can ultrasound help to define orthopedic surgical complications?
TRANSCRIPT

Tupw
CiefiiuMppsa
orscoct
cciuia
FRg3C©0d
C
Can Ultrasound Help to Define OrthopedicSurgical Complications?
Sonia Carbó, MD, Nuria Rosón, MD, Sara Vizcaya, MD,
Fernanda Escribano, MD, Manuela Zarcero, MD, and Santiago Medrano, MDbac
rr
ISwt
tra
brf
ecbcmmt
cBmrfif9
a
his article aims to describe and illustrate the usefulness ofltrasound in detecting complications of orthopedic im-lants, metal fixation devices, and other surgical material,ith an emphasis on soft-tissue pathology.
omputed tomography (CT) and magnetic resonancemaging (MRI) can have several limitations in thevaluation of soft tissue around metallic prostheses orxation devices. Beam hardening and the susceptibil-
ty to ferromagnetic artifacts make an adequate eval-ation difficult or impossible. Although new CT andRI technologies decrease these artifacts and make it
ossible to obtain diagnostic-quality images, specificlaces may remain occult in these techniques. Ultra-ound can provide relevant information that can obvi-te other complementary examinations in these cases.
The high capability of ultrasound (US) for detectionf metal bodies and the ability to study soft tissue ineal-time, as well as ease of use, low cost, patientatisfaction, and the lack of ionizing radiation, arelear advantages of this modality over others. More-ver, US is able to guide needle biopsy or aspiration toonfirm the diagnosis, as well as to perform therapeu-ic injections.
This report describes and illustrates the differentomplications of orthopedic surgery, such as fluidollections and postoperative seromas, periprostheticnfections, abscesses, pseudobursae, aggressive gran-lomatous disease (histiocytic response), stress shield-ng/endosteal resorption and breakage of cortical bone,nd soft-tissue impingement such as tendonitis or
rom the SDI Hospital General de Granollers, Barcelona, Spain.eprint requests: S. Carbó, Fundacio Hospital/Asil de Granollers, Avin-uda Francesc Ribas s/n, 08400 Granollers (Barcelona), Spain. E-mail:[email protected] Probl Diagn Radiol 2006;35:75-89.2006 Mosby, Inc. All rights reserved.
363-0188/2006/$32.00 � 0
ooi:10.1067/j.cpradiol.2006.03.001urr Probl Diagn Radiol, May/June 2006
ursitis. US can also provide additional informationbout delayed or nonunion fractures diagnosed byonventional radiography.
We have presented an extensive complementaryeview of the literature about the usefulness of sonog-aphy in orthopedic surgical complications.
nfectionuperficial infection in orthopedic hardware is some-hat more common but is more easily diagnostic and
reatable (incidence 3 to 4%).1
Although the rate of infection after primary implanto the hip and knee is lower (between 0.5 and 2%,espectively), infection of metallic hardware is gener-lly a serious complication.1
There is a large overlap between the morphology ofone findings in these entities at conventional radiog-aphy and it is essential to evaluate other parametersor correct diagnosis.2,3
Clinical parameters, laboratory findings (elevatedrythrocyte sedimentation rate, and blood whiteount), serial follow-up radiographs, and radionuclideone scan easily provide the correct diagnosis in mostases. Although an indolent infection may mimicechanical loosening of a prosthesis, the most com-on situation calls for ruling out of low-grade infec-
ion in cases of prosthetic loosening.Radionuclide studies are the imaging method of
hoice because of their high negative-predictive value.one scintigraphy reveals activity over a 6- to 12-onth postoperative period. It has limited value for
uling out loosening or prosthetic infection during therst year.4,5 The most specific radionuclide for in-ection (11Indium-labeled-leukocyte combined with9mTc-sulfur colloid) can help in the diagnosis with anccuracy of 90%.6 Other reports describe an accuracy
f 81%, specificity of 73% if the radionuclide is75
1
1
tta
pulocsn
i
rtdfipfji
teaid
isdciei(
bthinbat
Fpst
Fmim
7
1Indium, and a sensitivity of about 100% but only8% specificity if the radionuclide is technetium.1
However, the poor anatomic resolution of thisechnique makes it difficult or impossible to differen-iate among cellulitis, synovitis, and inflammatoryrthritis.4
