bhatia tardive syndromes aam - ucl discovery
TRANSCRIPT
TardiveSyndromes
EoinMulroy1,BettinaBalint1,2,KailashPBhatia11DepartmentofClinicalandMovementNeurosciences,UCLQueenSquare
InstituteofNeurology,LondonWC1N,3BG2DepartmentofNeurology,UniversityHospital,Heidelberg,Germany
CorrespondingAuthor:
EoinMulroy
DepartmentofClinicalandMovementNeurosciences,UCLQueenSquare
InstituteofNeurology,LondonWC1N3BG
Phone:02034567890
Wordcount:4141
Abstract
Dopaminereceptorblockingantipsychotics,firstintroducedtoclinicalpractice
in1952,werehailedasapanaceainthetreatmentofanumberofpsychiatric
disorders.Within5yearshowever,thisnotionwastobeshatteredbythe
recognitionofbothacuteandchronicdrug-inducedmovementdisorderswhich
canaccompanytheiradministration.Tardivesyndromes,denotingthedelayed
onsetofmovementdisordersfollowingadministrationofdopaminereceptor
blocking(andalsoother)drugs,comprisediversemanifestationsrangingfrom
theclassicoro-bucco-lingualdyskinesia,throughdystoniccraniocervicaland
trunkposturingtoabnormalbreathingpatterns.
Despitehavingbeenanimportantpartofclinicalmovementdisorderpracticefor
over60years,thepathophysiologicbasisoftardivesyndromesremainspoorly
understoodandtheoptimaltreatmentapproachremainsunclear.Thisreview
summarisesthecurrentstateofknowledgerelatingtotardivesyndromes,and
providesclinicianswithpragmatic,clinicallyfocusedguidancewithwhichto
tacklethedisorder.
Introduction
Movementdisordersoccurringasadirectiatrogenicconsequenceofthe
administrationofdopaminereceptorblockingneurolepticdrugswerefirst
reportedin1957,fiveyearsaftertheirintroductionintopsychiatricpractice.The
year1964sawtheirfirstcollectivedescriptionasa‘tardive’(drawnfromthe
latintardus,meaninglate)phenomenon[1],reflectingtheirdelayedonset
followingmedicationadministration,incontrastto‘acute’dystonicreactions,
whichcanalsooccurfollowingdopaminergicblockade.Thistermwasrapidly
adopted,andinthefollowingdecades,aflurryofpublicationsweretoexpand
thephenotypicspectrumofthedisorder.Concurrently,theoriesaimingto
explaindiseasepathogenesisbegantoemerge,andanumberoftherapeutic
strategieswereexplored.Thisreviewprovidesphysicianswithapragmatic,
clinically-basedplatformwithwhichtoapproachtardivesyndromes.Inaddition,
weexploresomerecentdevelopmentsinourunderstandingofdisease
pathophysiology,discusshowtoapproachtreatmentoftardivesyndromesand
trytodispelsomecommonlyheldmythsalongtheway.
Anecessarypreambletothisreviewisabriefforayintonosology.Indeed,
tardivesyndromes(TS)areplaguedbyinconsistentuseofdescriptivelanguage.
Theterm‘Tardivedyskinesia’,whenfirstintroduced,wasintendedtosubsume
therangeofdiversemovementswhichcanemergeinadelayedfashionfollowing
long-termneurolepticadministration.However,morerecently,alessconfusing
