children’s mercy hospitals and clinics
TRANSCRIPT

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
1
Children’s Mercy Hospitals and Clinics
Evidence Based Practice Clinical Practice Guideline
Acute Asthma in the Emergency Department/Urgent Care Center Algorithm:
Initial AssessmentBrief history, physical examination, (auscultation, use of accessory muscles, heart
rate, respiratory rate), oxygen saturation, and other tests as indicated
• Oxygen to achieve SaO2 >92%• Albuterol (nebulized)
15 mg/hour • Epinephrine 1:1000 IM
0.01 ml/kg (max. 0.5 ml)• Ipratropium (nebulized)
500 mcg every 20 minutes x 3• Methylprednisolone IV
2 mg/kg (max 80 mg) • Magnesium sulfate IV
50 mg/kg (max 2 grams)• Intubation and mechanical ventilation
with 100% oxygen• HeliOx 80:20 (when indicated)• Consider BiPap
• Oxygen to achieve SaO2 >92%• Continuous Albuterol (nebulized)
< 5 yo: 10 mg/hr≥ 5 yo: 15 mg/hr
• Ipratropium (nebulized)500 mcg every 20 minutes x 3
• Prednisolone/Prednisone (oral)2 mg/kg (max 60 mg)
• Albuterol (MDI with spacer)Dosing by age< 5 yo: 4 puffs≥ 5 yo: 8 puffs
• Consider steroids if ≥ 2 albuterol doses are required
• Prednisolone/Prednisone (oral)2 mg/kg (max 60 mg)
Assess response to treatment (Time Zero + 1 hour)
• Oxygen to achieve SaO2 >92%• Continuous Albuterol (nebulized)
< 5 yo: 10 mg/hr≥ 5 yo: 15 mg/hr
• Ipratropium (if not already administered)500 mcg every 20 minutes x 3
• Prednisolone/Prednisone (oral)(if not already administered)2 mg/kg (max 60 mg)
• Consider Magnesium sulfate IV 50 mg/kg (max 2 grams)
• Oxygen to achieve SaO2 >92%• Continuous Albuterol (nebulized)
< 5 yo: 10 mg/hr≥ 5 yo: 15 mg/hr
• Ipratropium (if not already administered)500 mcg every 20 minutes x 3
• Prednisolone/Prednisone (oral)(if not already administered)2 mg/kg (max 60 mg)
• Magnesium sulfate IV 50 mg/kg (max 2 grams)
• Consider HeliOx to deliver inhaled meds
Admit to Floor / Out of Guideline
Admit to PICU / Out of Guideline
Improved
Assess response to treatment (Time Zero + 2 hours)
To Discharge Algorithm
Mild/ModerateModerate/Severe
IncompleteResponse
Is there Impending/Actual Respiratory Arrest?
Mild/Moderate or Moderate/Severe
Exacerbation?
NoYes
Moderate/Severe
PoorResponse
Improved
Mild/Moderate
Admit to PICU / Out of Guideline

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
2
Epidemiology: The National Health Interview Survey (CDC, 2007) estimated 10 million children (14%) under the age of 18 years had been diagnosed with asthma during their lifetimes. Males are more likely than females to be diagnosed with asthma (16% vs. 12%). Nine percent of Missouri children and ten percent of Kansas children are currently diagnosed with asthma (CDC, 2011). Each day in the United States, 5000 people (children and adults) visit an emergency department for the care of an asthma exacerbation. One-thousand people are subsequently admitted to the hospital. The Asthma and Allergy Foundation of America (2011) reports 11 people die each day from asthma. Symptoms of asthma include difficulty breathing, coughing, and wheezing. The symptoms occur because of the temporary inflammation and narrowing of the airways that occur in response to exposure to inhaled irritants. This pathophysiology is the major cause of an asthma exacerbation. The offending irritants vary from person to person. Objective of Guideline: To standardize the care of children seen in the Emergency Department
for an asthma exacerbation Target Users: ED / UCC physicians, General Pediatricians, Pediatric Nurse Practitioners. Guideline Inclusion Criteria: Children 2- 18 years of age History consistent with asthma exacerbation Guideline Exclusion Criteria: Children < 2 years of age Clinical Questions Answered by the Guideline: The Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma, Full Report 2007 (EPR-3, 2007) is the basis of this guideline. Published medical literature since the creation of EPR-3(2007) has been searched and evaluated to answer the following questions:
Evidence Supports 1. What is the prognostic ability of oxygen saturation values for guiding treatment of
children with acute asthma exacerbations in the ED? 2. What level of oxygen saturation was used as a cutoff for initiation of supplemental
oxygen for subjects in studies of asthma exacerbations? 3. In the child with an asthma exacerbation in the ED, should intramuscular epinephrine
and/or theophylline/aminophylline be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
4. What are the maximum doses of continuous albuterol? 5. In the child with an asthma exacerbation in the ED, should albuterol with ipratropium vs.
albuterol alone be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
3
6. In the child with an asthma exacerbation in the ED, should intravenous magnesium sulfate be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
7. In the child with an asthma exacerbation in the ED, should Heliox-driven albuterol vs. standard albuterol therapy be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
8. In the child with a mild to moderate asthma exacerbation in the ED, should albuterol be administered by nebulizer or metered-dose inhaler (MDI) and spacer to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
9. In the child with an asthma exacerbation in the ED, should prednisolone/prednisone vs. dexamethasone be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
10. In the child with an asthma exacerbation in the ED, should inhaled steroids be initiated during an asthma exacerbation to prevent hospitalization, to decrease time in the ED, to improve pulmonary function, and/or to prevent repeat evaluations in the ED or by other health care providers?
11. In the child with an asthma exacerbation in the ED, should continuous positive airway pressure (CPAP) or bi-level positive airway pressure (BiPap) be used to prevent intubation, and/or to improve pulmonary function?
Evidence does not support: 12. In the child with an asthma exacerbation in the ED, should intravenous montelukast be
used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
13. What is the efficacy of a common MDI when treating patients with asthma exacerbations in the emergency department?
Differential Diagnosis: (EPR-3, 2007, p 46)
• Upper airway diseases o Allergic rhinitis and sinusitis
• Obstructions involving large airways o Foreign body in trachea or bronchus o Vocal cord dysfunction o Vascular rings or laryngeal webs o Laryngotracheomalacia, tracheal stenosis, or bronchostenosis o Enlarged lymph nodes or tumor
• Obstructions involving small airways o Viral bronchiolitis or obliterative bronchiolitis o Cystic fibrosis o Bronchopulmonary dysplasia

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
4
o Heart disease • Other causes
o Recurrent cough not due to asthma o Aspiration from swallowing mechanism dysfunction or gastroesophageal reflux
Practice Recommendations: Physical Exam: A child presenting with an asthma exacerbation should be triaged immediately. A brief history and physical exam focused on the signs and symptoms of the exacerbation should be performed. If a moderate, severe, or life-threatening exacerbation is recognized, treatment should begin without delay (EPR-3, 2007).
Diagnostics: Laboratory tests may be helpful, but are not required for most patients, and they should not delay the initiation of asthma treatment (EPR-3, 2007). Treatment: 1. Dose for continuous nebulized albuterol
a. For all children in impending / actual respiratory arrest the dose is 15 mg/hour. b. For children with a moderate / severe exacerbation the dose is age-based:
i. < 5 years of age 10 mg/hour ii. ≥ 5 years of age 15 mg/hour
2. Administer intravenous magnesium sulfate – 50 mg/kg (maximum 2 grams) to children in impending / actual respiratory arrest.
3. For children with mild to moderate asthma exacerbation, using an MDI with spacer is the recommended route for the administration of albuterol. The recommended dosage in children < 5 years of age is 4 puffs per dose and the recommended dosage in children ≥ 5 years of age is 8 puffs per dose.
4. Corticosteroids are indicated in all moderate-to-severe asthmatics, and in those mild-to-moderate asthma patients who require multiple doses of Albuterol MDI (>=to 2 MDI treatments). Oral steroids are as efficacious as parenteral steroids.
5. If a child with a moderate to severe asthma exacerbation shows limited response to therapy after one hour, administer intravenous magnesium sulfate – 50 mg/kg (maximum 2 grams).
Discharge Criteria: Discharge is appropriate when the patient exhibits:
1. Sustained response to therapy for 60 minutes 2. Improved physical exam 3. No respiratory distress
Outcome Measures:
Case counts- Overall Case counts- by acuity Order of administration (by patient) of medications of interest Medications received Length of stay in the ED by acuity level

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
5
Readmission counts Proportions for asthma cases initially seen in the ED who returned to this department within 72 hours Counts and proportions of ED visits that were asthma associated
Potential Cost Implications: Based upon available cost-analyses, we anticipate a reduction in total costs at Children's Mercy Hospital by replacing single-dose nebulized albuterol with albuterol MDI. Doan (2011) reported a savings of ~$155/patient with a change to MDI use from nebulizer therapy. This information will be tracked at Children's Mercy Hospital following implementation of the Asthma Clinical Practice Guidelines Potential Organizational Barriers: Two potential organizational barriers involve the method and dose of albuterol administration. First, the transition from single-dose nebulized albuterol to metered-dose inhalers (MDI) with spacers is a departure from the current practice at Children's Mercy Hospital. Specifically, we operationalized a process for the proper labeling of MDIs used for treatment in the ED and sent home with patients at discharge. Second, the implementation of a maximum dose of continuous albuterol is an organizational change for CMH.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
6
Supporting tools (i.e. power plans, policies and procedures, care cards, etc.)
1. Power Plan (Appendix A) 2. Physician Asthma Action Plan 2012, (Appendix B) 3. Patient Asthma Action Plans:
a. English AAP for patient http://www.childrensmercy.org/Content/uploadedfiles/7127-090.pdf
b. Spanish AAP for patients http://www.childrensmercy.org/Content/uploadedfiles/7127-090S.pdf
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
7
Question 1: What is the prognostic ability of oxygen saturation values for guiding treatment of children with acute asthma exacerbations in the ED?
Asthma Team Recommendation: The Asthma ED Team strongly recommends using supplemental oxygen to keep the patient’s oxygen saturation ≥ 92%. We value redu cing hospital admissions for children with asthma exacerbation. Data from Boychuk (2006), Mehta (2004), and Keahey (2002) show increases in admission rates when initial oxygen saturation level is ≤ 93%. The three included studies above are robust cohort studies with low indicators of bias. The benefits of an oxygen saturation ≥ 92% outweigh undesirable effects. This recommendation applies to most patients in most circumstances. Further research (if performed) is likely to have an important effect on our confidence in the estimate of effect and may change the estimate. Carruthers (1995) was reviewed but did not contain useful information. Twenty-nine percent of subjects were heavy smokers, and there was inconsistency in obtaining measures (i.e. some were taken while the subject was receiving supplemental oxygen, and some were taken either before or after a treatment with inspired albuterol.
Literature (see Appendix C) supporting this recommendation: Literature was searched since the publication of EPR-3 (2007). 14 citations were found from the search with four citations appearing to answer the question; however, only three articles addressed this specific question. (Boychuck (2006), Mehta (2004) & Keahey (2002)). All 14 citations were read to establish the oxygen saturation level utilized to determine therapy.
Question 2: What level of oxygen saturation was used as a cutoff for initiation of supplemental oxygen for subjects in studies of asthma exacerbations?
Asthma Team Recommendation: The Asthma ED Team strongly recommends using supplemental oxygen to maintain an oxygen saturation ≥ 92%. EPR-3 (2007) states supplemental oxygen should be used to maintain an oxygen saturation of > 90% and continue oxygen therapy until a “clear response to bronchodilator therapy has occurred.” The studies below were read to support a higher oxygen saturation level to guide therapy. The studies are of variable quality; most of them are observational studies with methodological flaws. This recommendation may change when higher quality evidence becomes available. Further research (if performed) is likely to have an important influence on our confidence in the estimate of effect and is likely to change the estimate.
Literature (see Appendix D) supporting this recommendation: Literature was searched since the publication of EPR-3. (2007). Ten of the 14 citations included for Question 1 were read to establish the oxygen saturation level utilized to guide therapy. The citations were reviewed for the oxygen saturation levels that differentiated subjects in any way (i.e. those admitted to the hospital, those who required increased therapy, or those who were readmitted to the ED or hospital). The table below reports the oxygen saturation level used the context of its use, and altitude of the study location.
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
8
Question 3: In the child with an asthma exacerbation in the ED, should intramuscular epinephrine and/or
theophylline/aminophylline be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Asthma ED Team Recommendation: Epinephrine: The Asthma ED Team recommends using intramuscular epinephrine for children in impending/actual respiratory arrest based on very low quality evidence (Consensus). We value preventing the need of mechanical ventilation via the use of parenteral beta agonists. We base this decision on clinical expertise regarding the use of epinephrine in cases of impending respiratory failure. EPR-3 (2007) states parenteral beta agonists have no proven advantage over aerosol therapy. Further research is likely to have an important influence on our confidence in the estimate of effect and may change the estimate of the effect.
Literature supporting this recommendation: Literature was searched since the publication of EPR-3. (2007). No literature was found to support this recommendation.
Theophylline/aminophylline EPR-3 (2007) does not recommend the use of methylxanthines. Specifically in the ED theophylline/aminophylline are not recommended because they appear to provide no additional benefit to optimal SABA therapy and increases the frequency of adverse effects If patients are currently taking a theophylline-containing preparation, determine serum theophylline concentration to prevent theophylline toxicity. The Asthma ED team concurs that methylxanthines should not be added to the treatment of acute asthma for children presenting to the ED, even for those patients with the most severe exacerbations. The D’Avila (2008) study did not demonstrate a decrease in hospital admission using this treatment. We put high value on avoiding a treatment that has not shown efficacy. The recommendation may apply to most patients in most circumstances. Further research is unlikely to change our confidence in the estimate of effect. Literature See (Appendix E) supporting this recommendation Literature was searched since the publication of EPR-3 (2007). One study randomized control trial since EPR-3 (2007) was identified.
Question 4: What is the maximum dose of continuous albuterol?
Asthma ED Team Recommendation: EPR-3 (2007) recommends with the following dosages for intermittent and continuous albuterol: • Child dose (≤ 12 years of age)—0.15 mg/kg (minimum dose 2.5 mg) every 20 minutes for 3 doses then 0.15–0.3 mg/kg up to 10 mg every 1–4
hours as needed, or 0.5 mg/kg/hour by continuous nebulization.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
9
• Adult dose—2.5–5 mg every 20 minutes for 3 doses, then 2.5–10 mg every 1–4 hours as needed, or 10–15 mg/hour continuously.
EPR- 3 (2007) recommends only selective beta2-agonists (albuterol, levalbuterol, pributerol). For optimal delivery, dilute aerosols to minimum of 3 mL at gas flow of 6–8 L/min. Use large volume nebulizers for continuous albuterol administration. Albuterol (as an intermittent or continuous administration) may be mixed with ipratropium nebulizer solution. The Asthma ED Team concurs with these recommendations, including the use of 15 mg/hour as the maximum dose per hour of continuous albuterol The Asthma ED Team values amelioration of symptoms while minimizing adverse effects of the medication. This is a strong recommendation based on EPR-3 (2007).
Question 5: In the child with an asthma exacerbation in the ED, should albuterol with ipratropium vs. albuterol alone be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Asthma ED Team Recommendation: The Asthma ED Team strongly recommends the use of ipratropium for the treatment of severe asthma exacerbations in the ED. This recommendation is included in the EPR-3 (2007) recommendations and is further supported by a well performed randomized controlled trial (Chakraborti, 2006). The recommendation can apply to most patients in most instances. We value timely improvement in pulmonary function and decreased hospitalization rates that have been shown to occur when ipratropium is used in this scenario. Literature (see Appendix F) supporting this recommendation: Literature was searched since the publication of EPR-3. Six citations were found from the search with four citations appearing to answer the question; however, only one article, Chakraborti (2006), answered the question. Question 6: In the child with an asthma exacerbation in the ED, should intravenous magnesium sulfate be administered to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function? Asthma ED Team Recommendation: The Asthma ED Team recommends the administration of intravenous magnesium sulfate 50 mg/kg with a maximum of 2 grams (single dose) for the management of severe asthma. In addition, we recommend the administration of intravenous magnesium sulfate at the same dose for children with moderate asthma exacerbations who fail to respond to continued therapy after one hour. We place a high value on ameliorating symptoms and reducing the hospitalization rate for children with moderate and severe asthma exacerbations.
One meta-analysis, Rowe (2000), reported fewer hospital admissions and shorter lengths of stay in the ED. In addition, in those subjects with severe asthma exacerbations, the change in pulmonary function was significantly better with the administration of magnesium sulfate based on high quality studies. One randomized control trial, Singh (2008), was identified. However, it is a low quality study due to the small number of subjects and large drop-out rate. This study also reported improved lung function as measured by %FEV1 at 120 minutes and decrease number of admission in children treated with intravenous magnesium. This recommendation is based on consistent results from well-performed studies. The recommendation may be

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
10
applied to most patients with severe asthma exacerbations, or to those with moderate asthma exacerbations that do not respond to conventional initial therapy.
Literature (see Appendix G) supporting this recommendation: Literature was searched since the publication of EPR-3. Four citations were found from the search with two citations answering the question, one of these was a Cochrane Collaborative meta-analysis (Rowe, 2000) and the other was a single study (Singh, 2008).
Question 7: In the child with an asthma exacerbation in the ED, should heliox-driven albuterol vs. standard albuterol therapy be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Asthma Team Recommendation: We recommend that heliox-driven albuterol be considered for patients who have life-threatening asthma exacerbations or for those who remain in the severe category after 1 hour of intensive therapy. The recommendation is based on agreement with the EPR-3 (2007) recommendation and two moderate quality papers. This recommendation may be applied to patients in most circumstances. Further research (if performed) is likely to have an important effect on our confidence in the estimate of effect and may change the estimate.
Literature (see Appendix H) supporting this recommendation: Literature was searched since the publication of EPR-3, 2007. Two citations were found from the search and both addressed the question. One of these was a Cochrane Collaborative meta-analysis (Rodrigo, 2010), the other was a randomized control trial reported by Bigham (2010). Both are of moderate quality.
Question 8: In the child with a mild to moderate asthma exacerbation in the ED, should albuterol be administered by nebulizer or MDI and spacer to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Asthma Team Recommendation: The Asthma ED Team strongly recommends an MDI with spacer (with mask in children <4-years-old) be used preferentially for mild to moderate asthma exacerbations in the ED. We placed high value on prompt resolution of symptoms and reduction in cost of treatment. There is consistent evidence from well-conducted, randomized-controlled trials. This recommendation applies to patients in most circumstances. Further research is unlikely to change our confidence in the estimate of effect.
• EPR-3 (2007) states MDI with spacer is as effective as nebulizer for delivering short acting bronchodilators in mild to moderate asthma exacerbations; data in severe exacerbations is severely limited. The EPR-3 (2007) concludes “it is important to assess inhaler techniques for all prescribed medications and reinforce correct technique before patients are discharged home” (p. 104).
• In mild-to-moderate exacerbations, MDI with spacer is as effective as nebulized therapy with appropriate administration technique and coaching by trained personnel. Add mask in children < 4 years
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
11
• One Cochrane meta analysis (Cates, 2006) and three subsequent randomized controlled trials, Jamalvi (2006), Rotta (2010), and Vangveeravong (2008), report improved lung function as assessed by % predicted FEV1, decrease in hospital admission, and decrease time in the ED when MDI with spacer was used over nebulized medication.
• Leversha (2000) reported for 60 children (1-4 years) with acute asthma a lower admission rate for the MDI group. Cost for the nebulizer group was $1282.00; cost for the MDI group was $825.00. Doan (2011) reported that the MDI group saved (Canadian) $155.00/patient
Literature (see Appendix I) supporting this recommendation:
In total, seven studies are included in this synthesis. Literature was searched since the publication of EPR-3 .Thirty nine citations were found from the search with five citations answering the question; four of these were single studies and one was a Cochrane Collaborative meta-analysis (Cates, 2006). One study, Schuh (1999) was selected from the EPR-3 (2007) reference list since it is considered a sentinel study and one study Doan (2011) was found by reviewing the table of contents of relevant publications.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
12
Question 9: In the child with an asthma exacerbation in the ED, should prednisolone/prednisone vs. dexamethasone be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Asthma Team Recommendation: The Asthma ED Team recommends the use of a 5-day course of oral prednisone for acute asthma exacerbations upon discharge. EPR-3 (2007) states dexamethasone is not preferred due to the increased duration of drug activity that increases the risk of adrenal suppression. For this recommendation, we placed a high value on decreasing unscheduled re-evaluations and re-admissions as well as cost of treatment. The Asthma ED Team placed a lower value on symptom scores and compliance with home medication administration.
Literature (see Appendix J) supporting this recommendation: Two of the citations found in the literature search since EPR-3 (2007) answered Question 9. Based on two studies (Altamimi 2006; Gordon 2007), of moderate to low quality, one dose of dexamethasone is comparable to a 5-day course of prednisone for (a) duration in the ED, (b) hospital admission and (c) mean PEF at 1-6 hours. However, unscheduled follow-ups or re-admissions to the ED were lower in the group treated with oral prednisone.
Question 10: In the child with an asthma exacerbation in the ED, should inhaled steroids be initiated during an asthma exacerbation to prevent hospitalization, to decrease time in the ED, to improve pulmonary function, and/or to prevent repeat evaluations in the ED or by other health care providers?
Asthma ED Team Recommendation: Based on the EPR-3 (2007) and studies completed since 2007, we do not recommend treating acute asthma exacerbations with inhaled corticoid steroids (ICS) in the ED. We placed a high value on the effectiveness of oral steroids and no evidence of an added effectiveness of inhaled steroids. Inhaled steroids do not appear to decrease hospitalization rate or time in the Emergency Department.
From EPR 3 (2007): “High doses of an ICS may be considered in the ED, although current evidence is insufficient to permit conclusions about using ICSs rather than oral systemic corticosteroids in the ED (Evidence B). Although simply doubling the dose of the ICS that a patient is taking for long-term therapy at the onset of an exacerbation does not appear to be effective (FitzGerald et al. 2004; Garrett et al. 1998; Harrison et al. 2004; Rice-McDonald et al. 2005), there is increasing evidence that multiple high doses of an ICS (6 mg flunisolide over 3 hours) (Rodrigo and Rodrigo 1998a) or 3 mg fluticasone/hour for 3 hours (Rodrigo 2005) are beneficial when initiated in adults early in the ED. The data on ICS use in children are inconsistent (Rowe et al. 2004). This may be a result of the inconsistency of dosing. One trial reporting greater efficacy for oral corticosteroids used a single high dose of an ICS (2 mg fluticasone) (Schuh et al. 2000), whereas a trial giving multiple doses of budesonide (1.2 mg total) reported increased efficacy for the inhaled route (Singhi et al. 1999). The level of acute asthma severity also may explain apparent discrepancies found in the literature. Although the data are suggestive, a meta-analysis concluded that evidence was insufficient for firm conclusions (Edmonds et al. 2003). Further investigations with greater attention to dosing and acute asthma severity level are required.”

