brain-computer interface controlled robotic gait orthosis · the bci using a pair of...
TRANSCRIPT

1
Brain-Computer Interface Controlled Robotic GaitOrthosis
An H. Do1, Po T. Wang2, Christine E. King2, Sophia N. Chun3, Zoran Nenadic2,4
Abstract—Background: Excessive reliance on wheelchairs inindividuals with tetraplegia or paraplegia due to spinal cordinjury (SCI) leads to many medical co-morbidities, such ascardiovascular disease, metabolic derangements, osteoporosis,and pressure ulcers. Treatment of these conditions contributesto the majority of SCI health care costs. Restoring able-body-like ambulation in this patient population can potentially reducethe incidence of these medical co-morbidities, in addition to in-creasing independence and quality of life. However, no biomedicalsolution exists that can reverse this loss of neurological function,and hence novel methods are needed. Brain-computer interface(BCI) controlled lower extremity prostheses may constitute onesuch novel approach.
Methods: One able-bodied subject and one subject withparaplegia due to SCI underwent electroencephalogram (EEG)recordings while engaged in alternating epochs of idling andwalking kinesthetic motor imagery (KMI). These data wereanalyzed to generate an EEG prediction model for online BCIoperation. A commercial robotic gait orthosis (RoGO) system(suspended over a treadmill) was interfaced with the BCIcomputer to allow for computerized control. The subjects werethen tasked to perform five, 5-min-long online sessions wherethey ambulated using the BCI-RoGO system as prompted bycomputerized cues. The performance of this system was assessedwith cross-correlation analysis, and omission and false alarmrates.
Results: The offline accuracy of the EEG prediction modelaveraged 86.30% across both subjects (chance: 50%). Thecross-correlation between instructional cues and the BCI-RoGOwalking epochs averaged across all subjects and all sessions was0.812±0.048 (p-value<10−4). Also, there were on average 0.8false alarms per session and no omissions.
Conclusion: These results provide preliminary evidence thatrestoring brain-controlled ambulation after SCI is feasible. Fu-ture work will test the function of this system in a populationof subjects with SCI. If successful, this may justify the futuredevelopment of BCI-controlled lower extremity prostheses forfree overground walking for those with complete motor SCI.Finally, this system can also be applied to incomplete motor SCI,where it could lead to improved neurological outcomes beyondthose of standard physiotherapy.
Index Terms—Brain computer interface, gait, walking, roboticgait orthosis, Lokomat.
I. INTRODUCTION
INdividuals with tetraplegia or paraplegia due to spinal cordinjury (SCI) are unable to walk and most are wheelchair
1Department of Neurology, University of California, Irvine, CA, USA,email: [email protected]
2Department of Biomedical Engineering, UCI, CA, USA3Department of Spinal Cord Injury, Long Beach Veterans Affairs Medical
Center, Long Beach, CA, USA4Department of Electrical Engineering and Computer Science, UCI, CA,
USA
bound. Decreased physical activity associated with prolongedwheelchair use leads to a wide range of co-morbidities suchas metabolic derangements, heart disease, osteoporosis, andpressure ulcers [1]. Unfortunately, no biomedical solutionscan reverse this loss of neurological function, and treatmentof these co-morbidities contributes to the bulk of medicalcare costs for this patient population [1]. While commerciallyavailable lower extremity prostheses can help restore basic am-bulation via robust manual control, their adoption among theSCI community remains low, likely due to cost, bulkiness, andenergy expenditure inefficiencies. Hence, novel approaches areneeded to restore able-bodied-like ambulation in people withSCI. If successful, these will improve the quality of life inthis population, and reduce the incidence and cost of medicalco-morbidities as well as care-giver burden.
A brain-computer interface (BCI) controlled lower extrem-ity prosthesis may be one such novel approach. It can beenvisioned that a combination of an invasive brain signalacquisition system and implantable functional electrical stim-ulation (FES) electrodes can potentially act as a permanentBCI prosthesis. However, for safety reasons, the feasibilityof brain-controlled ambulation must first be established usingnoninvasive systems.
This concept was explored in the authors’ prior work [2]–[4] in which subjects (both able-bodied and SCI) used anelectroencephalogram (EEG) based BCI to control the am-bulation of an avatar within a virtual reality environment. Inthese studies, subjects utilized idling and walking kinestheticmotor imagery (KMI) to complete a goal-oriented task ofwalking the avatar along a linear path and making stops at 10designated points. In addition, two out of five subjects withSCI achieved BCI control that approached that of a manuallycontrolled joystick. While these results suggest that accurateBCI control of ambulation is possible after SCI, the translationof this technology from virtual reality to a physical prosthesishas not been achieved. In this study, the authors report onthe first case of integrating an EEG-based BCI system with arobotic gait orthosis (RoGO), and its successful operation byboth able-bodied and SCI subjects.