approachwhichclassifiestardivemovementsaccordingtotheirindividual
clinicalphenomenologies,hasbeenpromoted,andwillbeusedinthisreview.
Accordingly,‘Tardivesyndrome’isemployedastheumbrellatermforany/all
potentialtardivemovementdisorders.Meanwhile,‘Tardivedyskinesia’is
reservedasadescriptorofaspecificclinicalentity,namelythatofthe
characteristicoro-bucco-lingualchoreiformmovements(seebelow).
Thescaleoftheproblem
Tardivesyndromes(TS)areapredictable,sometimespermanent,disabling
consequenceofmedicationadministration.Theyarepredominantlyencountered
inthepsychiatricpopulation,wheretheyexacerbatetheburdenofsocialstigma
andarelinkedtopoorerqualityoflifeandincreasedmorbidityand
mortality[2,3].Antipsychoticsarebyfarthemostcommonoffenders,though
numerousotherdrugshavealsobeenimplicated(table1).
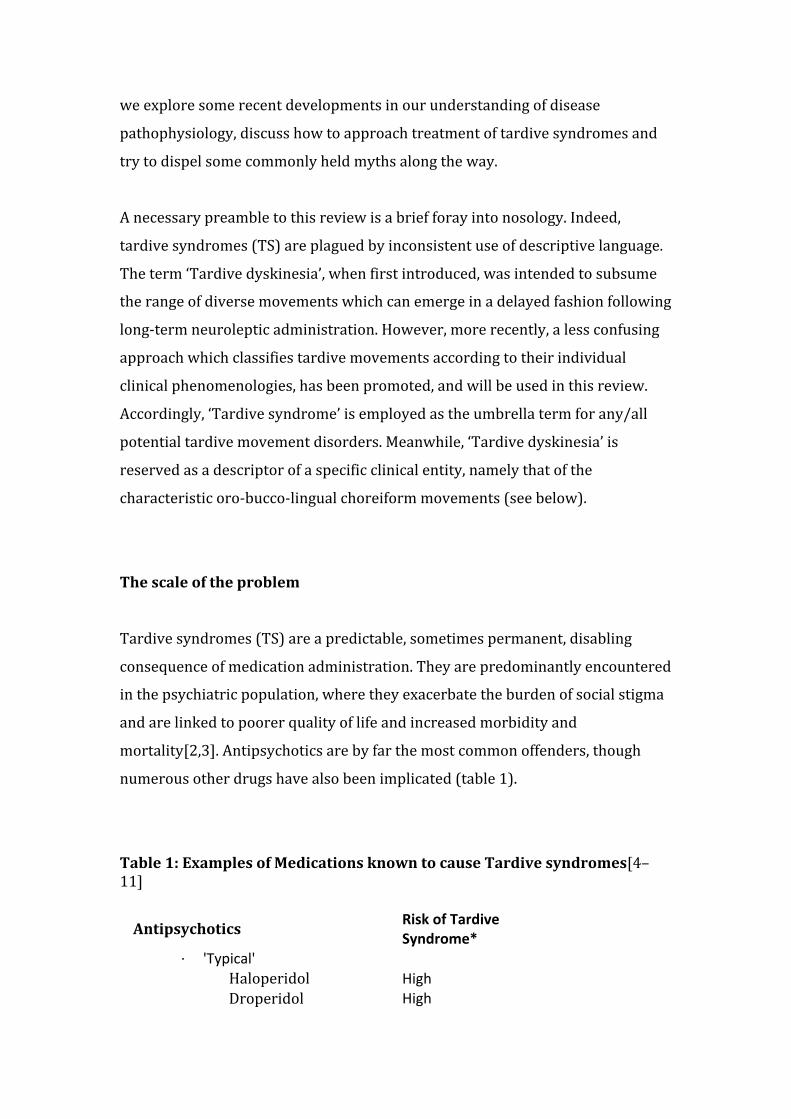
Table1:ExamplesofMedicationsknowntocauseTardivesyndromes[4–11]
Antipsychotics
Risk of Tardive Syndrome*
· 'Typical' Haloperidol High Droperidol High
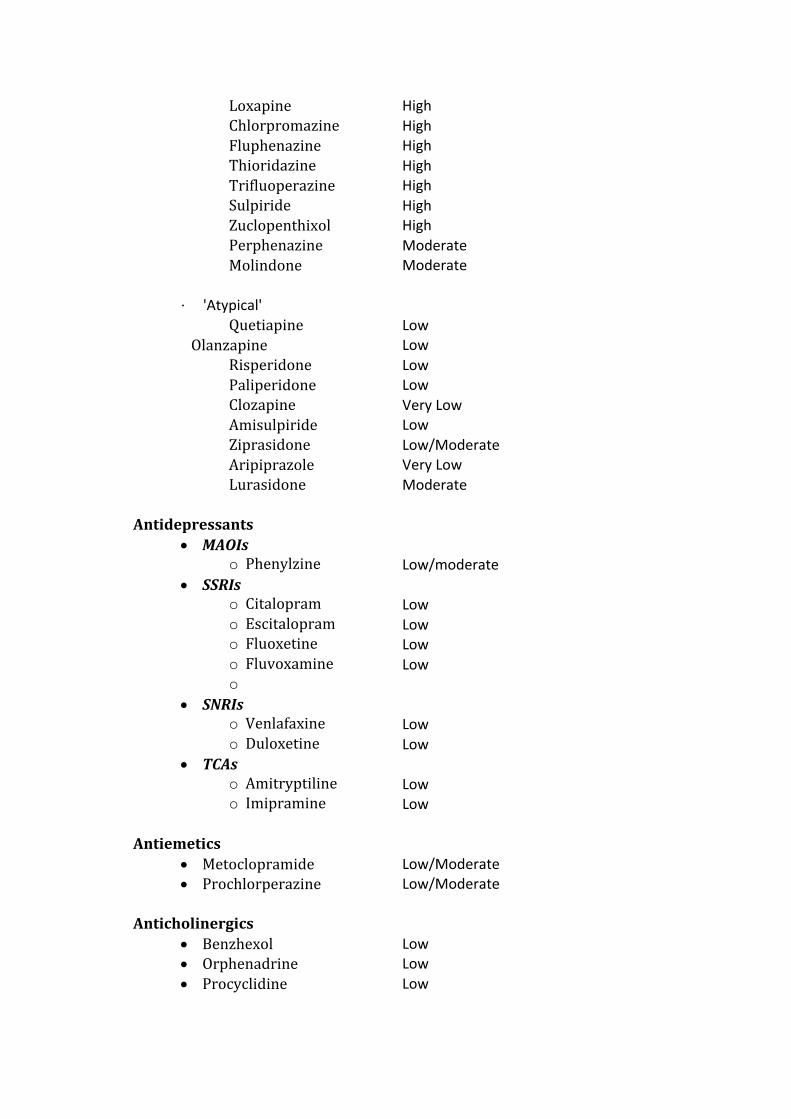
Loxapine High Chlorpromazine High Fluphenazine High Thioridazine High Trifluoperazine High Sulpiride High Zuclopenthixol High Perphenazine Moderate Molindone Moderate
· 'Atypical' Quetiapine Low
Olanzapine Low Risperidone Low Paliperidone Low Clozapine Very Low Amisulpiride Low Ziprasidone Low/Moderate Aripiprazole Very Low Lurasidone Moderate
Antidepressants • MAOIs
o Phenylzine Low/moderate • SSRIs
o Citalopram Low o Escitalopram Low o Fluoxetine Low o Fluvoxamine Low o
• SNRIs o Venlafaxine Low o Duloxetine Low
• TCAs o Amitryptiline Low o Imipramine Low
Antiemetics • Metoclopramide Low/Moderate • Prochlorperazine Low/Moderate
Anticholinergics • Benzhexol Low • Orphenadrine Low • Procyclidine Low
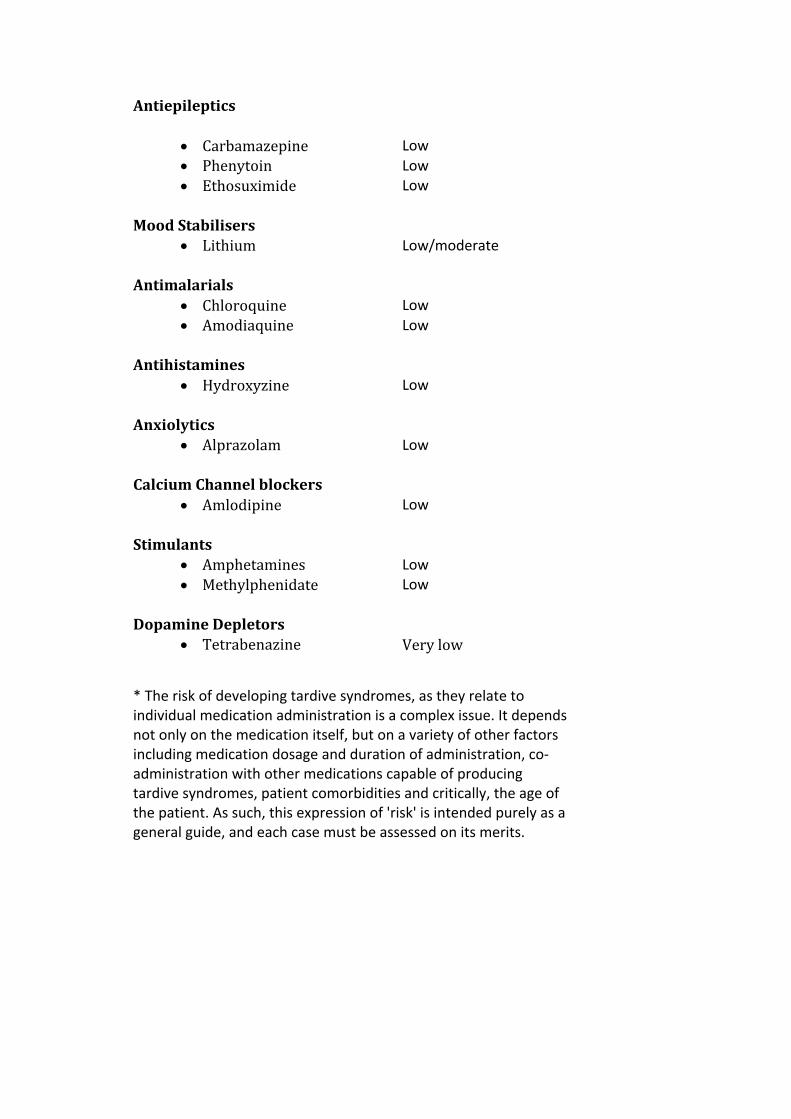
Antiepileptics • Carbamazepine Low • Phenytoin Low • Ethosuximide Low
MoodStabilisers
• Lithium Low/moderate
Antimalarials
• Chloroquine Low • Amodiaquine Low
Antihistamines • Hydroxyzine Low
Anxiolytics
• Alprazolam Low
CalciumChannelblockers
• Amlodipine Low
Stimulants • Amphetamines Low • Methylphenidate Low
DopamineDepletors • Tetrabenazine Verylow
* The risk of developing tardive syndromes, as they relate to individual medication administration is a complex issue. It depends not only on the medication itself, but on a variety of other factors including medication dosage and duration of administration, co-administration with other medications capable of producing tardive syndromes, patient comorbidities and critically, the age of the patient. As such, this expression of 'risk' is intended purely as a general guide, and each case must be assessed on its merits.
