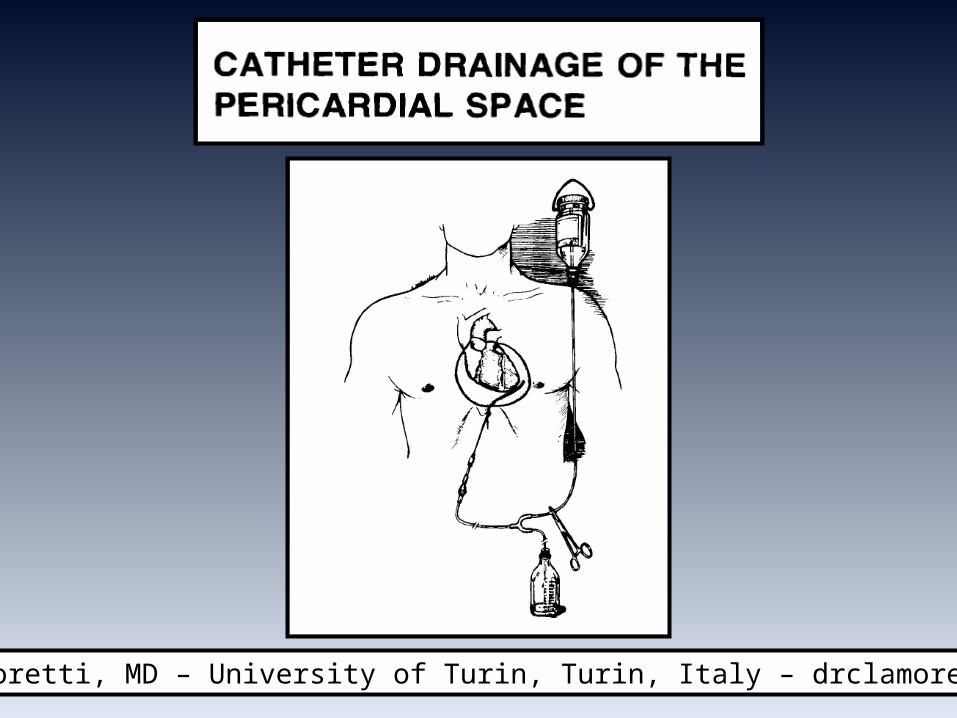
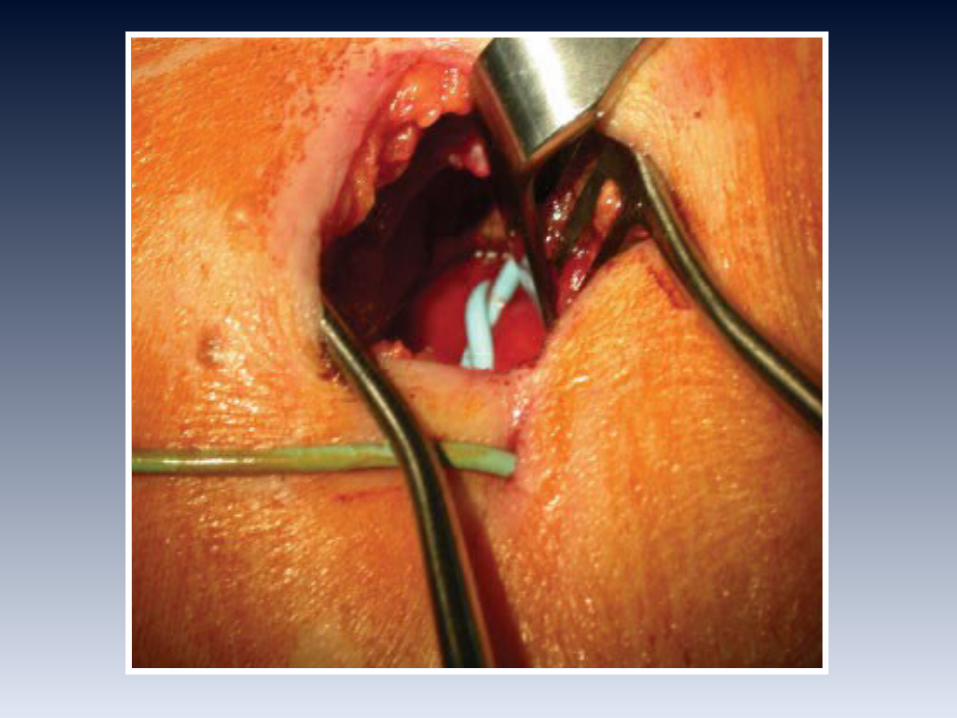
Pericardiocentesis is performed with the patient’s head and thorax propped up with a wedge so that the patient is sitting at 30- or 45-degree elevetion to promote anterior and inferior pooling of the effusion.
