career planning assistance at usa college of medicine
TRANSCRIPT
Career Planning Assistance atUSA College of Medicine
Spring, 2010
1
CONTENTSPreface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Guidelines for Faculty Advisors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Anesthesiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Emergency Medicine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Family Medicine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Internal Medicine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Combined Internal Medicine / Pediatrics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Neurological Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Neurology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Nuclear Medicine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Obstetrics and Gynecology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Ophthalmology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Orthopaedic Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Otorhinolaryngology - Head and Neck Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Pediatrics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Psychiatry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Radiation Oncology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Radiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Urological Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25

2
PREFACE
For some medical students, choosing a career path to follow after medical school is daunting.Second semester juniors are encouraged to self-assess for likes/dislikes, strengths/weaknesses, andgeneral aptitudes. They are provided with the AAMC Careers in Medicine website which has linksto self-assessment tools.
As the junior students are working through the process, clinical departments are expected toschedule an informational meeting between January 11, 2010 and March 26, 2010. The informationshared at that meeting should include a departmental statement about the philosophy of the specialty,general information about the residency experience in that specialty, and employment prospectsfollowing residency.
The final and essential step in this process is student guidance/counseling/mentorship on anindividual basis by members of the clinical departments. Students select their advisors from the listprovided by each department of the faculty who are interested and available to perform thisimportant function.
3
GUIDELINES FOR FACULTY ADVISORS
Faculty Advisors to senior students are volunteers who have agreed to help students:
1. Design a curriculum for their senior year.2. Make a career decision and assist in selection of potential residency programs, and3. Guide them through the process of applying for residency programs.
In the second half of their junior year, students choose their advisors from the lists provided by theclinical departments based on a tentative choice of specialty (a student who is probably interestedin pediatrics would choose a faculty member in the Department of Pediatrics). Should a student'sspecialty goals change, he/she may elect to choose a new advisor.
From the standpoint of the stated goals of the program each advisor should endeavor to help thestudent with the following tasks:
1. Design a curriculum for the senior year
Students are required to take five 4-week rotations from the following categories:
1. Acting Internship 3. Surgery Subspecialty•Two separate rotations are 4. Medical, Pediatric or OB/GYN subspecialty required
2. Ambulatory Care
After discussion of an advisee's strengths, weaknesses and interests, the advisor should help assessareas of educational need and help design a program of courses for the senior year that will meetthose needs using both the requirements above and the remaining sixteen weeks of elective time.Students who experienced academic difficulty in the third year may be required by the StudentPromotion and Evaluation Committee to take certain courses in the senior year.
2. Select a career discipline
An advisor should meet with his/her advisee toward the end of the junior year to discuss thestudent's chosen specialty. The advisor should attempt to inform the student of what he/she canexpect during postgraduate training and in practice. The student should discuss special needs suchas geographical or family requirements. While most faculty tend to encourage students to take theirpostgraduate education in university based programs, there may be an occasional individual whowould profit from a community based program. Advisees should be encouraged to apply to the bestpossible programs, but they should also have one or two less competitive programs which would beacceptable. Students who are applying in very competitive specialties (radiology, ophthalmology,orthopaedics, etc.) should have an additional specialty on their list should they fail to match in thefirst specialty. The list should consist of a rational number of programs and students should bediscouraged from applying to more than twenty programs without careful consideration.
4
Based on the student's needs for postgraduate education, the advisor and the student should developa rank order list of programs to which application will be made.
3. The residency application process
As a student starts the residency application process, his/her advisor should assist as questions arise.The advisor should help the student decide whom to ask to write letters of recommendation. Forexample, maybe one or more faculty colleagues are closely connected with the student's highestranking programs. The student would be advised to ask these faculty members to write letters forhim/her.
Most senior medical students have "survived" numerous interviews but some may feel that they needcoaching. Advisors should discuss questions commonly asked during interviews. The studentshould also be helped with questions they should ask to get a feel for the quality of a program.
It should be stressed to the advisee that the rank order list they submit to the NRMP is veryimportant. Under the rules of the Match, students are obligated to sign a contract with the programto which they match. No program should be on the student's final rank list if the student does notthink it will meet his/her needs. If a student does not match, advisors are expected to be availableto assist with the Scramble, which typically occurs on the Tuesday before the Match in March.
4. Schedule changes
The advisor has one additional duty. Senior students frequently make changes in their schedulesthroughout the year. It is the student's responsibility to bring the "Drop-Add," externship, andapproval forms to his/her advisor for approval and signature. The advisor should give carefulconsideration to the proposed schedule change and to the impact on the student's education. Theforms should not be "rubber stamped."
5
ANESTHESIOLOGY
Robert Marslender, DirectorUSA Medical Center, Room #333, 471-7035
Faculty Advisors to Senior Students
Dr. Wade Hutchens, Chief of Anesthesiology([email protected])
Dr. Robert Watson([email protected])
Meeting to Discuss Residency Training in this Discipline
Wednesday, March 3 at 3:00 p.m. at USA Medical Center, third floor, room #335
Informal Description of the Clinical Discipline
Anesthesiologists are involved in patient care in four main areas: 1) operating room anesthesia, 2)critical care medicine, 3) pain control, 4) obstetrics anesthesia.
The majority of the Anesthesiologist’s effort is in the operating room. There, the anesthesiologistrenders the patient insensitive to surgical pain and stimulation. In doing so, extremely potent drugsare used which markedly affect the patient’s physiology. Most noticeable affected are the neurologic,cardiovascular and respiratory systems. Operative care of the patient requires monitoring andmaintenance of physiologic functions. This requires pharmacologic intervention, inhibitingsensation, controlling respiration, and adjustment of fluid infusions. Considerable technology hasdeveloped around Anesthesiology to help facilitate measurement of physiologic variables. Areas ofsubspecialty interest have developed in cardiac, neuro, pediatric and obstetrical anesthesia.
Some anesthesiologists are involved in the care of critically ill surgical patients. If fact, moderncritical care medicine has its roots in the involvement of anesthesiologists perfecting he means tomechanically ventilate polio victims. The American Board of Anesthesiology offers a certificate ofSpecial Qualifications in Critical Care Medicine. Involvement in postoperative care is a logicalextension of the operating room care provided by the anesthesiologist. This usually includesmanagement of cardiovascular and pulmonary problems.
