burnout intervention studies for inpatient elderly care nursing staff: systematic literature review
TRANSCRIPT
Re
BuSy
Claa Unb Ins
International Journal of Nursing Studies 51 (2014) 63–71
A R
Artic
Rece
Rece
Acce
Keyw
Burn
Elde
Inte
Syst
Prev
Turn
Wor
*
Inst
Mar
fax:
a.ko
a.nie
002
http
view
rnout intervention studies for inpatient elderly care nursing staff:stematic literature review
udia Westermann a,*, Agnessa Kozak a, Melanie Harling a, Albert Nienhaus a,b
iversity Clinic Hamburg-Eppendorf, Institute for Health Service Research in Dermatology and Nursing, Germany
titution for Statutory Accident Insurance and Prevention in Healthcare and Welfare Services, Germany
What is already known about the topic?
� Workplace stress is a significant problem for employeesworking in healthcare, particularly among professionssuch as nursing.� Burnout in the nursing profession is associated with the
risk of absenteeism and high staff turnover.� A substantial economic impact can be inferred from this
syndrome.
T I C L E I N F O
le history:
ived 11 July 2012
ived in revised form 23 October 2012
pted 1 December 2012
ords:
out
rly care staff
rvention studies
ematic literature review
ention
over
kload
A B S T R A C T
Background: Staff providing inpatient elderly and geriatric long-term care are exposed to a
large number of factors that can lead to the development of burnout syndrome. Burnout is
associated with an increased risk of absence from work, low work satisfaction, and an
increased intention to leave. Due to the fact that the number of geriatric nursing staff is
already insufficient, research on interventions aimed at reducing work-related stress in
inpatient elderly care is needed.
Objective: The aim of this systematic review was to identify and analyse burnout
intervention studies among nursing staff in the inpatient elderly and geriatric long-term
care sector.
Methods: A systematic search of burnout intervention studies was conducted in the
databases Embase, Medline and PsycNet published from 2000 to January 2012.
Results: We identified 16 intervention studies. Interventions were grouped into work-
directed (n = 2), person-directed (n = 9) and combined approaches (work- and person-
directed, n = 5). Seven out of 16 studies observed a reduction in staff burnout. Among them
are two studies with a work-directed, two with a person-directed and three with a
combined approach. Person-directed interventions reduced burnout in the short term (up
to 1 month), while work-directed interventions and those with a combined approach were
able to reduce burnout over a longer term (from 1 month to more than 1 year). In addition
to staff burnout, three studies observed positive effects relating to the client outcomes.
Only three out of ten Randomised Control Trials (RCT) found that interventions had a
positive effect on staff burnout.
Conclusion: Work-directed and combined interventions are able to achieve beneficial
longer-term effects on staff burnout. Person-directed interventions achieve short-term
results in reducing staff burnout. However, the evidence is limited.
� 2012 Elsevier Ltd. All rights reserved.
Corresponding author at: University Clinic Hamburg-Eppendorf,
itute for Health Service Research in Dermatology and Nursing,
tinistrasse 52, 20246 Hamburg, Germany. Tel.: +49 40 7410 59516;
+49 40 7410 59708.
E-mail addresses: [email protected] (C. Westermann),
[email protected] (A. Kozak), [email protected] (M. Harling),
[email protected] (A. Nienhaus).
Contents lists available at SciVerse ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
0-7489/$ – see front matter � 2012 Elsevier Ltd. All rights reserved.
://dx.doi.org/10.1016/j.ijnurstu.2012.12.001
C. Westermann et al. / International Journal of Nursing Studies 51 (2014) 63–7164
What this paper adds
� Few reviews have been published on the effectiveness ofinterventions in preventing burnout in healthcare work-ers.� This paper identifies intervention studies in the work-
place aimed at preventing burnout for staff in theinpatient elderly care segment.� Limited evidence is available for the effectiveness of
work-, person-directed and combined interventions inreducing staff burnout.� Work-directed and combined intervention programmes
potentially have longer-lasting beneficial effects on staffburnout than person-directed intervention programmes.
1. Introduction
Within an occupational context, the term burnout isused to describe an individual reaction to chronic stress atwork. These reactions are characterised by emotional
exhaustion, a distanced, indifferent, cynical attitudetowards work and other people (depersonalisation) and adecline in personal accomplishment (Maslach et al., 2001).Burnout is a complex syndrome featuring a large numberof unspecific symptoms that can have far-reaching impactson an individual’s health (Von Kanel, 2008). Burnout is alsoassociated with an increased risk of absence from work,more work days lost due to illness, inability to work andlow work satisfaction, and the individuals affected are verylikely to give up work completely (Borritz et al., 2006;Camerino et al., 2006; Edwards et al., 2003). Staff whoprovide inpatient elderly and geriatric long-term care areexposed to a large number of factors that can lead to thedevelopment of burnout syndrome (Gandoy-Crego et al.,2009; Zimber, 1998). They are faced with time pressure,heavy workloads, few opportunities to influence theirwork, confrontation with suffering, dealing with people inneed of long-term care, physical stress, shift work and staffshortages (Gandoy-Crego et al., 2009; Glaser et al., 2008;Jenull et al., 2008; McHugh et al., 2011; Zimber, 1998).Other enabling factors include a lack of support andrecognition among colleagues and from management(Lewis et al., 2010). Factors not relating to work thatmay lead to the development of burnout include anindividual’s personality and social relationships (Gandoy-Crego et al., 2009; Narumoto et al., 2008). One particularchallenge faced by professional nursing staff that maycause burnout is providing care to people with dementia(Haberstroh et al., 2010; Mackenzie and Peragine, 2003;Rodney, 2000). Due to cognitive impairment and psycho-logical changes among clients, as well as the related loss ofability to cope with day-to-day life, this sort of work isintensive and emotionally demanding (Fuchs-Lacelle et al.,2008; Opie et al., 2002; Van Weert et al., 2005; Weyereret al., 2004). As a consequence of demographic changes inwestern societies, the proportion of people with complexdiseases (e.g., dementia) who are in need of intensive long-term care is continually on the rise (Prezewowsky, 2007).In the face of this trend the number of geriatric nursingstaff is already insufficient (Camerino et al., 2006;Mackenzie et al., 2006). Measures must be taken to boost
motivation and improve the health of the staff members(Borritz et al., 2006; Evers et al., 2002). Therefore, researchon interventions aimed at reducing work-related stressamong professional nursing staff is needed.
The aim of this paper is to investigate the currentresearch on burnout intervention studies in the field ofinpatient elderly and geriatric long-term care. The reviewfocuses on the following questions: Which interventionapproaches for burnout in the field of inpatient elderly andgeriatric long-term care have been published since 2000?Are there studies proving that burnout can be influencedby intervention? Which recommendations for futureinterventions can be derived from these studies?