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
13
Literature (see Appendix K) supporting this recommendation: The Team Leaders selected three articles from the PubMed search (57 articles found). Due to the dearth of studies, the references from the Rodrigo (2006) systematic review were synthesized (6 studies selected). Study comparisons and outcomes were disparate; therefore grouping of studies was not possible. Question 11: In the child with an asthma exacerbation in the ED, should CPAP or BiPap be administered to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function? Asthma ED Team Recommendation: The use of Bi-level Positive Airway Pressure (BiPAP) may be utilized to prevent endotracheal intubation in patients with severe asthma exacerbations with impending respiratory failure. We value the prevention of endotracheal intubation in pediatric asthmatics. This recommendation is based upon expert consensus and limited data from very low quality research. Future research on this topic, if performed, is likely to have an important influence on our confidence in the estimate of effect and may change the estimate. Literature (see Appendix L) supporting this recommendation: From the literature search performed by the EBP librarian, no articles were identified. However, two studies were identified by review of references of other studies. Beers (2007) is a retrospective chart review of children who were treated with BiPAP after conventional treatment failure. Brandao (2009) is a poorly reported study performed on adults. Evidence does not support: Question 12: In the child with an asthma exacerbation in the ED, should intravenous montelukast be administered to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Asthma ED Team Recommendation: The Asthma ED Team cannot recommend the use of intravenous montelukast as it is not available in the United States. We do not recommend the use of oral montelukast for the treatment of an acute asthma exacerbation. There is insufficient data to support the effectiveness of this treatment. We placed high value on using treatments with high efficacy (short acting beta agonist and oral corticosteroids) and low value to exposing patients to a medication without evidence to support its use.
Literature (see Appendix M) supporting this recommendation: Three studies were selected to address this question. All were randomized control trials. Studies could not be grouped. The Morris (2010) study looked at IV montelukast, whereas the Kumar (2010) and Harmanci (2006) did not use similar comparisons.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
14
Question 13: What is the efficacy of a shared MDI when treating patients with asthma exacerbations in the emergency department?
Asthma Team Recommendation The Asthma ED Team does not recommend the use of a common container MDI in the ED. Although three low quality papers report low cross-contamination rates, there are significant infection-control concerns with the administration of a shared albuterol canister. We value patient safety over potential cost-savings. Literature supporting this recommendation: Five studies were identified to address this question. Two abstracts (Sheils (2006) and Malik (2006)) evaluated contamination rates of common canister metered-dose inhalers. One narrative review (Smetzer 2009) looked at infection rate and cost. Another narrative review (Lamphere 009) looked at cost. One poster presentation (Mantz 2010) looked at infection rate (See Appendix N)

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
15
How guideline was piloted: 1. Discussed at Emergency Department Section meetings
Guideline Preparation: This guideline was prepared by The Office of Evidence Based Practice (EBP) in collaboration with content experts at Children’s Mercy Hospitals and Clinics. Development of this guideline supports the initiative of the Department of Clinical Effectiveness to promote care standardization that builds a culture of quality and safety that is evidenced by measured outcomes. If a conflict of interest is identified, the conflict will be disclosed next to the team member’s name. Acute Asthma in the Emergency Department/Urgent Care Center Team Members:
• Team Leaders: o K. Williams, MD, General Pediatrics o C. Condra, MD, MSc, Emergency and Urgent Care
• Team Members: o A. Donn, RRT, Clinical Specialist, Respiratory Care o B. John, PharmD, Pulmonology Specialist, Clinical Pharmacy o D. Miller, Family Centered Care Coordinatory, Family-Centered Care Services o H. Murphy, RRT AE-C, Asthma Coordinator, Respiratory Care o R. Yord, RN, Staff nurse, Emergency and Urgent Care o R. Ogden, PharmD, Manager, Pharmacy, Critical Care Services o T. Carver, MD, Medical Directory, Respiratory Care o T. Barnett, MD, Medical Director of Emergency Preparedness o C. Goodyear-Bruch RN, PhD, Senior Nurse Researcher
Office of EBP Team Members:
o N. Allen MS, MLS, RD, LD, CNSC Evidence Based Practice Research Specialist o K. Swaggart, MLIS, Medical Librarian o J. Newland, MD, Director of the Office of Evidence Based Practice o J. Bartlett, PhD (c), Evidence Based Practice Program Manager o T. Franklin, Data Base Coordinator
Guideline development funded by:

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
16
No external funding was obtained in the development of this guideline. Development Process: The review summary documents the following steps: 1. Review of existing internal and external guidelines and standards
a. Internal guidelines: Care of the Asthmatic Patient in the Emergency Department CPG developed in 2012. b. External guidelines: U. S. Department for Health and Human Services, National Institutes of Health, National Heart, Lung and Blood
Institute. (2007). Expert Panel Report 3: Guidelines for the diagnosis and management of asthma. (NIH Publication No. 91-3642). Retrieved from http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf
2. Review preparation a. PICOT (Patient, Intervention, Comparison, Outcome, Type of question) questions established b. Team leaders confirmed search terms employed by the Health Science Medical librarians, reviewed article titles and abstracts from the
search, and identified articles to be read and synthesized by the Evidence Based Practice Scholars. 3. Databases searched
a. AHRQ National Guideline Clearinghouse b. Cochrane c. Medline d. CINAHL
4. Critically analyze the evidence a. Guidelines
i. AGREE criteria were used to analyze published clinical guidelines. b. Single studies
i. The EBP Scholars used the Cochrane Collaborative’s electronic software, Review Manager 5 (RevMan), to produce systematic reviews of the evidence of the effects of healthcare and delivered these documents to the team for review. RevMan allowed the EBP Scholars to build the tables of study characteristics, tables of study biases, and analyze study data in a meta-analysis. . In instances when RevMan could not be used, CASP (Critical Appraisal Skills Programme) tools were utilized to analyze the literature.
ii. When a meta-analysis was found in the literature search, or created in RevMan, the GRADE criteria evaluated the literature using the Cochrane Collaborative’s electronic software known as GRADEprofiler (GRADEpro). GRADEpro assesses the meta-analysis for: 1. Limitations in study design and execution 2. Inconsistency between studies 3. Indirectness of study outcomes 4. Imprecision 5. Publication bias
iii. Table 1 defines how the quality of the evidence is rated and how the recommendation is established based on the type of evidence.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
17
Table 1. Grading of CPG Recommendations
Grade of Recommendation
Confidence in Clarity of Benefits vs Harms,
Burden, and Cost
Quality of Supporting Evidence Implications
Strong recommendation High quality evidence
Desirable effects clearly outweigh undesirable effects or vice versa
Consistent evidence from well-performed RCTs or exceptionally strong evidence from unbiased observational studies
Recommendation can apply to most patients in most circumstances. Further research is unlikely to change our confidence in the estimate of effect
Strong recommendation Moderate-quality evidence
Desirable effects clearly outweigh undesirable effect or vice versa
Evidence from RCTs with important limitations (inconsistent results, methodological flaws, indirect evidence, or imprecise results) or unusually strong evidence from unbiased observational studies
Recommendation can apply to most patients in most circumstances. Further research (if performed) is likely to have an important effect on our confidence in the estimate of effect and may change the estimate.
Strong recommendation Low-quality evidence
Desirable effects clearly outweigh undesirable effect or vice versa
Evidence for at least 1 critical outcome from observational studies, from RCTs with serious flaws or indirect evidence
Recommendation may change when higher-quality evidence becomes available. Further research (if performed) is likely to have an important influence on our confidence in the estimate of effect and is likely to change the estimate.
Strong recommendation Very-low-quality evidence (Very rarely applicable)
Desirable effects clearly outweigh undesirable effect or vice versa
Evidence for at least 1 of the critical outcomes from unsystematic clinical observations or very indirect evidence
Recommendation may change when higher-quality evidence becomes available; any estimate of effect, for at least 1 critical outcome, is uncertain.
Recommended High-quality evidence
Desirable effects closely balanced with undesirable effects
Consistent evidence from well-performed RCTs or exceptionally strong evidence from unbiased observational studies
The best action may differ, depending on circumstances or patients or societal values. Further research is unlikely to change our confidence in the estimate of effect.
Recommended Moderate-quality evidence
Desirable effects closely balanced with undesirable effects
Evidence from RCTs with important limitations (inconsistent results, methodological flaws, indirect evidence, or imprecise results) or unusually strong evidence from unbiased observational studies
Alternative approaches likely to be better for some patients under some circumstances. Further research (if performed) is likely to have an important influence on our confidence in the estimate of effect and may change the estimate.
Recommended Low-quality evidence
Desirable effects closely balanced with undesirable effects
Evidence for at least 1 critical outcome from observational studies, from RCTs with serious flaws or indirect evidence
Other alternatives may be equally reasonable. Further research is likely to have an important influence on our confidence in the estimate of effect and is likely to change the estimate.
Recommended Very-low-quality evidence
Desirable effects closely balanced with undesirable effects
Evidence for at least 1 critical outcome from unsystematic clinical observations or very indirect evidence
Other alternatives may be equally reasonable. Any estimate of effect, for at least 1 critical outcome, is uncertain.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
18
Adapted from: Schunemann, H. J., Vist, G. E., Jaeschke, R., Kunz, R., Cook, D. J., & Guyatt, G. (2002). Advanced topics in moving from evidence to action: Grading recommendations. In Guyatt, G., Rennie, D., Meade, M. O., & Cook, D. J.(Ed.), Users’ guides to the medical literature: A manual for evidence-based clinical practice (pp 679-701). New York, NY:McGraw-Hill.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
19
5. Recommendations for the guideline were developed by a consensus process incorporating the three principles of EBP (current literature, content experts [CPG Team], and patient and family preference [when possible]).
Approval Process: Guidelines are reviewed and approved by an internal and external reviewer, <insert internal and external expert reviewer>, the CPG Team comprised of content expert clinicians, the Office of EBP, Medical Executive Committee and other appropriate hospital committees as deemed suitable for the guideline’s intended use. Guidelines are reviewed and updated as necessary every 3 years within the Office of EBP at CMH&C. The CPG Team will be involved with every review and update.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
20
References Asthma and Allergy Foundation of America. (2011). Asthma facts and figures. Retrieved from
http://www.aafa.org/display.cfm?id=8&sub=42
Altamini, S., Robertson, G., Jastahiah, W., Davey, A., Dehghani, N., Chen, R., Leung, K., & Colburne, M. (2006). Single-dose oral dexamethasone in the emergency management of children with exacerbations of mild to moderate asthma. Pediatric Emergency Care 22(12), 786-793.
Bigham, M. T., Jacobs, B. R., Monaco, M. A., Brilli, R. J., Wells, D., Conway, E. M., Pettinichi, S., & Wheeler, D. S. (2010). Helium/oxygen-driven albuterol nebulization in the management of children with status asthmaticus: A randomized, placebo-controlled trial. Pediatric Critical Care Medicine, 11(3), 356-361.
Boychuk, R. B., Yamamoto, L. G., DeMesa, C. J., & Kiyabu, K. M. (2006). Correlation of initial emergency department pulse oximetry values in asthma severity classes (steps) with the risk of hospitalization. American Journal of Emergency Medicine, 24, 48-52.
Carruthers, D. M., & Harrison, B. D. W. (1995). Arterial blood gas analysis or oxygen saturation in the assessment of acute asthma? Thorax, 50, 186-188.
Cates, C. J., Crilly, J. A., & Rowe, B. H. (2006). Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. The Cochrane Database of Systematic Reviews, (2). doi: 10.1002/14651858.CD000052.pub2.
Chakraborti, A., Lodha, R., Pandey, R. M., & Kabra, S. K. (2006). Randomized controlled trial of ipratropium bromide and salbutamol versus salbutamol alone in children with acute exacerbation of asthma. Indian Journal of Pediatrics;73, 11, 979-983.
Change, A. B., Clark, R., Sloots, T. P., Petsky, H. L., Thearle, D., Champion, A. A., Wheeler, C., & Acworth, J. P. (2008). A 5- versus 3-day course of oral corticosteroids for children with asthma exacerbations who are not hospitalised: a randomised controlled trial. Medical Journal of Australia. 189(6), 306-310.
Connett, G. J., & Lenney, W. (1993). Use of pulse oximetry in the hospital management of acute asthma in childhood. Pediatric Pulmonology, 15, 345-349.
D'Avila, R. S., Piva, J.P., Marostica, P.J., Amantea, S .L. (2008). Early administration of two intravenous bolus of aminophylline added to the standard treatment of children with acute asthma. Respiratory Medicine, 1, 2. [doi: 10.1016/j.rmed.2007.07.030
Decimo, F., Maiello, N., DelGiudice, M., Capristo, C., & Capristo, A. F. (2009). High-dose inhaled flunisolide versus budesonide in the treatment of acute asthma exacerbations in preschool-age children. International Journal of Immunopathology and Pharmacology 22, (2), 363-370.
Doan. Q., Shefrin, A., & Johnson, D. (2011). Cost-effectiveness of metered-dose inhaler for asthma exacerbations in the pediatric emergency department. Pediatrics, 127(5), 1105-1111. doi: 10.1542/peds.2010-2963.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
21
Gordon, S., Tompkins, T., & Dayan, P. S. (2007). Randomized trial of single-does intramuscular dexamethasone compared with prednisolone for children with acute asthma. Pediatric Emergency Care, 23(8), 521-527.
Greenberg, R. A., Kerby, G., & Roosevelt, G. E. (2008). A comparison of oral dexamethasone with oral prednisone in pediatric asthma exacerbations treated in the emergency department. Clinics in Pediatrics, 47, 817-823. doi: 10.1177/0009922808316988.
Higgins, J. P. T., & Green, S. (Eds.). (2009). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.2. The Cochrane Collaboration, 2008. Retrieved from www.cochrane-handbook.org
Jamalvi, S. W., Raza, S. J., Naz, F., Shamim, S., & Jamalvi, Z. W. (2006). Management of acute asthma in children using metered dose inhaler and small volume nebulizer. Journal of the Pakistani Medical Association 56, 595-599. doi: 10.1007/s00228-010-0787-4.
Keahey, L., Bulloch, B., Becker, A. B., Pollack, C. V., Clark, S., & Camargo, C. A. (2002). Initial oxygen saturation as a predictor of admission in children presenting to the emergency department with acute asthma. Annals of Emergency Medicine, 40, 300-307.
Kelly, A. M., Kerr, D., & Powell, C. (2004). Is severity assessment after one hour of treatment better for predicting the need for admission in acute asthma? Respiratory Medicine, 98, 777-781.
Keogh, K. A., Macarthur, C., Parkin, P. C., Stephens, D., Arseneault, R., Tennis, O., Bacal, L., & Schuh, S. (2001). Predictors of hospitalization in children with acute asthma. Journal of Pediatrics, 139, 273-277.
Lamphere, T. (2009, April 29) Protocol power: A respiratory care department finds a common canister protocol reduces costs and wasted meds. [Web log post]. Retrieved from http://respiratory-care-sleep-medicine.advanceweb.com/article/protocol-power-3.aspx
Malik, I., Finch, C., Rudersdorf, T. & Price, K. (2006). Risk of bacterial contamination of shared used metered dose inhalers: Prospective surveillance from oncological ICU. Respiratory Care, Retrieved from: http://www.rcjournal.com/abstracts/2006/?id=OF-06-085
Mantz, H. D., Radke, L., & Gunn, J. (2010). Common canister process for delivering aerosol medication: The final steps to assure patient safety. Poster session presented at the 55th AARC International Respiratory Congress. San Antonio, Texas.
Mehta, S. V., Parkin, P. C., Stephens, D., & Schuh, S. (2004). Oxygen saturation as a predictor of prolonged, frequent bronchodilator therapy in children with acute asthma. Journal of Pediatrics, 145, 641-645.
Milani, G. K. M., Filho, N. A. R, Riedi, C. A., & Figueirdo, B. C. (2004). Nebulized budesonide to treat acute asthma in children. Journal of Pediatrics, 80(2), 106-112.
Nuhoglu, Y., Atas, E., Nuhoglu, C., Iscan, M., & Ozcay, S. (2005). Acute effect of nebulized budesonide in asthmatic children. Journal of Investigational Allergology and Clinical Immunology, 15(3), 197-200.
Razi, C. H., Turktas, I. & Bakirtas, A. (2008). Comparison of single 2,000 microgram dose treatment vs. sequential repeated-dose 500 microgram treatments with nebulized

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
22
budesonide in acute asthma exacerbations. Annals of Allergy, Asthma, and Immunology, 100(4), 370-376.
The Cochrane Collaboration. (2011). Review Manager (RevMan) [Computer program]. Copenhagen: The Nordic Cochrane Centre.
Rodrigo, G. J., Pollack, C. V., & Rowe, B. H. (2010). Heliox for non-intubated acute asthma patients (Review). The Cochrane Database of Systematic Reviews, (4). doi: 10.1002/1465858.CD002884.pub2
Rotta, E. T., Amantea, S. L., Froehlich, P. E., & Becker, A. (2010). Plasma concentrations of salbutamol in the treatment of acute asthma in a pediatric emergency. Could age be a parameter of influence? European Journal of Clinical Pharmacology, 66, 605-610.
Scarfone, R., Loiselle, J., Wiley, J., Decker, J., Henretig, F., Joffe, M. (1995). Nebulized dexamethasone versus oral prednisone in the emergency treatment of asthmatic children. Annals of Emergency Medicine, 26(4), 480-486.
Schuh, S., Johnson, D. W., Stephens, D., Callahan, S., Winders, P., & Canny, G. J. (1999). Comparison of albuterol delivered by a metered dose inhaler with spacer versus a nebulizer in children with mild acute asthma. Journal of Pediatrics, 135(1), 22-27.
Schünemann, H., Brożek, J., & Oxman, A. (Eds.). (2009). GRADE handbook for grading quality of evidence and strength of recommendation. Version 3.2. The GRADE Working Group. Retrieved from http://www.cc-ims.net/gradepro.
Sekerel, B. E., Sackesen, C., Tuncer, A., & Adalioglu, G. (2005). The effect of nebulized budesonide treatment in children with mild to moderate exacerbations of asthma. Acta Pediatrica, 94, 1372-1377.
Sheils, S. G., Duncan, J. L., & Wojciechowski, W. V. (2006. The common canister protocol using the Monaghan aerochamber reveals no cross-contamination and potential cost savings. Respiratory Care, Retrieved from http://www.rcjournal.com/abstracts/2000/?id=A00000303
Singhi, D. S., Kumar, L., & Jayshree, M. (1999). Efficacy of nebulized budesonide compared to oral prednisolone in acute bronchial asthma. Acta Pediatrica, 88, 835-40.
Smetzer, J., Cohen, M. R., & Jenkins, R. (Eds). (2009, April 9) Shared MDIs: Can cross-contamination be avoided? .ISMP Medication Safety Alert 14, 7. 1-7.
Sole, D., Komatsu, M. K., Carvalho, K. V. T., & Naspitz, C. K. (1999). Pulse oximetry in the evaluation of the severity of acute asthma and /or wheezing children. Journal of Asthma, 36(4), 327-333.
Sung, L., Osmond, M. H., & Klaussen, T. P. (1998). Randomized, controlled trial of inhaled budesonide as an adjunct to oral prednisone in acute asthma. Academy of Emergency Medicine, 5, 209-2123.
Tsai, Y., Lee, M., Yang, K. D., Chu, D., Yuh, Y., & Hung, C. ( 2001). A single dose of nebulized budesonide decreased exhaled nitric oxide in children with acute asthma. The Journal of Pediatrics, 139(3), 433-437. doi: 10.1067/mpd.2001.116295

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
23
Vangveeravong, M. (2008). A comparative study of efficacy of salbutamol via metered dose inhaler with volumatic spacer and via dry powder inhaler, Easyhaler, to nebulization in mild to moderate severity acute asthma exacerbation in childhood. Journal of the Medical Association of Thailand, 91, s115-s123.
Volovitz, B., Bilavsky, E., & Nussinovitch, M. (2008). Effectivness of high repeated doses of inhaled budesonide or fluticasone in controlling acute asthma exacerbations in young children. Journal of Asthma 45, 561-567. doi: 10.1080/02770900802005251.
Wright, R. O., Santucci, K. A., Jay, G. D., & Steele, D. W. (1997). Evaluation of pre and posttreatment pulse oximetry in acute childhood asthma. Academic Emergency Medicine, 4(2), 114-117.
U.S. Department of Health and Human Services. Centers for Disease Control and Prevention. (2007). National health 7: Interview survey data. Retrieved from http://www.cdc.gov/nchs/data/series/sr_10/sr10_250.pdf
U.S Department of Health and Human Services. Centers for Disease Control and Prevention. (2011). National environmental public tracking network. Retrieved from http://ephtracking.cdc.gov/showBOReport.action;jsessionid=QdKfTwQhFCG7Q6pwHtWQFM2pzcdnSKcQDC9jJpJmGmCGhC1HLDyk!502299171
U. S. Department for Health and Human Services. National Institutes of Health, National Heart, Lung and Blood Institute. (2007). Expert Panel Report 3: Guidelines for the diagnosis and management of asthma. (NIH Publication No. 91-3642). Retrieved from http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf
Excluded references that did not answer the questions Andrews, T., McGintee, E., Mittal, M., Tyler, L., Chew, A., Zhang, X., Pawlowski, N., & Zorc,
J. J. (2009). High-dose continuous nebulized levo albuterol for pediatric status asthmaticus: A randomized trial. Journal of Pediatrics, 155, 205-210.
Rodrigo, G. J., & Mannini, L. J. (2006). Comparison between nebulized adrenaline and b2 agonists for the treatment of acute asthma: A meta-analysis of randomized trials. American Journal of Emergency Medicine, 24. 217-222. doi: 10.1016/j.ajem.2005.10.008
Rowe, B. H., Bretzlaff, J., Bourdon, C., Bota, G., Blitz, S., & Camargo, C. A. (2000). Magnesium sulfate for treating exacerbations of acute asthma in the emergency department. The Cochrane Database of Systematic Reviews, (1). doi: 10.1002/14651858.CD001490.
Singh, A. K., Gaur, S., & Kumar, R. (2010). A randomized controlled trial of intravenous magnesium sulphate as an adjunct to standard therapy in acute severe asthma. Iran Journal of Allergy, Asthma, and Immunology, 7(4), 221-229.
Wantansomsiri, A., & Phipatanakul, W. (2006). Comparison of nebulized ipratropium bromide with salbutamol vs. salbutamol alone in acute asthma exacerbation in children. Annals of Allergy, Asthma and Immunology, 96, 701-706.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
24
Appendix A Power Plan- Under construction