Involvement of anesthesiologists into the management of chronic pain grew from intraoperative andpost operative control of responses to surgical stimulus. Both acute and chronic pain syndromes areaddressed by anesthesiologists. This area of anesthesiology can be very attractive to the physicianwishing to have more long term contact with patients.
Training requirements in anesthesiology start with a clinical base year which is best fulfilled by arotating type of internship. Medical, surgical and pediatric years are also acceptable. Three yearsof clinical anesthesiology are required. The third year may focus on a subspecialty area or onresearch, along with emphasis on becoming a true Consultant in Anesthesiology.
6
EMERGENCY MEDICINE
Frank S. Pettyjohn, M.D., Professor and Chair10th Floor, USAMC, 470-1649
Faculty Advisors to Senior StudentsDr. Melissa W. Costello ([email protected]) Dr. W. Scott McNair ([email protected])Dr. Frank S. Pettyjohn ([email protected]) Dr. Lynne A. McDonnell ([email protected])Dr. Michael L. Sternberg ([email protected]) Dr. Anthony Pacheco ([email protected])Dr. Terry N. Rivers ([email protected]) Dr. Michael Ambrose ([email protected])
Meeting to Discuss Residency Training in this DisciplineTuesday, January 12 at 1:30 p.m. in the Emergency Medicine Conference Room10th Floor of USAMC, Suite M
Informal Description of the Clinical DisciplineThe House of Delegates of the American Medical Association defined the emergencyphysician as a physician trained to engage in:
1. the immediate initial recognition, evaluation, care, and disposition of patients inresponse to acute illness and injury;
2. the administration, research, and teaching of all aspects of emergency medical care;3. the direction of the patient to sources of follow-up care, in or out of the hospital as
may be required;4. the provision when requested of emergency, but not continuing, care to inhospital
patients; and5. the management of the emergency medical system (EMS) for the provision of
prehospital emergency care.
Emergency medicine encompasses the immediate decision making and action necessary toprevent death or disability for patients with acute surgical or medical disease. Emergencymedicine is practiced as patient-demand and readily accessible care. It encompasses thecritical actions of initial recognition, rapid stabilization, followup, evaluation and treatment.The patient population is a full spectrum of ages and health care problems. Emergencymedicine is primarily hospital-based, but with extensive prehospital responsibilities.
The specialty involves the continuing assessment of the patient's condition beyond theimmediate life, limb, and disability threats. The use of advanced diagnostic techniques inradiologic, cardiovascular, and pulmonary medicine provides for a multi-skilled specialty.
7
FAMILY MEDICINE
Allen Perkins, M.D., Professor and ChairUSA Springhill, 434-3482
Faculty Advisors to Senior StudentsDr. Allen Perkins ([email protected]) Dr. Ehab Molokhia ([email protected])Dr. Carol Motley ([email protected]) Dr. Shyla Reddy ([email protected])Dr. Tangela Atkinson ([email protected]) Dr. Lamar Duffy ([email protected]) Dr. Michael Linder ([email protected])
Meeting to Discuss Residency Training in this DisciplineFriday, February 26 at 3:00 p.m. in the Mastin Building, Room 207, with Dr’s. Perkins and Motley.
The Specialty of Family MedicineThe specialty of Family Medicine has undergone tremendous changes in the last two years and continues to changeto meet the needs of the communities in which family physicians practice. The specialty of Family Medicine iscentered on lasting, caring relationships with patients and their families. Family physicians integrate thebiological, clinical and behavioral sciences to provide continuing and comprehensive health care. The scope ofFamily Medicine encompasses all ages, sexes, each organ system and every disease entity.
Scope of Family MedicineOf the primary care specialties (Family Medicine, General Internal Medicine, Pediatrics) family physicians providethe most care - managing nearly one-fourth of all primary care visits. Given the scope of Family Medicine, thiscomes as no surprise. Family Medicine is a three-dimensional specialty, incorporating (1) knowledge, (2) skilland (3) process. At the center of the process element is the patient-physician relationship with the patient viewedin the context of the family. It is the extent to which this relationship is valued, developed, nurtured andmaintained that distinguishes Family Medicine from all other specialties. Family physicians integrate thebiological, clinical and behavioral sciences to provide continuing and comprehensive health care. Unlikepediatricians who only provide care for children, and internists who only provide care for adults, Family Medicineencompasses all ages, sexes, each organ system and every disease entity. Family physicians also pay specialattention to their patients’ lives within the context of family and the community. While there are similaritiesbetween Family Medicine and the other primary care specialties, family physicians have an unprecedentedopportunity to have an impact on the health of an individual patient over that person’s entire lifetime.
Demand for Family PhysiciansThe case for maintaining an adequate family physician workforce is strong. Studies reveal that:
•Family Medicine reduces health care costs and increases health care quality.•Family physicians are geographically distributed across the country more equitably than physicians fromany other specialty.•Family physicians are geographically and financially more accessible to disadvantaged populations thatlack access to quality health care than other primary care physicians, which, in turn, helps to reduce healthdisparities.•Individuals who regularly visit a family physician are more likely to receive preventive services, bettermanagement of chronic illnesses and decreased chance of premature death.
Recruitment data indicates that family physicians are in demand. According to Merritt, Hawkins & Associates,in 2007, Family Medicine was the highest recruited specialty for the third consecutive year.
Go to the virtual FMIG at http://fmignet.aafp.org/online/fmig/index.html for more details on the specialty.
8
INTERNAL MEDICINE
Errol Crook, M.D., Professor and ChairUSAMC Mastin 400-A, 471-7900
Faculty Advisors to Senior StudentsDr. Ronald Allison ([email protected]) Dr. Kevin Green ([email protected])Dr. John Bass ([email protected]) Dr. Johnson Haynes ([email protected])Dr. Judy Blair-Elortegui ([email protected]) Dr. Clara Massey ([email protected])Dr. M. Culpepper ([email protected]) Dr. T. Montgomery ([email protected])Dr. John Schultz ([email protected]) Dr. John Vande Waa ([email protected])Dr. Jack DiPalma ([email protected]) Dr. Barry Warner ([email protected])Dr. T. J. Hundley ([email protected]) Dr. Grace Hundley ([email protected])Dr. Karen Fagan ([email protected]) Dr. Gregory Rutecki ([email protected])Dr. B. Burckhartt ([email protected])
Meeting to Discuss Residency Training in this DisciplineThursday, February 4 at 11:30 a.m. in the Eichold Room, 10th floor, USAMC
Informal Description of the Clinical DisciplineInternal Medicine is a broad-based primary care specialty focused on disease prevention andtreatment in young and older adults. The educational focus of the internal medicine training programis designed to allow optimum exposure to the many facets of internal medicine in order to preparethe individual for a position of leadership as a practitioner, consultant, subspecialist or academician.Educational programs emphasize pathophysiologic principles. The training program for a generalinternist is three years with graded responsibility for patient care. During this period the physicianis exposed to primary care and subspecialty disciplines and participates in the clinical activities ofcardiologists, gastroenterologists, endocrinologists, etc., as part of the training program. An internistis expected to become a well-read and well-rounded consultant, participating actively in the care ofadults with a variety of medical problems. The internist may serve as a primary care physician insome situations and as a consultant in others. Approximately half of the internists finishing the three-year training program become primary care health providers. Others enter a subspecialty fellowshiptraining program or become hospitalists.
