bowel dysfunction: assessment and management in neurological patients alison bardsley continence...
TRANSCRIPT
Bowel Dysfunction: Assessment and Management in Neurological Patients
Alison BardsleyContinence Advisor
Clinical Editor – Continence UK
Supported by an Educational Grant from:
Prevalence & Epidimiology• Stroke
– Commonest cause of neurological damage– Faecal incontinence reported by 23% of 135 consecutive stroke patients– Older people, women and those with severe strokes most at risk
• Multiple Sclerosis– Two thirds of patients will complain of bowel problems– 70% of people report monthly episodes of incontinence– Prevalence of faecal incontinence/constipation between 39% & 73%
• Spinal cord injury– Up to 95% will require at least one therapeutic procedure to initiate defaecation– 50% need help to manage their bowel– Up to 80% of spinal cord injury patients complain of constipation– 15-25% report faecal incontinence
• Parkinson’s disease– Constipation and evacuation difficulties are common– Up to 50% have slow transit or evacuation type constipation
• Autonomic neuropathy (disease or degeneration of autonomic nervous system for example diabetes)
– Constipation reported in 12-88% of diabetic patients– 20% of diabetics complain of faecal urgency and incontinence– Evidence of decreased rectal sensation or impaired function of anal sphincters
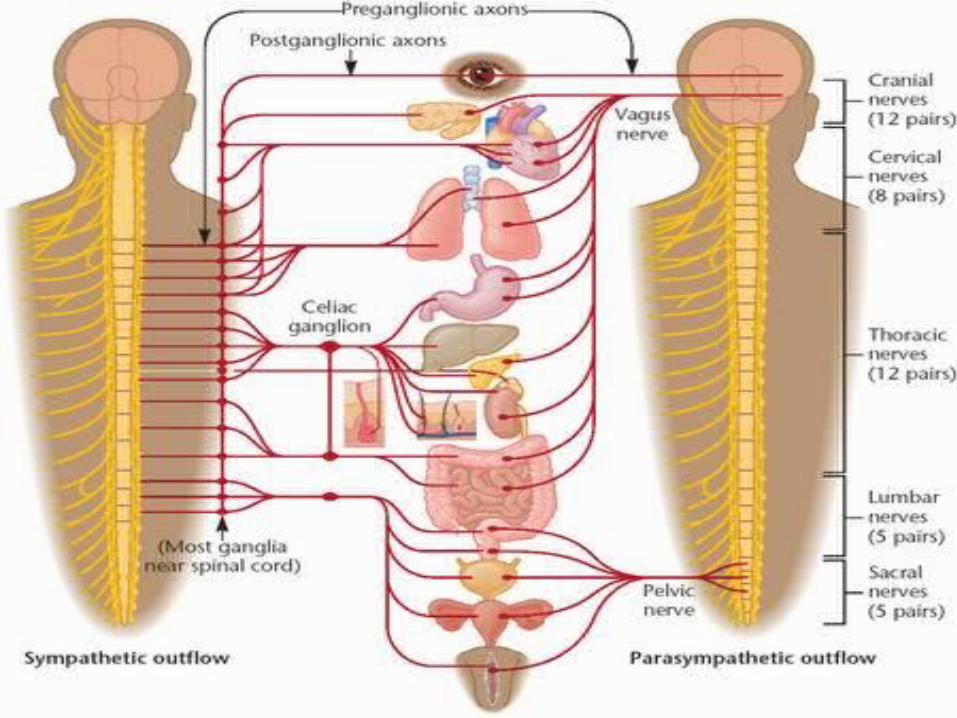
Neurophysiology of gastro-intestinal tract
• Extrinsic nervous control:– Autonomic nervous system (smooth muscle,
involuntary)• Parasympathetic and sympathetic fibres
– Somatic nerves (voluntary)• Supply motor and sensory control to large bowel &
pelvic floor
Neurophysiology (cont)
• Enteric Nervous system– Internal nervous system of the gut– Modulated via autonomic system to brain– Can mediate reflux activity independent of
central nervous system – Role in control of:
• Motility• Blood flow• Water and electrolyte transport• Acid secretion in digestive tract
Neurogenic bowel
• Bowel dysfunction due to:– Neuropathological process (e.g. spinal cord
injury)– Common causes unrelated to neurological
disease (e.g. low dietary fibre)– A combination of neuropathalogical and
common causes– Frontal lobe damage – emotional disturbance,
social relationships, reduced awareness, lack of voluntary control of pelvic floor.