2. Methods
2.1. Search strategy and selection criteria
Systematic literature research was performed using theMedline, Embase and PsycNet databases. This literaturesearch covered the period from January 2000 to January2012 and the languages were limited to German, English,French, Spanish, Portuguese and Italian. The search termsused were ‘‘burnout’’ combined with ‘‘occupation* ANDintervention’’, ‘‘employ* AND intervention’’, ‘‘interventionAND nursing AND geriatric’’, ‘‘intervention AND nursingAND homes’’. Relevant publications were included regard-less of the study design.
Included were primary studies, which analysed inter-vention programmes aimed at preventing burnout fornursing staff in the setting of inpatient elderly and geriatriclong-term care. We only included studies which metho-dically assess the issue of burnout among nursing staff.Studies which examined the effectiveness of burnoutintervention in diverse healthcare occupations, but did notprovide detailed information on the impatient elderly carestaff, where excluded.
Further literature sources were taken from thereference list of articles included and other reviews.Studies that did not meet the inclusion criteria, as well asduplicates were excluded and the reasons for theirexclusion noted. Wherever it was not possible to makea decision on a study’s inclusion or exclusion based on theabstract, the full text of the study was examined. Relevantpublications were assessed by two reviewers workingindependently. A consensus method was used to resolvedisagreements.
2.2. Presentation of intervention approaches and their effects
Marine et al. (2006) make a distinction between twotypes of intervention: work-directed (circumstance-oriented) and person-directed (behavioural). This paperalso refers to a third study approach: combined interven-tions (work- and person-directed). According to Marineet al. (2006) work-directed interventions are carried outwith the aim of changing the working environment, worktasks or working methods. Such interventions involve, forexample, decreasing workload or increasing job control.Person-directed interventions are aimed at teaching staffskills or techniques to lessen the effects of stressors for the
indcinbeh
skilenv
ideusethe
refetheyeayea(20
stanthe
2.3.
incl
levplaeffebe
liho200secstualwimpHowkeyJarlincthethislevobsdieobssecassstuexplevmaform(Ku
3. R
3.1.
incat pEdw
C. Westermann et al. / International Journal of Nursing Studies 51 (2014) 63–71 65
ividual. Such interventions involve, for example, redu-g the effects of stress through relaxation or cognitive-avioural techniques that increase coping skills.
Combined interventions are aimed at teaching personalls and also include measures to change the workironment or improve working methods.Intervention effects that are relevant to burnout werentified. An effect is deemed to exist if the interventiond has a statistically significant positive impact on one of
burnout sub-scales (p < .05).Furthermore, effects on burnout were classified byrence period as being short-term (up to 1 month after
intervention), medium-term (between 1 month and 1r after the intervention) and long-term (more than 1r after the intervention) in line with Marine et al.06).If reported in primary studies, mean values (M) and
dard deviation (SD) as well as p-values were stated in result part.
Quality and criteria for the evidence classification of
uded studies
The main component used in this paper to assess theel of evidence is the study design. The study designys a decisive role in determining the validity of thects observed. The best possible level of evidence canachieved with RCTs. These studies reduce the like-od of systematic design errors (Des Jarlais et al.,4). Often, however, the conditions in the healthcare
tor and a variety of associated issues call for differentdy designs (Kunz et al., 2009). Randomisation cannotays be justified from an ethical perspective or is oftenossible to implement due to organisational factors.ever, non-randomised designs can also contribute
findings to the body of evidence (Gordis, 2000; Desais et al., 2004). The evidence found in the studiesluded is assigned to quality categories in line with
system developed by Kunz et al. (2009). According to system, RCTs are assigned to the highest evidence
el I. Experimental studies without randomisation andervational studies with control groups (cohort stu-s, case control studies) are assigned to level II, whileervational studies without control groups (cross-tional, before and after studies, case series) areigned to level III. Case reports, pathophysiologicaldies or laboratory studies, expert opinions or theert consensus are assigned to the lowest evidence
el – level IV. Limitations affecting the design and thenner in which the intervention measures are per-
ed can potentially influence the quality of the resultsnz et al., 2008).
esults
Search results
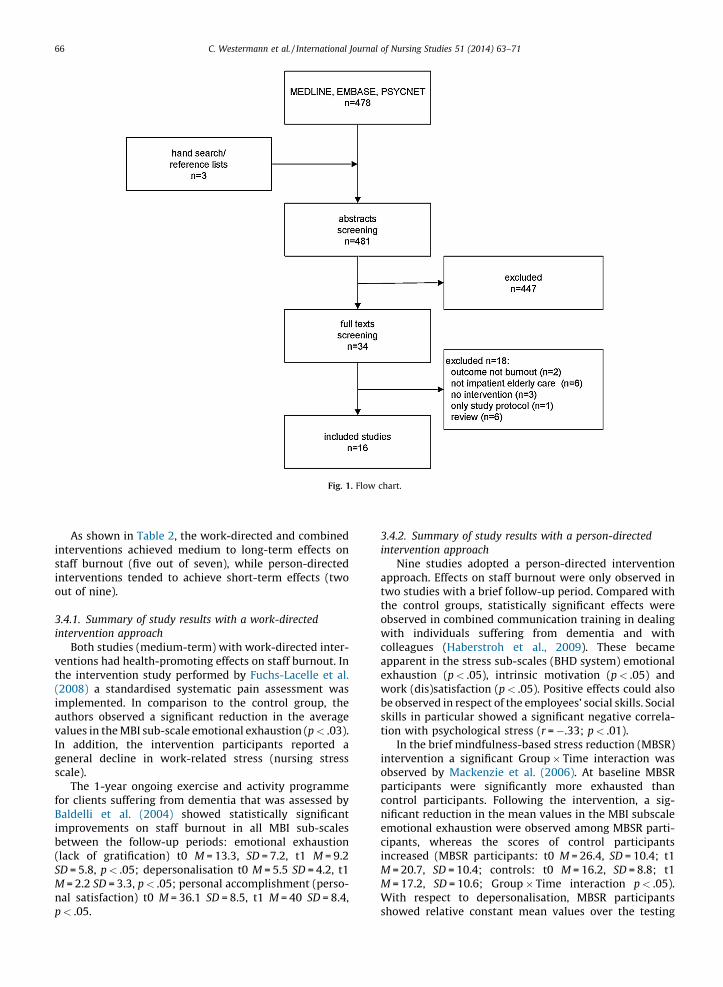
The search query resulted in a total of 478 studies,luding six reviews of intervention programmes aimedreventing stress and burnout at work (Awa et al., 2010;ards et al., 2003; Marine et al., 2006; Mimura and
Griffiths, 2003; Van Wyk and Pillay-Van Wyk, 2010; Vander Klink et al., 2001). Three further relevant studies werefound manually. A total of 16 original studies fulfilled theinclusion criteria and made up the basis of this review(Fig. 1).