9
COMBINED INTERNAL MEDICINE / PEDIATRICS
Judy Blair-Elortegui, M.D.Residency Program Director
Faculty Advisors to Senior StudentsDr. Judy Blair-Elortegui Dr. Franklin Trimm([email protected]) ([email protected])
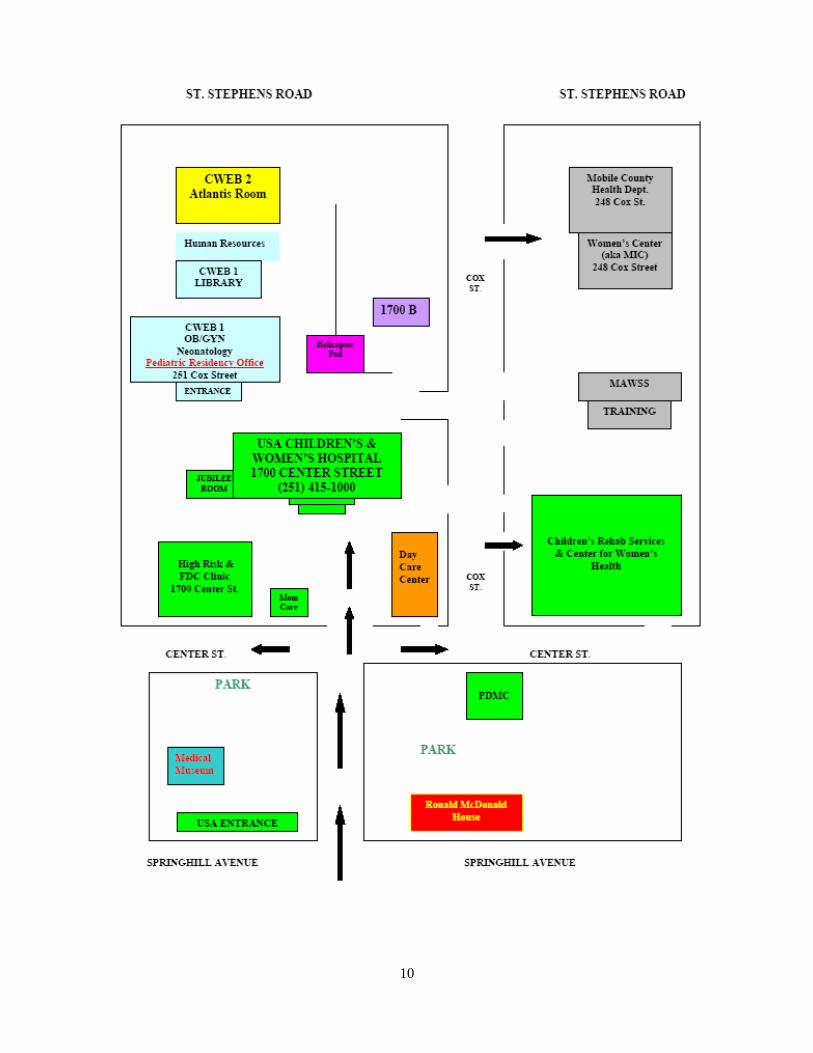
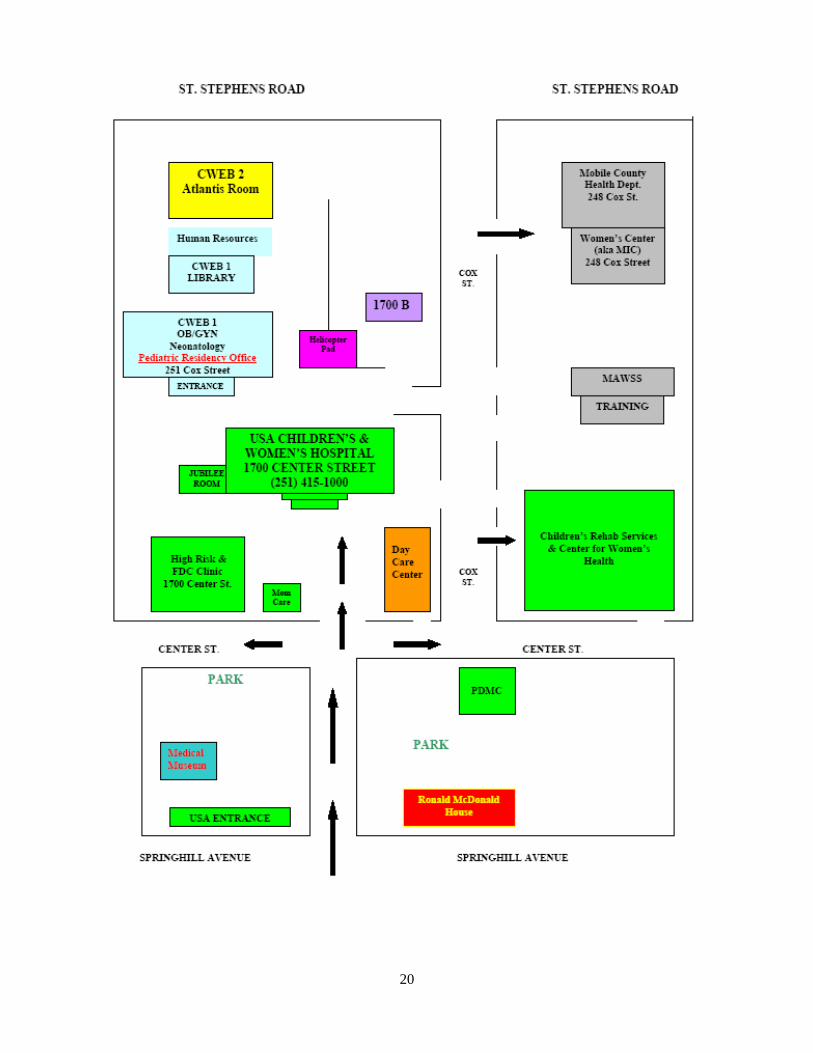
Meeting to Discuss Residency Training in this DisciplineThursday, February 11 at 11:00 a.m. in the Neonatology Conference Room at Children’s andWomen’s Hospital, CWEB 1 (map of building location on following page). Lunch isprovided.