Theconditionaffectsbetween20-50%ofpatientsreceivingneuroleptic
drugs[12].Advancingageisthemostrobustrisk-factorforthedevelopmentof
TS,withyearlyincidenceratesincreasingfrom5%inthoseunder40yearsof
ageto12%orhigherinolderagegroups[12–14].Riskincreasescumulatively
withdurationofexposureandcumulativedose,culminatinginanincidenceof
20-25%after5yearsofexposure[15,16].[17].Thesestatisticsmustalsobe
interpretedintheknowledgethatmedicationcomplianceratesamongthe
schizophrenicpopulationarearound50%,sothesefiguresmaywellbean
underestimate[18].
Numerousotherfactorsmayincreaseone’sriskfurther,includinghistoryofan
affectivedisorder,previousorganicbraindamage,diabetesmellitus,femalesex
(oestrogenperhapsbeingprotectivepre-menopausally)andrace[19].Indeed,
Asianshaveonaveragehavelower(roughly20%)andAfricanAmericanson
averagehigherdiseaseprevalenceascomparedtoCaucasians[19–21].
DiseasePathophysiology
Thepathophysiologicbasisoftardivesyndromesremainspoorlyunderstood.
Thisuncertaintyisreflectedinthegreatnumberoftheorieswhichpurportto
explainthedelayeddevelopmentofthesemovementdisorders.
Theearliesttheorytogainpopularacceptancewastheso-calleddopamine
receptorhypersensitivitytheory.Thissuggestedthatadministrationof
dopamineblockingneurolepticsledtocompensatoryup-regulationand/or
hypersensitivityofpost-synapticdopamine(particularlyD2)receptors[22,23].
Hypersensitivityofthesereceptors,whichareexpressedonindirectpathway
mediumspinyneuronsandareinhibitory,wouldhavetheneteffectofpallidal
andsubthalamicnucleusdis-inhibition,producingabnormalhyperkinetic
movements[22].Thishypothesiswaslargelybasedonclinicalobservations,such
asthegreaterlikelihoodofTSinpatientsreceivingpotentD2blockersandthe
apparentimprovementintardivedyskinesiawithadditionaldopaminergic
blockade,aswellasonsomeanimalstudies[22,23].However,evidencein
humansforsuchalterationsislacking.Thereisnocorrelationbetweenin-vivo
striatalD2receptorligandbindingassessedbyPETandTDseverity.Equally,
post-mortemstudieshavenotdemonstratedsignificantdifferencesinD2
receptornumbersinthosewithandwithoutTS[22].Moreover,thistheoryfails
toexplainwhymanypatientsfailtorecoverfollowingcessationoftheoffending
medication-iftheonlyproblemwasreceptorup-regulation/hypersensitivity,
onewouldexpectthistonormalizefollowingdrugwithdrawal.
AnalternativehypothesisisthatTSactuallyrepresentsaneurodegenerative
disorderofstriatalinterneuronsinducedbyoxidativestress.Thistheory,which
issupportedsomewhatbyanimalandhumanneuropathologicalstudies[24,25],
holdsthatdopaminergicreceptorblockadecausesincreaseddopamineturnover
andoxygenfreeradicalproductionbymonoamineoxidase[22].Thesefree
radicalsarethoughttobetoxictostriatalinterneurons,causinggliosiswithinthe
basalganglia,explainingthepersistenceofsymptomsaftermedication
discontinuation.Thesignificantandsustainedimprovementsometimes
observedfollowingdeepbrainstimulationforTSmayarguesomewhatagainst
thisideahowever.
AfurthertheoryimplicatesdamagedordysfunctionalstriatalGABAergic
neuronsinthepathogenesisofTD.Theseneuronssynapseonthesomaof
mediumspinyneurons,providingpotentfeedforwardinhibition,balancing
activityinthedirectandindirectbasalgangliapathwaysandprovidingsurround
inhibition[22,23].Selectivelesioningoftheseneuronshasbeenshownto
producedyskinesia[26].Long-termD2agonism,intheory,hasthepotentialto
damageGABAergicinterneuronsviaglutamate-mediatedexcitotoxicityand
increasedoxidativestressfromdopamineturnover[27].
Finally,alteredNMDA-mediatedsynapticplasticityhasbeensuggestedasa
somewhatunifyingtheory.AntipsychoticsareknowntoinfluenceNMDA
receptormediatedsynapticplasticity.Inthissetting,patternsofabnormal
neurotransmissione.g.secondarytoD2receptorhypersensitisationcouldbe
abnormallypotentiated,perpetuatingacycleofabnormalsensorimotor
integrationandabnormaltardivemovements[22].
Ofcourse,noteveryonewhoisexposedtoneurolepticdrugswilldevelopa
tardivesyndrome,implyingthatother,possiblygeneticfactorsareatplay,
conferringincreasedvulnerabilitytoTS.Genomewideassociationstudieshave
identifiedsomepotentialcandidategenes,thoughtheirrelevancetoclinical
practiceremainstobedetermined[28].
Makingthediagnosis-thedevilisinthedetail
Thefollowingsectiondescribesboththetypical(orperhapssimplybetter
recognized!)andlesstypicalpresentationsofTS.Onemustbemindfulhowever
thatindividualcomponentsofthesyndromerarelyoccurinisolation.Rather,
theygenerallycoexisttogreaterorlesserdegrees(thoughonemaybe
dominant),anditisoftentheidentificationofmultiplemovement
phenomenologiescompatiblewithTSwhichallowsaconfidentdiagnosistobe
made.Avitalpartoftheevaluationisthereforenotonlyidentificationofa
movementwhichispotentiallytardiveinaetiology,butactivelysearchingforthe
presenceofothercompatibleabnormalities.Failingnoticecluessuchasafidgety
patient(akathisia)whosighsdeeply(respiratorydyskinesia)andmoveshislegs
backandforthduringtheconsultation(stereotypies),canrapidlyleadonedown
thewrongdiagnosticpath.
ThoughdiagnosticcriteriaforTShavebeendeveloped(table2),inclinical
practice,therearereallyonlytwoquestionswhichmatter:
1. Isthereahistoryofdopaminereceptorblocking(orotherTS-causing)
drugadministration(eitherprescriptionmedication,overthe
counter/traditionalremedies,orpoisoning),andwhatisthetemporal
relationshipofthistotheonsetofthemovementdisorder?
2. Istheclinicalphenomenologycompatiblewithatardivesyndrome(see
below)?
Table2:DiagnosticandStatisticalManualofMentalDisorders,fifthedition
(DSM-5)definitionoftardivesyndromes
Tardivesyndromesaremovementdisordersdistinguishedbytheirlate
emergenceinthecourseoftreatmentandtheirpotentialpersistenceformonths
toyears,eveninthefaceofneurolepticdiscontinuationordosagereduction.
Symptomsdevelopinassociationwiththeuseofaneurolepticmedicationforat
leastafewmonths.
Symptomsmaydevelopafterashorterperiodofmedicationuseinolder
persons.
The‘typical’tardivesyndrome
‘Classic’tardivedyskinesiainvolvesstereotypedchoreoathetoidmovements
predominantlyinvolvingthelips,tongueandperioralregion.Themovements
tendtopredominateinthelowerface,withfrontalisinvolvementbeingunusual.
Patientsoftenmovethetongueinawrithingmotioninsidethemouth,areprone
tofrequentrapidtongueprotrusion(‘flycatchertongue’),andpushingofthe
tongueagainsttheinsideofthecheek,creatingabulge(‘bonbonsign’).Chewing
and/orgrimacingmovements,lipsmackingandpuckeringaretypical.Thismay
beaccompaniedbylowamplitudechoreiformmovementsofthedistallimbs,the
so-called‘pianoplayer’dyskinesia,duetotheirresemblancetofinger
movementsonpianokeys[29].Patientsareoftenunawareoftheseinvoluntary
movements,thoughthoseinvolvingthelipsandtonguemaycauseproblems
withfeeding.