II. METHODS
To facilitate the development of a BCI-controlled RoGO,EEG data were recorded from subjects as they engaged inalternating epochs of idling and walking KMI. These data werethen analyzed offline to generate an EEG prediction model foronline BCI operation. A commercial RoGO system (suspendedover a treadmill), was interfaced with the BCI computer to
arX
iv:1
208.
5024
v3 [
cs.H
C]
26
Aug
201
3

2
allow for computerized control. In a series of five, 5-min-long online tests, the subjects were tasked to ambulate usingthe BCI-RoGO system when prompted by computerized cues.The performance of this system was assessed by calculatingthe cross-correlation and latency between the computerizedcues and BCI-RoGO response, as well as the omission andfalse alarm rates.
A. Training Data AcquisitionEthical approval was obtained from the Institutional Review
Board at the Long Beach Veterans Affairs Medical Cen-ter (LBVA) and the University of California, Irvine (UCI).Subjects were recruited from a population of able-bodiedindividuals, or those with chronic, complete motor paraplegiadue to SCI (> 12 months post-injury). The exclusion criteriafor subjects with SCI were severe spasticity, contractures,restricted range of motion, or fractures in the lower extremities,pressure ulcers, severe osteoperosis, or orthostatic hypoten-sion. These criteria were ruled out in a safety screeningevaluation consisting of an interview, a physical exam, lowerextremity dual-energy x-ray absorptiometry (DEXA) scan andx-rays, and a tilt-table exam.
An actively shielded 64-channel EEG cap was first mountedon the subjects’ head and impedances were reduced to <10KΩ. EEG signals were acquired using 2 linked NeXus-32bioamplifiers (Mind Media, Roermond-Herten, The Nether-lands) at a sampling rate of 256 Hz. The subjects weresuspended into a treadmill-equipped RoGO (Lokomat, Ho-coma, Volketswil, Switzerland) using partial weight unloading(see Figure 1). Note that unlike overground orthoses, thissystem facilitates safe and easy testing conditions for the earlydevelopment of BCI-prostheses for ambulation. Finally, EEGdata were collected as the subjects alternated between 30-secepochs of idling and walking KMI for a total of 10 min,as directed by computer cues. This entails vivid imaginationof walking during walking KMI cues, and relaxation duringidling cues. During this procedure, the subjects stood still withtheir arms at their sides.
B. Electromyogram and Leg Movement MeasurementElectromyogram (EMG) was measured to rule out BCI
control by voluntary leg movements in able-bodied subjects.To this end, baseline lower extremity EMG were measuredunder 3 conditions: active walking (subject voluntarily walkswhile the RoGO servos are turned off); cooperative walking(subject walks synergistically with the RoGO); and passivewalking (the subject is fully relaxed while the RoGO makeswalking movements). Three pairs of surface EMG electrodeswere placed over the left quadriceps, tibialis anterior, andgastrocnemius (Figure 1), and signals were acquired witha bioamplifier (MP150, Biopac, Goleta, CA), bandpass fil-tered (0.1-1000 Hz), and sampled at 4 KHz. In addition,leg movements were measured by a gyroscope (Wii MotionPlus, Nintendo, Kyoto, Japan) with a custom wristwatch-likeenclosure, strapped to the distal left lower leg (proximal tothe ankle, see Figure 1) [5]. Approximately 85% body-weightunloading was necessary for proper RoGO operation. Thewalking velocity was set to 2 km/hr.
Fig. 1. The experimental setup showing a subject suspended in the RoGO,while donning an EEG cap, surface EMG electrodes, and a gyroscope on theleft leg. A monitor (not shown), placed in front of the subject at eye-level,presented instructional cues.
C. Offline Analysis
An EEG prediction model was generated using the meth-ods described in Wang et al. [3], which are briefly sum-marized here. First, the training EEG data were subjectedto an automated algorithm to exclude those EEG channelswith excessive artifacts. The EEG epochs corresponding to“idling” and “walking” states were then transformed into thefrequency domain, and their power spectral densities (PSD)were integrated over 2-Hz bins. The data then underwentdimensionality reduction using a combination of classwiseprincipal component analysis (CPCA) [6], [7] and approximateinformation discriminant analysis (AIDA) [8]. The resulting 1-D spatio-spectral features were extracted by:
f = TAΦC(d) (1)
where f ∈ R is the feature, d ∈ RB×C are single-trial spatio-spectral EEG data (B-the number of frequency bins, C-thenumber of retained EEG channels), ΦC : RB×C → Rm
is a piecewise linear mapping from the data space to them-dimensional CPCA-subspace, and TA : Rm → R is anAIDA transformation matrix. Detailed descriptions of thesetechniques are found in [7], [8]. A linear Bayesian classifier:
f? ∈
I, if P (I |f?) > P (W |f?)
