chilaiditi’s syndrome with associated angina - japi.org · the case of chilaiditi’s syndrome...
TRANSCRIPT
44 © JAPI • JANUARY 2010 • VOL. 58
Case Reports
Introduction
H epato-diaphragmatic interposition of a bowel segment, also known as Chilaiditi’s sign, is an uncommon and typically
asymptomatic anatomical abnormality. It can be either congenital or acquired and is more common in males. When associated with symptoms, it is termed as Chilaiditi’s syndrome1. Most of the symptoms are always related to the gastro intestinal tract itself such as, most commonly, abdominal pain, dyspepsia and intestinal obstruction due to volvulus. In the case described in this paper, the hepato-diaphragmatic migration of the hepatic flexure of the colon was associated with an angina-like pain, exclusively evoked by the left lateral position. Investigations conducted in our patient ruled out any ischemic cardiac aetiology and showed that the symptom was caused most likely by the motion of the colon into the chest. Only one such case has been reported worldwide with similar findings.3
AbstractSymptomatic hepato-diaphragmatic interposition of a bowel loop or Chilaiditi’s syndrome [Pronounced “Ky-La-Ditty”] is a very rare (0.1-0.25%) anatomical condition most often found by chance. Its described symptoms range from intermittent, mild abdominal pain and dyspepsia to acute intestinal obstruction.
We report a case of acquired hepato-diaphragmatic migration of the hepatic flexure of the colon associated to an unusual, angina-like pain more in the left lateral position. ECG, stress test, 2D echo and regional cardiac injury markers were within normal limits indicating that the pain was unlikely due to myocardial ischemia.
It is possible that the pain felt by the patient, concomitant to the migration of the hepatic flexure, was simply due to the transient stimulation of cardiac nervous fibers or to the internal compression of the chest or to overstretching of the major vessels-including the aorta and vena cava, or to a combination of these last two factors.
This case suggests that Chilaiditi’s syndrome should be included among the possible, although rare, causes of unexplained angina-like symptoms.
*Associate Professor, Dept. of Medicine; **PG Resident, General Medicine, Rajawadi Municipal Hospital, Ghatkopar; MumbaiReceived: 22.12.2008; Revised: 13.02.2009; Accepted: 25.03.2009
Case ReportA 70 years old man presented to our medical OPD with the
complaints of retrosternal chest pain radiating to the left arm, mild dyspnea, and a state of prostration for the past 2 years. The symptoms were exacerbated with the patient lying on his left side, and subsided in the supine position. For this reason, he had been previously referred to a cardiologist. However, ECG; 2D Echo and stress test were within normal limits.
He reported, during his symptoms, the subjective feeling of a mass moving from the abdomen toward the chest.
He was diagnosed with CA larynx three years back for which he underwent total laryngectomy and partial pharyngectomy followed by a course of chemotherapy. He was hypertensive under regular treatment. He was non diabetic and a chronic smoker in the past.
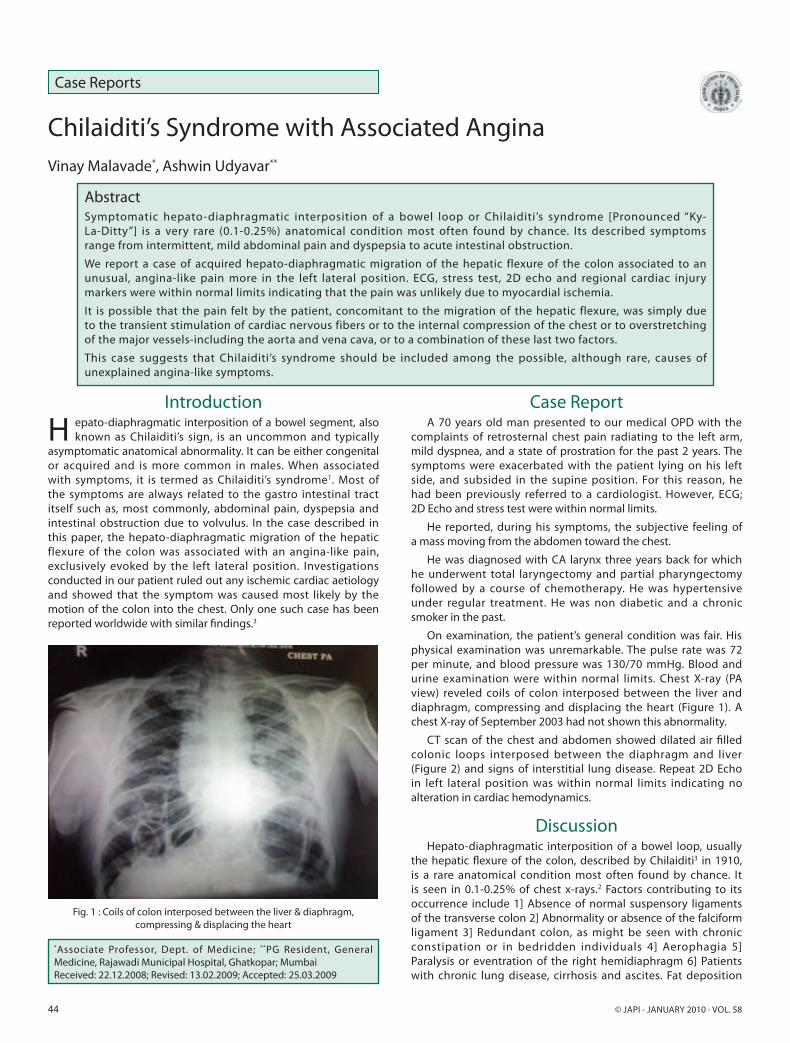