Tardivedyskinesiaisusuallyaccompaniedbyoneormoreofthefollowing
tardivephenomena:
-Tardiveakathisia,whichisanuncomfortablesenseofinnerrestlessness,
requiringtheaffectedindividualtorepeatedlymoveaboutinordertoeasethis
unpleasantsensation.Thiscanincluderockinginplacewhenseated,marching
whenstanding,repetitivescratchingorrubbingorindeedjustappearing
generally‘fidgety’duringtheconsultation.
-Tardivestereotypies:thesearepatterned,purposeless,repetitiveandsomewhat
ritualisticmovementswhichmayappearastruncalrocking,pelvicthrusting,to-
and-frolegmovements,handwringingorcrossing/uncrossingofthelegs.They
mayresembleakathisiabutincontrast,stereotypiesarenotaccompaniedby
innerrestlessness.
-Tardivedystonia:Aswithmosttardivesyndromes,tardivedystoniaadopts
distinctphenomenologicalcharacteristicswhichareeasilyidentifiedbythe
trainedobserver.Thedisorderfrequentlyinvolvesthecraniocervicalregion,
oftenmanifestingasretrocollis.Dystoniamayextendtothetrunk,as
opisthotonicposturing,whileinthearms,abduction,internalrotationandwrist
flexionistheclassicallyadoptedposture[29].Blepharospasmmayalsoemerge.
IncontrasttootherTS,tardivedystoniaappearsparticularlyprevalentinyoung
menaroundtheageof40years[24].Remissionisalsolesslikelythanwith
tardivedyskinesia,particularlywithdrugexposurebeyond10years[24].
Thefollowingtardivedisordersarelesswelldefined,withonlyahandfulof
casesreportedintheliterature.
-TardiveTourettismisararedisordercharacterizedbytheemergenceof
multiplemotorandverbalticsfollowingexposuretodopaminereceptor
blockingdrugs.Theticsaregenerallysimilartothoseofprimaryticdisorders,
exhibitingsuppressibility,buildupoftensionpriortotheticandreleaseof
tensionuponperformanceofsame[30,31].
-Tardivetremor
Theentityoftardivetremorwasfirstproposedina1992reportoffivepatients
witha3-5Hzposturalandactiongreaterthanresttremorwithoutcoexistent
parkinsonism[32].Thoughbearingsomesimilaritiestoparkinsoniantremor,
tardivetremorissaidtobedifferentiatedfromtheformerbyitsposturaland
kinetic(ratherthanrest)predominance,itscoarsedisablingnature,itslackof
responsivenesstolevodopaanditsoccasionalimprovementwithfurther
dopaminergicblockadeortetrabenazine[32,33].Thesyndromegenerally
persistsdespiteDRBAwithdrawal.
-Tardivemyoclonus
Tardivemyoclonusdescribesbrief,upper-limbpredominantposturalmyoclonic
movementswhicharesaidtobeaconsequenceoflong-termdopaminergic
blockade[34,35].Theliteratureonthisentityishighlylimitedhowever,and
thereforeshouldbeinterpretedwithcaution.
-ThephenomenonofTardiveGaithasalsobeendescribed.Thoughpoorly
characterizedandnotuniform,gaitdisturbanceshavebeendescribedas
‘dancing’(multipleshortstepsfollowedbyalongstep)or‘duck-like’(broad
basedwithshortstridelengthandsomesteppagefeatures).Otherabnormalities
includeinitialfloorcontactwithtoesratherthanheels,spasticqualitiesand
abnormalarmswing[36].
Somerather‘atypical’presentations
PatientswithTSnotinfrequentlyexhibitotherlessrecognized,butnonetheless
characteristicfeatureswhichpointtowardsthediagnosis.Amongthese,
respiratoryphenomena,tardivepisasyndromeandwithdrawalemergent
dyskinesiaareparticularlyimportanttobeawareof.
-Firstdescribedin1964,RespiratoryDyskinesiainvolvesperiodicdisturbancesof
respiratoryrate,rhythmandamplitude,sometimesaccompaniedbyrespiratory
pausesorforcedinspirationagainstaclosedglottis[37].Patientsmaycomplain
ofdyspnoea,dysphonia,ormaybeseentohuff,grunt,gasportakeshort,rapid
breaths[38].Theserespiratoryphenomenaoftenaccompanyothermoreclassic
tardivemotorfeatures.
-TardivePisasyndrome
Predominantlyaffectingolderwomen,tardivepisasyndromedescribesadrug-
inducedpersistenttruncaldystoniamanifestingastoniclateralflexion,
occasionallyaccompaniedbyslightrotation[39].The‘laterallyleaningpatient’is
animportantcluetoatardiveaetiology.
-Withdrawalemergentdyskinesiaisconsideredavariantoftardivedyskinesia
whichisgenerallyobservedfollowingeitherabruptdiscontinuationor
significantdosereductionsinneurolepticmedications[40].Thesyndrome
predominantlyaffectschildren,andusuallymanifestsasgeneralizedchorea(as
opposedtothefacial-predominantmovementsobservedinclassicTD).Itis
usuallyself-limitingafterdaystoweeks[40].
-Tardiveoculogyriccrises
Originallydescribedasacharacteristicfeatureofencephalitislethargicaand
nowmorecommonlyassociatedwithmedication-relatedacutedystonic
reactions(aswellasdopaminesynthesispathwaydefects),oculogyriccrisescan
rarelyoccurasatardivephenomenoninpatientschronicallyexposedto
antipsychoticmedications[41,42].Tardiveoculogyriccrisesoftenaccompany
othertardivemotorphenomenaandmaygounrecognized.Theyarenot
infrequentlyassociatedwithtransientrecurrencesofpsychiatricsymptoms
rangingfromanxiety,hallucinationsandbizarrebehaviortoauditory
hallucinations[41].
-Avarietyoftardivepainsyndromeshavealsobeendescribed,temporally
associatedwithneurolepticuseandoftenrespondingtostandardTStreatments.
Examplesincludetardiveoralpain,whichdescribesanuncomfortable,often
burningsensationinthemouthandlips,andpainfulgenitalsyndrome,with
similarafflictionofthegenitalregion[43].
-Tardivebruxism
Bruxism,ofeitherthegrindingormixedgrinding-clenchingtypehasbeen
describedasaside-effectoflong-termneurolepticexposure.Itlikelyrepresents
aformefrusteoftardiveoromandibulardystonia[44].Noiseproductionisoften
astrikingfeatureofthesyndrome,attimessosevereastoannoyroommates.
Themovementsdisappearduringsleep.
AssessingTSseverity
Priortoinitiatingapatientondopaminereceptorblockingdrugs,clinicians
shouldstrivetodocumentthepresenceofabsenceofabnormalinvoluntary
movements.Whilebothphysicianandnurse-ledstandardizedassessmenttools
(suchastheabnormalinvoluntarymovementscale(AIMS)andScanmove
instrument,respectively)maynotalwaysbepracticalinthebusyclinical
setting[45,46],afocusedexaminationisneverthelessimportant.Itwas
recognizedover140yearsagothatpsychiatricpatientsmayexhibitstereotypies,
choreaorabnormalfacialgrimacingasaresultoftheirdisease-failureto
documentthispriortotreatmentmayleadtotheselaterbeingmis-attributedto
adrugeffect[47,48].
