c c ? ? e e d d causal diagrams -- dags dags = directed acyclic graphs; aka chain graphs consist of...
TRANSCRIPT

CC??
EE
DD
Causal Diagrams -- DAGsCausal Diagrams -- DAGs• DAGs = directed acyclic graphs; aka chain graphs• Consist of nodes (variables) and arrows• “Directed”: all arrows have one-way direction and depict causal
relationships• “Acyclic”: there is never a complete circle (i.e. no factor can
cause itself)• Better than the rough criteria for confounding when planning
studies and analyses
• Identifies pitfalls of adjusting and not adjusting for certain variables
• Frontier of epidemiologic theory
Research Question: Does E cause D?
Research Question: Does E cause D?
• Forces investigator to conceptualize system

Birth DefectsBirth
Defects
Folate Intake
Folate Intake
StillbirthsStillbirths ??
RQ: Does lack of folate intake cause birth defects?
RQ: Does lack of folate intake cause birth defects?
Use of DAGs to Identify What is Not Confounding
Stillbirths are a “common effect” of both the exposure and disease – not a common cause.
Common effects are called “colliders”
Adjusting for colliders OPENS paths. Will actually result in bias. It is harmful.
Stillbirths are a “common effect” of both the exposure and disease – not a common cause.
Common effects are called “colliders”
Adjusting for colliders OPENS paths. Will actually result in bias. It is harmful.
Hernan AJE 2002Hernan AJE 2002

DAGs point out special issue when estimating direct effects
• RQ: Does aspirin prevent CHD in a pathway other than through platelet aggregation– Assumes no common cause of platelet agg. and D
Would be correct to adjust
But if– Assume common cause (e.g., genetic component)
– Need other statistical methods to resolve
AspirinAspirin
Coronary Heart Disease
Coronary Heart Disease
Platelet Aggregation
Platelet Aggregation ??
AspirinAspirin
Coronary Heart Disease
Coronary Heart Disease
Platelet Aggregation
Platelet Aggregation ??
Genetic factors (not measured)
Genetic factors (not measured)
Would be incorrect to
adjust OR not to adjust for
platelet aggregation
Would be incorrect to
adjust OR not to adjust for
platelet aggregation
Cole and Hernan IJE 2002Cole and Hernan IJE 2002

Confounding and Interaction: Part III
• Methods to reduce confounding– during study design:
• Randomization• Restriction• Matching
– during study analysis:• Stratified analysis
– Forming “Adjusted” Summary Estimates– Concept of weighted average
» Woolf’s Method» Mantel-Haenszel Method
– Handling more than one potential confounder– Role of an analysis plan
• Another design technique: Instrumental variables
• Quantitative assessment of unmeasured confounding
• Limitations of stratification
– motivation for multivariable regression
• Limitations of conventional adjustment
– motivation for other “causal” techniques

Effect-Measure Modification
DelayedNot
DelayedSmoking 15 61No Smoking 47 528
Stratified
Delayed Not DelayedSmoking 26 133No Smoking 64 601
Crude
No Caffeine Use
Heavy Caffeine Use
RR crude = 1.7
RRno caffeine use = 2.4
DelayedNot
DelayedSmoking 11 72No Smoking 17 73
RRcaffeine use = 0.7
. cs delayed smoking, by(caffeine) caffeine | RR [95% Conf. Interval] M-H Weight-----------------+------------------------------------------------- no caffeine | 2.414614 1.42165 4.10112 5.486943 heavy caffeine | .70163 .3493615 1.409099 8.156069 -----------------+------------------------------------------------- Crude | 1.699096 1.114485 2.590369 M-H combined | 1.390557 .9246598 2.091201-----------------+-------------------------------------------------Test of homogeneity (M-H) chi2(1) = 7.866 Pr>chi2 = 0.0050
Report interaction; confounding is not relevant
Association Between Smoking and Delayed Conception by Amount of Caffeine Use
Caffeine Use Risk Ratio 95% CI None 2.4* 1.4 to 4.1 Heavy 0.7* 0.35 to 1.4
* test of homogeneity, p = 0.005