Assessment
• Environment
• Individual
• Bowel
Environment
• Appropriate• Clean• Warm• Well lit• Toilet paper• Access• Help required?• Home/work• Involve multidisciplinary
team
Individual
• Impairment• Cognitive function• Mood/depression• Coping strategies• Concordance• Quality of life• Concomitant disease
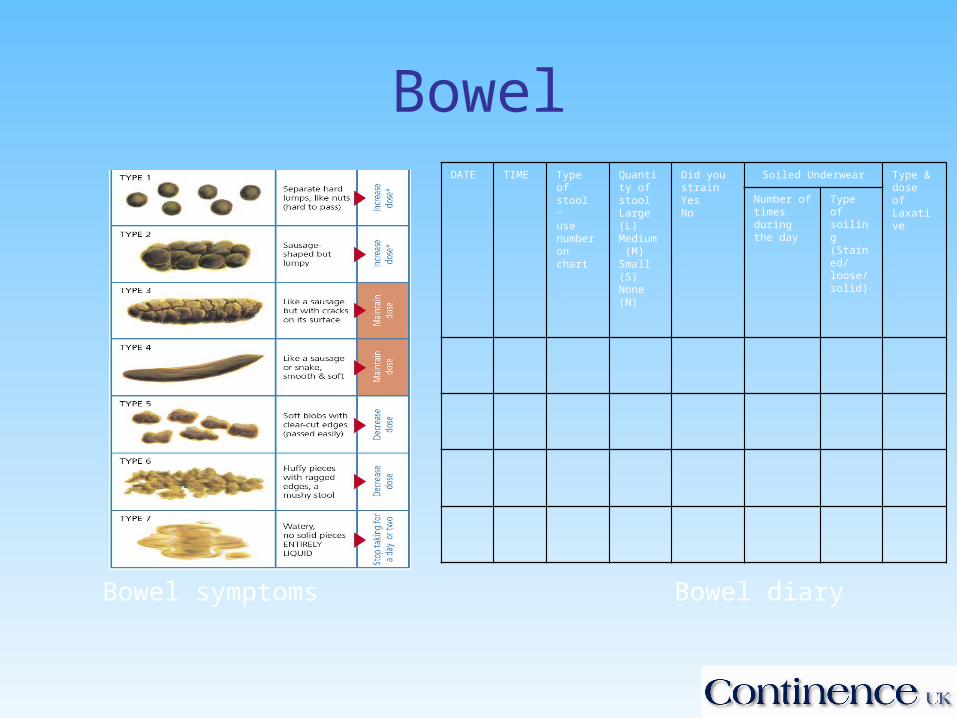
Bowel
Bowel symptoms Bowel diary
DATE TIME Type of stool ~ use number on chart
Quantity of stoolLarge (L)Medium (M)Small (S)None (N)
Did you strainYesNo
Soiled Underwear Type & dose of LaxativeNumber of
times during the day
Type of soiling(Stained/loose/solid)
Physical examination
• Digital Rectal examination– Anal/rectal tone– Sensation– Presence of faeces– Rectal prolapse
• Bowel transit• Anorectal manometry
Bowel management programmes
• Safe, private and pleasant environment
• Appropriate equipment / home adaptations
• Prevention of pressure damage
• Carers required?