Therehavealsobeenpublicationssuggestingthatacertainnumberofolder
peopledevelopspontaneousmovementsofthefaceaspartofnormalageing.
Whetherthisistrueormerelyrepresentstheemergenceoffacialorcranio-
cervicaldystonicsyndromeswithageisyettoberesolved.
Factsandfallacies
Mythno.1:Secondgenerationantipsychotics,withtheirlowerD2binding
affinity,havereducedtheincidenceoftardivesyndromes
Thishasbeenaparticularlycontentiousissueandmakingadefinitestatementin
eitherdirectionisdifficult.Whatcanbesaidwithcertaintyisthatthe
introductionofsecond-generationantipsychoticshasnotdoneawaywithTS.
Rather,duetorapiduptakeintheirprescription,includingoff-labeluseformood
disordersandsleep,theymayironicallyhavecontributedfurthertotheproblem.
WhilesomestudiessuggestthattheincidenceofTSwithsecondgeneration
antipsychoticsisnotvastlydissimilarfromthatoftheirfirstgeneration
counterparts[10,49],thelargestliteraturereviewto-dateinvolving34,555
patientstreatedwithantipsychoticsacross56studiesfoundanannualized
incidencerateof2.98%withsecond-generationantipsychoticsversus7.7%with
first-generationantipsychotics,supportingtheclaimthatSGAmayindeedcarry
alowerrisk[50].Thisisalsosupportedbyarecentlargemeta-analysisof57
studiesonTS[9].
Mythno.2:Prolongedexposuretoacausativedrugisnecessaryinorderto
beatriskofTS.
Though,asdetailedabove,thecumulativeriskofTSincreasesyear-on-yearand
mostpatientsdevelopthedisorderafteratleast1-2yearsofdrug
exposure[23,24],therearereportsofitsoccurrenceafterjustasingledoseof
neuroleptic.Prolongeddrugexposureisthereforenotanecessarypre-requisite.
MythNo.3Someneurolepticsaresafe
Therecognitionthatfirstgeneration(‘typical’)antipsychoticswereassociated
withanumberofextrapyramidalside-effectspromptedthedevelopmentof
newercompounds,termed‘atypical’antipsychotics,whichweresupposedly
definedbytheabsenceofextrapyramidalsymptomsattherapeuticdoses.
Numerousmechanisticdifferencesofthesenewercompounds,includingeffects
onserotonergicsignaling,morerapiddissociationfromtheD2receptor,limbic
selectivity,andinthecaseofaripiprazole,partialdopaminergicagonismwere
positedasthereasonbehindtheirmorefavourablesideeffectprofiles.
Whileitistruethatnoteveryneuroleptichasthesamepropensitytocause
tardivesyndromes,nonearedevoidofrisk.Allclassesofantipsychoticscan
producetardivesyndromes[20,51].Nevertheless,newer‘atypical’agents
probablycarryabouthalftheriskofproducinglaterTSascomparedtotheir
‘typical’counterparts[9].Furthermore,itisimportanttorememberthatitisnot
justneurolepticswhichareimplicatedinthedevelopmentoftardivesyndromes
(table1).
Differentialdiagnosesnottomiss,andhowtospotthem:
Differentiatingspontaneousfromdrug-inducedmovementdisordersinpatients
withpsychiatricillnesscanbeachallengingendeavor.Itisnonetheless
imperativetoensurethatadequatethoughthasbeengiventoexcludeimportant
differentialdiagnoseswhichcanpresentwiththecombinationofpsychiatric
diseaseandabnormalmovements[29].Thefollowingconditionsareimportant
tokeepinmind:
1. Huntington’sdisease
Asatrinucleotiderepeatexpansiondisorderwiththecardinalmanifestationsof
chorea,psychiatricdiseaseandcognitivedecline,HDisoneofthemost
importantdifferentialdiagnosesoftardivedyskinesia.Psychiatricdisease(often
requiringneuroleptictreatment),canprecedethedevelopmentofhyperkinetic
movementsinHDbyanumberofyears.Theemergenceofthelattercan
thereforeeasilybemis-diagnosedastardivebytheinexperiencedobserver.
Inthissetting,someclinicalcluescanbeparticularlyhelpful[52].Theseinclude:
a. Thenatureofthehyperkineticmovements:hyperkineticmovements
intardivedyskinesiatendtobestereotypedandsemi-purposeful,as
opposedtotherandom,flowingmovementsofchoreawhichtypify
HD.
b. Topographicaldistribution:inTS,movementstendtopredominate
aroundthelowerfaceandaxially(manifestingasretrocollisand
opisthotonus).Incontrast,HDpatientsoftenhavesignificantlimb
chorea,whichisunusualinTS.Hyperkineticmovementsofthe
frontalismusclearealsocommoninHD,butuncommoninTS
c. Eyemovements:Eyemovementdisordersareoftenaprominent,early
featureofHD.Theycaninvolvedisordersofsaccadicinitiation,
brokenpursuitsandgazeimpersistence.Eyemovementsaregenerally
normalinTD,makingacarefuloculomotorexaminationanimportant
partoftheevaluationofalltardivesyndromes.
d. Motorimpersistence(ofgrip,tongueprotrusionorgazefixation)isa
classicfeatureofHD,butisveryuncommoninTD,andthereforea
valuableclinicalsign.
e. Otherfeaturesoftardivesyndromessuchasakathisiaand
opisthotonusarehighlysuggestiveofTS.Conversely,afamilyhistory
suggestingdominantinheritanceandcaudateatrophyonMRIwould
pointtoadiagnosisofHD.
2. Anti-NMDAreceptorencephalitis
Anumberofautoimmunemovementdisorderscanhaveco-existent
neurobehaviouralfeatures-theseareextensivelyreviewedelsewhere[53].
Anti-NMDAreceptorencephalitisinparticularhowever,couldbe
confusedwithtardivedyskinesia,duetotheprominentstereotyped
perioraldyskinesiawhichtypifiesthedisorder.Theconditionpresents
differentlydependingonage,withchildrenhavingmore‘neurological’
(seizures,movementdisorders)phenotypes,whileadultstendtopresent
withneurobehaviouralsyndromes,whichcanbemistakenfor
psychosis[54].Sometimes,theneuropsychiatricfeaturesrequire
neuroleptictreatment,creatinganadditionalpitfallinthediagnostic
pathway.A‘fullhouse’ofsymptoms,includingautonomicdysfunction,
generallydevelopswithin1month[54].Clinicalsuspicionshouldleadto
testingforthecausativeantibodyinserumandcerebrospinalfluid.
3. Wilson’sdiseaseshouldalwaysbekeptinthedifferentialdiagnosisofany
movementdisorder,especiallyinpatientsundertheageof40years
(thoughlatepresentationsarereported).Psychiatricsymptomsare
commoninWilson’sdisease,andperioralmovementsarealsoclassic.
However,theytendtoassumeamoredystonicquality,frequently
producingrisussardonicus.Dysarthriaanddroolingarealsocommonin
WD,butunusualintardivedyskinesia.
4. Edentulousdyskinesiaisahyperkineticmovementdisorderaffecting15%
oftheedentulouspopulation[55]inwhichstereotyped,choreiform
perioralandlipmovementsbearstrikingresemblancetothetardiveoro-
bucco-lingualdyskinesia.Thedisorderispresentunderconditionsof
partialorcompleteedentulism,andoftenresolvesorsignificantly
improveswiththeintroductionofdenturestothemouth.Itspathogenesis
isthoughttorelatetoalteredsensoryfeedbackfromoralstructuresasa
resultofmalocclusion.