Informal Description of the Clinical Discipline
An internal medicine-pediatric residency offers a unique, challenging experience for thephysician in training to develop broad clinical skills in the two most respected primary carefields. Residents successfully completing this rigorous four-year program are eligible forboard certification in both disciplines.
The combined residency provides in-depth education for clinical practice careers. Internalmedicine-pediatric physicians provide diagnostic, treatment and follow-up care fornewborns, children, adolescents, and adults. Graduates of a combined residency mayfunction as generalists in private practice with hospital privileges in both pediatrics andinternal medicine.
Some graduates choose further subspecialty training in medicine, pediatrics or both, andmany continue to care for children and adults in those subspecialties. Graduates ofcombined medicine-pediatric programs have been integrated into private practices, healthmaintenance organizations and academic faculties.
Medical graduates who choose the challenge of combined training must be flexible andenergetic. Acquiring the broad knowledge base and skills for this combined specialtyrequires an intensive commitment on the part of the resident physician. A solid foundationin the basic and clinical sciences is a prerequisite for this rigorous residency.
The clinical skills and expertise gained through a combined medicine-pediatrics trainingprogram put the graduate in a very desirable position for meeting the biggest health careneed of the United States: well trained generalists. In addition, the graduate is also in aposition to pursue additional training in a wide variety of subspecialties.
10
11
NEUROLOGICAL SURGERY
Eugene Quindlen, M.D., Professor and ChairHealth Services Building, Suite 2150
Faculty Advisors to Senior StudentsDr. Eugene Quindlen ([email protected])Dr. Anthony Martino ([email protected])
Meeting to Discuss Residency Training in this DisciplineCall Dr. Quindlen or Dr. Martino for an appointment (665-8290)
Informal Description of the Clinical DisciplineRelatively speaking, the field of neuroscience is in its infancy. Although there have beengreat advances in diagnostic ability with the CAT and MRI scans, new methods aredeveloping currently concerning stereotactic and functional surgery. Electrostimulation maywell compensate for certain brain dysfunctions. Replacement or chemotherapy formovement disorders are on the horizon.
Because of the wide variety of treatment modalities now being developed by otherspecialties, an area of opportunity for the future of the neurosciences lies in thecollaborations developing the treatment of chronic conditions related to pain and functionaldisabilities.
Neurosurgery plans to capitalize on all these new methods and advance the science. Thefuture neurosurgeon will need to be a skilled diagnostician, electrophysiologist,pharmacotherapeutist as well as technician. Only those in the top 10% of the class shouldconsider neurosurgery as a career since the entry points are that competitive.

12
NEUROLOGY
Dean K. Naritoku, M.D., Professor and Chair3401 Medical Park Drive, Building #3 - Suite 205
660-5118 / FAX 660-5924
Faculty Advisors to Senior StudentsDr. Dean Naritoku ([email protected])Dr. Bassam Bassam ([email protected])Dr. Paul Maertens ([email protected])
Meeting to Discuss Residency Training in this DisciplineSchedule with Department of Neurology, 660-5506
Informal Description of the Clinical DisciplineNeurology is the field of medicine involved with the diagnosis and treatment of diseases ofthe nervous system, i.e., the brain, spinal cord, peripheral nerve and muscle. Patients withneurological disease present with a wide variety of difficult, challenging and compellingproblems. Practicing this specialty, the physician performs comprehensive and detailedneurological histories and examinations, and performs and interprets a variety ofneurodiagnostic studies, including lumbar puncture, computerized tomography, magneticresonance imaging, angiography, myelography, electroencephalography, and neurosonologicexams. Careful clinical analysis of patients with nervous system disease allows forlocalization and characterization of the underlying abnormalities. Most importantly,treatment of neurological disease has advanced significantly in recent years, and the numberand scope of illnesses now amenable to treatment has been increasing at an extraordinarilyrapid rate.
13
NUCLEAR MEDICINE
Samuel A. McQuiston, M.D., Assistant ProfessorDepartment of Radiology
USAMC Mastin 301, 471-7861
Faculty Advisor to Senior StudentsDr. Samuel McQuiston ([email protected])
Meeting to Discuss Residency Training in this DisciplineTuesday, February 23 at 3:30 p.m. in the Richards Room, second floor at USAMC, with Dr.McQuiston. (This is a combined meeting with Radiology).
Informal Description of the Clinical DisciplineResidency training in nuclear medicine requires two years of AMA approved training inInternal Medicine, Pathology or Radiology or any other Primary Care specialty prior to entryinto the nuclear medicine residency. The duration of nuclear medicine residency approvedby the AMA is two years. Upon completion of successful training, trainees become boardeligible in the nuclear medicine specialty.
The field of nuclear medicine consists of in vitro tracer kinetic studies, in vivo imaging (themost common type of NM practice), therapeutic uses of unsealed isotope sources, andresearches using various radioactive tracers.
Nuclear Medicine procedures are based upon physiologic, metabolic and functional naturerather than anatomical information used in U-S, C-T and MRI. There are ampleopportunities for basic and clinical researches in addition to clinical practice.Radioimmunodetection using radiolabeled monoclonal antibodies, the continuousdevelopment of new radiopharmaceuticals, single photon emission computer tomography(SPECT), and positron emission tomography (PET) are exciting developments in nuclearmedicine in recent years.