Recent articles predict that fluorodeoxyglucoseositron emission tomography (FDG-PET) will besed to differentiate between infection and mechanicaloosening in the future; at present it has no advantagever three-phase bone scintigraphy. These studiesoncluded that FDG-PET was more specific but lessensitive than conventional radiography for the diag-osis of infection.7
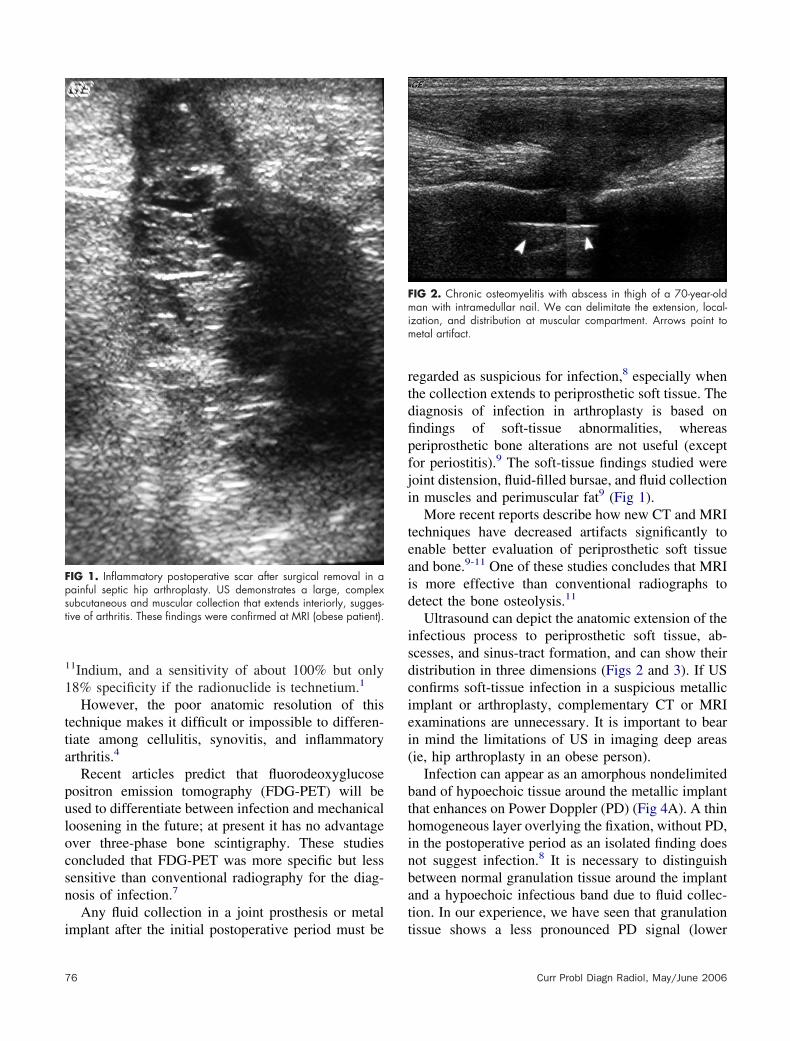
Any fluid collection in a joint prosthesis or metal
IG 1. Inflammatory postoperative scar after surgical removal in aainful septic hip arthroplasty. US demonstrates a large, complexubcutaneous and muscular collection that extends interiorly, sugges-ive of arthritis. These findings were confirmed at MRI (obese patient).
mplant after the initial postoperative period must be t
6
egarded as suspicious for infection,8 especially whenhe collection extends to periprosthetic soft tissue. Theiagnosis of infection in arthroplasty is based onndings of soft-tissue abnormalities, whereaseriprosthetic bone alterations are not useful (exceptor periostitis).9 The soft-tissue findings studied wereoint distension, fluid-filled bursae, and fluid collectionn muscles and perimuscular fat9 (Fig 1).
More recent reports describe how new CT and MRIechniques have decreased artifacts significantly tonable better evaluation of periprosthetic soft tissuend bone.9-11 One of these studies concludes that MRIs more effective than conventional radiographs toetect the bone osteolysis.11
Ultrasound can depict the anatomic extension of thenfectious process to periprosthetic soft tissue, ab-cesses, and sinus-tract formation, and can show theiristribution in three dimensions (Figs 2 and 3). If USonfirms soft-tissue infection in a suspicious metallicmplant or arthroplasty, complementary CT or MRIxaminations are unnecessary. It is important to bearn mind the limitations of US in imaging deep areasie, hip arthroplasty in an obese person).
Infection can appear as an amorphous nondelimitedand of hypoechoic tissue around the metallic implanthat enhances on Power Doppler (PD) (Fig 4A). A thinomogeneous layer overlying the fixation, without PD,n the postoperative period as an isolated finding doesot suggest infection.8 It is necessary to distinguishetween normal granulation tissue around the implantnd a hypoechoic infectious band due to fluid collec-ion. In our experience, we have seen that granulation
IG 2. Chronic osteomyelitis with abscess in thigh of a 70-year-oldan with intramedullar nail. We can delimitate the extension, local-
zation, and distribution at muscular compartment. Arrows point toetal artifact.
issue shows a less pronounced PD signal (lower
Curr Probl Diagn Radiol, May/June 2006

iht
httbdhsJpoctrsnddflancbF
flhin
ceto2rapc
Fhgt
Fsi(ra
C
ntensity and fewer vessels), less thickness, and a moreomogeneous distribution around the hardware thanhe infectious band (Fig 4B).
The value of PD US in the detection of soft-tissueyperemia is well known and extensively reported inhe literature.12-14 The knee is more accessible to UShan the hip. The effectiveness of PD to detect lowlood flow in the synovial tissues of the hip has beenemonstrated.15 This can be extrapolated for detectingyperemia in other inflammatory-infectious diseasesuch as orthopedic septic complications (Figs 5 and 6).oint effusion is easily detected and correlated with hiprosthesis infection when an anterior pseudocapsulever the proximal femur is present (mean bone-to-apsule distance 10.2 mm)16 (Fig 7). In some cases,his technique has its limitations: a distended anteriorecess or one with internal echoes can be foundecondary to synovitis; in others cases, hyperemia isot always present, and the recess can be filled withebris due to plastic wear. Moreover, it can be veryifficult to differentiate anechoic from hypoechoicuid in patients with altered anatomy due to surgerynd in those with large bodies.17 Some reports haveot found a relation between joint effusion and me-hanical or septic loosening because joint effusion cane present in both conditions and secondary causes.18
or this reason, aspiration must be performed.Ultrasound-guided aspiration is simple when the
uid collection is accessible. Routine aspiration of theip joint before revision is controversial. The sensitiv-ty (S), specificity (Sp), and positive-predictive and
IG 3. Partial shoulder arthroplasty after comminuted fracture of theumeral head. Note the hypoechoic band around the prosthesis andleno-humeral joint (small arrow) and sinus tract formation in the soft
issues (arrows); the fistulous tract does not extend to subcutaneous fat.