5. Meigesyndromeisaprimarydystonicdisordermostlyaffectingwomenin
their50sand60s,characterizedbythecombinationofblepharospasm
andoromandibulardystonia.Differentiationfromtardiveconditionson
purelyclinicalgroundscanbeparticularlydifficult,henceahistoryof
exposuretodopaminereceptorblockingagentsiscriticaltothoroughly
exploreinthehistory.
Treatment
Managementoftardivesyndromesshouldincorporatethreekeyaspects.
First,preventionisalwaysbetterthancure.Assuch,medicationswith
documentedpotentialforinducingTSshouldbeusedatthelowestpossibledose
fortheshortestperiodoftimepossible.Thismayofcoursenotalwaysbe
possible.
Secondcomesthequestionofmedicationwithdrawal.Inactualfact,theevidence
thatwithdrawingtheoffendingdrugsignificantlyaltersthenaturalhistoryof
tardivesyndromesisnotasstrongasonemightthink[56].Nevertheless,thisis
anintuitivemoveinclinicalmedicine-removethethingwhichiscausingthe
problem.Mostmovementdisorderphysicianswouldthereforeadvocate
stoppingtheoffendingDRBA,oratleastchangingtoadrugwithlesspotential
fortardivephenomena,ifpossible.Thealternativedrugofchoiceinthissetting
isoftenclozapine,bothduetoitsprovenefficacyinthetreatmentof,andits
lowerriskofinducingTS[57–59].Closeconsultationwiththepsychiatric
servicesisnecessarypriortoembarkingonsuchacourseofaction.Itisalso
importanttorealizethattardivesymptomsmayinitiallyworsenfollowing
neurolepticdrugwithdrawal,andthatequallythesymptomsmaybesuppressed
byswitchingtoamorepotentdopaminereceptorblockingagent[60].
Finallycomesthequestionofsymptomatictreatmentsfortardivesyndromes.
Numerousagentshavebeentrialledinthisregard,withvaryingevidencefor
theireffectiveness.
Asmentionedbefore,TSareoftenacomplexmedleyofdifferentmovement
disorders,andapproacheswhichmaybeeffectiveforonemovementmay
worsenanother.Atailoredapproach,focusedonaddressingtheissuewhichis
primarilybothersomeforthepatientisthereforeparamount;generally,thiswill
beeithertardivedyskinesiaortardivedystonia.
Concerningtardivedyskinesia,themainstayofmedicaltreatmentresides
aroundtheadministrationofvesicularmonoaminetransporter-2(VMAT-2)
inhibitors(tetrabenazine,deutetrabenazine,valbenazine-thelattertwobeingthe
onlyFDAapproveddrugsforthetreatmentofTD),whichactthroughpre-
synapticdopaminedepletion.Themainsideeffectsofthesemedicationsarethe
developmentofreversibleparkinsonism,aswellasdose-dependentmood
changes,particularlyintheelderly;theside-effectprofilesofdeutetrabenazine
andvalbenazineappearsignificantlymorefavourable[61].
OthercompoundswhichareworthamentionincludeAmantadine,whichhas
shownantidyskineticpropertiesinmultiplecontrolledanduncontrolledstudies,
andissupportedbyAANguidelinesforshort-termtreatmentoftardive
dyskinesia.Propranololhassurprisinglygooddatatosupportitsuse,thoughthis
islikelyduetoitseffectofincreasingneurolepticdruglevels[47].Clonazepam
alsoappearseffective,thoughintherandomizedcontrolledtrialsettingit
appearedtoloseitsefficacyafter5-8monthsandthuscanonlybetentatively
recommendedforshort-termuse.Anumberofantioxidantshavealsobeen
trialled.Datasurroundingtheirefficacyislargelyinconclusive[60].Otheroptions
suchasadditionaldopaminergicblockadee.g.withhaloperidol,haveproven
efficacyinreducingtardivedyskinesia,atleastintheshort-term.Thishowever
comesatthecostofanincreaseinakineticrigidsyndromes.Furthermore,there
isinsufficientdataonthelong-termeffectsofsuchapproaches,andgiventhat
theseagentshavegreatpropensitytocauseTS,additionalpotentdopaminergic
blockadeisnotrecommendedasatreatmentstrategyinTS[60].
Fortardivedystonia,botulinumtoxinisaneffectiveoption[23].Trihexyphenidyl
canalsoimprovedystonicsyndromes,thoughoccasionallyatthecostof
worseningdyskinesia.
Forbothtardivedyskinesiaanddystonia,anapproachwhichisgaining
increasingrecognitionisthatoffunctionalneurosurgery.Indeed,pallidaldeep
brainstimulationcanbegreatlybeneficial,andearlyreferraltoacentrewith
experienceinthisprocedureshouldbeencouragedinrefractoryordebilitating
cases[62].Physiciansmaybereluctanttorecommendthisprocedureduetothe
riskofworseningunderlyingpsychiatriccomorbidity,thoughinpractice,thisis
seldomanissue,especiallywithpallidaltargets[62].Pallidotomycanalsobeen
consideredinpoorsurgicalcandidates.
Tardiveakathisiacanbeequallybothersome,butthereisadearthofevidence
regardingitsoptimaltreatment.Clonidine,moclobemide,benzodiazepinesand
evenelectroconvulsivetherapy(ECT)hasbeenusedinsomeinstances,with
varyingdegreesofsuccess[63–66].Tardivepainsyndromesoftenrespondto
VMAT-2inhibitors,thoughotheroptionssuchasECThavebeenused[43].
Withdrawalemergentdyskinesiaoftensettlesspontaneouslyoverafewweeks
withouttreatment.Severesymptomscanhoweverbemanagedby
reintroductionoftheoffendingdrug,followedbyaslowertaper.
Patientoutcomes
Inanidealworld,patientsdevelopingTSwouldhavetheircausativeneuroleptic
treatmentstopped.Then,andonlythen,couldthetruereversibilityofthe
syndromebeassessed.Thenatureofpsychiatricdiseasehowevermeansthat
ongoingtreatmentisoftennecessary,makingassessmentofTSoutcomes
difficult.PredictorsofpooroutcomeappearsimilartothoseofdevelopingTSin
thefirstplace,andincludeadvancedage,longerdurationofantipsychotic
treatmentandgreatercumulativedose[67].Onceestablished,TSseverityoften
fluctuatesovertime,thoughinasignificantproportion,theTSfailsto
resolve[56,68].
Keypoints
• Tardivesyndromesoftencompriseamultitudeofcharacteristic
movementdisorders.Eachoftheseshouldbecarefullyexaminedforin
suspectcases.