14
OBSTETRICS AND GYNECOLOGY
Kathy Porter, M.D., Professor and ChairUSA Children’s and Women’s Hospital, CWEB 1005, 415-1566
Faculty Advisors to Senior StudentsDr. Sheri Owens ([email protected])Dr. Kathy Porter ([email protected])
Meeting to Discuss Residency Training in this Discipline Friday, March 5 at 12:00 p.m. in the Children’s and Women’s Education Building, behind
Children’s and Women’s Hospital, with Dr’s. Owens and Porter. If there are any questions,call 415-1550.
Informal Description of the Clinical DisciplineThe field of Obstetrics and Gynecology encompasses comprehensive health care for women.The obstetrician-gynecologist provides primary health service for women including educationand preventive care, treatment for routine and complex gynecologic and obstetric problems, andconsultative services to other physicians and paramedical personnel in problems relative to thereproductive and the lower urinary systems. The Ob/Gyn specialist must have a comprehensiveunderstanding of the embryology, genetics, physiology, endocrinology, and pathology of thefetus and female reproductive system in order to provide care to the female from pre-menarcheto post-menopause. Residency programs in Obstetric and Gynecology are structured to providethe medical, obstetrical and surgical skills required of the consultant obstetrician-gynecologist.As these skills are absorbed, the judgmental processes for patient care will be developed in thephysician.
Residency programs consist of four years of postgraduate education, and are governed by theAccreditation Council for Graduate Medical Education on recommendation by the ResidencyReview Committee for Obstetrics and Gynecology (RRC).
Programs in Obstetrics and Gynecology stress training in both hospital based and ambulatorycare settings and include experience in: both routine Obstetrics and Gynecology; maternal-fetalmedicine; immediate care of the newborn; urogynecology and pelvic surgery; pelvic pathology;reproductive endocrinology and infertility; family planning; genetics; medical ethics;gynecologic oncology including chemotherapy, radiation therapy, and robotics; psychosexualand psychosomatic counseling; and a host of diagnostic and therapeutic procedures includingfetal and pelvic sonography. General primary care of women is now taught.
At present, there are four recognized subspecialties in Obstetrics and Gynecology: GynecologicOncology, Reproductive Endocrinology and Infertility, Maternal-Fetal Medicine andGynecologic Urology. Preparation for certification in a subspecialty is via a three to four yearpost-residency fellowship in a program accredited by the appropriate division of the AmericanBoard of Obstetrics and Gynecology. Satisfactory completion of such training confers eligibilityto take the examination for sub-certification of special competence in that field. Fellowshiptraining currently not leading to certification is also available in some centers in infectiousdiseases, and pelvic and fetal sonography.
15
OPHTHALMOLOGY
William O. Richards, M.D., F.A.C.S., Professor and ChairDepartment of Surgery, Mastin 721, 471-7993, ([email protected])
Roy E. Gandy, M.D., ProfessorDepartment of Surgery, Mastin 717, 471-7974, ([email protected])
Meeting to Discuss Residency Training in this DisciplineTuesday, February 9 at 1:00 p.m. in the Mastin Building, 7th floor conference room. This isa combined meeting with Surgery and Urology. Call 471-7990 if you have any questions.
Informal Description of the Clinical DisciplineAlthough Ophthalmology is sometimes regarded as a highly specialized field, the generalophthalmologist is, in fact, a primary care physician. Patients who consult an ophthalmologistusually are self-referred and range in age from the newborn to the geriatric. Theophthalmologist, like other primary care physicians, has the opportunity to get to know andfollow patients and their families, allowing for continuity of care.
Most ophthalmologists practice a mixture of medicine and surgery, ranging from lensprescriptions and standard medical treatment to the most delicate and precise operativeprocedures. The average American Ophthalmologist will see over one hundred patients in awork week and will perform two major medical surgical procedures, the most common beingcataract extraction. Ophthalmologists have always ranked among the most professionallysatisfied physicians. This is probably due to the opportunity to practice general ophthalmologyin both the medical and surgical fields, the broad diversity of the patient population and theoption to become subspecialized if one desires.
Like many other specialties, ophthalmology has undergone considerable subspecialization. Thisusually requires a fellowship of one or two years. The common areas of subspecializationinclude Cornea, Vitreoretinal Disease, Glaucoma, Neuro-ophthalmology, Ophthalmic Pathology,Ophthalmic Plastic Surgery and Pediatric Ophthalmology.
Nationally, approximately 90% of applicants obtained a first year position. Experience has shownthat no single factor assures an applicant of obtaining a residency. Academic performance iscertainly one factor. This is measured by college grade point, medical school class rank andgrades, and Standardized Board scores. Letters of recommendation, particularly the Dean'sLetter, are important. Applications are screened to select those to be interviewed Someprograms interview most applicants, while others are very selective. A good interview canovercome deficiencies in other areas and a bad interview can dim an otherwise fine application.It should be emphasized that each residency program weighs these factors differently, someplacing more emphasis on academic, some on research and others on the interview.Ophthalmology uses an early matching system to determine the selections.
16
ORTHOPAEDIC SURGERY
Frederick N. Meyer, M.D., Professor and ChairMedical Park 2, 665-8251
Faculty Advisors to Senior StudentsDr. Frederick N. Meyer ([email protected])Dr. Prasit Nimityongskul ([email protected])
Meeting to Discuss Residency Training in this DisciplineMonday, March 8 at 4:30 p.m. in Resident’s Office, Medical Park 2.If there are any questions, please call the Resident Coordinator at the above number.
Informal Description of the Clinical DisciplineOrthopaedic surgery focuses on the diagnosis and treatment of injured, deformed or diseasedparts of the musculoskeletal system. Specialists in this field employ medicine, surgery andphysical rehabilitation to restore normal function. Orthopaedic surgeons may engage in abroad practice or may focus on a narrower area of special interest, such as hand surgery,sports medicine, joint replacement, spine, foot and ankle and pediatric orthopaedic trauma.
Specialists treat patients of all ages and both sexes, mostly on a short-term basis. Becausemany of their patients have been involved in accidents, orthopaedic surgeons often mustdevote time to assessing disability in legal actions.
Orthopaedic surgeons are mechanically minded, fascinated by tools and gadgets, and enjoy“fixing things”. They find satisfaction in their ability to attain good results relatively quicklyfor most of their patients. They believe their work is fun, challenging, worthwhile, anddemanding. Orthopaedics is a dynamic field with constant updating of techniques andequipment.
Orthopaedics is an extremely competitive specialty. It is difficult, although not impos-sible, for students in the lower two-thirds of their class to get into orthopaedic surgeryresidency programs. It is also important for students to have good Board scores.