Out of the 16 studies included, three studies originatedfrom Australia, Germany and Canada in each case, two eachfrom the US and the Netherlands, and one study each fromDenmark, Italy and the UK. Ten studies have a randomisedcontrolled design, four have a quasi-experimental design,one has a pre-post design and one a longitudinalcomparative design.
3.2. Study population and sample size
In most of the studies (n = 15) the interventions tookplace in psychogeriatric long-term care, with the exceptionof the study by Jensen et al. (2006). Fourteen studies (withexception to Mackenzie et al., 2006) looked specifically atcare for clients with dementia. The sample examinedconsisted of professional nurses working in inpatientelderly and geriatric long-term care. Three studies alsoexamined a small percentage of activity staff members,consenting managers and social workers (Fritsch et al.,2009; Jeon et al., 2012; Richardson et al., 2002). Thenumber of participants varied between 21 and 300.
3.3. Survey instruments used to measure burnout
The most common instrument used to measureburnout was the MBI (n = 14). Three of the studies usedother/additional survey instruments: the stress screeningsystem for human service providers (BHD system) devel-oped by Hacker et al. (1995) and the General HealthQuestionnaire developed by Goldberg and Hillier (GHQ,1979). Because of the different MBI and scales versionsused in the studies, only a limited comparison of the effectswas possible (Table 1).
3.4. Approaches and study period of interventions
Due to the different intervention concepts used in thestudies, we grouped them according to their interventionapproach. As shown in Table 1, the person-directedapproach was the most common type of intervention(n = 9) in this review. Five studies used a combined whiletwo used a work-directed approach.
In seven out of the 16 studies, a significant health-promoting effect was identified. Out of these seven studies,which achieved a statistically significant effect on staffburnout, two applied a person-directed (Haberstroh et al.,2010; Mackenzie et al., 2006), two a work-directed(Baldelli et al., 2004; Fuchs-Lacelle et al., 2008) and threea combined (Jeon et al., 2012; Schrijnemaekers et al., 2003;Van Weert et al., 2005) intervention approach.
The duration of the interventions varied from 4 weeksto 18 months (Table 1). Two studies were conducted over along period of time (up to 18 months of follow-up). Tenstudies stretched the study period between 2 months and 1year. The remaining four studies only observed short timeperiods (up to 1 month after intervention).
C. Westermann et al. / International Journal of Nursing Studies 51 (2014) 63–7166
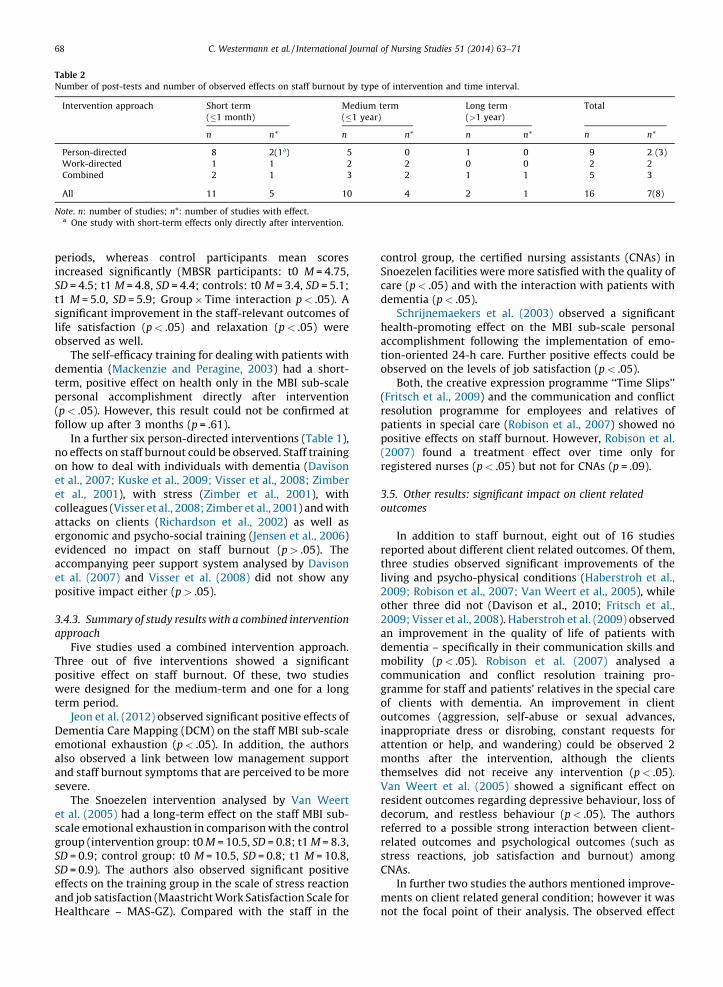
As shown in Table 2, the work-directed and combinedinterventions achieved medium to long-term effects onstaff burnout (five out of seven), while person-directedinterventions tended to achieve short-term effects (twoout of nine).
3.4.1. Summary of study results with a work-directed
intervention approach
Both studies (medium-term) with work-directed inter-ventions had health-promoting effects on staff burnout. Inthe intervention study performed by Fuchs-Lacelle et al.(2008) a standardised systematic pain assessment wasimplemented. In comparison to the control group, theauthors observed a significant reduction in the averagevalues in the MBI sub-scale emotional exhaustion (p < .03).In addition, the intervention participants reported ageneral decline in work-related stress (nursing stressscale).
The 1-year ongoing exercise and activity programmefor clients suffering from dementia that was assessed byBaldelli et al. (2004) showed statistically significantimprovements on staff burnout in all MBI sub-scalesbetween the follow-up periods: emotional exhaustion(lack of gratification) t0 M = 13.3, SD = 7.2, t1 M = 9.2SD = 5.8, p < .05; depersonalisation t0 M = 5.5 SD = 4.2, t1M = 2.2 SD = 3.3, p < .05; personal accomplishment (perso-nal satisfaction) t0 M = 36.1 SD = 8.5, t1 M = 40 SD = 8.4,p < .05.
3.4.2. Summary of study results with a person-directed
intervention approach
Nine studies adopted a person-directed interventionapproach. Effects on staff burnout were only observed intwo studies with a brief follow-up period. Compared withthe control groups, statistically significant effects wereobserved in combined communication training in dealingwith individuals suffering from dementia and withcolleagues (Haberstroh et al., 2009). These becameapparent in the stress sub-scales (BHD system) emotionalexhaustion (p < .05), intrinsic motivation (p < .05) andwork (dis)satisfaction (p < .05). Positive effects could alsobe observed in respect of the employees’ social skills. Socialskills in particular showed a significant negative correla-tion with psychological stress (r = �.33; p < .01).