45°
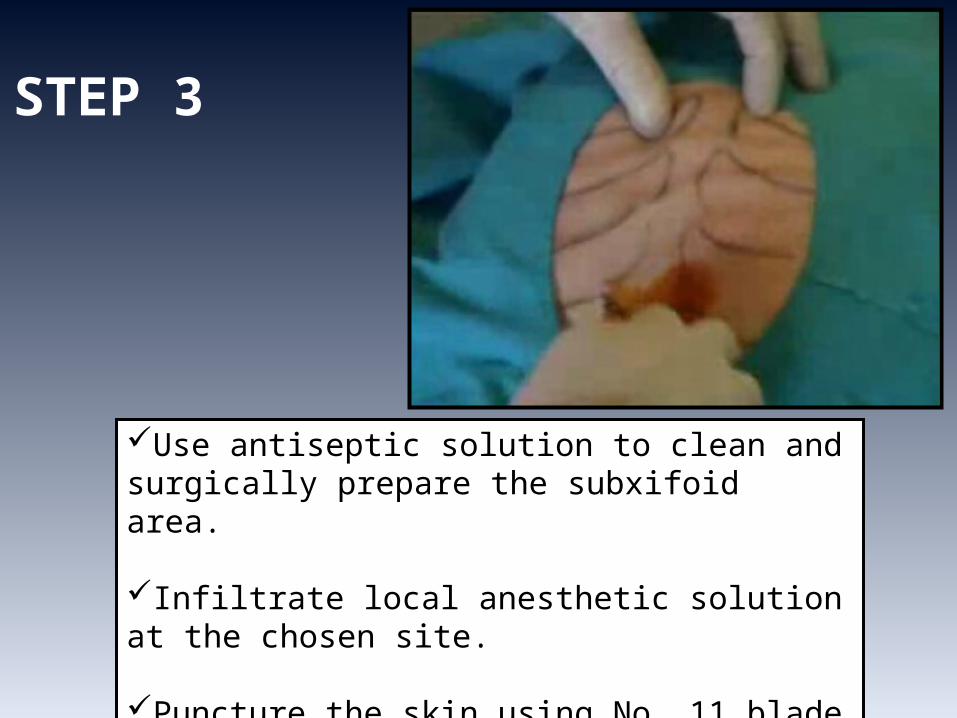
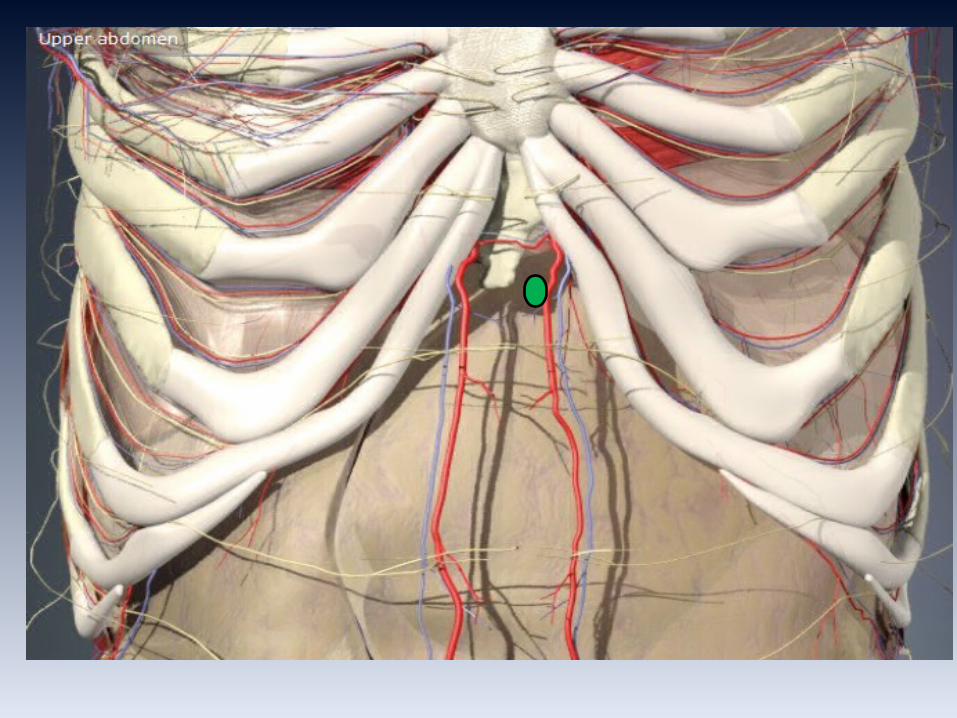
Use antiseptic solution to clean and surgically prepare the subxifoid area.
