cardiovascular health and menopause a cme slide library from the council on hormone education
TRANSCRIPT
Cardiovascular Health and Menopause
A CME Slide Library From the
Council on Hormone Education
Cardiovascular Health and Menopause
Section 1: IntroductionSection 2: Cardiovascular Effects of EstrogenSection 3: Clinical Trials of Hormone Therapy (HT) and
Cardiovascular Outcomes3a. HERS3b. ERA3c. WAVE3d. ESPRIT3e. WELL-HART3f. PHASE3g. EPAT3h. WHI
Section 4: Timing of HT InitiationSection 5: Summary and Conclusions

Section 1:
Introduction
Cardiovascular Health and Menopause
Impact of Cardiovascular Disease (CVD) in Women
Single largest killer of American women
– About 500,000 women die annually from CVD
More women than men die each year from CVD
In women, CVD-related deaths exceed the next 7 causes of death combined
One woman dies of CVD ~ every minute 2/3 of women who die had no prior symptoms
American Heart Association. Heart Disease and Stroke Statistics–2004 Update. 2004:1-50.

National Center for Health Statistics. 1999:164-7.
Mortality Rates in WomenAt Every Age, More Women Die of Heart Disease Than Breast Cancer
Coronary Artery Disease
Stroke
Lung Cancer
Breast Cancer
Colon Cancer
Endometrial Cancer
Age (years)
Mo
rtal
ity
Rat
e p
er 1
00,0
00
6500
4500
2500
1600
1200
800
400
075–7970–7465–6960–6455–5950–5445–49 80–84 85+
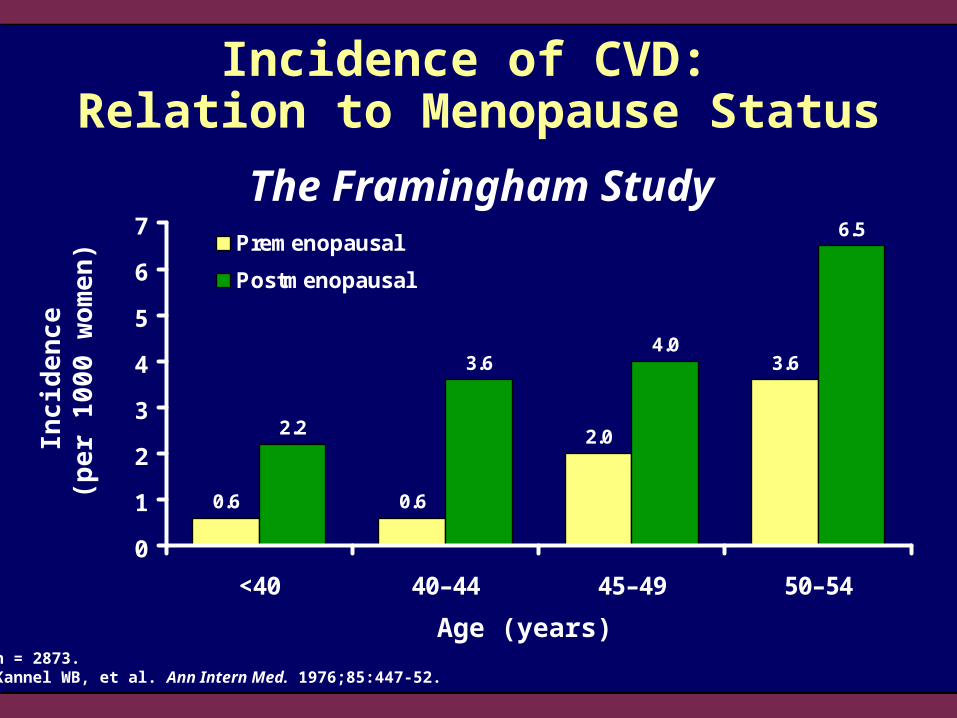
0.6 0.6
2.0
3.6
2.2
3.64.0
6.5
0
1
2
3
4
5
6
7
<40 40–44 45–49 50–54
Premenopausal
Postmenopausal
Incidence of CVD: Relation to Menopause Status
Inci
den
ce
(p
er
10
00
wo
men
)
Age (years)n = 2873.Kannel WB, et al. Ann Intern Med. 1976;85:447-52.
The Framingham Study
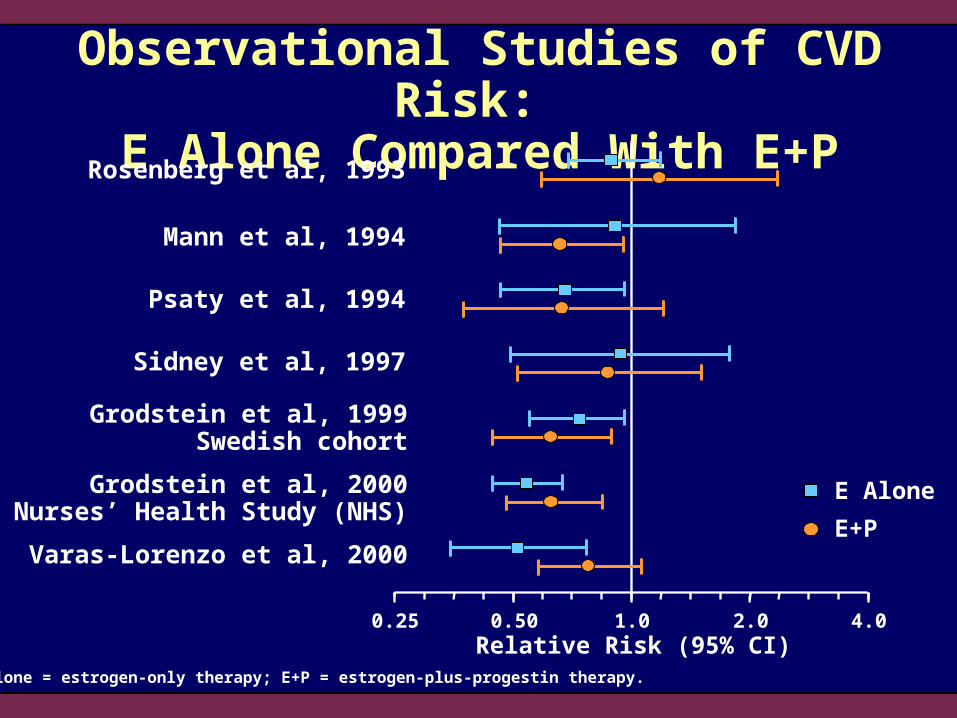
Observational Studies of CVD Risk: E Alone Compared With E+P
0.25 0.50 1.0 2.0 4.0
Grodstein et al, 1999Swedish cohort
Grodstein et al, 2000Nurses’ Health Study (NHS)
Varas-Lorenzo et al, 2000
Relative Risk (95% CI)
E Alone
E+P
Rosenberg et al, 1993
Mann et al, 1994
Psaty et al, 1994
Sidney et al, 1997
E alone = estrogen-only therapy; E+P = estrogen-plus-progestin therapy.

Section 2:Cardiovascular Effects
of Estrogen
Cardiovascular Health and Menopause
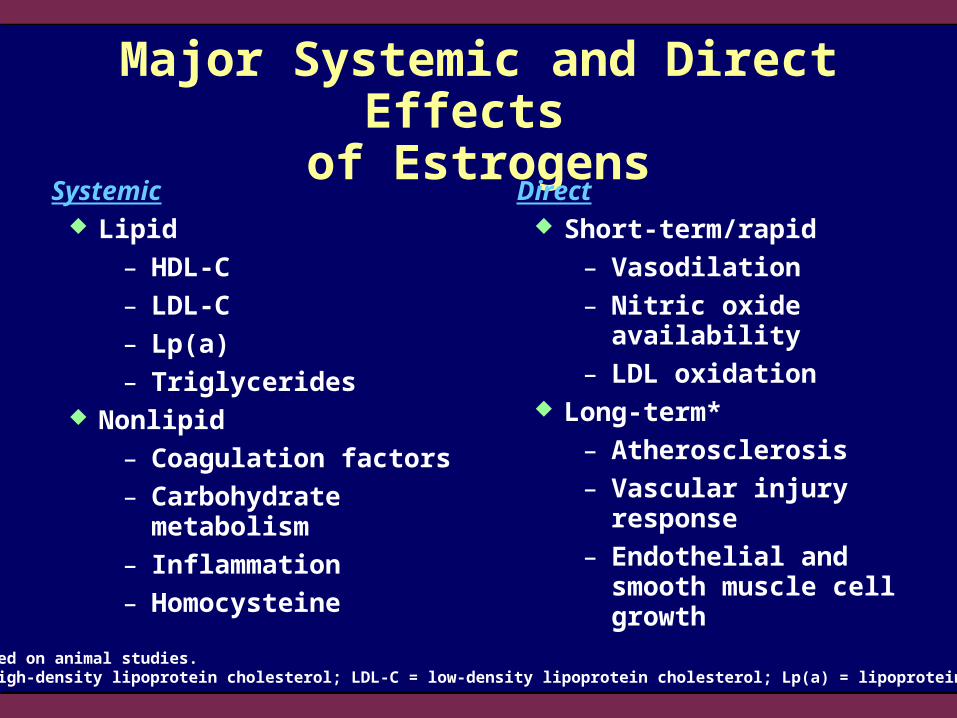
*Data based on animal studies.HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; Lp(a) = lipoprotein(a).
Major Systemic and Direct Effects of Estrogens
Systemic Lipid
– HDL-C
– LDL-C
– Lp(a)
– Triglycerides Nonlipid
– Coagulation factors
– Carbohydrate metabolism
– Inflammation
– Homocysteine
Direct Short-term/rapid
– Vasodilation
– Nitric oxide availability
– LDL oxidation Long-term*
– Atherosclerosis
– Vascular injury response
– Endothelial and smooth muscle cell growth

Adapted from Mendelsohn ME, Karas RH. N Engl J Med. 1999;340:1801-11. ©1999 Massachusetts Medical Society. All rights reserved.
Endothelial cells
Smooth-musclecells
Estrogen
Rapid Effects Without alteration ofgene expression
Long-Term Effects
Related to alterationof gene expression
Direct Effects of Estrogen on Arterial Vessels
Section 3:Clinical Trials of Hormone
Therapy (HT) and Cardiovascular Outcomes
Cardiovascular Health and Menopause

Section 3a:
Heart and Estrogen/progestin
Replacement Study
(HERS)

Heart and Estrogen/progestin Replacement Study (HERS)
Study Design:Randomized, double-blind, placebo- controlled, secondary prevention trial
Subjects:2763 postmenopausal women, <80 years old (mean age, 66.7 years) with CAD
Intervention:CEE 0.625 mg + MPA 2.5 mg daily or placebo
Follow-up:HERS I, 4.1 years HERS II, open-label 2.7 years
1° Endpoint:Nonfatal MI or CHD death
CAD = coronary artery disease; CEE = conjugated equine estrogen; MPA = medroxyprogesterone acetate; MI = myocardial infarction; CHD = coronary heart disease.Hulley S, et al. JAMA. 1998;280:605-13.Grady D, et al. JAMA. 2002;288:49-57.
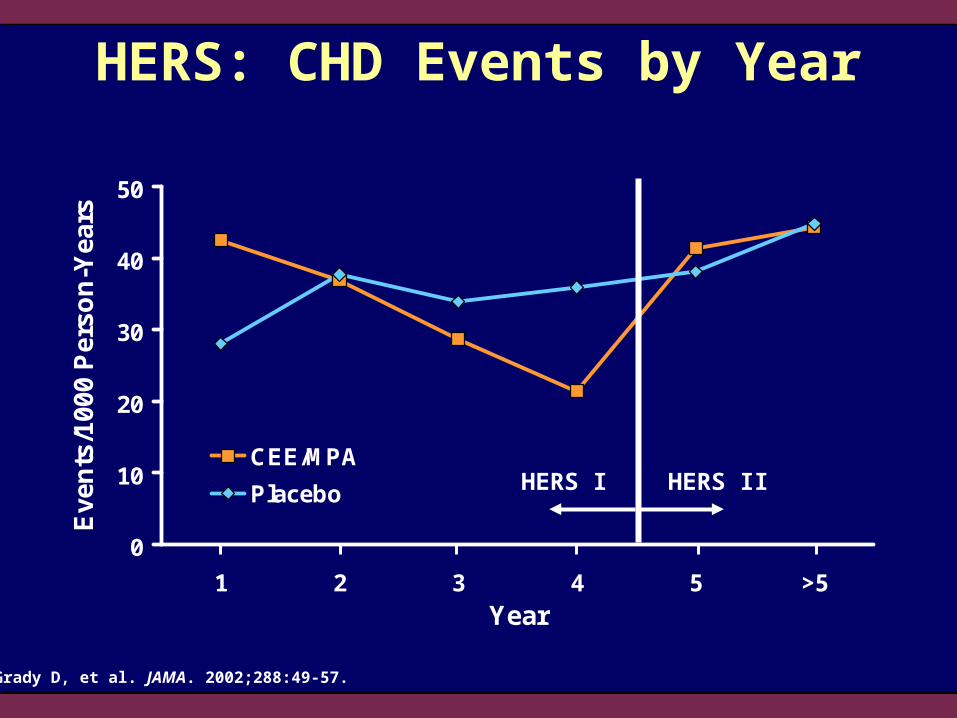
HERS: CHD Events by Year
0
10
20
30
40
50
1 2 3 4 5 >5Year
Eve
nts
/100
0 P
erso
n-Y
ears
CEE/MPA
Placebo HERS I HERS II
Grady D, et al. JAMA. 2002;288:49-57.
0
5
10
15
20
0 1 2 3 4 5
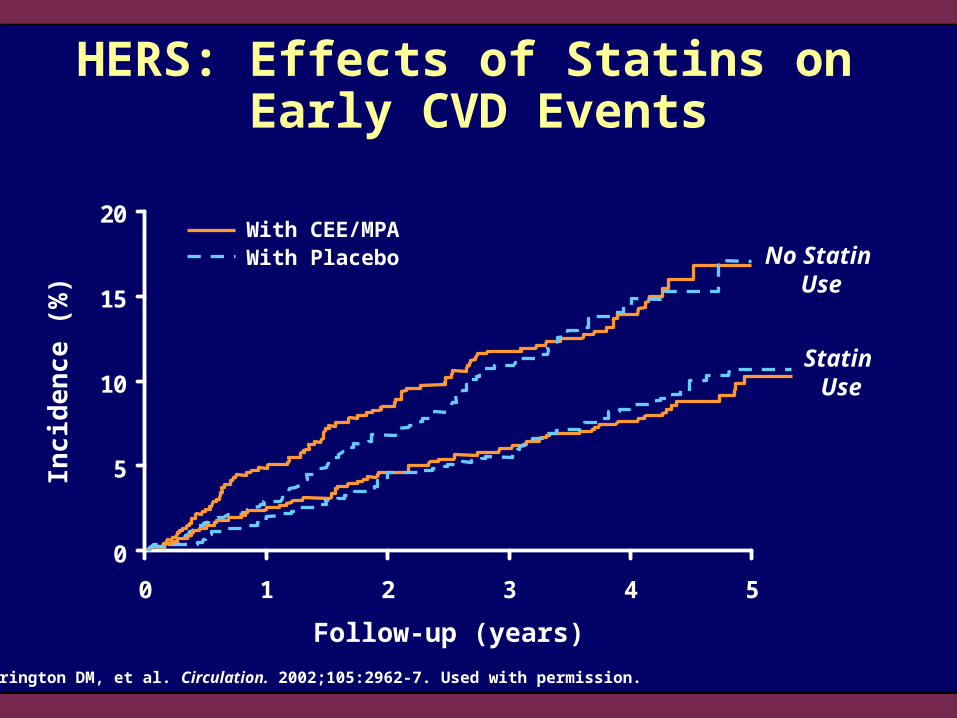
HERS: Effects of Statins on Early CVD Events
Herrington DM, et al. Circulation. 2002;105:2962-7. Used with permission.
Inci
den
ce
(%
)
No Statin Use
Statin Use
With CEE/MPAWith Placebo
Follow-up (years)

