burn managment
TRANSCRIPT
Management of Acute Burn
BYPROF GOUDA ELLABBAN
Introduction Burn: Coagulative destruction of the skin and/or
its contents by thermal energy or absorption of physical energy.
Thermal damage occurs above 48 ºC.
Caused by
Heat
Chemical Electrical
Irradiation
magnitude of Damage
The magnitude of injury depend on:1. Duration of exposure2. Temp. of the conductor3. The mode of transmission. (wither by contact,
radiated heat, or flame)
- age- extent (percentage)- depth- location- Associated factors
Factors to evaluate the patient:
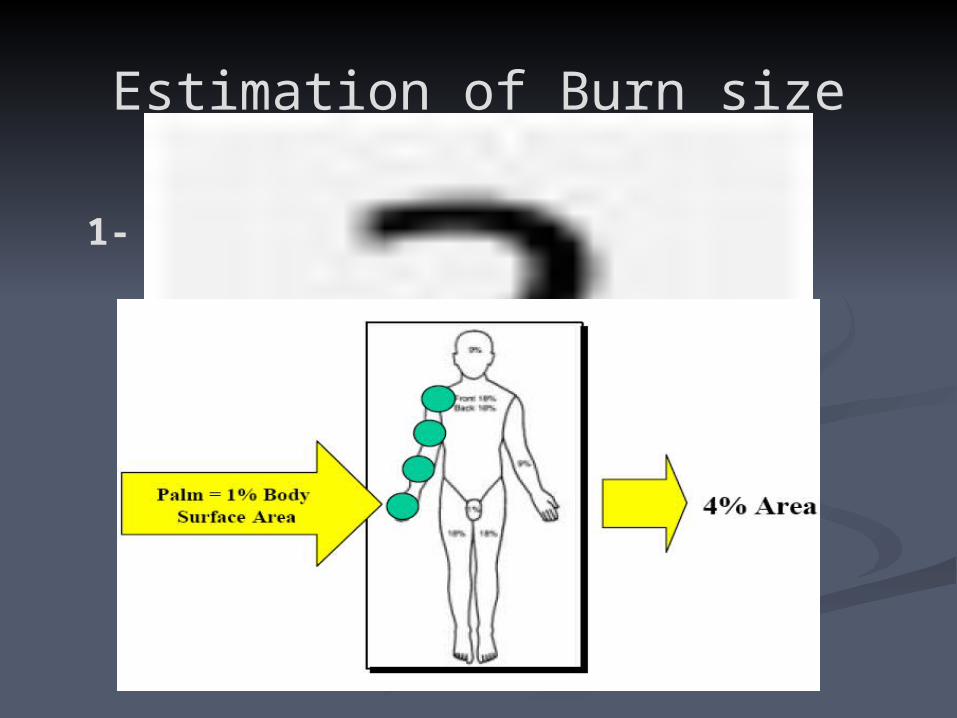
Estimation of Burn size
1- Estimation of Burn Size Using Palm.
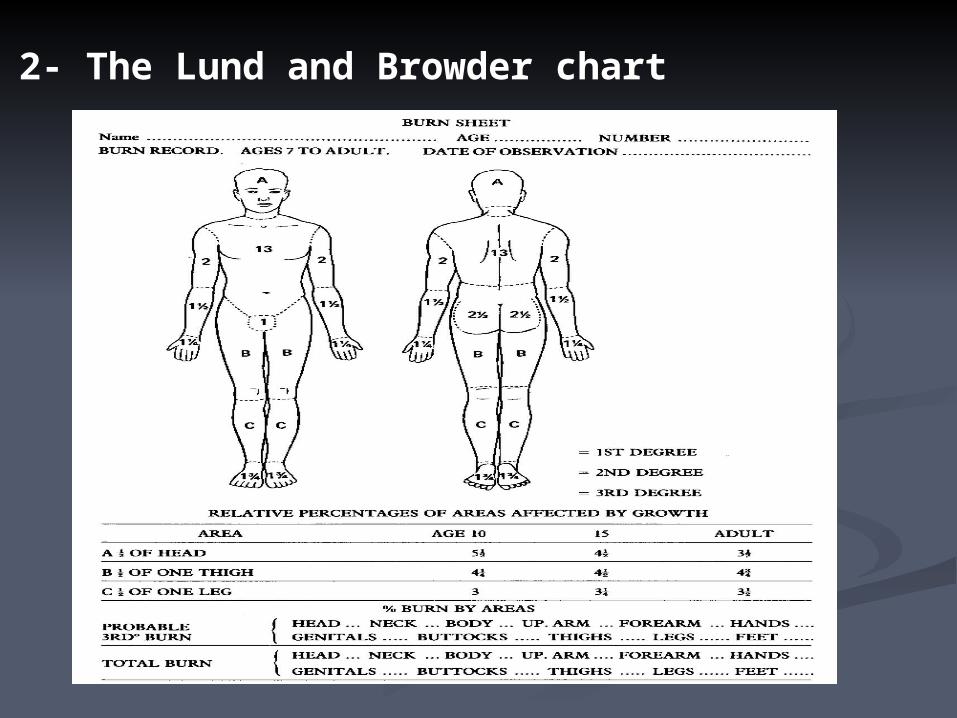
2- The Lund and Browder chart
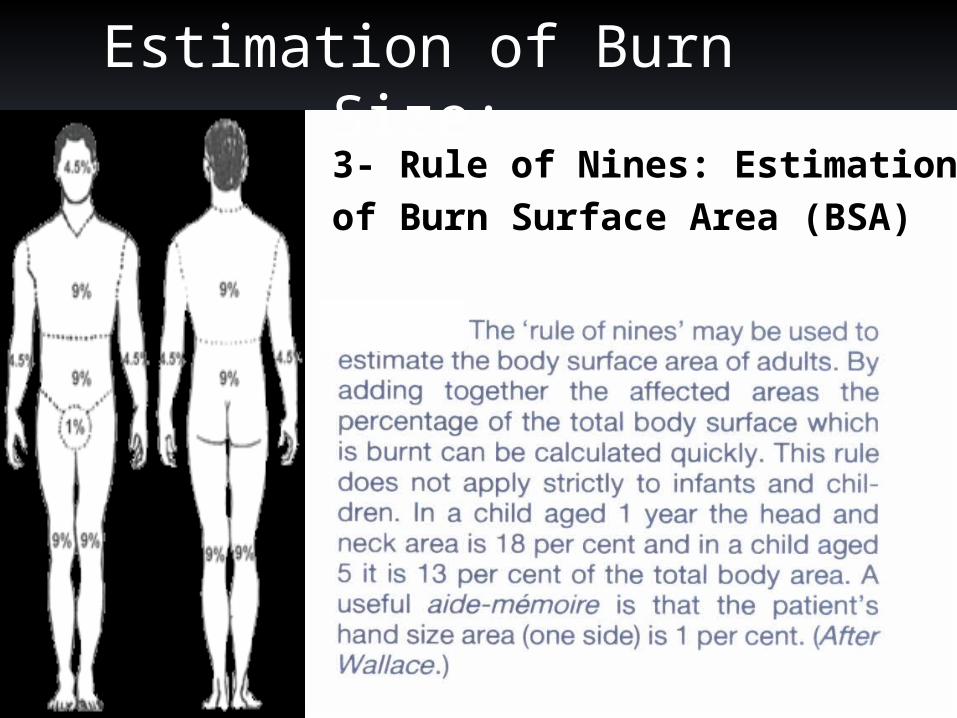
Estimation of Burn Size:3- Rule of Nines: Estimation of Burn Surface Area (BSA)
Classification of Burn severity:
1)minor burns:-in children :< 10% provided that it is superfacial & not
involving critical area-in adult: < 15%- no need for admission
Classification of Burn severity:
2) moderate burns: -children:10-20 % -adult:15-25%
3)major: -children >20 % -adult>25 % -or involving critical area or deep or associated with
other problems
Classification of Burn Depth
1. Partial skin thickness (superficial) or 1st degree: Burns extend through the epidermis and as far as the
most superficial dermis only. They are characterized by reactive processes in the
residual dermis (erythema, blistering) Heal spontaneously without scarring in two weeks. The treatment is non-surgical.

1st degree Burn:
Continue..
2- Deep dermal burns or 2nd degree: extend more deeply in to the dermis, but with
preservation of enough skin adnexal structures in the remaining dermis to allow spontaneous healing from these in three or more weeks.