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
25
Appendix B Physician AAP – 12

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
26

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
27

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
28

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
29
Appendix C
Question 1: What is the prognostic ability of oxygen saturation values for guiding treatment of children with acute asthma exacerbations in the ED?
Synthesis of relevant studies: Author, date, country, and industry of
funding Patient Group
Level of Evidence (Oxford)
Research design Significant results Limitations
Boychuk, R. B., Yamamoto, L.G., DeMesa, C.J., & Kiyabu, K.M. (2006).
1219 encounters of 1008 unique children with acute asthma in 5 EDs/clinics, including urban, suburban and rural settings.
Children were> 12 months and < 18 years, presenting with wheezing or bronchospasm. Convenience enrollment
Prospective cohort study.
Asthma severity was determined by NIH severity class groups.
Phase 1 subjects received usual care.
Phase 2 subjects received an educational video, and a written asthma action plan
Phase 1 and Phase 2 groups were similar except Phase 2 subjects were older. (Phase 1 mean age was 3.6 + 2.3 and Phase 2 mean age was 4.3 + 3.4 [p< 0.0001]).
The overall hospitalization rate was 15%. The greater the severity classification, the
higher the hospitalization rate. The lowest severity group was least likely
to have an asthma action plan. Hospitalization rates by presenting oxygen
saturation: Presenting oxygen
saturation Admission rate 98% or > 6% 95%-97% 12% 93%-94% 28% 90%-92% 45% 85%-89% 65% 80%-84$ 100%
The mean O2 saturation across severity scores ranged from 96.0 +3.0 to 96.8+2.5. There was no significance among initial O2 saturation and severity score. Severity score was not related to admission rate.
Severity Score is a global score of asthma, not a measure of the event that brought the child to the ED. It is easy to confuse the term “severity score” in relation to the acute event versus the burden of the disease which the score measures.
The age difference between Phase 1 and Phase 2 subjects could be a concern for bias.
Some of the initial O2 saturation measures may have been obtained with the subject getting O2.
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
30
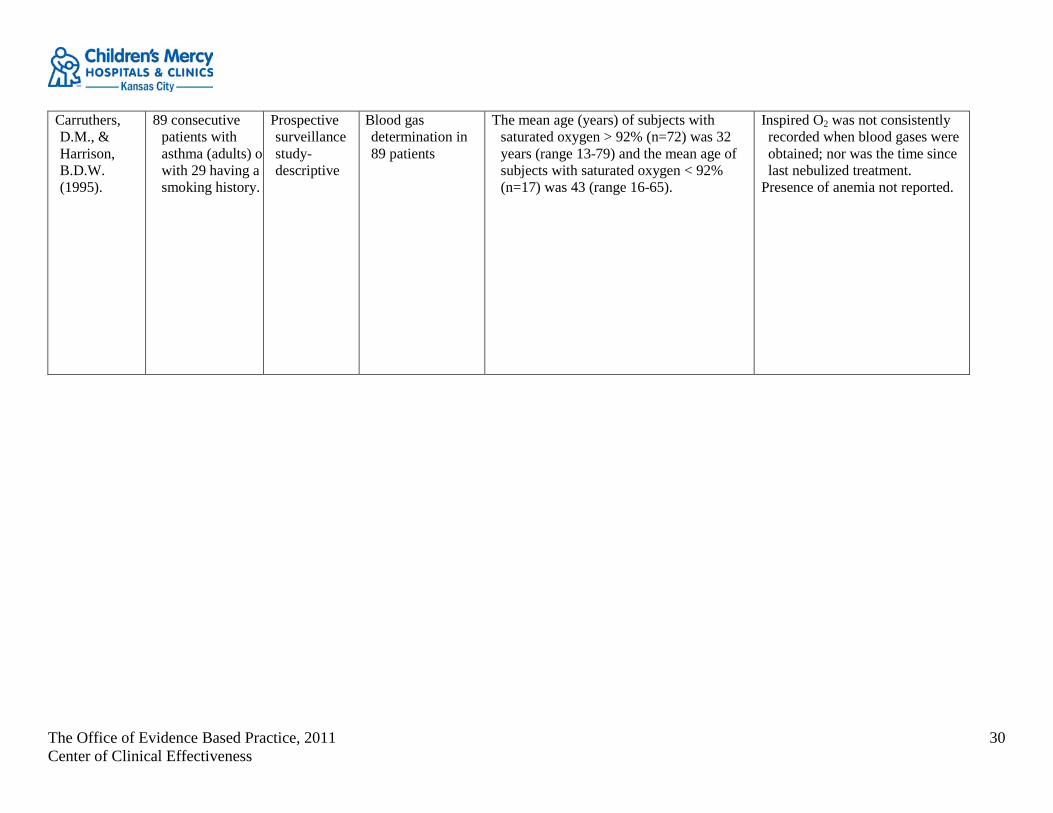
Carruthers, D.M., & Harrison, B.D.W. (1995).
89 consecutive patients with asthma (adults) of with 29 having a smoking history.
Prospective surveillance study- descriptive
Blood gas determination in 89 patients
The mean age (years) of subjects with saturated oxygen > 92% (n=72) was 32 years (range 13-79) and the mean age of subjects with saturated oxygen < 92% (n=17) was 43 (range 16-65).
Inspired O2 was not consistently recorded when blood gases were obtained; nor was the time since last nebulized treatment.
Presence of anemia not reported.
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
31
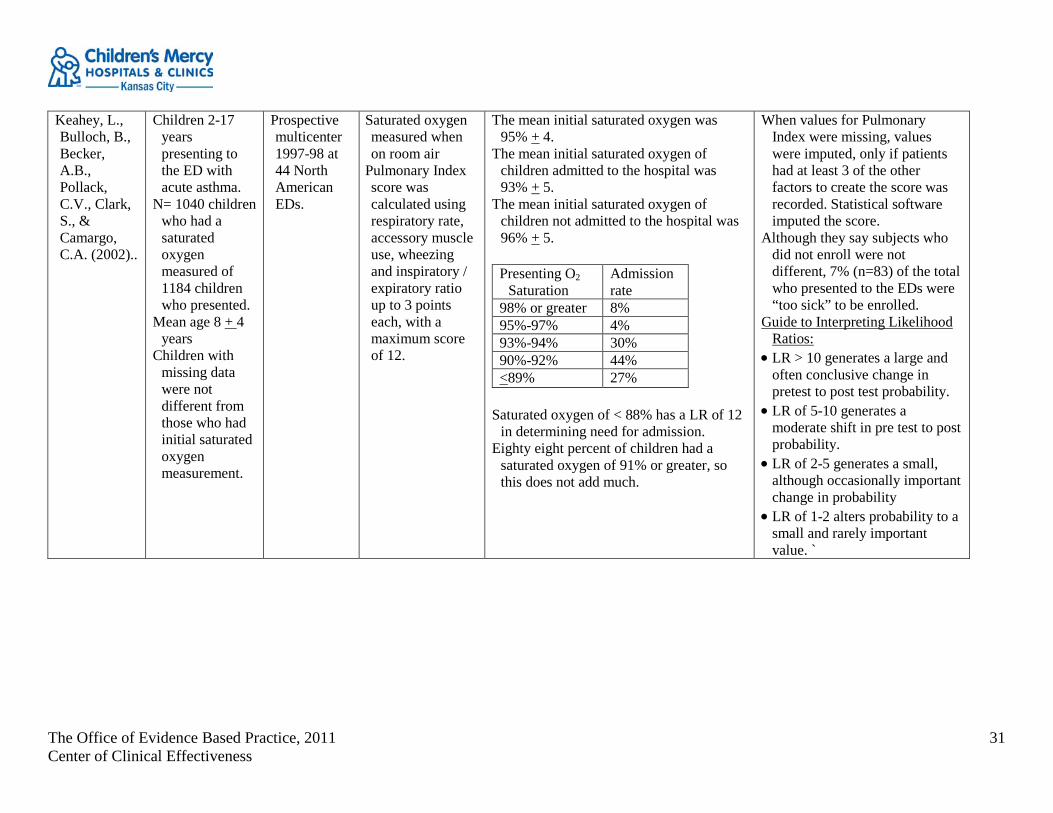
Keahey, L., Bulloch, B., Becker, A.B., Pollack, C.V., Clark, S., & Camargo, C.A. (2002)..
Children 2-17 years presenting to the ED with acute asthma.
N= 1040 children who had a saturated oxygen measured of 1184 children who presented.
Mean age 8 + 4 years
Children with missing data were not different from those who had initial saturated oxygen measurement.
Prospective multicenter 1997-98 at 44 North American EDs.
Saturated oxygen measured when on room air
Pulmonary Index score was calculated using respiratory rate, accessory muscle use, wheezing and inspiratory / expiratory ratio up to 3 points each, with a maximum score of 12.
The mean initial saturated oxygen was 95% + 4.
The mean initial saturated oxygen of children admitted to the hospital was 93% + 5.
The mean initial saturated oxygen of children not admitted to the hospital was 96% + 5.
Presenting O2
Saturation Admission rate
98% or greater 8% 95%-97% 4% 93%-94% 30% 90%-92% 44% <89% 27%
Saturated oxygen of < 88% has a LR of 12
in determining need for admission. Eighty eight percent of children had a
saturated oxygen of 91% or greater, so this does not add much.
When values for Pulmonary Index were missing, values were imputed, only if patients had at least 3 of the other factors to create the score was recorded. Statistical software imputed the score.
Although they say subjects who did not enroll were not different, 7% (n=83) of the total who presented to the EDs were “too sick” to be enrolled.
Guide to Interpreting Likelihood Ratios:
• LR > 10 generates a large and often conclusive change in pretest to post test probability.
• LR of 5-10 generates a moderate shift in pre test to post probability.
• LR of 2-5 generates a small, although occasionally important change in probability
• LR of 1-2 alters probability to a small and rarely important value. `

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
32
Mehta, S.V., Parkin, P.C., Stephens, D., & Schuh, S. (2004).
Children 1 to 17 years of age.
N= 273 All required
corticosteroids. 4 groups,
subjects can be in more than one group
1. Needing frequent bronchodilator therapy (FBT) < 4 hours; N=107
2. Needing FBT > 4 hours; N= 166
3. needing FBT < 12 hours; N=194
4. needing FBT > 12 hours; N=79
The data was from a previously published prospective cohort study.
All subjects in the first hour were treated with: • Prednisone 2
mg/kg po Albuterol 0.15 mg/kg and ipratropium 250 micrograms / dose - 3 consecutive doses
and either • Dexamethasone
0.3 mg/kg po or • Hydrocortisone
5 mg/kg or • Prednisone 2
mg/kg po
The mean baseline saturated oxygen in the < 4 hour group was 95.5%.
The mean baseline saturated oxygen in the > 4 hour group was 93.3%.
The mean baseline saturated oxygen in the <12 hour group was 95.0%.
The mean baseline saturated oxygen in the > 12 hours group was 92.1%
The authors preformed a secondary data analysis for this study.
There is a small number of subjects with low oxygen saturation values. This causes wide confidence intervals around the odds ratios and likelihood ratios. Therefore the results are not precise.
Synthesis Author: Allen, N. Date: February 2011

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
33
Appendix D Question 2: What level of oxygen saturation was used as a cutoff for initiation of supplemental oxygen for subjects in
studies of asthma exacerbations? First Author, Year Saturated Oxygen Values Locations
Kelly 2004 Mild > 94%, Moderate 94-90% and Severe < 90% 36 Australian centers Keogh 2001 Used a saturated oxygen of < 92% to administer supplemental oxygen Toronto Canada, altitude: 105 m. (347 ft.)
Solé 1999 92% was the cut off predicting the necessity to repeat treatment Sao Paulo Brazil, altitude: 637 ft. above sea level.
Wright 1997 Pretreatment saturated oxygen < 91% was not useful in predicting admission/relapse (sensitivity 0.24, specificity 0.86, likelihood ratio of 1.77) and Post treatment saturated oxygen < 91% had a sensitivity of 0.34 and a specificity of 0.98 with a likelihood ratio of 16.43 to predict admission/relapse.
Providence RI, altitude: 50 ft.
Keahey 2002 The mean saturated oxygen of children admitted was 93 + 5% and the mean saturated oxygen of children not admitted was 96% + 3%
44 Emergencies 18 in US states and 4 Canadian provinces.
Carruthers 1995 Adults 32% were smokers used a saturated oxygen of < 92 > for differentiation
Norwich UK, altitude: 30 m. (28 ft.)
Mehta 2004 In the group (n= 107) that needed < 4 hours of frequent bronchodilator treatment (FBT) presenting saturated oxygen was 95.5 + 2. In the group (n=166) that needed > 4 hours of FBT, presenting saturated oxygen was 93.3 + 3.8
Toronto Canada, altitude: 105 m. (347 ft.)
Boychuk 2006 Presenting saturated oxygen < 90 related to increased hospitalization Honolulu HI, altitude: 4 m. (9 ft.)
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
34
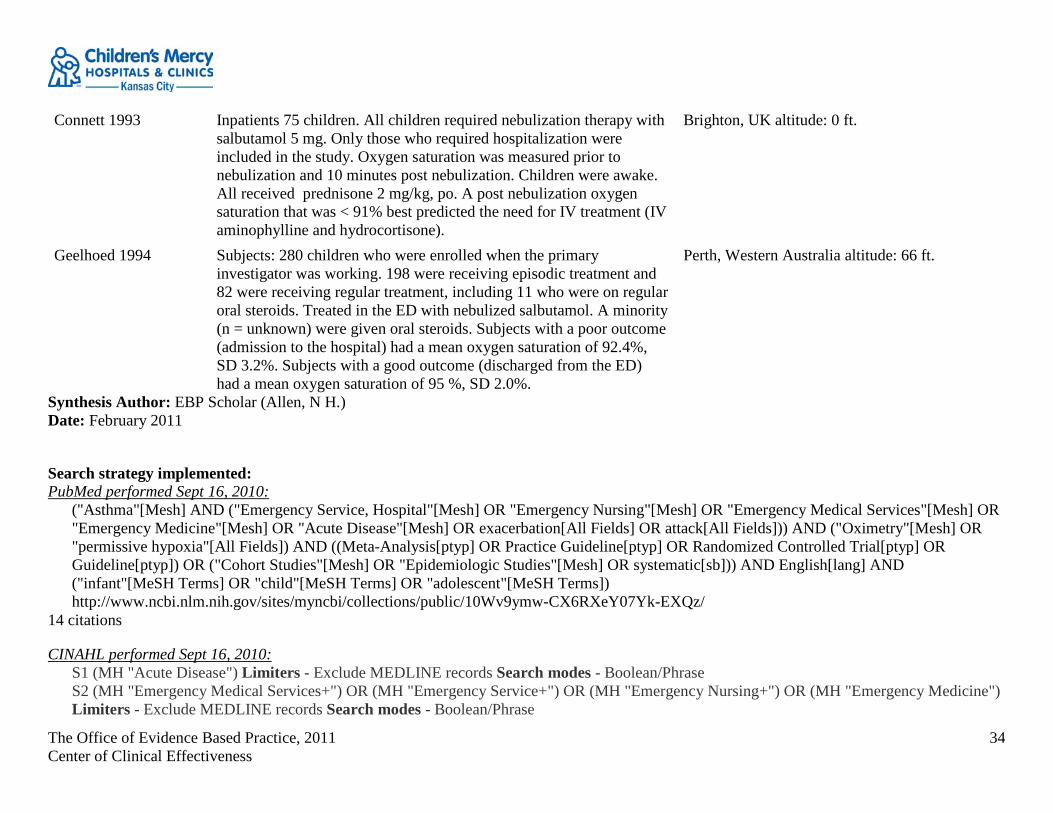
Connett 1993 Inpatients 75 children. All children required nebulization therapy with salbutamol 5 mg. Only those who required hospitalization were included in the study. Oxygen saturation was measured prior to nebulization and 10 minutes post nebulization. Children were awake. All received prednisone 2 mg/kg, po. A post nebulization oxygen saturation that was < 91% best predicted the need for IV treatment (IV aminophylline and hydrocortisone).
Brighton, UK altitude: 0 ft.
Geelhoed 1994 Subjects: 280 children who were enrolled when the primary investigator was working. 198 were receiving episodic treatment and 82 were receiving regular treatment, including 11 who were on regular oral steroids. Treated in the ED with nebulized salbutamol. A minority (n = unknown) were given oral steroids. Subjects with a poor outcome (admission to the hospital) had a mean oxygen saturation of 92.4%, SD 3.2%. Subjects with a good outcome (discharged from the ED) had a mean oxygen saturation of 95 %, SD 2.0%.
Perth, Western Australia altitude: 66 ft.
Synthesis Author: EBP Scholar (Allen, N H.) Date: February 2011
Search strategy implemented: PubMed performed Sept 16, 2010:
("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Oximetry"[Mesh] OR "permissive hypoxia"[All Fields]) AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp]) OR ("Cohort Studies"[Mesh] OR "Epidemiologic Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms]) http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/10Wv9ymw-CX6RXeY07Yk-EXQz/
14 citations
CINAHL performed Sept 16, 2010: S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S2 (MH "Emergency Medical Services+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
35
S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 (MH "Disease Exacerbation") Search modes - Boolean/Phrase S5 S1 or S2 or S4 Search modes - Boolean/Phrase S6 S3 and S5 Search modes - Boolean/Phrase S7 (MH "Oximetry+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S8 permissive hypoxia Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase Search modes - Boolean/Phrase S9 S6 and S7 Search modes - Boolean/Phrase S10 S6 and S7 Limiters - English Language; Human; Age Groups: All Child
0 citations

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
36
Appendix E Question 3: In the child with an asthma exacerbation in the ED, should intramuscular epinephrine and/or theophylline/aminophylline be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
GRADEprofiler Table: D'Avila, R. S., Piva, J.P., Marostica, P.J., Amantea, S .L. Early administration of two intravenous bolus of aminophylline added to the standard treatment of children with acute asthma. Respiratory Medicine 2008,102. [DOI: 10.1016/j.rmed.2007.07.030] Country of origin: Brazil.
Quality assessment Summary of findings
Importance No of patients Effect
Quality No of studies Design Limitations Inconsistency Indirectness Imprecision Other
considerations
Aminophylline added to
standard care control Relative
(95% CI) Absolute
Admission (follow-up 0-6 hours; hospitalization) 11 randomised
trials no serious limitations
no serious inconsistency
no serious indirectness
serious2 none
5/30 (16.7%) 9/30 (30%)
OR 0.47 (0.14 to 1.61)
132 fewer per 1000 (from 243 fewer to
108 more)
MODERATE CRITICAL
1 D"Avila 2008 2 small study Synthesis Author: EBP Scholar, (Allen, N.H) Date:2 011-1-25 Forest Plot of Single Studies since EPR 3 (2007)

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
37
Forest plot: Aminophylline vs. saline, outcome: O2
Use.
Study or SubgroupD"Avila 2008
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.64 (P = 0.52)
Events23
23
Total30
30
Events25
25
Total30
30
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.66 [0.18, 2.36]
0.66 [0.18, 2.36]
Aminophylline--Exp Saline--Control Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours experimental Favours control
Forest plot: Aminophylline vs. saline, outcome: Admission.
Study or SubgroupD"Avila 2008
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.21 (P = 0.23)
Events5
5
Total30
30
Events9
9
Total30
30
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.47 [0.14, 1.61]
0.47 [0.14, 1.61]
Aminophylline--Exp Saline--Control Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours experimental Favours control
Included Single Study Characteristics and Risk of Bias Tables: D"Avila 2008 Characteristic of included study:
Methods Randomized, Double Blind, Placebo Controlled Clinical Trial Participants 60 children (2–5 years old), admitted to the Pediatric Emergency Room (PER) at Hospital de Clınicas de Porto Alegre (Brazil), due
to an episode of acute asthma, refractory to conventional therapy (an oral dose of steroids and at least three doses of inhaled albuterol, associated or not with oxygen.
Interventions The intervention group (group I) received two doses of IV aminophylline (5 mg/kg—at 6 h of interval) diluted in saline solution (up to 20 cc) and the placebo group (group II) received two infusions (at 6 h of interval) of normal saline (NS) solution (20 cc). The placebo solution (NS solution) and aminophylline infusion had the same color and volume (20 mL) infused at a rate of 1 cc/h over 20 min.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
38
Outcomes The main outcomes considered were length of supplemental oxygen, number of bronchodilator nebulizations or aerosol puffs, length of stay in the PER (in h).
Notes Patients who needed immediate tracheal intubation, had known allergy to methylxanthines, had used such medication in the previous hours, had a history of difficult to control convulsive seizures in the last week, had a seizure episode at the time of admission, were excluded. To avoid drug interactions, patients who were in current use of erythromycin, cimetidine, phenytoin, phenobarbital, carbamazepine or rifampicin were also excluded.
Risk of bias table: Bias Authors' judgement Support for judgment
Random sequence generation (selection bias) Unclear risk The patients were allocated in two treatment groups. Randomization was generated in blocks of 10 patients (5 in each group).
Allocation concealment (selection bias) Low risk The head nurse of the PER was responsible for disclosing the codes and preparing the solutions according to the sequence of randomization.
Blinding (performance bias and detection bias) Low risk The head nurse was not involved with the patient care. Incomplete outcome data (attrition bias) Unclear risk Selective reporting (reporting bias) Unclear risk Other bias Unclear risk
Search Strategy: PubMed search September 16, 2010
(("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Magnesium Sulfate"[Mesh] OR "heliox "[Substance Name] OR "Continuous Positive Airway Pressure"[Mesh] OR "Epinephrine"[Mesh] OR "Terbutaline"[Mesh] OR "zafirlukast "[Substance Name] OR "zileuton "[Substance Name] OR "montelukast "[Substance Name] OR "Receptors, Leukotriene"[Mesh] OR "Leukotriene Antagonists"[Mesh] OR "methylxanthine "[Substance Name] OR "Phosphodiesterase Inhibitors"[Mesh] OR "Theophylline"[Mesh] OR "Aminophylline"[Mesh])) AND ("humans"[MeSH Terms] AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp]) OR ("Cohort Studies"[Mesh] OR "Epidemiologic Studies"[Mesh]