HERS: Summary CEE/MPA in postmenopausal women with
established CHD did not reduce the overall risk of MI and CHD death
CEE/MPA significantly increased risk of events in the first year followed by a significant reduction in Years 4 and 5
In HERS II, the reduction in events did not continue
As previously shown, venous thrombo- embolic events were significantly increased with CEE/MPA

Hulley S, et al. JAMA. 1998;280:605-13.Grady D, et al. JAMA. 2002;288:49-57.Blumenthal RS, et al. Am J Cardiol. 2000;85:1015-7.
HERS: Lessons Learned
Women were on average 18 years postmenopause, suggesting that years since menopause may have an important influence on the cardiovascular effects associated with initiation of E+P
Cardiovascular risks of E+P in this population were observed early and did not occur in individuals taking concomitant statin therapy
Section 3b:
Estrogen Replacement and
Atherosclerosis (ERA) Study

Postmenopausal women with >30% coronary artery stenosis
Mean follow-up, 3.2 years
Angiographic follow-up in 248 patients
Mean cholesterol, 216 mg/dL
Compliance: 86% placebo, 84% E+P, 74% E alone
CEE only(0.625 mg)
n = 100
CEE (0.625 mg)+
MPA (2.5 mg)n = 104
Placebon = 105
Estrogen Replacement and Atherosclerosis (ERA) Study
Herrington DM, et al. N Engl J Med. 2000;343:522-9.
randomization
309Women
With Documented Coronary Artery
Stenosis(mean age, 65 years)

P = .38-0.16
-0.14
-0.12
-0.10
-0.08
-0.06
-0.04
-0.02
0.00
Placebo CEE CEE + MPA
Pro
gre
ssio
no
f Ath
eros
clero
sis
ERA Study: Change in Minimal Lumen Diameter
*Adjusted for length of follow-up, location of segment, clinic, and use of lipid-lowering therapy.Herrington DM, et al. N Engl J Med. 2000;343:522-9.
Ad
just
ed
Ch
ang
e in
Min
ima
l L
um
en
Dia
me
ter
Fro
m B
ase
line
*
(n = 79) (n = 85) (n = 84)
P = .97
Herrington DM, et al. N Engl J Med. 2000;343:522-9.
ERA Study: Summary
Neither CEE alone nor CEE plus MPAaffected the progression of coronary atherosclerosis in women with angiographically documented coronary artery stenosis who were on average 23 years postmenopausal
These findings are consistent with those of HERS

Section 3c:
Women’s Angiographic
Vitamin and Estrogen
(WAVE) Trial
Study Design:Randomized, double-blind, placebo-controlled trial
Subjects:423 postmenopausal women with at least one 15% to 75% coronary stenosis; mean age, 65 years
Intervention:CEE 0.625 mg + MPA 2.5 mg daily, or placebo; or vitamins E and C, or placebo
Follow-up:2.8 years (average)
1° Endpoint:Annualized mean change in minimum lumen diameter by quantitative coronary angiography
Women’s Angiographic Vitamin and Estrogen (WAVE) Trial
Waters DD, et al. JAMA. 2002;288:2432-40.

Lack of Effect of CEE/MPA and Antioxidant Vitamin Supplements on Progression of Coronary
Artery Atherosclerosis: WAVE Results
-0.07
-0.06
-0.05
-0.04
-0.03
-0.02
-0.01
0
0.01
Ch
ang
e/Y
ear
in M
inim
um
Lu
men
D
iam
eter
(m
ean
± S
E,
mm
)
Placebo/Placebon = 87
E+P/Placebon = 77
Placebo/Vitamins
n = 71
E+P/Vitamins
n = 85
Pro
gressio
no
f Ath
erosclero
sis
Waters DD, et al. JAMA. 2002;288:2432-40.
P = .30
Section 3d:
Oestrogen in the Prevention of
Reinfarction Trial (ESPRIT)

Oestrogen in the Prevention of Reinfarction Trial (ESPRIT)
Study Design:Randomized, double-blind, placebo- controlled, secondary prevention trial
Subjects:1017 postmenopausal women,
50 to 69 years old (mean age, 62.6 years) with CAD
Intervention:Estradiol valerate 2 mg daily or placebo
Follow-up:2 years
1° Endpoint:Reinfarction or cardiac death and all-cause mortality
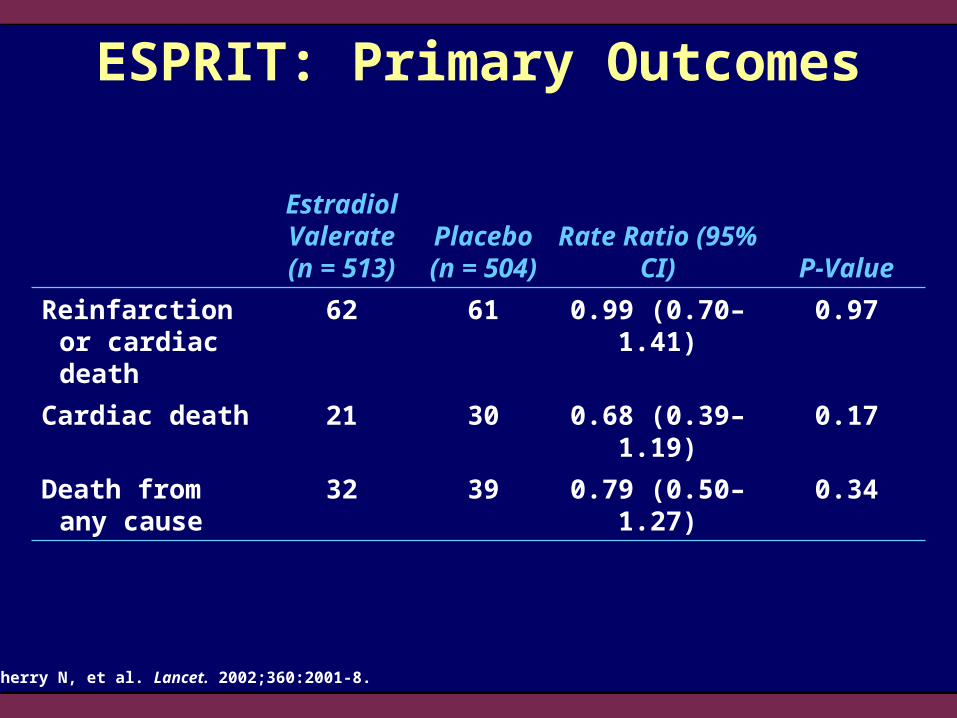
Cherry N, et al. Lancet. 2002;360:2001-8.
Cherry N, et al. Lancet. 2002;360:2001-8.
ESPRIT: Primary Outcomes
Estradiol Valerate(n = 513)
Placebo(n = 504)
Rate Ratio (95% CI) P-Value
Reinfarction or cardiac death
62 61 0.99 (0.70–1.41) 0.97
Cardiac death 21 30 0.68 (0.39–1.19) 0.17
Death from any cause
32 39 0.79 (0.50–1.27) 0.34
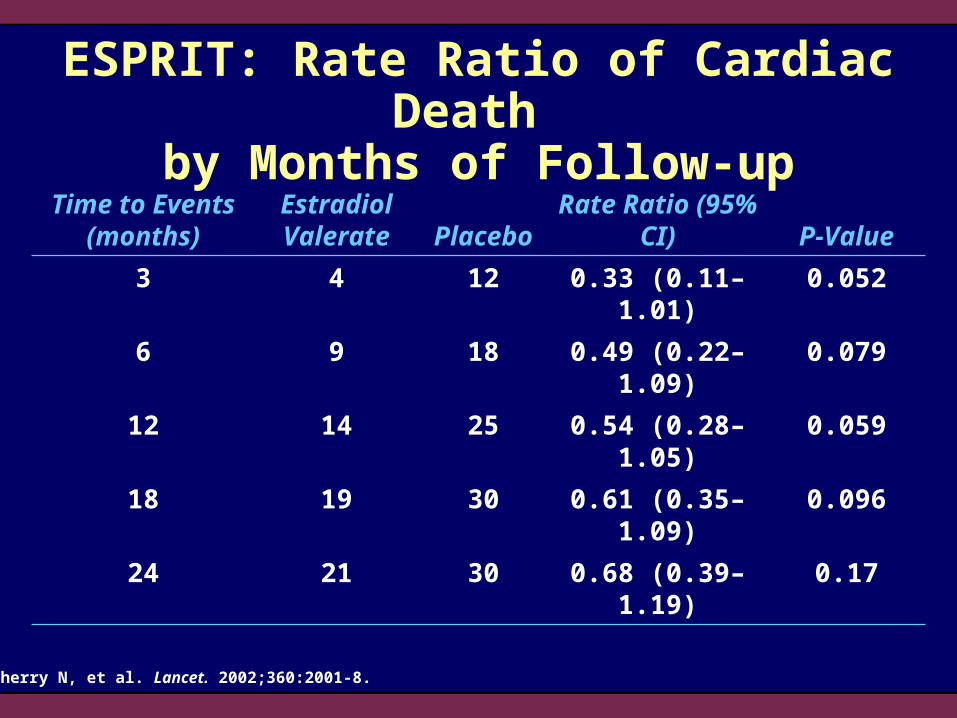
ESPRIT: Rate Ratio of Cardiac Death by Months of Follow-up
Cherry N, et al. Lancet. 2002;360:2001-8.
Time to Events (months)
Estradiol Valerate Placebo
Rate Ratio (95% CI) P-Value
3 4 12 0.33 (0.11–1.01) 0.052
6 9 18 0.49 (0.22–1.09) 0.079
12 14 25 0.54 (0.28–1.05) 0.059
18 19 30 0.61 (0.35–1.09) 0.096
24 21 30 0.68 (0.39–1.19) 0.17

Time to Events (months)
Estradiol Valerate Placebo
Rate Ratio (95% CI) P-Value
3 8 14 0.56 (0.29–1.33) 0.19
6 14 20 0.68 (0.34–1.35) 0.27
12 20 30 0.65 (0.37–1.14) 0.13
18 27 39 0.67 (0.41–1.10) 0.11
24 32 39 0.79 (0.50–1.27) 0.34
ESPRIT: Rate Ratio of Any Death by Months of Follow-up
Cherry N, et al. Lancet. 2002;360:2001-8.

Section 3e:
Women’s Estrogen-progestin
Lipid-Lowering Hormone
Atherosclerosis Regression Trial
(WELL-HART)
Hodis HN, et al. N Engl J Med. 2003;349:535-45.
Women’s Estrogen-progestin Lipid-Lowering Hormone Atherosclerosis Regression Trial
(WELL-HART)
Study Design
Randomized, double-blind, placebo-controlled trial
226 postmenopausal women with CAD (mean age, 63.5 years)
Oral 17-estradiol (1 mg/d), taken with or without 5 mg MPA administered 12 days/month, or usual care
Median follow-up = 3.3 years
LDL-C reduced to <130 mg/dL by diet and lipid-lowering therapy
Primary Outcome
Average change in percent stenosis measured by quantitative coronary angiography

0
1
2
3
Usual Care Estradiol Estradiol +Sequential MPA
Ch
ang
e in
% S
ten
osi
s ±
SE
WELL-HART: Change in Percent Stenosis
Pro
gre
ssio
n
P = NS
n = 76n = 76
n = 74
Hodis HN, et al. N Engl J Med. 2003;349:535-45.