Usually lead to hypertrophic scarring.

2nd degree Burn:
Continue..
3- Full thickness (deep) or 3rd degree: Deep burns destroy all dermal elements. There is therefore no reactive erythema, the skin is
often white in colour but may be charred where damage is extreme.
There is no skin sensation on pinprick due to skin innervation.

3rd degree Burn:
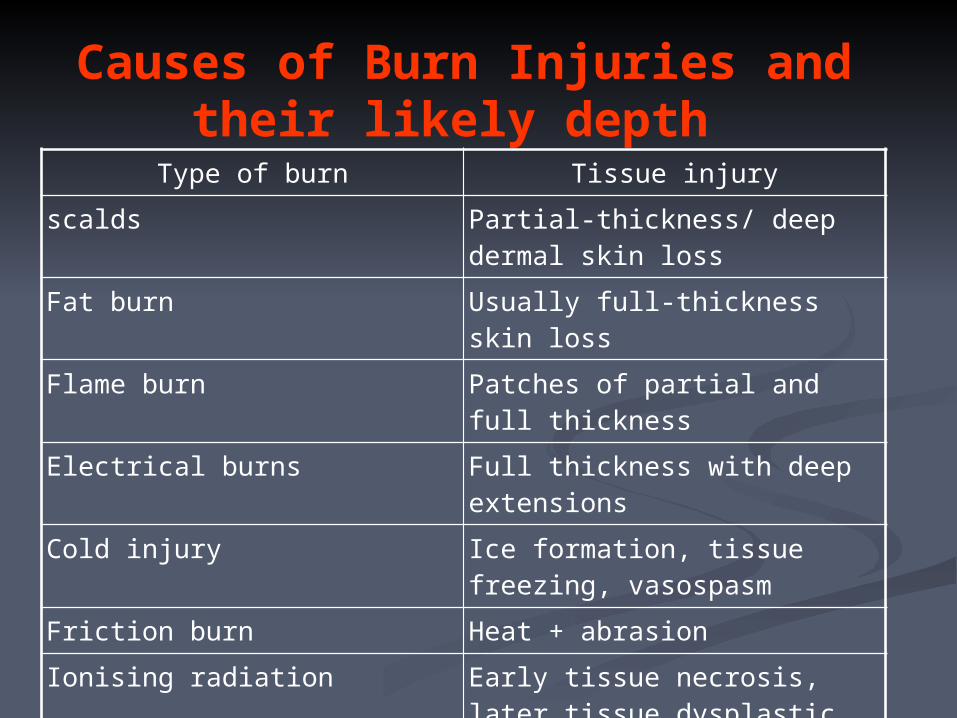
Causes of Burn Injuries and their likely depth
Type of burn Tissue injury
scalds Partial-thickness/ deep dermal skin loss
Fat burn Usually full-thickness skin loss
Flame burn Patches of partial and full thickness
Electrical burns Full thickness with deep extensions
Cold injury Ice formation, tissue freezing, vasospasm
Friction burn Heat + abrasion
Ionising radiation Early tissue necrosis, later tissue dysplastic changes
Chemical burn Inflammation, tissue necrosis, systemic effects
The effects of burn The effects of the burn upon the patient can be
considered as: * local: direct cellular damage, Inflammation &
Infection. * regional
* systemic
Local effect:1)Direct cellular damage: direct cell rupture or cell necrosis. denaturation of the connective tissue matrix. The capillaries are either thrombosed where the
damage is severe or in less damaged areas there is increased capillary permeability such that the tissues become oedematous and there is external leakage of serous fluid.
2)Inflammation:
marked and immediate inflammatory response. More severely damaged tissue may develop a more
prolonged inflammatory response. Macrophages produce inflammatory mediators and
phagocytose necrotic cells.
3)Infection: The damaged tissue represents a nidus for infection. Burn wounds will almost inevitably be colonised by micro-
organisms within 24-48 hours and this may remain as a local wound or regional infection.
There may in addition be a bacteraemia or septicaemia and metastatic infections may develop at other sites.
Bacteraemia is a common cause of fatality in a severe burn and may occur at any time from the first day until the point when all the wounds have entirely healed.
