burns- modern management
TRANSCRIPT

MODERN
MANAGEMENT
MODERN
MANAGEMENT
M
M
M
C

Dr.B.SELVARAJ,MS;Mch;FICS; Dr.B.SELVARAJ,MS;Mch;FICS;
Pediatric Surgeon
Associate Professor
Melaka Manipal Medical College
Melaka; Malaysia
M
M
M
C

OBJECTIVES You should be able to
• Identify types of Burns and their
causes
• Understand the pathophysiology of
Burn injury
• Describe the principles of managing
a patient with Burns
• Explain proper wound management
techniques for treating Burns and
Burn scars

Definition
“ It is the response the of skin,
mucous membrane and
subcutaneous tissues to the
thermal and few nonthermal
injuries”

Types and Causes • Thermal injury
- Scalds� Spillage of hot liquids
- Flame burns
- Flash burns due to hot gases and
combustible liquids
- Contact burns�contact with hot metals
• Electrical injury
• Chemical injury� acid & alkali
• Cold injury� frostbite
• Ionising radiation
•


Pathophysiology
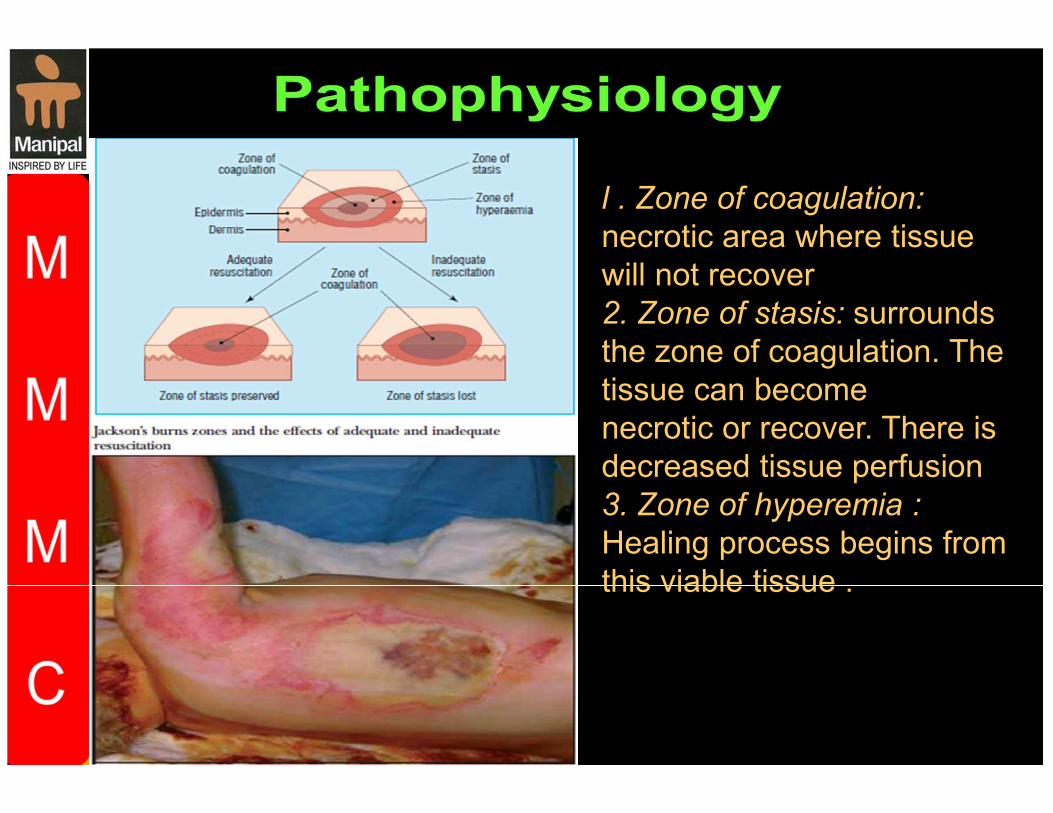
l . Zone of coagulation:
necrotic area where tissue
will not recover
2. Zone of stasis: surrounds
the zone of coagulation. The
tissue can become
necrotic or recover. There is
decreased tissue perfusion
3. Zone of hyperemia :
Healing process begins from
this viable tissue .