W, otherwise(2)
was then designed in the feature domain, where P (I |f?) andP (W |f?) are the posterior probabilities of “idling” and “walk-ing” classes, respectively. The performance of the Bayesianclassifier (2), expressed as a classification accuracy, was thenassessed by performing stratified 10-fold cross-validation [9].This was achieved by using 90% of the EEG data to trainthe parameters of the CPCA-AIDA transformation and theclassifier. The remaining 10% of the data then underwentthe above transformation and classification. This process was

3
repeated 10 times, each time using a different set of 9 foldsfor training and the remaining 1 fold for testing. Finally, theoptimal frequency range [FL, FH ] was found by increasing thelower and upper frequency bounds and repeating the aboveprocedure until the classifier performance stopped improv-ing [10]. The parameters of the prediction model, including[FL, FH ], the CPCA-AIDA transformation, and the classifierparameters, were then saved for real-time EEG analysis duringonline BCI-RoGO operation. The above signal processing andpattern recognition algorithms were implemented in the BCIsoftware and were optimized for real-time operation [10].
D. BCI-RoGO Integration
To comply with the institutional restrictions that prohibitsoftware installation, the RoGO computer was interfaced withthe BCI using a pair of microcontrollers (Arduino, Smart-Projects, Turin, Italy) to perform mouse hardware emulation.Microcontroller #1 relayed commands from the BCI computerto microcontroller #2 via an Inter-Integrated Circuit (I2C)connection. Microcontroller #2 then acted as a slave deviceprogrammed with mouse emulation firmware [11] to auto-matically manipulate the RoGO’s user interface. This setupenabled the BCI computer to directly control the RoGO idlingand walking functions.
E. Online Signal Analysis
During online BCI-RoGO operation, 0.75-sec segments ofEEG data were acquired every 0.25 sec in a sliding overlap-ping window. The PSD of the retained EEG channels werecalculated for each of these segments and used as the inputfor the signal processing algorithms described in Section II-C.The posterior probabilities of idling and walking classes werecalculated using the Bayes rule, as explained in Section II-C.
F. Calibration
Similar to the authors’ prior work [2]–[4], [10], [12], [13],the BCI-RoGO system is modeled as a binary state machinewith “idling” and “walking” states. This step is necessary toreduce noise in the online BCI operation and minimize themental workload of the subject. To this end, the posteriorprobability was averaged over 2 sec of EEG data, P (W |f?),and compared to two thresholds, TI and TW , to initiate statetransitions. Specifically, the system transitioned from “idling”to “walking” state (and vice versa) when P > TW (P < TI ),respectively. Otherwise, the system remained in the currentstate.
The values of TI and TW were determined from a shortcalibration procedure. Specifically, the system was set to runin the online mode (with the RoGO walking disabled) as thesubject alternated between idling or walking KMI for ∼5 min.The values of P were plotted in a histogram to empiricallydetermine the values of TI and TW . A brief familiarizationonline session with feedback was used to further fine-tunethese threshold values.
G. Online Evaluation
In an online evaluation, the subjects, while mounted inthe RoGO, used idling/walking KMI to elicit 5 alternating1-min epochs of BCI-RoGO idling/walking, as directed bystatic, textual computer cues (see Additional Files for videos).Ideally, during walking KMI, the underlying EEG changesshould initiate and maintain BCI-RoGO walking until walkingKMI stops. The subjects were instructed to make no voluntarymovements and to keep their arms still at their side. Leftleg EMG and movements were measured as described inSection II-B. This online test was performed 5 times in a singleexperimental day.
Online performance was assessed using the following met-rics [10], [12], [13]:
1) Cross-correlation between the cues and BCI-RoGOwalking
2) Omissions (OM)—failure to activate BCI-RoGO walk-ing during the “Walk” cues
3) False Alarms (FA)—initiation of BCI-RoGO walkingduring the “Idle” cues
For able-bodied subjects, analysis of EMG and leg move-ment data was performed to ascertain whether RoGO walkingwas entirely BCI controlled. First, to demonstrate that covertmovements were not used to initiate BCI-RoGO walking,gyroscope and rectified EMG data (in the 40-400 Hz band)were compared to the BCI decoded “walking” states in eachsession. Ideally, the initiation of these states should precedeEMG activity and leg movements. Then, to establish whethervoluntary movements were used to maintain BCI-RoGO walk-ing, EMG during these epochs were compared to the baselines(see Section II-B). To this end, EMG data were segmentedby individual steps based on the leg movement pattern [5], asmeasured by the gyroscope. The PSD of these EMG segmentswere then averaged and compared to those of the baselinewalking conditions. Ideally, the EMG power during BCI-RoGO walking should be similar to that of passive walkingand different from those of active and cooperative walking.