egative-predictive values (PPV and NPV) of aspirate s
urr Probl Diagn Radiol, May/June 2006
ultures reported in the literature vary widely. Thearliest studies reported 13% incidence of false posi-ives and a sensitivity between 2 and 12%.19,20 An-ther series showed 17% false negatives (in a total of05 aspirations).21 In contrast, other studies haveeported 91 to 92.8% S and 82 to 91.7% Sp22,23;nother study found 54.2% PPV and 99.2% PNV forreoperative aspiration guided by arthrography andoncluded that aspiration should only be done in
IG 4. (A) Infectious humeral component of partial arthroplasty in theame patient as Fig 3. The PD signal is more intense, with more vesselsnvolved, and the infectious band is more heterogeneous and thickerarrow shows prosthesis) than in granulation tissue (B). The artifact ofeverberation at the bone–metal interface at left. (Color version of figure isvailable online.)
elected patients with high risk of infection rather than
77

oec
cpy
tmpcspd
sonwitsdnoc
Faw
F1pbPfa
Ffcps
7
n a routine basis. The high risk consists of anlevated erithrocyte sedimentation rate or white blood
IG 5. Fever in a 60-year-old woman with elbow prosthesis. Intra-rticular heterogeneous fluid with high PD enhancement is consistentith infection. (Color version of figure is available online.)
IG 6. Open comminuted fracture of the distal femoral diaphysis in a0-year-old child with external fixation. A bone graft was latererformed for pseudoarthrosis. Fever appeared 2 months after theone graft was performed. US findings were a hypoechoic band withD signal around the cortical bone, osteosynthetic material, and in theracture foci. The medial gastrocnemius also shows inflammatoryctivity. (Color version of figure is available online.)
ell count and pain disproportionate to radiographic t
8
hange.23,24 They also found that infection has lowrevalence in hip arthroplasty performed more than 5ears prior.25
Positive culture of fluid obtained during surgery ishe gold standard for the diagnosis of infection. If theaterial obtained is purulent or the Gram stain is
ositive with polymorphonuclear cells in a clinicalontext of medium-high risk of infection, the diagno-is is practically ensured.26 US is useful because it canrovide relevant information and thereby obviate ad-itional complementary tests.
Sometimes, the radiologist is faced with the oppo-ite situation, a clinical sign of local cellulitis, veryften the only clinical sign with or without subcuta-eous abscess in the skin scar, and must determinehether it is merely a superficial infection or whether
t represents the extension of a hardware infection tohe surgical approach. US can determine whetheruperficial affection represents the extension of aeeper infectious process (Figs 8 and 9). US exami-ation with normal results does not allow exclusion ofsteomyelitis. It is necessary to find a correlation tolinical findings, laboratory data, and other imaging
IG 7. Fracture of a femoral component in a 75-year-old man who hadever and signs of infection at the surgical approach during convales-ence. US confirms the concomitant arthritis. Arrows mark the dis-laced pseudocapsule of hypoechoic fluid. Infection was confirmed aturgery. The small arrows mark the prostheses.
echniques.8
Curr Probl Diagn Radiol, May/June 2006

ETpslttmd
dnftapsbta
dvsm
FobTco
Fpssec
C
arly Postoperative Periodhe most common and important problem in the earlyostoperative period after hip or knee arthroplasty is awollen limb. Thrombosis of the popliteal vein, cellu-itis, the rupture of an occult residual Baker’s cyst afterotal arthroplasty, hematomas, seromas and collec-ions, and, less frequently, compartment syndromeust be considered. US plays an important role in
ifferentiating these entities.It is well known that US is very sensitive in the
etection of deep-vein thrombosis.27 This capability isot restricted to the great veins such as the popliteal,emoral, or tibioperoneal vein. US can also evaluatehe veins of the calf, gastrocnemius, or soleus veins,nd its performance is best when the patient has a focaloint of tenderness. In some cases the fibrovascularepta and the muscular areas and surrounding throm-ophlebitic vein show increased echogenicity in con-rast to the hypoechogenicity of fibrovascular septae
IG 8. Inflammatory reaction in the later postoperative period of tibialsteotomy with signs of incipient pseudo-arthrosis. The hypoechoicand is thick and heterogeneous, with PD increase, without collection.he bone scan, clinical history, fever, and sonography findings wereompatible with infection. Arrow marks the hardware. (Color versionf figure is available online.)
ffected by infectious or acute compartment syn- t
urr Probl Diagn Radiol, May/June 2006
rome. The efficiency of Doppler US in detecting deepein thrombosis in patients undergoing orthopedicurgery was estimated. Soleal vein thrombosis was theost prevalent and US was more efficient than con-
IG 9. Patient with distal amputation of tibia 10 years prior whoresented with superficial tenderness and inflammatory signs. (A) UShows subcutaneous fat involvement with increased PD signal in theuperficial scar without deeper extension. (B) MRI ruled out osteomy-litis. Intramedullary vessels should not be confused with an infectiousollection (arrows). (Color version of figure is available online.)
rast venography at detecting it.27 However, thrombo-
79

sp
tugsmasfluease
tptepi
apdrtittT
lm
sdovpicprtai
Fw
Fapw
Fmeacwc
8
is will extend to the popliteal vein in only 3% ofatients in a follow-up period of 3 months.28
Cellulitis is usually the other entity that complicateshe postoperative period. A swollen and painful leg issually a sign and the diagnosis is made on clinicalrounds. Predisposing conditions are venous stasis,kin infections, burns, and immunosuppression. Theore common microorganisms are Staphylococcus
ureus and Streptococcus pyogenes.5,18 Cellulitis pre-ents a cobblestone pattern with strands of hypoechoicuid in the fibroadipose septa delimiting fat lob-les.29,30 If it progresses, destroyed tissue showingnhanced PD and coalescent hypo-anechoic areasppears, forming an abscess. The first step is notpecific and we cannot differentiate subcutaneousdema secondary to other causes.