Upon completion of residency training, orthopaedists may choose to practice generalorthopaedics or sub-specialize. There are numerous choices of orthopaedic sub-specialtyfellowships, and good residents are very likely to attain a fellowship position in their sub-specialty field of interest.
Currently, there are a variety of orthopaedics practice opportunities in almost any area ofthe country. Income may vary by region, but it is almost always lucrative.
17
OTORHINOLARYNGOLOGY - HEAD AND NECK SURGERY
Frederick M. Silver, M.D., Associate Professor of SurgeryMed Park 1, Suite 101
Faculty Advisors to Senior StudentsDr. Frederick M. Silver([email protected])
Meeting to Discuss Residency Training in this DisciplineSchedule with Department of Surgery - Division of Otorhinolaryngology -Head and Neck Surgery (Call Nan at 660-5776)
Informal Description of the Clinical DisciplineThe field of Otorhinolaryngology - Head and Neck Surgery - involves the structures abovethe clavicle. Several major sensory organs are located in this area: vision, olfaction,hearing, balance and taste. An otolaryngologist prevents the deterioration of the abovefunctions from various pathology, or restores them in patients of all age groups by medicalor surgical means. The otolaryngologist is also involved in the field of communication, bypreserving or restoring hearing, speech, and facial function.
Otorhinolaryngology, as any other field of medicine, emphasizes morphology,pharmacology, pathophysiology, biochemistry, immunology, allergy and neurology relevantto the head and neck. It combines medicine and surgery and is diverse enough to allowindividuals to subspecialize in just one aspect such as allergy, neurotology, facial plastic andreconstructive surgery, rhinology, and head and neck surgery. Some otorhinolaryngologistsprefer to deal primarily with adult patients, while others choose to treat the pediatricpopulation (pediatric otorhinolaryngologist).
An otorhinolaryngologist is expected to be a well-rounded physician with a comprehensivefund of knowledge, not only of the head and neck, but also the remainder of the body. Heor she should be critical and constructive in their thinking, and should practice the specialtywith compassion and understanding.

18
PATHOLOGY
J. Allan Tucker, M.D., Professor and ChairUSAMC, 471-7799
Faculty Advisors to Senior StudentsDr. Carole Boudreaux ([email protected]) Dr. Jacek Polski ([email protected])Dr. Elliot Carter ([email protected]) Dr. Allan Tucker ([email protected])
Meeting to Discuss Residency Training in this Discipline
Tuesday, February 9 at 3:00 p.m. in the Pathology Library at USAMC
Informal Description of the Clinical DisciplineThe practice of pathology involves application of modern technology to the scientific study of diseasein the living patient. Morphological observations are made at the gross, light microscopic and electronmicroscopic level, and specialized laboratory tests utilize a variety of techniques from disciplines suchas chemistry, immunology, and microbiology. New scientific developments are being continuallyintroduced into pathology to enhance diagnostic capabilities. These include techniques such as use ofDNA probes to identify viruses and bacteria, use of monoclonal antibodies to identify cell surfaceantigens by flow cytometry or tumor markers by immunohistochemistry, and gas chromatography-massspectrometry to identify drugs of abuse.
The general field of pathology includes many subspecialty areas. Most pathologists obtain their basiccertification from the American Board of Pathology in Anatomic and Clinical Pathology. AnatomicPathology includes surgical pathology, cytopathology, autopsy pathology, and forensic pathology.Clinical Pathology, sometimes called Laboratory Medicine, encompasses clinical chemistry,hematopathology, immunology, microbiology, and transfusion medicine. Residency training alsoincludes instruction in molecular diagnostic techniques which may be applicable to a variety ofdisciplines within both anatomic and clinical pathology. Because many pathologists' practices includeresponsibility for directing large laboratories, training in management and medical informatics is animportant part of the residency programs.
Board certification in anatomic and clinical pathology requires four years of training in an approvedprogram following graduation from medical school.
Pathologists practice in a variety of environments. Most work in community hospitals and combineanatomic pathology with direction of the clinical laboratories. In medical schools, most pathologistsselect one or two subspecialty areas for their practice, and many conduct related research programs.They also are involved in teaching programs for undergraduate medical students and residents, and theycollaborate in presenting conferences with all of the clinical departments. Some pathologists directindependent laboratories (not hospital-associated), and some pathology group practices provide servicesto several hospitals Pathologists' efforts are directed towards providing all patients with the best medicalcare possible. This is done by supplying clinicians with essential information and expert medicalopinions to assist them in their direct patient care responsibilities. Many medical students are attractedto the field of pathology because it offers the opportunity, which is unique in medicine, for the in-depth,scientific study of the entire spectrum of diseases in all patients.
19
PEDIATRICS
Loran Clement, M.D., Professor and ChairUSA Springhill, Room 5309, 434-3919
Faculty Advisors to Senior StudentsDr. Loran Clement ([email protected]) Dr. Kenneth Rettig ([email protected])Dr. Karen Crissinger ([email protected]) Dr. LaDonna CrewsDr. Benjamin Estrada ([email protected]) Dr. Sheryl Falkos ([email protected])Dr. Franklin Trimm ([email protected]) Dr. Mary Mancao ([email protected])Dr. Felicia Wilson ([email protected]) Dr. Scott Clements ([email protected])Dr. Kathie Savells ([email protected]) Dr. S. Anderson ([email protected])Dr. Samar Bhowmick ([email protected]) Dr. A. Kaulfers ([email protected])Dr. Judy Blair-Elortegui ([email protected])
Meeting to Discuss Residency Training in this DisciplineTuesday, March 2 at 11:00 a.m. in the Neonatology Conference Room at Children’s and Women’sHospital, CWEB 1, with Drs. Clement, Estrada, Rettig, and Trimm (see map on next page)
Informal Description of the Clinical DisciplineThe specialty of Pediatrics combines the intellectual challenge of the practice of medicine and thesatisfaction of helping the children develop to their full potential through preventive medicine andthe guidance of families in child growth and development. When pediatrics first emerged as aclinical discipline, children died from a wide variety of causes, most of which have now beenbrought under control. Today, the largest killer of children from birth through fourteen years of ageis accidents. Birth defects, metabolic-endocrine disease, hereditary diseases, oncology and chronicdiseases have assumed a much greater proportion of the pediatrician's or pediatric subspecialist'stime. The changes in the threats posed to children have dictated changes in the way health care istaught and practiced.