H. Controls
To determine the significance of each online BCI-RoGOsession’s performance, a nonlinear auto-regressive model wascreated:
Xk+1 = αXk + βWk, X0 ∼ U(0, 1) (3)Yk = h(Xk) (4)
where Xk is the state variable at time k, Wk ∼ U (0, 1) isuniform white noise, Yk is the simulated posterior probability,and h is a saturation function that ensures Yk ∈ [0, 1]. LetPk := P (W|f?k ) be a sequence of online posterior probabili-ties calculated in Section II-C. Assuming the sequence Pkis wide-sense stationary with mean µ and variance σ2, thecoefficients α and β can be determined from:
α = ρ (5)
αµ+β
2= µ (6)
4
TABLE IDEMOGRAPHIC DATA OF THE STUDY SUBJECTS. ASIA = AMERICAN
SPINAL INJURY ASSOCIATION.
Subject Age Gender Prior BCI Experience SCI Status1 42 Male ∼5 hours N/A2 25 Male ∼3 hours T6 ASIA B
where ρ is the correlation coefficient between Pk+1 andPk. Using these coefficients, 10,000 Monte Carlo trials wereperformed for each online session. Each sequence of simulatedposteriors, Yk, was then processed as in Section II-F above,and the cross-correlation between the cues and simulatedBCI-RoGO state sequence was calculated. An empirical p-value was defined as a fraction of Monte Carlo trials whosemaximum correlation was higher than that of the onlinesession.
III. RESULTS
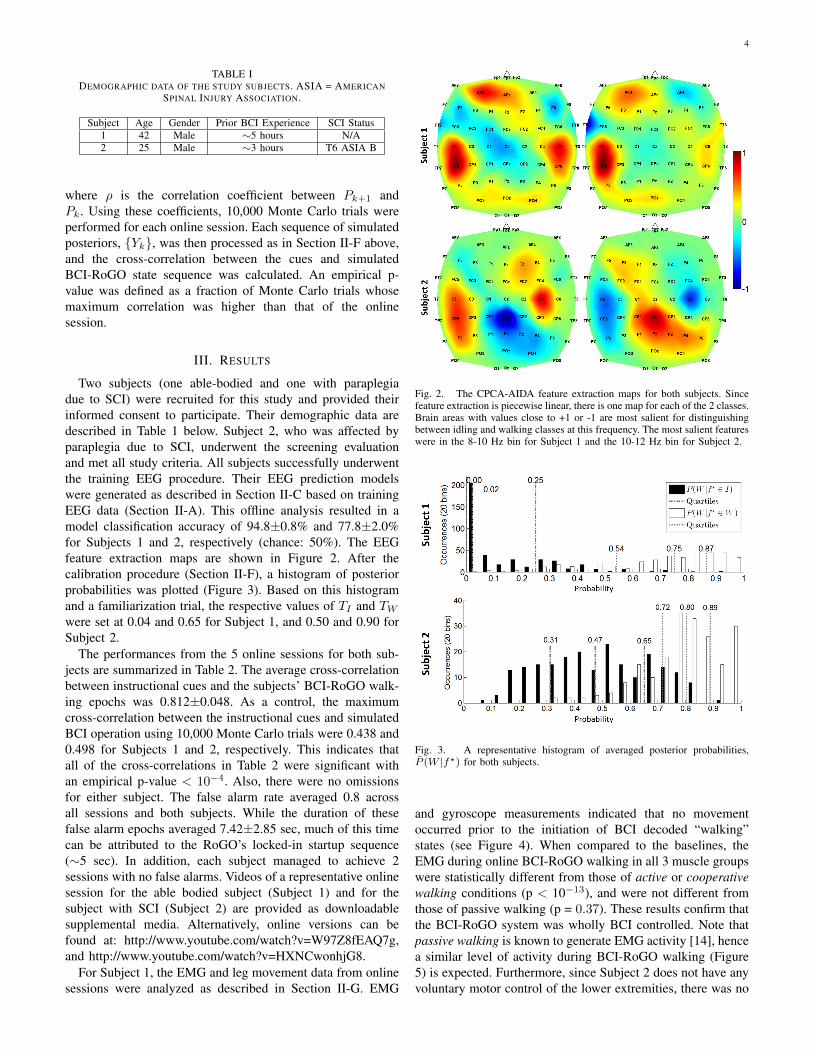
Two subjects (one able-bodied and one with paraplegiadue to SCI) were recruited for this study and provided theirinformed consent to participate. Their demographic data aredescribed in Table 1 below. Subject 2, who was affected byparaplegia due to SCI, underwent the screening evaluationand met all study criteria. All subjects successfully underwentthe training EEG procedure. Their EEG prediction modelswere generated as described in Section II-C based on trainingEEG data (Section II-A). This offline analysis resulted in amodel classification accuracy of 94.8±0.8% and 77.8±2.0%for Subjects 1 and 2, respectively (chance: 50%). The EEGfeature extraction maps are shown in Figure 2. After thecalibration procedure (Section II-F), a histogram of posteriorprobabilities was plotted (Figure 3). Based on this histogramand a familiarization trial, the respective values of TI and TWwere set at 0.04 and 0.65 for Subject 1, and 0.50 and 0.90 forSubject 2.
