bio mechanics of edentulous state
TRANSCRIPT

good afternoon
Biomechanics of edentulous state
Guided by- Presented by- dr.indrani dasDr P.N. Sharma p.g. 1st year student
Outline-IntroductionCauses of patients becoming edentulousMechanism of tooth supportMechanisms of Complete denture SupportDIFFERENCES between persons with natural teeth and persons wearing CDRR changes following teeth lossOcclusionDistribution of StressMorphologic Changes in the face associated with the edentulous stateIndividual behavioural responses Adaptive & psychological responses
Introduction
The edentulous patient represents a compromise in
the integrity of the masticatory system that is
frequently accompanied by
adverse functional and cosmetic sequelae,
which are varyingly perceived by edentulous patient.
Perceptions of the edentulous state may vary from feelings of inconvienience to feelings of handicap.
This seminar provides an understanding of the effects of edentulous condition and its clinical management.
Causes of patients becoming edentulous
•Caries•Periodontal disease
•Non disease factors•Attitude•Behavior•Dental attendance•Characteristics of health
system•Low occupational levels
Mechanism of tooth support
The masticatory system is made up of following components-
•morphologic•Functional •Behavioral
•When natural teeth are replaced by artificial teeth ,interaction among these are affected
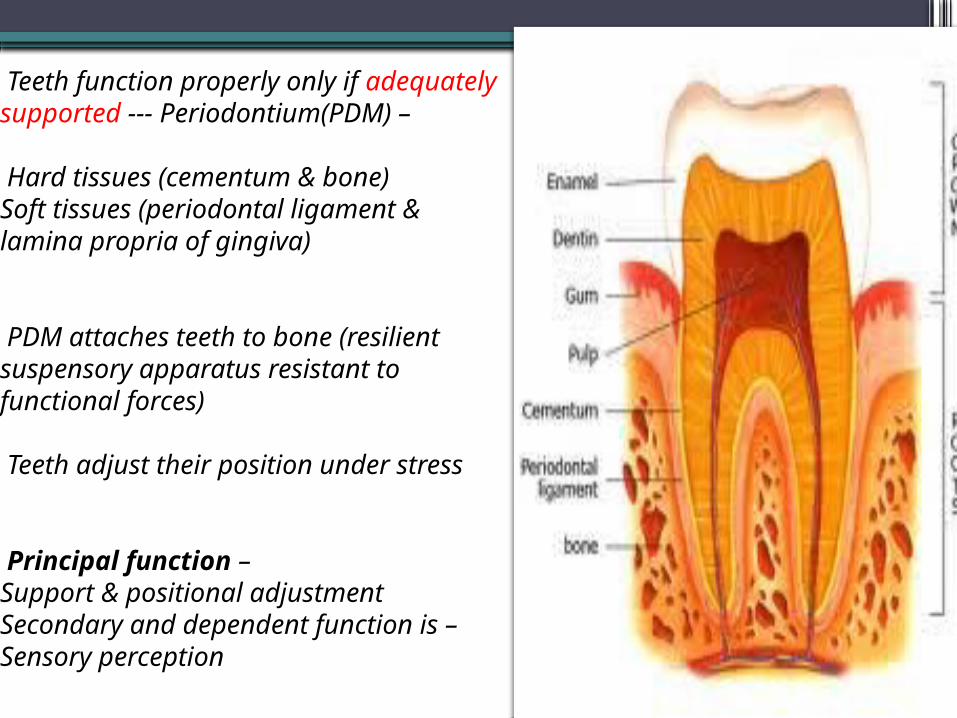
Teeth function properly only if adequately supported --- Periodontium(PDM) –
Hard tissues (cementum & bone)Soft tissues (periodontal ligament & lamina propria of gingiva)
PDM attaches teeth to bone (resilient suspensory apparatus resistant to functional forces)
Teeth adjust their position under stress
Principal function – Support & positional adjustmentSecondary and dependent function is –Sensory perception
•Occlusal forces exerted are controlled by neuromuscular mechanisms of masticatory system
•Reflex mechanisms with receptors in muscles, tendons, joints & periodontal structures --- regulate mandibular movements
•Greatest force produced – mastication & deglutition, short & vertical in direction
•Tongue & circumoral musculature – longer duration & horizontal in direction
