chronic kidney injury
TRANSCRIPT

CHRONIC KIDNEY DISEASE
• CKI is a progressive, irreversible kidney injury and kidney function doesnot recover.
• When kidney function is too poor to sustain life, CKD becomes End Stage Kidney Disease (ESKD/ ESRD)
• Progressive, irreversible deterioration in renal function in which the body’s ability to maintain metabolic and fluid and electrolyte balance fails resulting in Uremia or Azotemia
INCIDENCE• The incidence of end stage renal disease in
men (239/million) is much greater than in women (162/million). It is much higher in African-Americans (595/million) than Asians (205/million) or Caucasians (150/million).
• More in men than women
• More seen at 65 years of age and older.

ETIOLOGY AND RISK FACTORS
•MORPHOLOGIC•ETIOLOGIC

MORPHOLOGICa) Glomerular disease
Glomerulonephritis Basement membrane disease Goodpasture’s disease
b) Tubular disease Chronic hypercalcemia Chronic potassium depletion Heavy metal poisoining
c) Vascular disease of the KidneyIschemic disease of the KidneyBilateral renal artery stenosisNephrosclerosisHyperparathyroidism
d) Urinary Tract DiseaseObstructive uropathy
e) Inherited or Genetic conditionsHypoplastic kidneyPolycystic & Medullary cystic KidneyDiabetic NephropathySarcoidosis (inflammation of multiple organ; liver
failure, heart failure)
ETIOLOGICa) Infection
Pyelonephritis TB
b) Systemic Vascular Disease Intrarenal renovascular hypertension Extrarenal renovascular hypertension
c) Metabolic Renal Disease Amyloidosis Gout Diabetic Nephropathy
d) Connective tissue diseaseProgressive systemic sclerosis ( a systemic
connective tissue disease leading to collagen accumulation in the kidney)
SLEPolyarteritis (vasculitis: arteries damaged or
swollen)
CLASSIFICATION OF C K D
Stage 1Stage 2Stage 3Stage 4Stage 5
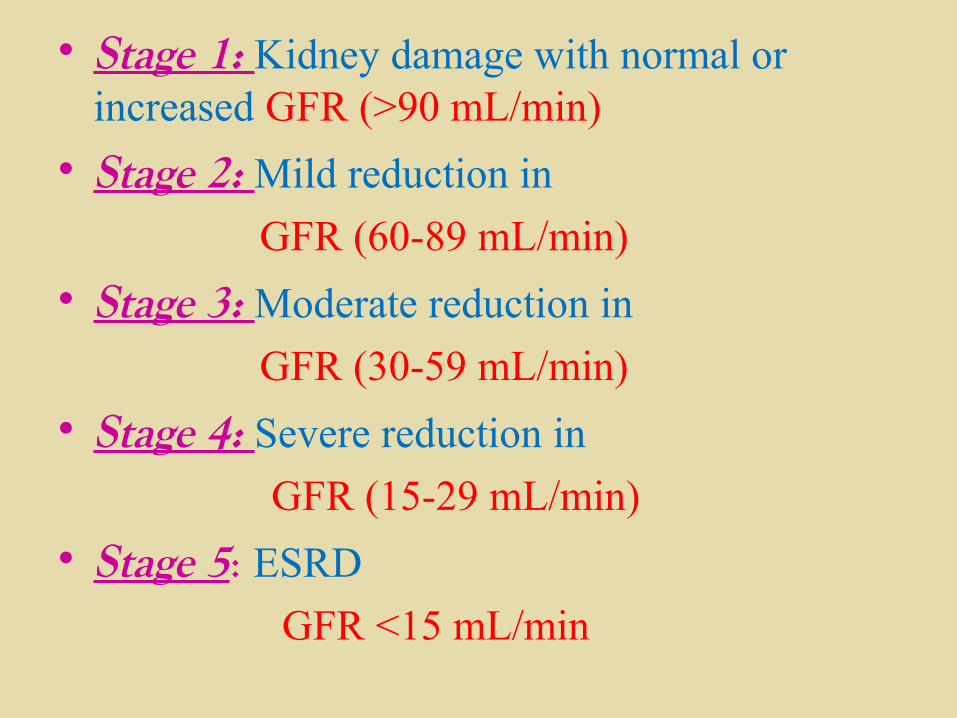
• Stage 1: Kidney damage with normal or increased GFR (>90 mL/min)
• Stage 2: Mild reduction in
GFR (60-89 mL/min)
• Stage 3: Moderate reduction in
GFR (30-59 mL/min)
• Stage 4: Severe reduction in
GFR (15-29 mL/min)
• Stage 5: ESRD
GFR <15 mL/min
PATHOPHYSIOLOGYTissue injury
Decline in renal function
accumulation of end products of protein metabolism
Uremia
CONSEQUENCES OF DECRESED RENAL
FUNCTION• Retension of Na and water-edema, CHF,
hypertension, ascites.• Decreased GFR- stimulation of renin
angiotensin axis and increased aldosterone secretion –increased BP
• Kidneys inability to excrete hydrogen ions , produce ammonia and conserve bicarbonates-metabolic acidosis
• Decreased GFR –increased P-decrease in serum calcium-bone reabsorption of calcium
CONSEQUENCES CONT….