• Scheduled bowel evacuation
• Diet and fluid intake
• Catheterisation
Assistive methods
• Abdominal massage
• Valsalva manoeuvre
• Deep breathing and leaning forward
• Digital ano-rectal stimulation
• Manual evacuation
• Biofeedback
• Rectal irrigation
AUTONOMIC DYSREFLEXIAUnique to spinal injury above T6
SYMPTOMS Headaches Severe hypertension Flushing above the lesion Sweating below the lesion Blotching of the skin Nasal congestion Bradycardia / tachycardia Palpitations Dilation of the pupils
Consent and legal issues
Lawful Consent
• Consent should be given by someone with the mental ability to do so
• sufficient information should be given to the patient
• Consent must be freely givenConsiderations – • Adults unable to give consent • Children
Dietary management
General Recommendations
• Dietary fibre: 18 to 30 g per day
• Fluid intake: 1.5 to 2 litres per day
• Fruit and vegetables: 5 portions per day
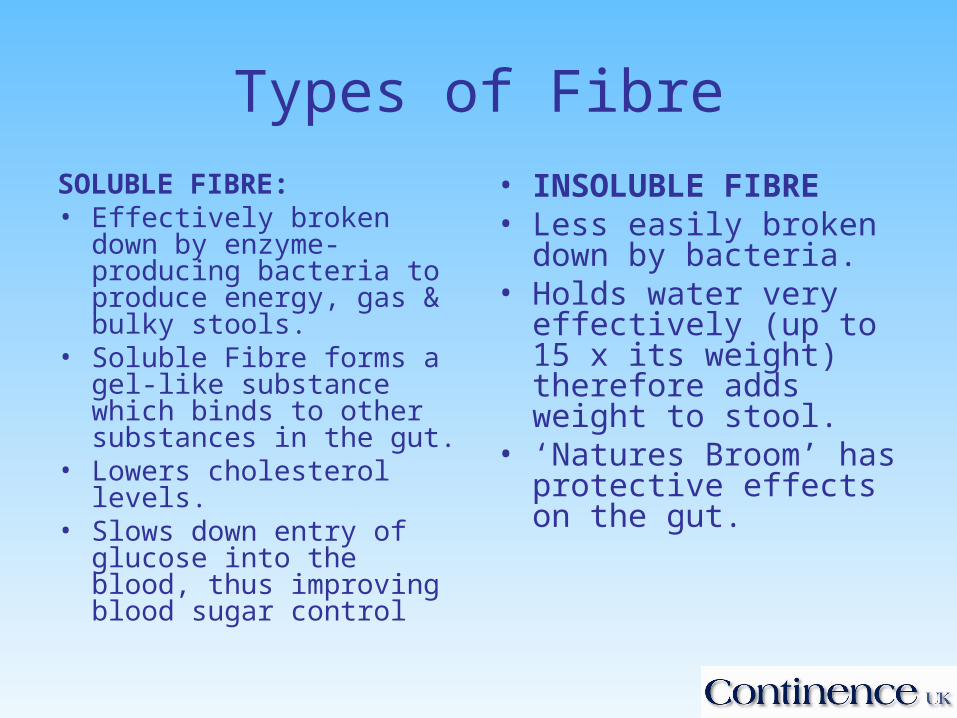
Types of Fibre
SOLUBLE FIBRE: • Effectively broken down by
enzyme-producing bacteria to produce energy, gas & bulky stools.
• Soluble Fibre forms a gel-like substance which binds to other substances in the gut.
• Lowers cholesterol levels.• Slows down entry of
glucose into the blood, thus improving blood sugar control
• INSOLUBLE FIBRE• Less easily broken down
by bacteria.• Holds water very
effectively (up to 15 x its weight) therefore adds weight to stool.
• ‘Natures Broom’ has protective effects on the gut.
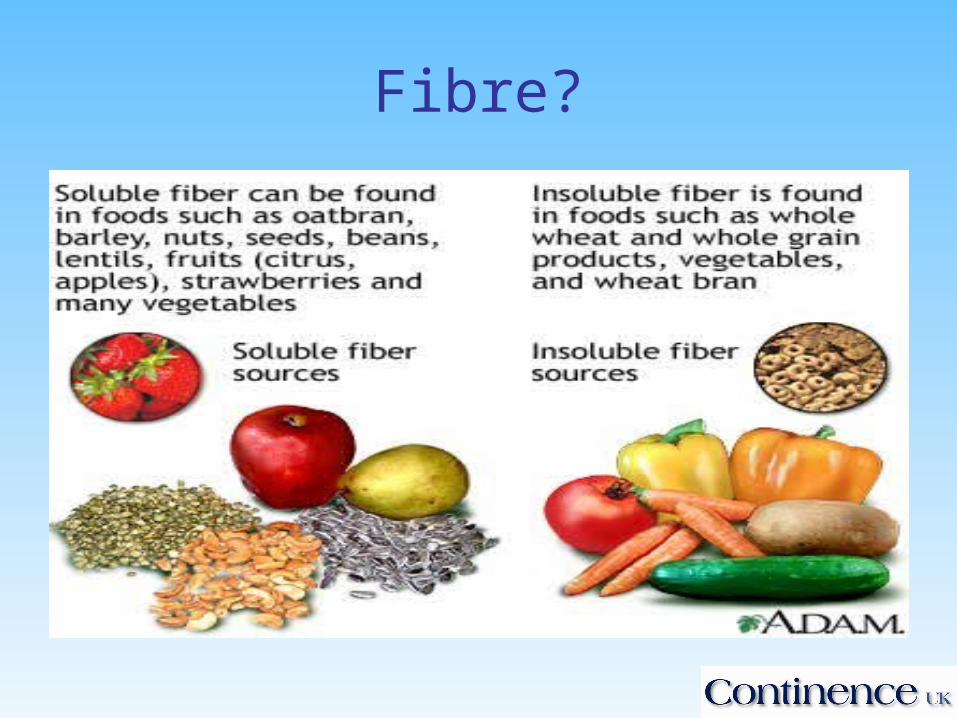
Fibre?

