canadian public health association 2011...
TRANSCRIPT
Montreal Quebec - June 22nd, 2011
Canadian Public Health Association2011 Conference
Public Health in Canada: Innovative Partnership for Action
Education for Health Care Reform: The Brazilian Case
Authors:Fabiano Borges
Eduardo SiqueiraCléa Garbin
Suzely Moimaz
University of Massachusetts/ LowellSchool of Health and Environment
Community health and Sustainability
Montreal, 06/22/2011UNESP Sao Paulo State UniversityAraçatuba School of Dentistry
Dental Public Health Graduate Program
Education for Health Care Reform: The Brazilian Case
Study made possible by a partnership of
And by the support of CAPES Foundation, Ministry of Education of Brazil Grant 2343-10-0

Key Points
Brazil’s Unified Health System (SUS) has its own assets for training healthcare resources and conducting mass educational programs for allied health personnel.
An educational network was established, and embedded in four domains of SUS: healthcare delivery, management, social participation, and public policy.
Beyond well-trained workers, the National Policy of Permanent Health Education has become an important tool for the Brazilian Healthcare Reform, as well as played a key role in developing advocates of universal healthcare.
Objective
To develop critical analysis of the theoretical
framework – Permanent Health Education (PHE) – used to
guide the education of healthcare workers in the SUS
(Unified Health System), focusing on allied health
personnel training.
Methods
Comprehensive literature review of peer-reviewed journals, grey literature, government documents, and books, from 1988 to 2010. The following databases were searched:
• PUBMED; • SCIELO;• BIREME; • WEB OF SCIENCE; • Brazilian Ministry of Health; • Pan American Health Organization Library.
Study Question
What is the role of educational
programs for allied health
personnel in engaging human
resources to support universal
healthcare systems? Figure 1- Educational Meetings for allied health personnel in Brazil’s countryside
Unified Health System (SUS)
Intense social participation has been a cornerstone of the SUS since the grassroots movements that resulted in Brazilian healthcare system reform in the 1970s and 1980s.
The implementation of a universal healthcare system in Brazil began in an unfavorable political and economic climate, which promoted a neoliberal, private delivery of care rather than an universal approach.
Brazil has profited from a strong and committed healthcare system reform movement, including not only academics, policy makers, and managers, but also health workers from all levels (allied healthpersonnel, support staff, nurses, and doctors), trade unionists, and citizens.
Permanent Health Education (PHE)
The PHE policy was formulated by the Pan American Health Organization (PAHO) in the early 1990’s in Latin America.
The aim of this policy was to support healthcare reforms in Latin America, providing tools to improve the quality of healthcare delivery by increasing the skills of healthcare workers.
PHE started by assuming the incapability of traditional educational models to shift older healthcare practices toward universal healthcare in the Americas.

Permanent Health Education (PHE)
PHE consists of on-the-job learning, where learning and teaching embrace the day-to-day activities of healthcare facilities, building knowledge from the grassroots up.
How???
No Pedagogical Recipes.Workers learn from and teach each other.Workers take ownership of seeking changes in
healthcare delivery.
PHE becomes reality by reflecting the day-to-day practices inside the healthcare workplace, aiming at their transformation and respecting the “library” of knowledge that each and every worker has.
PHE does not just focus on medical education, but also on broader education programs for all majors in healthcare professions, as well as all levels of training.
The key principle of PHE lies in the educational network embracing the entire healthcare system.