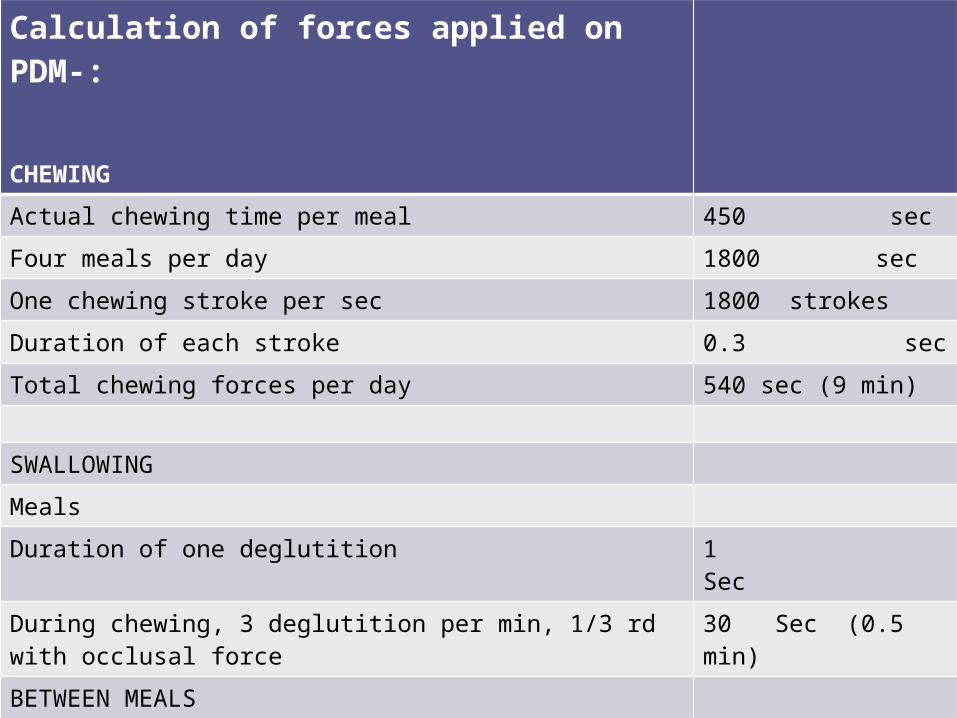
Calculation of forces applied on PDM-:
CHEWING
Actual chewing time per meal 450 sec
Four meals per day 1800 sec
One chewing stroke per sec 1800 strokes
Duration of each stroke 0.3 sec
Total chewing forces per day 540 sec (9 min)
SWALLOWING
Meals
Duration of one deglutition 1 Sec
During chewing, 3 deglutition per min, 1/3 rd with occlusal force
30 Sec (0.5 min)
BETWEEN MEALS
Daytime 25 / hr (16 hr) 400 sec (6.6 min)
Sleep : 10 / hr (8 hr) 80 sec (1.3 min)
TOTAL 1050 sec = 17.5 min
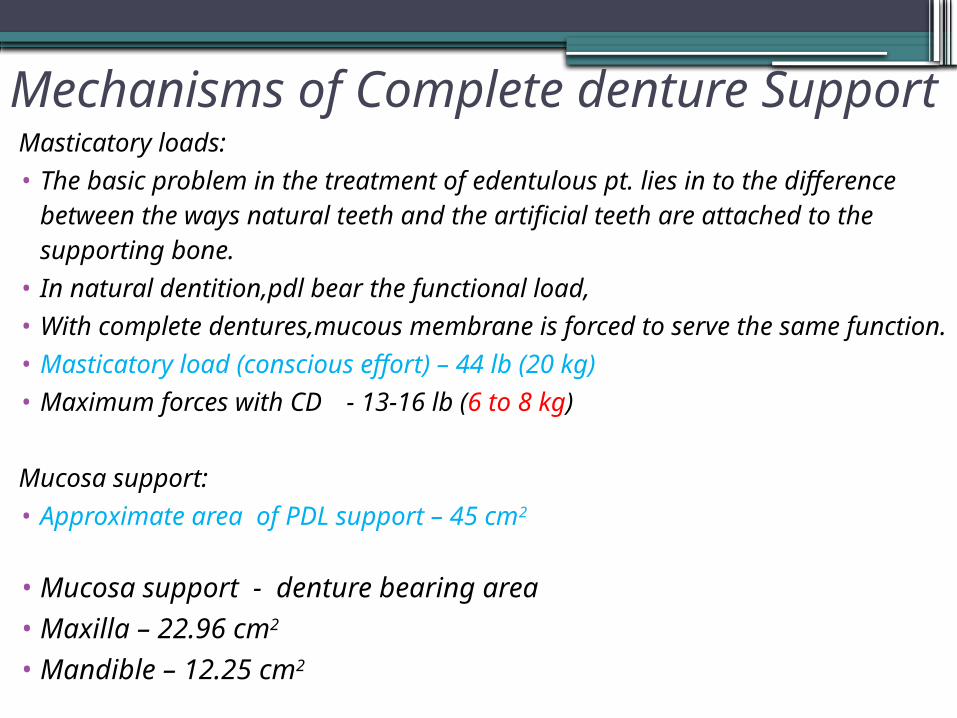
Mechanisms of Complete denture SupportMasticatory loads:• The basic problem in the treatment of edentulous pt. lies in
to the difference between the ways natural teeth and the artificial teeth are attached to the supporting bone.
• In natural dentition,pdl bear the functional load,• With complete dentures,mucous membrane is forced to
serve the same function.• Masticatory load (conscious effort) – 44 lb (20 kg)• Maximum forces with CD - 13-16 lb (6 to 8 kg)
Mucosa support:• Approximate area of PDL support – 45 cm2