In the brief mindfulness-based stress reduction (MBSR)intervention a significant Group � Time interaction wasobserved by Mackenzie et al. (2006). At baseline MBSRparticipants were significantly more exhausted thancontrol participants. Following the intervention, a sig-nificant reduction in the mean values in the MBI subscaleemotional exhaustion were observed among MBSR parti-cipants, whereas the scores of control participantsincreased (MBSR participants: t0 M = 26.4, SD = 10.4; t1M = 20.7, SD = 10.4; controls: t0 M = 16.2, SD = 8.8; t1M = 17.2, SD = 10.6; Group � Time interaction p < .05).With respect to depersonalisation, MBSR participantsshowed relative constant mean values over the testing
Fig. 1. Flow chart.
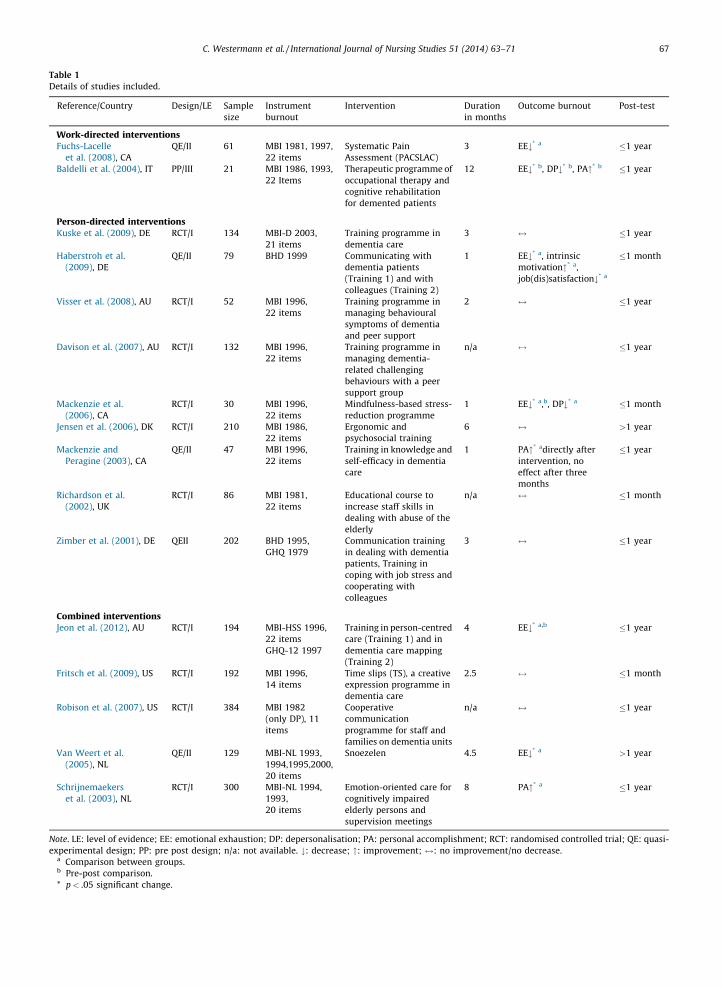
Table 1
Details of studies included.
Reference/Country Design/LE Sample
size
Instrument
burnout
Intervention Duration
in months
Outcome burnout Post-test
Work-directed interventionsFuchs-Lacelle
et al. (2008), CA
QE/II 61 MBI 1981, 1997,
22 items
Systematic Pain
Assessment (PACSLAC)
3 EE#* a �1 year
Baldelli et al. (2004), IT PP/III 21 MBI 1986, 1993,
22 Items
Therapeutic programme of
occupational therapy and
cognitive rehabilitation
for demented patients
12 EE#* b, DP#* b, PA"* b �1 year
Person-directed interventionsKuske et al. (2009), DE RCT/I 134 MBI-D 2003,
21 items
Training programme in
dementia care
3 $ �1 year
Haberstroh et al.
(2009), DE
QE/II 79 BHD 1999 Communicating with
dementia patients
(Training 1) and with
colleagues (Training 2)
1 EE#* a, intrinsic
motivation"* a,
job(dis)satisfaction#* a
�1 month
Visser et al. (2008), AU RCT/I 52 MBI 1996,
22 items
Training programme in
managing behavioural
symptoms of dementia
and peer support
2 $ �1 year
Davison et al. (2007), AU RCT/I 132 MBI 1996,
22 items
Training programme in
managing dementia-
related challenging
behaviours with a peer
support group
n/a $ �1 year
Mackenzie et al.
(2006), CA
RCT/I 30 MBI 1996,
22 items
Mindfulness-based stress-
reduction programme
1 EE#* a,b, DP#* a �1 month
Jensen et al. (2006), DK RCT/I 210 MBI 1986,
22 items
Ergonomic and
psychosocial training
6 $ >1 year
Mackenzie and
Peragine (2003), CA
QE/II 47 MBI 1996,
22 items
Training in knowledge and
self-efficacy in dementia
care
1 PA"* adirectly after
intervention, no
effect after three
months
�1 year
Richardson et al.
(2002), UK
RCT/I 86 MBI 1981,
22 items
Educational course to
increase staff skills in
dealing with abuse of the
elderly
n/a $ �1 month
Zimber et al. (2001), DE QEII 202 BHD 1995,
GHQ 1979
Communication training
in dealing with dementia
patients, Training in
coping with job stress and
cooperating with
colleagues
3 $ �1 year
Combined interventionsJeon et al. (2012), AU RCT/I 194 MBI-HSS 1996,
22 items
GHQ-12 1997
Training in person-centred
care (Training 1) and in
dementia care mapping
(Training 2)
4 EE#* a,b �1 year
Fritsch et al. (2009), US RCT/I 192 MBI 1996,
14 items
Time slips (TS), a creative
expression programme in
dementia care
2.5 $ �1 month
Robison et al. (2007), US RCT/I 384 MBI 1982
(only DP), 11
items
Cooperative
communication
programme for staff and
families on dementia units
n/a $ �1 year
Van Weert et al.
(2005), NL
QE/II 129 MBI-NL 1993,
1994,1995,2000,
20 items
Snoezelen 4.5 EE#* a >1 year
Schrijnemaekers
et al. (2003), NL
RCT/I 300 MBI-NL 1994,
1993,
20 items
Emotion-oriented care for
cognitively impaired
elderly persons and
supervision meetings
8 PA"* a �1 year
Note. LE: level of evidence; EE: emotional exhaustion; DP: depersonalisation; PA: personal accomplishment; RCT: randomised controlled trial; QE: quasi-
experimental design; PP: pre post design; n/a: not available. #: decrease; ": improvement; $: no improvement/no decrease.a Comparison between groups.b Pre-post comparison.