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
39
OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms])) AND ("2006/03"[PDAT] : "2010"[PDAT]) http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/10Snxom1j-gcPHZmWk6XHW85-/
39 results
CINAHL search September 16, 2010 S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes -Boolean/Phrase S2 (MH "Emergency MedicalServices+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine")
Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 heliox OR zileuton OR zarfirlukast OR
methylxanthines Search modes - Boolean/Phrase S5 (MH "Disease Exacerbation") Search modes - Boolean/Phrase S6 (MH "Magnesium Sulfate") OR (MH "Continuous Positive Airway Pressure") OR (MH "Epinephrine+") OR (MH "Terbutaline") OR (MH
"Leukotriene Antagonists+") OR (MH "Montelukast") OR (MH "Phosphodiesterase Inhibitors+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase
S7 S1 or S2 or S5 Search modes - Boolean/Phrase S8 S3 and S7 Search modes - Boolean/Phrase S9 S4 or S6 Search modes - Boolean/Phrase S10 S8 and S9 Search modes - Boolean/Phrase S11 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Human; Publication Type: Algorithm, Clinical Trial,
Journal Article, Nursing Interventions, Practice Guidelines, Protocol, Systematic Review; Age Groups: All Child Search modes - Boolean/Phrase
S12 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Age Groups: All Child Search modes - Boolean/Phrase 1 result

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
40
Appendix F Question 5: In the child with an asthma exacerbation in the ED should albuterol with ipratropium vs. albuterol alone be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Forest Plots of Single Studies since EPR-3 (2007): Albuterol versus. albuterol with ipratropium, Outcome- Symptom Score.
Study or SubgroupChakraborti 2006
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 0.50 (P = 0.62)
Mean1.27
SD1.2
Total30
30
Mean1.43
SD1.28
Total30
30
Weight100.0%
100.0%
IV, Fixed, 95% CI-0.16 [-0.79, 0.47]
-0.16 [-0.79, 0.47]
Experimental Control Mean Difference Mean DifferenceIV, Fixed, 95% CI
-2 -1 0 1 2Favours experimental Favours control
Albuterol versus albuterol with ipratropium, Outcome- PEF %.
Study or SubgroupChakraborti 2006
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 2.14 (P = 0.03)
Mean82.32
SD25.93
Total30
30
Mean69.53
SD19.87
Total30
30
Weight100.0%
100.0%
IV, Fixed, 95% CI12.79 [1.10, 24.48]
12.79 [1.10, 24.48]
Experimental Control Mean Difference Mean DifferenceIV, Fixed, 95% CI
-20 -10 0 10 20Favours control Favours experimental
Included Single Study Characteristics and Risk of Bias Tables: Chakraborti 2006
Characteristics of included study: Methods RCT Participants Children (N = 60) between 5 and 15 years with mild to moderate asthma exacerbation. Children had to be able to perform
spirometry. Interventions Each subject was administered 4 actuations of salbutamol (100 micrograms) via MDI. Study drug or placebo was

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
41
administered after that. Experimental- 100 micrograms ipratropium X 4 actuations Control- placebo
Outcomes Asthma score and spirometric parameters % predicted PEF
Risk of bias: Bias Scholars' judgment Support for judgment
Random sequence generation (selection bias) Low risk Computer generated block randomization Allocation concealment (selection bias) Low risk Blinding (performance bias and detection bias) Unclear risk Study drug preparation and analysis were blinded. Masking of
study drug was assessed by medical residents. Incomplete outcome data (attrition bias) Low risk Selective reporting (reporting bias) Low risk Other bias Low risk Met numbers required for detecting a difference.
Synthesis Author: EBP Scholar (Allen, N H.) Date: 2010-10-25
Search Strategy: PubMed performed August 25, 2010:
(("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Ipratropium"[Mesh] OR ("Albuterol"[Mesh] AND "Ipratropium"[Mesh]) OR "albuterol-ipratropium "[Substance Name])) AND ("humans"[MeSH Terms] AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp] OR Comparative Study[ptyp]) OR ("Cohort Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms])) AND ("2006/03"[PDAT] : "2010"[PDAT])
6 citations http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/1J5opi9rKsoR15o8LVnMj5KQN/
CINAHL performed August 25, 2010: S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes Boolean/Phrase

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
42
S2 (MH "Emergency Medical Services+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 (MH "Disease Exacerbation") Search modes - Boolean/Phrase S5 S1 or S2 or S4 Search modes - Boolean/Phrase S6 S3 and S5 Search modes - Boolean/Phrase S7 (MH "Ipratropium") AND (MH "Albuterol") Search modes - Boolean/Phrase S8 (MH "Ipratropium") Search modes - Boolean/Phrase S9 albuterol-ipratropium Search modes - Boolean/Phrase S10 S7 or S8 Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S11 S9 or S10 Search modes - Boolean/Phrase S12 S6 and S11 Search modes - Boolean/Phrase S13 S6 and S11 Limiters - Published Date from: 20060301-20101031; English Language; Age Groups: All Child Search modes - Boolean/Phrase
0 citations

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
43
Appendix G Question 6: In the child with an asthma exacerbation in the ED should intravenous magnesium sulfate be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
GRADEprofiler Table: Rowe BH, Bretzlaff J, Bourdon C, Bota G, Blitz S, Camargo CA.( 2000). Magnesium sulfate for treating exacerbations of acute asthma in the emergency department. Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD001490. DOI: 10.1002/14651858.CD001490.
Quality assessment Summary of findings
Importance No of patients Effect
Quality No of studies Design Limitations Inconsistency Indirectness Imprecision Other
considerations IV
magnesium control Relative
(95% CI)
Absolute
Admission- Severe Group (follow-up 2-15 hours1; admission) 42,3,4,5 randomized
trials no serious limitations
no serious inconsistency
no serious indirectness
no serious imprecision
none 34/70 (48.6%)
57/63 (90.5%)
OR 0.14 (0.07 to
0.3)
334 fewer per 1000 (from 165 fewer to 505 fewer)
HIGH CRITICAL
Pulmonary Function % predicted (follow-up median 2-15 hours1; measured with: % predicted FEV1; Better indicated by higher values) 32,3,6 randomized
trials no serious limitations
serious7 no serious indirectness
serious8 none 209 206 - MD 4.33 lower (10.95 lower to 2.3 higher)9
LOW CRITICAL
Pulmonary Function Absolute PEF (follow-up 2-15 hours1; Better indicated by higher values) 53,5,6,10,11 randomized
trials no serious limitations11
no serious inconsistency
no serious indirectness
serious8 none 234 240 -
MD 29.4 lower (62.2 lower to 3.4 higher)9
MODERATE CRITICAL
Duration in the ED (follow-up 2-15 hours1; measured with: time; Better indicated by lower values) 24,11 randomized
trials no serious limitations
no serious inconsistency
no serious indirectness
serious8 none 82 85 - MD 5.28 lower (9.34 to 1.21 lower)
MODERATE CRITICAL
Pulmonary Function severe group % predicted FEV1 (follow-up 2-15 hours1; Better indicated by higher values) 32,3,6 randomized
trials no serious limitations
no serious inconsistency
no serious indirectness
no serious imprecision
none 163 152 - MD 9.81 lower (15.82 to 3.8 lower)9
HIGH CRITICAL
Pulmonary Function severe group absolute PEF (follow-up 0.75-15 hours; Better indicated by higher values) 3 randomized
trials no serious limitations
no serious inconsistency
no serious indirectness
no serious imprecision
none 161 157 - MD 52.25 lower (77.5 to 27 lower)9
HIGH CRITICAL
Pulmonary Function severe absolute FEV1 (follow-up < 15 hours; Better indicated by higher values)

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
44
14 randomized trials
no serious limitations
no serious inconsistency
no serious indirectness
no serious imprecision
none
15 16 - MD 17 lower (22.76 to 11.24 lower)9
HIGH CRITICAL
1 The range is the time after admission to the ED when assessments of subjects who were enrolled in the study began. In all studies, subjects who were too ill to receive at least 3 SABA treatments were not randomized to the magnesium study. Three of the four studies starting assessing for admission at 2 hours after being in the ED (or 1 hour after Mg administration) and made the decision to admit within 4 hours. The Devi (1997) assessed patients out to 15 hours. The timing of the admission assessment was not described in this study. 2 Bloch 1995 3 Ciarallo 1997 Pediatric study 4 Devi 1997 Pediatric study 5 Skobeloff 1989 6 Silverman 1996 7 I squared stat 73% 8 Estimate of effect includes zero. 9 For the measurement of effect of all pulmonary functions in this review better is indicated by lower numbers. All measures are the difference between the baseline value and the treated value. As difference between the treated value and the base line value becomes more negative as the the treatment value becomes greater. 10 Tiffany 1993 11 Green 1992 did not blind
Synthesis Author: EBP Scholar (Allen, N H.) Date: 2010-11-04
Forest Plot of Single Studies since EPR-3 (2007) Effect of IV Magnesium added to Standard Therapy, outcome: %FEV1 at 120 minutes.
Study or SubgroupSingh 2008
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 2.85 (P = 0.004)
Mean62.84
SD10.02
Total30
30
Mean56.7
SD6.2
Total30
30
Weight100.0%
100.0%
IV, Fixed, 95% CI6.14 [1.92, 10.36]
6.14 [1.92, 10.36]
Favours experimental Control-standard care Mean Difference Mean DifferenceIV, Fixed, 95% CI
-100 -50 0 50 100Favours control Favours experimental
Effect of IV Magnesium added to Standard Therapy, outcome: Hospitalization

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
45
Study or SubgroupSingh 2008
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 2.15 (P = 0.03)
Events2
2
Total30
30
Events9
9
Total30
30
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.17 [0.03, 0.85]
0.17 [0.03, 0.85]
Favours experimental Control-standard care Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours experimental Favours control
Synthesis Author: EBP Scholars (Allen, N.H., Bartlett, J. A., Dusin, J. D., Gordon, B., Hodges, K., Newman, R. E., Pirvu, D., & Shubat, S. J.) Date: 2010-11-04
Risk of bias summary figure:
Rand
om se
quen
ce g
ener
ation
(sele
ction
bias
)
Singh 2008 +
Alloc
ation
conc
ealm
ent (
selec
tion
bias)
?
Blind
ing (p
erfo
rman
ce b
ias a
nd d
etec
tion
bias)
?
Inco
mple
te o
utco
me
data
(attr
ition
bias)
+
Selec
tive
repo
rting
(rep
ortin
g bia
s)
+
Othe
r bias
+
Included Single Study Characteristics and Risk of Bias Tables: Singh 2008
Characteristics of included study:

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
46
Methods placebo controlled, randomized single blind Participants Adults 18-60 years of age with acute asthma as evidenced by FEV1 < 30% predicted, willing to remain in the ED for 3
hours and fulfilled most of the criteria for severe asthma according to the GINA criteria. Interventions Group A (IV MgSO4 group): Patients received 1 mL of 2.5% salbutamol (2.5 mg), 250 micrograms of 1.5 ml ipratropium
administered in 2.5 mL of normal saline via wet nebulizer with 100% oxygen at 0,20,40 minutes after admission into the protocol. At 30 min, the patient received 2 g magnesium sulphate in 250 mL of normal saline solution given slowly over 20 minutes. Group B (control group): Patients received 1 mL of 2.5% salbutamol (2.5 mg), 250 micrograms of 1.5 ml ipratropium administered in 2.5 mL of normal saline via wet nebulizer with 100% oxygen at 0,20,40 minutes after admission into the protocol. At 30 min, the patient received like-appearing placebo in 250 mL of normal saline solution.
Outcomes Primary: % predicted FEV1 at 120 minutes. Secondary: Admission to the hospital Notes Excluded: History of COPD or other chronic lung disease, known cardiac, renal, or hepatic dysfunction, pregnant or
lactating, Patients unable to perform spirometry or those who required intubation. Power was calculated to detect a 0.32 L difference in FEV1 and a 15% difference in hospital admissions at 80% power.
Risk of bias: Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk Random numbers table, 1:1 randomization table Allocation concealment (selection bias) Unclear risk Envelope concealment, until patient was included in the
assigned group. Blinding (performance bias and detection bias) Unclear risk Not sure who was blinded in the ED, however the staff
making the decision to discharge or admit the subject was blinded.
Incomplete outcome data (attrition bias) Low risk 75 screened, 5 excluded, 10 protocol violations. Selective reporting (reporting bias) Low risk Other bias Low risk
Synthesis Author: EBP Scholar (Allen, N H.) Date: 2010-11-04
Search Strategy: PubMed search September 16, 2010
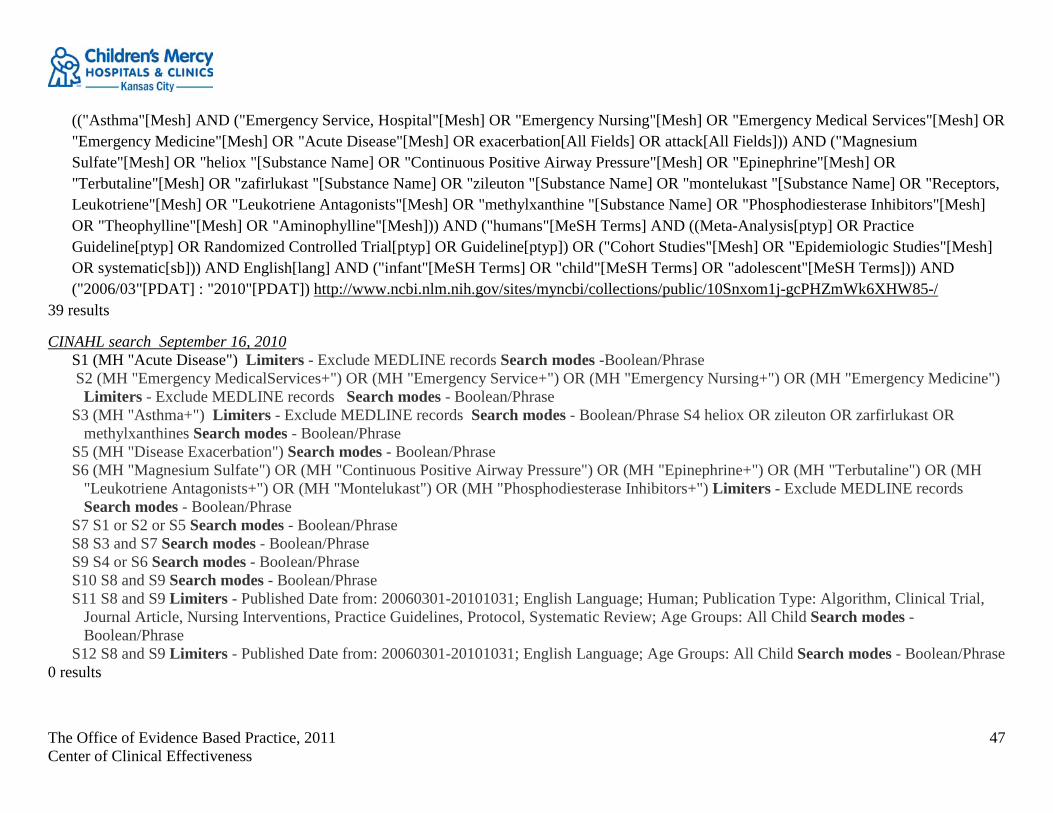
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
47
(("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Magnesium Sulfate"[Mesh] OR "heliox "[Substance Name] OR "Continuous Positive Airway Pressure"[Mesh] OR "Epinephrine"[Mesh] OR "Terbutaline"[Mesh] OR "zafirlukast "[Substance Name] OR "zileuton "[Substance Name] OR "montelukast "[Substance Name] OR "Receptors, Leukotriene"[Mesh] OR "Leukotriene Antagonists"[Mesh] OR "methylxanthine "[Substance Name] OR "Phosphodiesterase Inhibitors"[Mesh] OR "Theophylline"[Mesh] OR "Aminophylline"[Mesh])) AND ("humans"[MeSH Terms] AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp]) OR ("Cohort Studies"[Mesh] OR "Epidemiologic Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms])) AND ("2006/03"[PDAT] : "2010"[PDAT]) http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/10Snxom1j-gcPHZmWk6XHW85-/
39 results
CINAHL search September 16, 2010 S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes -Boolean/Phrase S2 (MH "Emergency MedicalServices+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine")
Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 heliox OR zileuton OR zarfirlukast OR
methylxanthines Search modes - Boolean/Phrase S5 (MH "Disease Exacerbation") Search modes - Boolean/Phrase S6 (MH "Magnesium Sulfate") OR (MH "Continuous Positive Airway Pressure") OR (MH "Epinephrine+") OR (MH "Terbutaline") OR (MH
"Leukotriene Antagonists+") OR (MH "Montelukast") OR (MH "Phosphodiesterase Inhibitors+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase
S7 S1 or S2 or S5 Search modes - Boolean/Phrase S8 S3 and S7 Search modes - Boolean/Phrase S9 S4 or S6 Search modes - Boolean/Phrase S10 S8 and S9 Search modes - Boolean/Phrase S11 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Human; Publication Type: Algorithm, Clinical Trial,
Journal Article, Nursing Interventions, Practice Guidelines, Protocol, Systematic Review; Age Groups: All Child Search modes - Boolean/Phrase
S12 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Age Groups: All Child Search modes - Boolean/Phrase 0 results
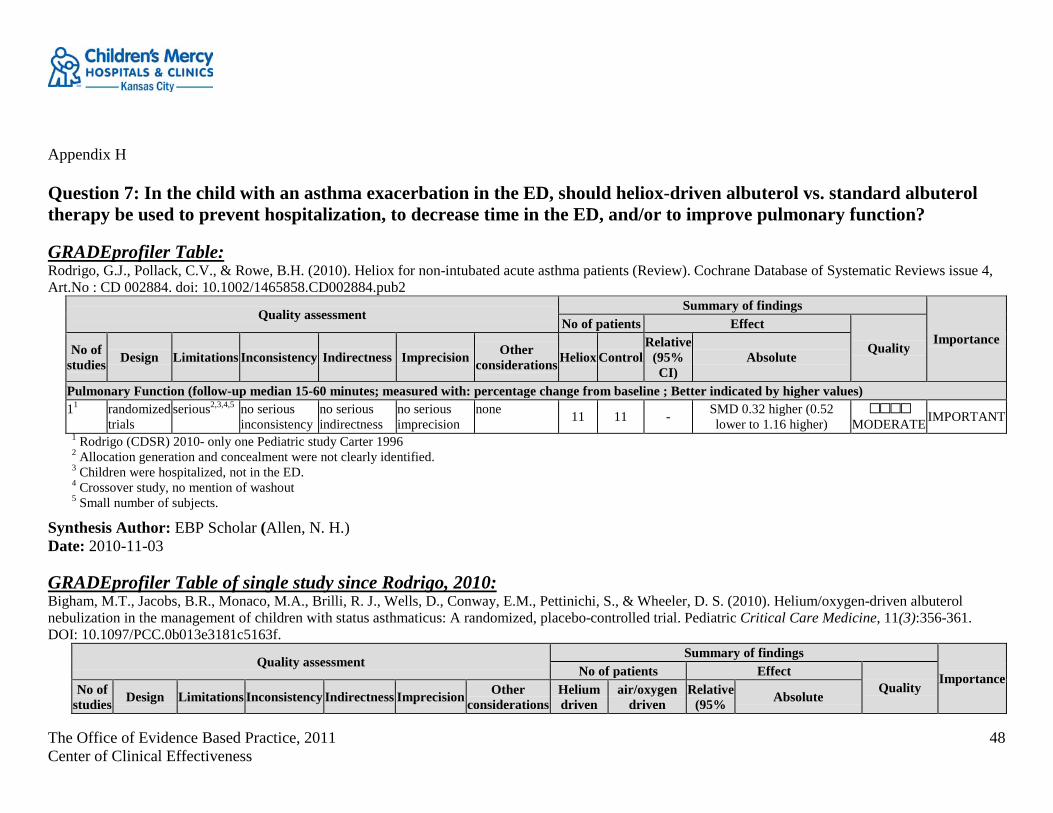
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
48
Appendix H Question 7: In the child with an asthma exacerbation in the ED, should heliox-driven albuterol vs. standard albuterol therapy be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
GRADEprofiler Table: Rodrigo, G.J., Pollack, C.V., & Rowe, B.H. (2010). Heliox for non-intubated acute asthma patients (Review). Cochrane Database of Systematic Reviews issue 4, Art.No : CD 002884. doi: 10.1002/1465858.CD002884.pub2
Quality assessment Summary of findings
Importance No of patients Effect
Quality No of studies Design Limitations Inconsistency Indirectness Imprecision Other
considerations Heliox Control Relative
(95% CI)
Absolute
Pulmonary Function (follow-up median 15-60 minutes; measured with: percentage change from baseline ; Better indicated by higher values) 11 randomized
trials serious2,3,4,5 no serious
inconsistency no serious indirectness
no serious imprecision
none 11 11 - SMD 0.32 higher (0.52 lower to 1.16 higher)
MODERATE IMPORTANT
1 Rodrigo (CDSR) 2010- only one Pediatric study Carter 1996 2 Allocation generation and concealment were not clearly identified. 3 Children were hospitalized, not in the ED. 4 Crossover study, no mention of washout 5 Small number of subjects.
Synthesis Author: EBP Scholar (Allen, N. H.) Date: 2010-11-03
GRADEprofiler Table of single study since Rodrigo, 2010: Bigham, M.T., Jacobs, B.R., Monaco, M.A., Brilli, R. J., Wells, D., Conway, E.M., Pettinichi, S., & Wheeler, D. S. (2010). Helium/oxygen-driven albuterol nebulization in the management of children with status asthmaticus: A randomized, placebo-controlled trial. Pediatric Critical Care Medicine, 11(3):356-361. DOI: 10.1097/PCC.0b013e3181c5163f.
Quality assessment Summary of findings
Importance No of patients Effect Quality No of
studies Design Limitations Inconsistency Indirectness Imprecision Other considerations
Helium driven
air/oxygen driven
Relative (95% Absolute