Beta-haemolytic streptococci and pseudomonads produce protease enzymes that prevent skin graft adhesion.
Regional : Limb circulation may be compromised (swelling and
tissue tension may lead to venous obstruction) muscle compartment syndrome ischaemic fibrosis and contractures
Systemic effects: Fluid loss & dehydration Multiple organ failure. Inhalation injury systemic complications Nonspecific complications
Fluid loss: may be lost from damaged capillaries either by
visible external loss or internally into the tissues from oedema in the region of the burn.
It is likely that this is mediated by cytokines acting on the microcirculation.
Multiple organ failure:
There may be progressive failure of renal or hepatic function or heart failure.
cerebral toxaemia, particularly in children, which has been attributed to electrolyte imbalance but other factors almost certainly apply.
Inhalalion injury: is not primarily thermal in origin but more of an
allergic response to inhaled irritants.
Pulmonary damage and failure can also be caused by circulating cellular debris and toxins from the burn wound; this is the pulmonary manifestation of multiple organ failure.
Systemic complications:
There are well-documented systemic complications in association with burns such as Curling's (gastric or duodenal) ulcer which may result in acute haematemesis.
Later there is a catabolic response to trauma with severe weight loss.
Nonspecific complications:
urinary tract infection from catheterisation deep vein thrombosis pulmonary embolism.

Management..
1- prehospital care :
The principles of prehospital care are as follows: Ensure rescuer safety Stop the burning process Check for other injuries Cool the burn wound Give oxygen Elevate
2- Hospital care :
The principles of managing an acute burn injury are the same as any acute trauma case
The priorities in the management of a major
burn: Airway
BreathingCirculationDisabilityExposure
Fluid resuscitation
Airway

Early intubation of suspected airway burn is the treatment of choice
The burned airway creates symptoms by swelling and if not managed can occlude the upper airway completely
Delay can make intubation very difficult due to swelling
Be ready to perform an emergency cricothyroidotomy if intubation is delayed
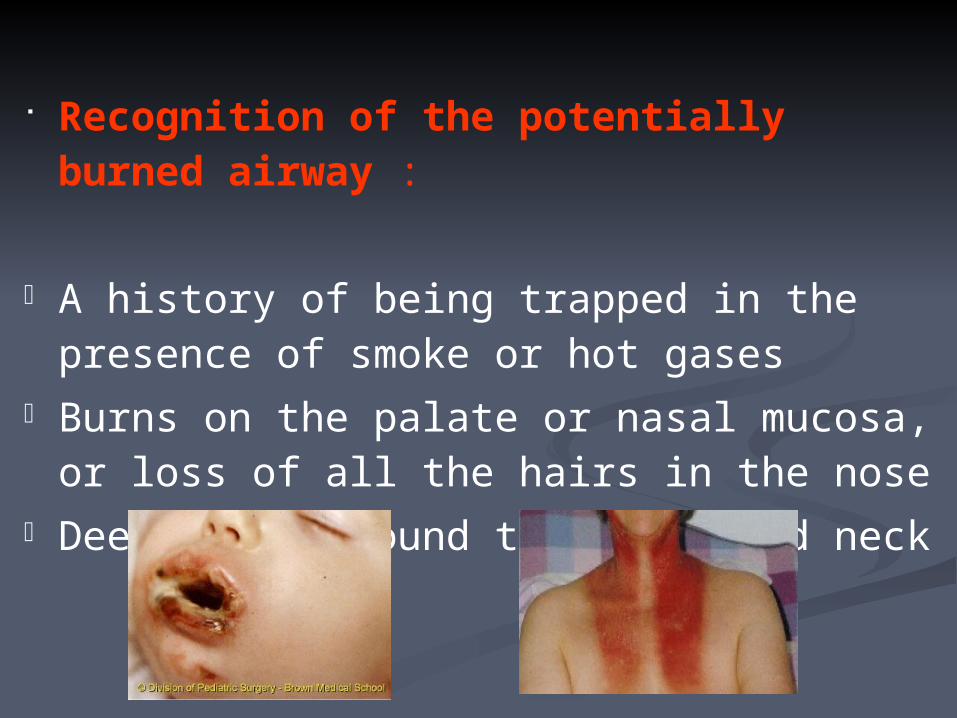
Recognition of the potentially burned airway :
A history of being trapped in the presence of smoke or hot gases
Burns on the palate or nasal mucosa, or loss of all the hairs in the nose
Deep burns around the mouth and neck
Breathing
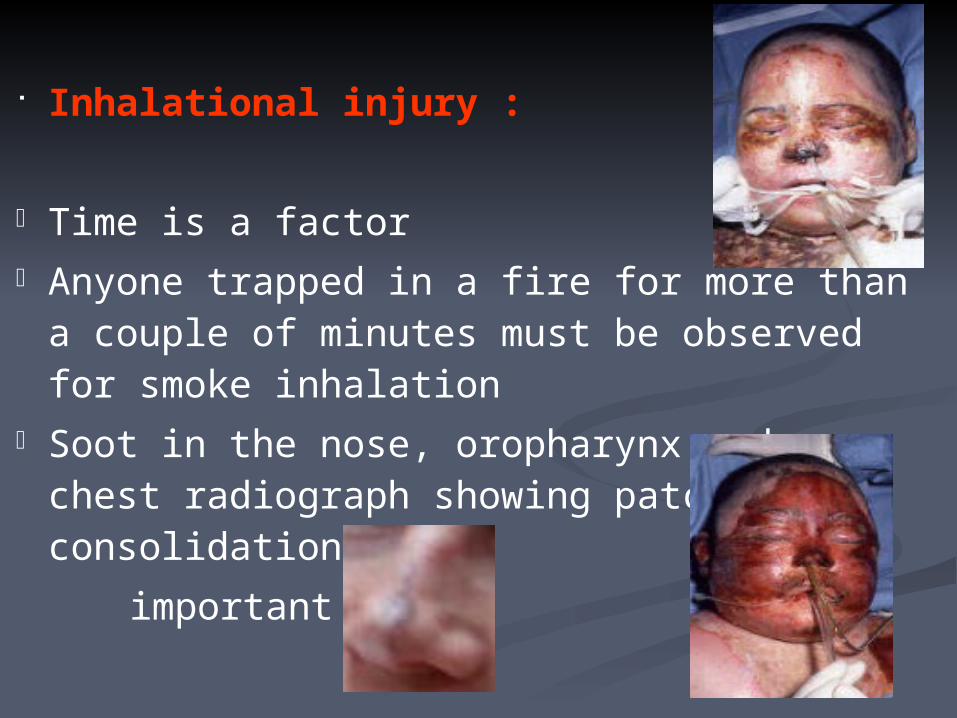
Inhalational injury :
Time is a factor Anyone trapped in a fire for more than a couple of
minutes must be observed for smoke inhalation Soot in the nose, oropharynx and a chest radiograph