Report vs Ignore Effect-Measure Modification?Some Guidelines
Risk Ratios for a Given Exposure and Disease
Potential Effect Modifier Present Absent
P value for heterogeneity
Report or Ignore
Interaction
2.3 2.6 0.45 Ignore
2.3 2.6 0.001 Ignore
2.0 20.0 0.001 Report
2.0 20.0 0.10 Report
2.0 20.0 0.40 Ignore
3.0 4.5 0.30 Ignore
3.0 4.5 0.001 +/-
0.5 3.0 0.001 Report
0.5 3.0 0.20 +/-
Is an art form: requires consideration of clinical, statistical and practical considerations

Does AZT after needlesticks prevent HIV?
HIVNo
HIVAZT 8 40No AZT 16 28
24 68 92
Minor Severity
Major Severity
Crude
Stratified
HIV No HIVAZT 8 131No AZT 19 189
27 320 347
HIVNo
HIVAZT 0 91No AZT 3 161
3 252 255
ORcrude =0.61
OR = 0.0 OR = 0.35
Report or ignore interaction?. cc HIV AZTuse,by(severity)
severity | OR [95% Conf. Interval] M-H Weight-----------------+------------------------------------------------- minor | 0 0 2.302373 1.070588 major | .35 .1344565 .9144599 6.956522-----------------+-------------------------------------------------
Test of homogeneity (B-D) chi2(1) = 0.60 Pr>chi2 = 0.4400

General Framework for Stratification
• Design phase: Create a DAG– Decide which variables to control for
• Implementation phase: measure the confounders (or other variables needed to block path)
• Analysis phase:
Report Effect-Measure Modification? (assess clinical, statistical, and practical considerations)
yesno
Derive summary “adjusted” estimate
Report stratum-specific estimates
Report crude estimate, 95% CI, p value
Decide which variables to adjust for in final estimate
none someReport adjusted estimate, 95% CI, p value

Assuming Interaction is not Present, Form a Summary of the Unconfounded
Stratum-Specific Estimates
• Construct a weighted average– Assign weights to the individual strata– Summary Adjusted Estimate = Weighted
Average of the stratum-specific estimates
– a simple mean is a weighted average where the weights are equal to 1
– which weights to use depends on type of effect estimate desired (OR, RR, RD), characteristics of the data, and goal of research
– e.g., • Woolf’s method• Mantel-Haenszel method• Standardization (see text)
ii
ii
w
istratuminestimateeffectw )] ([
5)1)(4(
)8(1)6(1)4(1)2(1mean simple

Forming a Summary Adjusted Estimate for Stratified Data
Minor Severity
Major Severity
Crude
Stratified
HIV No HIVAZT 8 131No AZT 19 189
27 320 347
HIVNo
HIVAZT 0 91No AZT 3 161
3 252 255
ORcrude = 0.61
OR = 0.0
HIVNo
HIVAZT 8 40No AZT 16 28
24 68 92
OR = 0.35
How would you weight these strata?

Summary Estimators: Woolf’s Method
• aka Directly pooled or precision estimator• Woolf’s estimate for adjusted odds ratio
– where wi
– wi is the inverse of the variance of the stratum-specific log(odds ratio)
idicibia1111
1
i
i
i
ii
Woolfw
w )]OR (log[
OR log
)(OR logOR WoolfWoolf e
Disease No DiseaseExposed ai bi
Unexposed ci di

Calculating a Summary Effect Using the Woolf Estimator
• e.g., AZT use, severity of needlestick, and HIV
Minor Severity
Major Severity
Crude
Stratified
HIV No HIVAZT 8 131No AZT 19 189
27 320
HIVNo
HIVAZT 0 91No AZT 3 161
3 252 255
ORcrude =0.61
OR = 0.0
HIVNo
HIVAZT 8 40No AZT 16 28
24 68 92
OR = 0.35
281
161
401
81
1
1611
31
911
01
1
)]0.35 log(
281
161
401
81
1[)]0 log(
1611
31
911
01
1[
WoolfOR log
Problem: cannot take log of 0; cannot divide by zero

Summary Adjusted Estimator: Woolf’s Method
• Conceptually straightforward
• Best when:– number of strata is small– sample size within each strata is large
• Cannot be calculated when any cell in any stratum is zero because log(0) is undefined– 1/2 cell corrections have been suggested but
are subject to bias
• Formulae for Woolf’s summary estimates for other measures (e.g., risk ratio, RD) available in texts and software documentation