* p < .05 significant change.
C. Westermann et al. / International Journal of Nursing Studies 51 (2014) 63–71 67
C. Westermann et al. / International Journal of Nursing Studies 51 (2014) 63–7168
periods, whereas control participants mean scoresincreased significantly (MBSR participants: t0 M = 4.75,SD = 4.5; t1 M = 4.8, SD = 4.4; controls: t0 M = 3.4, SD = 5.1;t1 M = 5.0, SD = 5.9; Group � Time interaction p < .05). Asignificant improvement in the staff-relevant outcomes oflife satisfaction (p < .05) and relaxation (p < .05) wereobserved as well.
The self-efficacy training for dealing with patients withdementia (Mackenzie and Peragine, 2003) had a short-term, positive effect on health only in the MBI sub-scalepersonal accomplishment directly after intervention(p < .05). However, this result could not be confirmed atfollow up after 3 months (p = .61).
In a further six person-directed interventions (Table 1),no effects on staff burnout could be observed. Staff trainingon how to deal with individuals with dementia (Davisonet al., 2007; Kuske et al., 2009; Visser et al., 2008; Zimberet al., 2001), with stress (Zimber et al., 2001), withcolleagues (Visser et al., 2008; Zimber et al., 2001) and withattacks on clients (Richardson et al., 2002) as well asergonomic and psycho-social training (Jensen et al., 2006)evidenced no impact on staff burnout (p > .05). Theaccompanying peer support system analysed by Davisonet al. (2007) and Visser et al. (2008) did not show anypositive impact either (p > .05).
3.4.3. Summary of study results with a combined intervention
approach
Five studies used a combined intervention approach.Three out of five interventions showed a significantpositive effect on staff burnout. Of these, two studieswere designed for the medium-term and one for a longterm period.
Jeon et al. (2012) observed significant positive effects ofDementia Care Mapping (DCM) on the staff MBI sub-scaleemotional exhaustion (p < .05). In addition, the authorsalso observed a link between low management supportand staff burnout symptoms that are perceived to be moresevere.
The Snoezelen intervention analysed by Van Weertet al. (2005) had a long-term effect on the staff MBI sub-scale emotional exhaustion in comparison with the controlgroup (intervention group: t0 M = 10.5, SD = 0.8; t1 M = 8.3,SD = 0.9; control group: t0 M = 10.5, SD = 0.8; t1 M = 10.8,SD = 0.9). The authors also observed significant positiveeffects on the training group in the scale of stress reactionand job satisfaction (Maastricht Work Satisfaction Scale forHealthcare – MAS-GZ). Compared with the staff in the
control group, the certified nursing assistants (CNAs) inSnoezelen facilities were more satisfied with the quality ofcare (p < .05) and with the interaction with patients withdementia (p < .05).
Schrijnemaekers et al. (2003) observed a significanthealth-promoting effect on the MBI sub-scale personalaccomplishment following the implementation of emo-tion-oriented 24-h care. Further positive effects could beobserved on the levels of job satisfaction (p < .05).
Both, the creative expression programme ‘‘Time Slips’’(Fritsch et al., 2009) and the communication and conflictresolution programme for employees and relatives ofpatients in special care (Robison et al., 2007) showed nopositive effects on staff burnout. However, Robison et al.(2007) found a treatment effect over time only forregistered nurses (p < .05) but not for CNAs (p = .09).
3.5. Other results: significant impact on client related
outcomes
In addition to staff burnout, eight out of 16 studiesreported about different client related outcomes. Of them,three studies observed significant improvements of theliving and psycho-physical conditions (Haberstroh et al.,2009; Robison et al., 2007; Van Weert et al., 2005), whileother three did not (Davison et al., 2010; Fritsch et al.,2009; Visser et al., 2008). Haberstroh et al. (2009) observedan improvement in the quality of life of patients withdementia – specifically in their communication skills andmobility (p < .05). Robison et al. (2007) analysed acommunication and conflict resolution training pro-gramme for staff and patients’ relatives in the special careof clients with dementia. An improvement in clientoutcomes (aggression, self-abuse or sexual advances,inappropriate dress or disrobing, constant requests forattention or help, and wandering) could be observed 2months after the intervention, although the clientsthemselves did not receive any intervention (p < .05).Van Weert et al. (2005) showed a significant effect onresident outcomes regarding depressive behaviour, loss ofdecorum, and restless behaviour (p < .05). The authorsreferred to a possible strong interaction between client-related outcomes and psychological outcomes (such asstress reactions, job satisfaction and burnout) amongCNAs.
In further two studies the authors mentioned improve-ments on client related general condition; however it wasnot the focal point of their analysis. The observed effect
Table 2
Number of post-tests and number of observed effects on staff burnout by type of intervention and time interval.
Intervention approach Short term
(�1 month)
Medium term
(�1 year)
Long term
(>1 year)
Total
n n* n n* n n* n n*
Person-directed 8 2(1a) 5 0 1 0 9 2 (3)
Work-directed 1 1 2 2 0 0 2 2
Combined 2 1 3 2 1 1 5 3
All 11 5 10 4 2 1 16 7(8)
Note. n: number of studies; n*: number of studies with effect.a One study with short-term effects only directly after intervention.

wa200
3.6.
assposandSchet atheasson
et
assstuthisof tAn
4. D
stutermOnequaallostuappparinsusevenof t
mefor
spe
4.1.
a rinteperup
comburTheassburdirestafSec
termhowFucpro
C. Westermann et al. / International Journal of Nursing Studies 51 (2014) 63–71 69
s only mentioned in the discussion part (Baldelli et al.,4; Jeon et al., 2012).
Quality of the included studies
Ten out of 16 studies were classified as RCTs (62.5%) andigned to evidence level I. Of these, three showeditive correlations between the interventions analysed
staff burnout (Jeon et al., 2012; Mackenzie et al., 2006;rijnemaekers et al., 2003). The results of Mackenziel. (2006), however, have to be viewed critically given
small sample size (n < 50). In three out of five studiesigned to evidence level II, positive effects could be seenstaff burnout (Haberstroh et al., 2009; Fuchs-Lacelleal., 2008; Van Weert et al., 2005). One study wasigned to evidence level III (Baldelli et al., 2004). Thisdy showed a positive effect on staff burnout. However,
result had to be viewed critically due to the limitationshe study design (no control group, small sample size).overview is shown in Table 1.
iscussion
This paper provides an overview of the interventiondies on burnout in inpatient elderly and geriatric long-
care from the period between 2000 and January 2012. positive aspect is the relatively large number of high-lity studies. The publications available, however, onlyw for a limited comparison of the effects achieved. The
dies differed in terms of the conceptual nature of theroach (design, intervention, number of participants,ticipant group) as well as with respect to the surveytruments employed. Although 14 out of the 16 studiesd the MBI system, a comparison between the inter-tions observed was restricted by the heterogeneous usehe tool (version, scale items).The need to address increasing psychogeriatric require-nts in elderly care was reflected in the settings chosenthe interventions. The setting chosen was primarilycialised dementia care.