• ClozapineisthedrugofchoiceforpatientswithTSwhorequireongoing
neuroleptictreatment
• VMAT-2inhibitorssuchastetrabenazine,deutetrabenazineand
valbenazinearethebestmedicaltreatmentoptionsfortardivedyskinesia
• Pallidaldeepbrainstimulationisaneffectivetreatmentoptionin
refractoryordebilitatingtardivesyndromes
Acknowledgments
Nil
CompetingInterests
Nil
Fundingdeclaration
Thisresearchreceivednospecificgrantfromanyfundingagencyinthepublic,
commercialornot-for-profitsectors
References
1 FaurbyeA,RaschP-J,PetersenPB,etal.NEUROLOGICALSYMPTOMSIN
PHARMAGOTHERAPYOFPSYCHOSES.ActaPsychiatrScand1964;40:10–
27.doi:10.1111/j.1600-0447.1964.tb05731.x
2 BrowneS,RoeM,LaneA,etal.Qualityoflifeinschizophrenia:relationship
tosociodemographicfactors,symptomatologyandtardivedyskinesia.Acta
PsychiatrScand1996;94:118–24.doi:10.1111/j.1600-
0447.1996.tb09835.x
3 BallesterosJ,González-PintoA,BulbenaA.TardiveDyskinesiaAssociated
WithHigherMortalityinPsychiatricPatients:ResultsofaMeta-Analysisof
SevenIndependentStudies.JClinPsychopharmacol2000;20:188–94.
doi:10.1097/00004714-200004000-00011
4 LernerV,MiodownikC.MotorSymptomsofSchizophrenia:IsTardive
DyskinesiaaSymptomorSideEffect?AModernTreatment.Curr
PsychiatryRep2011;13:295–304.doi:10.1007/s11920-011-0202-6
5 DresslerD.Tardivedystonicsyndromeinducedbythecalcium-channel
blockeramlodipine.JNeuralTransm2014;121:367–9.
doi:10.1007/s00702-013-1108-8
6 CaroffSN,HurfordI,LybrandJ,etal.MovementDisordersInducedby
AntipsychoticDrugs:ImplicationsoftheCATIESchizophreniaTrial.Neurol
Clin2011;29:127–48.doi:10.1016/j.ncl.2010.10.002
7 WoodsSW,MorgensternH,SaksaJR,etal.IncidenceofTardiveDyskinesia
WithAtypicalVersusConventionalAntipsychoticMedications.JClin
Psychiatry2010;71:463–74.doi:10.4088/JCP.07m03890yel
8 LeuchtS,KisslingW,DavisJM.Second-generationantipsychoticsfor
schizophrenia:canweresolvetheconflict?PsycholMed2009;39:1591.
doi:10.1017/S0033291709005455
9 CarbonM,KaneJM,LeuchtS,etal.Tardivedyskinesiariskwithfirst-and
second-generationantipsychoticsincomparativerandomizedcontrolled
trials:ameta-analysis.WorldPsychiatry2018;17:330–40.
doi:10.1002/wps.20579
10 MillerDD,CaroffSN,DavisSM,etal.Extrapyramidalside-effectsof
antipsychoticsinarandomisedtrial.BrJPsychiatry2008;193:279–88.
doi:10.1192/bjp.bp.108.050088
11 SolmiM,MurruA,PacchiarottiI,etal.Safety,tolerability,andrisks
associatedwithfirst-andsecond-generationantipsychotics:astate-of-the-
artclinicalreview.TherClinRiskManag2017;Volume13:757–77.
doi:10.2147/TCRM.S117321
12 D’AbreuA,AkbarU,FriedmanJH.Tardivedyskinesia:Epidemiology.J
NeurolSci2018;389:17–20.doi:10.1016/j.jns.2018.02.007
13 JesteDV.,WyattRJ.Changingepidemiologyoftardivedyskinesia:an
overview.AmJPsychiatry1981;138:297–309.doi:10.1176/ajp.138.3.297
14 TarsyD,BaldessariniRJ.Epidemiologyoftardivedyskinesia:Isrisk
decliningwithmodernantipsychotics?MovDisord2006;21:589–98.
doi:10.1002/mds.20823
15 MorgensternH.IdentifyingRiskFactorsforTardiveDyskinesiaAmong
Long-termOutpatientsMaintainedWithNeurolepticMedications.Arch
GenPsychiatry1993;50:723.
doi:10.1001/archpsyc.1993.01820210057007
16 KaneJM,WoernerM,WeinholdP,etal.Incidenceoftardivedyskinesia:
Five-yeardatafromaprospectivestudy.PsychopharmacolBull1984;20
(3):387–9.
17 YassaR,JesteDV.GenderDifferencesinTardiveDyskinesia:ACritical
ReviewoftheLiterature.SchizophrBull1992;18:701–15.
doi:10.1093/schbul/18.4.701
18 CorriganPW,LibermanRP,EngelJD.FromNoncomplianceto
CollaborationintheTreatmentofSchizophrenia.PsychiatrServ
1990;41:1203–11.doi:10.1176/ps.41.11.1203
19 WonodiI,AdamiHM,CassadySL,etal.EthnicityandtheCourseofTardive
DyskinesiainOutpatientsPresentingtotheMotorDisordersClinicatthe
MarylandPsychiatricResearchCenter.JClinPsychopharmacol
2004;24:592–8.doi:10.1097/01.jcp.0000144888.43449.54
20 KimJ,MacMasterE,SchwartzT.Tardivedyskinesiainpatientstreated
withatypicalantipsychotics:caseseriesandbriefreviewofetiologicand
treatmentconsiderations.DrugsContext2014;3:1–9.
doi:10.7573/dic.212259
21 GoCL,RosalesRL,CaraosRJ,etal.Thecurrentprevalenceandfactors
associatedwithtardivedyskinesiaamongFilipinoschizophrenicpatients.
ParkinsonismRelatDisord2009;15:655–9.
doi:10.1016/j.parkreldis.2009.02.015
22 TeoJT,EdwardsMJ,BhatiaK.Tardivedyskinesiaiscausedbymaladaptive
synapticplasticity:Ahypothesis.MovDisord2012;27:1205–15.
doi:10.1002/mds.25107
23 WalnO,JankovicJ.Anupdateontardivedyskinesia:fromphenomenology
totreatment.TremorOtherHyperkinetMov(NY)2013;3.
doi:10.7916/D88P5Z71
24 KiriakakisV.Thenaturalhistoryoftardivedystonia.Along-termfollow-
upstudyof107cases.Brain1998;121:2053–66.
doi:10.1093/brain/121.11.2053
25 NielsenEB,LyonM.Evidenceforcelllossincorpusstriatumafterlong-
termtreatmentwithaneurolepticdrug(flupenthixol)inrats.
Psychopharmacology(Berl)1978;59:85–9.doi:10.1007/BF00428036
26 GittisAH,LeventhalDK,FensterheimBA,etal.SelectiveInhibitionof
StriatalFast-SpikingInterneuronsCausesDyskinesias.JNeurosci
2011;31:15727–31.doi:10.1523/JNEUROSCI.3875-11.2011
27 DeKeyserJ.ExcitotoxicMechanismsMayBeInvolvedinthe
PathophysiologyofTardiveDyskinesia.ClinNeuropharmacol
1991;14:562–6.doi:10.1097/00002826-199112000-00009
28 LeeH-J,KangS-G.GeneticsofTardiveDyskinesia.In:InternationalReview
ofNeurobiology.2011.231–64.doi:10.1016/B978-0-12-381328-2.00010-
9
29 BhidayasiriR,BoonyawairojS.Spectrumoftardivesyndromes:clinical
recognitionandmanagement.PostgradMedJ2011;87:132–41.
doi:10.1136/pgmj.2010.103234
30 BharuchaKJ,SethiKD.Tardivetourettismafterexposuretoneuroleptic
therapy.MovDisord1995;10:791–3.doi:10.1002/mds.870100613
31 FountoulakisKN,SamaraM,SiaperaM,etal.TardiveTourette-like
syndrome.IntClinPsychopharmacol2011;26:237–42.