• Mucosa support - denture bearing area• Maxilla – 22.96 cm2
• Mandible – 12.25 cm2
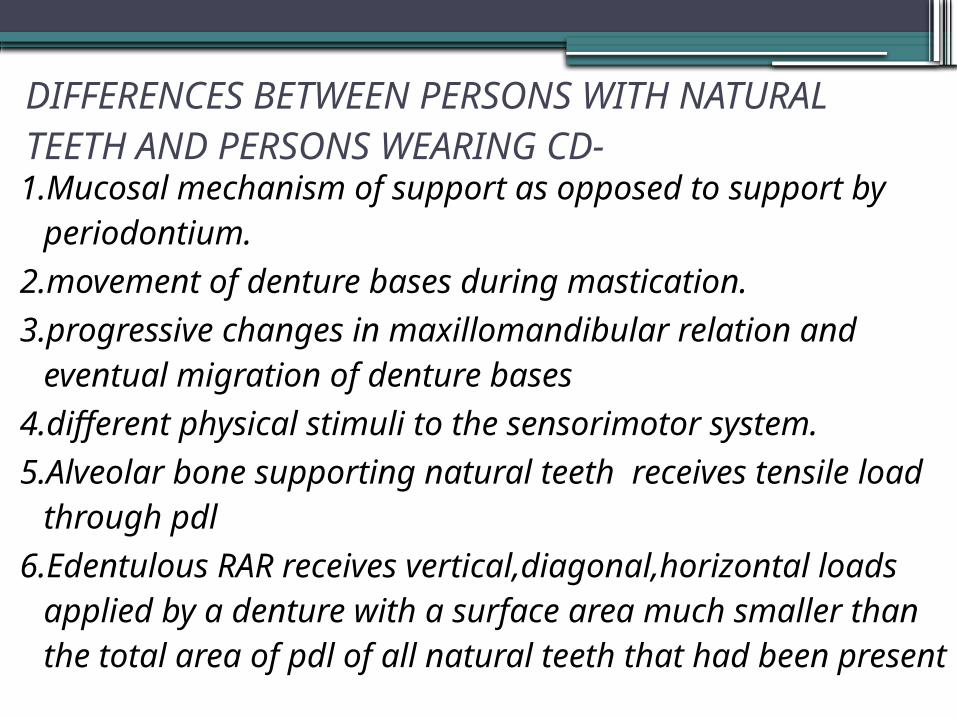
DIFFERENCES BETWEEN PERSONS WITH NATURAL TEETH AND PERSONS WEARING CD-1.Mucosal mechanism of support as opposed to support
by periodontium.2.movement of denture bases during mastication.3.progressive changes in maxillomandibular relation
and eventual migration of denture bases4.different physical stimuli to the sensorimotor system.5.Alveolar bone supporting natural teeth receives
tensile load through pdl6.Edentulous RAR receives vertical,diagonal,horizontal
loads applied by a denture with a surface area much smaller than the total area of pdl of all natural teeth that had been present
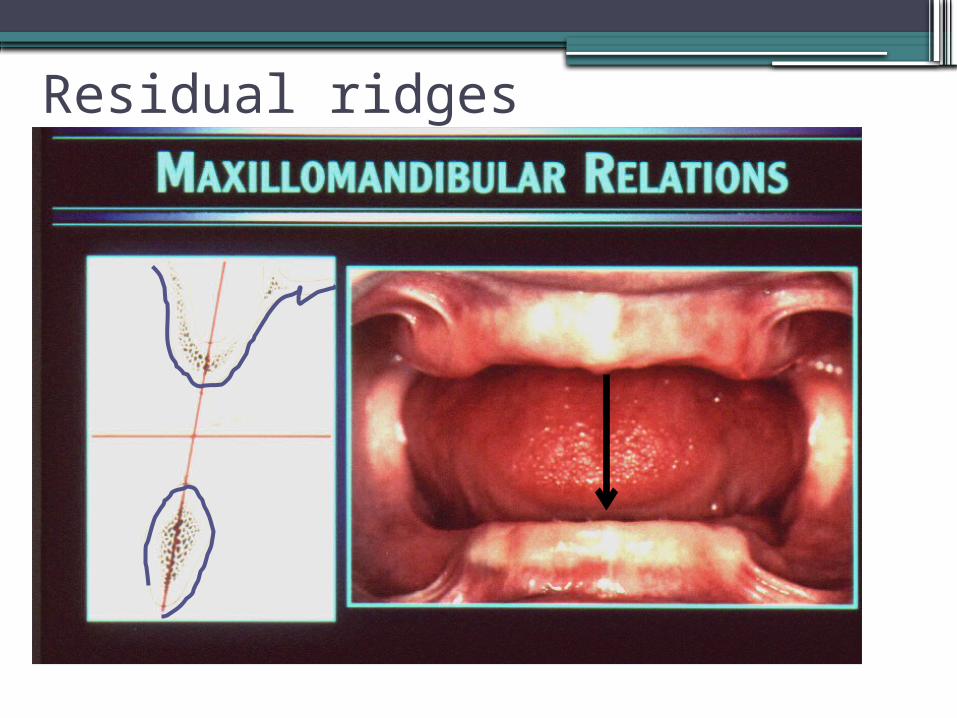
Residual ridges
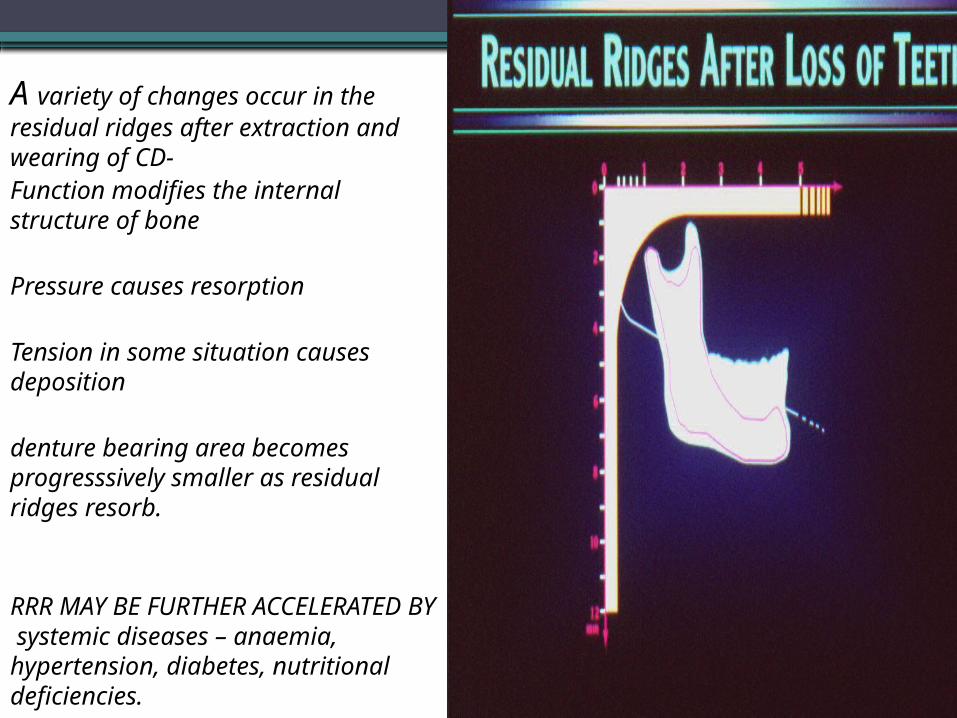
A variety of changes occur in the residual ridges after extraction and wearing of CD-Function modifies the internal structure of bone
Pressure causes resorption
Tension in some situation causes deposition
denture bearing area becomes progresssively smaller as residual ridges resorb.