• Erythropoetin production by kidney decreases-anemia
• Uremia affects CNS –altered mental function ,personality changes, seizures and coma
CLINICAL MANIFESTATIONS
• GIanorexia, nausea, vomiting, hiccups, ulcer,
hemorrhage, metallic taste in mouth, constipation, stomatitis, diarrhea.
• CVSECG changes, hypertension, pericarditis,
pericardial tamponade, cardiomyopathy, peripheral edema, heart failure.
• UrinaryAnuria/ oliguria, protenuria, hematuria, diluted
straw like urine
• RESPIRATORYPulmonary edema, pleural effusion , pleural
rub, uremic halitosis, tachypnea, deep sighing, yawning, Kussmaul respiration, uremic pneumonitis, shortness of breath, depressed cough reflex, crackles.
• NEUROLOGIC Fatigue, sleep disorders, head ache,
lethargy, muscular irritability, peripheral neuropathy , seizures, slurred speech, asterixis, tremor, twitching or jerky movements, myoclonus, ataxia, paresthesia.
INTEGUMENTARY
Decrease skin turgor, Yellow- gray pallor, Dry skin, Prurirtis, Echchymosis, Purpura, Soft tissue, calcifications, Uremic frost.
MUSCULOSKELETAL
Muscle weakness, bone pain, pathologic fractures, renal osteodystrophy
REPRODUCTIVE
Decreased fertility, decrease libido, impotence.
• HEMATOLOGIC
Anemia, increased bleeding tendency
• PSYCHOSOCIAL
Personality and behaviour changes, alteration in cognitive processes

DIAGNOSTIC EVALUATION
• Renal function test• ABG• Creatinine clearance test
MEDICAL MANAGEMENT