Summary Adjusted Estimators: Mantel-Haenszel
• Mantel-Haenszel estimate for odds ratios
– ORMH =
– wi =
– wi is inverse of the variance of the stratum-specific odds ratio under the null hypothesis (OR =1)
i
ii
N
cb
i
ii
i
ii
Ncb
Nda
i
ii
i
i
i
i
i
ii
Ncb
dbca
Ncb
*
Disease No DiseaseExposed ai bi
Unexposed ci di
ai+ bi + ci + di = Ni

Summary Adjusted Estimator: Mantel-Haenszel
• Relatively resistant to the effects of large numbers of strata with few observations
• Resistant to cells with a value of “0”
• Computationally easy
• Most commonly used in commercial software

Calculating a Summary Adjusted Effect Using the Mantel-Haenszel Estimator
• ORMH =
• ORMH =
Minor Severity
Major Severity
Crude
Stratified
HIV No HIVAZT 8 131No AZT 19 189
27 320
HIVNo
HIVAZT 0 91No AZT 3 161
3 252 255
ORcrude =0.61
OR = 0.0
HIVNo
HIVAZT 8 40No AZT 16 28
24 68 92
OR = 0.35
i
ii
ii
ii
i
ii
N
cbcb
da
N
cb*
i
ii
i
ii
Ncb
Nda
30.0
921640
255391
92288
2551610

Calculating a Summary Effect in Stata
• To stratify by a third variable:
– cs varcase varexposed, by(varthird variable)
– cc varcase varexposed, by(varthird variable)
• Default summary estimator is Mantel-Haenszel– “ , pool” will also produce Woolf’s method
epitab command - Tables for epidemiologists

Calculating a Summary Effect Using the Mantel-Haenszel Estimator
• e.g. AZT use, severity of needlestick, and HIV
• . cc HIV AZTuse,by(severity) pool• severity | OR [95% Conf. Interval] M-H Weight• -----------------+-------------------------------------------------• minor | 0 0 2.302373 1.070588 • major | .35 .1344565 .9144599 6.956522 • -----------------+-------------------------------------------------• Crude | .6074729 .2638181 1.401432 • Pooled (direct) | . . .• M-H combined | .30332 .1158571 .7941072 • -----------------+-------------------------------------------------• Test of homogeneity (B-D) chi2(1) = 0.60 Pr>chi2 = 0.4400• Test that combined OR = 1:• Mantel-Haenszel chi2(1) = 6.06• Pr>chi2 = 0.0138
Minor Severity
Major Severity
Crude
Stratified
HIV No HIVAZT 8 131No AZT 19 189
27 320
HIVNo
HIVAZT 0 91No AZT 3 161
3 252 255
ORcrude =0.61
OR = 0.0
HIVNo
HIVAZT 8 40No AZT 16 28
24 68 92
OR = 0.35

Calculating a Summary Effect Using the Mantel-Haenszel Estimator
• In addition to the odds ratio, Mantel-Haenszel estimators are also available in Stata for:
– risk ratio
• “cs varcase varexposed, by(varthird variable)”
– rate ratio
• “ir varcase varexposed vartime, by(varthird variable)”

After Confounding is Managed: Confidence Interval Estimation and Hypothesis Testing for the Mantel-
Haenszel Estimator
• e.g. AZT use, severity of needlestick, and HIV
• . cc HIV AZTuse,by(severity) pool• severity | OR [95% Conf. Interval] M-H Weight• -----------------+-------------------------------------------------• minor | 0 0 2.302373 1.070588 • major | .35 .1344565 .9144599 6.956522 • -----------------+-------------------------------------------------• Crude | .6074729 .2638181 1.401432 • Pooled (direct) | . . .
M-H combined | .30332 .1158571 .7941072
• -----------------+-------------------------------------------------• Test of homogeneity (B-D) chi2(1) = 0.60 Pr>chi2 = 0.4400
• Test that combined OR = 1:• Mantel-Haenszel chi2(1) = 6.06• Pr>chi2 = 0.0138
• What does the p value = 0.0138 mean?