Permanent Health Education (PHE)
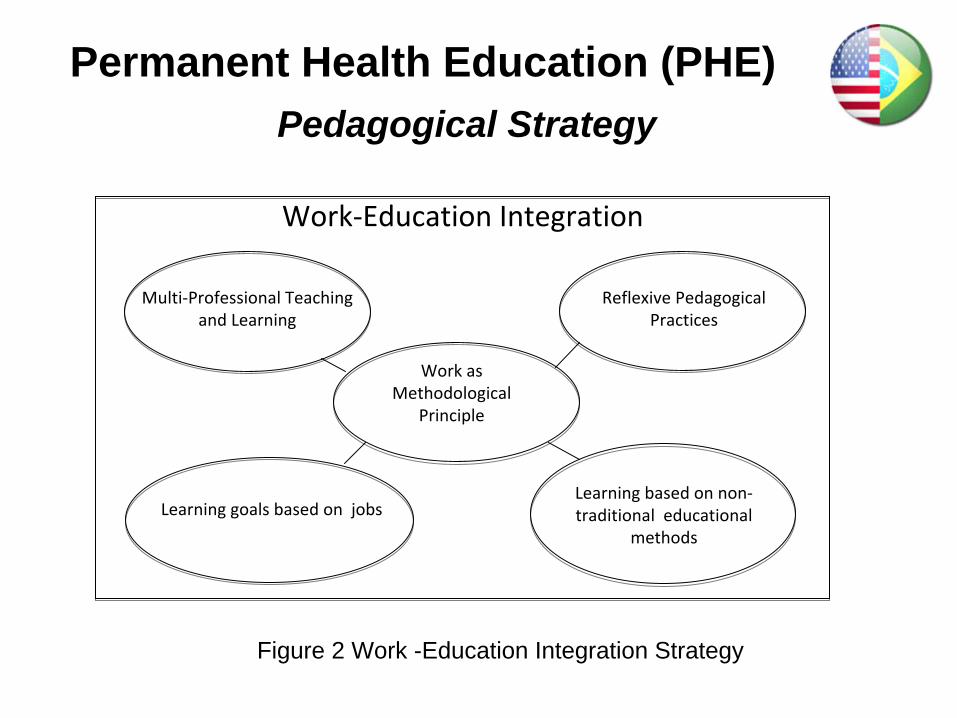
Pedagogical StrategyPermanent Health Education (PHE)
Multi‐Professional Teaching
and Learning
Reflexive Pedagogical
Practices
Work as
Methodological
Principle
Learning based on non‐
traditional educational
methods
Learning goals based on jobs
Work‐Education Integration
Figure 2 Work -Education Integration Strategy
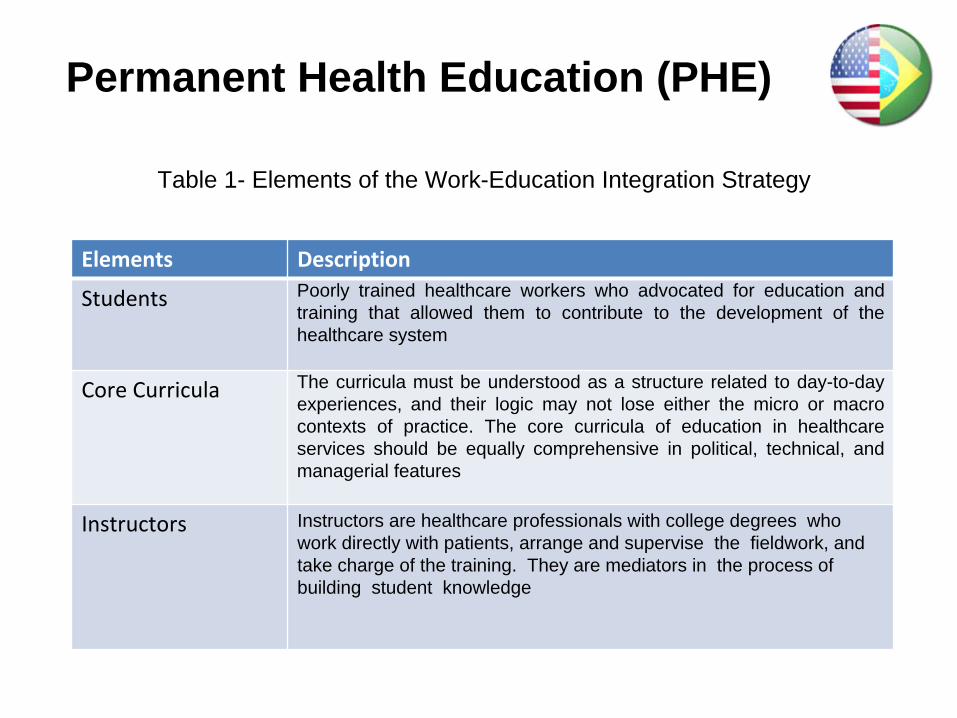
Table 1- Elements of the Work-Education Integration Strategy
Elements Description
Students Poorly trained healthcare workers who advocated for education and training that allowed them to contribute to the development of the healthcare system
Core Curricula The curricula must be understood as a structure related to day-to-day experiences, and their logic may not lose either the micro or macro contexts of practice. The core curricula of education in healthcare services should be equally comprehensive in political, technical, and managerial features
Instructors Instructors are healthcare professionals with college degrees who work directly with patients, arrange and supervise the fieldwork, and take charge of the training. They are mediators in the process of building student knowledge
Permanent Health Education (PHE)
Figure 3- PHE training: workers train workers wherever they are
Emerged initially as Educational Projects-Programs in the 1980’s and 1990’s.