A recent survey of pediatricians conducted by the American Academy of Pediatrics showed anincrease in the frequency of patient visits involving school health problems, behavioral difficultiesand psychosocial counseling as well as the diseases historically associated with the practice ofpediatrics.
Contemporary pediatrics also places increased emphasis on preventive medicine. It views childhealth care as a continuing process, not as a series of acts or examinations performed at prescribedintervals. It demands increased involvement by health professionals in all aspects of child health.
General pediatric training offers a very broad based training that can lead to the practice of generalpediatrics in an urban or rural setting or it can prepare the physician for training in one of the manypediatric subspecialties that include cardiology, neurology, nephrology, gastroenterology, infectiousdisease, endocrinology, critical care, neonatology, allergy and immunology, pulmonology,hematology/oncology, rheumatology, psychiatry, developmental/behavioral pediatrics or adolescentmedicine. Opportunities as practitioners or academicians in all these fields are varied and plentiful.
This is an exciting time. The demands and the challenges are great. But the potential rewards, bothfor children and for the child health professional, are even greater.
20
21
PSYCHIATRY
Kenan Penaskovic, M.D., Psychiatry Clerkship DirectorAltaPointe, 2400 Gordon Smith Drive, Mobile, AL 36617
450-4367
Faculty Advisors to Senior StudentsKenan Penaskovic, M.D.
Meeting to Discuss Residency Training in this DisciplineTuesday, March 2 at 3:00 p.m.BayPointe Hospital Conference Room(5800 Southland Drive, Mobile, AL 36693)
Informal Description of the Clinical DisciplinePsychiatry is the medical discipline that employs medical principles for the evaluation and treatmentof mental disorders. Like other fields of medicine, this requires a thorough understanding of thephysiological, psychological, and socio-cultural components of normal as well as pathologicalmental functioning. The psychological and socio-cultural components are perhaps more importantin Psychiatry than other fields of medicine since the specific pathophysiology of most mentaldisorders is far from being pinpointed. A number of technological advances are on the horizon, butthe psychiatrist must learn to function in a state of uncertainty. The hallmarks of a good psychiatristare flexibility and creativity. Psychiatrists must become expert at utilizing all the available resourcesto assist in maximizing patient recovery. These qualities require a demanding and constant attentionto education beyond the formal residency training years. The residency, then, is designed to teachspecific practice skills as well as skills in investigation and critical thinking.
The two main forms of treatment employed by individual psychiatrists are "somatic" therapy andpsychotherapy. Somatic therapy (including pharmacotherapy and electroconvulsive therapy) is, atthis point, the exclusive domain of duly licensed physicians. Consequently, mastery of thesemodalities is essential. It is highly unusual, though, for psychiatrists not to employpsychotherapeutic techniques as well, either in combination with somatic therapy or alone. Thevariety of psychotherapeutic techniques is great and involves individual, group, and family settings.It is important for psychiatrists to be able to tailor the psychotherapeutic approach to the individualpatient's disorder and circumstances. It is almost impossible for an individual psychiatrist to becomeskilled in providing all the psychotherapeutic techniques. It is crucial, however, to understand thedifferences among them and be prepared to refer patients to appropriate experts when indicated.
Several subspecialty areas of Psychiatry have emerged. Child and Adolescent Psychiatry has beenin existence the longest. It requires two years of training in an approved program to become eligibleto take specific certification examination. Psychiatrists must pass the certification exam in generalpsychiatry before being eligible for the Child and Adolescent certification exam, though full trainingin general psychiatry is also required. The American Board of Psychiatry and Neurology also nowoffers examinations for "added qualifications" in geropsychiatry, substance use disorders, andforensic psychiatry. Other organizations offer examinations in administrative psychiatry, etc. Someof these require extra training beyond the standard approved residency. It should be understood,however, that nothing precludes the trained general psychiatrist from practicing fully in these specialareas of interest.
Psychiatrists rank at the top among physicians regarding satisfaction with their specialty choice.Psychiatry continues to be among the most family friendly specialties. On average, psychiatristswork among the least hours per week, but earn a salary above the average primary care physician.
22
RADIATION ONCOLOGY
John R. Russell, M.D.Chief, Radiation Oncology Services
USA Mitchell Cancer Institute, Terrace Level, Radiation Oncology445-9615
Faculty Advisors to Senior StudentsDr. John Russell
Meeting to Discuss Residency Training in this DisciplinePlease call and make an appointment (call Kathy at 445-9819)
Informal Description of the Clinical DisciplineRadiation Oncology (also known as Radiation Therapy) is the field of Medicine which dealswith the use of ionizing radiation as a medical treatment modality. Included in this field isthe evaluation, treatment and follow-up of patients. The field also includes usage ofchemical and biologic modifiers of ionizing radiations.
There are 68 Radiation Oncology residency programs which provide four years of trainingbeginning in PGY 2. Residents are usually scheduled on three month rotations to include allanatomical sites in addition to brachytherapy and remote afterloading, as well as radiationphysics, radiobiology, intra operative and hyperthermic therapy. The resident rotatesthrough other oncology subspecialties in order to obtain a broad understanding of oncology.
A separate matching program exists for students in this discipline.
23
RADIOLOGY
Jeffrey C. Brandon, M.D., Interim Chair and ProfessorUSAMC Mastin 315, 471-7879
Faculty Advisors to Senior StudentsJeffrey C. Brandon, M.D. ([email protected])Samuel A. McQuiston, M.D. ([email protected])
Meeting to Discuss Residency Training in this DisciplineTuesday, February 23 at 3:30 p.m. in the Richards Room, second floor USAMC, with Dr.McQuiston. (This is a combined meeting with Nuclear Medicine).
Informal Description of the Clinical DisciplineAs is evident to any reader of the weekly clinical pathologic conferences in the NewEngland Journal of Medicine, Radiology has assumed an increasingly important role inclinical medicine. In the past Radiology was confined to plain film examination of thechest, abdomen, skull, spine, and extremities as well as barium contrast examination of theG.I. tract, and intravenous contrast of the G.U. system. Today, new imaging modalities andprocedures have considerably expanded the role of radiology in diagnosis, treatment, andscreening.