Mantel-Haenszel Confidence Interval and Hypothesis Testing
stratumeach in cell a
for the valueexpected theis E
)1(
5.0
eCI %95
;;;
)(2
)(
))((2
)(
)(2
)(
OR) (logSE
i
12
2121
2
1 121
)MH
OR SE(log x (1.96 MH
OR log
1
2
1
1 1
1
1
2
1
where
NN
mmnn
Ea
N
cbw
N
daR
N
cbQ
N
daP
where
w
wQ
wR
RQwP
R
RP
k
i ii
iiii
k
i
k
iii
i
iii
i
iii
i
iii
i
iii
k
ii
k
iii
k
i
k
iii
k
iiiii
k
ii
k
iii
Disease No DiseaseExposed ai bi m1i
Unexposed ci di m2i
n1i n2i Ni

Mantel-Haenszel Techniques
• Mantel-Haenszel estimators• Mantel-Haenszel chi-square statistic• Mantel’s test for trend (dose-response)

Spermicides, maternal age & Down Syndrome
•
Down No Down Spermicide use 4 109 No spermicide use 12 1145
Down No Down
Spermici use 3 104 No spermic. 9 1059 1175
Age < 35 Age > 35
Crude
Stratified Down No
Down
Spermic. use 1 5 No spermic. 3 86 95
OR = 3.4 OR = 5.7
OR = 3.5
. cc downs spermici , by(matage) pool
matage | OR [95% Conf. Interval] M-H Weight-----------------+------------------------------------------------- < 35 | 3.394231 .9800358 11.80389 .7965957 >= 35 | 5.733333 0 50.8076 .1578947-----------------+------------------------------------------------- Crude | 3.501529 1.171223 10.49699 Pooled (direct) | 3.824166 1.196437 12.22316 M-H combined | 3.781172 1.18734 12.04142-----------------+-------------------------------------------------Test for heterogeneity (direct) chi2(1) = 0.137 Pr>chi2 = 0.7109Test for heterogeneity (M-H) chi2(1) = 0.138 Pr>chi2 = 0.7105
Test that combined OR = 1: Mantel-Haenszel chi2(1) = 5.81 Pr>chi2 = 0.0159
Which answer should you report as “final”?
What undesired feature has stratification caused?

Effect of Adjustment on Precision (Variance)
• Adjustment can increase or decrease standard errors (and CI’s) depending upon:– Nature of outcome (interval scale vs. binary)– Measure of association desired– Method of adjustment (Woolf vs M-H vs MLE)– Strength of association between potential
confounding factor and exposure/disease
• Complex and difficult to memorize
• Good news: adjustment for strong confounders removes bias and often improves precision
• Bad news: adjustment for less-than-strong confounders can often (but not always) worsen precision
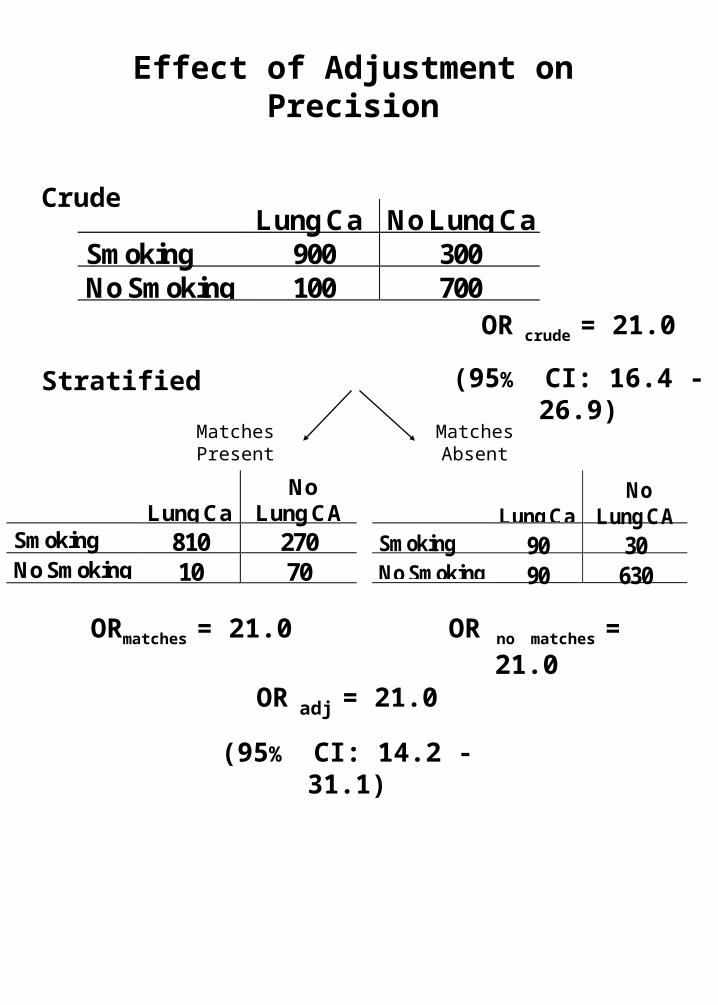
Effect of Adjustment on Precision
Lung Ca No Lung CaSmoking 900 300No Smoking 100 700
Lung CaNo
Lung CASmoking 810 270No Smoking 10 70
Stratified
Crude
Matches Absent
Matches Present
Lung CaNo
Lung CASmoking 90 30No Smoking 90 630
OR crude = 21.0
(95% CI: 16.4 - 26.9)
ORmatches = 21.0 OR no matches = 21.0
OR adj = 21.0
(95% CI: 14.2 - 31.1)