Came about via the struggle of undertrained Allied Personnel (mainly nursing assistants) who were already employed in healthcare services.
Became a national public policy for human resources training in the healthcare system through Decree 198 /2004.
Updated through Decree 1996/2007, which empowered the SUS’s Bipartite and Tripartite Management Committees.
Set training programs for all levels of education in human resources in healthcare.
Permanent Health Education in Brazil
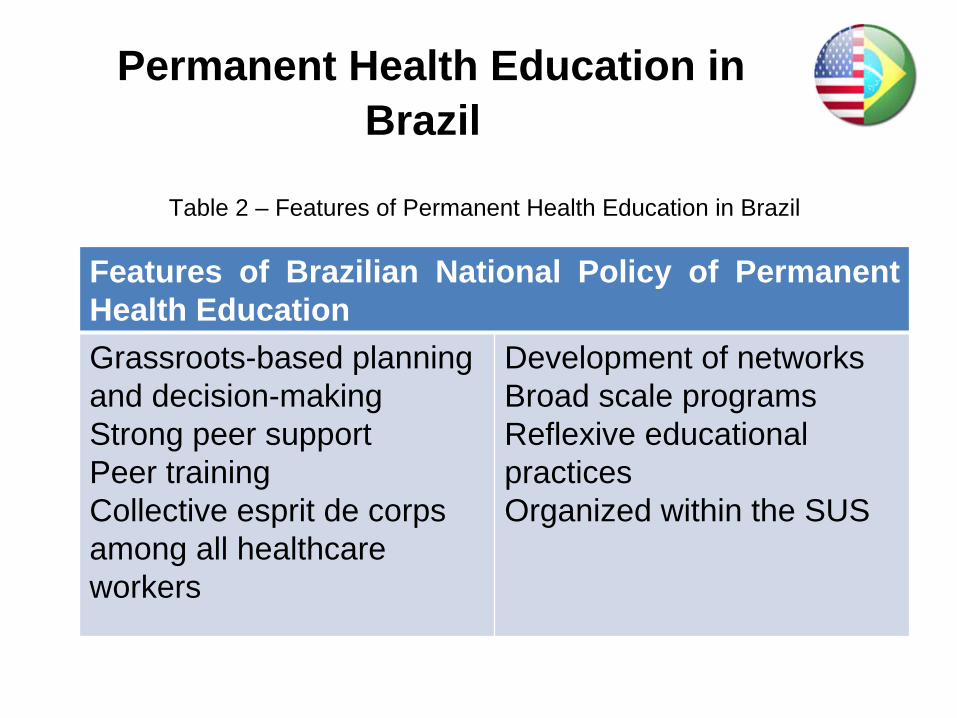
Permanent Health Education in Brazil
Features of Brazilian National Policy of Permanent Health Education Grassroots-based planning and decision-makingStrong peer supportPeer training Collective esprit de corps among all healthcare workers
Development of networksBroad scale programsReflexive educational practicesOrganized within the SUS
Table 2 – Features of Permanent Health Education in Brazil

Table 3- Programs Developed by PHE in Brazil for allied healthcare personnel
Programs Description Number of Workers
Graduated/duration of
program
Allied
Health
Personnel
Broad
Scale
Training
Program (LARGA ESCALA)
Allied
Personnel
who
attended
the
program
fulfilled
broad
tasks
in
the
healthcare
field,
from
management
to
health
care team support
96,000
in
19
years
(1981‐
1989)
Nursing
Staff
Professional
Training Project (PROFAE)
The
program
aimed
at
qualifying
nursing
assis
‐
tants
who
were
required
to have
minimal
education
standards
for
employment in healthcare
319,518 in 09 years (2000
‐2009)
Community
Health
Workers
Training
for
Family
Health Teams
(PACS)
The
training
was
designed
for
Community
Health
Workers
so
as
to
make
them Community
Health
Technicians
153,435 in
07
years
(2004‐now)

DiscussionPHE Origins
PHE originated in the Latin American Social Medicine – known in Brazil as Collective Health – Movement, and advocated for universal health care in the Americas.
The Collective Health’s political and ideological views regarded health not as an exclusively biological issue to be resolved by medicalservices, but as a social and political issue to be addressed by the state.