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
49
albuterol albuterol CI) Hours to discharge (follow-up mean 67 hours; Better indicated by higher values) 11 randomised
trials no serious limitations
no serious inconsistency
serious2 no serious imprecision
none 22 20 - MD 2.8 higher (14.15 lower to 19.75 higher)
MODERATE CRITICAL
Asthma Score at 24 hours (follow-up 24 hours; range of scores: 0-12; Better indicated by lower values) 1 randomised
trials no serious limitations
no serious inconsistency
serious2 no serious imprecision
none 22 20 - MD 0.5 higher (0.44 lower to 1.44 higher)
MODERATE
2 Subjects are hospitalized, not in the ED.
Synthesis Authors: EBP Scholars (Allen, N. H., Bartlett, J., Dusin, J., Gordon, B., Hodges, K., Newman, R., Pirvu, D., & Shubat, S.) Date: 2011-01-25
Forest Plot of Single Studies since Rodrigo (2010) Helium driven albuterol v air/oxygen albuterol, outcome: Time to hospital discharge.
Study or SubgroupBingham 2010
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 0.32 (P = 0.75)
Mean66.2
SD28.16
Total22
22
Mean63.4
SD27.84
Total20
20
Weight100.0%
100.0%
IV, Fixed, 95% CI2.80 [-14.15, 19.75]
2.80 [-14.15, 19.75]
Heliox- Experimental Air/Oxygen- Control Mean Difference Mean DifferenceIV, Fixed, 95% CI
-20 -10 0 10 20Favours control Favours experimental
Helium driven albuterol v air/oxygen albuterol, outcome: Asthma Score at 24 hours.
Study or SubgroupBingham 2010
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 1.04 (P = 0.30)
Mean2.9
SD0.97
Total22
22
Mean2.4
SD1.94
Total20
20
Weight100.0%
100.0%
IV, Fixed, 95% CI0.50 [-0.44, 1.44]
0.50 [-0.44, 1.44]
Heliox- Experimental Air/Oxygen- Control Mean Difference Mean DifferenceIV, Fixed, 95% CI
-1 -0.5 0 0.5 1Favours experimental Favours control
Risk of bias summary figure:

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
50
Ran
dom
seq
uenc
e ge
nera
tion
(sel
ectio
n bi
as)
Bingham 2010 +
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
+
Blin
ding
(per
form
ance
bia
s an
d de
tect
ion
bias
)
+
Inco
mpl
ete
outc
ome
data
(attr
ition
bia
s)
+
Sele
ctiv
e re
porti
ng (r
epor
ting
bias
)
+
Oth
er b
ias
+
Included Single Study Characteristics and Risk of Bias Tables: Bingham 2010
Characteristics of included study: Methods RCT Participants N= 42 children aged 2-21 years of age with moderate to severe status asthmaticus. Interventions Treatment 1: helium powered nebulized albuterol (70% helium/ 30% oxygen mixture). Flow 16 L/min
Treatment 2: air/oxygen powered nebulized albuterol. Flow 10 L/min. Both groups received 15 mg/hour
Outcomes Hospital length of stay; clinical asthma score (CAS) using trained observers; adverse events Notes USA; end point- no need for continuous albuterol or discharge from the hospital. Removed from the study if
invasive or noninvasive respiratory support was needed.
Risk of bias: Bias Authors' judgment Support for judgment

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
51
Random sequence generation (selection bias) Low risk In blocks of five, using a random number generator Allocation concealment (selection bias) Low risk Sealed envelope Blinding (performance bias and detection bias) Low risk Observer was blinded to treatment Incomplete outcome data (attrition bias) Low risk Used intention to treat analysis Selective reporting (reporting bias) Low risk Other bias Low risk
Search Strategy: PubMed search September 16, 2010
(("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Magnesium Sulfate"[Mesh] OR "heliox "[Substance Name] OR "Continuous Positive Airway Pressure"[Mesh] OR "Epinephrine"[Mesh] OR "Terbutaline"[Mesh] OR "zafirlukast "[Substance Name] OR "zileuton "[Substance Name] OR "montelukast "[Substance Name] OR "Receptors, Leukotriene"[Mesh] OR "Leukotriene Antagonists"[Mesh] OR "methylxanthine "[Substance Name] OR "Phosphodiesterase Inhibitors"[Mesh] OR "Theophylline"[Mesh] OR "Aminophylline"[Mesh])) AND ("humans"[MeSH Terms] AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp]) OR ("Cohort Studies"[Mesh] OR "Epidemiologic Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms])) AND ("2006/03"[PDAT] : "2010"[PDAT]) http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/10Snxom1j-gcPHZmWk6XHW85-/
39 results
CINAHL search September 16, 2010 S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes -Boolean/Phrase S2 (MH "Emergency MedicalServices+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine")
Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 heliox OR zileuton OR zarfirlukast OR
methylxanthines Search modes - Boolean/Phrase S5 (MH "Disease Exacerbation") Search modes - Boolean/Phrase S6 (MH "Magnesium Sulfate") OR (MH "Continuous Positive Airway Pressure") OR (MH "Epinephrine+") OR (MH "Terbutaline") OR (MH
"Leukotriene Antagonists+") OR (MH "Montelukast") OR (MH "Phosphodiesterase Inhibitors+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase
S7 S1 or S2 or S5 Search modes - Boolean/Phrase

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
52
S8 S3 and S7 Search modes - Boolean/Phrase S9 S4 or S6 Search modes - Boolean/Phrase S10 S8 and S9 Search modes - Boolean/Phrase S11 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Human; Publication Type: Algorithm, Clinical Trial,
Journal Article, Nursing Interventions, Practice Guidelines, Protocol, Systematic Review; Age Groups: All Child Search modes - Boolean/Phrase
S12 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Age Groups: All Child Search modes - Boolean/Phrase 0 results
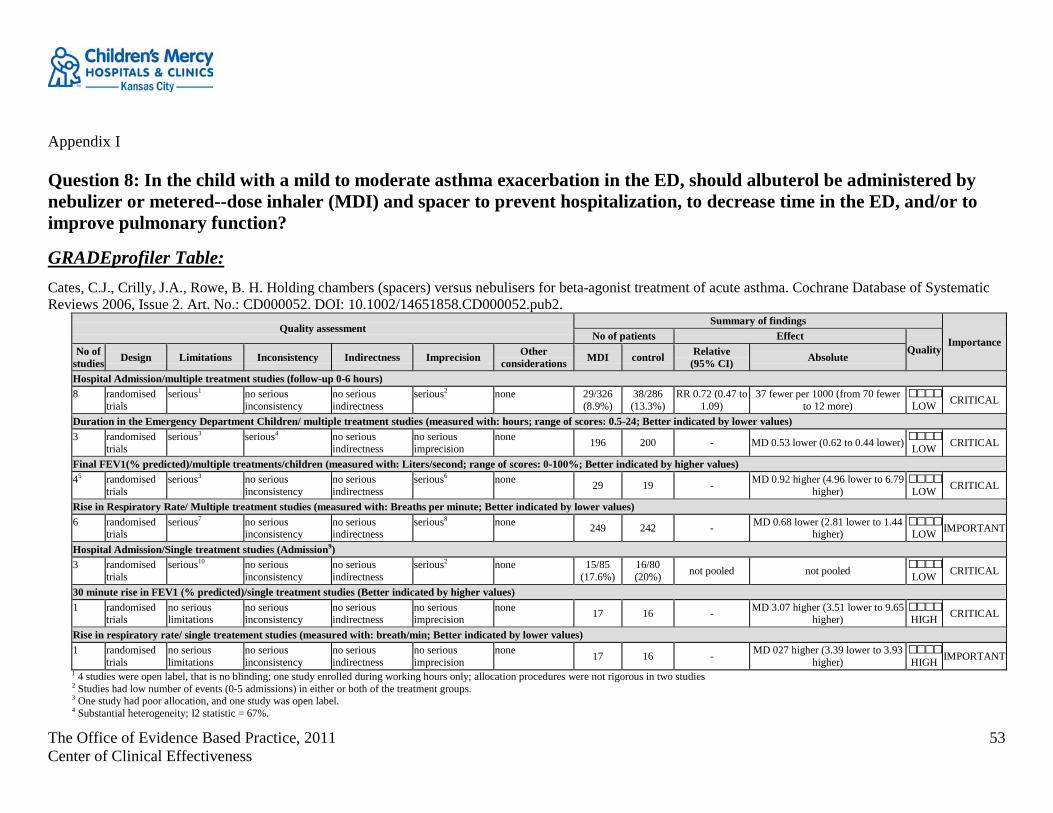
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
53
Appendix I Question 8: In the child with a mild to moderate asthma exacerbation in the ED, should albuterol be administered by nebulizer or metered--dose inhaler (MDI) and spacer to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
GRADEprofiler Table: Cates, C.J., Crilly, J.A., Rowe, B. H. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD000052. DOI: 10.1002/14651858.CD000052.pub2.
Quality assessment Summary of findings
Importance No of patients Effect Quality No of
studies Design Limitations Inconsistency Indirectness Imprecision Other considerations MDI control Relative
(95% CI) Absolute
Hospital Admission/multiple treatment studies (follow-up 0-6 hours) 8 randomised
trials serious1 no serious
inconsistency no serious indirectness
serious2 none 29/326 (8.9%)
38/286 (13.3%)
RR 0.72 (0.47 to 1.09)
37 fewer per 1000 (from 70 fewer to 12 more)
LOW CRITICAL
Duration in the Emergency Department Children/ multiple treatment studies (measured with: hours; range of scores: 0.5-24; Better indicated by lower values) 3 randomised
trials serious3 serious4 no serious
indirectness no serious imprecision
none 196 200 - MD 0.53 lower (0.62 to 0.44 lower) LOW CRITICAL
Final FEV1(% predicted)/multiple treatments/children (measured with: Liters/second; range of scores: 0-100%; Better indicated by higher values) 45 randomised
trials serious3 no serious
inconsistency no serious indirectness
serious6 none 29 19 - MD 0.92 higher (4.96 lower to 6.79 higher)
LOW CRITICAL
Rise in Respiratory Rate/ Multiple treatment studies (measured with: Breaths per minute; Better indicated by lower values) 6 randomised
trials serious7 no serious
inconsistency no serious indirectness
serious8 none 249 242 - MD 0.68 lower (2.81 lower to 1.44 higher)
LOW IMPORTANT
Hospital Admission/Single treatment studies (Admission9) 3 randomised
trials serious10 no serious
inconsistency no serious indirectness
serious2 none 15/85 (17.6%)
16/80 (20%) not pooled not pooled
LOW CRITICAL
30 minute rise in FEV1 (% predicted)/single treatment studies (Better indicated by higher values) 1 randomised
trials no serious limitations
no serious inconsistency
no serious indirectness
no serious imprecision
none 17 16 - MD 3.07 higher (3.51 lower to 9.65 higher)
HIGH CRITICAL
Rise in respiratory rate/ single treatement studies (measured with: breath/min; Better indicated by lower values) 1 randomised
trials no serious limitations
no serious inconsistency
no serious indirectness
no serious imprecision
none 17 16 - MD 027 higher (3.39 lower to 3.93 higher)
HIGH IMPORTANT
1 4 studies were open label, that is no blinding; one study enrolled during working hours only; allocation procedures were not rigorous in two studies 2 Studies had low number of events (0-5 admissions) in either or both of the treatment groups. 3 One study had poor allocation, and one study was open label. 4 Substantial heterogeneity; I2 statistic = 67%.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
54
5 8 from studies from Cates 2009 Cochrane review, Jamalvi 2006, Rotta, 2010 and Vangveervong 2010 6 Small number of subjects in both studies. 7 5 of 6 studies were not blinded. 8 No explanation was provided 9 Studies for this outcome were not pooled, so RR for overall treatment effect was not calculated. The three studies are not methodologically strong; they are inconsistent and imprecise. 10 2 of 3 studies were not blinded.
Synthesis Author: EBP Scholar (Allen, N. H.) Date: 2010-11-03
Synthesis Authors: Evidence Based Scholars (Gutierrez, C., Dusin, J., Hodges, K. & Allen, N. H.) Date: 2010-10-11
Forest Plots of Single Studies since EPR-3 (2007) with the exception of Schuh (1999) MDI with spacer vs. Nebulizer: Outcome Hospitalization
MDI with spacer vs. Nebulizer: Outcome- Respiratory Rate
Study or SubgroupDeerojanawong 2005Jamalvi 2006
Total (95% CI)Heterogeneity: Chi² = 0.00, df = 1 (P = 0.98); I² = 0%Test for overall effect: Z = 0.64 (P = 0.52)
Mean42.6
30
SD14.5
9.2
Total2484
108
Mean43.5
31
SD12.510.9
Total2366
89
Weight15.3%84.7%
100.0%
IV, Fixed, 95% CI-0.90 [-8.63, 6.83]-1.00 [-4.28, 2.28]
-0.98 [-4.01, 2.04]
MDI Nebulizer Mean Difference Mean DifferenceIV, Fixed, 95% CI
-10 -5 0 5 10Favours experimental Favours control
MDI with spacer vs. Nebulizer: Outcome Asthma Score
Study or Subgroup Jamalvi 2006 Rotta 2010 Schuh 1999 Vangveeravong 2008
Total (95% CI) Total events Heterogeneity: Chi² = 1.58, df = 3 (P = 0.66); I² = 0% Test for overall effect: Z = 1.09 (P = 0.28)
Events 4
14 4 1
23
Total 84 25 60 18
187
Events 7
14 2 0
23
Total 66 21 30 18
135
Weight 43.6% 39.1% 14.5%
2.7%
100.0%
M-H, Fixed, 95% CI 0.42 [0.12, 1.51] 0.64 [0.19, 2.12] 1.00 [0.17, 5.79]
3.17 [0.12, 83.17]
0.66 [0.32, 1.39]
MDI Nebulizer Odds Ratio Odds Ratio M-H, Fixed, 95% CI
0.01 0.1 1 10 100 Favors experimental Favors control
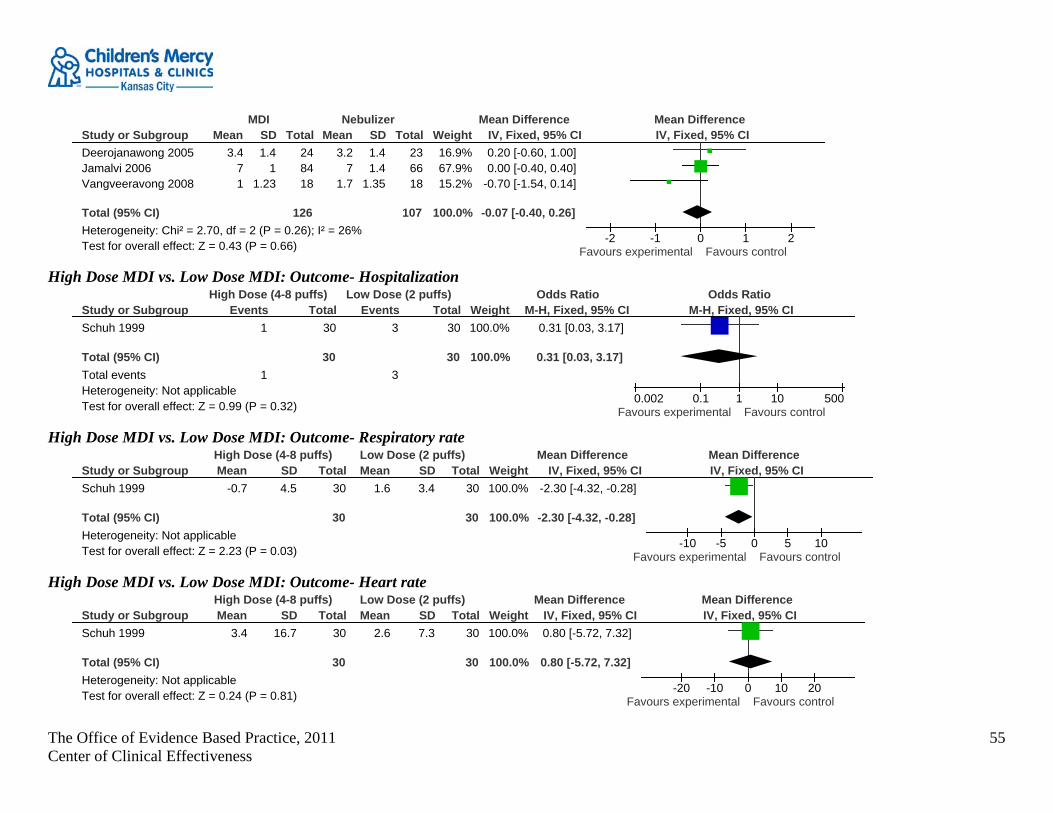
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
55
Study or SubgroupDeerojanawong 2005Jamalvi 2006Vangveeravong 2008
Total (95% CI)Heterogeneity: Chi² = 2.70, df = 2 (P = 0.26); I² = 26%Test for overall effect: Z = 0.43 (P = 0.66)
Mean3.4
71
SD1.4
11.23
Total248418
126
Mean3.2
71.7
SD1.41.4
1.35
Total236618
107
Weight16.9%67.9%15.2%
100.0%
IV, Fixed, 95% CI0.20 [-0.60, 1.00]0.00 [-0.40, 0.40]
-0.70 [-1.54, 0.14]
-0.07 [-0.40, 0.26]
MDI Nebulizer Mean Difference Mean DifferenceIV, Fixed, 95% CI
-2 -1 0 1 2Favours experimental Favours control
High Dose MDI vs. Low Dose MDI: Outcome- Hospitalization
Study or SubgroupSchuh 1999
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.99 (P = 0.32)
Events1
1
Total30
30
Events3
3
Total30
30
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.31 [0.03, 3.17]
0.31 [0.03, 3.17]
High Dose (4-8 puffs) Low Dose (2 puffs) Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.002 0.1 1 10 500Favours experimental Favours control
High Dose MDI vs. Low Dose MDI: Outcome- Respiratory rate
Study or SubgroupSchuh 1999
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 2.23 (P = 0.03)
Mean-0.7
SD4.5
Total30
30
Mean1.6
SD3.4
Total30
30
Weight100.0%
100.0%
IV, Fixed, 95% CI-2.30 [-4.32, -0.28]
-2.30 [-4.32, -0.28]
High Dose (4-8 puffs) Low Dose (2 puffs) Mean Difference Mean DifferenceIV, Fixed, 95% CI
-10 -5 0 5 10Favours experimental Favours control
High Dose MDI vs. Low Dose MDI: Outcome- Heart rate
Study or SubgroupSchuh 1999
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 0.24 (P = 0.81)
Mean3.4
SD16.7
Total30
30
Mean2.6
SD7.3
Total30
30
Weight100.0%
100.0%
IV, Fixed, 95% CI0.80 [-5.72, 7.32]
0.80 [-5.72, 7.32]
High Dose (4-8 puffs) Low Dose (2 puffs) Mean Difference Mean DifferenceIV, Fixed, 95% CI
-20 -10 0 10 20Favours experimental Favours control
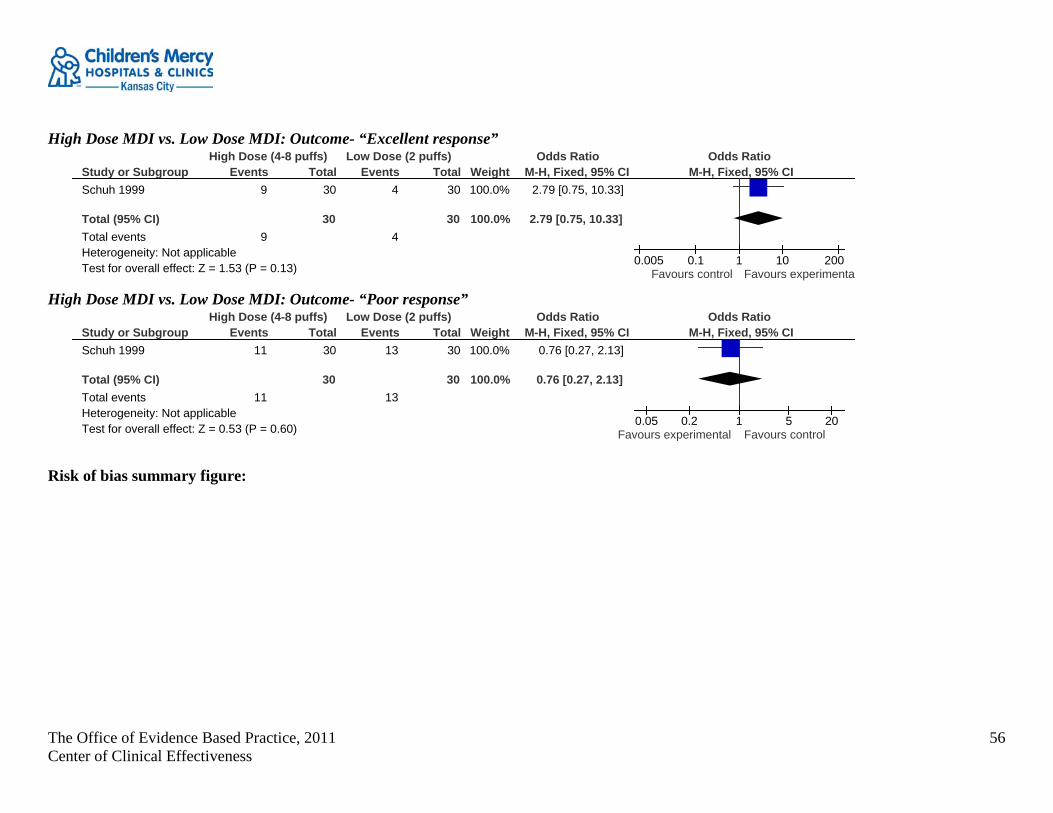
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
56
High Dose MDI vs. Low Dose MDI: Outcome- “Excellent response”
Study or SubgroupSchuh 1999
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.53 (P = 0.13)
Events9
9
Total30
30
Events4
4
Total30
30
Weight100.0%
100.0%
M-H, Fixed, 95% CI2.79 [0.75, 10.33]
2.79 [0.75, 10.33]
High Dose (4-8 puffs) Low Dose (2 puffs) Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.005 0.1 1 10 200Favours control Favours experimenta
High Dose MDI vs. Low Dose MDI: Outcome- “Poor response”
Study or SubgroupSchuh 1999
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.53 (P = 0.60)
Events11
11
Total30
30
Events13
13
Total30
30
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.76 [0.27, 2.13]
0.76 [0.27, 2.13]
High Dose (4-8 puffs) Low Dose (2 puffs) Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.05 0.2 1 5 20Favours experimental Favours control
Risk of bias summary figure:

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
57
Ran
dom
seq
uenc
e ge
nera
tion
(sel
ectio
n bi
as)
Deerojanawong 2005 ?
Doan 2011
Jamalvi 2006 +
Rotta 2010 ?
Schuh 1999 +
Vangveeravong 2008 ?
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
?
?
+
+
?
Blin
ding
(per
form
ance
bia
s an
d de
tect
ion
bias
)
+
?
+
+
?
Inco
mpl
ete
outc
ome
data
(attr
ition
bia
s)
+
+
?
+
+
Sel
ectiv
e re
porti
ng (r
epor
ting
bias
)
+
–
+
+
+
Oth
er b
ias
+
+
+
+
+
Cost study unable to analyze