RRR MAY BE FURTHER ACCELERATED BY systemic diseases – anaemia, hypertension, diabetes, nutritional deficiencies.
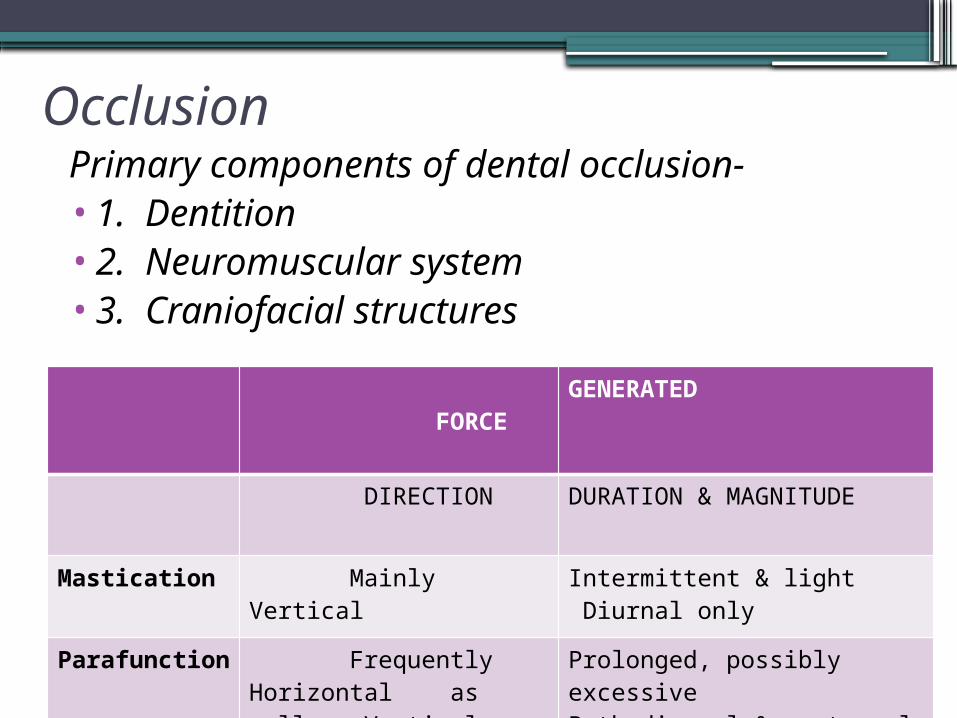
OcclusionPrimary components of dental occlusion-•1. Dentition•2. Neuromuscular system•3. Craniofacial structures
FORCE
GENERATED
DIRECTION DURATION & MAGNITUDE
Mastication Mainly Vertical Intermittent & light Diurnal only
Parafunction
Frequently Horizontal as well as Vertical
Prolonged, possibly excessiveBoth diurnal & nocturnal
CD ARE SO DESIGNED THAT THEIR OCCLUSAL SURFACES PERMIT BOTH FUNCTIONAL AND PARAFUNCTIONAL MOVEMENTS OF MANDIBLE.
Orofacial and tongue muscles play an important role in retaining and stabilizing CD.This is accomplished by arrangement of teeth in neutral zone where there is functional balance of orofacial and tongue musculature.