On examination, the patient’s general condition was fair. His physical examination was unremarkable. The pulse rate was 72 per minute, and blood pressure was 130/70 mmHg. Blood and urine examination were within normal limits. Chest X-ray (PA view) reveled coils of colon interposed between the liver and diaphragm, compressing and displacing the heart (Figure 1). A chest X-ray of September 2003 had not shown this abnormality.
CT scan of the chest and abdomen showed dilated air filled colonic loops interposed between the diaphragm and liver (Figure 2) and signs of interstitial lung disease. Repeat 2D Echo in left lateral position was within normal limits indicating no alteration in cardiac hemodynamics.
DiscussionHepato-diaphragmatic interposition of a bowel loop, usually
the hepatic flexure of the colon, described by Chilaiditi3 in 1910, is a rare anatomical condition most often found by chance. It is seen in 0.1-0.25% of chest x-rays.2 Factors contributing to its occurrence include 1] Absence of normal suspensory ligaments of the transverse colon 2] Abnormality or absence of the falciform ligament 3] Redundant colon, as might be seen with chronic constipation or in bedridden individuals 4] Aerophagia 5] Paralysis or eventration of the right hemidiaphragm 6] Patients with chronic lung disease, cirrhosis and ascites. Fat deposition
Chilaiditi’s Syndrome with Associated AnginaVinay Malavade*, Ashwin Udyavar**
Fig. 1 : Coils of colon interposed between the liver & diaphragm, compressing & displacing the heart

© JAPI • JANUARY 2010 • VOL. 58 45
between the liver and the colon, in obese individuals, widens the space between the two organs and can also favor the migration of the colon1. When associated with symptoms from mild abdominal pain and dyspepsia to acute intestinal obstruction-it is termed Chilaiditi’s syndrome1 [Pronounced “Ky-La-Ditty”].
The case of Chilaiditi’s syndrome reported here is peculiar with regard to its symptoms- i.e. angina like pain with left arm irradiation caused most likely by the motion of the colon into the chest. Our patient had interstitial lung disease as a predisposing factor.4
His chest X-ray and CT scan show that the colon (with the interposition of the diaphragm) was clearly touching the heart,
displaced and compressing it (Figures 1, 2).
The cardiac hemodynamics is not expected to be affected since the pressure inside the heart chambers far exceeds that inside the colon. Thus, it is possible that the pain felt by the patient, concomitant to the migration of the hepatic flexure, was simply due to the transient stimulation of cardiac nervous fibers or to the internal compression of the chest or to overstretching of the major vessels-including the aorta and vena cava, or to a combination of these factors.5
In conclusion, Chilaiditi’s syndrome should be included among the possible, although rare, causes of unexplained angina-like symptoms.
References1. Lekkas CN, Lentino W. Symptom-producing interposition of the
colon. JAMA 1978; 240: 747-750
2. Walsh SD, Cruikshank JG. Chilaiditi’s syndrome. Age Ageing 1976; 6: 51-57
3. Sorrentino D, Bazzocchi M, Badano L, Toso F, Giagu P. Heart touching Chilaiditi’s syndrome. World J Gastroenterol 2005; 11: 4607-4609
4. Schubert SR. Chilaiditi’s syndrome: an unusual cause of chest or abdominal pain. Geriatrics 1998; 53: 85-88
5. Braunwald E. The History. In: Braunwald E. ed: Heart Disease, Philadelphia, PA WB Saunders 2000: 1-13.
Fig. 2 : Dilated loops of colon displacing the heart