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
58
Included Single Study Characteristics and Risk of Bias Tables:
Deerojanawong 2005 Characteristics of included study: Methods RCT Participants Children up to 5 years of age. 47 children were studied. Interventions Group 1: two puffs placebo via MDI with spacer followed by 0.15 mg/kg salbutamol respiratory via jet nebulizer
N=23 Group 2: 2 puffs (100 micrograms per puff) of salbutamol via MDI spacer followed by placebo via jet nebulizer. N=24 For each group spacer was actuated into the spacer 30 seconds apart. Patients were allowed to take 5 tidal breaths after each actuation. All patients received 50 mg/kg/ of chloral hydrate 30 minutes prior to the study. Pulmonary function tests were completed 30 minutes after the assigned aerosol treatments.
Outcomes Clinical scores Tidal breathing pulmonary function test Vital signs
Notes Thailand. Nebulizer takes longer and is more expensive?
Risk of bias: Bias Scholars' judgment Support for judgment
Random sequence generation (selection bias) Unclear risk Probably, but does not give details Allocation concealment (selection bias) Unclear risk Probably, but does not give details Blinding (performance bias and detection bias) Low risk Probably, pulmonary testing done by an investigator
who was blinded to treatment. Incomplete outcome data (attrition bias) Low risk Performed power calculation preformed on airway
resistance as the outcome. The calculated sample size was 21 per group.
Selective reporting (reporting bias) Low risk Other bias Low risk

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
59
Doan 2011 Characteristics of included study: Methods Not an RCT: objective of the study was to determine the incremental cost and effects of using MDIs and spacers compared
with wet nebulization in averting hospital admission in children with mild to moderate asthma. Timeframe- ED admission + 2 days
Participants Children enrolled in RCTs in Cates (2006), 2-018 y ears old with acute asthma Interventions Built a decision model between the two treatments. Outcomes Probabilities of admission, ED LOS from a Cochrane review, Cost data obtained from two 3º academic pediatric health centers
in Western Canada-- costs were averaged. Cost analysis and sensitivity analysis done. Notes Not from a patient's perspective, rather from the hospital's perspective. Discharge from hospital is a success; admission for
treatment is a failure.
Risk of bias: Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Unclear risk Difficult to assess bias in this study. Allocation concealment (selection bias) Unclear risk Difficult to assess bias in this study. Blinding (performance bias and detection bias) Unclear risk Difficult to assess bias in this study. Incomplete outcome data (attrition bias) Unclear risk Difficult to assess bias in this study. Selective reporting (reporting bias) Unclear risk Difficult to assess bias in this study. Other bias Unclear risk Difficult to assess bias in this study.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
60
Jamalvi 2006 Characteristics of included study: Methods Cross-sectional study. Participants 150 children > 6 months Interventions Group A: standard dose of beta agonist (salbutamol) by MDI/accessory device (100 microgram/puff) 2 puffs three times per
hour at 20 minute intervals with the help of a one way valve accessory device. Two types of spacers, a mouthpiece spacer for older children and a babyhaler with mask for younger children. (N= 84)
Group B: standard dose of beta agonist (salbutamol) by small volume nebulizer (0.3 mg/kg/ salbutamol solution) Salbutamol solution with 2 ml Normal Saline in one hour with 20 minutes interval with the help of New Nebulizer type 3 Nuova S.P.A. Bresia, Italy (N= 66)
Outcomes Clinical exam Peak Expiratory Flow Rate (PEF) Assessment at 10, 20 minutes and 2 hours. after completion of treatment.
Notes 3 drop outs- no indication of which group they came from
Risk of bias: Bias Scholars’ Judgment Support for judgment
Random sequence generation (selection bias) Low risk But there was not description Allocation concealment (selection bias) Unclear risk No description Blinding (performance bias and detection bias) Unclear risk Not described, but probably not since children used
different equipment Incomplete outcome data (attrition bias) Low risk Selective reporting (reporting bias) High risk Other bias Low risk

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
61
Rotta 2010 Characteristics of included study: Methods RCT Participants Children 1-5 years of age with the diagnosis of acute asthma in the ED Interventions Experimental: salbutamol MDI with spacer 50 microgram per kilo, 1 puff for every 2 kg of body weight. Each dose was
administered 3 times in a one hour period. Control: salbutamol nebulizer 150 microgram per kilo. Each dose was administered 3 times in a one hour period. each patient received 1 mg/kg/ prednisone after the first treatment one blood sample drawn for plasma conc of salbutamol drawn 10 minutes after third treatment
Outcomes Plasma salbutamol concentration <2 years and > 2 years reported as median and interquartile range- cannot use. need for hospitalization
Notes Brazil Exclusion criteria O2 sat < 90% on ambient air, fever > 38 degrees C., signs of cardiac instability, use of beta agonist in 12 prior to ED visit.
Risk of bias: Bias Scholars’ Judgment Support for judgment
Random sequence generation (selection bias) Unclear risk Computer generated, blocks of five, children were "selected by the clinical staff" not certain what this means
Allocation concealment (selection bias) Low risk Medication prepared independent from the care team. Blinding (performance bias and detection bias) Low risk but not described Incomplete outcome data (attrition bias) Low risk Used a pilot study to determine sample size, 46 patients
and 23 in each group. Selective reporting (reporting bias) Low risk Other bias Low risk
Schuh 1999 Characteristics of included study: Methods RCT

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
62
Participants 90 children between 5 and 17 years of age, % predicted FEV1 between 50-79%. Interventions High MDI group 4-8 puffs of albuterol via MDI number of puffs based on weight: < 25 kg 4 puffs, 25-34 kg 6 puffs and > 35
kg 8 puffs Low MDI group 2 puffs albuterol regardless of weight Nebulizer 0.15 mg/kg albuterol (maximum 5 mg) by jet nebulizer.
Outcomes Primary outcome: % predicted FEV1. Secondary outcomes respiratory rate, heart rate, room air oxygen saturation, and accessory muscle score, wheezing score and dyspnea score.
Notes Exclusion criteria- 6000 potential subjects were treated in the ED in the 2.5 year time frame. Exclusion criteria- < 5 years of age, able to perform spirometry, FEV1 < 50% or greater than 80% predicted, first wheezing or bronchodilator treatment, use albuterol within the previous 4 hours, associated medical problem, language barriers, refusal to participate, arrived at the ED outside 0800-2200 when study nurses were available.
Risk of bias: Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk Randomized in the pharmacy using a block randomization schedule and random numbers.
Allocation concealment (selection bias) Low risk Since randomization occurred in the pharmacy, and study drug came up with identical labels, concealment was attained.
Blinding (performance bias and detection bias) Low risk Only the pharmacy knew the allocation. Incomplete outcome data (attrition bias) Low risk Use intent to treat analysis. There was a protocol
violation. 16 subjects received albuterol within 4 hours of being enrolled. High Dose group- 6 subjects, low dose group- 2 subjects and nebulizer group-8 subjects.
Selective reporting (reporting bias) Low risk Report was made on all outcomes. Other bias Low risk
Vangveeravong 2008 Characteristics of included study: Methods RCT multicenter- 7 study sites

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
63
Participants children 5-18 years of age mild to moderate asthma Interventions Group 1 nebulizer- 0.5% Ventolin respiratory solution 0.03 ml/kg/dose (maximum dose 1 ml) diluted with NSS to 3 ml,
delivered via an oxygen-driven flow 6-8 liters per minute. Group 2 MDI with volumatic spacer- MDI spacer, using 6 puffs of Ventolin evohaler (100mg/puff) delivered via volumatic spacer 2 puffs at a time for 3 times. Group 3 DPI Easyhaler- DPI (Easyhaler) using 6 puffs of Buventol Easyhaler (100 mg/puff), 1 puff at a time for 6 times. 3 actuations in an hour
Outcomes Asthma score, Oxygen saturation, vital signs, side effects (tremor, palpitations). Improvement defined at clinical score reduces < 50% form baseline, or clinical score < 3, or a total of 3 treatments. Subjects will be admitted if they failed 3 treatments.
Notes Thailand
Risk of bias: Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Unclear risk no description Allocation concealment (selection bias) Unclear risk no description Blinding (performance bias and detection bias) Unclear risk no description Incomplete outcome data (attrition bias) Low risk Selective reporting (reporting bias) Low risk Other bias Low risk
Author, date, country, and industry of
funding
Patient Group
Level of Evidence (Oxford) Research design Significant results Limitations

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
64
Doan, Q., Shefrin, A., Johnson, D (2011).
Reviewed data from the Cates (2006) Cochrane Systematic Review 2-18 year old with asthma exacerbation in the ED in Canada
2 b Analysis based on clinically sensible costs or alternatives; limited review(s) of the evidence, or single studies: and including multi-way analysis of variance.
Retrospective cost comparison. They built a decision model to measure the incremental cost effectiveness between the 2 methods to deliver albuterol in the ED. Outcomes: considered: Probability of admission, ED LOS, from Cates (2006) Costs: averaged from 2 tertiary pediatric medical centers in western Canada, BC and Alberta. Sensitivity analysis was performed. Assumptions: two treatment schemes were considered, one with ipratropium and one without
Without ipratropium Three to six inhalations (200-1000µg) for MDI/spacer vs. three to six treatments via wet nebulization (2500-5000µg) at 20 minute intervals.
With ipratropium Three treatments of ipratropium bromide 60 to 100g via MDI at 20-minute intervals or nebulized ipratropium administered at 3 treatments of 500 g at 20-minute intervals.
Costs: ED staffing costs Drug and Delivery-Device Costs Hospital Stay Costs
Model Assumptions: Steroids and other medications Human Resource Costs assoc with
treatment delivery Hospital Admission- LOS
The pooled difference in the probability of admission was 0.062 (95% CI: - 0.0043 to 0.1304) which is not significant, but favors the MDI protocol Cost MDI/spacer in the ED
Without ipratropium- Can$262.73, (USD $275.43) With ipratropium- Can$417.68 (USD$437.87)
Net Cost savings- Can$154.95 (USD$162.44) for choosing MDI/Spacer.
Incremental cost effectiveness ratio
Without ipratropium: prevention of hospitalization Can$2499 (USD$2169.77) per admission averted With ipratropium: prevention of hospitalization Can$2226.98 (USD$2334.61)
Retrospective averages of group outcomes such as LOS, treatment doses, and physician fees are separate from ED charges. Canada is a single payer health care system, may differ in the US with private and public payers.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
65
Search Strategies: PubMed search September 24, 2010
("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Metered Dose Inhalers"[Mesh] OR "Nebulizers and Vaporizers"[Mesh]) AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp]) OR ("Cohort Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms]) AND ("2006/03"[PDAT] : "2010"[PDAT])
36 results
CINAHL search September 24, 2010 S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S2 (MH "Emergency Medical Services+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 (MH "Disease Exacerbation") S5 S1 or S2 or S4 Search modes - Boolean/Phrase Search modes - Boolean/Phrase S6 S3 and S5 Search modes - Boolean/Phrase S7 (MH "Nebulizers and Vaporizers") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S8 multi dose inhaler Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S9 multi dose inhalers Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S10 S6 and S7 Search modes - Boolean/Phrase S11 S6 and S7 Limiters - Published Date from: 20060301-20101031; English Language; Human; Age Groups: All Child Search modes - Boolean/Phrase
3 results

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
66
Appendix J Question 9: In the child with an asthma exacerbation in the ED should prednisolone/prednisone vs. dexamethasone be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Forest Plots Oral dexamethasone vs. 5 day oral prednisone, Outcome: Length of Stay in ED (hrs).
Study or SubgroupAltamimi 2006
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 1.34 (P = 0.18)
Mean3.5
SD1.93
Total56
56
Mean4.3
SD3.97
Total54
54
Weight100.0%
100.0%
IV, Fixed, 95% CI-0.80 [-1.97, 0.37]
-0.80 [-1.97, 0.37]
Dex single dose Pred- 5 day course Mean Difference Mean DifferenceIV, Fixed, 95% CI
-4 -2 0 2 4Favours experimental Favours control
Oral dexamethasone vs. 5 day oral prednisone, outcome: Hospital admission.
Study or SubgroupAltamimi 2006
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.90 (P = 0.37)
Events6
6
Total56
56
Events9
9
Total54
54
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.60 [0.20, 1.82]
0.60 [0.20, 1.82]
Dex single dose Pred- 5 day course Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.02 0.1 1 10 50Favours experimental Favours control
Oral dexamethasone vs. 5 day oral prednisone, outcome: PEF at discharge.
Study or SubgroupAltamimi 2006
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 0.75 (P = 0.45)
Mean275
SD70.04
Total9
9
Mean241
SD86.18
Total5
5
Weight100.0%
100.0%
IV, Fixed, 95% CI34.00 [-54.32, 122.32]
34.00 [-54.32, 122.32]
Dex single dose Pred- 5 day course Mean Difference Mean DifferenceIV, Fixed, 95% CI
-200 -100 0 100 200Favours control Favours experimental
Oral Dexamethasone vs. Oral Prednisone, outcome: Unscheduled follow up appointment(s).

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
67
Study or SubgroupAltamimi 2006Greenberg 2008
Total (95% CI)Total eventsHeterogeneity: Chi² = 0.06, df = 1 (P = 0.81); I² = 0%Test for overall effect: Z = 1.91 (P = 0.06)
Events48
12
Total5626
82
Events13
4
Total5423
77
Weight30.0%70.0%
100.0%
M-H, Fixed, 95% CI4.08 [0.44, 37.70]2.96 [0.68, 12.91]
3.30 [0.97, 11.22]
Dexamethasone Prednisone Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours experimental Favours control
Synthesis Authors: EBP Scholars (Allen, N. H., Carlson, E., Dusin, J., Gutierrez, C., Hodges, K., & Pirvu, D.) Date: 10/21/2011
Risk of bias summary figure:
Ran
dom
seq
uenc
e ge
nera
tion
(sel
ectio
n bi
as)
Altamimi 2006 +
Greenberg 2008 ?
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
+
+
Blin
ding
(per
form
ance
bia
s an
d de
tect
ion
bias
)
+
+
Inco
mpl
ete
outc
ome
data
(attr
ition
bia
s)
–
+
Sel
ectiv
e re
porti
ng (r
epor
ting
bias
)
+
Oth
er b
ias
–
+
Included Single Study Characteristics and Risk of Bias Tables:

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
68
Altamimi 2006 Characteristics of included study:
Methods Randomization: prepared sealed randomization cards, prepared the cards, as well as the study drugs. Blinding: medications were made to look and taste the same. Excluded: Withdrawals: 2 patients vomited in the ED; for the five day follow up 9 in the dexamethasone group and 13 in the prednisone group were admitted or lost to follow up. Baseline characteristics:110 subjects enrolled, 56 in dexamethasone group and 54 in the prednisone group. Similar base line characteristics. Per protocol analysis Power calculation: non-inferiority was accepted if single dose oral dexamethasone was no worse that 1 extra day. Chose a small beta of 0.05 d/t non-inferiority. Power calc= 134 or 67 in each group.
Participants Setting: British Columbia CANADA urban ED. Inclusion Criteria: children 2-16 in the ED with mild to moderate asthma, with at least one episode of "asthma like" symptoms. Defined mild to moderate with a Pulmonary Index Score (PIS) of < 9 and a PEF of 60% or more of predicted value for height Exclusion Criteria: signs and symptoms of severe asthma ( PEF less than 60% predicted for height. PIS > 10, compete recovery after first salbutamol treatment, use of oral steroids over the the last 2 weeks
Interventions Group A: ED medication-0.6 mg/kg of dexamethasone in 1 ml/kg, Discharge medication: Placebo Group B: ED medication: 1 mg/kg prednisone in 1 ml/kg Discharge medication: 1 mg/kg prednisone per dose
Outcomes Primary outcome: number of days needed for asthma score to return to baseline or PEF to return to 80% predicted for height Secondary: short term improvement in PEF asthma score at the time of discharge from the ED, actual time to discharge, number of salbutamol therapies needed in the ED, initial admission rate, number of salbutamol therapies given at home, return to the ED, need for admission after initial discharge and improvement in asthma score on day 5.
Risk of bias: Bias Authors' judgment Support for judgment
Random sequence generation (selection bias) Low risk Allocation concealment (selection bias) Low risk

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
69
Blinding (performance bias and detection bias) Low risk Incomplete outcome data (attrition bias) High risk They powered the study for 67 enrolled in each group, but had
inherent drop out points. Did not meet power at time of analysis Selective reporting (reporting bias) Low risk Other bias High risk competing nurse project initiated nursing guideline implemented
at the same time as the study started, patients were quickly treated with beta agonists and oral steroids prior to study enrollment
Greenberg 2008 Characteristic of included study: Methods Randomization: Block randomization < 7 years and > 7 years,
Blinding: pharmacy prepared drugs to look identical as a white powder capsule. Excluded: children who were admitted, lost to follow-up, or vomited study drug twice. 9 subjects were excluded for unknown reasons. Excluded patients had higher PAS, but admission was a criterion for exclusion. Withdrawals: Baseline characteristics: There were more Caucasians in the Dexamethosone group and more "others" in the prednisone group Intention to treat: Power calculation:
Participants Children 2-18 years of age with a history of asthma ( 2 or more episodes of wheezing treated with Beta agonists. Urban tertiary ED Inclusion Criteria Exclusion Criteria the use of oral steroids in the past month; history of intubation for a previous asthma exacerbation; varicella exposure in the past 3 weeks; possible foreign body aspiration; any chronic lung disease (e.g., cystic fibrosis) that would affect the patient’s management; chronic heart, liver, or kidney disease; significant respiratory distress necessitating airway intervention (e.g., intubation); previous enrollment in this study; no telephone for follow-up; and ≥2 episodes of emesis after steroid administration in the ED.
Interventions Experimental: 2 doses of oral dexamethasone 0.6 mg/kg, maximum dose 16 mg- rounded to nearest 2 mg. Control: 5 day course of oral prednisone 2 mg/kg, maximum dose 80 mg. rounded to the nearest 5 mg.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
70
Outcomes Primary: relapse in 10 days Secondary: vomiting in the ED
Risk of bias: Bias Authors' judgment Support for judgment
Random sequence generation (selection bias) Unclear risk They used block randomization, but do say how. Allocation concealment (selection bias) Low risk Blinding (performance bias and detection bias) Low risk All received 5 pills to take one per day. In the
dexamethasone group, only one pill had study drug. In the prednisone group, all pills had study drug.
Incomplete outcome data (attrition bias) Low risk Selective reporting (reporting bias) Unclear risk Other bias Low risk
Search Strategies:
PubMed search Sept 23, 2010 (("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND (("Dexamethasone"[Mesh] OR "Dexamethasone Isonicotinate"[Mesh] OR "Methylprednisolone"[Mesh] OR "Methylprednisolone Hemisuccinate"[Mesh] OR "Prednisolone"[Mesh] OR "Prednisone"[Mesh] OR "Hydrocortisone"[Mesh]) AND ("Injections, Intramuscular"[Mesh] OR "Administration, Oral"[Mesh] OR "Infusions, Intravenous"[Mesh] OR "Injections, Intravenous"[Mesh] OR "administration and dosage "[Subheading]))) AND (((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp] OR Comparative Study[ptyp]) OR ("Cohort Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms]) AND ("2006/03"[PDAT] : "2010"[PDAT])) http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/1HidMRUlNvAzvk-zGa6rC1UQ6/
16 results
CINAHL search Sept 23, 2010 S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
71
S2 (MH "Emergency Medical Services+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase
S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 (MH "Disease Exacerbation") Search modes - Boolean/Phrase S5 S1 or S2 or S4 Search modes - Boolean/Phrase S6 S3 and S5 Search modes - Boolean/Phrase S7 (MH "Dexamethasone") OR (MH "Methylprednisolone") OR (MH "Prednisolone+") OR (MH "Prednisone") OR (MH "Hydrocortisone")
Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S8 dexamethasone isonicotinate OR Methylprednisolone hemisuccinate Limiters - Exclude MEDLINE records Search modes -
Boolean/Phrase S9 (MH "Injections, Intramuscular+") OR (MH "Administration, Oral+") OR (MH "Infusions, Intravenous") OR (MH "Injections,
Intravenous") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S10 S7 or S8 Search modes - Boolean/Phrase S11 S6 and S9 and S10 Search modes - Boolean/Phrase S12 S6 and S9 and S10 Limiters - Published Date from: 20060301-20101031; English Language; Age Groups: All Child Search modes -
Boolean/Phrase 0 results

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
72
Appendix K Question 10: In the child with an asthma exacerbation in the ED, should inhaled steroids be initiated during an asthma exacerbation to prevent hospitalization, to decrease time in the ED, to improve pulmonary function, and/or to prevent repeat evaluations in the ED or by other health care providers?
Forest Plots of Single Studies since EPR-3 (2007) Flunisolide v. budesonide, Outcome- Lung function.
Study or SubgroupDecimo 2009
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 1.96 (P = 0.05)
Mean5.041
SD1.4
Total20
20
Mean5.91
SD1.4
Total20
20
Weight100.0%
100.0%
IV, Fixed, 95% CI-0.87 [-1.74, -0.00]
-0.87 [-1.74, -0.00]
flunisolide budesonide Mean Difference Mean DifferenceIV, Fixed, 95% CI
-10 -5 0 5 10Favours control Favours experimental
Single dose 2000 mcg vs. repeated dose 500 mcg X 4 doses budesonide-Outcome-FEV1 at 90 minutes.
Study or SubgroupRazi 2008
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 1.09 (P = 0.28)
Mean19.9
SD14.77
Total20
20
Mean15
SD13.66
Total20
20
Weight100.0%
100.0%
IV, Fixed, 95% CI4.90 [-3.92, 13.72]
4.90 [-3.92, 13.72]
Single Dose 2000 mcg Repeated Dose 500 mcg X 4 Mean Difference Mean DifferenceIV, Fixed, 95% CI
-100 -50 0 50 100Favours control Favours experimental
Fluticasone v. budesonide, Outcome- Good response to treatment 4 day protocol.
Study or SubgroupVolovitz 2008
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.25 (P = 0.21)
Events63
63
Total72
72
Events16
16
Total21
21
Weight100.0%
100.0%
M-H, Fixed, 95% CI2.19 [0.64, 7.43]
2.19 [0.64, 7.43]
fluticasone budesonide Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours experimental Favours control