Ch
an
ge
in M
inim
al L
um
ina
l D
iam
ete
r (m
m)
± S
E
-0.2
-0.1
0
Usual Care Estradiol Estradiol +Sequential MPA
WELL-HART: Change in Minimal Luminal Diameter
Hodis HN, et al. N Engl J Med. 2003;349:535-45.
Pro
gre
ssio
n
P = NS
n = 76 n = 76n = 74

Section 3f:
Papworth HRT
Atherosclerosis Study
(PHASE)

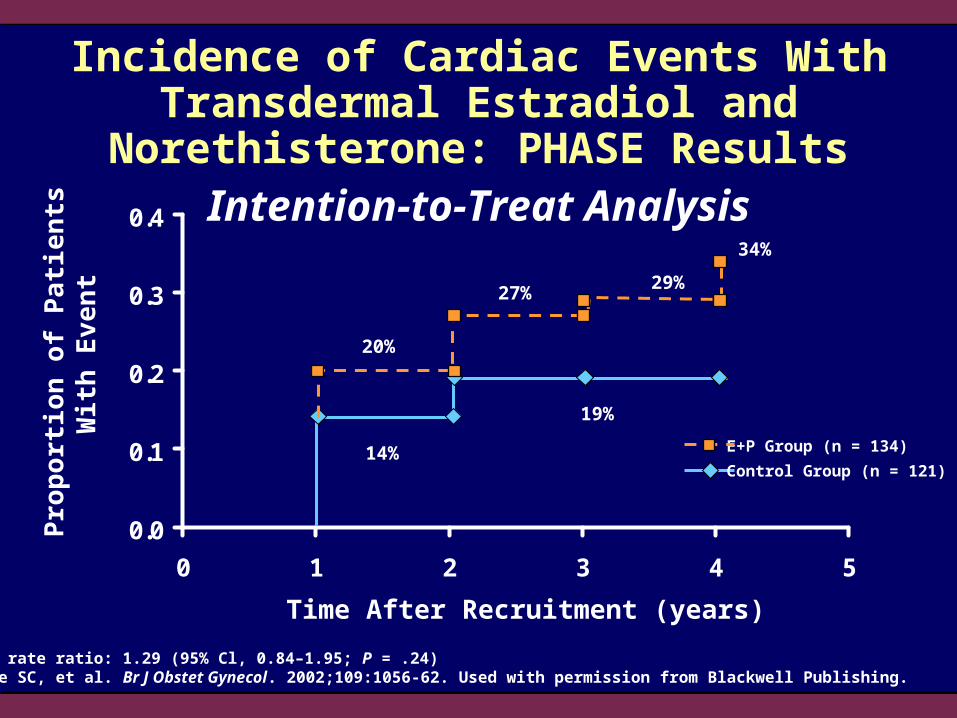
Papworth HRT Atherosclerosis Study (PHASE)
Study Design:Randomized, prospective trial
Subjects:Postmenopausal women with one or more coronary stenoses 50%; mean age, 66 to 67 years
Intervention:Transdermal estradiol 80 for 14 daysTransdermal estradiol 80/norethisterone 120 for 14 days(all doses g/patch/day) (n = 134)
Placebo control (n = 121)
Mean Follow-up:30.8 months
1° Outcome:Proven MI, cardiac death, or admission to hospital with unstable angina
Clarke SC, et al. Br J Obstet Gynecol. 2002;109:1056-62.
0.0
0.1
0.2
0.3
0.4
0 1 2 3 4 5
Incidence of Cardiac Events With Transdermal Estradiol and Norethisterone: PHASE Results
Event rate ratio: 1.29 (95% Cl, 0.84–1.95; P = .24)Clarke SC, et al. Br J Obstet Gynecol. 2002;109:1056-62. Used with permission from Blackwell Publishing.
Pro
po
rtio
n o
f P
ati
ents
W
ith
Ev
en
t
Time After Recruitment (years)
14%
19%
20%
27%29%
34%
E+P Group (n = 134)
Control Group (n = 121)
Intention-to-Treat Analysis
Section 3g:
Estrogen in the Prevention of
Atherosclerosis Trial
(EPAT)
IMT = intima-media thickness.Hodis HN, et al. Ann Intern Med. 2001;135:939-53.
Estrogen in the Prevention of Atherosclerosis Trial (EPAT)
Study Design Randomized, double-blind, placebo-controlled trial 222 apparently healthy postmenopausal women
(mean age, ~61 years) No pre-existing CVD and LDL-C levels 130 mg/dL Micronized 17-estradiol (1 mg/d) or placebo
for 2 years Lipid-lowering drugs given if LDL-C exceeded
160 mg/dLPrimary Outcome Rate of change in carotid artery IMT
-0.005
0
0.005
0.01
0.015
0.02
Rat
e o
f IM
T C
han
ge
(mm
/yea
r) PlaceboEstradiol
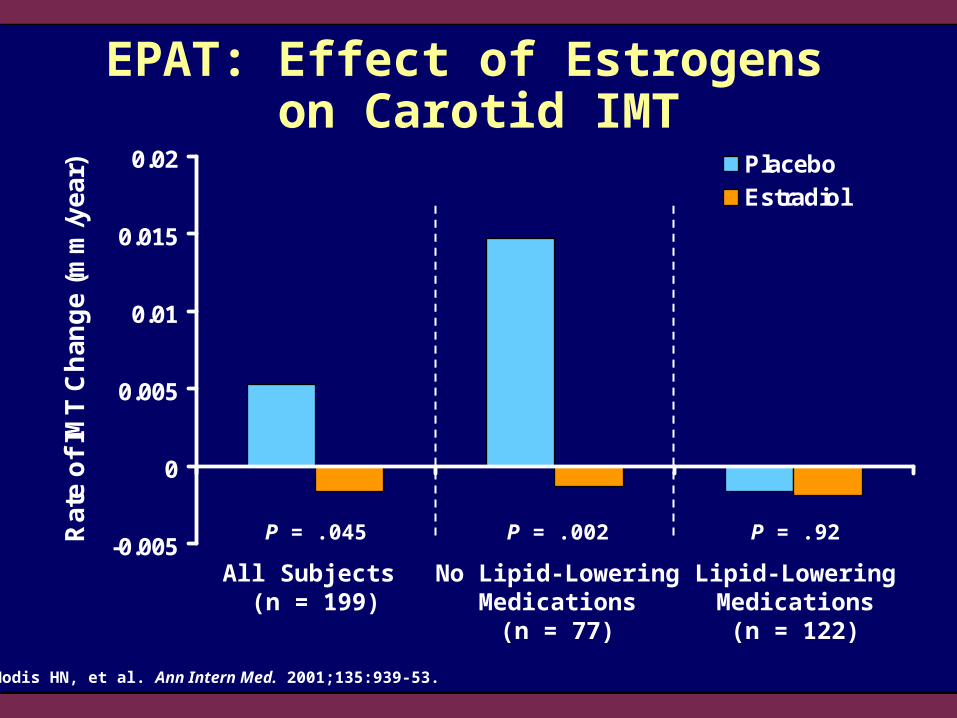
EPAT: Effect of Estrogens on Carotid IMT
All Subjects (n = 199)
No Lipid-LoweringMedications
(n = 77)
Lipid-LoweringMedications
(n = 122)
Hodis HN, et al. Ann Intern Med. 2001;135:939-53.
P = .045 P = .002 P = .92

EPAT: Summary
Primary finding: women randomized to unopposed micronized 17-estradiol had a significant reduction in the progression of subclinical atherosclerosis compared with women randomized to placebo
The results from EPAT are consistent with the more than 20 observational studies that indicate that postmenopausal women who use E alone have lower rates of CHD than postmenopausal women who do not use E alone
Hodis HN, et al. Ann Intern Med. 2001;135:939-53.

Section 3h:
Women’s Health Initiative
(WHI)

Women’s Health Initiative (WHI)
Study Design:Randomized, double-blind, placebo-controlled trial
Subjects:16,608 postmenopausal women without vasomotor symptoms 50 to 79 years old (mean age, 63.3 years)
Intervention:CEE 0.625 mg + MPA 2.5 mg daily or placebo
Follow-up:5.6 years (average)—terminated early (8.5 years planned)
1° Endpoint:Nonfatal MI or CHD death
Manson JE, et al. N Engl J Med. 2003;349:523-34.
CEE/MPA Arm

Definition of Endpoints for WHI Primary outcome: CHD events
(nonfatal MI and CHD death) Primary adverse outcome: invasive
breast cancer Global index:
– CHD event (nonfatal MI, CHD death)– Breast cancer– Stroke– Pulmonary embolism (PE)– Endometrial cancer– Colorectal cancer– Hip fracture– Death due to other causes
Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33.

WHI: Baseline Characteristics
*Values are means; †Overall incidence of prior CVD = 7.7%; ‡P = .04 vs CEE/MPA.BMI = body mass index; CABG/PTCA = coronary artery bypass graft/percutaneous transluminal coronary angioplasty.Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33.
CharacteristicCEE/MPA (n = 8506)
Placebo (n = 8102)
Age at screening, years* 63.2 63.3
Prior hormone use, % 26.1 25.6
BMI, kg/m2* 28.5 28.5
Never smokers, % 49.6 50.0
Diabetes, % 4.4 4.4
Hypertension, % 35.7 36.4
Statin use at baseline, % 6.9 6.8
Family history breast cancer, % 16.0 15.3
History of MI, %† 1.6 1.9
History of CABG/PTCA, %† 1.1 1.5‡

Age Groups
Data are number (%) of patients; CEE/MPA and placebo groups were similar.Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33.
WHI: Baseline Characteristics
Age Group at Screening
CEE/MPA (n = 8506)
Placebo (n = 8102)
50–59 years 2839 (33.4) 2683 (33.1)
60–69 years 3853 (45.3) 3657 (45.1)
70–79 years 1814 (21.3) 1762 (21.7)

WHI: Statistical Analyses
Primary analyses: time-to-event analyses based on intention to treat
Outcome comparisons presented as hazard ratios (HR) with nominal and adjusted 95% CIs
Nominal CI (nCI): describes variability in risk estimates that would result from a trial with a single outcome
– Used for primary outcomes (CHD, breast cancer) and global index
Adjusted CI (aCI): variability of risk estimates corrected for multiple comparisons
– Used for all other outcomes
Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33.

EventOverall
HR
Confidence Intervals
Increased Absolute Risk
per 10,000 Women/Year
Increased Absolute Benefit
per 10,000 Women/Year
95% Nominal
95% Adjusted
CHD 1.29 1.02–1.63 0.85–1.97 7
Strokes 1.41 1.07–1.85 0.86–2.31 8
Breast cancer 1.26 1.00–1.59 0.83–1.92 8
VTE 2.11 1.58–2.82 1.26–3.55 18
Colorectal cancer 0.63 0.43–0.92 0.32–1.24 6
Hip fractures 0.66 0.45–0.98 0.33–1.33 5
Total fractures 0.76 0.69–0.85 0.63–0.92 44
Absolute and Relative Risk or Benefit of CEE/MPA
VTE = venous thromboembolism.Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33.
WHI: Statistical Analyses