Medication treatment of Constipation
• LaxativesChoice of agent will depend on
– Presenting symptoms– Nature of complaint– Efficacy– Side –effects– Speed of action– Patient acceptability– Compliance– Cost
Types of laxatives
• Bulk forming
– Fybogel®, Celvevac® Normacol®, Regulan®
Act like dietary fibre increasing water content and faecal mass – increase stool
weight and frequency
Usually work within 24 -36 hours
Stimulant Laxatives
• Senna, Bisacodyl, co-danthramer, co-danthrasate, dioctyl, docusol
Stimulate an increase in colonic motility (peristalsis) and mucus secretion
Rapid acting 8-12 hours
Best taken in evening or at bedtime
Osmotic/iso-osmotic Laxatives• Lactulose and Magnesium salts – Osmotic
Act by drawing fluid from the body into the bowel by osmosis
• MOVICOL® - iso-osmotic
MOVICOL increases stool water content and directly triggers colonic propulsive activity and defaecation.
4 in 1 mode of action: Bulks, softens, stimulates and lubricates.
Rectal stimulants
• Bisacodyl and Glycerine
Used alone or in combination with digital stimulationPredictable
Consider a suppository inserter if hand function insufficient
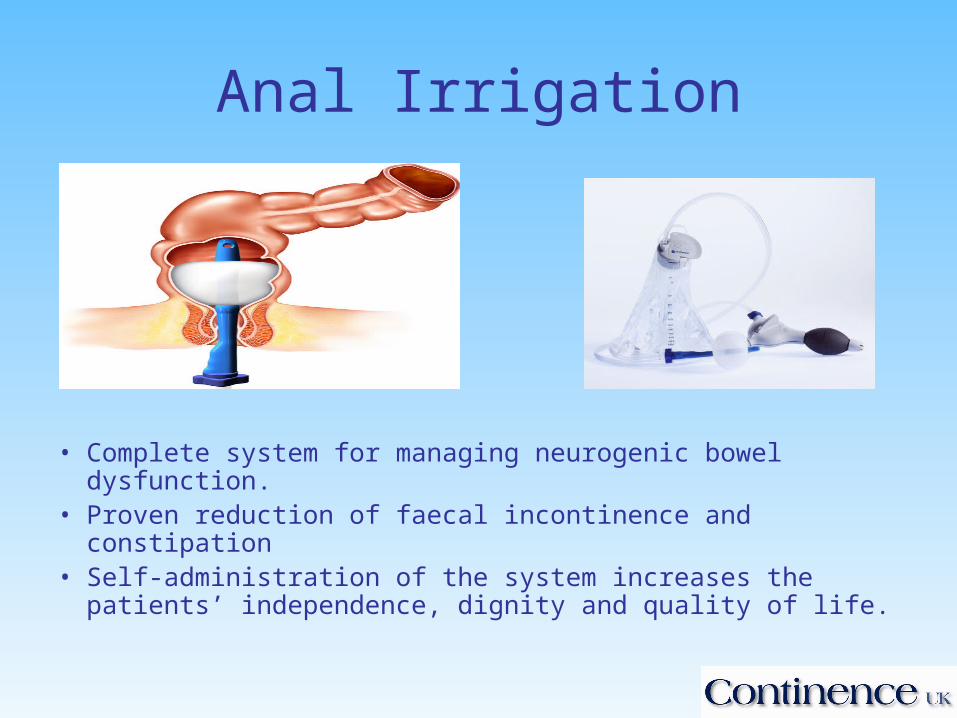
Anal Irrigation
• Complete system for managing neurogenic bowel dysfunction.