Summary – effects of interventions on staff burnout
All studies (n = 2) with a work-directed approach led toeduction in staff burnout, lasting up to 1 year afterrvention (Table 2). Two out of nine interventions with a
son-directed approach had an effect on staff burnout forto 1 month after the intervention. Three out of fivebined interventions led to positive effects on staff
nout lasting from up to 4 months to more than 1 year. majority of RCTs (seven out of ten) found no
ociation between the interventions examined and staffnout. Evidence for the effectiveness of work-, person-cted and combined interventions in terms of reducingf burnout is thus limited. Possible causes are listed intion 4.3.The two work-directed interventions had medium-
effects on staff burnout. The interventions were,ever, very different – pain assessment in the case of
hs-Lacelle et al. (2008) and exercise and activitygrammes for clients with dementia in the case of
Baldelli et al. (2004). Direct comparisons were thereforenot feasible.
Out of the nine studies using person-directed inter-vention, only two had a positive impact on staff burnout,with any effects only recorded over the short term. Thebrief mindfulness-based stress reduction intervention forstaff revealed a significant health-promoting effect on theburnout sub-scale emotional exhaustion (Mackenzie et al.,2006). This study was also mentioned in the reviewperformed by Van Wyk and Pillay-Van Wyk (2010), butwas assessed differently. The authors only compared meanvalues in the intervention group with those in the controlgroup at the post-training. Consequently, the differentstarting values of the two groups were disregarded,meaning that the effect was underestimated.
4.1.1. Unconfirmed short-term effects on staff burnout
In a study by Mackenzie and Peragine (2003) short-term effects on staff burnout could be observed onlydirectly after intervention, but not at follow up (after 3months). In order to maintain the effects achieved, theauthors recommended a continuous approach. As arguedby Zimber et al. (2001), a lack of continuity in the trainingprogrammes will lead to limited effects.
4.2. Other effects on client-related outcomes
In addition to staff burnout, three studies observedpositive effects relating to the client outcomes (Haberstrohet al., 2009; Robison et al., 2007; Van Weert et al., 2005).Within this context, Van Weert et al. (2005) referred to apossible marked interaction between factors such asworkload, client-related outcomes and psychological out-comes for employees. In line with this hypothesis,Haberstroh et al. (2009) confirmed, on the basis of thepre-post data, significant simultaneous correlationsbetween the social skills of nursing staff and client qualityof life.
4.3. Reasons for lack of effects on staff burnout
In nine studies, the interventions showed no impact onstaff burnout. The following possible reasons were referredto: the fact that the training units do not focus enough,from an organisational perspective, on the participants(Robison et al., 2007; Zimber et al., 2001), lack of objectivemeasuring instruments aimed at ensuring the optimumcontrol of intervention implementation (Jensen et al.,2006), different working conditions and work require-ments in the settings analysed (Jensen et al., 2006), too fewparticipants in the nursing facility in question (Davisonet al., 2007; Mackenzie and Peragine, 2003; Visser et al.,2008), lack of evaluation at administrative level in theinterests of sustainability (Robison et al., 2007; Zimberet al., 2001), lack of continuity (Davison et al., 2007; Kuskeet al., 2009; Mackenzie and Peragine, 2003; Zimber et al.,2001), lack of time to devote to care and rigid workingconditions (Kuske et al., 2009), inadequate staffing levelsand high levels of work-related demands (Davison et al.,2007), insufficient resources for the facilities, e.g. lack ofspace, lack of aids and means of transportation (Jensen

C. Westermann et al. / International Journal of Nursing Studies 51 (2014) 63–7170
et al., 2006) and ethical problems relating to clientobservation (Jensen et al., 2006).
The accompanying peer support meetings were wellreceived by employees but did not have any impact on staffburnout. Amongst other things, this was due to the factthat the programmes did not last long enough. Moreover,employees were not released from their duties in order toattend the meetings and there were not enough partici-pants. Lack of time and administrative support werefurther reasons for neglecting peer meetings after theintervention (Davison et al., 2007; Visser et al., 2008).
Several studies showed that possible barriers to changehave to be identified in the facility itself. The mostfrequently mentioned factor was a lack of support atmanagement level (Davison et al., 2007; Schrijnemaekerset al., 2003; Visser et al., 2008; Zimber et al., 2001).
4.4. Comparison of results with other reviews
Four reviews identified in this literature searchexamined the effectiveness of stress management inter-vention in healthcare occupations (Edwards et al., 2003;Mimura and Griffiths, 2003; Marine et al., 2006; Van Wykand Pillay-Van Wyk, 2010). Two further reviews analysedthe effectiveness of interventions to prevent stress andburnout across a number of different sectors (Van der Klinket al., 2001; Awa et al., 2010). In contrast to our results, Vander Klink et al. (2001) reported that work-directedinterventions did not lead to success in staff coping withstress. The authors identified only one study with acombined approach that yielded a significant effect.Edwards et al. (2003) found that lack of time for clientcontact was associated with high stress levels amonghealthcare staff, particularly in long-term nursing careoccupations. They also looked at how effective interven-tions (solely person-directed) are when it comes to dealingwith stress. Stress management training combined withrelaxation exercises and training measures, includingpsycho-social training units, helped to reduce burnoutamong long-term care staff. Mimura and Griffiths (2003)found more evidence in favour of person-directed thanwork-directed interventions. They were not able torecommend any particular approach for practical imple-mentation, however, as the number of studies examinedwas too small. Limited evidence was available regardingthe effectiveness of person- and work-directed interven-tions in reducing stress levels in healthcare settings byMarine et al. (2006). The authors proposed that the bestperiod for proving stress-reducing effects is between 6months and 2 years after the intervention. Van Wyk andPillay-Van Wyk (2010) stated that short-term measuresdid not yield any results. The most convincing evidencewas delivered by long-term measures. The authors were infavour of regular refresher courses (within 18 months)after the intervention in order to maintain the positiveeffects of the interventions on staff stress.