The rupture of an occult residual Baker’s cyst afterotal knee arthroplasty can often mimic a thromboticopliteal vein. It is easily diagnosed as a cystic mass inhe popliteal fossa with an anechoic band of fluid thatxtends and dissects anatomic planes. Adjacent hy-erechoic subcutaneous or popliteal fat owing tonflammatory reaction may be present.
Hematomas or seromas around the hardware arenother cause of swollen limbs in the postsurgicaleriod (Figs 10 and 11). These lesions are wellemonstrated and defined by US without inflammatoryeaction and without PD signal (Fig 12). It is importanto note that PD cannot reliably differentiate betweennflammatory collections of infectious or noninfec-ious origin18,31 (Fig 10). Seromas can present with ahick capsule delimited by a thin hyperechoic line.
IG 10. A large hematoma within the thigh muscles of a patient inhom anticoagulant treatment was reintroduced after hip arthroplasty.
his line is an epithelial layer that obstructs physio- s
0
ogical resorption; it sometimes needs surgical treat-ent (Fig 13).Acute compartment syndrome is muscle edema
econdary to high pressure in the muscular spaceelimited by compartmental fascia. The compromisef space could be secondary to hematomas, difficultenous return32 in cases of massive thrombosis, com-ression due to muscular injuries, or inflammatory-nfectious processes that cause ischemic changes. In-ipient findings on US include a hyperechoiceripheral area in each muscle that does not affect theegion adjacent to the fibroadipose septa. Unlessreated early, these findings evolve into hypo-anechoicnd heterogeneous areas with hyperechogenic foci thatndicate regions of irreversible infarction and necro-
IG 11. An elderly woman with swollen and painful leg and kneefter knee arthroplasty. US ruled out thrombosis and showed aathologic soft-tissue collection surrounding the quadricipital tendonith extension to subcutaneous fat and rectus femoris.
IG 12. Knee arthroplasty performed for tumor infection in a youngan with a severely atrophied thigh incapacitated for both flexion andxtension of the knee. US shows integrity of the fibers of the quadricepsnd lateral retinacula extensor. An extensive capsulated anechoicollection can be seen between the bone and vastus intermediusithout PD signal. The small arrow points to the femoral prostheticomponent. The collection was a seroma.
is.33
Curr Probl Diagn Radiol, May/June 2006

LHapasutttwtrf
oLsaipmt
SMt
rmt
iUtb
cocMsmvso
ccgmp
Fisht
FS
Fm
C
ate Postoperative Periodeterotopic ossification is a bone metaplasia that
ppears after prior surgery, most commonly in arthro-lasties of the hip, occurring in as many as 50%. It issymptomatic but can limit articular function whenevere (1 to 5%). Conventional radiographs can besed for diagnosis. Predisposing factors are inflamma-ory disease (ankylosing spondylitis, rheumatoid ar-hritis), diffuse idiopathic skeletal hyperostosis, infec-ion, Paget disease, and a severely degenerated hipith significant muscular contraction in men. The best
reatment is prophylactic use of indomethacin andadiotherapy, although neither usually achieves satis-actory results.1,4
Complications involving surgical sutures in tendonsr nerves are possible later in the postoperative period.imited mobility is not uncommon after surgicaluture of a tendon. The cause can be a suture failure,
hypertrophic scar that impedes correct mobility,ntra-articular adherence, or a neurological lesion. USrovides information about the static anatomy and,ore importantly, the dynamic examination can define
he scar and the degree of entrapment (Fig 14).
oft-Tissue Impingementusculoskeletal US provides useful information when
IG 13. Seroma after hip arthroplasty in an obese man. The collections anechoic, multiseptated with thin and mobile septa without PDignal. The arrows point to a thick capsule delimited by a thin lineyperechoic (small arrow). This line is an epithelial layer that impedeshe fluid absorption. This was confirmed by aspiration.
here is a specific or localized clinical finding. The n
urr Probl Diagn Radiol, May/June 2006
eal-time capability of US performed during jointotion can show painless impingement of a sliding
endon that occurs only during specific movements.While conventional radiographs and clinical exam-
nation may be useful to suspect tendon impingement,S enables the direct visualization of the degree of
his impingement, as well as tendonitis, tenosynovitis,ursitis, and partial, full, or split tendon sections.
Ultrasound also detects impingement due to directontact between the metal fixation and the soft tissues,sseous fracture fragments, or osteophytes.34 Bothonditions and impingement are difficult to identity byRI because artifacts obscure these tightly adjoining
tructures and the low MR signal of the bone frag-ents can be misinterpreted (Fig 15). This condition is
ery common in ankle fractures where the tendonsurrounding the ankle joint are in contact with the headf a screw or interlocking fixation (Fig 16).
The appearance of pain or other complaints after alinically silent postoperative period in metal implantsan be regarded as a possible complication. Serial radio-raphs can show a change or hardware migration. Theigration of large intramedullary nails, such as Hoffa fat
ad migration (Fig 17), and intra-articular, intratendi-
IG 14. A finger with distal flexion failure after surgical suture.uperficial flexor tendon gap by sonography marked by arrows.
IG 15. Bimaleolar fracture with intra-articular fragments. The arrowsark the capsule and the joint effusion.
ous, or subcutaneous tip position, are signs of postop-
81

er
j
lp
ooo
na
ocbtd
Ft
FH
Fand places it in intra-articular localization (arrows).
Fbursitis (arrows).
Fp
8
rative complication. Sometimes, this is an indication toemove the osteosynthetic material ( Fig 18).