The performances from the 5 online sessions for both sub-jects are summarized in Table 2. The average cross-correlationbetween instructional cues and the subjects’ BCI-RoGO walk-ing epochs was 0.812±0.048. As a control, the maximumcross-correlation between the instructional cues and simulatedBCI operation using 10,000 Monte Carlo trials were 0.438 and0.498 for Subjects 1 and 2, respectively. This indicates thatall of the cross-correlations in Table 2 were significant withan empirical p-value < 10−4. Also, there were no omissionsfor either subject. The false alarm rate averaged 0.8 acrossall sessions and both subjects. While the duration of thesefalse alarm epochs averaged 7.42±2.85 sec, much of this timecan be attributed to the RoGO’s locked-in startup sequence(∼5 sec). In addition, each subject managed to achieve 2sessions with no false alarms. Videos of a representative onlinesession for the able bodied subject (Subject 1) and for thesubject with SCI (Subject 2) are provided as downloadablesupplemental media. Alternatively, online versions can befound at: http://www.youtube.com/watch?v=W97Z8fEAQ7g,and http://www.youtube.com/watch?v=HXNCwonhjG8.
For Subject 1, the EMG and leg movement data from onlinesessions were analyzed as described in Section II-G. EMG
Fig. 2. The CPCA-AIDA feature extraction maps for both subjects. Sincefeature extraction is piecewise linear, there is one map for each of the 2 classes.Brain areas with values close to +1 or -1 are most salient for distinguishingbetween idling and walking classes at this frequency. The most salient featureswere in the 8-10 Hz bin for Subject 1 and the 10-12 Hz bin for Subject 2.
Fig. 3. A representative histogram of averaged posterior probabilities,P (W |f?) for both subjects.
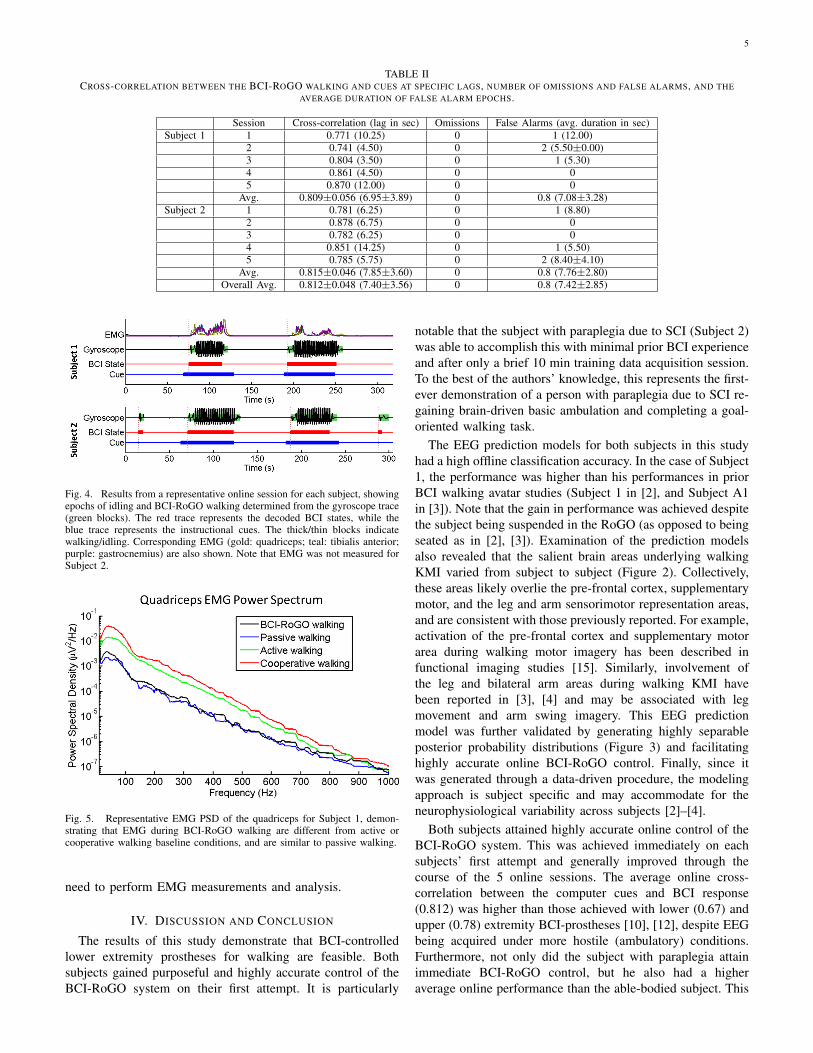
and gyroscope measurements indicated that no movementoccurred prior to the initiation of BCI decoded “walking”states (see Figure 4). When compared to the baselines, theEMG during online BCI-RoGO walking in all 3 muscle groupswere statistically different from those of active or cooperativewalking conditions (p < 10−13), and were not different fromthose of passive walking (p = 0.37). These results confirm thatthe BCI-RoGO system was wholly BCI controlled. Note thatpassive walking is known to generate EMG activity [14], hencea similar level of activity during BCI-RoGO walking (Figure5) is expected. Furthermore, since Subject 2 does not have anyvoluntary motor control of the lower extremities, there was no