Awa et al. (2010) analysed cross-sector interventionstudies with different approaches (work- and person-directed as well as combined). In line with Van Wyk andPillay-Van Wyk (2010), they confirmed that interventions
accordance with our results, they found that person-directed interventions tended to have short-term effects,whereas interventions based on work-directed and com-bined approaches tended to have longer-term effects.
4.5. Limitations of this systematic literature review
The results may be influenced by publication bias.Studies published in journals that were not listed in thedatabases used in our review could not be identified in thisdatabase search.
Due to the heterogeneous methods used and themissing data in individual studies, this paper does notinclude a comparison of the effect estimates. Thissystematic literature review is purely descriptive in nature.
5. Conclusion
Although only a few interventions were able to achievea positive effect on staff burnout, we found that all threeintervention approaches are potentially useful in order toachieve positive effects on staff burnout. Work-directedand combined intervention programmes seem to achievepotentially longer-lasting effects than person-directedintervention programmes. More evidence is needed tomake a clear recommendation for an interventionapproach to prevent staff burnout. A more comprehensiveexamination of the causal links between burnout and otherfactors, e.g. client outcomes and employees’ professionalskills, is required. Similarly, there is a need for furtherlongitudinal studies with representative samples andsufficiently long investigation periods. Long-term aspectsshould be taken into account in future projects.
Contributions
CW, AN, and MH were responsible for project manage-ment. CW and AK were responsible for data collection andanalysis. CW was responsible for drafting the manuscript.AK, AN, and MH reviewed the paper for importantintellectual content.
Competing interests
The authors declare that they have no competinginterests.
References
Awa, W.L., Plaumann, M., Walter, U., 2010. Burnout prevention: a reviewof intervention programs. Patient Education and Counseling 78 (2),184–190.
Baldelli, M.V., Fabbo, A., Costopulos, C., Carbone, G., Gatti, R., Zucchl, P.,2004. Is it possible to reduce job burnout of the health care staffworking with demented patients? Archives of Gerontology andGeriatrics (Suppl. 9), 51–56.
Borritz, M., Rugulies, R., Bjorner, J.B., Villadsen, E., Mikkelsen, O.A., Kris-tensen, T.S., 2006. Burnout among employees in human service work:design and baseline findings of the PUMA study. Scandinavian Journalof Public Health 34 (1), 49–58.
Camerino, D., Conway, P.M., Van der Heijden, B.I., Estryn-Behar, M.,Consonni, D., Gould, D., Hasselhorn, H.M., 2006. Low-perceived work
ability, ageing and intention to leave nursing: a comparison among 10European countries. Journal of Advanced Nursing 56 (5), 542–552. with regular refresher courses had longer-term effects. In
Dav
Des
Edw
Ever
Frits
Fuch
Gan
Glas
Gold
GordHab
Hab
Hac
Jens
Jenu
Jeon
Kun
Kun
Kus
Lew
Mac
C. Westermann et al. / International Journal of Nursing Studies 51 (2014) 63–71 71
ison, T.E., McCabe, M.P., Visser, S., Hudgson, C., Buchanan, G., George,K., 2007. Controlled trial of dementia training with a peer supportgroup for aged care staff. International Journal of Geriatric Psychiatry22 (9), 868–873.
Jarlais, D.C., Lyles, C., Crepaz, N., 2004. Improving the reportingquality of nonrandomized evaluations of behavioral and public healthinterventions: the TREND statement. American Journal of PublicHealth 94 (3), 361–366.ards, D., Burnard, P., Owen, M., Hannigan, B., Fothergill, A., Coyle, D.,2003. A systematic review of the effectiveness of stress-managementinterventions for mental health professionals. Journal of Psychiatricand Mental Health Nursing 10 (3), 370–371.s, W., Tomic, W., Brouwers, A., 2002. Aggressive behaviour andburnout among staff of homes for the elderly. International Journalof Mental Health Nursing 11 (1), 2–9.ch, T., Kwak, J., Grant, S., Lang, J., Montgomery, R.R., Basting, A.D.,2009. Impact of TimeSlips, a creative expression intervention pro-gram, on nursing home residents with dementia and their caregivers.The Gerontologist 49 (1), 117–127.s-Lacelle, S., Hadjistavropoulos, T., Lix, L., 2008. Pain assessment as
intervention: a study of older adults with severe dementia. ClinicalJournal of Pain 24 (8), 697–707.doy-Crego, M., Clemente, M., Mayan-Santos, J.M., Espinosa, P., 2009.Personal determinants of burnout in nursing staff at geriatric centers.Archives of Gerontology and Geriatrics 48 (2), 246–249.er, J., Lampert, B., Weigl, M., 2008. Arbeit in der stationaren Altenp-flege - Analyse und Forderungern von Arbeitsbedingungen, Interak-tion Gesundheit und Qualitat. Wirtschaftsverlag NW - Verlag fur neueWissenschaft, Dortmund, Berlin, Dresden.berg, D.P., Hillier, V.F., 1979. A scaled version of the General Health
Questionnaire. Psychological medicine 9 (1), 139–145.is, L., 2000. Epidemiologie. W.B. Saunders, Marburg.
erstroh, J., Hampel, H., Pantel, J., 2010. Optimal management ofAlzheimer’s disease patients: clinical guidelines and family advice.Neuropsychiatric Disease and Treatment 6, 243–253.erstroh, J., Neumeyer, K., Schmitz, B., Pantel, J., 2009. Evaluation einesKommunikationstrainings fur Altenpfleger in der stationarenBetreuung demenzkranker Menschen (Tandem im Pflegeheim).(De-velopment and evaluation of a training program for nursing homeprofessionals to improve communication in dementia care). Zeits-chrift fur Gerontologie und Geriatrie 42 (2), 108–116.ker, W., Reinhold, S., Darm, A., Hubner, I., Wollenberger, E., 1995.Beanspruchungsscreening bei Humandienstleistungen (BHD-Sys-tem). TU Dresden. Institut fur Allgemeine Psychologie und Methodender Psychologie, Dresden.en, L.D., Gonge, H., Jors, E., Ryom, P., Foldspang, A., Christensen, M.,Vesterdorf, A., Bonde, J.P., 2006. Prevention of low back pain in femaleeldercare workers: randomized controlled work site trial. Spine 31(16), 1761–1769.ll, B., Brunner, E., Ofner, M., Mayr, M., 2008. Burnout und Coping in derstationaren Altenpflege. Ein regionaler Vergleich an examiniertenPflegekraften.(Burnout and coping in long term care units. A regionalcomparison in registered nurses). Pflege 21 (1), 16–24., Y.H., Luscombe, G., Chenoweth, L., Stein-Parbury, J., Brodaty, H.,King, M., Haas, M., 2012. Staff outcomes from the Caring for AgedDementia Care REsident Study (CADRES): a cluster randomised trial.International Journal of Nursing Studies 49 (5), 508–518.z, R., Burnand, B., Schunemann, H.J., 2008. Das GRADE-System. Eininternationaler Ansatz zur Vereinheitlichung der Graduierungvon Evidenz und Empfehlungen in Leitlinien.(The GRADE System.An international approach to standardize the graduation of evi-dence and recommendations in guidelines). Der Internist 49 (6),673–680.z, R., Khan, K.S., Kleijnen, J., Antes, G., 2009. Systematische Ubersicht-sarbeiten und Meta-Analysen - Einfuhrung in Instrumente der evi-denzbasierten Medizin fur Arzte klinische Forscher und Experten imGesundheitswesen. Verlag Hans Huber, Hogrefe AG, Bern.ke, B., Luck, T., Hanns, S., Matschinger, H., Angermeyer, M.C., Behrens,J., Riedel-Heller, S.G., 2009. Training in dementia care: a cluster-randomized controlled trial of a training program for nursing homestaff in Germany. International Psychogeriatric 21 (2), 295–308.is, R., Yarker, J., Donaldson-Feilder, E., Flaxman, P., Munir, F., 2010.Using a competency-based approach to identify the managementbehaviours required to manage workplace stress in nursing: a criticalincident study. International Journal of Nursing Studies 47 (3), 307–313.kenzie, C.S., Peragine, G., 2003. Measuring and enhancingself-efficacy among professional caregivers of individuals with
dementia. American Journal of Alzheimer’s Disease & Other Demen-tias 18 (5), 291–299.