Inflammatory skin signs can be a translation of sub-acent bursitis, usually in olecranon fractures ( Fig 19).
The wires used in patella fractures or intramedul-ary nails that migrate upward can cause tendonitis orartial tendon sectioning (Fig 20).
Painful tendonitis is very common at the beginningf the rehabilitation period; in these cases, US can ruleut a possible complication and confirm the integrityf tendinous structures (Fig 21).
Another entity is synovitis, which is easily diag-osed in superficial articulation of the knee, wrist, ornkle (Fig 22).
Snapping syndrome or iliopsoas impingement (IPI)n the acetabular component is an infrequent compli-ation in total hip replacement. It consists of frictionetween the iliopsoas tendon and the cup or the screwshat fix it. CT is the modality of choice to make the
IG 16. Focal synovitis of anterior tibial tendon due to friction againsthe head of the screw. (Color version of figure is available online.)
IG 17. Patellar tendonitis due to migration of fixation hardware tooffa’s fat pad. The arrows show the tip of the nail.
iagnosis: more than 12 mm overhang of the acetab- p
2
IG 18. The head of the interlocking screw displaces the synovium
IG 19. Tip of the intramedullary nails inside the triceps tendon and
IG 20. Cerclage wire with a portion inside the patellar tendon. Theatient experienced pain at the beginning of rehabilitation. The arrows
oint to the artifact and an area of tendonitis around the wires.Curr Probl Diagn Radiol, May/June 2006

udt
epvtqoonc
o
epedlt
capm
tpkIawm
b
FtU
F(
C
lar cup is a sensitive and specific parameter foriagnosis of IPI.35 A report in the literature describeshe IPI by US.36
US can estimate the function of the medial collat-ral ligament in cases of lateral instability of a kneerosthesis. This complication is usually seen withalgus stress maneuvers but sometimes the results ofhe clinical examination are inconclusive. This is oneuestion that the orthopedic surgeon may ask a radi-logist. The treatment is “orthopedic external fixation”r, if significant clinical findings are present, it may beecessary to replace the prosthesis with a tight-fittingentral peg to provide medial-lateral stability.
Patients who have undergone shoulder arthroplasty
IG 21. (A) Section of metal fixation suture with preservation of theendon after reconstruction of complete previous patellar rupture. (B)S confirms integrity tendinous in a sagittal plane.
ccasionally complain of pain around the shoulder b
urr Probl Diagn Radiol, May/June 2006
ven though radiographic examination shows correctositioning of the implant without any signs of loos-ning or migration. US can define the soft-tissueisorder as a possible cause of pain such as rotator cuffesions, subdeltoid bursitis, joint effusion, or synovi-is.37
Greater trochanteric bursitis is a common compli-ation of total hip replacement; however, it has few ifny radiological findings. It is said to be the cause ofain in up to 20% of patients following hip replace-ent, presumably because of abnormal stress.1
The bursae that occur around the wires of greaterrochanteric osteotomy are formed by friction and arerobably not normally present. They form around thenots in the wires, which are potential sites of friction.nfectious arthritis of the hip causes increased intra-rticular pressure, which may lead to communicationith one or more of the bursae present around the hip,ost often the iliopsoas bursa.It is important to exclude infection or loosening
ecause the first sign of this can be an incidental
IG 22. Proliferative synovitis in a painful arthroplasty knee (arrows).Color version of figure is available online.)
ursae finding.2,38
83

LMpda
rntfpfwi
crp
dafi
iipcnpcp
sc“
FtT(
8
ooseningechanical loosening is the most common cause of
ain and late complications after hip prosthesis proce-ures and the most common indication for revisionnd removal.39
The diagnosis is reached on the basis of clinical andadiological findings. Follow-up radiographs show aonfocal lucent zone greater than 2 mm surroundinghe entire prosthesis. This is the most sensitive patternor detecting osteolysis in the movement of a painfulrosthesis.39 Another osteolytic pattern corresponds toocal lucencies. We will only discuss the situations inhich US can be useful and can provide valuable
nformation (Fig 23).Foreign-body granulomatosis, which includes mi-
roparticle disease, is an aggressive granulomatouseaction to various components used in arthroplasty:
IG 23. Conventional radiograph of total arthroplasty 5 years postopibial plateau with extension to soft tissue. (B) Color PD signal increase1-weighted MRI sequences. Biopsy ruled out infection and granulomatColor version of figure is available online.)