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
73
Forest Plots of Single Studies: Citations from Rodrigo, 2006 Budesonide versus Placebo, Outcome- Rescue Inhalations
Study or SubgroupMilani 2004
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.61 (P = 0.54)
Events5
5
Total17
17
Events3
3
Total15
15
Weight100.0%
100.0%
M-H, Fixed, 95% CI1.67 [0.32, 8.59]
1.67 [0.32, 8.59]
Oral Prednisone Placebo Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours experimental Favours control
Budesonide v. Placebo, Outcome- FEV1 after treatment.
Budesonide v Placebo, Outcome- FEV1 improvement on Day 6
Study or SubgroupSekerel 2005
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 1.20 (P = 0.23)
Mean9.1
SD0.68
Total33
33
Mean8.9
SD0.68
Total34
34
Weight100.0%
100.0%
IV, Fixed, 95% CI0.20 [-0.13, 0.53]
0.20 [-0.13, 0.53]
Budesonide Control Mean Difference Mean DifferenceIV, Fixed, 95% CI
-1 -0.5 0 0.5 1Favours control Favours experimental
Nebulized budesonide vs. placebo, Outcome- Pulmonary Score by PIS.
Study or SubgroupSekerel 2005
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 1.19 (P = 0.24)
Mean5.5
SD7.94
Total33
33
Mean3.2
SD7.94
Total34
34
Weight100.0%
100.0%
IV, Fixed, 95% CI2.30 [-1.50, 6.10]
2.30 [-1.50, 6.10]
Budesonide Placebo Mean Difference Mean DifferenceIV, Fixed, 95% CI
-20 -10 0 10 20Favours control Favours experimental
Study or SubgroupNohoglu 2005
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 1.03 (P = 0.30)
Mean2.25
SD0.87
Total12
12
Mean2.71
SD1.38
Total14
14
Weight100.0%
100.0%
IV, Fixed, 95% CI-0.46 [-1.33, 0.41]
-0.46 [-1.33, 0.41]
Experimental Control Mean Difference Mean DifferenceIV, Fixed, 95% CI
-2 -1 0 1 2Favours control Favours experimental

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
74
Nebulized budesonide vs. placebo, Outcome-PEFR.
Study or SubgroupNohoglu 2005
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 0.88 (P = 0.38)
Mean222.5
SD40.48
Total12
12
Mean240.71
SD64.03
Total14
14
Weight100.0%
100.0%
IV, Fixed, 95% CI-18.21 [-58.82, 22.40]
-18.21 [-58.82, 22.40]
Experimental Control Mean Difference Mean DifferenceIV, Fixed, 95% CI
-100 -50 0 50 100Favours control Favours experimental
Forest Plots of Budesonide versus Oral Steroid Budesonide vs. Prednisone, Outcome- Rescue Inhalations.
Study or SubgroupMilani 2004
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.24 (P = 0.22)
Events2
2
Total17
17
Events5
5
Total17
17
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.32 [0.05, 1.95]
0.32 [0.05, 1.95]
Budesonide Prednisone- oral Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours experimental Favours control
Nebulized budesonide vs. oral prednisolone, Outcome Hospitalization.
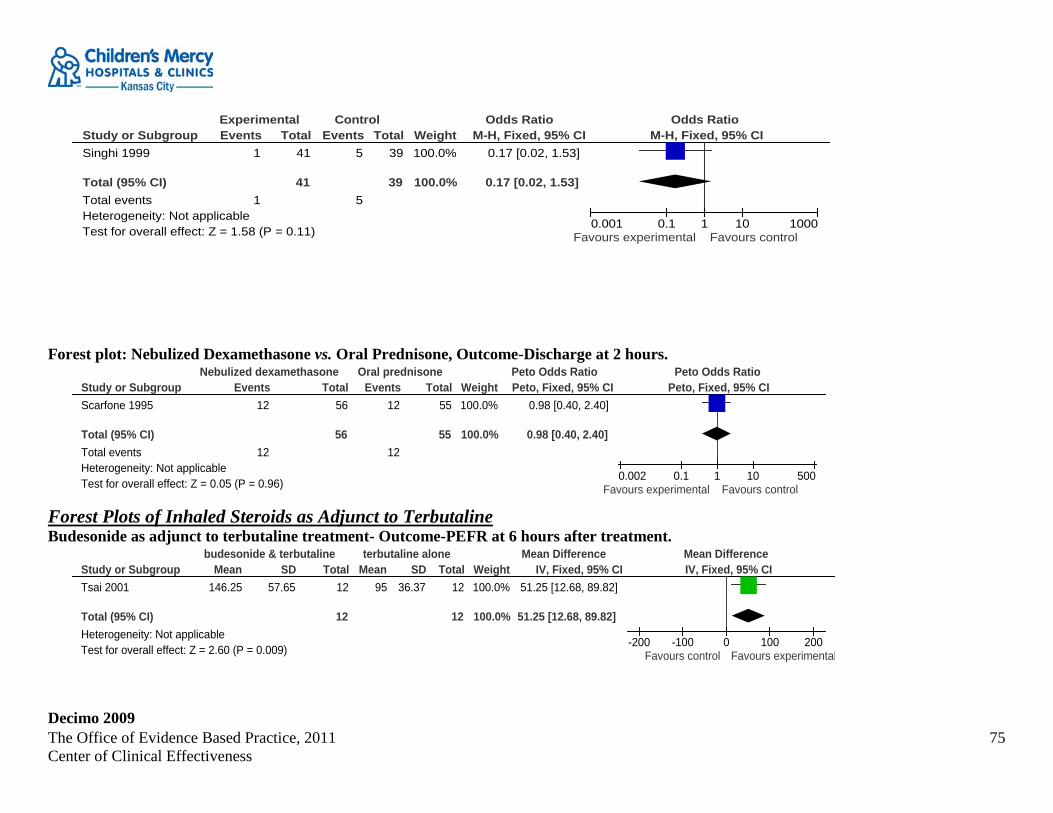
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
75
Study or SubgroupSinghi 1999
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.58 (P = 0.11)
Events1
1
Total41
41
Events5
5
Total39
39
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.17 [0.02, 1.53]
0.17 [0.02, 1.53]
Experimental Control Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.001 0.1 1 10 1000Favours experimental Favours control
Forest plot: Nebulized Dexamethasone vs. Oral Prednisone, Outcome-Discharge at 2 hours.
Study or SubgroupScarfone 1995
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.05 (P = 0.96)
Events12
12
Total56
56
Events12
12
Total55
55
Weight100.0%
100.0%
Peto, Fixed, 95% CI0.98 [0.40, 2.40]
0.98 [0.40, 2.40]
Nebulized dexamethasone Oral prednisone Peto Odds Ratio Peto Odds RatioPeto, Fixed, 95% CI
0.002 0.1 1 10 500Favours experimental Favours control
Forest Plots of Inhaled Steroids as Adjunct to Terbutaline Budesonide as adjunct to terbutaline treatment- Outcome-PEFR at 6 hours after treatment.
Study or SubgroupTsai 2001
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 2.60 (P = 0.009)
Mean146.25
SD57.65
Total12
12
Mean95
SD36.37
Total12
12
Weight100.0%
100.0%
IV, Fixed, 95% CI51.25 [12.68, 89.82]
51.25 [12.68, 89.82]
budesonide & terbutaline terbutaline alone Mean Difference Mean DifferenceIV, Fixed, 95% CI
-200 -100 0 100 200Favours control Favours experimental
Decimo 2009

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
76
Characteristic of included study: Methods randomized parallel group Participants 46 subjects between 3-5 years Interventions Group one: nebulized flunisolide 40 micrograms/kg twice daily for 7 days and 20 micrograms/kg twice daily for 14 days.
Group two: budesonide 0.5 mg twice daily for 7 days then 0.25 mg twice daily for 15 days. Inhaled salbutamol (MDI + spacer) 200 micrograms 4 times daily was administered during the first 3 days of the study and then as needed.
Outcomes Air resistance as measured by forced oscillation technique (FOT) before and after inhalation of salbutamol (200 micrograms) Symptoms symptom score Drug use- use of rescue salbutamol, systemic corticosteroids, morning serum cortisol concentration Measured on T0, T7, and T21 days
Notes Forty children finished the study. Reasons given for non finishers, but not included in analysis. Graph only analysis for symptom score and use of rescue medications.
Risk of bias table Bias Scholars' judgment Support for judgment
Random sequence generation (selection bias) Unclear risk not stated Allocation concealment (selection bias) High risk Blinding (performance bias and detection bias) High risk "Simple blind" not certain what this means; only parents and
patients were blinded? Incomplete outcome data (attrition bias) High risk All outcomes Incomplete outcome data (attrition bias)
Unclear risk All outcomes; 6 subjects did not complete the trial. Reasons for not completing were given, but subjects were not included in the analysis
Selective reporting (reporting bias) Low risk Other bias Low risk
Milani 2004 Characteristic of included study: Methods Randomized double-blind, double-dummy and placebo-controlled clinical trial.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
77
Participants 49 children aged 2 to 7 years with acute asthma who sought treatment at a Pediatric Walk-in Clinic. Interventions After receiving nebulized salbutamol (0.15 mg/kg),
Group I: received placebo both as tablets and nebulization, Group II: was treated with a single dose of oral prednisone (1 mg/kg) and inhaled placebo Group III received a single dose of placebo tablet and nebulized budesonide (2 mg). Nebulized salbutamol was repeated in case of increasing symptom score or lower saturation.
Outcomes Patients were evaluated in terms of symptom score and transcutaneous hemoglobin saturation. Notes The objective of this study was to evaluate the efficacy of budesonide suspension, prepared for inhalation in 2 mg single doses,
as an auxiliary treatment to inhaled ß2, compared with single-dose oral prednisone for patients in acute asthma crises.
Risk of bias table Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Unclear risk Randomization not explained. Allocation concealment (selection bias) Low risk Blinding (performance bias and detection bias) Low risk Incomplete outcome data (attrition bias) High risk All outcomes; Did not adequately explain why some patients
did not complete the study. Incomplete outcome data (attrition bias) Low risk All outcomes Selective reporting (reporting bias) Low risk Other bias Low risk
Nohoglu 2005 Characteristic of included study:
Methods Double blind, placebo controlled study. Patients who attended the pediatric emergency unit due to an acute attack of asthma over a six month period were evaluated for the study. At the admittance ages, usage of an inhaled prophylactic steroid was documented for each patient.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
78
Participants Children 5-15 years with acute asthma. Interventions All received salbutamol 3 doses (0.15 mg/kg/dose) and methylprednisolone 1 mg/kg/dose IM then randomized to
Group 1: nebulized budesonide (1 mg/dose) Group 2: Placebo
Outcomes PEFR Pulmonary Score as measured by PIS
Notes it is a very small study (they only had 12-14 patients in each group)
Risk of bias table Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) High risk generated by social security number, odd and even numbers Allocation concealment (selection bias) High risk based on social security number, so all new which group
subject would be assigned Blinding (performance bias and detection bias) Unclear risk they stated but they did not explain Incomplete outcome data (attrition bias) All outcomes
Low risk
Incomplete outcome data (attrition bias) All outcomes
Low risk
Selective reporting (reporting bias) Low risk They report 25 subjects, but report on 26. Not sure if it is just a typo
Other bias Low risk
Razi 2008 Characteristic of included study: Methods Randomized double blind parallel group study design. for the first 90 minutes after admission Participants children 7-16 years with moderate or severe acute asthma Interventions Experimental: Single nebulized dose of 2000 micrograms budesonide n= 20
Control: repeated nebulized doses of 400 micrograms budesonide each n=20 Same total dose in each group. All children received a 2.5-5 mg dose of salbutamol every 20 minutes for 4 doses just before every study drug administration.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
79
Outcomes at 90 minutes FEV1 % predicted, asthma score, Notes Exclusions: patients receiving more than 400 micrograms of inhaled budesonide or equivalent per day or any change in the dose
of ICS in the past 2 months or had taken systemic steroids within the past 2 months. Patients with life threatening asthma attack, concurrent pneumonia or any other chronic illness, previous intensive care unit admission or hospitalizations for asthma in the previous 3 months. Asthma score is measured at median and Interquartile range, not included. Country of Origin: Turkey
Risk of bias table: Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk Computer generated. Allocation concealment (selection bias) Low risk Blinding (performance bias and detection bias) Low Study medications prepared in pharmacy and sent study drug
to the ED in identical packaging. Incomplete outcome data (attrition bias) All outcomes
Low risk All completed the study.
Incomplete outcome data (attrition bias) All outcomes
Low risk
Selective reporting (reporting bias) Low risk Other bias Low risk
Scarfone 1995 Characteristic of included study: Methods A randomized, double-blind, double-placebo study. Participants Patients aged 1 to 17 years with moderate acute asthma exacerbation. Interventions Group 1 aerosolized albuterol and either 1.5 mg/kg of
nebulized dexamethasone or Group 2:aerosolized albuterol 2 mg/kg of oral prednisone
Outcomes Hospitalization rates Degree of clinical improvement, measured by pulmonary index (score) and oxygen saturation numbers.
Notes

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
80
Risk of bias table: Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk Allocated randomly in blocks of 10 to the lactose/dexamethasone or the prednisone/saline solution group.
Allocation concealment (selection bias) Low risk Blinding (performance bias and detection bias) Low risk Incomplete outcome data (attrition bias) Low risk All outcomes Incomplete outcome data (attrition bias) Low risk All outcomes Selective reporting (reporting bias) Low risk Other bias Low risk
Sekerel 2005 Characteristic of included study: Methods Randomized, double-blind, placebo-controlled parallel-group clinical trial Participants Children 6 to 15 y who presented for an unscheduled visit with mild to moderate asthma exacerbation.
After three nebulized salbutamol treatments, children with mild to moderate obstruction (basal FEV1 between 70 and 90% of personal best) and those who met the inclusion/exclusion criteria were considered for enrolment.
Interventions All children were treated with nebulized salbutamol solution at a dose of 0.15 mg/kg (max. 5 mg) every 20 min for three doses. Twenty minutes after the third dose of salbutamol, spirometry was performed to determine basal FEV1.
Treatment group: three doses of budesonide (1 mg/2 ml) with salbutamol (0.15 mg/kg/ dose, max. 5 mg) every hour,
Control group: normal saline (2 ml) as well as salbutamol (0.15 mg/kg/ dose, max. 5 mg) every hour.
Thirty minutes after the last dose of study medication, FEV1 and physical examination were re-evaluated in order to determine the short-term effects of nebulized budesonide.
Outcomes The primary outcome measure was to evaluate whether nebulized CS therapy could decrease the need for systemic CS intervention. Secondary outcomes considered included forced expiratory volume in 1 s (FEV1), peak expiratory flow rates (PEFRs), rescue b-2 agonist use and hospitalization.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
81
Notes
Risk of bias table Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk Randomized in blocks of six Allocation concealment (selection bias) Low risk The randomization list was concealed in sealed opaque envelopes until
data analysis was performed. Blinding (performance bias and detection bias) Low risk Incomplete outcome data (attrition bias) Low risk All outcomes; Initial lung functions were assessed in only 64 of 67,
since in three, according to the decision of the evaluating physician, their condition required immediate beta-2-agonist inhalation.
Incomplete outcome data (attrition bias) Low risk All outcomes Selective reporting (reporting bias) High risk Comparison of the proportions of hospitalizations showed no significant
difference between the groups ( p>0.05), however the number of patients in these groups is not reported.
Other bias Low risk
Singhi 1999 Characteristic of included study: Methods Randomized double-blind, double placebo-controlled trial Participants Eighty children, 2 - 12 years acute moderate asthma. 39 in the prednisolone group and 41 in the budesonide group. Study
occurred India Interventions Group one: received O2 (6–10 lpm), nebulized salbutamol (0.5% solution, 0.15 mg/kg diluted 1:2 with normal saline), placebo
nebulization and oral prednisolone (prednisolone group). Group two: was assigned to receive O2, nebulized salbutamol, nebulized budesonide (800 mg) and oral placebo tablets (budesonide group). Salbutamol and budesonide/placebo nebulization was given at admission and at half-hourly intervals for three doses. The nebulization were given with the help of a Micromist1 nebulizer chamber (Hudson RCI) using a mask and oxygen at the rate of 8/lpm from a wall mounted oxygen source. Prednisolone (2 mg/kg/day rounded off to the nearest 5 mg) or placebo tablets was given as a single dose at admission immediately prior to nebulization.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
82
Outcomes Effect of drug regimens as evidenced by: mean RR, HR, pulsus paradoxus, PI, RDA score, SaO2 and PEFR. Requirements of intravenous steroids, hospitalization evidenced by time to full recovery from acute episode after three nebulization treatments; and/or hospitalization. PEFR could be monitored in 20 patients in the prednisolone group and 24 in the budesonide group.
Notes
Risk of bias table Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk Children were randomized to one of the two treatment groups based on previously allotted random numbers.
Allocation concealment (selection bias) Low risk Packets containing either budesonide solution and placebo tablets or placebo solution and prednisolone tablets were prepared and numbered beforehand. Placebo solution contained saline, which was stored in translucent vials of the same size and color as budesonide solution. Placebo tablets contained lactose and were of same size and color as prednisolone tablets (5 mg/tablet). These were dispensed in identical packets containing a minimum of eight tablets each.
Blinding (performance bias and detection bias) Low risk Preparation and administration of nebulization solution and dispensing of tablets was done by a staff nurse. Evaluation of patient before and after treatment was done by one of the authors (DD), who was unaware of the patient assignment and drugs received.
Incomplete outcome data (attrition bias) Unclear risk All outcomes 80 kids were randomized. Prednisolone n =39: 19 x 2-5 year olds and 20 x 6-12 year olds and Budesonide n= 41: 16 x 2-5 year olds and 25 x 6-12 year olds. PEFR could be monitored in 20 patients in the prednisolone group and 24 in the budesonide group. The authors do not say which age groups exactly could be monitored.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
83
Incomplete outcome data (attrition bias) Unclear risk All outcomes; Not stated Selective reporting (reporting bias) Unclear risk Not stated Other bias Unclear risk Not stated
Sung 1998 Characteristic of included study: Methods Randomized, controlled, double-blind trial with parallel design. Participants Children 6 months to 18 years with a moderate to severe exacerbation of asthma Interventions Treatment: 2000 micrograms (4ml) of nebulized budesonide or Placebo: 4 ml of nebulized normal saline.
Both groups received regular nebulized salbutamol at 0.15 mg/kg of body weight (maximum 5 mg) with 2 ml of normal saline every 30 minutes for 3 doses. then hourly for 4 doses. Both groups were given a single oral dose of prednisone of 1 mg/kg/(maximum of 50 mg) and supplemental oxygen to maintain O2 sat > 92%
Outcomes Asthma Score: Pulmonary Index Score. Notes Canada
Risk of bias table Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk Allocation concealment (selection bias) Low risk Blinding (performance bias and detection bias) Low risk Incomplete outcome data (attrition bias) Low risk All outcomes Incomplete outcome data (attrition bias) Low risk All outcomes Selective reporting (reporting bias) Low risk Other bias Low risk
Tsai 2001 Characteristic of included study: Methods Randomized, double-blinded, placebo-controlled trial Participants 30 children initially with asthma & confirmed allergic to Dermatophagoides pteronyssinus between the ages of 6 & 17 attending

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
84
ED; 24 subjects completed study (12 control/12 experimental) Interventions Treatment: terbutaline & budesonide together -0.1 mg/kg per dose terbutaline in combination with 0.05 mg/kg max 2 mg
budesonide in 3 ml isotonic sodium chloride solution on enrolment, followed by terbutaline nebulization alone for 6 hours after initial treatment. Control: subjects received either terbutaline alone @ 0.1 mg/kg dose in 3 ml isotonic sodium chloride solution every 6 hours for 2 doses or 12 hour follow up
Outcomes The PEFR (peak expiratory flow rate) and PIS (pulmonary index scores) were more significantly improved in the budesonide group than in the control group 6 hours after treatment
Notes Excluded: subjects with febrile respiratory tract infection; those who received corticosteroid or leukotriene D4 receptor antagonist treatment within 4 weeks before study & subjects who were hospitalized Taiwan
Risk of bias table Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk Allocation concealment (selection bias) Unclear risk does not specify Blinding (performance bias and detection bias) Low risk does not specify Incomplete outcome data (attrition bias) Low risk All outcomes Incomplete outcome data (attrition bias) Low risk All outcomes Selective reporting (reporting bias) Low risk Other bias Low risk Apparently
Volovitz 2008 Characteristic of included study: Methods Controlling asthma at home. Quasi randomized crossover design Participants 100 children; Children 5 months to 5 years with severe recurrent asthma. Interventions Treatment: 2 puffs terbutaline followed by 200 micrograms inhaled fluticasone
Control: 2 puffs terbutaline followed by 125 micrograms budesonide Mild attack- 4 day protocol- beta2 agonists 2 puffs 2 times per day for 2 days, and one puff of study drug 4 times per day, than 3 times per day for 2 days then 2 times per day for one day. Severe attack- 8 day protocol beta2 agonists 2 puffs per day twice a day for day 1-4. One or two puffs per day study drug 4 times per day, than 3 times per day for 2 days then1 puff one time per day for one day.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
85
Outcomes Absence of asthma symptoms at the end of the 4th or 8th day. Notes Not blinded.
Risk of bias table Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Low risk "Determined by external circumstance" - budesonide was not available from Dec 2004- February 2005.
Allocation concealment (selection bias) High risk Blinding (performance bias and detection bias) High risk Incomplete outcome data (attrition bias) Low risk All outcomes Incomplete outcome data (attrition bias) Low risk All outcomes Selective reporting (reporting bias) Low risk Other bias Low risk
Synthesis Authors: EBP Scholars (Allen, N H., Collum, K., Gordon, B., Hodges, K., Dusin, J., Pirvu, D., Newman, R., Jones, M.R., Toppass, M., & Shubat, S.) Date: 11/2010
Search Strategies: PubMed search
("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Adrenal Cortex Hormones"[Mesh] OR "Glucocorticoids"[Mesh] OR "inhaled corticosteroids" OR "ciclesonide "[Substance Name] OR "fluticasone "[Substance Name] OR "fluticasone propionate - salmeterol combination "[Substance Name] OR "flunisolide "[Substance Name] OR "Beclomethasone"[Mesh] OR "Budesonide"[Mesh] OR "mometasone furoate "[Substance Name] OR "Triamcinolone"[Mesh] OR "Drug Therapy, Combination"[Mesh]) AND ("Administration, Inhalation"[Mesh] OR "Nebulizers and Vaporizers"[Mesh] OR "nebulizer") AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp]) OR ("Cohort Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms]) AND ("2006/03"[PDAT] : "2010"[PDAT]) http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/1jYpSgv_x6nChw-mYcUQseMAx/
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
86
57 results