Cauley JA, et al. JAMA. 2003;290:1729-38; Chlebowski RT, et al. JAMA. 2003;289:3243-53; Manson JE, et al. N Engl J Med. 2003;349:523-34; Wassertheil-Smoller S, et al. JAMA. 2003;289:2673-84; Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33.
WHI: Revised ResultsAbsolute and Relative Risk or Benefit of CEE/MPA
EventOverall
HR
Confidence Intervals
Increased Absolute Risk
per 10,000 Women/Year
Increased Absolute Benefit
per 10,000 Women/Year
95% Nominal
95% Adjusted
CHD 1.24 1.00–1.54 0.97–1.60 6
Strokes 1.31 1.02–1.68 0.93–1.84 7
Breast cancer 1.24 1.01–1.54 0.97–1.59 8
VTE 2.11 1.58–2.82 1.26–3.55 18
Colorectal cancer 0.63 0.43–0.92 0.32–1.24 6
Hip fractures 0.67 0.47–0.96 0.41–1.10 5
Total fractures 0.76 0.69–0.83 — 47
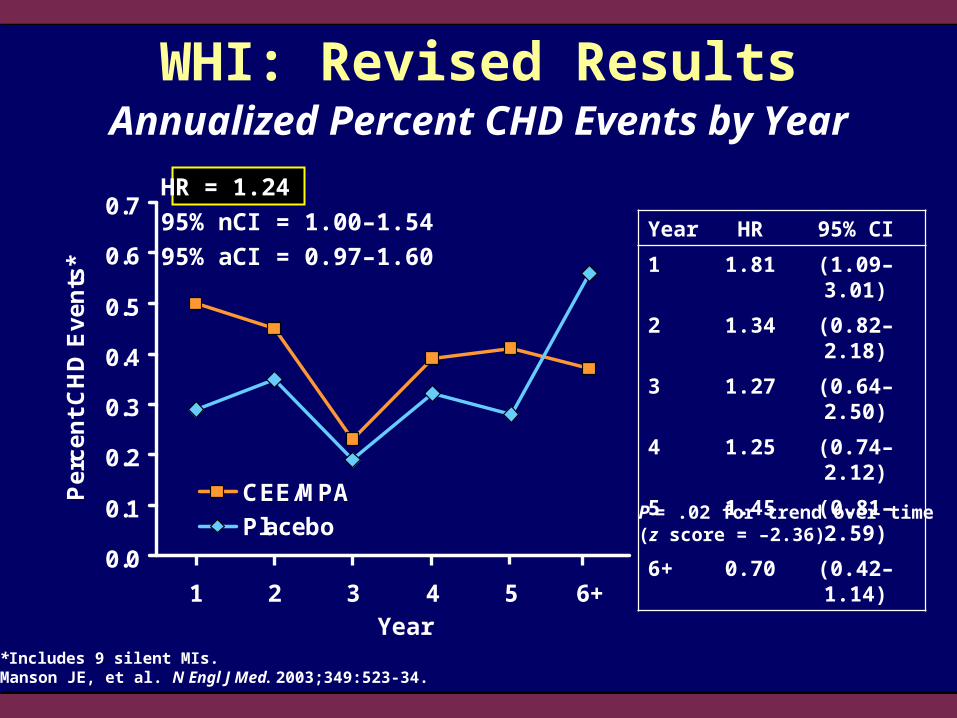
Year HR 95% CI
1 1.81 (1.09–3.01)
2 1.34 (0.82–2.18)
3 1.27 (0.64–2.50)
4 1.25 (0.74–2.12)
5 1.45 (0.81–2.59)
6+ 0.70 (0.42–1.14)
Annualized Percent CHD Events by Year
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
1 2 3 4 5 6+
Pe
rce
nt
CH
D E
ve
nts
*
CEE/MPA
Placebo
WHI: Revised Results
Year
P = .02 for trend over time (z score = –2.36).
HR = 1.24
95% nCI = 1.00–1.54
95% aCI = 0.97–1.60
*Includes 9 silent MIs.Manson JE, et al. N Engl J Med. 2003;349:523-34.
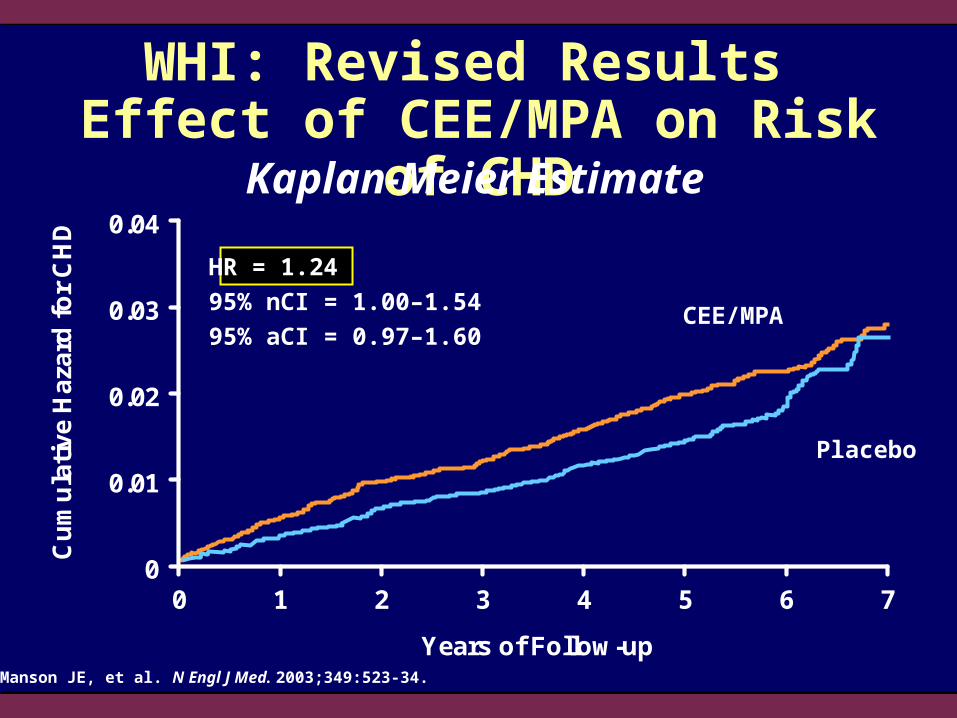
CEE/MPA
Placebo
0
0.01
0.02
0.03
0.04
0 1 2 3 4 5 6 7
Years of Follow-up
Cu
mu
lati
ve H
azar
d f
or
CH
DWHI: Revised Results
Effect of CEE/MPA on Risk of CHDKaplan-Meier Estimate
Manson JE, et al. N Engl J Med. 2003;349:523-34.
HR = 1.24
95% nCI = 1.00–1.54
95% aCI = 0.97–1.60
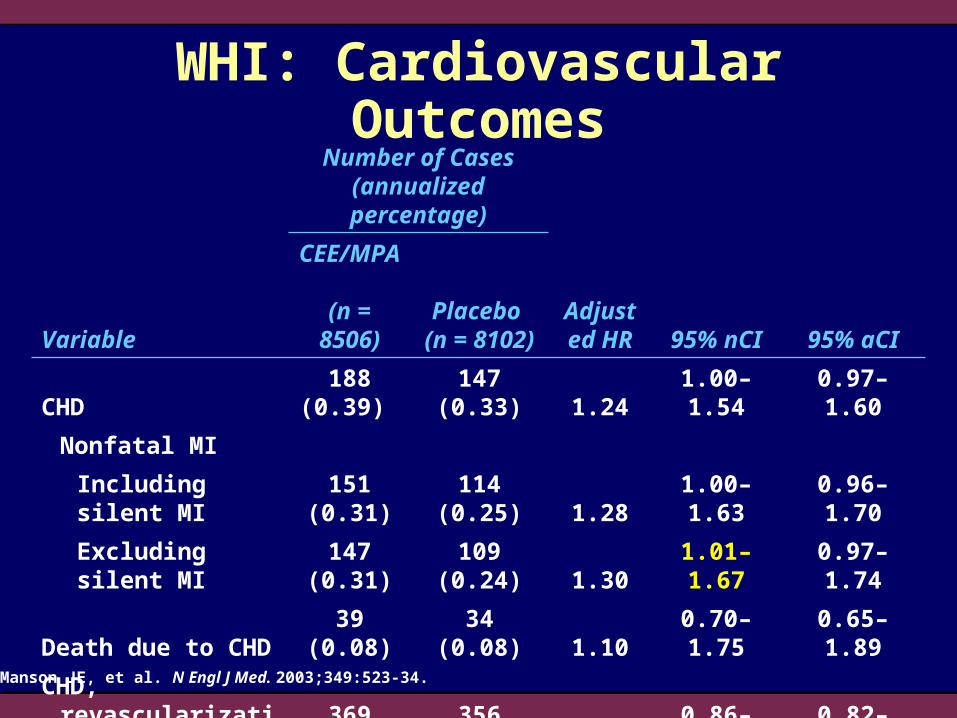
WHI: Cardiovascular Outcomes
Manson JE, et al. N Engl J Med. 2003;349:523-34.
Number of Cases (annualized percentage)
VariableCEE/MPA (n = 8506)
Placebo (n = 8102)
Adjusted HR 95% nCI 95% aCI
CHD 188 (0.39) 147 (0.33) 1.24 1.00–1.54 0.97–1.60
Nonfatal MI
Including silent MI 151 (0.31) 114 (0.25) 1.28 1.00–1.63 0.96–1.70
Excluding silent MI 147 (0.31) 109 (0.24) 1.30 1.01–1.67 0.97–1.74
Death due to CHD 39 (0.08) 34 (0.08) 1.10 0.70–1.75 0.65–1.89
CHD, revascularization, or angina 369 (0.77) 356 (0.79) 1.00 0.86–1.15 0.82–1.22
Congestive heart failure 113 (0.23) 109 (0.24) 0.99 0.76–1.29 0.69–1.42

WHI: Effect of CEE/MPA on Risk of CHD: No Effect of Age, But Possible Effect of Years Since Menopause
The dotted vertical line indicates the overall CHD odds ratio (1.24). P-values for interaction were not significant.Manson JE, et al. N Engl J Med. 2003;349:523-34.
0.5 1.0 1.5 2.0 2.5
Hazard Ratio for CHD
1.27
1.05
1.44
0.89
1.22
1.71
Number of Cases of CHD (annualized percentage)
Subgroup CEE/MPA Placebo
Age (years)
50–59 37 (0.22) 27 (0.17)
60–69 75 (0.35) 68 (0.34)
70–79 76 (0.78) 52 (0.55)
Years Since Menopause
<10 31 (0.19) 34 (0.22)
10–19 63 (0.38) 51 (0.32)
20 74 (0.75) 44 (0.46)
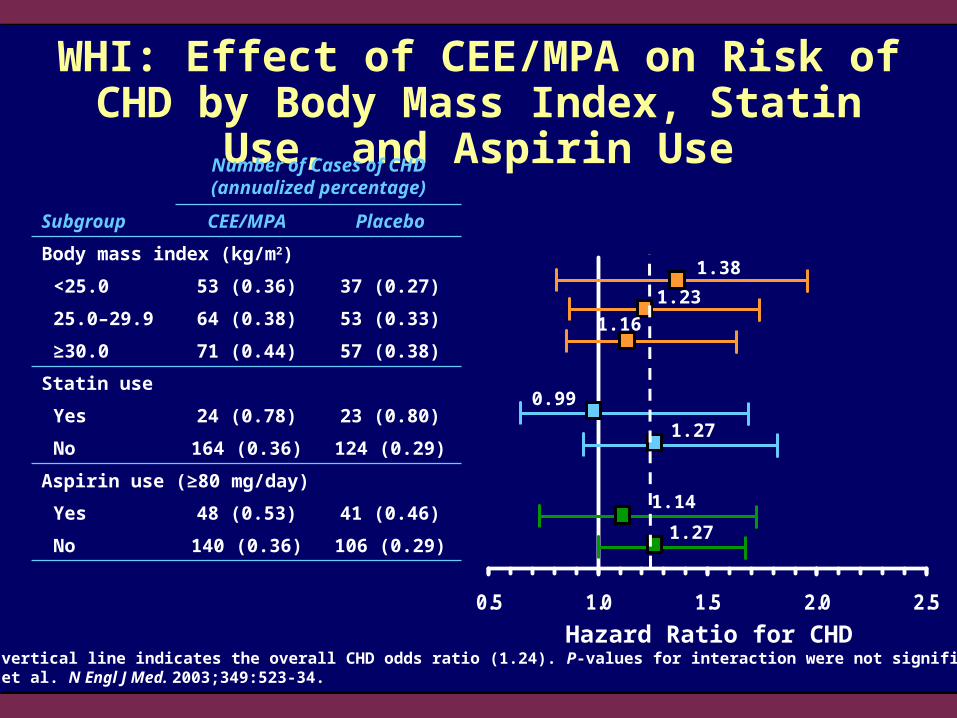
WHI: Effect of CEE/MPA on Risk of CHD by Body Mass Index, Statin Use, and Aspirin Use
The dotted vertical line indicates the overall CHD odds ratio (1.24). P-values for interaction were not significant.Manson JE, et al. N Engl J Med. 2003;349:523-34.
0.5 1.0 1.5 2.0 2.5
Hazard Ratio for CHD
0.99
1.27
1.14
1.27
1.23
1.38
Number of Cases of CHD (annualized percentage)
Subgroup CEE/MPA Placebo
Body mass index (kg/m2)
<25.0 53 (0.36) 37 (0.27)
25.0–29.9 64 (0.38) 53 (0.33)
≥30.0 71 (0.44) 57 (0.38)
Statin use
Yes 24 (0.78) 23 (0.80)
No 164 (0.36) 124 (0.29)
Aspirin use (≥80 mg/day)
Yes 48 (0.53) 41 (0.46)
No 140 (0.36) 106 (0.29)
1.16

WHI: Effect of CEE/MPA on Risk of CHD by Baseline Lipid Levels
The dotted vertical line indicates the overall CHD odds ratio.Manson JE, et al. N Engl J Med. 2003;349:523-34.
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
Hazard Ratio for CHD
0.76
1.28
2.03
1.43
0.86
1.68
1.86
1.50
0.88
Number of Cases of CHD
P-Value for InteractionBiomarker CEE/MPA Placebo
Total cholesterol .07
<208 mg/dL 22 25
208–242 mg/dL 49 25
>242 mg/dL 51 32
LDL cholesterol .01
<126 mg/dL 24 21
126–155 mg/dL 41 23
>155 mg/dL 51 34
HDL cholesterol .20
<47 mg/dL 60 40
47–58 mg/dL 36 21
>58 mg/dL 25 20

0.5 1.0 1.5 2.0 2.5 3.0
WHI: Effect of CEE/MPA on Risk of CHD by Baseline Triglycerides and C-Reactive Protein
The dotted vertical line indicates the overall CHD odds ratio. No interaction between subgroups was significant.Manson JE, et al. N Engl J Med. 2003;349:523-34.
Hazard Ratio for CHD
1.24
1.63
1.36
1.44
1.56
1.08
Number of Cases of CHD
Biomarker CEE/MPA Placebo
Triglycerides
<109 mg/dL 28 17
109–168 mg/dL 46 31
>168 mg/dL 48 34
C-reactive protein
<1.28 mg/L 25 16
1.28–3.57 mg/L 50 26
>3.57 mg/L 45 37

Timing of Initiation
WHI: Effect of CEE/MPA on CHD in Postmenopausal Women
Manson JE, et al. N Engl J Med. 2003;349:523-34.
0 1.0 2.5
Yes
No
Hazard Ratio (95% CI)
0.5 1.5 2.0
Hot Flushes in Women 50–59 Years Old
0.95
1.98
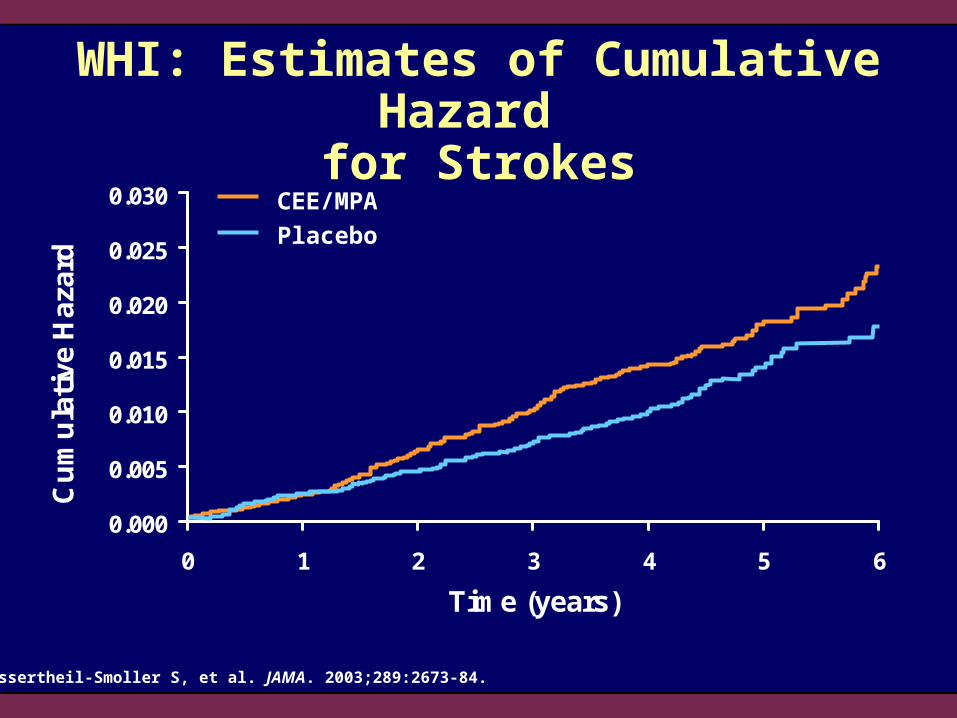
0.000
0.005
0.010
0.015
0.020
0.025
0.030
0 1 2 3 4 5 6
Time (years)
Cu
mu
lati
ve H
azar
dWHI: Estimates of Cumulative Hazard
for Strokes
Wassertheil-Smoller S, et al. JAMA. 2003;289:2673-84.
CEE/MPA
Placebo

0
0.1
0.2
0.3
0.4
0.5
1 2 3 4 5 6+
Str
ok
e E
ve
nts
(a
nn
ua
lize
d %
)
CEE/MPA
Placebo
WHI: Effect of CEE/MPA on Annualized Percent of Stroke Events
Year of Follow-Up
Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33.
HR = 1.3195% nCI = 1.02–1.6895% aCI = 0.93–1.84