olyethylene, polymethylmethacrylate, or metal. The g
4
isease presents as an intraosseous lytic mass associ-ted with endosteal scalloping. This low aggressiveeature differs from the bone-aggressive findings ofnfection found in conventional radiographs.1-4
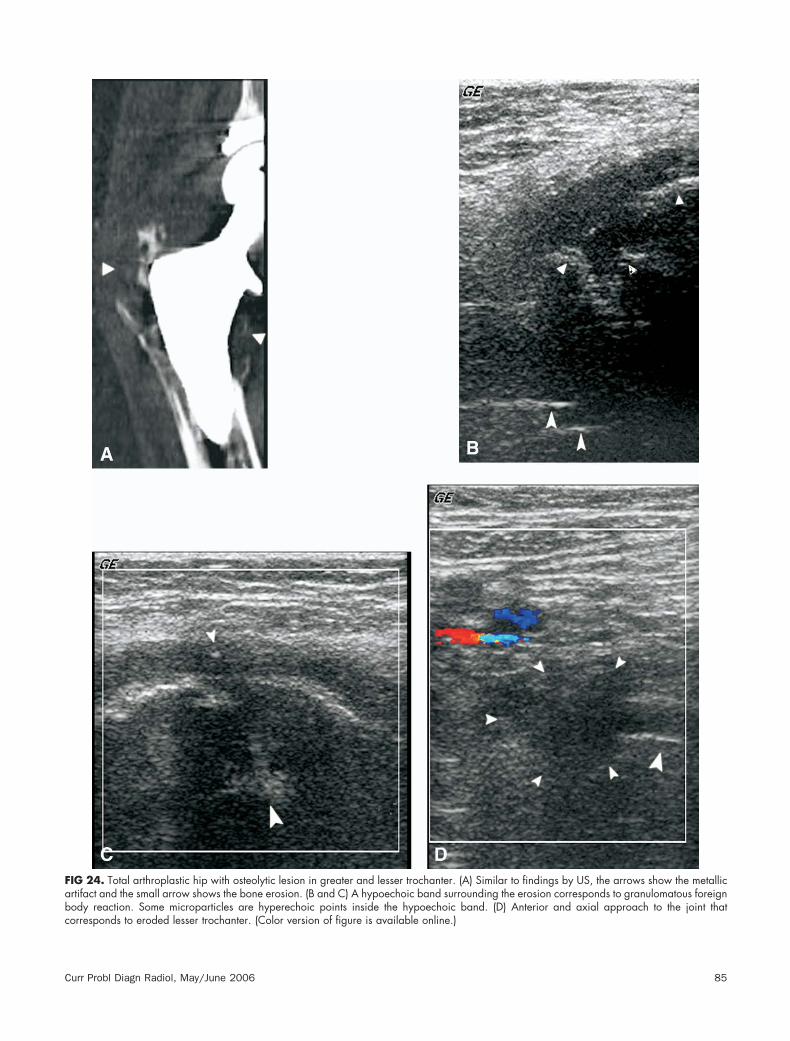
This diagnosis is usually confirmed by radionuclidemaging, CT, or MRI. New CT techniques based onmproved transformation algorithms and image post-rocessing, and special MRI sequences have signifi-antly reduced metal artifacts (Fig 24A). These tech-iques can enable optimal diagnosis; however,roblems may arise when the region of interest lieslose to or inside the “artifact field” (bilateral hiprostheses, the great and minor trochanter area1,3,40).
US shows a heterogeneous mass against a “starryky”8 background; the hypoechoic homogeneousomponent represents histiocytic tissue and thestars” are the microparticles ( Fig 24B-D). This
ve (A) and US (B and C) show lytic lesions of fibular head and laterale periphery of the lesion, which correlates with gadolinium uptake onsion, and the definitive diagnosis was a ganglion cyst inside the bone.
eratis at thous le
ives acoustic shadowing. US can guide biopsy or
Curr Probl Diagn Radiol, May/June 2006
Fabc
C
IG 24. Total arthroplastic hip with osteolytic lesion in greater and lesser trochanter. (A) Similar to findings by US, the arrows show the metallicrtifact and the small arrow shows the bone erosion. (B and C) A hypoechoic band surrounding the erosion corresponds to granulomatous foreignody reaction. Some microparticles are hyperechoic points inside the hypoechoic band. (D) Anterior and axial approach to the joint that
orresponds to eroded lesser trochanter. (Color version of figure is available online.)urr Probl Diagn Radiol, May/June 2006 85

ap
srrgtts
ul
c
CCt
Fswa
8
spiration to rule out infection or to confirm otherossible diagnoses.
Stress shielding is caused by decreased transmis-ion of forces in the native bone because the prosthesisedirects these forces and determines areas of boneesorption. The most affected areas are the lesser andreater trochanter. Stress shielding must not be mis-aken for a lytic lesion, and it is important to note thathis is the first step to focal loosening or complications
IG 25. (A) Olecranon fracture treated with intramedullary nail aonographic planes (anterior, posterior, lateral, and oblique and laterithout vascularization. No periosteal reaction was noted. Pseudo-available online.)
uch as fractures. Shielding is more common in d
6
ncemented areas with excessive filling in which aarge, long femoral component has been fitted.1,2
As a result, sound is transmitted through the thinnedortex8 without expansive or lytic bone lesion.