showing patchy consolidation are important signs
Clinical features of inhalational injury :
Increase in respiratory effort and rate Rising pulse Anxiety Confusion Decreased oxygen saturation
These symptoms may not be apparent immediately and can take 24h to 5 days to develop
Treatment of inhalational injury :
Physiotherapy Nebulizers Warm humidified oxygen
The patient’s progress should be monitored using respiratory rate and blood gas measurements
Fluid resuscitation
The principle is that the intravascular volume must be maintained following a burn in order to provide sufficient circulation to perfuse to essential visceral organs and peripheral tissues
In children with burns over 10% TBSA and adults with burns over 15% consider the need for intravenous fluid resuscitation
If oral fluids are to be used salt must be added
Fluids needed can be calculated from a standard formula and the most used one is parkland formula
Total percentage body surface area*
Weight in kilograms*4=
Volume in ml
Half of this volume is given in the first 8 hours and the second half is given in the subsequent 16 hours
There are 3 types of fluids used1. Ringer’s lactate2. Hartman’s solution3. Human albumin sloution or fresh frozen plasma
Key of monitoring resuscitation is urine output
Treating the brun wound
Escharotomy : Circumferential full-thickness burns to the limbs require
emergency surgery The tourniquet effect of this injury is easily treated by
incising the whole length of full-thickness burn. This should be done in the mid-axial line avoiding major
nerves Thereafter the management of the burn wound remains
the same irrespective of the size of the injury

Full thickness burns and obvious deep dermal wounds : The 4 most common dressings are :-
1% sulphardiazine cream 0.5% silver nitrate solution Mafenide acetate cream Serum nitrate
Superficial partial thickness wounds :-
Will heal almost irrespective of the dressing Thus the key lies with dressings that are easy to
apply ,non painful ,simple and locally available The simplest method of treatment is by exposure The initial exudate needs to be managed by frequent
changes in clean linen around the patient
Additional aspects of treating the burned
patient
Analgesia :1. Acute: Superficial small burns
respond well to simple oral analgesia
Topical cooling is specially soothing
Large burns require intravenous opiates
2. Subacute: patients with large
burns need continuous analgesia
Beginning with infusion and continuing with
oral tablets
Energy balance and nutrition :
Burns patients need extra feeding A nasogastric tube should be used in all
patients with burns over 20% TBSA Burn injuries are catabolic in acute episode. The catabolic drive continues while the wound
remains unhealed. Removing the burn and achieving healing
stops the catabolic drive.