Radiology consists of a group of sub-specialties. Although radiologists in private practicemay cover many or most aspects of these specialties, they do specialize to some extent. Areas/techniques of specialty include Neuroradiology, Cardiovascular/InterventionalRadiology, Ultrasound, Computer Tomography (CT), Mammography, Pediatric Radiology,Magnetic Resonance Imaging (MRI), Nuclear Medicine, and Muskuloskeletal Imaging.
The qualities necessary to make a good radiologist include acute visual perception andability to make a differential diagnosis. Since a good portion of residency training includesradiologic physics, ability in the physical sciences is also important.
Following 1997, a clinical internship year is required by the American Board of Radiology.The period of radiology residency is four years.
Following the residency, one or two-year fellowships are available in subspecialty areassuch as Pediatric Radiology, Cardiovascular/Interventional Radiology, Neuroradiology, orUltrasound/CT/MRI for those desiring greater knowledge in these areas. The job market inRadiology is excellent. There is a shortage of radiologists. Recent graduates of USA’sRadiology program have had little or no difficulty obtaining a desirable practice and/orfellowship opportunities. Most radiologists enter hospital practice or group practice. Among the medical and surgical specialties, radiologists probably fall in the mid to upperrange monetarily, and selected residents are usually from the top quartile of their medicalschool class.
24
SURGERY
William O. Richards, M.D., F.A.C.S., Professor and ChairDepartment of Surgery, Mastin 721, 471-7993, ([email protected])
Patrick L. Bosarge, Jr., M.D., Program Director, Assistant ProfessorDepartment of Surgery, Mastin 706, 471-7197, ([email protected])
Faculty Advisors to Senior StudentsDr. Michael F. Damrich - Vascular Dr. Dimitris K. Kyriazis - VascularDr. Celeste N. Hollands - Pediatric Surgery Dr. Arnold Luterman - BurnDr. Gerhard A. W. Boehm - General Dr. Carl Maltese - VascularDr. Patrick L. Bosarge, Jr. - General Dr. David H. Mull - VascularDr. Donna Lynn Dyess - General Dr. Ronald O’Gorman - VascularDr. C. Neal Ellis, Jr. - Colorectal Dr. G. Travis Paul - GeneralDr. Karen J. Frye - Burn Dr. Lee Thompson - OncologyDr. Roy Gandy - General Dr. Daniel Beals - Pediatric SurgeryDr. J. N. Gavras - General Dr. Paul Rider - ColorectalDr. Richard Gonzalez - Traumatology Dr. Charles B. Rodning - GeneralDr. Curtis N. Harris - Plastic/Reconstructive Dr. William R. Higgs - VascularDr. Frederick M. Silver - Head/Neck Dr. Juvonda S. Hodge - GeneralDr. C. B. Smith - General Dr. Albert L. Kline - General
Meeting to Discuss Residency Training in this DisciplineTuesday, February 9 at 1:00 p.m. in the Mastin Building, 7th floor conference room. This is a combinedmeeting with Ophthalmology and Urology. Call 471-7990 if you have any questions.
Informal Description of the Clinical DisciplineThe discipline of surgery encompasses many fields. General Surgery Residency requires a minimum offive years of graduate training. Several subspecialties require completion of a General SurgeryResidency prior to subspecialty training (e.g. Cardiothoracic Surgery, Vascular Surgery, PediatricSurgery). Other subspecialties require one to two years of General Surgery training. General SurgeryResidency is a rigorous but exciting experience. Over the course of the residency, progressiveresponsibility is given to the trainee. During the five years, the residents gain exposure to a broadspectrum of surgical and nonsurgical diseases. Although acquisition of technical skills is important, thetime and experience required to develop mature clinical judgment is the reason for a five year program.
Most surgeons would agree that there is tremendous immediate and tangible satisfaction in the successfuloutcome of a well performed operative procedure. Surgical decision making is both an art and a scienceand demands a constant updating of current knowledge as well as the ability to put that knowledge topractical clinical use. Surgery incorporates proven practices while at the same time fosteringtechnological innovation.
In these days of financial turmoil in the medical world as well as reorganization of the delivery of healthcare, medical students are often plagued by doubts as to their future education in medicine. However, asthe science and art of clinical surgery are further refined, the rewards of surgical practice in terms ofpersonal satisfaction as well as patient appreciation will remain great. These rewards are unique to thefield and will remain unscathed by future economic and political events. The foundation of surgery issolid and the future is bright.
25
UROLOGICAL SURGERY
William O. Richards, M.D., F.A.C.S., Professor and ChairDepartment of Surgery, Mastin 721, 471-7993, ([email protected])
Roy E. Gandy, M.D., ProfessorDepartment of Surgery, Mastin 717, 471-7974, ([email protected])
Meeting to Discuss Residency Training in this DisciplineTuesday, February 9 at 1:00 p.m. in the Mastin Building, 7th floor conference room. This isa combined meeting with Surgery and Ophthalmology. Call 471-7990 if you have anyquestions.
Informal Description of the Clinical DisciplineUrology is the specialty involved with the male and female genitourinary tract. It is primarilya surgical discipline but is broad enough to interact with a variety of other disciplines:nephrology, oncology, endocrinology, behavioral science, and neurology. During the last twodecades, a notable shift from structure to function has occurred in the diagnosis and treatmentof such problems as male sexual dysfunction, voiding disorders, benign prostatic hyperplasia,and female incontinence.
Traditionally, urologists were distinguished by their use of diagnostic and therapeuticinstrumentation of the genitourinary tract. Recent developments in the field of urologicinstrumentation such as extracorporeal shock wave lithotripsy, laparoscopy, and lasertechnology have replaced open surgery in the treatment of various urologic disorders, primarilyin the treatment of stone disease. Nevertheless, abdominal, pelvic and retroperitoneal surgeryis a prominent feature in the treatment of urologic cancers and in reconstruction of the urinarytract. Therefore, the student planning a career in urology will recognize the important roles ofbasic science, clinical medicine, urotechnology, and operative technique in the diagnosis andtreatment of urologic pathology.
Future manpower trends in urology portend favorably to a career choice. Despite the diffusionof urologic procedures into other specialties, the role of the urologist will be increasinglydemanded particularly as the field of geriatric medicine emerges. A decrease in the totalnumber of urology residency positions currently available requires that students gain earlyexposure to urology during their clinical rotations and submit applications to residencyprograms in a timely manner. As a constantly evolving field, urology provides both thepractitioner and academician with challenges and rewards of treating patients by a variety ofmodalities.