Infiltrate local anesthetic solution at the chosen site.
Puncture the skin using No. 11 blade scalpel at the chosen site (between the xiphoid)
STEP 3
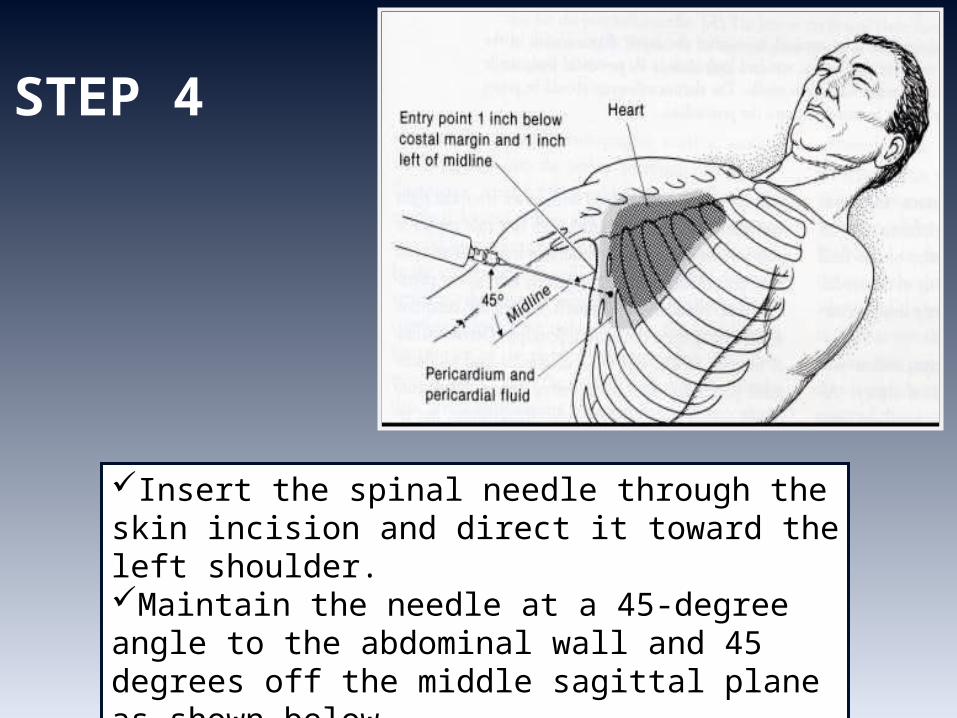
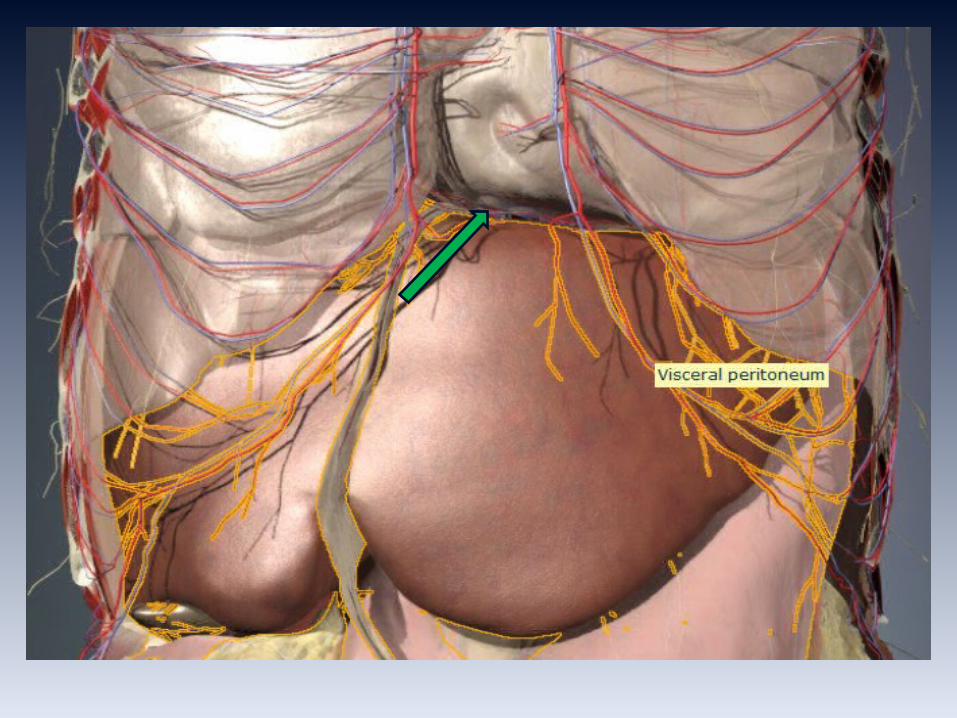
Insert the spinal needle through the skin incision and