Whether or not to accept the “adjusted” summary estimate instead
of the crude?• Methodologic literature is inconsistent on this
– Bias-variance tradeoff
• Scientifically most rigorous approach is to:– Create the DAG and identify potential confounders– Prior to adjustment, create two lists of potential
confounders• “A” List: Those factors for which you will accept
the adjusted result no matter how small the difference from the crude.
– Factors strongly believed to be confounders
• “B” List: Those factors for which you will accept the adjusted result only if it meaningfully differs from the crude (with some pre-specified difference, e.g., 5 to 10%).
– “Change-in-estimate” approach– Factors you are less sure about
• For some analyses, may have no factors on A list. For other analyses, no factors on B list.
• Always putting all factors on A list may seem conservative, but not necessarily the right thing to do in light of penalty of statistical imprecision
Bias control paramount
Need for tradeoffs

Choosing the crude or adjusted estimate?
• Assume all factors are on B list and a 10% change-in-estimate rule is in place
Risk Ratios Crude Third
Factor Present
Third Factor Absent
Adjusted
Crude or Adjusted?
4.1 1.9 2.1 2.0 Adjusted
4.0 1.2 1.0 1.1 Adjusted
0.2 0.7 0.9 0.8 Adjusted
4.0 3.8 4.2 4.1 Crude
4.0 8.2 7.7 7.9 Adjusted
1.0 3.1 2.7 3.0 Adjusted
1.9 1.6 1.9 1.8 Crude
0.9 0.1 0.2 0.1 Adjusted
4.0 0.4 0.6 0.5 Adjusted

No Role for Statistical Testing for Confounding
• Testing for statistically significant differences between crude and adjusted measures is inappropriate
– e.g., examining an association for which a factor is a known confounder (say age in the association between hypertension and CAD)
– if the study has a small sample size, even large differences between crude and adjusted measures may not be statistically different
• yet, we know confounding is present• therefore, the difference between crude and adjusted
measures cannot be ignored as merely chance. • bias must be prevented and hence adjusted estimate
is preferred• we must live with whatever effects we see after
adjustment for a factor for which there is a strong a priori belief about confounding
– the issue of confounding is one of bias, not of sampling error.
• Other than in RCTs, we’re not concerned that sampling error is causing confounding and therefore we don’t have to worry about testing for role of chance

Spermicides, maternal age & Down Syndrome
•
Down No Down Spermicide use 4 109 No spermicide use 12 1145
Down No Down
Spermici use 3 104 No spermic. 9 1059 1175
Age < 35 Age > 35
Crude
Stratified Down No
Down
Spermic. use 1 5 No spermic. 3 86 95
OR = 3.4 OR = 5.7
OR = 3.5
. cc downs spermici , by(matage) pool
matage | OR [95% Conf. Interval] M-H Weight-----------------+------------------------------------------------- < 35 | 3.394231 .9800358 11.80389 .7965957 >= 35 | 5.733333 0 50.8076 .1578947-----------------+------------------------------------------------- Crude | 3.501529 1.171223 10.49699 Pooled (direct) | 3.824166 1.196437 12.22316 M-H combined | 3.781172 1.18734 12.04142-----------------+-------------------------------------------------Test for heterogeneity (direct) chi2(1) = 0.137 Pr>chi2 = 0.7109Test for heterogeneity (M-H) chi2(1) = 0.138 Pr>chi2 = 0.7105
Test that combined OR = 1: Mantel-Haenszel chi2(1) = 5.81 Pr>chi2 = 0.0159
Which answer should you report as “final”?