Wassertheil-Smoller S, et al. JAMA. 2003;289:2673-84.
0.1 0.5 1.0 5.02.0
WHI: Effect of CEE/MPA on Hemorrhagic Stroke and Ischemic Stroke
Hemorrhagic Stroke
Ischemic Stroke
Hazard Ratio
WHI: Study Considerations
Average age at screening was 63 years
Study stopped when two thirds of patients were 68 years or older
High rates of discontinuation in the CEE/MPA group (42%) and crossover to active treatment in the placebo group (10.7%)
Women with moderate or severe menopausal symptoms were discouraged from participating
Results do not necessarily relate to lower dosages of these drugs or other formulations or routes of administration
0
5
10
15
20
25
40–44 45–49 50–54 55–59 60–64 65–69 70–74 75+
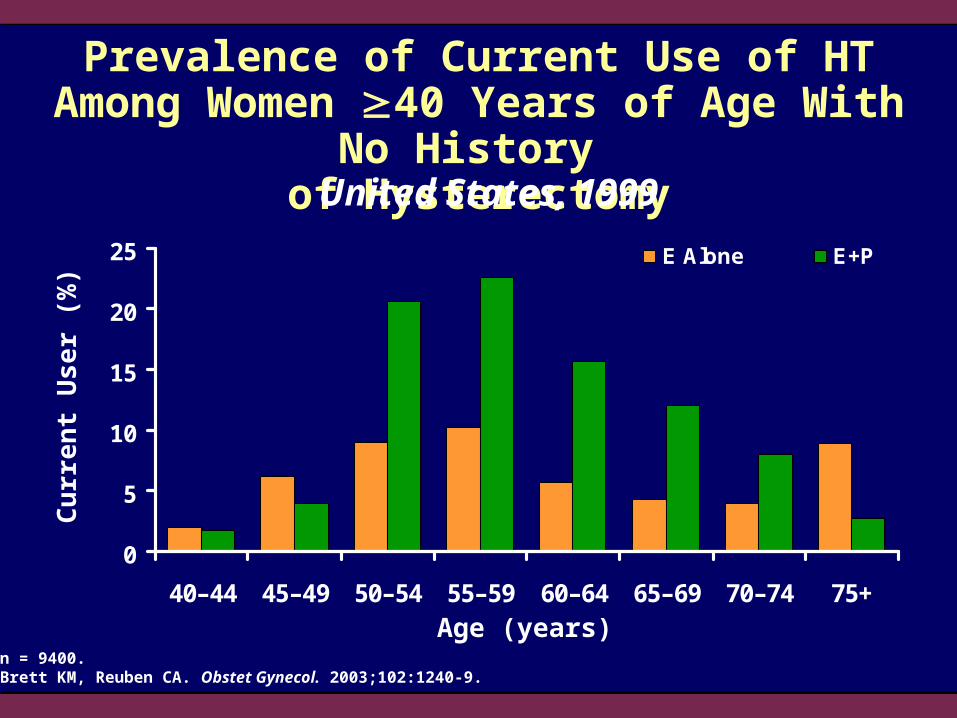
E Alone E+P
Prevalence of Current Use of HT Among Women 40 Years of Age With No History
of Hysterectomy
Cu
rre
nt
Us
er (
%)
Age (years)n = 9400.Brett KM, Reuben CA. Obstet Gynecol. 2003;102:1240-9.
United States, 1999

0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
22 24 27 >29
RH
fo
r C
VD
BMI (kg/m2)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
WHI*
RH
for C
VD
The Effect of Body Mass on the Risk of CHD: Putting the WHI Results in Perspective
RH = relative hazard.*Mean BMI 28.5 kg/m2.BMI data from Willett WC, et al. JAMA. 1995;273:461-5.WHI data from Manson JE, et al. N Engl J Med. 2003;349:523-34.
WHI: Surprises?
None except for CHD
No surprise for CHD if WHI is considered a secondary prevention trial (consistent with HERS and other data)

All-Cause Mortality Was Not Affected by E+P in WHI or HERS
0
0.05
0.1
0.15
0 1 2 3 4 5 6 7
Time (years)
Cu
mu
lati
ve H
azar
d
E+P Placebo
HR = 0.98P = NS
WHI (cumulative hazard)
0
5
10
15
0 1 2 3 4 5
Follow-up, Years (number at risk)
Inci
den
ce (
%)
E+P Placebo
HERS (incidence %)
P = NS
Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33. ©2002 American Medical Association. All rights reserved.Hulley S, et al. JAMA. 1998;280:605-13. ©1998 American Medical Association. All rights reserved.

Relative Risk of CHD: Nurses’ Health Study (NHS) Versus WHI
wy = woman-years.Grodstein F, et al. Ann Intern Med. 2000;133:933-41; Manson JE, et al. N Engl J Med. 2003;349:523-34.
NHS
Never-Users(358,125 wy)
E Alone(175,140 wy)
E+P(90,063 wy)
WHI
Placebo(42,130 wy)
E+P(42,312 wy)
0.5 1.0 5.02.0
95% aCI
Risk Estimate
95% nCI
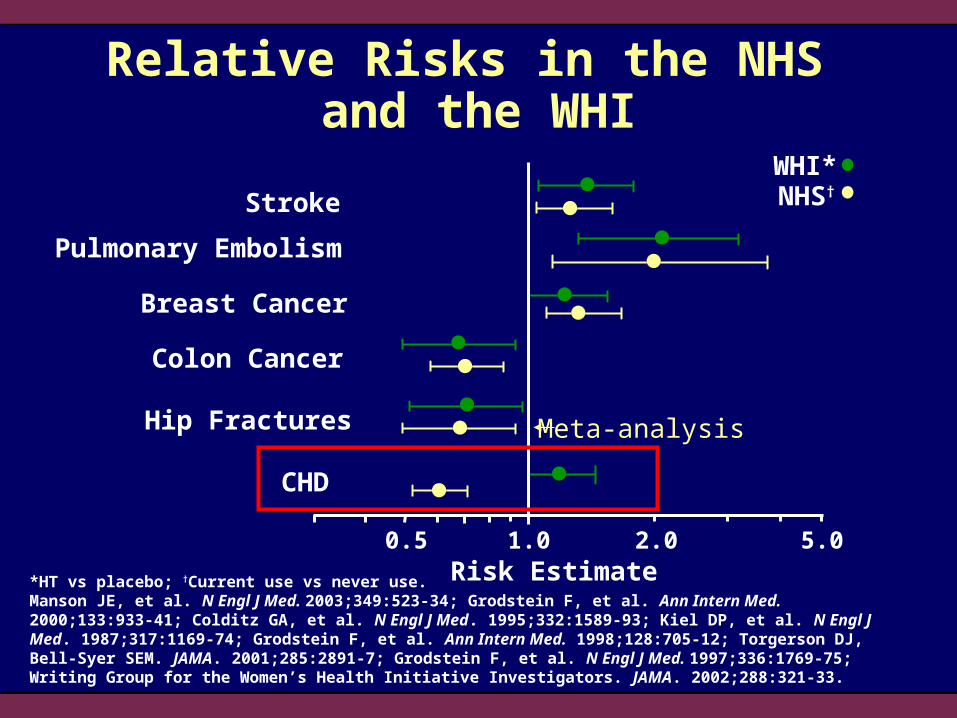
Relative Risks in the NHS and the WHI
*HT vs placebo; †Current use vs never use.Manson JE, et al. N Engl J Med. 2003;349:523-34; Grodstein F, et al. Ann Intern Med. 2000;133:933-41; Colditz GA, et al. N Engl J Med. 1995;332:1589-93; Kiel DP, et al. N Engl J Med. 1987;317:1169-74; Grodstein F, et al. Ann Intern Med. 1998;128:705-12; Torgerson DJ, Bell-Syer SEM. JAMA. 2001;285:2891-7; Grodstein F, et al. N Engl J Med. 1997;336:1769-75; Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288:321-33.
CHD
Risk Estimate0.5 1.0 5.02.0
NHS†
Hip Fractures
Stroke
Pulmonary Embolism
WHI*
Breast Cancer
Colon Cancer
Meta-analysis
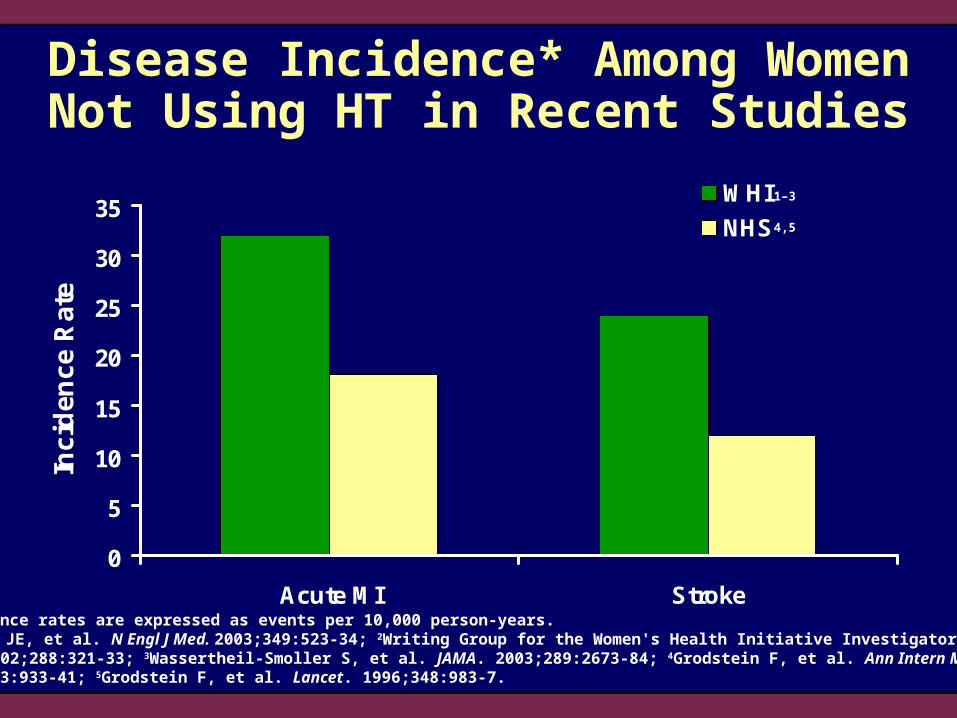
Disease Incidence* Among Women Not Using HT in Recent Studies
*Incidence rates are expressed as events per 10,000 person-years. 1Manson JE, et al. N Engl J Med. 2003;349:523-34; 2Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33; 3Wassertheil-Smoller S, et al. JAMA. 2003;289:2673-84; 4Grodstein F, et al. Ann Intern Med. 2000;133:933-41; 5Grodstein F, et al. Lancet. 1996;348:983-7.
0
5
10
15
20
25
30
35
Acute MI Stroke
Inci
den
ce R
ate
WHI
NHS
1–3
4,5
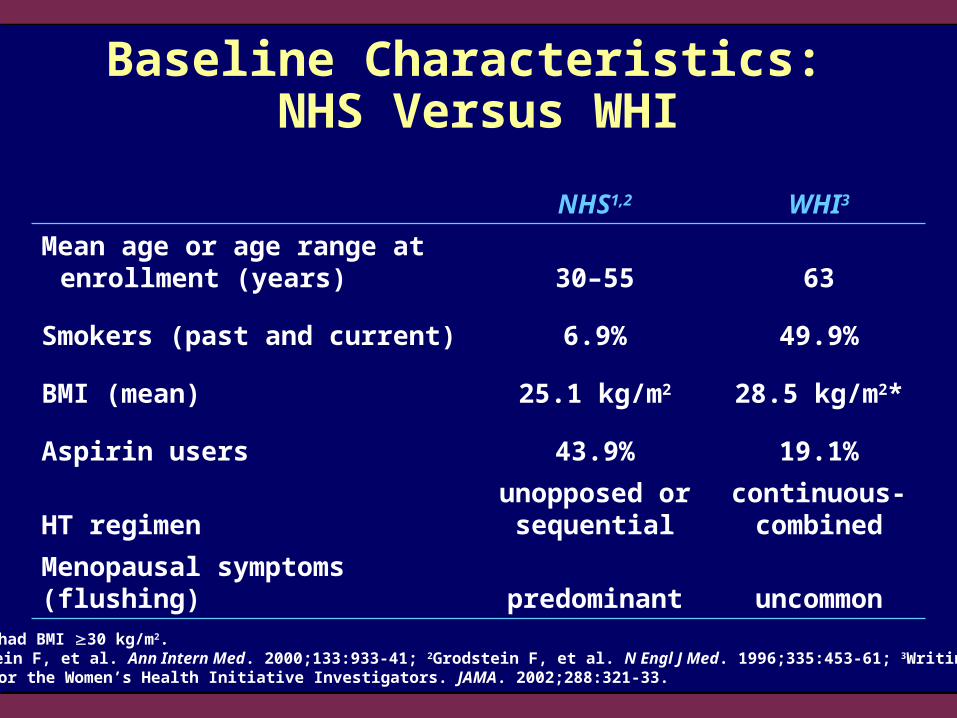
Baseline Characteristics: NHS Versus WHI
*34.1% had BMI 30 kg/m2.1Grodstein F, et al. Ann Intern Med. 2000;133:933-41; 2Grodstein F, et al. N Engl J Med. 1996;335:453-61; 3Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288:321-33.
NHS1,2 WHI3
Mean age or age range at enrollment (years) 30–55 63
Smokers (past and current) 6.9% 49.9%
BMI (mean) 25.1 kg/m2 28.5 kg/m2*
Aspirin users 43.9% 19.1%
HT regimenunopposed or
sequentialcontinuous-combined
Menopausal symptoms (flushing) predominant uncommon
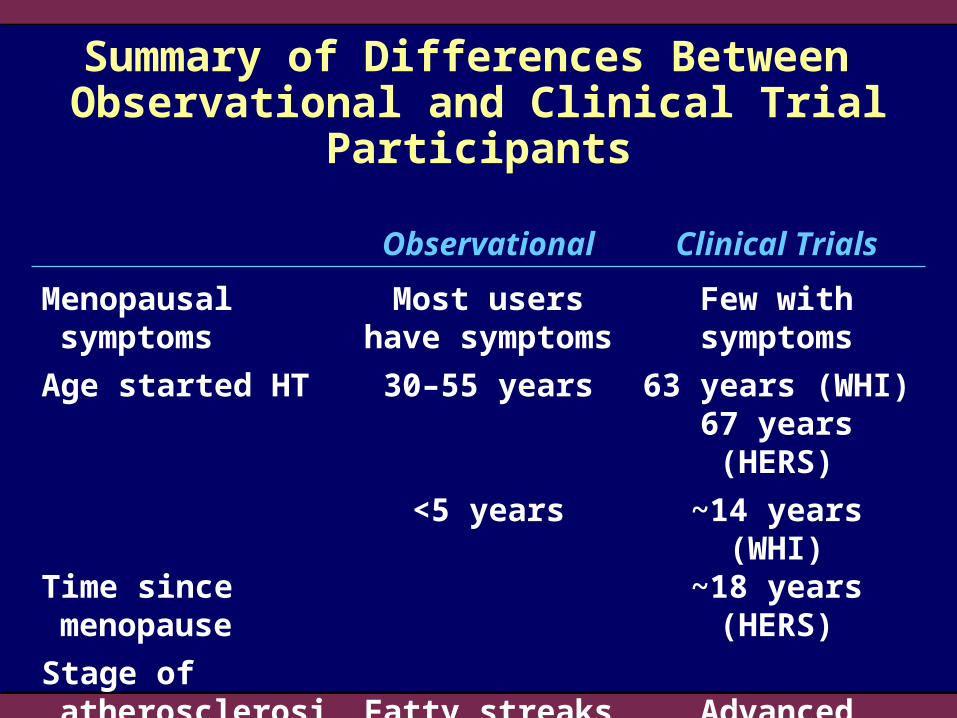
Summary of Differences Between Observational and Clinical Trial Participants
Observational Clinical Trials
Menopausal symptoms
Most users have symptoms
Few with symptoms
Age started HT 30–55 years 63 years (WHI)67 years (HERS)
Time since menopause
<5 years ~14 years (WHI)~18 years (HERS)
Stage of atherosclerosis
Fatty streaks and plaques
Advanced plaques
Section 4:Timing of HT Initiation
Cardiovascular Health and Menopause