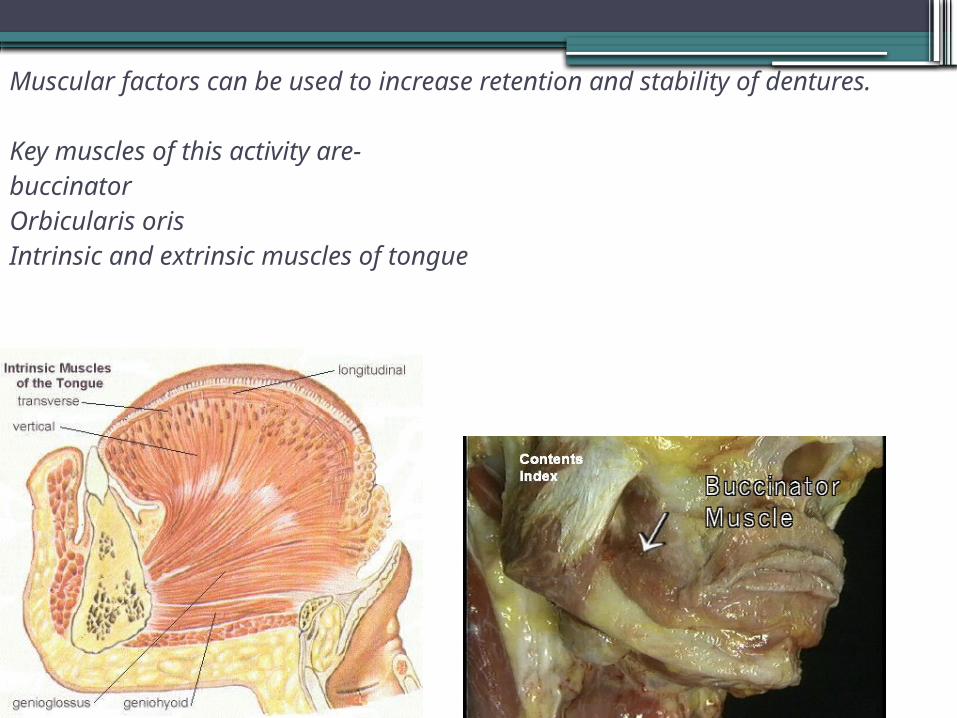
Muscular factors can be used to increase retention and stability of dentures.
Key muscles of this activity are-buccinatorOrbicularis orisIntrinsic and extrinsic muscles of tongue
Parafunction-
• The initial discomfort associated with new denture is known to evoke unusual pattern of behaviour in the surrounding musculature.
• Habit of thrusting tongue against-sore tongue• EMG-strong response of lower lip and mentalis
in long term denture wearers with impaired retention and stability of lower denture.
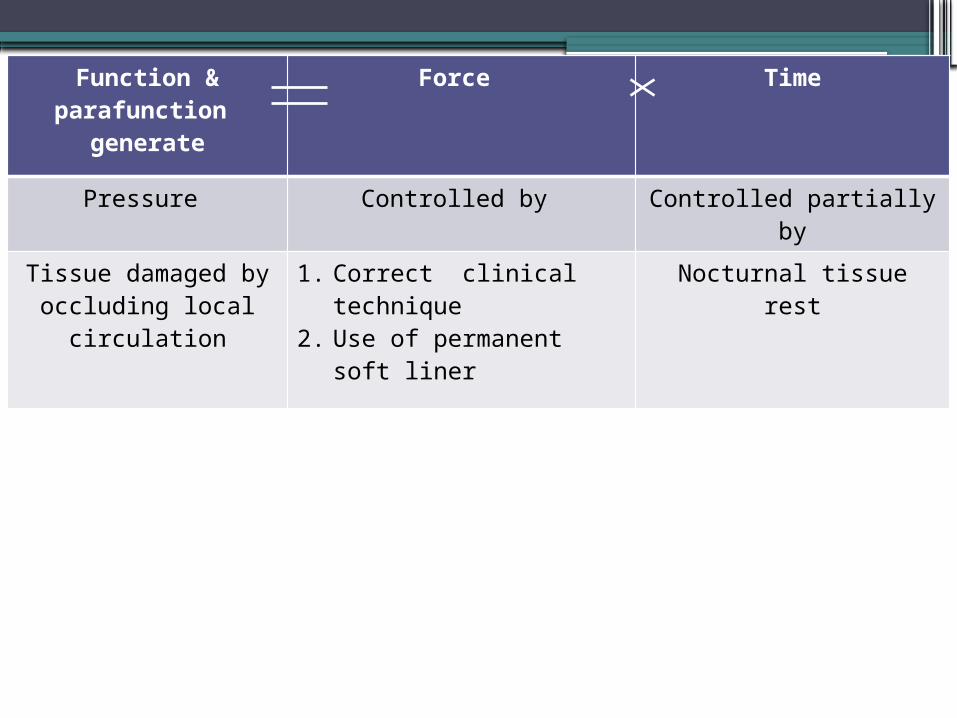
Function & parafunction
generate
Force Time
Pressure Controlled by Controlled partially by
Tissue damaged by occluding local
circulation
1. Correct clinical technique
2. Use of permanent soft liner
Nocturnal tissue rest
Distribution of Stress• Denture supporting tissues-viscoelastic.• On application of load-Initially elastic compression of tissues Delayed elastic deformation of tissue {slow and
continues to diminish in rate as duration of load is extended}
• On removal of load-Elastic decompressionContinuing delayed elastic recovery
4 hours to recover after moderate loading of 10 minutes.
Longer period for recovery of displaced mucosa is required in elderly people[68-70 yrs] than in young[21-27 yrs]