Mackenzie, C.S., Poulin, P.A., Seidman-Carlson, R., 2006. A brief mind-fulness-based stress reduction intervention for nurses and nurseaides. Applied Nursing Research 19 (2), 105–109.
Marine, A., Ruotsalainen, J., Serra, C., Verbeek, J., 2006. Preventing occu-pational stress in healthcare workers. Cochrane Database of Systema-tic Reviews (4), CD002892.
Maslach, C., Schaufeli, W.B., Leiter, M.P., 2001. Job burnout. The AnnualReview of Psychology 52, 397–422.
McHugh, M.D., Kutney-Lee, A., Cimiotti, J.P., Sloane, D.M., Aiken, L.H.,2011. Nurses’ widespread job dissatisfaction, burnout, and frustrationwith health benefits signal problems for patient care. Health Affairs30 (2), 202–210.
Mimura, C., Griffiths, P., 2003. The effectiveness of current approaches toworkplace stress management in the nursing profession: an evidencebased literature review. Occupational and Environmental Medicine60 (1), 10–15.
Narumoto, J., Nakamura, K., Kitabayashi, Y., Shibata, K., Nakamae, T.,Fukui, K., 2008. Relationships among burnout, coping style andpersonality: study of Japanese professional caregivers for elderly.Psychiatry and Clinical Neurosciences 62 (2), 174–176.
Opie, J., Doyle, C., O’Connor, D.W., 2002. Challenging behaviours in nur-sing home residents with dementia: a randomized controlled trial ofmultidisciplinary interventions. International Journal of GeriatricPsychiatry 17 (1), 6–13.
Prezewowsky, M., 2007. Demografischer Wandel und Personalmanage-ment: Herausforderungen und Handlungsalternativen vor dem Hin-tergrund der Bevolkerungsentwicklung. Deutscher Universitats-Verlag.
Richardson, B., Kitchen, G., Livingston, G., 2002. The effect of education onknowledge and management of elder abuse: a randomized controlledtrial. Age and ageing 31 (5), 335–341.
Robison, J., Curry, L., Gruman, C., Porter, M., Henderson Jr., C.R., Pillemer,K., 2007. Partners in caregiving in a special care environment: coop-erative communication between staff and families on dementia units.The Gerontologist 47 (4), 504–515.
Rodney, V., 2000. Nurse stress associated with aggression in people withdementia: its relationship to hardiness, cognitive appraisal and cop-ing. Journal of Advanced Nursing 31 (1), 172–180.
Schrijnemaekers, V.J., van Rossum, E., Candel, M.J., Frederiks, C.M., Derix,M.M., Sielhorst, H., van den Brandt, P.A., 2003. Effects of emotion-oriented care on work-related outcomes of professional caregivers inhomes for elderly persons. The Journals of Gerontology Series B:Psychological Sciences and Social Sciences 58 (1), S50–S57.
Van der Klink, J.J., Blonk, R.W., Schene, A.H., van Dijk, F.J., 2001. Thebenefits of interventions for work-related stress. American Journal ofPublic Health 91 (2), 270–276.
Van Weert, J.C., van Dulmen, A.M., Spreeuwenberg, P.M., Bensing, J.M.,Ribbe, M.W., 2005. The effects of the implementation of snoezelen onthe quality of working life in psychogeriatric care. InternationalPsychogeriatric 17 (3), 407–427.
Van Wyk, B.E., Pillay-Van Wyk, V., 2010. Preventive staff-support inter-ventions for health workers. Cochrane Database of SystematicReviews (3), CD003541.
Visser, S.M., McCabe, M.P., Hudgson, C., Buchanan, G., Davison, T.E.,George, K., 2008. Managing behavioural symptoms of dementia:effectiveness of staff education and peer support. Aging and MentalHealth 12 (1), 47–55.
Von Kanel, R., 2008. Das Burnout Syndrom: Eine medizinische Perspekk-tive. Praxis (Bern. 1994) 97 (9), 477–487.
Weyerer, S., Schaufele, M., Schrag, A., Zimber, A., 2004. DemenzielleStorungen, Verhaltensauffalligkeiten und Versorgung von Klientenin Einrichtungen der Altentagespflege im Vergleich mit Heimbewoh-nern: Eine Querschnittsstudie in acht badischen Stadten.(Dementiadisorders, behavior problems and the care of clients in geriatric day-care compared to residents in homes for the elderly: a cross-sectionalstudy in eight communities in Baden). Psychiatrische Praxis 31 (7),339–345.
Zimber, A., 1998. Beanspruchung und Stress in der Altenpflege: For-schungsstand und Forschungsperspektiven.(Job strain and stressamong geriatric caregivers: A review and a research agenda). Zeits-chrift fur Gerontologie und Geriatrie 31 (6), 417–425.
Zimber, A., Rudolf, A., Teufel, S., 2001. Arbeitsbelastungen in der Altenp-flege reduzieren: Ein Trainingsprogramm fur Mitarbeiter und Lei-tungskrafte.(Reducing work stress in geriatric care: a trainingprogram for nursing team and administrators). Zeitschrift fur Ger-ontologie und Geriatrie 34 (5), 401–407.