The Challenge How can we integrate the findings of all of the
published studies into one consistent concept?
A Hypothesis The timing of initiation of HT in relation to the
development of atherosclerosis has a major impact on its potential efficacy
What Do Recent Randomized Studies Have in Common?
They all involve the initiation of HT in older women (age 64 to 67 years)
They have not tested whether HT has primary cardiovascular prevention effects as defined by vascular biologists
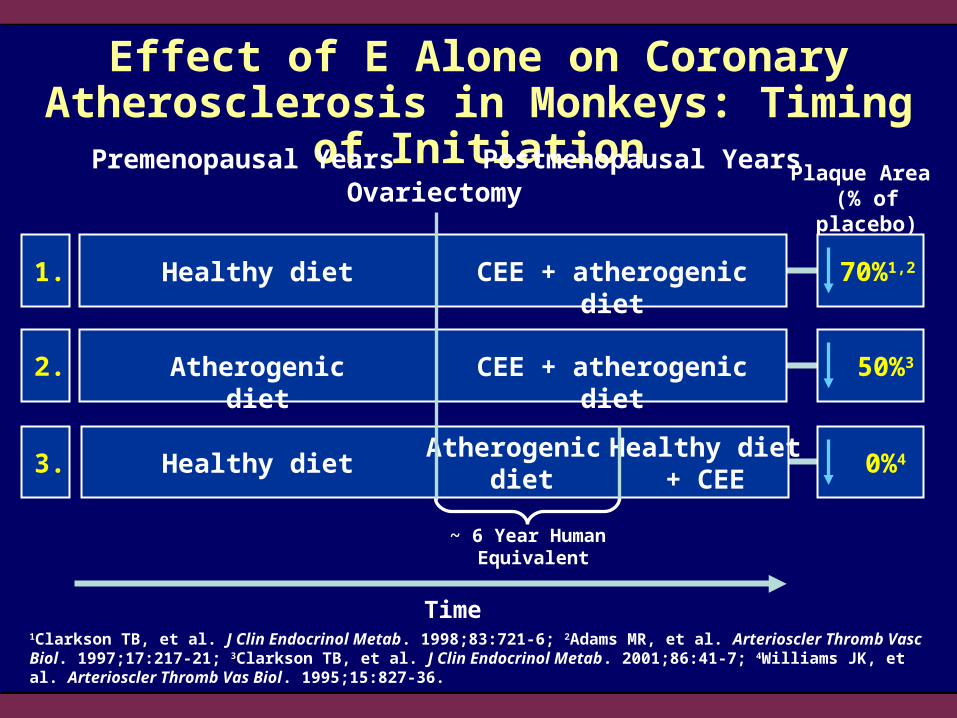
1Clarkson TB, et al. J Clin Endocrinol Metab. 1998;83:721-6; 2Adams MR, et al. Arterioscler Thromb Vasc Biol. 1997;17:217-21; 3Clarkson TB, et al. J Clin Endocrinol Metab. 2001;86:41-7; 4Williams JK, et al. Arterioscler Thromb Vas Biol. 1995;15:827-36.
Effect of E Alone on Coronary Atherosclerosis in Monkeys: Timing of Initiation
Premenopausal Years Postmenopausal YearsOvariectomy
Plaque Area (% of placebo)
Time
Healthy diet CEE + atherogenic diet1. 70%1,2
Atherogenic diet CEE + atherogenic diet2. 50%3
Healthy dietAtherogenic
dietHealthy diet
+ CEE3. 0%4
~ 6 Year Human Equivalent

Placebo CEE
Co
ron
ary
Art
ery
Pla
qu
e S
ize
(m
m2)
0.10
0.20
0.30
0.40
0Baseline Placebo CEE CEE+MPA
A. Early Intervention B. Late Intervention*
P < .05
P = NS
Effect of HT on Coronary Atherosclerosis in Monkeys: Timing of Initiation of HT
*Comparable to approximately 6 patient-years after menopause.Karas RH, Clarkson TB. Menopausal Med. 2003;10:8-12.

Effect of the Extent of Preexisting Atherosclerosis on Effectiveness of CEE Treatment of Surgically
Postmenopausal Cynomolgus Monkeys
-0.30
-0.25
-0.20
-0.15
-0.10
-0.05
0.00
Pla
qu
e S
ize
Co
mp
are
d
Wit
h P
lace
bo
(m
m2)
High Moderate Low
P = .71
P = .33
P = .0001
Tertile of Initial Plaque Burden
Karas RH, Clarkson TB. Menopausal Med. 2003;10:8-12.

0123456789
10
4 10 16 22 28 34 40
Weeks
Nu
mb
er
of
Mic
e W
ith
Le
sio
ns
Iliac –EstradiolIliac +Estradiol
New Lesions Established Lesions
Estrogen Inhibits Initiation but not Progression of Established Lesions in Mice
Rosenfeld ME, et al. Atherosclerosis. 2002;164:251-9.
0123456789
10
4 10 16 22 28 34 40
Weeks
Nu
mb
er
of
Mic
e W
ith
Le
sio
ns
Carotid –EstradiolCarotid +Estradiol
2.0
2.5
3.0
3.5
4.0
4.5
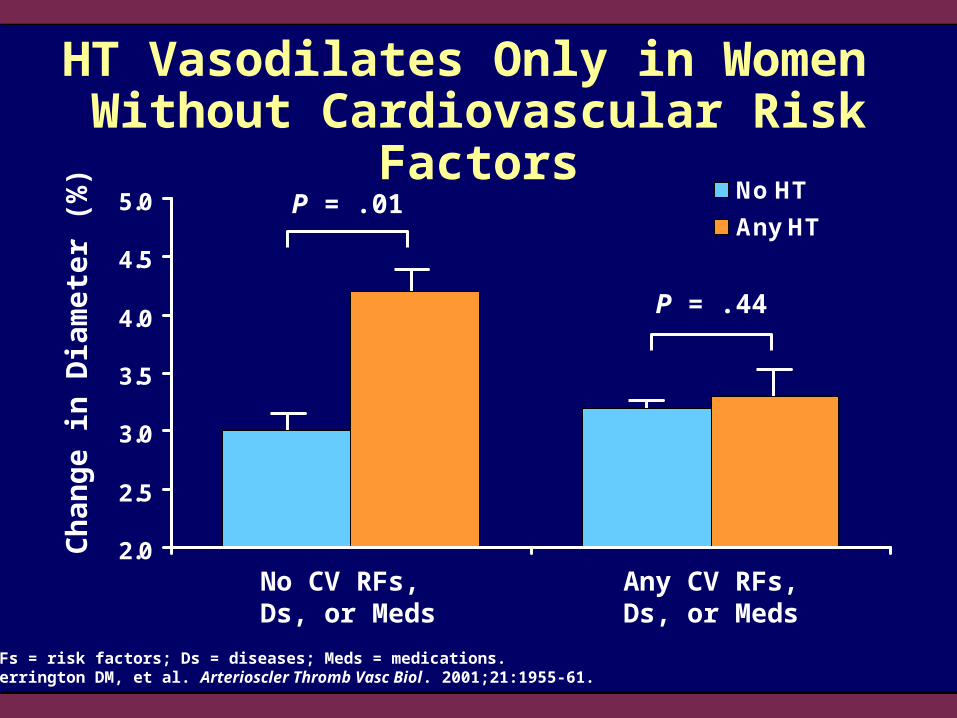
5.0 No HT
Any HT
HT Vasodilates Only in Women Without Cardiovascular Risk Factors
RFs = risk factors; Ds = diseases; Meds = medications.Herrington DM, et al. Arterioscler Thromb Vasc Biol. 2001;21:1955-61.
Ch
ang
e in
Dia
met
er (
%)
No CV RFs, Ds, or Meds
Any CV RFs,Ds, or Meds
P = .01
P = .44
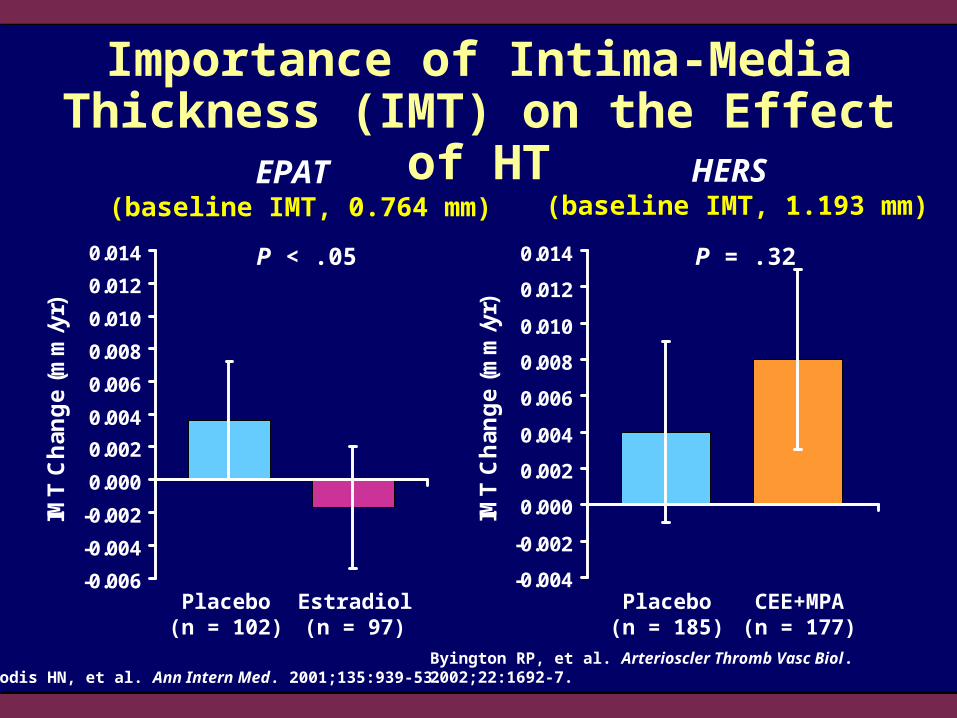
Importance of Intima-Media Thickness (IMT) on the Effect of HT
-0.006
-0.004
-0.002
0.000
0.002
0.004
0.006
0.008
0.010
0.012
0.014
IMT
Ch
ang
e (m
m/y
r)
-0.004
-0.002
0.000
0.002
0.004
0.006
0.008
0.010
0.012
0.014
IMT
Ch
ang
e (m
m/y
r)
P = .32P < .05
Estradiol(n = 97)
CEE+MPA(n = 177)
Placebo(n = 102)
Placebo(n = 185)
Byington RP, et al. Arterioscler Thromb Vasc Biol. 2002;22:1692-7.Hodis HN, et al. Ann Intern Med. 2001;135:939-53.
HERS (baseline IMT, 1.193 mm)
EPAT (baseline IMT, 0.764 mm)

-4
-2
0
2
4
6
8
<100 100–400 >400
Pe
rce
nt
Dif
fere
nc
e*
(95
% C
I)Percent Difference in Distribution
of the Coronary Artery Calcium Score in HT Versus Non-HT Groups
Coronary Artery Calcium Score*Percent difference in distribution of the coronary artery calcium score in HT versus non-HT groups.Odds ratio for a coronary artery calcium score >400: 0.5; P = .02.Akhrass F, et al. J Clin Endocrinol Metab. 2003;88:5611-4.
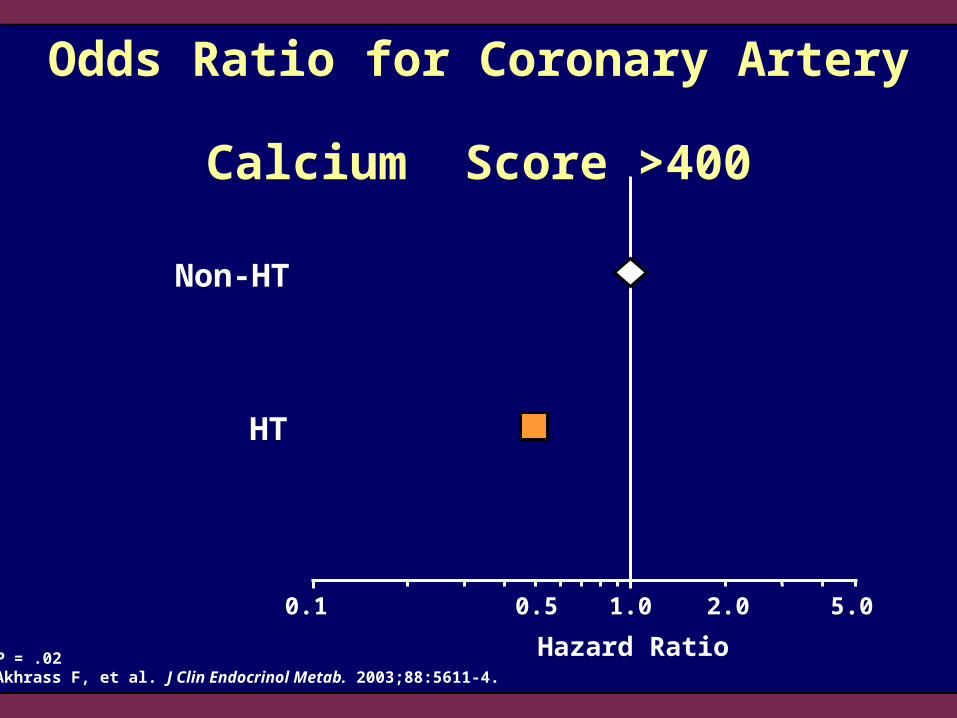
Odds Ratio for Coronary Artery Calcium Score >400
Non-HT
Hazard Ratio
0.1 0.5 1.0 5.02.0
HT
P = .02Akhrass F, et al. J Clin Endocrinol Metab. 2003;88:5611-4.