5
TABLE IICROSS-CORRELATION BETWEEN THE BCI-ROGO WALKING AND CUES AT SPECIFIC LAGS, NUMBER OF OMISSIONS AND FALSE ALARMS, AND THE
AVERAGE DURATION OF FALSE ALARM EPOCHS.
Session Cross-correlation (lag in sec) Omissions False Alarms (avg. duration in sec)Subject 1 1 0.771 (10.25) 0 1 (12.00)
2 0.741 (4.50) 0 2 (5.50±0.00)3 0.804 (3.50) 0 1 (5.30)4 0.861 (4.50) 0 05 0.870 (12.00) 0 0
Avg. 0.809±0.056 (6.95±3.89) 0 0.8 (7.08±3.28)Subject 2 1 0.781 (6.25) 0 1 (8.80)
2 0.878 (6.75) 0 03 0.782 (6.25) 0 04 0.851 (14.25) 0 1 (5.50)5 0.785 (5.75) 0 2 (8.40±4.10)
Avg. 0.815±0.046 (7.85±3.60) 0 0.8 (7.76±2.80)Overall Avg. 0.812±0.048 (7.40±3.56) 0 0.8 (7.42±2.85)
Fig. 4. Results from a representative online session for each subject, showingepochs of idling and BCI-RoGO walking determined from the gyroscope trace(green blocks). The red trace represents the decoded BCI states, while theblue trace represents the instructional cues. The thick/thin blocks indicatewalking/idling. Corresponding EMG (gold: quadriceps; teal: tibialis anterior;purple: gastrocnemius) are also shown. Note that EMG was not measured forSubject 2.
Fig. 5. Representative EMG PSD of the quadriceps for Subject 1, demon-strating that EMG during BCI-RoGO walking are different from active orcooperative walking baseline conditions, and are similar to passive walking.
need to perform EMG measurements and analysis.
IV. DISCUSSION AND CONCLUSION
The results of this study demonstrate that BCI-controlledlower extremity prostheses for walking are feasible. Bothsubjects gained purposeful and highly accurate control of theBCI-RoGO system on their first attempt. It is particularly
notable that the subject with paraplegia due to SCI (Subject 2)was able to accomplish this with minimal prior BCI experienceand after only a brief 10 min training data acquisition session.To the best of the authors’ knowledge, this represents the first-ever demonstration of a person with paraplegia due to SCI re-gaining brain-driven basic ambulation and completing a goal-oriented walking task.