Latin American movements relied on the potential of healthcare workers to become leaders of transformations in health care systems.
It was based on the ability of education to transform unfair healthcare systems into affordable ones in the Americas.
Discussion
The state of the SUS todayImplementation of the SUS has been complicated by
state support for the private sector, the concentration of healthcare services in more developed regions, and chronic underfunding of the public healthcare infrastructure.
Despite these limitations, the SUS has managed to vastly improve access to primary and emergency care, reach universal coverage of vaccination and prenatal care, and invest heavily in the expansion of human resources and technology, including major efforts to produce the country’s essential drugs.
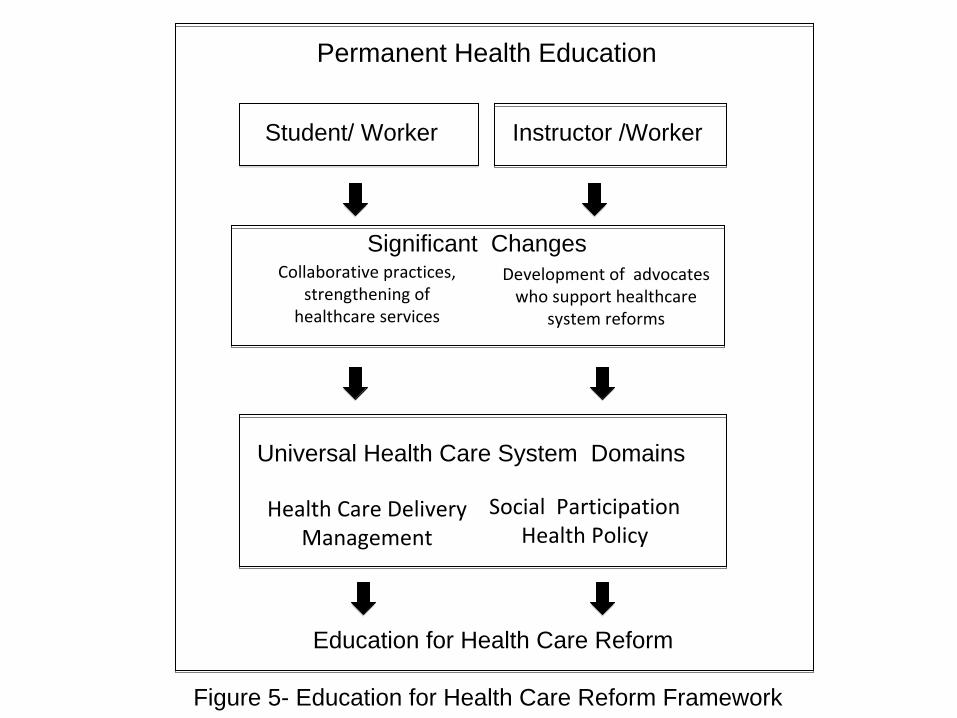
Permanent Health Education
Development of advocates
who support healthcare
system reforms
Universal Health Care System Domains
Health Care DeliveryManagement
Collaborative practices,
strengthening of
healthcare services
Figure 5- Education for Health Care Reform Framework
Student/ Worker Instructor /Worker
Education for Health Care Reform
Social ParticipationHealth Policy
Significant Changes
Conclusion
The Permanent Heath Education Framework has surpassed the role of a mere educational strategy and become an important political tool for the SUS in the ongoing Brazilian healthcare reform.
Mass educational programs for allied healthcare personnel can strengthen the grassroots human resources of the healthcare system. Healthcare workers may become advocates who stand for universal healthcare in their communities.
Finally….
This speculative approach must be validated by
the academic community, using qualitative
research to assess the influence of mass
educational programs for allied healthcare
personnel in creating pro healthcare reform
advocates.

References
1. Armstrong P, Armstrong H. About Canada Health Care. Manitoba: Fernwood Publishing; 2008. 2. Arouca ASS. O Dilema Preventivista Contribuição para Compreensão e Crítica da Medicina Preventiva. Campinas: UNICAMP; 1975 (Tese de Doutorado). 3. Paim J, Travassos C, Almeida C, Bahia L, Macinko J. The Brazilian health system: history, advances, and challenges. Lancet 2011; 377: 1778–1797.4. Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet 2010; 376:1923-1958.5. Tang KC, Nutbeam D, Kong L, Wang R Yan J. Building capacity for health promotion—a case study from China. Health Promot Int 2005; 20(3);285-295.6. Ceccim RB, Feuerwerker LCM. O quadrilátero da formação para a área da saúde: ensino, gestão, atenção e controle social. Physis Rev Saúde Coletiva 2004; 14(1):41-65.