Incidence of Carotid Artery Plaque by Menopausal Status and Duration
0
10
20
30
40
50
60
Ag
e-S
tan
dar
diz
ed I
nci
den
ce R
ate
(per
100
0 p
erso
n-y
ears
)
>10 Men1–5 5–10Postmenopausal (years)
Premenopausal
Kiechl S, Willeit J. Arterioscler Thromb Vasc Biol. 1999;19:1484-90.
The Bruneck Study
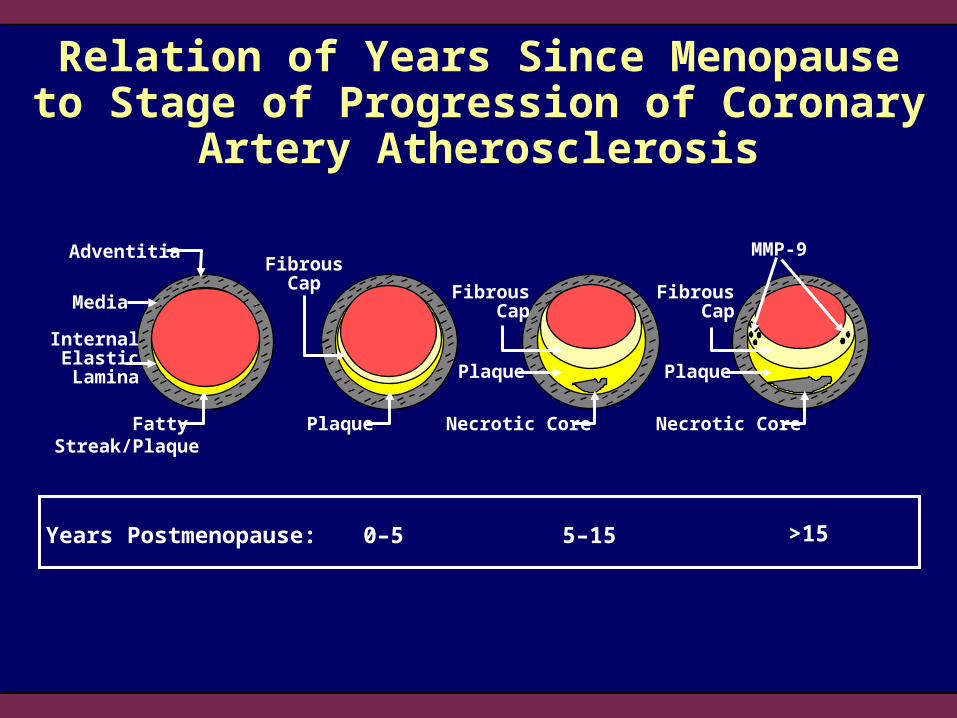
Relation of Years Since Menopause to Stage of Progression of Coronary Artery Atherosclerosis
Adventitia
Media
Fatty Streak/Plaque
InternalElastic
Lamina
Necrotic Core
Plaque
FibrousCap
FibrousCap
Plaque Necrotic Core
Plaque
FibrousCap
MMP-9
Years Postmenopause: 0–5 5–15 >15

No HTHypothetical Pathogenetic Sequence
Adventitia
Media
Fatty Streak/Plaque
InternalElastic
Lamina
Necrotic Core
Plaque
FibrousCap
FibrousCap
Plaque Necrotic Core
Plaque
FibrousCap
MMP-9
HT Early & Continued
HT Late
HT
Age 35–45 years Age 45–55 years Age 55–65 years Age >65 years
HT
Mural Thrombus

Relation of Years Since Menopause in WHI to Stage of Progression of Coronary Artery Atherosclerosis
Adventitia
Media
InternalElastic
Lamina Plaque
FibrousCap
FibrousCap
Plaque
FibrousCap
MMP-9
5 to <1019%Years Postmenopause 10 to <15
21%≥1543%
<517%
Fatty Streak/Plaque
Necrotic CorePlaque Necrotic Core

Estrogen Effects on the Natural History of AtherosclerosisAdventitia
Media
InternalElastic
Lamina Plaque
FibrousCap
FibrousCap
Plaque
FibrousCap
MMP-9
Estrogen Effects in AtherogenesisLDL oxidation LDL atherogenicityLDL binding/accum lesion
progressionCAMs monocyte adhesion/
macrophage accumulation
SMC proliferation lesion progressionEndothelial function vasodilation
Estrogen Effects in Established PlaquesInflammation PQ instability
lesion progressionMMP expression PQ instability/ruptureNeovascularization PQ hemorrhage
Loss of Estrogen Benefits Expression of estrogen receptors Vascular responsivity
Benefits of estrogen on atherosclerosis prevention
Potentially adverse effects ofestrogen on atherosclerosis/CHD
PlaqueFatty Streak/Plaque
Necrotic Core Necrotic Core
Mea
n C
han
ge
Fro
m B
asel
ine
in %
CR
P C
on
cen
trat
ion
s
-20
0
20
40
60
80
100
Oral CEE TransdermalEstradiol
Oral CEE TransdermalEstradiol
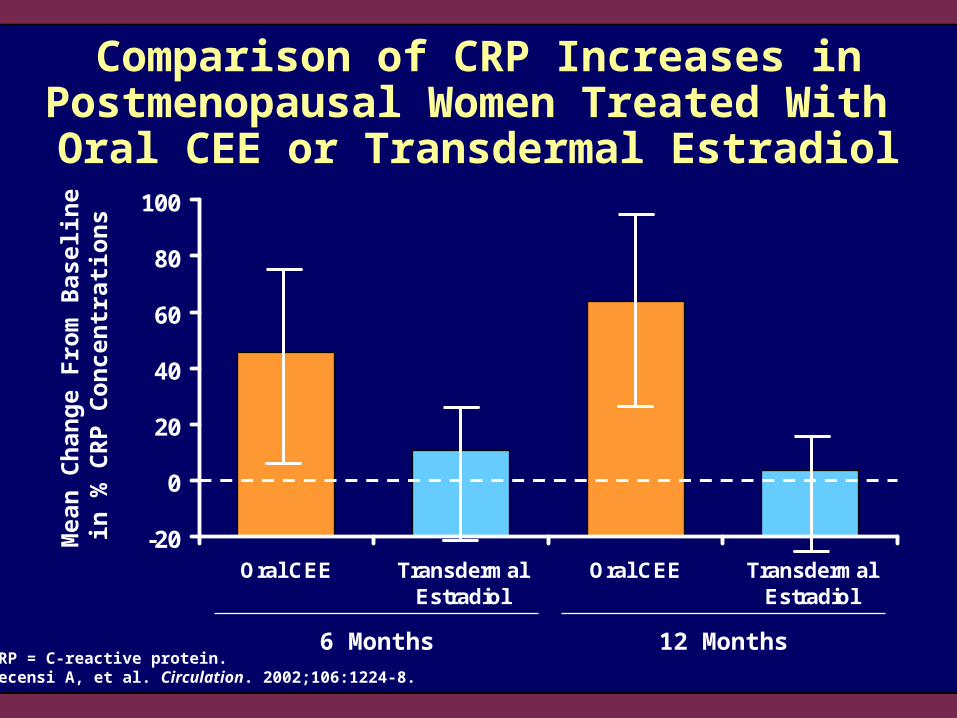
Comparison of CRP Increases in Postmenopausal Women Treated With
Oral CEE or Transdermal Estradiol
6 Months 12 MonthsCRP = C-reactive protein.Decensi A, et al. Circulation. 2002;106:1224-8.
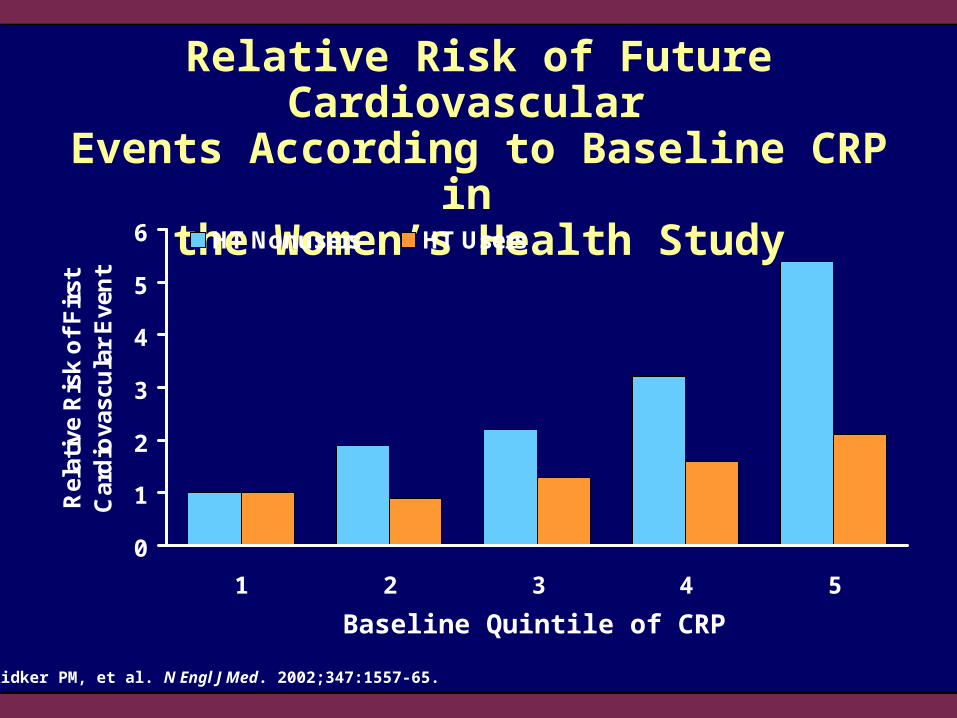
Relative Risk of Future Cardiovascular Events According to Baseline CRP in
the Women’s Health Study
0
1
2
3
4
5
6
1 2 3 4 5
Rel
ativ
e R
isk
of
Fir
st
Car
dio
vasc
ula
r E
ven
t
HT Nonusers HT Users
Baseline Quintile of CRP
Ridker PM, et al. N Engl J Med. 2002;347:1557-65.

90
100
110
120
130
140
150
0.0
0.1
0.2
0.3
0.4
0.5
0.6
Pla
sm
a C
RP
(n
g/m
L)
Control CEE Control CEE
Co
ron
ary A
rtery A
the
rosc
leros
isP
laqu
e S
ize (mm
2)
P = .028 P < .05
Lack of Effect of Increased CRP on the Coronary Artery Atheroprotective Effect of CEE in Surgically
Postmenopausal Micropigs
Goodrich JA, et al. Fertil Steril. 2003;79:779-88.

The Pathophysiology of Plaque Rupture
Heistad DD. N Engl J Med. 2003;349:2285-7.

Metalloproteinase Staining and Gelatinolytic Activity of Human Coronary
Artery Atherosclerotic Plaques
Galis ZS, et al. J Clin Invest. 1994;94:2493-503. Used with permission.
0
200
400
600
800
0
500
1000
1500
2000
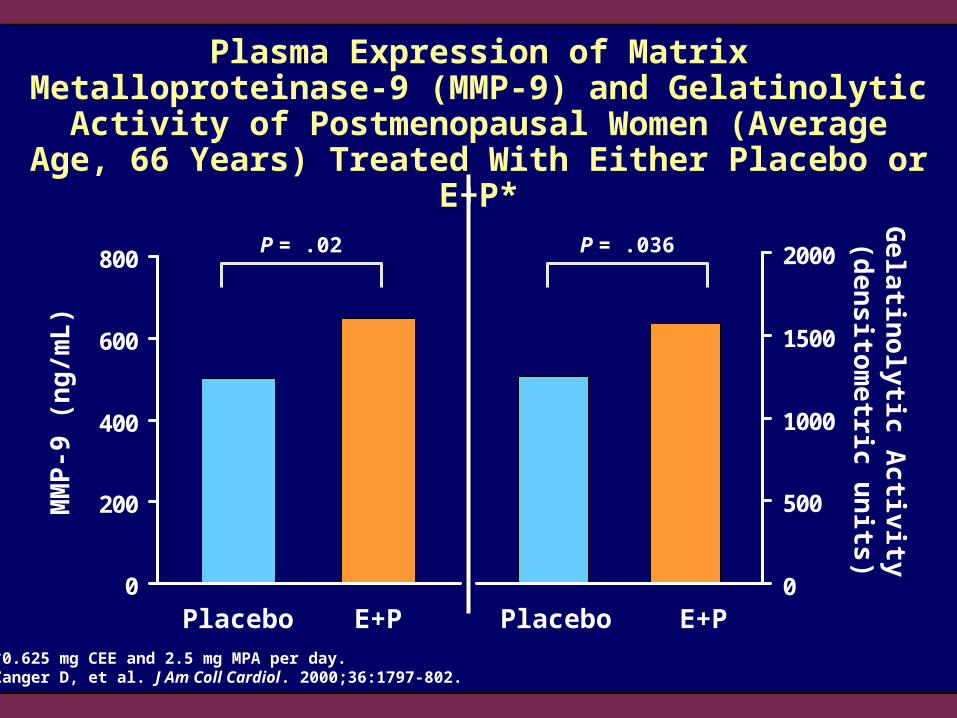
MM
P-9
(n
g/m
L)
Placebo E+P Placebo E+P
Ge
latino
lytic A
ctivity
(de
ns
itom
etric
un
its)
P = .02 P = .036
Plasma Expression of Matrix Metalloproteinase-9 (MMP-9) and Gelatinolytic Activity of Postmenopausal Women (Average Age,
66 Years) Treated With Either Placebo or E+P*
*0.625 mg CEE and 2.5 mg MPA per day.Zanger D, et al. J Am Coll Cardiol. 2000;36:1797-802.
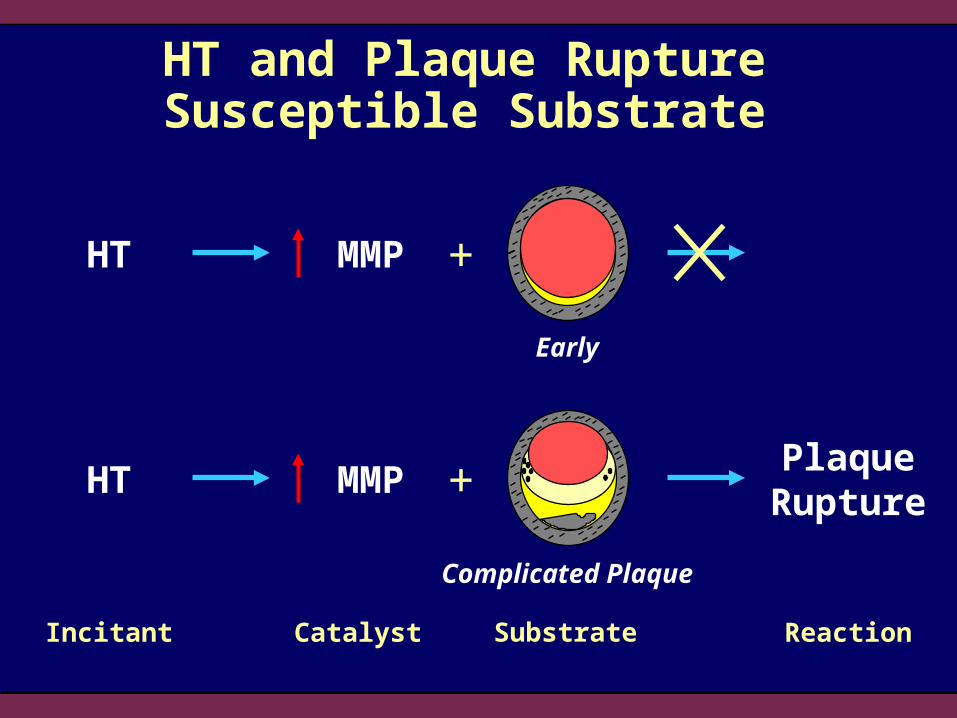
HT and Plaque Rupture Susceptible Substrate
Incitant
PlaqueRupture
+
Early
Complicated Plaque
MMPHT +
MMPHT
ReactionCatalyst Substrate