Stratifying by Multiple Potential Confounders
Crude
Stratified
<40 smokers
>60 non-smokers40-60 non-smokers
CAD NoCAD
Chlamydia
NoChlamydia
<40 non-smokers
40-60 smokers >60 smokers
CAD No CADChlamydiaNo chlamydia
CAD NoCAD
Chlamydia
NoChlamydia
CAD NoCAD
Chlamydia
NoChlamydia
CAD NoCAD
Chlamydia
NoChlamydia
CAD NoCAD
Chlamydia
NoChlamydia
CAD NoCAD
Chlamydia
NoChlamydia

The Need for Evaluation of Joint Confounding
• Variables that evaluated alone show no confounding may show confounding when evaluated jointly
Crude
Stratified by Factor 1 alone
by Factor 2 alone
by Factor 1 & 2
Disease No DiseaseExposed 12 4Unexposed 30 22
OR = 2.2
F1 +Disease
NoDisease
Exposed 6 2Unexposed 15 11
OR = 2.2
F1+F2+Disease
NoDisease
Exposed 1 1Unexposed 10 10
OR = 1.0
F1-F2+Disease
NoDisease
Exposed 5 1Unexposed 5 1
OR = 1.0
F1+F2-Disease
NoDisease
Exposed 5 1Unexposed 5 1
OR = 1.0
F1-F2-Disease
NoDisease
Exposed 1 1Unexposed 10 10
OR = 1.0
F1 -Disease
NoDisease
Exposed 6 2Unexposed 15 11
OR = 2.2
F2 +Disease
NoDisease
Exposed 6 2Unexposed 15 11
OR = 2.2
F2 -Disease
NoDisease
Exposed 6 2Unexposed 15 11
OR = 2.2

Murray et al. Population Health Metrics 2003
WHO Causal Model of Coronary Heart Disease

Approaches for When More than One Potential Confounder is Present
• Backward vs forward variable selection strategies
– relevant both for stratification and multivariable regression modeling (“model selection”)
• Backwards Strategy
– initially evaluate all potential confounders together (i.e., look for joint confounding)
– preferred because in nature variables act together
– Procedure:
• with all potential confounders considered, form adjusted estimate. This is the “gold standard”
• Of variables on the B list, one variable can then be dropped and the adjusted estimate is re-calculated (adjusted for remaining variables)
• if the dropping of the first variable results in a non-meaningful (eg < 5 or 10%) change compared to the gold standard, it can be eliminated
• continue until no more variables can be dropped (i.e. all remaining variables are relevant)
– Problem:
• With many potential confounders and multiple stratified analyses, p values (too small) & confidence intervals (too narrow) lose their nominal interpretation
– Active area of methodologic interpretation
• With many potential confounders, cells become very sparse and many strata provide no information
Approaches for When More than One Potential Confounder is Present
• Forward Strategy– start with the variable that has the biggest
“change-in-estimate” impact when evaluated individually
– then add the variable with the second biggest impact
– keep this variable if its presence meaningfully changes the adjusted estimate
– procedure continues until no other added variable has an important impact
– Advantage:• avoids the initial sparse cell problem of
backwards approach
– Problem:• does not evaluate joint confounding effects
of many variables • Multiple analyses again lead to problems in
interpreting p values and CI’s

An Analysis Plan
• Available methods often arbitrary and invite fishing for desired answers
• Solution: Analysis plan
• Written before the data are analyzed
• Content– Detailed description of the techniques to be used to
analyze data, step by step– Forms the basis of “Statistical Analysis” section in
manuscripts– Parameters/rules/logic to guide key decisions:
• which variables will be assessed for interaction and for adjustment?
• what p value will be used to guide reporting of interaction?
• what is a meaningful change-in-estimate threshold between two estimates (e.g., 10%) to determine model selection?
• Utility: A plan helps to keep the analysis:– Focused– Transparent– Reproducible– Honest (avoids p value shopping)

Instrumental Variables to Manage Confounding
C1C1 ??
EE
DD
Unmeasured C
Unmeasured C
Instrumental variable (IV)
Instrumental variable (IV)
C2C2
IV must be related to E but nothing else
IV must be related to E but nothing else
Assess association between IV and D to estimate E-D relationship
Assess association between IV and D to estimate E-D relationship
??Length of stayLength of stay
Neonatal outcomes
Neonatal outcomes
Unmeasured C
Unmeasured C
Hour of birthHour of birth
Prenatal complications
Prenatal complications
Malkin et al. Heath Serv. Res., 2000
RQ: Does length of stay determine neonatal outcomes?
RQ: Does length of stay determine neonatal outcomes?