doi:10.1097/YIC.0b013e32834aa924
32 StacyM,JankovicJ.Tardivetremor.MovDisord1992;7:53–7.
doi:10.1002/mds.870070110
33 KerteszDP,SwartzMV,TadgerS,etal.TetrabenazineforTardiveTremor
inElderlyAdults.ClinNeuropharmacol2015;38:23–5.
doi:10.1097/WNF.0000000000000061
34 LittleJT,JankovicJ.Tardivemyoclonusa.MovDisord1987;2:307–11.
doi:10.1002/mds.870020408
35 TominagaH,FukuzakoH,IzumiK,etal.TARDIVEMYOCLONUS.Lancet
1987;329:322.doi:10.1016/S0140-6736(87)92042-3
36 KuoS-H,JankovicJ.Tardivegait.ClinNeurolNeurosurg2008;110:198–
201.doi:10.1016/j.clineuro.2007.09.013
37 HunterR,EarlCJ,ThornicroftS.ToxicityofPsychotropicDrugs.ProcRSoc
Med1964;57:758–62.doi:10.1177/003591576405700835
38 RichMW,RadwanySM.RespiratoryDyskinesia.Chest1994;105:1826–32.
doi:10.1378/chest.105.6.1826
39 SuzukiT,MatsuzakaH.Drug-InducedPisaSyndrome(Pleurothotonus).
CNSDrugs2002;16:165–74.doi:10.2165/00023210-200216030-00003
40 MejiaNI,JankovicJ.Tardivedyskinesiaandwithdrawalemergent
syndromeinchildren.ExpertRevNeurother2010;10:893–901.
doi:10.1586/ern.10.58
41 SachdevP.Tardiveandchronicallyrecurrentoculogyriccrises.MovDisord
1993;8:93–7.doi:10.1002/mds.870080117
42 FitzGeraldPM,JankovicJ.Tardiveoculogyriccrises.Neurology
1989;39:1434–1434.doi:10.1212/WNL.39.11.1434
43 FordB,GreeneP,FahnS.Oralandgenitaltardivepainsyndromes.
Neurology1994;44:2115–2115.doi:10.1212/WNL.44.11.2115
44 MicheliF,PardalMF,GattoM,etal.BruxismSecondarytoChronic
AntidopaminergicDrugExposure.ClinNeuropharmacol1993;16:315–23.
doi:10.1097/00002826-199308000-00003
45 LANERD,GLAZERWM,HANSENTE,etal.AssessmentofTardive
DyskinesiaUsingtheAbnormalInvoluntaryMovementScale.JNervMent
Dis1985;173:353–7.doi:10.1097/00005053-198506000-00005
46 BalintB,KillaspyH,MarstonL,etal.Developmentandclinimetric
assessmentofanurse-administeredscreeningtoolformovement
disordersinpsychosis.BJPsychOpen2018;4:404–10.
doi:10.1192/bjo.2018.55
47 LernerPP,MiodownikC,LernerV.Tardivedyskinesia(syndrome):
Currentconceptandmodernapproachestoitsmanagement.Psychiatry
ClinNeurosci2015;69:321–34.doi:10.1111/pcn.12270
48 FentonWS.Prevalenceofspontaneousdyskinesiainschizophrenia.JClin
Psychiatry2000;61:10–4.
49 PelusoMJ,LewisSW,BarnesTRE,etal.Extrapyramidalmotorside-effects
offirst-andsecond-generationantipsychoticdrugs.BrJPsychiatry
2012;200:387–92.doi:10.1192/bjp.bp.111.101485
50 CorrellCU,SchenkEM.Tardivedyskinesiaandnewantipsychotics.Curr
OpinPsychiatry2008;21:151–6.doi:10.1097/YCO.0b013e3282f53132
51 ErtugrulA,DemirB.Clozapine-inducedtardivedyskinesia:Acasereport.
ProgNeuro-PsychopharmacologyBiolPsychiatry2005;29:633–5.
doi:10.1016/j.pnpbp.2005.01.014
52 KumarH,JogM.MissingHuntington’sDiseaseforTardiveDyskinesia:A
PreventableError.CanJNeurolSci/JCandesSciNeurol2011;38:762–4.
doi:10.1017/S0317167100012294
53 BalintB,VincentA,MeinckH-M,etal.Movementdisorderswithneuronal
antibodies:syndromicapproach,geneticparallelsandpathophysiology.
Brain2018;141:13–36.doi:10.1093/brain/awx189
54 TitulaerMJ,McCrackenL,GabilondoI,etal.Treatmentandprognostic
factorsforlong-termoutcomeinpatientswithanti-NMDAreceptor
encephalitis:anobservationalcohortstudy.LancetNeurol2013;12:157–
65.doi:10.1016/S1474-4422(12)70310-1
55 KollerWC.Edentulousorodyskinesia.AnnNeurol1983;13:97–9.
doi:10.1002/ana.410130121
56 GardosG,CaseyDE,ColeJO,etal.Ten-yearoutcomeoftardivedyskinesia.
AmJPsychiatry1994;151:836–41.doi:10.1176/ajp.151.6.836
57 KaneJM,WoernerMG,PollackS,etal.Doesclozapinecausetardive
dyskinesia?JClinPsychiatry1993;54(9):327–30.
58 PardisP,RemingtonG,PandaR,etal.Clozapineandtardivedyskinesiain
patientswithschizophrenia:Asystematicreview.JPsychopharmacol
2019;33:1187–98.doi:10.1177/0269881119862535
59 MentzelTQ,vanderSnoekR,LieverseR,etal.ClozapineMonotherapyasa
TreatmentforAntipsychotic-InducedTardiveDyskinesia.JClinPsychiatry
2018;79.doi:10.4088/JCP.17r11852
60 BhidayasiriR,FahnS,WeinerWJ,etal.Evidence-basedguideline:
Treatmentoftardivesyndromes.Neurology2013;81(5):463–9.
61 ToumaKTB,ScarffJR.ValbenazineandDeutetrabenazineforTardive
Dyskinesia.InnovClinNeurosci2018;15:13–6.
62 MacerolloA,DeuschlG.Deepbrainstimulationfortardivesyndromes:
Systematicreviewandmeta-analysis.JNeurolSci2018;389:55–60.
doi:10.1016/j.jns.2018.02.013
63 PengL-Y,LeeY,LinP-Y.ElectroconvulsiveTherapyforaPatientWith
PersistentTardiveDyskinesia.JECT2013;29:e52–4.
doi:10.1097/YCT.0b013e31829e0aea
64 AmannB,ErfurthA,GrunzeH.Treatmentoftardiveakathisiawith
clonidine:acasereport.IntJNeuropsychopharmacol
1999;2:S1461145799001376.doi:10.1017/S1461145799001376
65 EmmanuelT.Remissionoftreatment-resistantdepressionwithtardive
akathisiawithelectroconvulsivetherapy.BMJCaseRep2019;12:e229714.
doi:10.1136/bcr-2019-229714
66 EbertD,DemlingJ.SuccessfulTreatmentofTardiveAkathisiawith
Moclobemide,aReversibleandSelectiveMonoamine-Oxidase-AInhibitor.
Pharmacopsychiatry1991;24:229–31.doi:10.1055/s-2007-1014473
67 CavallaroR,RegazzettiMG,MundoE,etal.TardiveDyskinesiaOutcomes:
ClinicalandPharmacologicCorrelatesofRemissionandPersistence.
Neuropsychopharmacology1993;8:233–9.doi:10.1038/npp.1993.26
68 KaneJM,WoernerM,BorensteinM,etal.Integratingincidenceand
prevalenceoftardivedyskinesia.PsychopharmacolBull1986;22:254–8.