Mucosal health can be promoted•Hygienic measures•Therapeutic measures•Tissue-conditioning techniques
OCCLUSAL LOAD can be reduced by•Maximum extension•Reduction of area of occlusal table•Frequent rest periods (8 hours)
Factors affecting retention that are under control of dentist:
• Maximal extension of denture base
• Maximal area of contact between mucous membrane and denture base
• intimate contact of denture base & its basal seat
• ALMOST ALL ‘PRINCIPLES’ OF CD CONSTRUCTION HAVE BEEN FORMULATED TO MINIMIZE THE FORCES TRANSMITTED TO SUPPORTING STRUCTURES OR TO DECREASE THE MOVEMENT OF THE PROSTHESIS IN RELATION TO THEM.
.
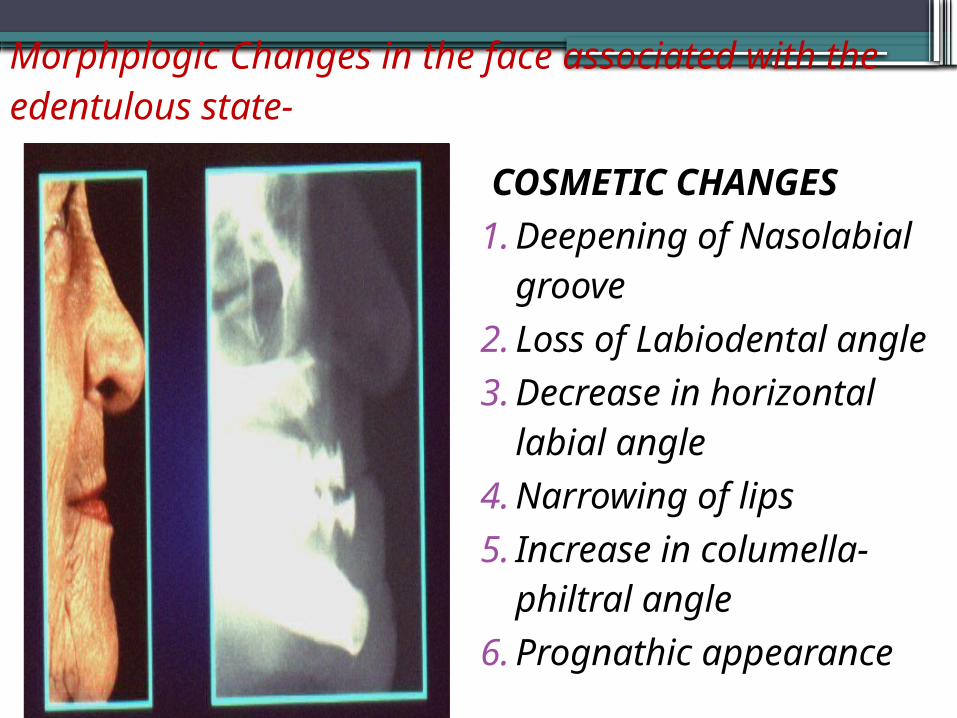
Morphplogic Changes in the face associated with the edentulous state-
COSMETIC CHANGES1.Deepening of
Nasolabial groove2.Loss of Labiodental
angle3.Decrease in horizontal
labial angle4.Narrowing of lips5.Increase in columella-
philtral angle6.Prognathic
appearance
Individual behavioural responses -
• Early communication about a patient’s cosmetic expectations should be established to avoid later misunderstanding
• Photographs of their predentulous appearance• Careful explanation of prosthodontic objectives
and methods is the basis for good communication with pt.