History
• Find out the exact mechanism, including
temperature of flame or water,duration of
contact, concentration of chemical, voltage etc
• Record factors suggesting inhalation injury,
e.g. burns in a confined space,flash burns.
• Enquire about other injuries.
• Document first aid given so far.
• Document timings of injury, first aid, and
resuscitation
Estimating depth of burn: • Epidermal: Erythema only.
• Superficial dermal: Pink, wet or blistered,
sensate, blanches and refills.
• Deep dermal: Blotchy red, wet or blistered, no
blanching, insensate.
• Full thickness: White or charred, leathery, no
blanching, insensate

Estimating depth of burn:

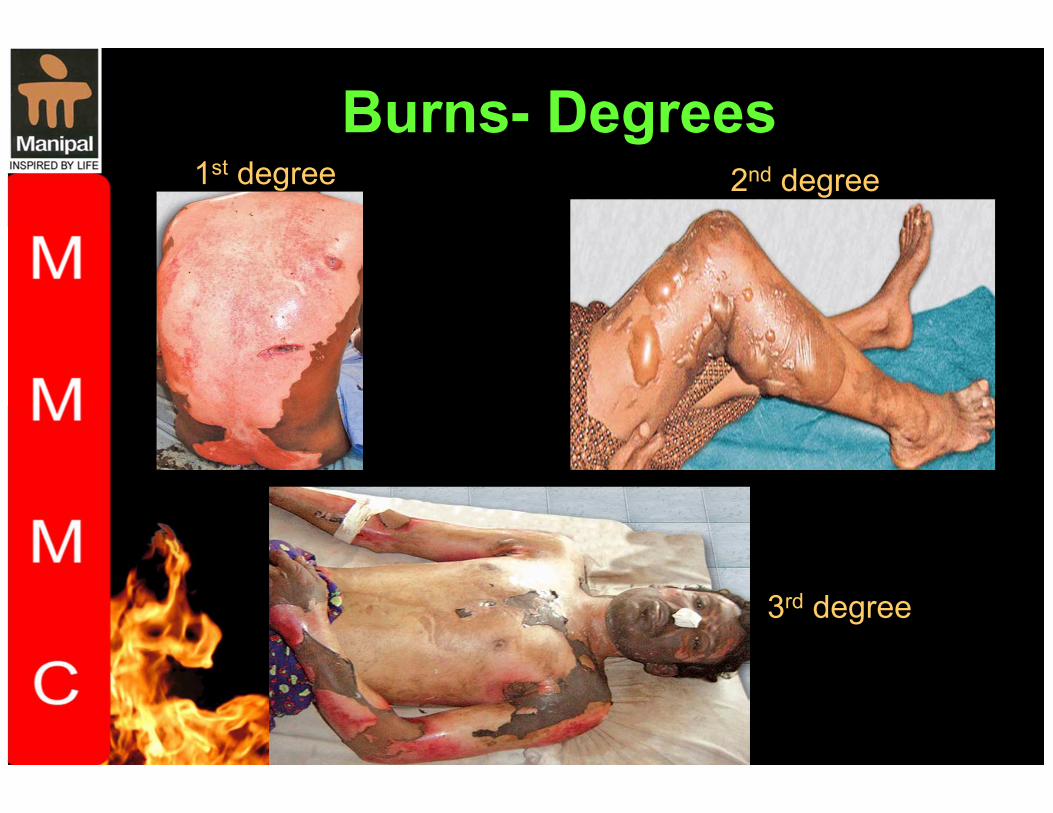
Burns- Degrees 1st degree 2nd degree
3rd degree

Physical Examination
Estimate area of burn(TBSAB) Do not include areas of unblistered erythema.
• Rule of nines
• Rule of palm� Patient’s hand is
approximately 1% total body surface area
(TBSA).
• Lund and Browder chart is the most accurate
method� Fillup the chart

Estimate area of burn(TBSAB)

Signs of inhalation injury • Singed nasal hair.
• Burns to face or oropharynx. Look for
blistered palate.
• Sooty sputum.
• Drowsiness or confusion due to carbon
monoxide inhalation.
• Respiratory effort, breathlessness, stridor,
or hoarseness are signs of impending
airway obstruction and require immediate
intubation

Burns- Initial management
Immediate first aid • Stop the burning process (do not
endanger yourself ).
• Cool the wound. Douse with running
water at 2–15*C for 20min (beware risk of
hypothermia in infants, young children,
and adults with >25% TBSA).