allus Formationonventional radiography should be used to moni-
or healing fractures. US can help in cases where a
ires. (B-D) Artifacts caused by the metal implant were seen on allique views points with arrows). Note the hypoechoic endosteal callussis was confirmed after surgical revision. (Color version of figure is
nd wal oblrthro
elayed or nonunion fracture is detected at conven-
Curr Probl Diagn Radiol, May/June 2006
tUhhshiiapcvsmd
pfpo
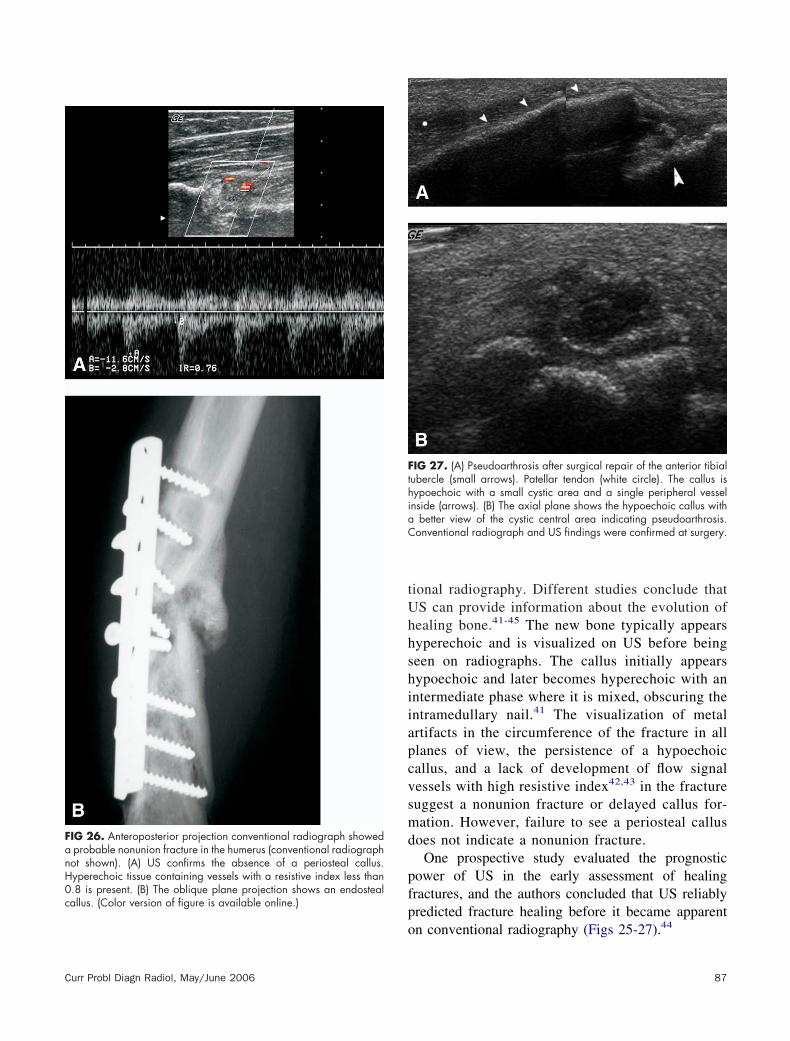
FanH0callus. (Color version of figure is available online.)
FthiaC
Curr Probl Diagn Radiol, May/June 2006
ional radiography. Different studies conclude thatS can provide information about the evolution ofealing bone.41-45 The new bone typically appearsyperechoic and is visualized on US before beingeen on radiographs. The callus initially appearsypoechoic and later becomes hyperechoic with anntermediate phase where it is mixed, obscuring thentramedullary nail.41 The visualization of metalrtifacts in the circumference of the fracture in alllanes of view, the persistence of a hypoechoicallus, and a lack of development of flow signalessels with high resistive index42,43 in the fractureuggest a nonunion fracture or delayed callus for-ation. However, failure to see a periosteal callus
oes not indicate a nonunion fracture.One prospective study evaluated the prognostic
ower of US in the early assessment of healingractures, and the authors concluded that US reliablyredicted fracture healing before it became apparent
IG 27. (A) Pseudoarthrosis after surgical repair of the anterior tibialubercle (small arrows). Patellar tendon (white circle). The callus isypoechoic with a small cystic area and a single peripheral vesselnside (arrows). (B) The axial plane shows the hypoechoic callus with
better view of the cystic central area indicating pseudoarthrosis.onventional radiograph and US findings were confirmed at surgery.
IG 26. Anteroposterior projection conventional radiograph showedprobable nonunion fracture in the humerus (conventional radiographot shown). (A) US confirms the absence of a periosteal callus.yperechoic tissue containing vessels with a resistive index less than.8 is present. (B) The oblique plane projection shows an endosteal
n conventional radiography (Figs 25-27).44
87

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
8
REFERENCES1. Griffiths HJ. Imaging of orthopedic hardware. Radiol Clin
1995;33:2.2. Tigges S, Stiles RG, Roberson JR. Appearance of septic hip
prostheses on plain radiographs. AJR 1994;163:377-80.3. Tigges S, Stiles RG, Roberson JR. Complications of hip
arthroplasty causing periprostetic radiolucency on plain radio-graphs. AJR 1994;164:1387-91.
4. Keogh CF, Munk PL, Gee R, et al. Imaging of the painful hiparthroplasty. AJR 2003;180:115-20.
5. Cardinal E, Bureau NJ, Aubin B, Chhem RK. Role ofultrasound in musculoskeletal infections. Radiol Clin NorthAm 2001;39:191-201.
6. Palestro CJ, Love C, Tronco GG, et al. Role of radionuclideimaging in the diagnosis of postoperative infection. Radio-graphics 2000;20:1649-60.
7. Stumpe KDM, Nötzli HP, Zanetti M, et al. FDG PET fordifferentiation of infection and aseptic loosening in total hipreplacements: comparison with conventional radiography andthree-phase bone scintigraphy. Radiology 2004;231:333-41.
8. Gibbon WW, Long G, Barron DA, et al. Complications oforthopedic implants: sonographic evaluation. J Clin Ultra-sound 2002;30:288-99.
9. Cyteval C, Hamm V, Sarrabère M, et al. Painful infection at thesite of hip prosthesis: CT imaging. Radiology 2002;224:477-83.
0. White L, Kim JK, Mehta M, et al. Complications of total hiparthroplasty: MR imaging—initial experience. Radiology2000;215:254-62.
1. Potter HG, Nestor BJ, Sofka CM, et al. Magnetic resonanceimaging after total hip arthroplasty: evaluation of peripros-thetic soft tissue. J Bone Joint Surg 2004;86:1947-54.
2. Newman JS, Adler RS, Bude RO. Detection of soft-tissuehyperemia: value of Power Doppler sonography. AJR 1994;163:385-9.
3. Martinoli C, Pretolesi F, Crespi G, et al. Power Dopplersonography: clinical applications. Eur J Radiol 1998;27:S133-40.
4. Martinoli C, Derchi LE, Rizzatto G, et al. Power Dopplersonography: general principles, clinical applications, and fu-ture prospects. Eur Radiol 1998;8:1224-35.