References
7. World Health Organization. The World Health Report 2006 – Working Together for Health. Geneva: WHO; 2006. 8. World Health Organization. The World Health Report 2008 Primary Health Care – Now More Than Ever. Geneva: WHO; 2008. 9. World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice. Geneva: WHO; 2010.10. Cohen JJ. Medical Education in an Era of Health-Care Reform. Perspect Biol Med 2011;54(1):61-67.11. Rieselbach RE, Crouse BJ, Frohna JG. Teaching Primary Care in Community Health Centers: Addressing the Workforce Crisis for the Underserved. Ann Intern Med 2010; 19;152(2):118-122. 12. Sales CS, Schlaff AL. Reforming medical education: A review and synthesis of five critiques of medical practice. Soc Sci Med 2010;70(11):1665-1668.13. Davini MC. Bases Conceptuales y Metodológicas para la Educación Permanente del Personal de Salud. No 19. Buenos Aires: Organização Pan Americana da Saúde OPAS; 1989.
14. Souza AMA, Galvão EA, dos Santos I, Roschke MA. Processos educativos nos serviços de saúde. Série desenvolvimento de Recursos Humanos n0 1. Brasília: OPAS; 1991. 15. Davini MC, Nervi L, Roschke MA. La Capacitación del Personal de Los Serviços de Salud en Proyectos Relacionados con los Procesos de Reforma Sectorial. Programa de Desarrollo de recursos Humanos. Washington D.C.: OPAS; 2002 16. Organização Pan Americana da Saúde. Saúde nas Américas, 2007. Washington, D.C.: OPAS; 2007.17. Bosi MLM, Mercado-Martinez FJ. Evaluation models and Brazilian health reform: a qualitative participatory approach. Rev Saúde Pública 2010; 44(3);1-418. Brasil. Ministério da Saúde. Portaria n0198 de 13 de fevereiro de 2004 que Institui a Política Nacional de Educação Permanente em Saúde como estratégia do Sistema Único de Saúde para a formação e o desenvolvimento de trabalhadores para o setor e dá outras providências. Brasília: Diário Oficial da União; 2004.
References

19. Ceccim RB. Educação Permanente em Saúde: descentralização e disseminação de capacidade pedagógica na saúde. Ciênc. saúde coletiva 2005;10(4): 975-986. 20. Marandola TR, Marandola CMR, Regina Melchior, Baduy RS. Educação Permanente: conhecer para compreender. Rev Espaço para Saúde 2009 jun;10(2): 53-60.21. Pan American Health Organization. Health Systems and Services Profile – Brazil. Monitoring and Analysis of Health Systems Change/Reform. Brasília: PAHO; 2008.22. Sório RER. Educação profissional em saúde no Brasil: a proposta das Escolas Técnicas de Saúde do Sistema Único de Saúde. Formação 2002; 2(5): 45-57.23. Santos I. Escolas Técnicas de Saúde do Sistema Único de Saúde (ETSUS). Formação 2002; 2 (5): 87-95.24. Fundação Oswaldo Cruz. Um balanço da política Nacional de Educação Permanente em Saúde. RET-SUS. 2010; 5 (39): 12-16.
References
25. Fundação Oswaldo Cruz. Antes da Rede. RET-SUS 2011; 5 (41): 05-06.Campos, GWS. Reforma da Reforma repensando a saúde. 2a Ed. São Paulo: Ed. Hucitec 1997.26. Revista Formação. Oferta de qualificação é necessária para melhorar a atenção à saúde. Brasília: Ministério da Saúde.;2001.27. Paim, JS. O que é o SUS. Rio de Janeiro: Editora Fiocruz: 2009. 28. Brasil. Ministério da Saúde. Secretaria de Gestão do Trabalho e da Educação na Saúde. (Personal Communication Dec 20 2010).29. Amestoy SC, Schveitzer MC, Meirelles BHS, Backes VMS, Erdmann AL. Paralelo entre educação permanente em saúde e administração complexa. Rev Gaúcha Enferm 2010;31(2):383-387.30. Brasil. Ministério da Saúde. Secretaria de Gestão do Trabalho e da Educação na Saúde. Relatório de Gestão. Brasília, 2006.31. Conselho Nacional de Secretários de Estado de Saúde. Avaliação dos Pólos de Educação Permanente. Brasília: CONASS; 2006.32. Brasil. Decreto Nº 7.385, de 8 de dezembro de 2010. Institui a Universidade Aberta do SUS – UMA-SUS, e dá outras providências. Brasíla: Diário Oficial da União; 2010.