• Detection and treatment of reversible causes of renal failure
• Dietary regulation
• Correction of anemia, acidosis, hyperkalemia, fluid retention

MAIN MANAGEMENT
RRT (RENAL REPLACEMENT THERAPY)
• DIALYSIS• RENAL TRANSPLANTATION
DIALYSISHEMODIALYSIS
PERITONEAL DIALYSIS
CONCEPTS
• DEFINITION• DIALYSIS MACHINE• PRINCIPLES• DIALYSER• DIALYSATE• VASCULAR ASCESS• COMPLICATIONS

HEMODIALYSIS MACHINE
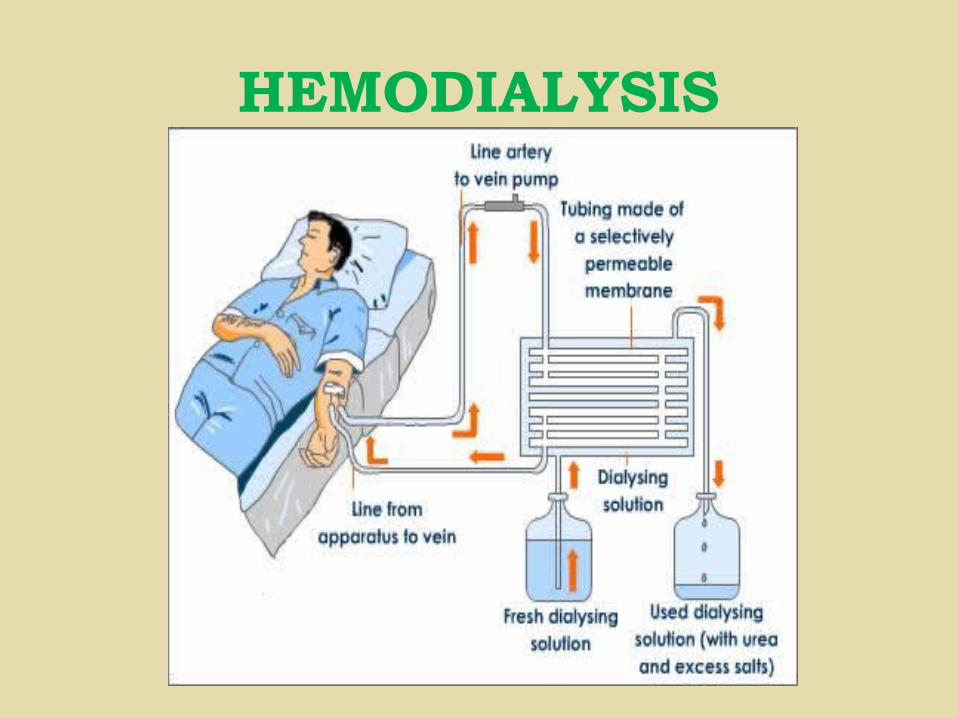
HEMODIALYSIS
DIALYZER

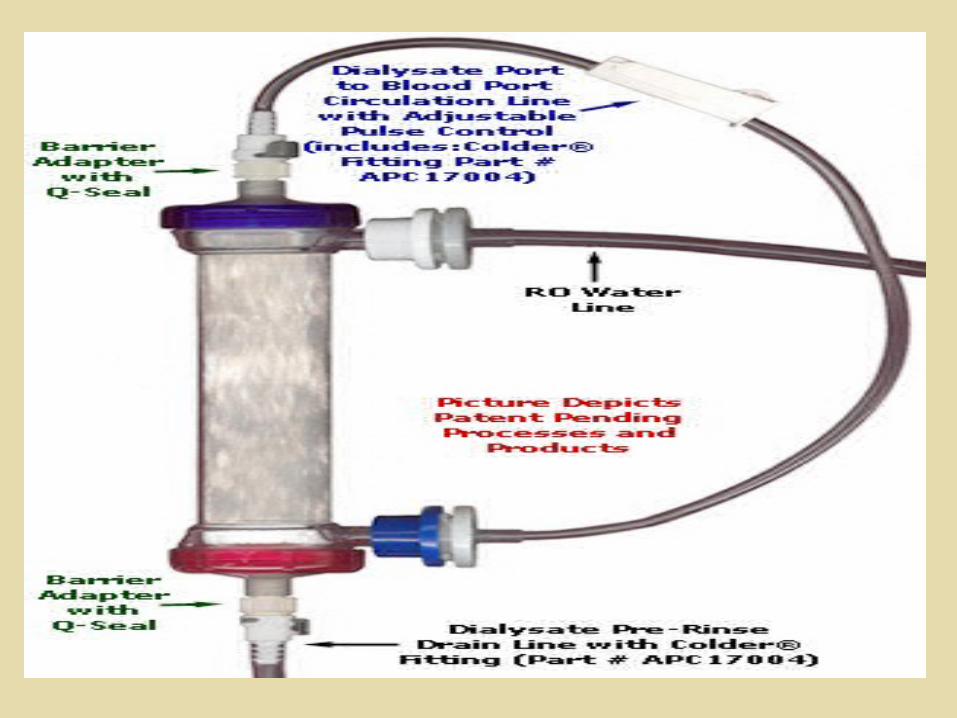
DIALYSATE OR DIALYSIS SOLUTION


VASCULAR ACCESS
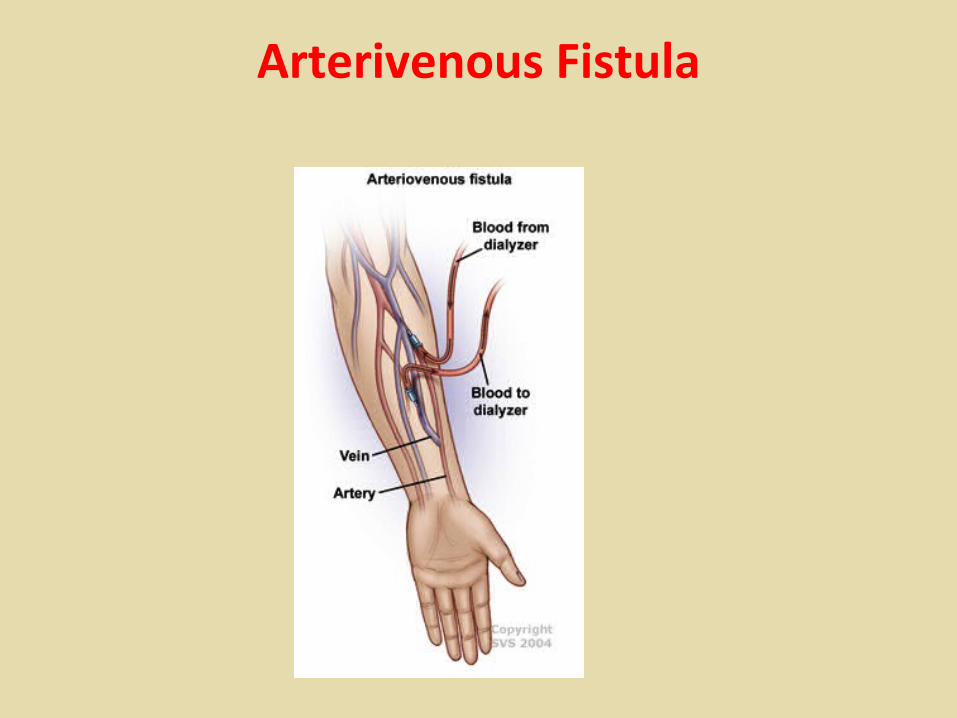
Arterivenous Fistula
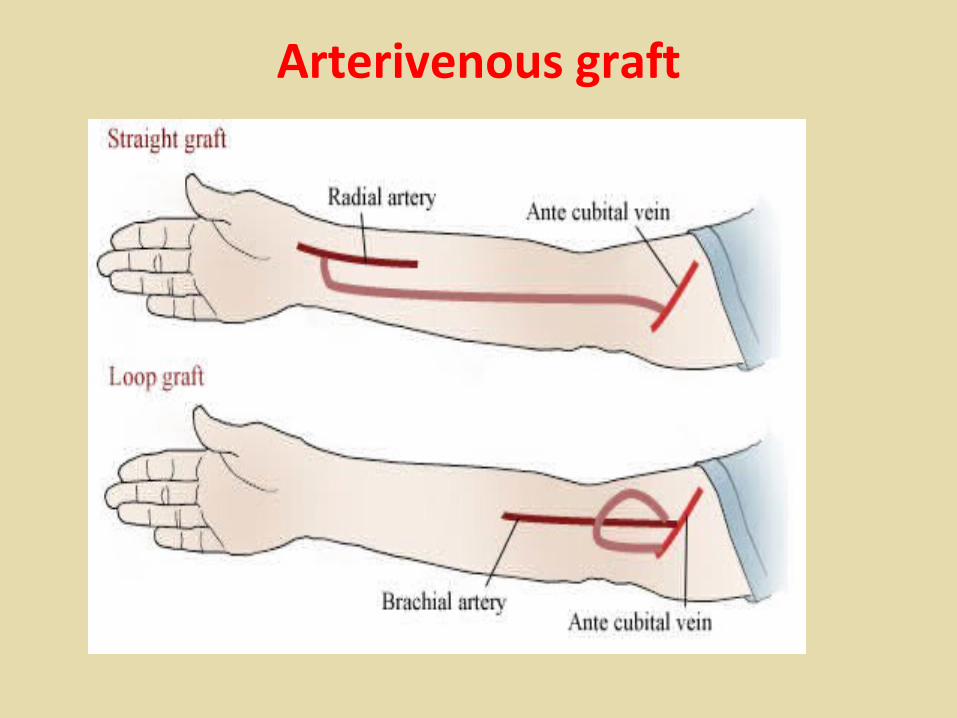
Arterivenous graft
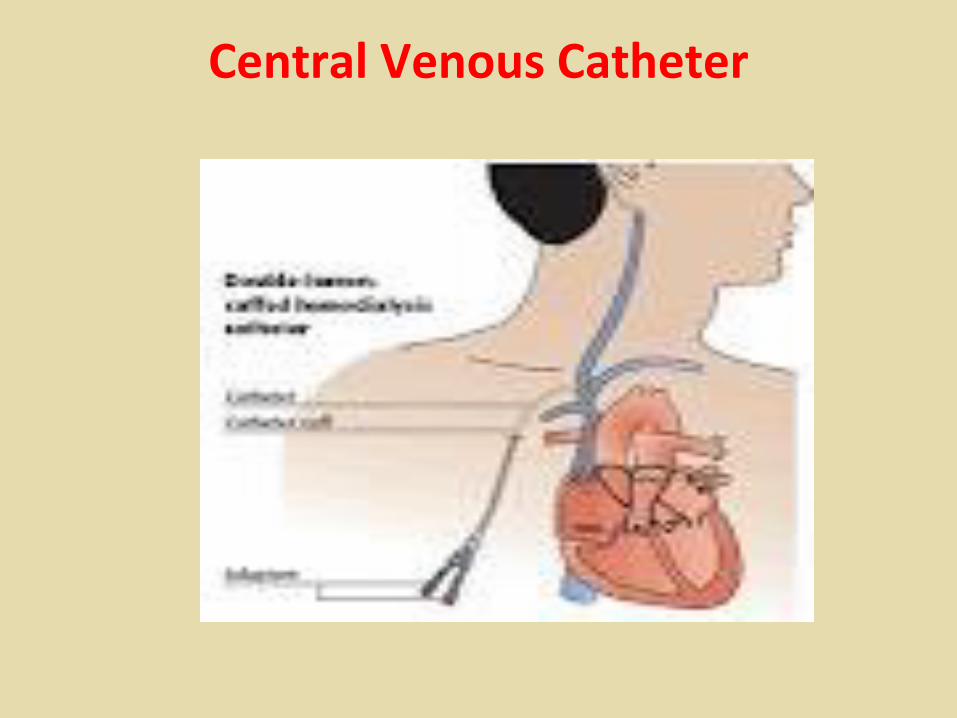
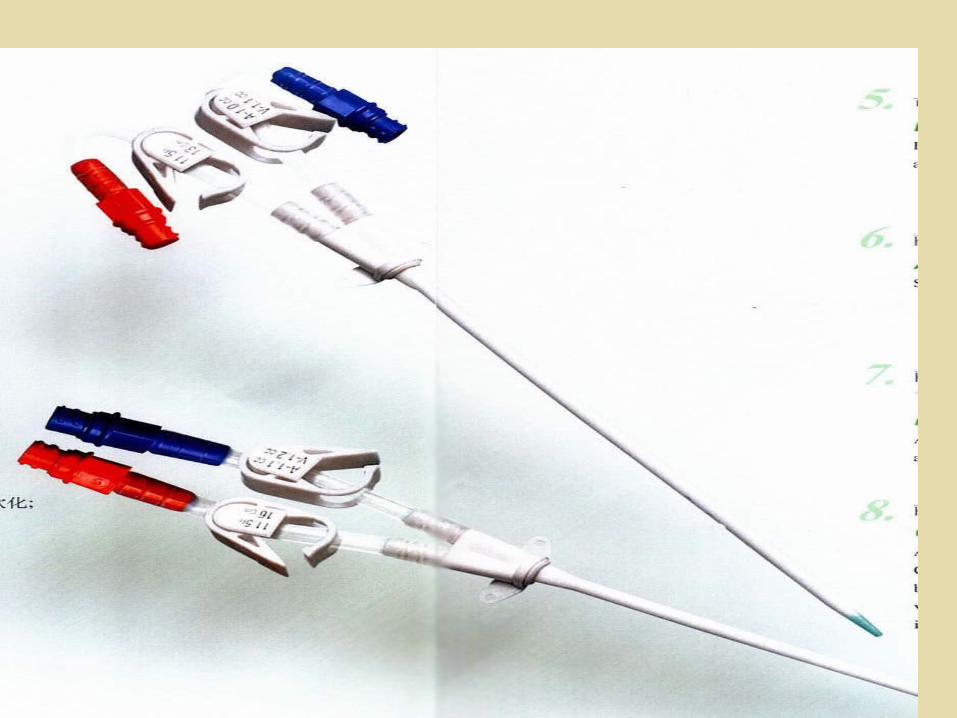