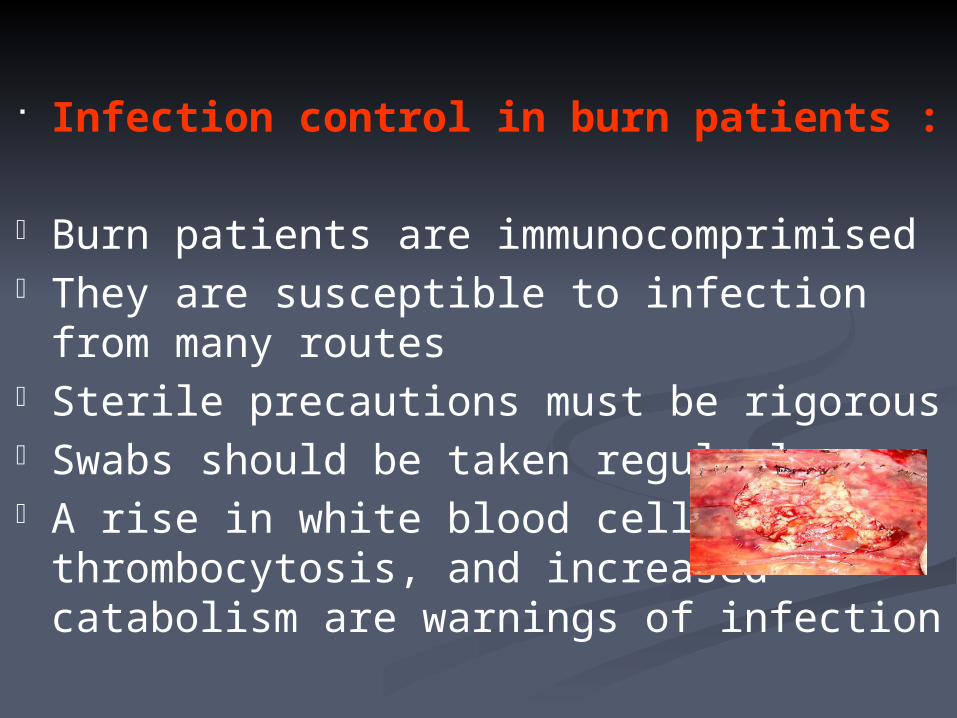
Infection control in burn patients :
Burn patients are immunocomprimised They are susceptible to infection from many
routes Sterile precautions must be rigorous Swabs should be taken regularly A rise in white blood cell count,
thrombocytosis, and increased catabolism are warnings of infection
Others :
Nursing care Physiotherapy Psychological
Surgery for the acute burn wound :
Deep dermal burns need tangential shaving and split-skin grafting
All but the smallest full-thickness burns need surgery and excision
The anesthetist needs to be ready for significant blood loss
Topical adrenaline reduces bleeding All burnt tissue needs to be excised Stable cover, permanent or temporary, should be applied
at once to reduce burn load
Delayed reconstruction of burns :
Eyelids must be treated before exposures keratitis arises Transposition flaps and Z-plasties with or without tissue
expansion are useful Full thickness grafts and free flaps may be needed for
large or difficult areas Hypertrophy is treated with pressure garments Pharamalogical treatment of itch is important

THANK YOU !!