direct it toward the left shoulder.Maintain the needle at a 45-degree angle to the abdominal wall and 45 degrees off the middle sagittal plane as shown below.
STEP 4
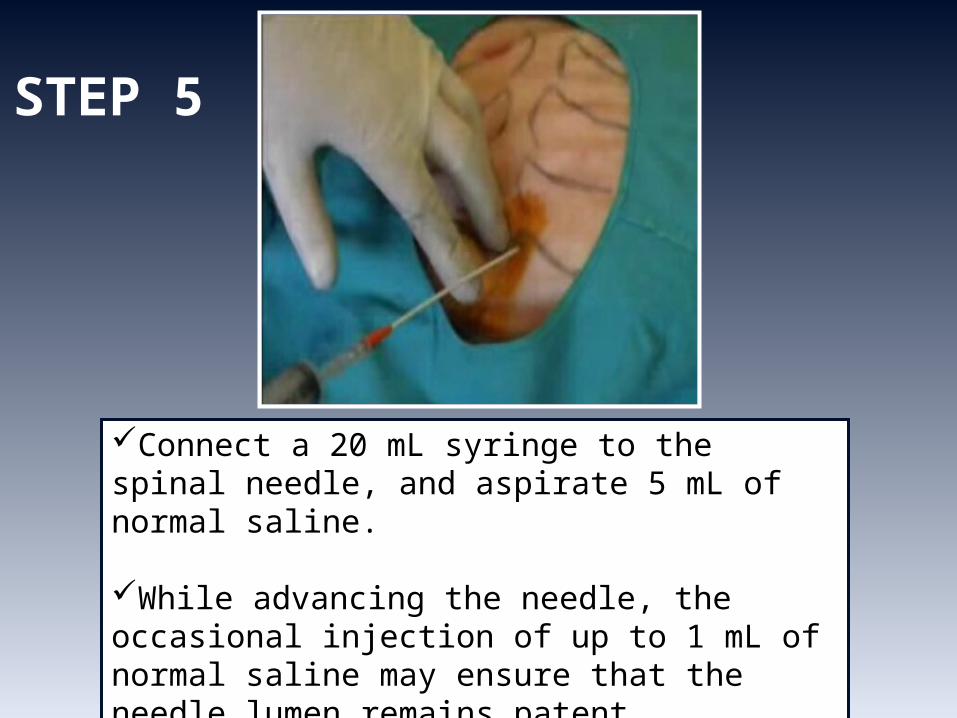
Connect a 20 mL syringe to the spinal needle, and aspirate 5 mL of normal saline.