The EEG prediction models for both subjects in this studyhad a high offline classification accuracy. In the case of Subject1, the performance was higher than his performances in priorBCI walking avatar studies (Subject 1 in [2], and Subject A1in [3]). Note that the gain in performance was achieved despitethe subject being suspended in the RoGO (as opposed to beingseated as in [2], [3]). Examination of the prediction modelsalso revealed that the salient brain areas underlying walkingKMI varied from subject to subject (Figure 2). Collectively,these areas likely overlie the pre-frontal cortex, supplementarymotor, and the leg and arm sensorimotor representation areas,and are consistent with those previously reported. For example,activation of the pre-frontal cortex and supplementary motorarea during walking motor imagery has been described infunctional imaging studies [15]. Similarly, involvement ofthe leg and bilateral arm areas during walking KMI havebeen reported in [3], [4] and may be associated with legmovement and arm swing imagery. This EEG predictionmodel was further validated by generating highly separableposterior probability distributions (Figure 3) and facilitatinghighly accurate online BCI-RoGO control. Finally, since itwas generated through a data-driven procedure, the modelingapproach is subject specific and may accommodate for theneurophysiological variability across subjects [2]–[4].
Both subjects attained highly accurate online control of theBCI-RoGO system. This was achieved immediately on eachsubjects’ first attempt and generally improved through thecourse of the 5 online sessions. The average online cross-correlation between the computer cues and BCI response(0.812) was higher than those achieved with lower (0.67) andupper (0.78) extremity BCI-prostheses [10], [12], despite EEGbeing acquired under more hostile (ambulatory) conditions.Furthermore, not only did the subject with paraplegia attainimmediate BCI-RoGO control, but he also had a higheraverage online performance than the able-bodied subject. This

6
implies that future BCI-prostheses for restoring overgroundwalking after SCI may be feasible. Additionally, all of thesubjects’ online BCI-RoGO sessions were purposeful with a100% response rate (no omissions). Although Subject 1 hadno false alarms by the end of the experiment, Subject 2 stillexperienced false alarms in the final session. Although fewin number and short in duration, false alarms carry the riskof bodily harm, and this problem must be addressed in thedevelopment of future BCI-prostheses for overground walking.Table 2 also shows that the maximum correlation is attained atan average lag of 7.4 sec. Most of this lag can be attributed tothe RoGO’s locked-in power-down sequence (∼5 sec). Minorsources of delay include a combination of user response timeand the 2-sec long posterior probability averaging window (seeSection II-F). This delay can potentially be minimized withadditional user training in a controlled environment. Also,reducing the averaging window may eliminate some of thedelay, but this would be at the expense of increasing the falsealarm and omission rates. This trade-off will be examined infuture studies.
With no more than ∼5 hr of relevant BCI experience(operating the BCI walking avatar as described in [2]–[4]),both subjects attained a high-level of control of the BCI-RoGO system after undergoing a series of short procedures(i.e. 10 min training data acquisition, 5 min calibration, 5 minfamiliarization). This indicates that a data-driven EEG predic-tion model as well as prior virtual reality training may havefacilitated this rapid acquisition of BCI control. In addition,this model enables BCI operation using an intuitive controlstrategy, i.e. walking KMI to induce walking and idling KMIto stop. This is in contrast to requiring subjects to undergomonths of training in order to acquire a completely new skillof modulating pre-selected EEG signal features as frequentlydone in operant conditioning BCI studies. However, it remainsunclear whether applying an EEG decoding model generatedfrom idling/walking KMI will be robust enough against EEGperturbations caused by other simultaneous cognitive andbehavioral processes common during ambulation (e.g. talking,head turning). Anecdotally, no disruption of BCI operation wasobserved in this study and related previous BCI studies [3], [4]when the subjects engaged in brief conversations or hand andarm gestures during the familiarization session. Formalizedtesting of this hypothesis would require additional studies tobe performed.
Based on the above observations, this data-driven BCIapproach may be necessary for future intuitive and practicalBCI-controlled lower extremity prostheses for people withSCI. This approach would enable subjects with SCI to useintuitive BCI control strategies such as KMI of walking orattempted (albeit ineffective) walking. Similar to Subject 2 inthis study, this can potentially be accomplished with minimaluser training and supervision from the experiment operator.Finally, this approach may enhance the appeal and practical-ity of future BCI-controlled lower extremity prostheses forambulation by reducing the time burden and associated costs.