• Proven reduction of faecal incontinence and constipation • Self-administration of the system increases the patients’
independence, dignity and quality of life.
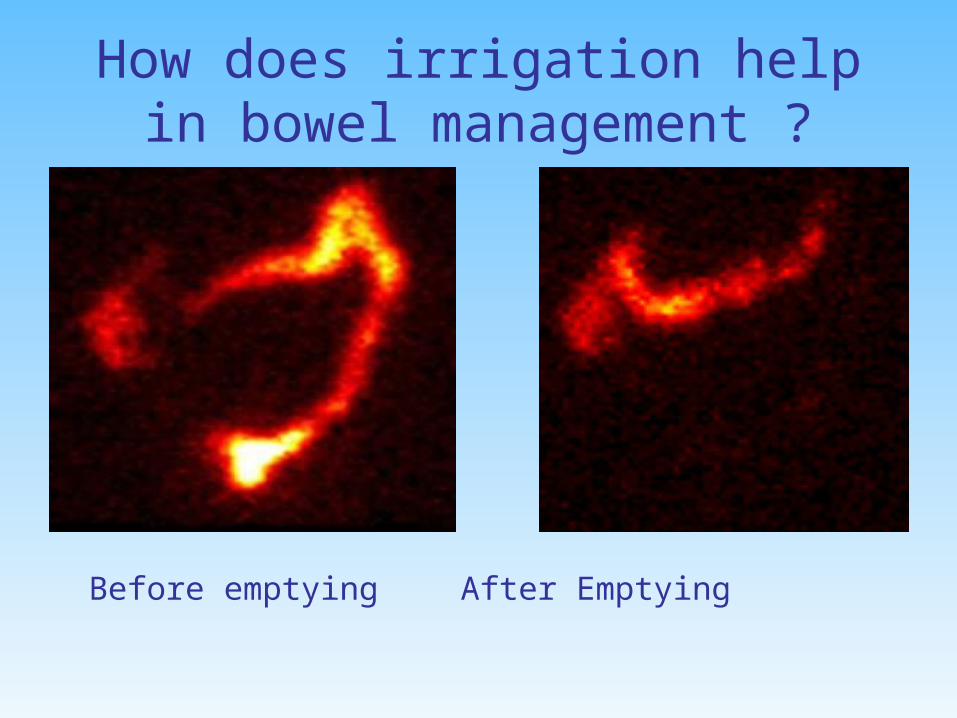
How does irrigation help in bowel management ?
Before emptying After Emptying
Faecal incontinence
• Address non-neurological causes– Anal sphincter damage– Infectious diarrhoea
• Exclude constipation or impaction
Conservative Measures
Patient education Bowel habit Defaecation posture Review medications (many can cause problems of hard
or loose stool) Diet & fluids Toilet facilities Support Practical management
Anti-Diarrhoeals
Loperamide up to 16mg (8 tablets) daily if stool loose
Take care not to constipate Half hour before meals At night for morning urgency PRN before going out Codeine phosphate an alternative Diarrhoea may need investigating
Loperamide
Reduces faecal incontinence & stool weight Improves stool consistency Raises resting pressure (Read et al, 1982) Increases water absorption, slows transit Decreases IAS & EAS relaxation upon rectal
distension (Rattan & Culver, 1987) May deliberately stop spontaneous evacuation &
empty with evacuants (Tobin & Brocklehurst, 1986)
Managing Faecal Incontinence
• No easy answers
• Difficult to disguise smells and prevent soreness
• Products
• Skin care
• Odour control
• Support
Anal Plug Many cannot tolerate due
to discomfort Not suitable for patients
with frequency, diarrhoea or inflammation
Can use up to 12 hrs Very good for a few May be most suitable for
those with less sensation (neurological)
Conclusion
• Healthcare professionals play a key role:– Promoting
independence– Support– Link/co-ordination with
other services– Advice and information

Any questions?
Contact details:
For further information and handouts
www.continence-uk.com
Our thanks go to Norgine Pharmaceuticals Ltd. for providing an educational grant to support this
workshop