Adaptive & psychological responses
• CD – requires adaptation of learning, muscular skill & motivation
• Patient’s ability & willingness to accept & learn to use dentures ---- success
• Also – Habituation – gradual diminution of responses to continued or repeated stimuli
• In old age – Memory & Storage is difficult, so adaptation to CD becomes difficult (as progressive atrophy of elements in cerebral cortex & consequent loss in facility of coordination occurs)
• So Dentist’s role is to MOTIVATE the patients & make understand their NEEDS has proven to be of greatest clinical value

Adaptation problems that may be encountered by PT previously wearing CD opposing a few natural anterior mandibular teeth:
•MAY FIND CD Difficult to adapt,altered size and orientation of tongue.
•insertion of new denture-new environment for the tongue,
•intrinsic muscle reorganizes shape of tongue to conform to altered space available.
•Retraining of tongue
•posterior RR are now exposed to new sensation from overlying denture
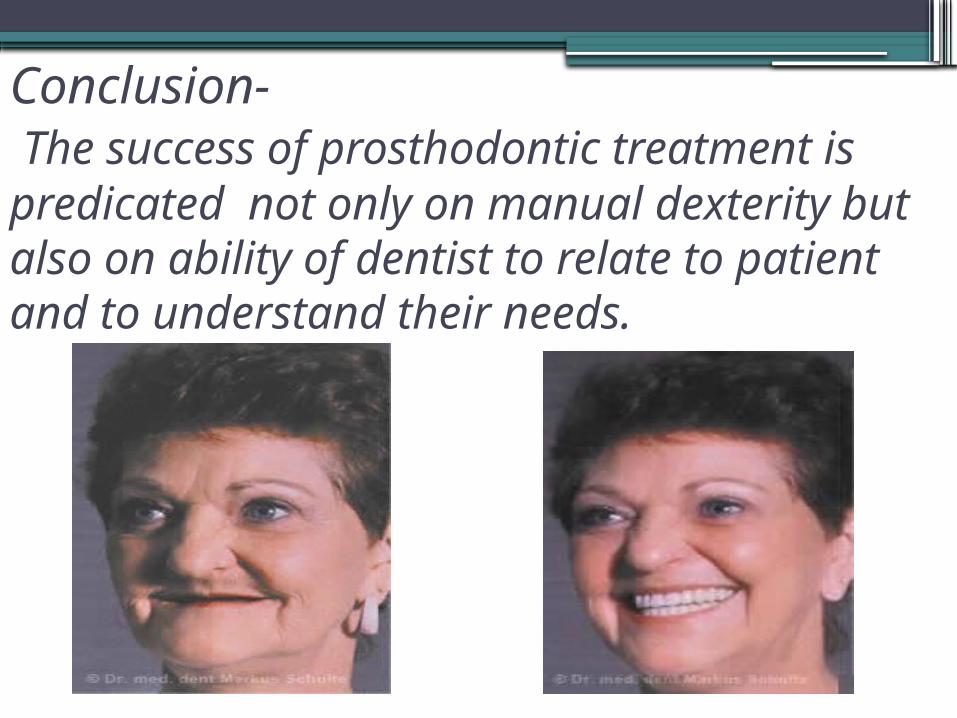
Conclusion- The success of prosthodontic treatment is predicated not only on manual dexterity but also on ability of dentist to relate to patient and to understand their needs.
Index- prosthodontic treatment of edentulous patient,boucher Complete dentures,hugh delvin

Thank you…