5. Walther M, Harms H, Krenn V, et al. Synovial tissue of thehip at Power Doppler US: correlation between vascularity andPower Doppler US signal. Radiology 2002;225:225-31.
6. Van Holsbeeck MT, Eyler WR, Sherman LS, et al. Detectionof infection in loosened hip prostheses: efficacy of sonogra-phy. AJR 1994;163:381-4.
7. Weybright PN, Jacobson JA, Murry KH, et al. Limitedeffectiveness of sonography in revealing hip joint effusion:preliminary results in 21 adult patients with native andpostoperative hips. AJR 2003;181:215-8.
8. Bureau NJ, Chhem RK, Cardinal E. Musculoskeletal infections:US manifestations. Radiographics 1999;19:1585-92.
9. Barrack RL, Harris WH. The value of aspiration of the hipjoint before revision total hip arthroplasty. J Bone Joint SurgAm 1993;75:66-76.
0. Jhonson JA, Cristie MJ, Sandler MP. Detection of occultinfection following total joint arthroplasty using sequentialtechnecium-99m HDP bone scintigraphy and indium-11 WBC
imaging. J Nucl Med 1988;29:1347-53.8
1. Buchholz HW, Elson RA, Engelbrecht E. Management ofdeep infection of total hip replacement. J Bone Joint Surg Br1981;63:342-53.
2. Cheung A, Lachiewicz PF, Renner JB. The role of aspirationand contrast-enhanced arthrography in evaluating the unce-mented hip arthroplasty. AJR 1997;168:1305-9.
3. Tigges S, Stiles RG, Meli RJ, et al. Hip aspiration: acost-effective and accurate method of evaluating the poten-tially infected hip prosthesis. Radiology 1993;189:485-8.
4. Gould ES, Potter Hg, Bober SE. Role of routine percutaneouship aspirations prior to prosthesis revision. Skeletal Radiol1990;19:427-30.
5. Lachiewicz PF, Rogers GD, Thomason HC. Aspiration of thehip joint before revision total hip arthroplasty. J Bone JointSurg 1996;78-A:749-54.
6. Hasan S, Smith JW. Septic arthritis. Curr Treatment OptionsInfect Dis 2001;3:279-86.
7. Barrellier MT, Bosson JL, Vignon C, et al. Dépistage desthromboses veineuses profondes des membres inférieurs parécho-doppler en chirurgie orthopédique et traumatologique.Rev Chir Orthop Reparatrice Appar Mot 1994;80:711-9.
8. Macdonald PS, Kahn SR, Miller N, et al. Short-term naturalhistory of isolated gastrocnemius and soleal vein thrombosis.J Vasc Surg 2003;37:523-7.
9. Bureau NJ, Ali SS, Orth D, et al. Ultrasound of musculoskel-etal infections. Semin Musculoskel Radiol 1998;2:299-306.
0. Chau CLF, Griffith JF. Musculoskeletal infections: ultrasoundappearances. Clin Radiol 2005;60:149-59.
1. Breidahl WH, Newman JS, Taljanovic MS, et al. PowerDoppler sonography in the assessment of musculoskeletalfluid collections. AJR 1996;166:1443-6.
2. Birtles DB, Rayson MP, Casey A, et al. Venous obstruction inhealthy limbs: a model for chronic compartment syndrome?Med Sci Sports Exerc 2003;35:1638-44.
3. Lund PJ, Nisbet JK, Valencia FG, et al. Current sonographicapplications in orthopedics. AJR 1996;166:889-95.
4. Shetty M, Fessell DP, Femino JE, et al. Sonography of ankletendon impingement with surgical correlation. AJR 2002;179:949-53.
5. Cyteval C, Sarrabère MP, Cottin A, et al. Iliopsoas impinge-ment on the acetabular component: radiologic and computedtomography findings of rare hip prosthesis complications ineight cases. J Comput Assist Tomogr 2003;27:183-8.
6. Rezig R, Copercini M, Montet X, et al. Ultrasound diagnosisof anterior iliopsoas impingement in total hip replacement.Skeletal Radiol 2004;33:112-6.
7. Westhoff B, Wild A, Werner A, et al. The value of ultrasoundafter shoulder arthroplasty. Skeletal Radiol 2002;31:695-701.
8. Berquist TH, Bender CE, Maus TP, et al. Pseudobursae: auseful finding in patients with painful hip arthroplasty. AJR1987;148:103-6.
9. Goiz TH, Goiz RJ. Watson orthopedic implants: a guide toradiographic analysis. Curr Probl Diagn Radiol 1996;4:114-68.
0. Bernat Z, Carles AE, Goken E. Patterns of osteolysis aroundtotal hip components inserted with and without cement.J Bone Joint Surg 1995;3:432-8.
1. Craig JG, Jacobson JA, Moed BR. Ultrasound of fracture and
bone healing. Radiol Clin North Am 1999;37:737-51.Curr Probl Diagn Radiol, May/June 2006

4
4
4
4
C
2. Bottinell O, Calliada F, Campani R. Bone callus: possibleassessment with color Doppler ultrasonography. Normal bonehealing process. Radiol Med 1996;91:537-41.
3. Caruso G, Lagalla R, Derchi L, et al. Monitoring of fracturecalluses with color Doppler sonography. J Clin Ultrasound
2000;28:20-7.urr Probl Diagn Radiol, May/June 2006
4. Moed BR, Subramanian S, Van Holsbeeck M, et al. Ultra-sound for the early diagnosis of tibial fracture healing afterstatic interlocked nailing without reaming clinical results.J Orthop Trauma 1998;12:206-16.
5. Marsh D. Concepts of fracture union, delayed union, and
nonunion. Clin Orthop 1998;355S:S22-30.89