In conclusion, these results provide convincing evidencethat BCI control of ambulation after SCI is possible, whichwarrants future studies to test the function of this system in
a population of subjects with SCI. Since participants withSCI were able to operate the BCI-walking simulator [3], [4],it is expected that they can readily transfer these skills tothe BCI-RoGO system, similar to Subject 2. If successful,such a system may justify the future development of BCI-controlled lower extremity prostheses for free overgroundwalking for those with complete motor SCI. This includesaddressing issues such as additional degrees of freedom (e.g.turning, velocity modulation, transitioning between sitting andstanding), as well as appropriate solutions for signal acquisi-tion (e.g. invasive recordings). Finally, the current BCI-RoGOsystem can also be applied to gait rehabilitation in incompletemotor SCI. It can be hypothesized that coupling the behavioralactivation of the supraspinal gait areas (via the BCI) andspinal cord gait central pattern generators (feedback driving viathe RoGO) may provide a unique form of Hebbian learning.This could potentially improve neurological outcomes afterincomplete SCI beyond those of standard gait therapy.
ACKNOWLEDGMENT
This project was funded by the Long Beach Veterans Af-fairs Southern California Institute for Research and Education(SCIRE) Small Projects Grant, the Long Beach VeteransAffairs Advanced Research Fellowship Grant, the AmericanBrain Foundation, the National Institutes of Health (Grant UL1TR000153), and the National Science Foundation (Award:1160200).
REFERENCES
[1] R. L. Johnson, C. A. Brooks, and G. G. Whiteneck. Cost of trau-matic spinal cord injury in a population-based registry. Spinal Cord,34(8):470–480, 1996.
[2] P. T. Wang, C. E. King, L. A. Chui, Z. Nenadic, and A. H. Do. BCIcontrolled walking simulator for a BCI driven FES device. In Proc ofRESNA Ann Conf, 2010.
[3] Po T Wang, Christine E King, Luis A Chui, An H Do, and ZoranNenadic. Self-paced brain–computer interface control of ambulation in avirtual reality environment. Journal of Neural Engineering, 9(5):056016,2012.
[4] Christine E King, Po T Wang, Luis A Chui, An H Do, and ZoranNenadic. Operation of a brain-computer interface walking simulatorfor individuals with spinal cord injury. Journal of Neuroengineeringand Rehabilitation, 10: 77(1), 2013.
[5] K. Aminian, B. Najafi, C. Bula, P. F. Leyvraz, and Ph. Robert. Spatio-temporal parameters of gait measured by an ambulatory system usingminiature gyroscopes. J Biomech, 35(5):689–699, 2002.
[6] K. Das, S. Osechinskiy, and Z. Nenadic. A classwise PCA-basedrecognition of neural data for brain-computer interfaces. In Proc IEEEEng Med Biol Soc, pages 6519–6522, 2007.
[7] K. Das and Z. Nenadic. An efficient discriminant-based solution forsmall sample size problem. Pattern Recogn, 42(5):857–866, 2009.
[8] K. Das and Z. Nenadic. Approximate information discriminant analysis:A computationally simple heteroscedastic feature extraction technique.Pattern Recogn, 41(5):1548–1557, 2008.
[9] R. Kohavi. A study of cross-validation and bootstrap for accuracyestimation and model selection. In Int Joint C Art Int, pages 1137–1145, 1995.
[10] A. H. Do, P. T. Wang, A. Abiri, C. E. King, and Z. Nenadic. Brain-computer interface controlled functional electrical stimulation system forankle movement. J Neuroeng Rehabil, 8(49), 2011.
[11] Arduino UNO Mouse HID version 0.1, Mar 2011.http://hunt.net.nz/users/darran/.
[12] C. E. King, P. T. Wang, M. Mizuta, D. J. Reinkensmeyer, A. H. Do,S. Moromugi, and Z. Nenadic. Noninvasive brain-computer interfacedriven hand orthosis. In Proc 33rd Ann Int Conf of the IEEE Eng inMed and Biol Soc, pages 5786–5789, 2011.

7
[13] A. H. Do, P. T. Wang, C. E. King, A. Schombs, S. C. Cramer, andZ. Nenadic. Brain-computer interface controlled functional electricalstimulation device for foot drop due to stroke. In Proc 34th Ann IntConf of the IEEE Eng in Med and Biol Soc (accepted), 2012.
[14] S. Mazzoleni, G. Stampacchia, E. Cattin, E. Bradaschia, M. Tolaini,B. Rossi, and M. C. Carrozza. Effects of a robot-mediated locomotortraining on EMG activation in healthy and SCI subjects. In Proc IEEEInt Conf Rehab Robotics, pages 378–382, 2009.
[15] Christian La Fougere, Andreas Zwergal, Axel Rominger, Stefan Forster,Gunther Fesl, Marianne Dieterich, Thomas Brandt, Michael Strupp,Peter Bartenstein, and Klaus Jahn. Real versus imagined locomotion:a [18F]-FDG PET-fMRI comparison. Neuroimage, 50(4):1589–1598,2010.