Central Venous Catheter
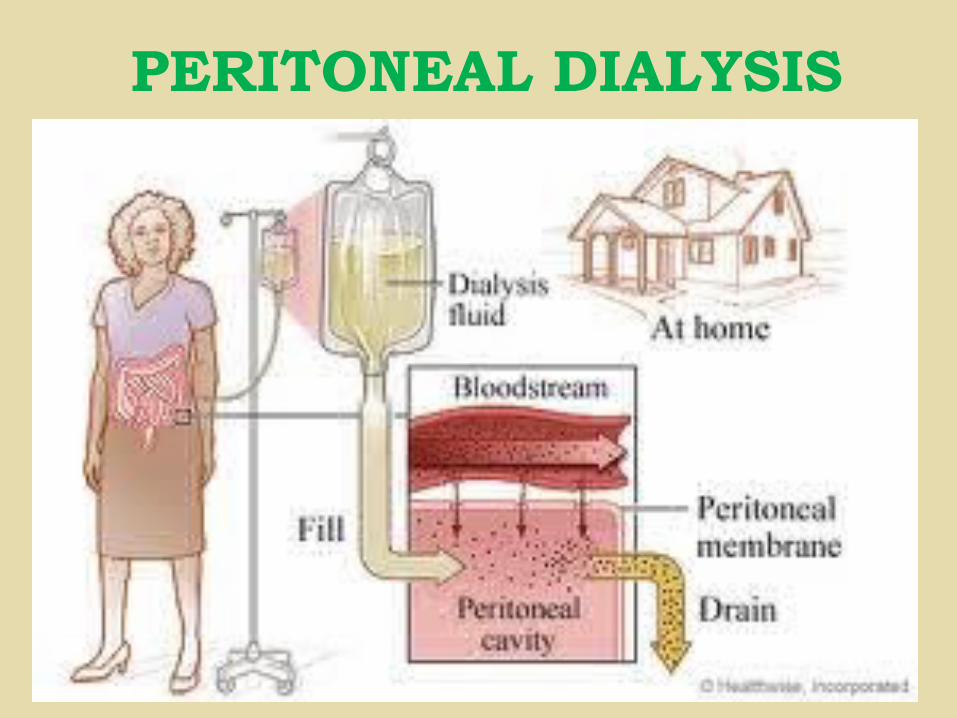
PERITONEAL DIALYSIS
CONCEPTS
• DEFINITION• METHODS/ STEPS• DIALYSATE SOLUTION• COMPLICATIONS
RENAL TRANSPLANTATION
• LIVE DONOR TRANSPLANTATION
• DISEASED DONOR TRANSPLANTATION
CONCEPTS
• GRAFT• RECEPIENT• DONOR• IMMUNO SUPPRESENTS
PHARMACOLOGICAL THERAPY
A) CALCIUM CHANNEL BLOCKERS Nifedipine (Adalat, Procardia) Adult10-30 mg orally tid; not to exceed 120-180 mg/d30-60 mg orally qid; not to exceed 90-120 mg/dPediatric0.25-0.5 mg/kg tid/qid
Effects are believed to be mediated through vasodilation , relaxes smooth muscle and produces vasodilation, which, in turn, improves blood flow and oxygen delivery.
B) BETA BLOCKERS/ BETA RECEPTOR ANTAGONIST( BLOCKERS)
Atenolol
10 – 40 mg/ day
Action
It blocks the beta receptors thereby causes vasodilation and bronchodilation
C) SYNTHETIC ERYTHROPOIETIN
• Epoetin Alfa
50 – 100 Units/ kg Subq or IV three times a week for patient on dialysis.
It stimulate RBC growth and maturation in the bone marrow
DIETARY MANAGEMENTProtein
0.55 – 0.60 g/kg/day
Fluid
1500 mL
Potttasium
60 – 70 mEq/ day
Sodium
1 – 3 g/day
Phosphorus
700 mg/ day
NURSING MANAGEMENT
• Fluid volume excess related to decreased GFR and sodium retension–Monitor sign and symptoms of hypovolemia or
hypervolemia–Monitor urinary output and urine specific
gravity–Monitor serum and urine electrolyte
concentrations–Weigh the patient daily
NURSING MANAGEMENT CONT…..