Resuscitation • A. Airway maintenance with C-spine control.
Intubate if suspected
inhalation injury; airway edema can be rapidly
fatal.
• B. Breathing and ventilation.
• C. Circulation with haemorrhage control.
• D. Disability and neurological status.
• E. Exposure and environmental control.
• F. Fluid resuscitation: child, >10% TBSA;
adult, >15% TBSA burned.
• Two large peripheral IV lines, preferably through
unburned skin.
• Send blood for FBC, U&E, clotting, amylase,
carboxyhaemoglobin.
• Give 3–4mL Hartmann’s solution/kg/% TBSA burned.
Half of this is given over the first 8h following injury, half
over the next 16h.
• Children need maintenance fl uid in addition.
• Monitor resuscitation with urinary catheter (aim for
urine output0.5–1mL/kg/h in adults and 1–1.5mL/kg/h in
children).
• Consider ECG, pulse, BP, respiratory rate, pulse
oximetry, ABGs.
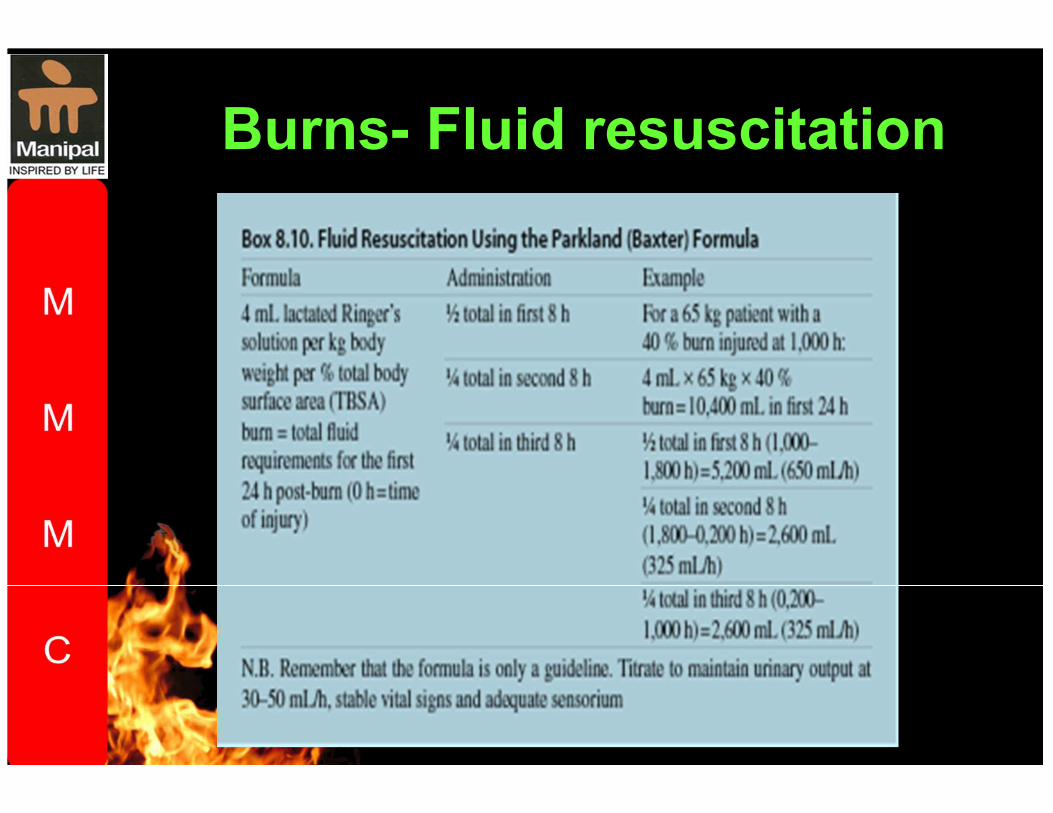
Burns- Fluid resuscitation

Management of burns wound
• Superfi cial dermal burns will heal without
scarring within 2 weeks as long as infection does
not deepen the burn.
• For small burns, outpatient treatment with
simple, non-adherent dressings and twice weekly
wound inspection is sufficient.
• Wash burns with normal saline or chlorhexidine.
• Debride large blisters. Elevate limbs to reduce
pain and swelling.
• Dress hands in plastic bags to allow mobilization

• Topical silver sulphadizine is used on deep burns to reduce risk of infection.
• Escharotomy Performed for circumferential full thickness burns to the chest that limit ventilation or
to the limbs that limit circulation. Patients may also
need fasciotomies.
• Excision and skin grafting Performed for deep dermal or full thickness burns that are too large to
heal rapidly by secondary intention.

Criteria for referral to a burns unit
• >15% TBSA burn in adult; >10% TBSA in child.
• Burns to face, hands, feet, perineum, genitalia,
major joints.
• Full thickness burns >5% TBSA.
• Electrical or chemical burns.
• Associated inhalation injury—always intubate
before transfer.
• Circumferential burns of limbs or chest.
• Burns in very young or old, pregnant women, and
patients with significant comorbidities.
• Any burn associated with major trauma.

Burns- Video podcast