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
87
Appendix L Question 11: In the child with an asthma exacerbation in the ED should continuous positive airway pressures (CPAP) or bi-level positive airway pressure (BiPap) be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Synthesis Author(s): Allen, N. H. Date: January 2012 Search Strategy Implemented:
PubMed search September 16, 2010 (("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Magnesium Sulfate"[Mesh] OR "heliox "[Substance Name] OR "Continuous Positive Airway Pressure"[Mesh] OR "Epinephrine"[Mesh] OR "Terbutaline"[Mesh] OR "zafirlukast "[Substance Name] OR "zileuton "[Substance Name] OR "montelukast "[Substance Name] OR "Receptors, Leukotriene"[Mesh] OR "Leukotriene Antagonists"[Mesh] OR "methylxanthine "[Substance Name] OR "Phosphodiesterase Inhibitors"[Mesh] OR "Theophylline"[Mesh] OR "Aminophylline"[Mesh])) AND ("humans"[MeSH Terms] AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp]) OR ("Cohort Studies"[Mesh] OR "Epidemiologic Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms])) AND ("2006/03"[PDAT] : "2010"[PDAT]) http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/10Snxom1j-gcPHZmWk6XHW85-/
39 results
CINAHL search September 16, 2010 S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes -Boolean/Phrase S2 (MH "Emergency MedicalServices+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine")
Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 heliox OR zileuton OR zarfirlukast OR
methylxanthines Search modes - Boolean/Phrase S5 (MH "Disease Exacerbation") Search modes - Boolean/Phrase

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
88
S6 (MH "Magnesium Sulfate") OR (MH "Continuous Positive Airway Pressure") OR (MH "Epinephrine+") OR (MH "Terbutaline") OR (MH "Leukotriene Antagonists+") OR (MH "Montelukast") OR (MH "Phosphodiesterase Inhibitors+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase
S7 S1 or S2 or S5 Search modes - Boolean/Phrase S8 S3 and S7 Search modes - Boolean/Phrase S9 S4 or S6 Search modes - Boolean/Phrase S10 S8 and S9 Search modes - Boolean/Phrase S11 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Human; Publication Type: Algorithm, Clinical Trial,
Journal Article, Nursing Interventions, Practice Guidelines, Protocol, Systematic Review; Age Groups: All Child Search modes - Boolean/Phrase
S12 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Age Groups: All Child Search modes - Boolean/Phrase 1 result Synthesis of relevant studies:
Author, date, country, and industry of
funding
Patient Group
Level of Evidence (Oxford)
Research design Significant results Limitations
Beers, S. L., Abramo, T. J., Bracken, A., & Wiebe, R. A. (2007).
All children with status astmaticus that did not respond to conventional treatment. Children treated from April 1 2003-August 31,
Level 5 Retrospective chart review without a comparison group
83 patient charts were identified. Demographics: median age was 8
years (25th quartile, 5 years; 75th quartile, 11 years) range 2-17 years. 64% were male.
Tolerated BiPAP- 73 patients (88%)
Of those who tolerated BiPAP, 77% showed a decrease in respiratory rate. No patients had an increase in respiratory rate while on BiPAP.
Of those who tolerated BiPAP, 88% showed improved oxygen saturation,
Only one chart reviewer. It is a retrospective chart review; therefore, there is no control group.
High heterogeneity of treatment prior to the initiation of BiPAP

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
89
2004 are included in the review.
Twelve percent had no change in oxygen saturation. No patient had a decrease in oxygen saturation.
Of the patients who tolerated BiPAP, 78% were admitted to the PICU.
Of the patients who tolerated BiPAP 16 (22%) were weaned off BIPAP in the ED and admitted to the floor. None of these patients were transferred to the ED during this admission.
There were no deaths. Brandao, D. C.,
Lima, V. M., Filho, V. G., Silva, T. S., Campos, T. F., Dean, E., & deAndrade, A. D. (2009).
36 Adults (18-65 years of age) with severe asthma – FEV1 < 60% predicted
2b- Low quality RCT-does not describe sequence generation, allocation concealment, blinding of participant or outcome assessors.
Randomized control trial
Did not use RevMan because data was presented graphically only.
Measures of lung function, forced vital capacity (FVC), forced expiratory volume in the first second (FEV1); peak expiratory flow (PEF1) and forced expiratory volume in 25-75% (FEV 25-75%) were all significantly improved in the experimental groups compared to the control group for both levels of BiPAP.
No report of complications, including barotraumas.
The examiner held the BiPAP mask in place. Therefore the examiner was present during the treatment. Cannot tell if the control group was treated the same.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
90
Appendix M Question 12: In the child with an asthma exacerbation in the ED should intravenous montelukast be used to prevent hospitalization, to decrease time in the ED, and/or to improve pulmonary function?
Montelukast vs, placebo children 2-5 years of age, outcome: Pulmonary Index Score at 4 hours
Study or SubgroupHarmanci 2006
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 4.90 (P < 0.00001)
Mean-2.4
SD1.25
Total24
24
Mean-0.9
SD0.86
Total26
26
Weight100.0%
100.0%
IV, Fixed, 95% CI-1.50 [-2.10, -0.90]
-1.50 [-2.10, -0.90]
Experimental- montelukast Control- placebo Mean Difference Mean DifferenceIV, Fixed, 95% CI
-100 -50 0 50 100Favours experimental Favours control

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
91
Comparison of oral montelukast vs. standard treatment in acute moderate to severe asthma in children between 5 and 15 years of age: outcome: Use of rescue drugs (ipratropium bromide).

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
92
Study or SubgroupKumar 2010
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.08 (P = 0.94)
Events28
28
Total60
60
Events27
27
Total57
57
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.97 [0.47, 2.01]
0.97 [0.47, 2.01]
Experimental Control Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours experimental Favours control
Comparison of oral montelukast vs. standard treatment in acute moderate to severe asthma in children between 5 and 15 years of age: outcome: Pulmonary score of <9, 4 hours after montelukast dose.
Study or SubgroupKumar 2010
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.90 (P = 0.37)
Events33
33
Total60
60
Events36
36
Total57
57
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.71 [0.34, 1.50]
0.71 [0.34, 1.50]
Experimental Control Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours control Favours experimenta

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
93
Montelukast vs. Placebo children 6-14 years, outcome: Change in FEV1 at 60 minutes.
Study or SubgroupMorris, 2010
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 0.28 (P = 0.78)
Mean0.08
SD0.3
Total145
145
Mean0.07
SD0.3
Total131
131
Weight100.0%
100.0%
IV, Fixed, 95% CI0.01 [-0.06, 0.08]
0.01 [-0.06, 0.08]
IV montelukcast placebo Mean Difference Mean DifferenceIV, Fixed, 95% CI
-100 -50 0 50 100Favours experimental Favours control
Forest plot: Montelukast vs. Placebo children 6-14 years, outcome: Change in mPI (Mean Pulmonary Index) at 60 minutes.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
94
Study or SubgroupMorris, 2010
Total (95% CI)Heterogeneity: Not applicableTest for overall effect: Z = 0.04 (P = 0.96)
Mean-2.95
SD1.89
Total145
145
Mean-2.96
SD1.89
Total131
131
Weight100.0%
100.0%
IV, Fixed, 95% CI0.01 [-0.44, 0.46]
0.01 [-0.44, 0.46]
IV montelukcast placebo Mean Difference Mean DifferenceIV, Fixed, 95% CI
-100 -50 0 50 100Favours experimental Favours control
Synthesis Author(s): EBP Scholar (Allen, N H., Collum, K., Gordon, B., Hodges, K., Dusin, J., Pirvu, D., Newman, R., Jones, M.R., Toppass, M., & Shubat, S.) Date: October 2010 Search Strategy Implemented:
PubMed search September 16, 2010 (("Asthma"[Mesh] AND ("Emergency Service, Hospital"[Mesh] OR "Emergency Nursing"[Mesh] OR "Emergency Medical Services"[Mesh] OR "Emergency Medicine"[Mesh] OR "Acute Disease"[Mesh] OR exacerbation[All Fields] OR attack[All Fields])) AND ("Magnesium Sulfate"[Mesh] OR "heliox "[Substance Name] OR "Continuous Positive Airway Pressure"[Mesh] OR "Epinephrine"[Mesh] OR "Terbutaline"[Mesh] OR "zafirlukast "[Substance Name] OR "zileuton "[Substance Name] OR "montelukast "[Substance Name] OR "Receptors, Leukotriene"[Mesh] OR "Leukotriene Antagonists"[Mesh] OR "methylxanthine "[Substance Name] OR "Phosphodiesterase Inhibitors"[Mesh] OR "Theophylline"[Mesh] OR "Aminophylline"[Mesh])) AND ("humans"[MeSH Terms] AND ((Meta-Analysis[ptyp] OR Practice Guideline[ptyp] OR Randomized Controlled Trial[ptyp] OR Guideline[ptyp]) OR ("Cohort Studies"[Mesh] OR "Epidemiologic Studies"[Mesh] OR systematic[sb])) AND English[lang] AND ("infant"[MeSH Terms] OR "child"[MeSH Terms] OR "adolescent"[MeSH Terms])) AND ("2006/03"[PDAT] : "2010"[PDAT]) http://www.ncbi.nlm.nih.gov/sites/myncbi/collections/public/10Snxom1j-gcPHZmWk6XHW85-/
39 results
CINAHL search September 16, 2010 S1 (MH "Acute Disease") Limiters - Exclude MEDLINE records Search modes -Boolean/Phrase S2 (MH "Emergency MedicalServices+") OR (MH "Emergency Service+") OR (MH "Emergency Nursing+") OR (MH "Emergency Medicine")
Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S3 (MH "Asthma+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase S4 heliox OR zileuton OR zarfirlukast OR
methylxanthines Search modes - Boolean/Phrase S5 (MH "Disease Exacerbation") Search modes - Boolean/Phrase

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
95
S6 (MH "Magnesium Sulfate") OR (MH "Continuous Positive Airway Pressure") OR (MH "Epinephrine+") OR (MH "Terbutaline") OR (MH "Leukotriene Antagonists+") OR (MH "Montelukast") OR (MH "Phosphodiesterase Inhibitors+") Limiters - Exclude MEDLINE records Search modes - Boolean/Phrase
S7 S1 or S2 or S5 Search modes - Boolean/Phrase S8 S3 and S7 Search modes - Boolean/Phrase S9 S4 or S6 Search modes - Boolean/Phrase S10 S8 and S9 Search modes - Boolean/Phrase S11 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Human; Publication Type: Algorithm, Clinical Trial,
Journal Article, Nursing Interventions, Practice Guidelines, Protocol, Systematic Review; Age Groups: All Child Search modes - Boolean/Phrase
S12 S8 and S9 Limiters - Published Date from: 20060301-20101031; English Language; Age Groups: All Child Search modes - Boolean/Phrase 1 result
Harmanci 2006 Characteristic of included study: Methods Randomized, double-blind, placebo-controlled, parallel-group study Participants Children between 2 and 5 years intermittent asthma Interventions 4 mg tablet of montelukast or placebo. All received nebulized salbutamol (0.15 mg/kg) prior to randomization and up to 2 more
doses at 20 minute intervals within the first hour and at 180 minutes thereafter. Outcomes Reported on: PI score; Not reported on: respiratory rate and pulse Notes Excluded subjects who had taken inhaled or parenteral corticosteroids and leukotriene receptor antagonists in the month previous,
subjects with severe of life threatening asthma attacks. subjects who were born prematurely, low birthweight, mothers smoked during pregnancy; history of respiratory distress syndrome; BPD, broncho malacia, reflux disease, cystic fibrosis.
Risk of bias table Bias Scholars’ judgment Support for judgment
Random sequence generation (selection bias) Unclear risk created outside of the ED probably adequate Allocation concealment (selection bias) Unclear risk created outside of the ED, probably adequate Blinding (performance bias and detection bias) Low risk Tablets were prepared in the Pharmacy, Incomplete outcome data (attrition bias) Unclear risk Selective reporting (reporting bias) Unclear risk

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
96
Other bias Unclear risk Skin prick testing for atopy was completed on all children enrolled. It is not mentioned in the research question as a related factor.
Kumar 2010 Characteristic of included study: Methods Randomized, double-blind, placebo controlled trial. Participants Children between 5-15 years old with moderate to severe asthma. Interventions Children received montelukast (5–12years: 5 mg and >12 years: 10 mg) or placebo orally in addition to the standard therapy. MPIS
and forced expiratory volume in 1 second (FEV1) were recorded before administering study medication and thereafter, hourly for 4 hours.
Outcomes The primary outcome measure was decrease in MPIS to less than 9 at the end of 4 hours. The secondary outcome measures were change in FEV1 (percentage predicted), adverse effects (headache, nausea, vomiting, and abdominal pain) and the need for hospitalization in the two groups at the end of 4 hours.
Notes
Risk of bias table Bias Scholars' judgment Support for judgment
Random sequence generation (selection bias) Low risk Computer-block design. Allocation concealment (selection bias) Low risk Yes, someone not involved in the study. Blinding (performance bias and detection bias) Low risk Double blinded. Incomplete outcome data (attrition bias) High risk No incomplete data. Selective reporting (reporting bias) Unclear risk Other bias Low risk Pharmaceutical company not involved in study.
Morris, 2010 Characteristic of included study: Methods Randomized, double-blind, placebo controlled study Multi centered Participants Children 6-14 years of age. Subjects with an FEV1 of 75% or less predicted value and a modified Pulmonary Index (mPI) score of
5 or higher on 2 occasions Interventions 60 minutes standard care, followed by the pre-study period up to 60 minutes where standard treatment continued, and
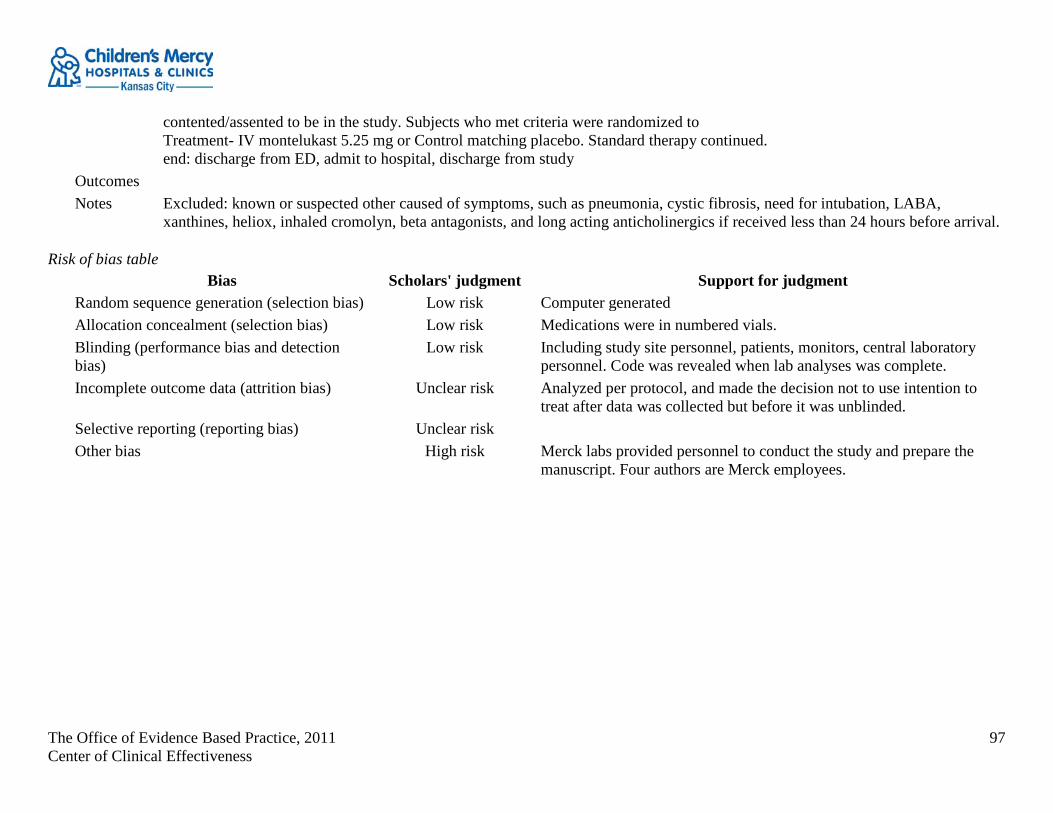
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
97
contented/assented to be in the study. Subjects who met criteria were randomized to Treatment- IV montelukast 5.25 mg or Control matching placebo. Standard therapy continued. end: discharge from ED, admit to hospital, discharge from study
Outcomes Notes Excluded: known or suspected other caused of symptoms, such as pneumonia, cystic fibrosis, need for intubation, LABA,
xanthines, heliox, inhaled cromolyn, beta antagonists, and long acting anticholinergics if received less than 24 hours before arrival.
Risk of bias table Bias Scholars' judgment Support for judgment
Random sequence generation (selection bias) Low risk Computer generated Allocation concealment (selection bias) Low risk Medications were in numbered vials. Blinding (performance bias and detection bias)
Low risk Including study site personnel, patients, monitors, central laboratory personnel. Code was revealed when lab analyses was complete.
Incomplete outcome data (attrition bias) Unclear risk Analyzed per protocol, and made the decision not to use intention to treat after data was collected but before it was unblinded.
Selective reporting (reporting bias) Unclear risk Other bias High risk Merck labs provided personnel to conduct the study and prepare the
manuscript. Four authors are Merck employees.
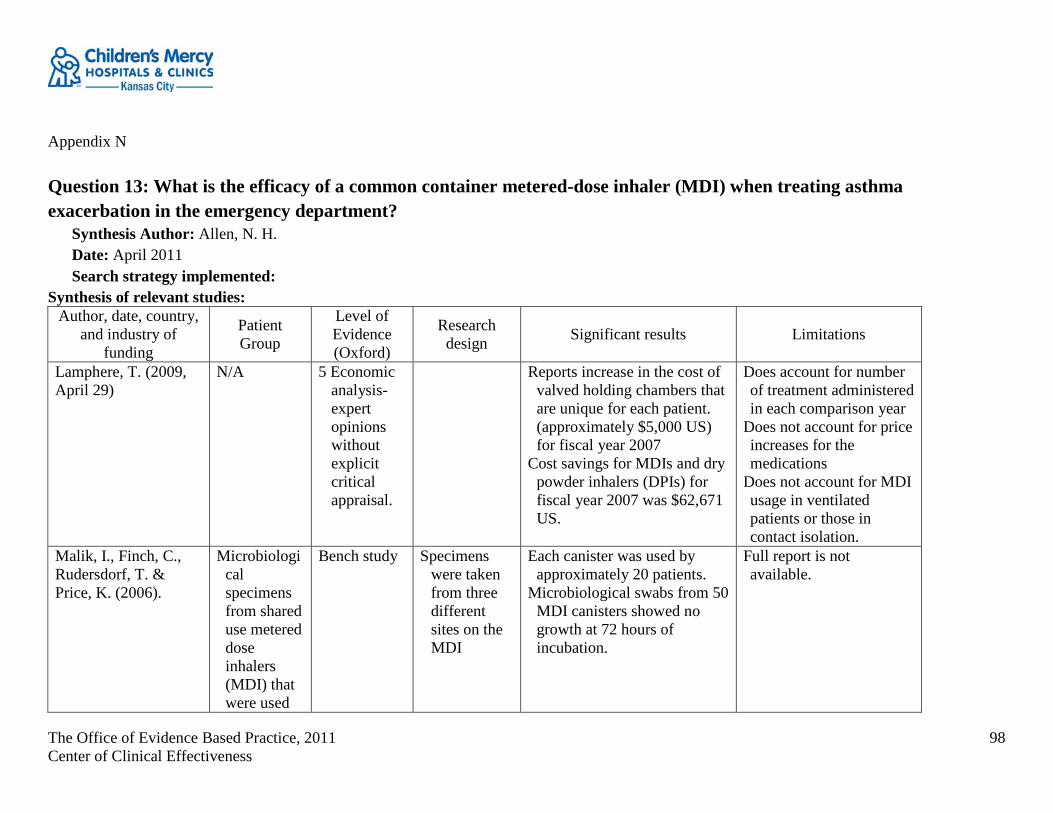
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
98
Appendix N Question 13: What is the efficacy of a common container metered-dose inhaler (MDI) when treating asthma exacerbation in the emergency department?
Synthesis Author: Allen, N. H. Date: April 2011 Search strategy implemented:
Synthesis of relevant studies: Author, date, country,
and industry of funding
Patient Group
Level of Evidence (Oxford)
Research design Significant results Limitations
Lamphere, T. (2009, April 29)
N/A 5 Economic analysis- expert opinions without explicit critical appraisal.
Reports increase in the cost of valved holding chambers that are unique for each patient. (approximately $5,000 US) for fiscal year 2007
Cost savings for MDIs and dry powder inhalers (DPIs) for fiscal year 2007 was $62,671 US.
Does account for number of treatment administered in each comparison year
Does not account for price increases for the medications
Does not account for MDI usage in ventilated patients or those in contact isolation.
Malik, I., Finch, C., Rudersdorf, T. & Price, K. (2006).
Microbiological specimens from shared use metered dose inhalers (MDI) that were used
Bench study Specimens were taken from three different sites on the MDI
Each canister was used by approximately 20 patients.
Microbiological swabs from 50 MDI canisters showed no growth at 72 hours of incubation.
Full report is not available.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
99
over 3 months
Mantz, H. D., Radke, L., & Gunn, J. (2010).
9000 common canister treatments
2c Outcomes research
Protocol change analysis
MRSA infection rate did not increase during the time the common canister treatments were in use.
Is MRSA the correct organism to evaluate infection risk?
Sheils, S. G., Duncan, J. L., & Wojciechowski, W. V. (2006).
17 patients had shared Monaghan aero chamber MDIs swabbed at three time surrounding actuations
Pre actuation after swabbing with an alcohol pad
Post actuation prior to swabbing with an alcohol pad
Post actuation after swabbing
Bench study Specimens were taken at three different times from the MDI.
There was no growth from any sample at 24, 48 or 72 hours.
Report a potential reduction in MDI purchase cost of 55%.

The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness
100
with an alcohol swab
Smetzer, J., Cohen, M. R., & Jenkins, R. (Eds). (2009, April 9)
None Narrative review
Reiterates the findings of the Sheils (2006) and Malik (2006) studies which are reported here.
Adds greater potential for contamination comes from the outside of the canister. Proper cleaning of the canister, and hand washing are paramount to prevent infection.
Cost of one infection may be greater than any savings incurred from sharing MDIs.
Opinion