–Adjust fluid intake to avoid fluid overload and dehydration–Measure blood pressure regularly–Auscultate lung fields for rales– Inspect neck veins for engorgement and
extremities, abdomen, sacrum and eyelids for edema–Evaluate for sign and symptoms of
hyperkalemia and monitor serum K levels
NURSING MANAGEMENT CONT……..
–Administer sodium bicarbonate or glucose and insulin to shift potassium into the cells–Administer cation exchange resin to correct
hyperkalemia –Watch for cardiac arrythmia and CHF–Have resuscitation equipments in hands in
case of cardiac arrest–Advice patient to avoid foods high in
potassium
NURSING MANAGEMENT CONT…..
–Prepare for dialysis when rapid lowering of potassium is needed
–Administer blood transfusions during dialysis to prevent hyperkalemia from stored blood
–Monitor acid base balance
NURSING MANAGEMENT CONT….
• Risk for infection related to alterations in the immune system and host defenses–Monitor for all signs of infection–Remove bladder catheter as soon as possible–Monitor for UTI–Use intensive pulmonary hygiene–Carry out meticulous wound care– If antibiotics are administered care must be
taken to adjust the dosage
NURSING MANAGEMENT CONT….
• Altered nutrition less than body requirements related to catabolic state, anorexia and malnutrition–Regulate protein intake–Offer high carbohydrate feedings–Weigh daily–Restrict food and fluids containing large
amounts of Na, K ,P–Prepare for hyperalimentation
NURSING MANAGEMENT CONT….
• Risk for injury related to GI bleeding–Examine all stools and emesis for gross
and occult blood
–Administer H2 receptor antagonist and antacids for gastric stress ulcers
–Prepare for endoscopy
NURSING MANAGEMENT CONT…..
• Altered thought processes related to uremic toxins on CNS –Speak to the patient in simple orienting
statements ,using repetitions when necessary
–Maintain predictable routine and keep change to a minimum
–Watch for and report changes in mental status and seizure precautions
NURSING MANAGEMENT CONT….
–Encourage and assist patient to turn and move because drowsiness and lethargy may prevent activity
–Use music tape to promote relaxation
–Prepare for dialysis which may help prevent neurologic complications
NURSING MANAGEMENT CONT…..
• Constipation related to fluid restriction and ingestion of phosphate binding agents• Encourage high fibre diet• Use stool softners as prescribed• Avoid laxatives and cathartics that cause
electrolyte toxicities• Increase activity as tolerated
NURSING MANAGEMENT CONT…..
• Impaired skin integrity related to uremic frost and changes in oil and sweat gland–Keep skin clean while relieving itching and
dryness
–Apply oilments and creams for comfort and to relieve itching
–Keep nails short to prevent excoriation
–Keep hair clean and moisturised
NUSING MANAGEMENT CONT…
• RISK FOR INJURY WHILE AMBULATING RELATED TOPOTENTIAL FRACTURES AND MUSCLE CRAMPSDUE TO CALCIUM DEFICIENCY
• Monitor serum ca and p levels• Inspect pts gait , range of motion and muscle strength• Monitor x rays and bone scans for fractures ,
demineralization and joint deposits• Increase activity as tolerated• Administer ca supplements , vitamin d, phosphate
binding agents
NURSING MANAGEMENT CONT…
• NONCOMPLIANCE WITH THE THERAPUETIC REGIMEN RELATED TORESTRICTIONS IMPOSED BY C R F AND ITS TREATMENT
• prepare pt for DIALYSIS or K T P• Assess pts understanding of treatment regimen• Explore alternatives that may reduce or eliminate
side effects of treatment• Encourage strengthening of social support system
and coping mechanisms• Supportive psychotherapy for depression• Refer to renal support agencies and self help
groups
NURSING MANAGEMENT CONT….
• Knowledge defecit related to disease condition– Explain about residual defects in kidney
function– Encourage routine follow up–Advice avoidance of any other medications
unless prescribed– Encourage resuming activity gradually–Weigh daily– Fluid restriction