While advancing the needle, the occasional injection of up to 1 mL of normal saline may ensure that the needle lumen remains patent.
STEP 5

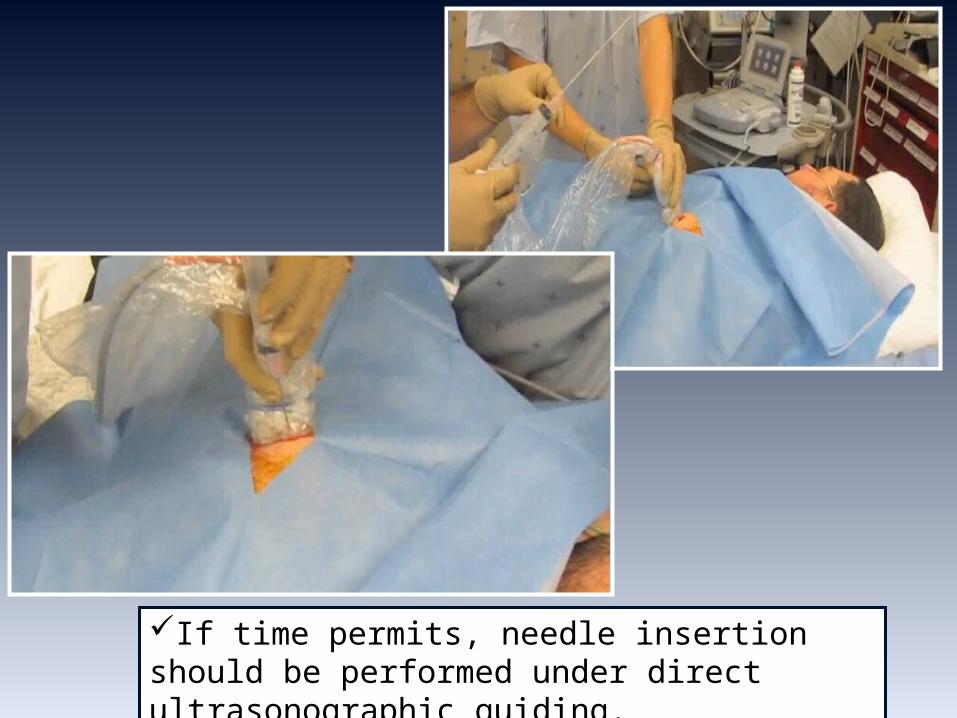
If time permits, needle insertion should be performed under direct ultrasonographic guiding.
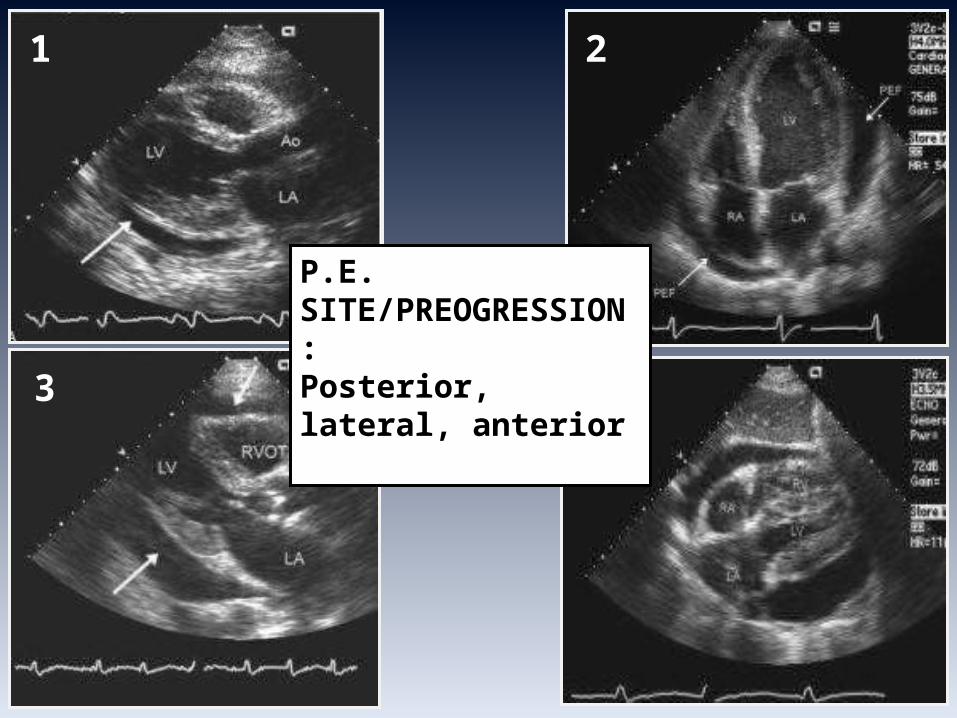
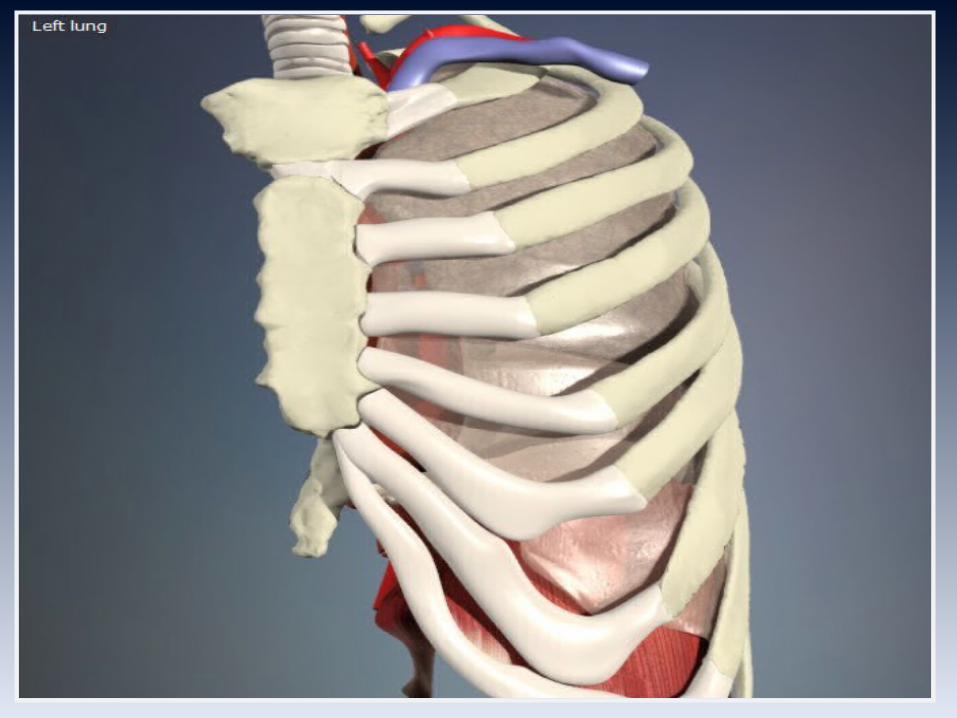
P.E. SITE/PREOGRESSION:Posterior, lateral, anterior
1 2
3 4
Claude Schaeffer Beck (1894-1971)Claude Schaeffer Beck (1894-1971)He graduated from Franklin & Marshall College (Lancaster, Pa.) in 1916, receiving his M.D. from Johns Hopkins University in 1921 and worked under Dr Harvey Cushing at Harvard in 1923-1924. The first american professor of cardiovascular surgery.
He assisted Dr. Elliott Cuttlerin in the first mitral valve operations in the 1920s.
He performed the first successful defibrillation of the human heart in 1947.
He was the first to remove a heart tumor.
Beck and his colleagues developed cardiopulmonary resuscitation techniques. They began teaching medical professionals in 1950, training more than 3,000 doctors and nurses in less than 20 years.
He performed the first "Beck I" operation (cardiopericardiopexy) in 1935.
The Beck II operation came about in the late 1940s, which created a vein graft between the aorta and coronary sinus.
Beck is also credited with describing the physiological basis for the signs of acute cardiac tamponade. The medical signs classically associated with acute cardiac tamponade are collectively called
Beck's triad
For these and further slides on these topics please feel free to visit the
metcardio.org website:
http://www.metcardio.org/slides.html