References
33. Camargo KR. Celebrating the 20th Aniversary of Ulisses Guimaraes’ Rebirth of Brazilian Democracy and Creation of Brazil’s National Health Care System. American Journal of Public Health 2009; 99 (1):30-31.34. Waitzkin H, Iriart C; Estrada A, Lamadrid S. Social medicine then and now: Lessons from Latin America. Am J Public Health 2001;91(10);1592- 1601. 35. Tajer D. Latin American Social Medicine: Roots, Development During the 1990s, and Current Challenges. Am J Public Health 2003:93(12); 2023-2027.36. Freire P. Pedagogia do oprimido. 47 ª ed. Rio de Janeiro: Paz e Terra; 2005.37. Foucault M. Microfísica do poder. Rio de Janeiro, Graal: 1985.Fleury, SMT. A análise necessária da Reforma Sanitária In: Saúde e Debate n0 22.CEBES, 1988.38. Fleury S. Brazil’s health-care reform: social movements and civil society. Lancet 2011;377:1724-1725.39. Fleury S, Ouverney ALM, Kronemberger TS, Zani FB. Governança local no sistema descentralizado de saúde no Brasil. Rev Panam Salud Publica 2010; 28(6): 446-455. 40. Paim JS, Nunes TCM. Contribuições para um Programa de Educação Continuada em Saúde Coletiva. CAD Saúde Pública. 1992:8(3);262-269.
References
41. Kopp W, Farr S. A chance to make history. New York: Public Affairs; 2011.42. Ocké-Reis CO, Marmor TR. The Brazilian national health system: an unfulfilled promise? Int J Health Plann Manage 2010; 25 (4): 318-329.43. Coelho IB. Democracia sem equidade: um balanço da reforma sanitária e dos dezenove anos de implantação do Sistema Único de Saúde no Brasil. Ciênc. saúde coletiva 2010; 15(1): 171-183 44. Instituto de Pesquisa Econômica Aplicada. Sistema de Indicadores de Percepção Social-Saúde. Rio de Janeiro: IPEA; 2011.45. Macinko J, de Oliveira VB, Turci MA, Guanais FC, Bonolo PF, Lima-Costa MF. The Influence of Primary Care and Hospital Supply on Ambulatory Care- Sensitive Hospitalizations Among Adults in Brazil, 1999-2007. Am J Public Health. 2011. [Epub ahead of print]46. European Observatory on Health Care Systems. Health Care System in Transition: United kingdom. London: WHO Europe;1999.47. European Observatory on Health Care Systems and Policy. Health Care System in Transition: France. Copenhagen: WHO Europe; 2004. Ceccin RB. 48. Resenha Saúde é luta: lutar com a formação? Cad. Saúde Pública 2009; 254(10):2299-02.
References
49. Medicc. Cuba & the Global Health Workforce: Health Professionals Abroad. Medical Education Cooperation with Cuba. 2007. Available from: http://www.medicc.org/ns/index.php?s=12&p=0. Accessed 19 Apr 11.50. Feo O. Neoliberal Policies and their Impact on Public Health Education: Observations on the Venezuelan Experience. Social Medicine 2008; 3(4); 223- 231.51. Trotsky-Sirr R. Adentro Barrio Adentro: An American Medical Student in Venezuela. Social Medicine 2008; 3(4); 248-252.52. Patel K; McDonough J. From Massachusetts To 1600 Pennsylvania Avenue: Aboard The Health Reform Express. Health Aff 2010; 29 (6);1106-1111.53. Barr DA. Health Disparities in the United States. Baltimore: The Johns Hopkins University Press: 2008.54. Reid TD. The Healing of America: A Global Quest for Better, Cheaper, and Fairer Health Care. New York: Penguin Books: 2009.55. Milstein B, Homer J, Hirsch G. Analyzing National Health Reform Strategies With a Dynamic Simulation Model. Am J Public Health 2010; 100;811-819.56. World report. Political tussle continues over US health-care reform. Lancet 2011;377:1821-1822. 57. Editorial. Brazilian Democracy and Creation of Brazil’s National Health Care System. Am J Public Health 2009; 99 (1):30-31.
References