Effect of HT on Risk of Nonfatal Acute MI
HT Never-User
HT Ever-User
Chilvers CE, et al. Eur Heart J. 2003;24:2197-205.
Odds Ratio
0.1 0.5 1.0 5.02.0

Effect of Duration of HT Use on Risk of Nonfatal Acute MI
Never Use
Odds Ratio
0.1 0.5 1.0 5.02.0
<12 Months
13–60 Months
>60 Months
HT Use
Chilvers CE, et al. Eur Heart J. 2003;24:2197-205.

Association Between Estrogen Receptor Gene Variation and MI in Men
CT or TT Genotype
Hazard Ratio
0.5 1.0 5.02.0
CC Genotype
P < .001.CC = ESR1 c.454-397CC homozygous.CT = ESR1 c.454-397CT heterozygous.TT = ESR1 c.454-397TT homozygous.Shearman AM, et al. JAMA. 2003;290:2263-70.
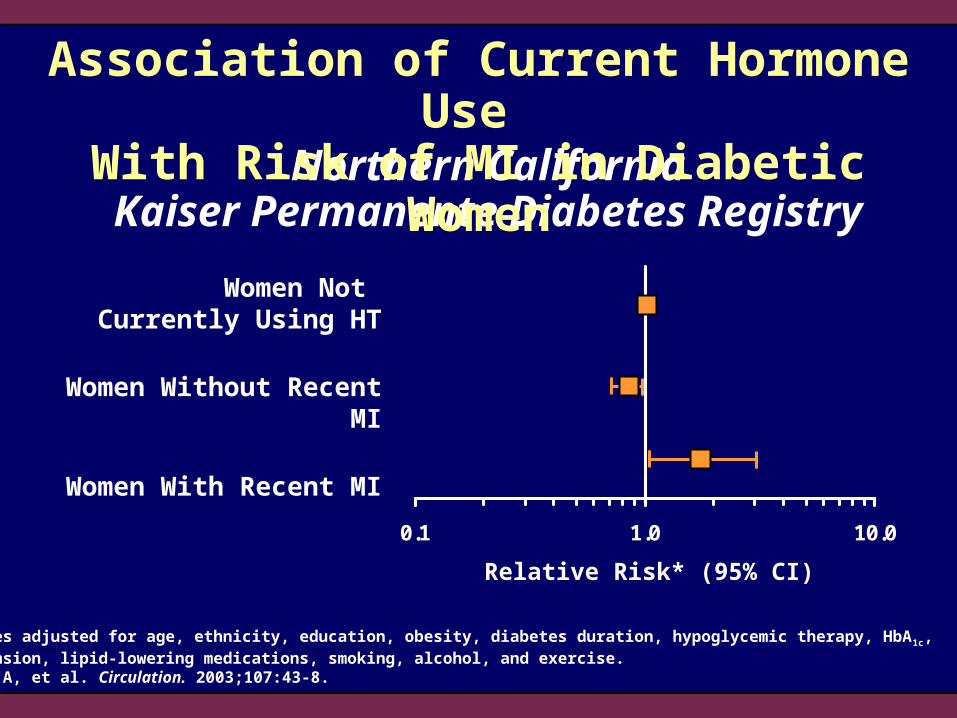
Northern California Kaiser Permanente Diabetes Registry (1995-1998) Study
Study Design:Observational cohort study
Subjects:25,000 diabetic women 50 years of age identified by the Northern California Kaiser Permanente Diabetes Registry
Follow-up:3 years (1995–1998)
Outcome:Risk of acute MI associated with current use of different HT regimens, estrogen doses, and time since initiation of hormonesFerrara A, et al. Circulation. 2003;107:43-8.
0.1 1.0 10.0
Northern CaliforniaKaiser Permanente Diabetes Registry
*Analyses adjusted for age, ethnicity, education, obesity, diabetes duration, hypoglycemic therapy, HbA 1c, hypertension, lipid-lowering medications, smoking, alcohol, and exercise.Ferrara A, et al. Circulation. 2003;107:43-8.
Association of Current Hormone Use With Risk of MI in Diabetic Women
Women Not Currently Using HT
Women Without Recent MI
Women With Recent MI
Relative Risk* (95% CI)
0.1 1.0 10.0
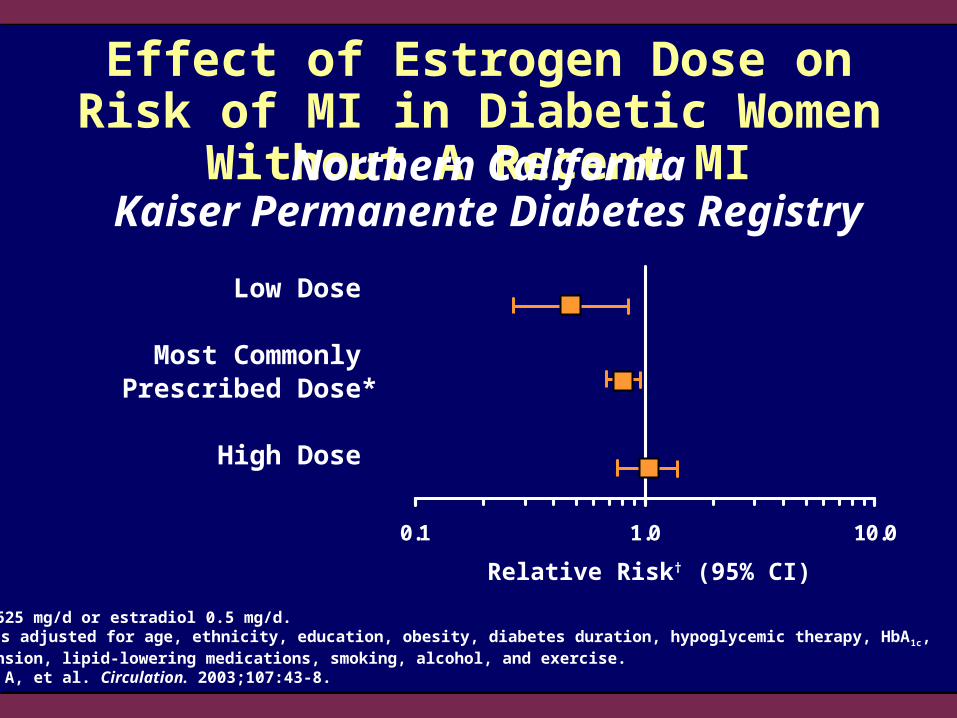
Relative Risk† (95% CI)
Effect of Estrogen Dose on Risk of MI in Diabetic Women Without A Recent MI
*CEE 0.625 mg/d or estradiol 0.5 mg/d.†Analyses adjusted for age, ethnicity, education, obesity, diabetes duration, hypoglycemic therapy, HbA 1c, hypertension, lipid-lowering medications, smoking, alcohol, and exercise.Ferrara A, et al. Circulation. 2003;107:43-8.
Northern CaliforniaKaiser Permanente Diabetes Registry
Low Dose
Most Commonly Prescribed Dose*
High Dose
0.1 1.0 10.0
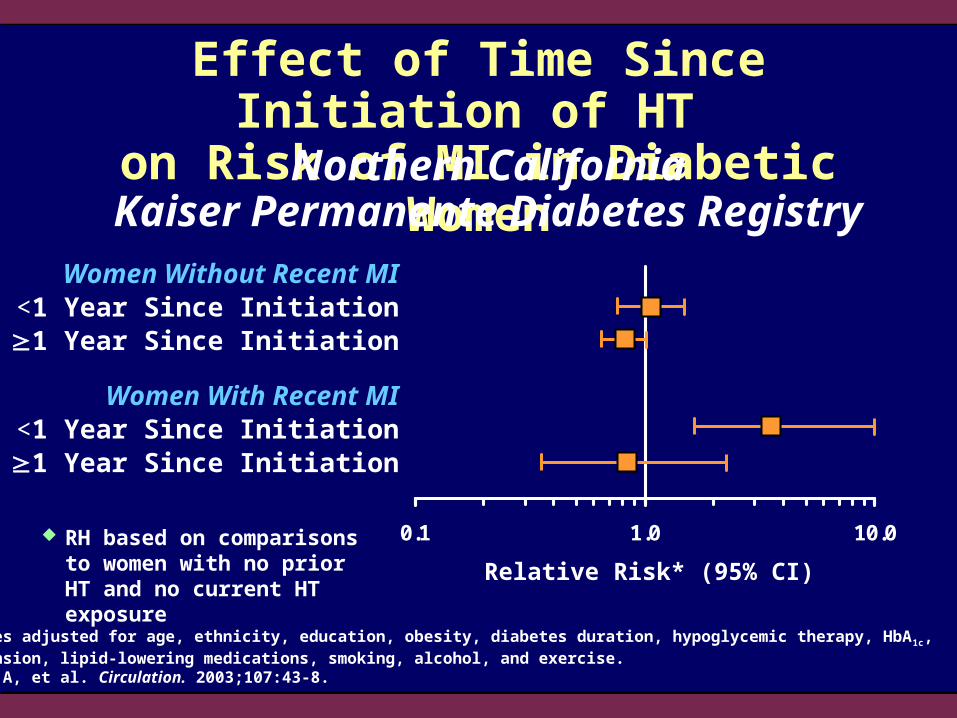
Effect of Time Since Initiation of HT on Risk of MI in Diabetic Women
RH based on comparisons to women with no prior HT and no current HT exposure
Women Without Recent MI<1 Year Since Initiation1 Year Since Initiation
Women With Recent MI<1 Year Since Initiation1 Year Since Initiation
Northern CaliforniaKaiser Permanente Diabetes Registry
Relative Risk* (95% CI)
*Analyses adjusted for age, ethnicity, education, obesity, diabetes duration, hypoglycemic therapy, HbA 1c, hypertension, lipid-lowering medications, smoking, alcohol, and exercise.Ferrara A, et al. Circulation. 2003;107:43-8.

Glycemic Effects of HT: Results From HERS
2029 HERS participants with coronary disease who were not diabetic at enrollment were followed for incident diabetes and fasting glucose levels
Fasting glucose levels did not change among the E+P group but increased significantly among women assigned to placebo
The risk for incident diabetes was significantly reduced by 35% in the E+P group (RH, 0.65; 95% CI, 0.48–0.89)
Kanaya AM, et al. Ann Intern Med. 2003;138:1-9.

Recommended Therapies for Cardiovascular Treatment in Women
Statins
Aspirin
Angiotensin-converting enzyme inhibitors
Beta-blockers
Therapeutic lifestyle change
Section 5:Summary and Conclusions
Cardiovascular Health and Menopause
Mosca L, et al. Circulation. 2001;104:499-503; Mendelsohn ME, Karas R. Circulation. 2001;104:2256-9.
Summary of Cardiovascular Effects of HT in Women
Large deficit in public awareness that heart disease is leading cause of mortality in women
More than 20 observational studies in younger postmenopausal women support the conclusion that HT has cardiovascular benefit in postmenopausal women
Data from the randomized controlled trials of older postmenopausal women have not supported the observational data
Current Perspectives on HT in Women
Potential of cardiovascular benefits may be decreased by
– Time since menopause
– Presence of diabetes and other risk factors
– Presence of subclinical atherosclerosis
– Concomitant event reducing therapies
Initiation and continuation of HT should be based on approved indications (ie, treatment of hot flushes and osteoporosis prevention)
Mosca L, et al. Circulation. 2001;104:499-503; Mendelsohn ME, Karas R. Circulation. 2001;104:2256-9.

Major Unresolved Issues
What is the effect of early initiation of HT on CVD endpoints?
Why haven’t recent clinical studies demonstrated cardiovascular benefit despite improvements in surrogate endpoints?
What are the differences between different formulations of E+P or E alone?
Are there particular patient populations who are likely to benefit or who are prone to harm?