Residual Confounding
Four Mechanisms• Categorization of confounder too broad
– e.g., Association between natural menopause and prevalent CHD
Szklo and Nieto, 2007
Method of age adjustment OR 95% CI Crude 4.54 2.67-7.85 2 categories: 45-54, 55-64 3.35 1.60-6.01 4 categories: 45-49, 50-54, 55-59, and 60-64
3.04 1.37-6.11
Continuous variable 2.47 1.31-4.63
• Misclassification of confounders – Can be differential or non-differential
with respect to exposure and disease– If non-differential, will lead to adjusted
estimates somewhere in between crude and true adjusted
– If differential, can lead to a variety of unpredictable directions of bias

Residual Confounding
Mechanisms – cont’d
• Variable used for adjustment is imperfect surrogate for true confounder
CRP level
CRP level ??
Periodontal disease
Periodontal disease
CADCAD
Inflammatory
Predisposition
Inflammatory
Predisposition
• Unmeasured confounders
AgeAge??
E E
DD
Unmeasured C
Unmeasured C

Quantitative Analysis of Unmeasured Confounding
• Can back calculate to determine how a confounder would need to act in order to spuriously cause any apparent odds ratio. Example: OR= 2.0
Prevalence of “high” level of unmeasured confounder
Association between unmeasured confounder and disease (risk ratio)
Ass
ocia
tion
betw
een
unm
easu
red
conf
ound
er a
nd
expo
sure
(pr
eval
ence
rat
io)
A (low prevalence scenario) = 7 B (high prevalence scenario) = 3.4
Winkelstein et al., AJE 1984

Stratification to Manage Confounding
• Advantages– straightforward to implement and comprehend– easy way to evaluate interaction
• Limitations– Requires continuous variables to be discretized
• loses information; possibly results in “residual confounding”
• Discretizing often brings less precision– Deteriorates with multiple confounders
• e.g., suppose 4 confounders with 3 levels– 3x3x3x3=81 strata needed– unless huge sample, many cells have “0”’s
and strata have undefined effect measures– Solution:
• Mathematical modeling (multivariable regression)– e.g.
» linear regression» logistic regression» proportional hazards regression

Limitation of Conventional Stratification (and Regression)
• RQ: Does coffee use cause CAD?
??
CoffeeCoffee
CADCAD
Cholesterol level
Cholesterol level
Behavioral factors (unmeasured)
Behavioral factors (unmeasured)
• RQ: Does HAART prevent AIDS/Death?
Simultaneous desire to control for cholesterol/CD4 to manage confounding and NOT to control because they are intermediary variables
AIDSAIDS
HAART HAART
CD4 countCD4 count
Severity of HIV (unmeasured)
Severity of HIV (unmeasured)
??

When factors are simultaneously confounders and intermediaries, conventional techniques fail and
“causal methods” are needed
Causal methods: g-estimation, structural nested models, marginal structural models
Cole et al, AJE 2003

Regression is ahead but don’t forget about the simple
techniques …..• “Because of the increased ease and availability of
computer software, the last few years have seen a flourishing of the use of multivariate analysis in the biomedical literature. These highly sophisticated mathematic models, however, rarely eliminate the need to examine carefully the raw data by means of scatter diagrams, simple n x k table, and stratified analyses.” Szklo and Nieto 2007
• “The widespread availability and user-friendly nature of computer software make the method accessible to some data analysts who may not have had adequate instruction in its appropriate applications. When they are misapplied, multivariate techniques have the potential to contribute to incorrect model development, misleading results, and inappropriate interpretation of the effect of hypothesized confounders.”
Friis and Sellers, 2009• “Statistical software is like raising the gas pedal in a
car for a 4 year old.” Peter Bachetti (UCSF), date unknown

• Next Tuesday (12/9/08) – 8:45 to 10:15: Journal Club
– 1:30 to 3:00 pm: Mitch Katz• “Conceptual approach to
multivariable regression”• Note chapters in his textbook
– 3:15 to 4:45: Last Small Group Section• Web-based course evaluation• Bring laptop
– Distribute Final Exam (on line)• Exam due 12/16 in hands of Olivia by
4 pm by email ([email protected]) or China Basin 5700